Amyloidose aus Sicht eines Nephrologen - Thomas Reiter Klin. Abteilung für Nephrologie & Dialyse Univ.-Klinik für Innere Medizin III - Innere ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Amyloidose aus Sicht eines Nephrologen Thomas Reiter Klin. Abteilung für Nephrologie & Dialyse Univ.-Klinik für Innere Medizin III
Interessenskonflikte
• Amgen Reiseunterstützung
• Janssen Cilag nationales Advisory Board
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 2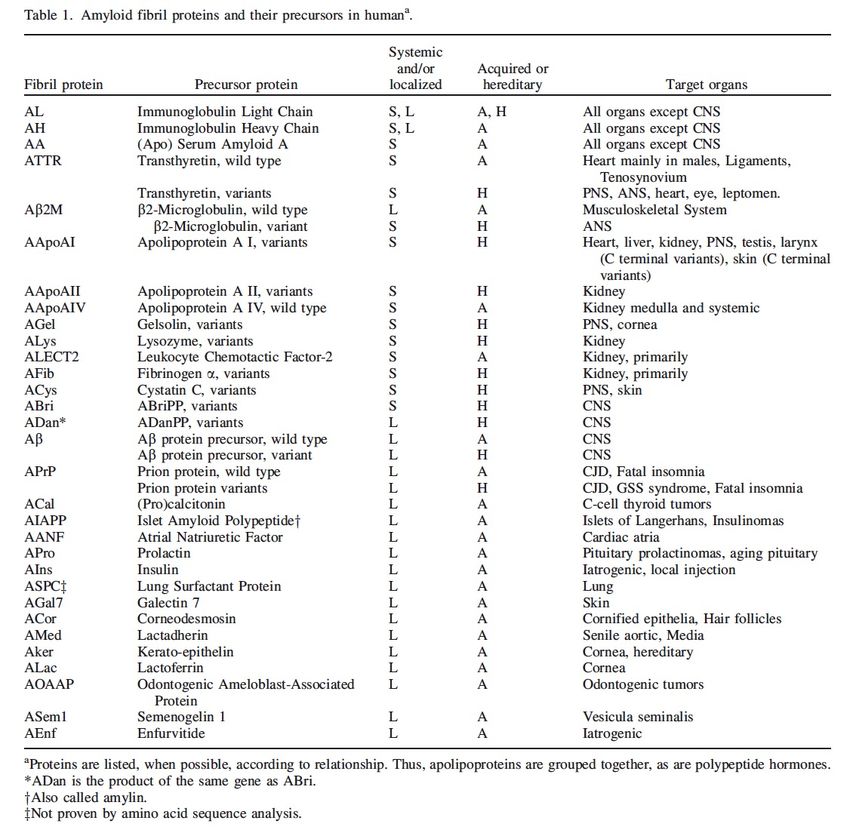
Inhalt
1. Einleitung - Was ist Amyloid?
2. Renale Amyloidosen
3. Kurzer Refresher – renale Anatomie/Physiologie
4. Diagnostik
5. Therapiemöglichkeiten
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 3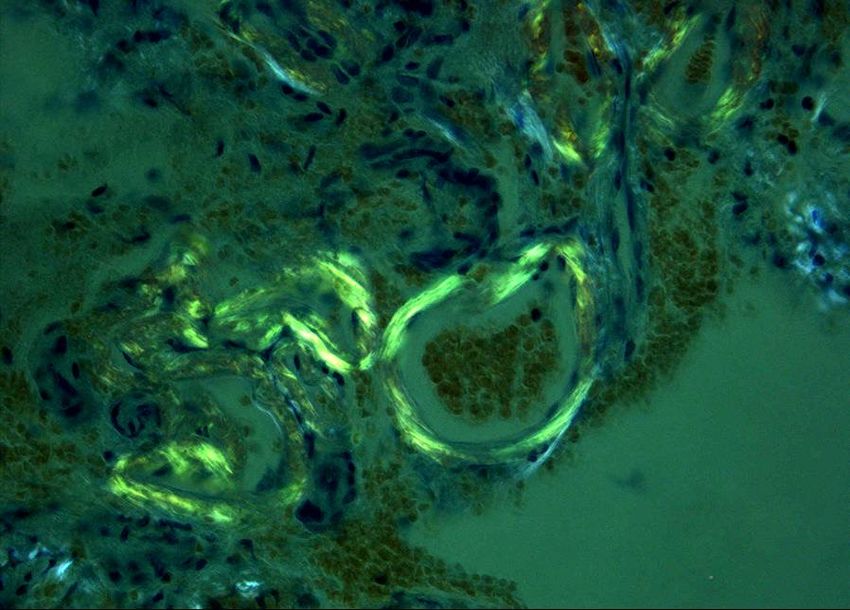
Was ist Amyloidose?
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 4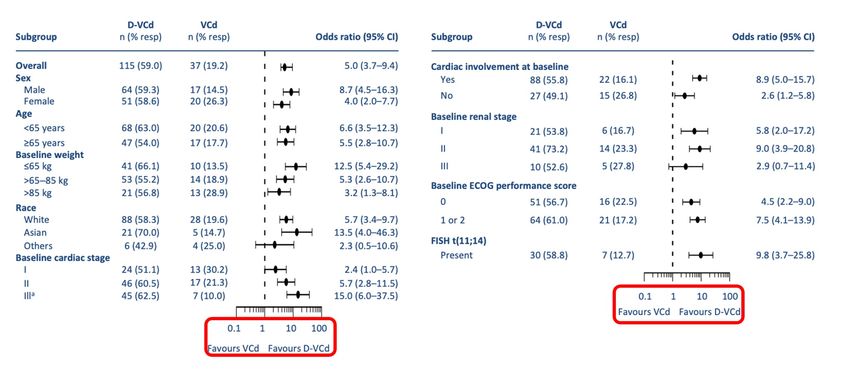
In a cell, proteins are synthesized on ribosomes from the genetic chaperone, contains a cavity in which incompletely folded polypep-
information encoded in the cellular DNA. Folding in vivo is in some tide chains can enter and undergo the final steps in the formation of
cases co-translational; that is, it is initiated before the completion of their native structures while sequestered and protected from the
protein synthesis, whereas the nascent chain is still attached to the outside world.
ribosome26. Other proteins, however, undergo the major part of their Molecular chaperones do not themselves increase the rate of indi-
folding in the cytoplasm after release from the ribosome, whereas yet vidual steps in protein folding; rather, they increase the efficiency of
others fold in specific compartments, such as mitochondria or the the overall process by reducing the probability of competing reac-
endoplasmic reticulum (ER), after trafficking and translocation tions, particularly aggregation. However, there are several classes of
through membranes27,28. Many details of the folding process depend folding catalyst that accelerate potentially slow steps in the folding
on the particular environment in which folding takes place, although process. The most important are peptidylprolyl isomerases, which
the fundamental principles of folding, discussed above, are undoubt- increase the rate of cis–trans isomerization of peptide bonds involving
edly universal. But because incompletely folded proteins must proline residues, and protein disulphide isomerases, which enhance
Synthese von Proteinen
inevitably expose to the solvent at least some regions of structure that
are buried in the native state, they are prone to inappropriate interac-
tion with other molecules within the crowded environment of a cell29.
the rate of formation and reorganization of disulphide bonds30.
Despite these factors, given the enormous complexity and the stochas-
tic nature of the folding process, it would be remarkable if misfolding
Living systems have therefore evolved a range of strategies to prevent never occurred. Clear evidence that molecular chaperones are needed
such behaviour27–29. to prevent misfolding and its consequences comes from the fact that
the concentrations of many of these species are substantially increased
Ribosome
Globuläre Form von
during cellular stress; indeed, the designation of many as heat shock
proteins (Hsps) reflects this fact. It is also clear that some molecular
Transport out
Transport
in Funktionsproteinen ist
chaperones are able not only to protect proteins as they fold but also to
rescue misfolded and even aggregated proteins and enable them to
Voraussetzung für:
have a second chance to fold correctly27,28. Active intervention in the
Misfolded Modification folding process requires energy, and ATP is required for most of the
and folding
U biquitin- molecular chaperones to function with full efficiency.
proteasome In eukaryotic systems, many of the proteins that are synthesized in
system
a cell are destined for secretion to the extracellular environment.
• Proteinlöslichkeit
These proteins are translocated into the ER, where folding takes place
C orrectly before secretion through the Golgi apparatus. The ER contains a wide
folded range of molecular chaperones and folding catalysts, and in addition
the proteins that fold here must satisfy a ‘quality-control’ check • korrekte Interaktion
before being exported (Fig. 2)31,32. Such a process is particularly
important because there seem to be few molecular chaperones out- - Protein & Protein
side the cell, although one (clusterin), at least, has recently been dis-- Protein &
covered33. This quality-control mechanism involves a remarkable
Degraded ER
series of glycosylation and deglycosylation reactions that enables cor-
microenvironment
protein
31
rectly folded proteins to be distinguished from misfolded ones . The
importance of these regulatory systems is underlined by recent
experiments that suggest that a large fraction of all polypeptide • effiziente, schnelle
Vesicle
degradation34. Like the ‘heat shock response’ in the cytoplasm, the
Konformationsänderung
chains synthesized in a cell fail to pass this test and are targeted for
‘unfolded protein response’ in the ER is also stimulated (upregulated)
during stress and, as we shall see below, is strongly linked to the avoid-
➜ Aktivität
G olgi
ance of misfolding diseases35.
Figure 2 Regulation of protein folding in the ER. Many newly synthesized proteins Folding and unfolding are the ultimate ways of generating and
are translocated into the ER, where they fold into their three-dimensional structures abolishing specific types of cellular activity. In addition, processes as
with the help of a series of molecular chaperones and folding catalysts (not shown). apparently diverse as translocation across membranes, trafficking,
Correctly folded proteins are then transported to the Golgi complex and then secretion, the immune response and regulation of the cell cycle are
delivered to the extracellular environment. However, incorrectly folded proteins are
detected by a quality-control mechanism and sent along another pathway (the
Dobson CM, Nature 2003; 426(6968):884-90
directly dependent on folding and unfolding events2. Failure to fold
correctly, or to remain correctly folded, will therefore give rise to the
unfolded protein response) in which they are ubiquitinated and then degraded in the malfunctioning of living systems and hence to disease36–38. Some of
36 39
cytoplasm by proteasomes. Adapted from ref. 32. these diseases (such as cystic fibrosis and some
Amyloidose austypes
Sichtof
descancer )
Nephrologen
result from proteins folding incorrectly
Wien, and not being able to exercise
21.06.2022 5
886 © 2003 Nature Publishing GroupNATURE | VOL 426 |18/25 DECEMBER 2003 | www.nature.com/nature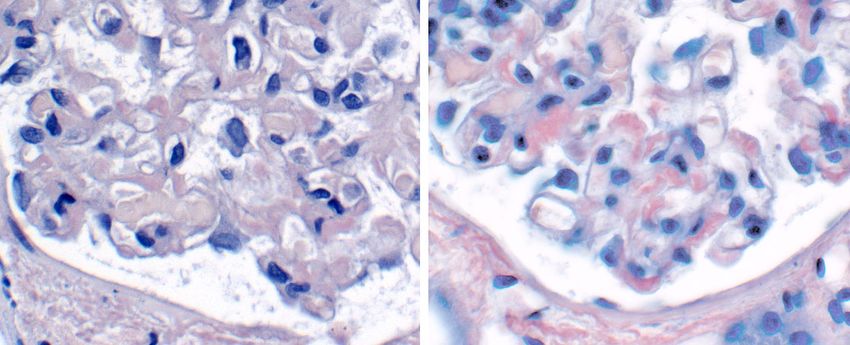
Proteinstruktur
Primärstruktur
(Aminosäuresequenz)
lokale Einheit
(Sekundärstruktur)
Untereinheit
(Tertiärstruktur)
Komplex
(Quartärstruktur)
Linderstrøm-Lang KU,1952; Lane Medical Lectures;6:1-115
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 6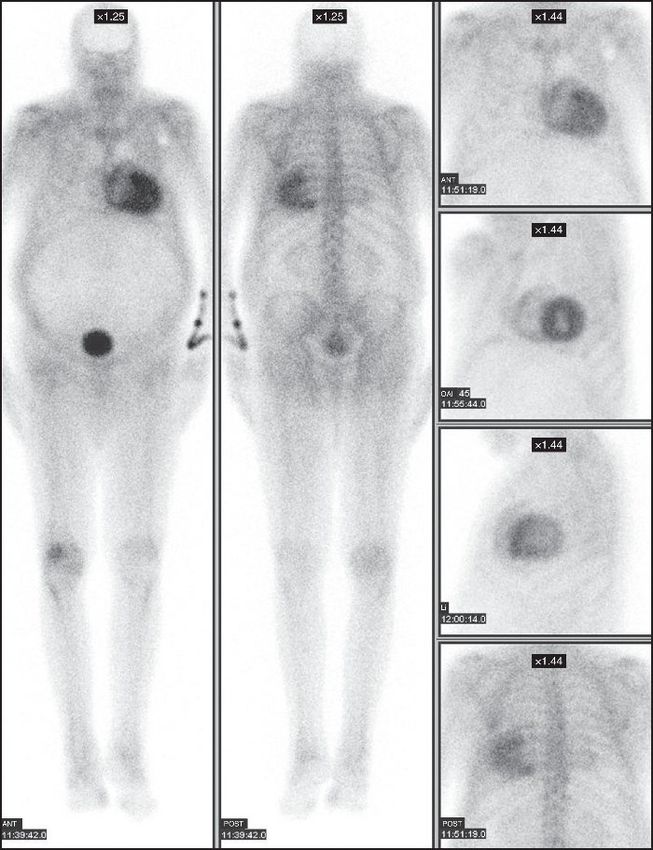
Bildung von Amyloid
• Störung in der Synthese, • Protein-abhängig
dem Abbau und dem
- Mutation
Gleichgewicht von Proteinen - hohe Bildungsrate
- Instabilität
führen zu Fehlfaltungen (β-
Faltblatt) • „Microenvironment“-
abhängig
• Fibrillen (≈ 10 nm), unlöslich
- niedriger pH
und aggregieren zu - hohe Temperatur
- Alter
➜ Amyloid
Merlini G, N Engl J Med 2003;349:583-595
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 7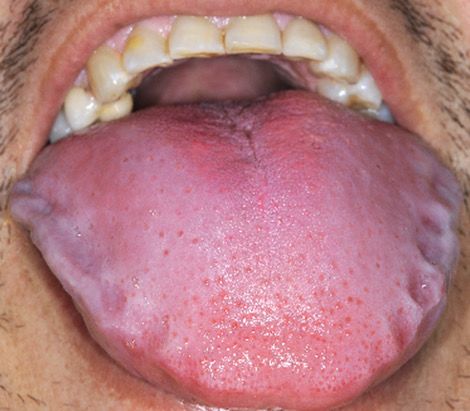
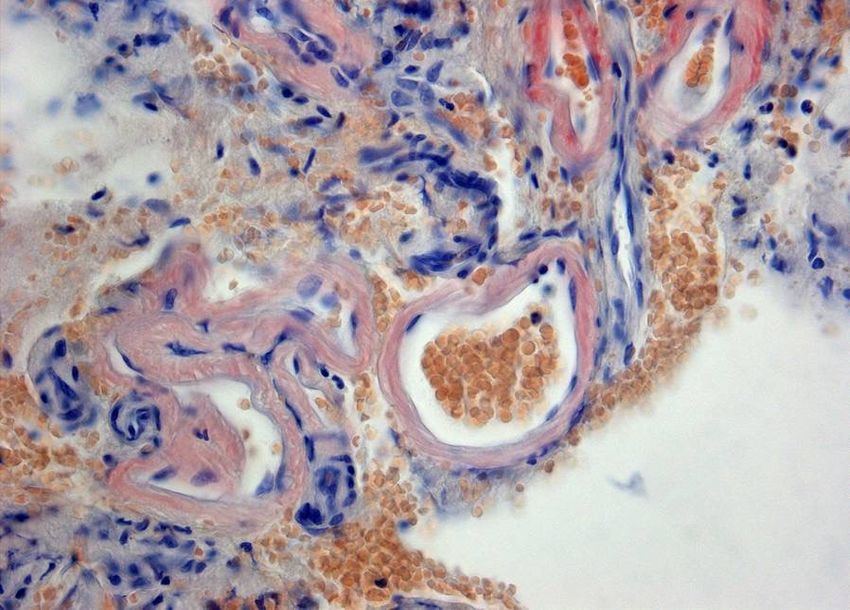
Eigenschaften von Amyloid
• heterogene Proteine mit homogener Strukturbildung
- Interaktion mit Extrazellulärmatrix und Gylkosaminoglykanen
- immer Beteiligung von Serum Amyloid P (SAP)
• β-Faltblattstruktur führt zur Aufnahme von Kongorot
➜ alle Arten färben Kongorot mit grüner Doppelbrechung im Phasenkontrast
• charakteristische Fibrillen (7,5 – 10 nm) in der Elektronenmikroskopie
• keine physiologische Funktion
Merlini G, N Engl J Med 2003;349:583-595
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 8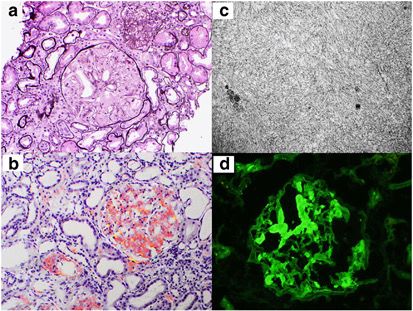
Eigenschaften von Amyloid
Abb. 1 Abb. 2
Amyloid-Angiopathie, Kongorot Amyloid-Angiopathie, grün doppelbrechend im
Wiki Commons, 2009 Phasenkontrast
Wiki Commons, 2009
Abb. 3
Amyloidfibrille im Elektronenmikroskop
Dobson CM, Nature, 2003; 426(6968):884-90
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 9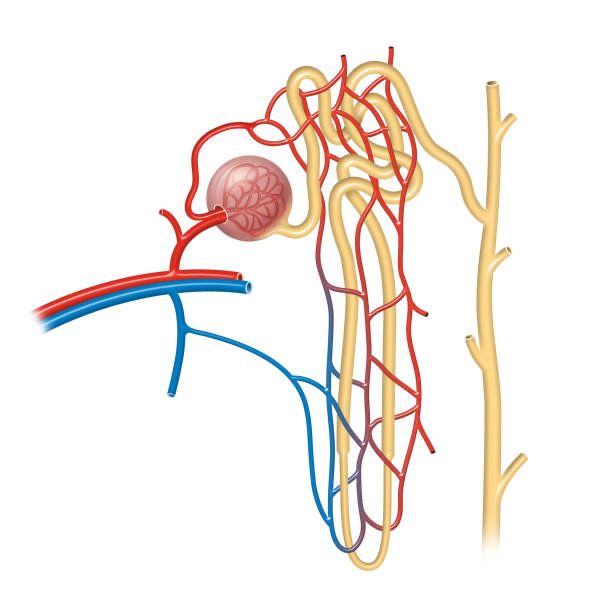
Amyloidose
• Ablagerung und Anhäufung von unlöslichen, fibrillären
Proteinen in Geweben, die zum Organversagen und zum
Tod führen kann
Sipe J D, Amyloid, 2014;21(4):221-224
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 10Bekannte Typen der Amyloidose
• > 280
bekannte
Precursor!
Sipe J D, Amyloid, 2014;21(4):221-224
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 11Renale Amyloidosen
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 12Amyloidosen mit renaler Beteiligung
Bezeichnung Protein Lokalisation
AL Ig Leichtketten systemisch, Niere
AH Ig schwere Ketten systemisch, Niere
AA Serum Amyloid A systemisch, Niere
AApoAI Apolipoprotein AI Niere, Haut, Larynx
AApoAII Apoliporotein AII Niere
AApoAIV Apolipoprotein AIV Niere
ALECT2 Leukocyte chemotactic Niere
factor-2
AFib Fibrinogen α Niere, primär
ALys Lyszym Niere
nach: Khalighi MA, Clin Kidney J 2014;7:97-106
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 13AL(ight)-/AH(eavy)-/AHL(heavy/light)-Amyloidose
• Precursor-Protein:
Schwere oder Leichte Ketten(anteile) von Immunglobulinen ➔
Paraproteine
AL (> AH > AHL), Verhältnis λ:κ = 3:1 Gertz MA, Kidney Int, 2002;61:1-19
• Assoziation mit Multiplem Myelom und MGUS, aber eigene
Krankheitsentität
• heute häufigste Form der systemischen und renalen Amyloidose
(68 -81%) Bergesio F, Nephrol Dial Transplant, 2008;23:941-951
• 50% der AL-Amyloidosen manifestieren sich
primär/ausschließlich renal
• Lokalisation renal:
vorwiegend glomerulär, aber überall möglich
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 14AL-Amyloidose
• alle Immunglobulinklassen möglich
• freie Leichtketten (fLC) in der Serumelektropherese oft nicht ersichtlich ➜
Immunfixation obligat!
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 15AA-Amyloidose
• Precursor-Protein:
Serum Amyloid-A (SAA1, SAA2)
• zweithäufigste systemische Amyloidose, 30% der renalen
Amyloidosen Bergesio F, Nephrol Dial Transplant, 2008;23:941-951
• sekundäre Erkrankung, Ursache immer Aktivierung des
Inflammasoms:
- Chronische Polyarthritis, andere rheumatische Erkrankungen
- Chronisch entzündliche Darmerkrankungen (Mb. Crohn, CU)
- Chronische Infekte
- Periodische Fiebersyndrome (Familiäres Mittelmeerfieber)
- Castleman-Syndrom
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 16AA-Amyloidose
• Nierenbeteiligung ist die häufigste Affektion bei AA!
• 97% der PatientInnen haben Proteinurie > 500 mg/d und/oder ein Serumkreatinin >1,5
mg/dL
• Nephrotisches Syndrom häufig
Lachmann HJ, N Engl J Med 2007;356:2361-2371
• Lokalisation renal:
- vorwiegend glomerulär, aber häufig tubulär
- selten durch Aktivierung von glomerulären endokapillären Leukozyten ➜ crescentic
GN
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 17AA-Amyloidose
Starke Assoziation
Brunger AF, Amyloid 2020;27:1,1-12
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 18AA-Amyloidose
Schwache Assoziation
Brunger AF, Amyloid 2020;27:1,1-12
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 19AA-Amyloidose
Unwahrscheinliche/sehr seltene Assoziation
Brunger AF, Amyloid 2020;27:1,1-12
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 20ALECT2-Amyloidose
• Precursor-Protein:
Leukocyte Chemotactic Factor 2 (LECT2)
• dritthäufigste renale Amyloidose weltweit (3%), vorwiegend PatientInnen mexikanischer und
südamerikanischer Herkunft
• Pathophysiologie nicht voll verstanden
• Pulmo-renales Syndrom möglich!
• Lokalisation renal:
glomerulär und interstitiell
Murphy CL, Am J Kidney Dis 2010;56:1100-1107
Said SM, Mod Pathol 2013;26 (Supp 2):392A
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 21Aβ2-Amyloidose
• Precursor-Protein:
β2-Mikroglobulin
• keine renale sondern ausschließlich neurologische Manifestation
• Dialyse-assoziiert
• heute selten(er)
• Lokalisation:
Peripheres Nervengewebe (häufigste Ursache des Karpaltunnelsyndroms bei RRT & PNP)
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 22Hereditär bedingte Amyloidosen
• Es wird kompliziert...
- ATTR (vorwiegend kardial)
- AFib
- AApoI-IV
- AGel
....Sie werden sehen, alle haben etwas gemeinsam...
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 23Renale Anatomie/Physiologie
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 24Nephron
Glomerulum
- Vas afferens Distaler Tubulus
- Vas efferens
proximaler Tubulus
pars convuluta & pars recta
Sammelrohr
Henle-Schleife
Wiki Commons, 2021
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 25Der Ort entscheidet...
• Präglomeruläre Gefäße
→ fortschreitende Niereninsuffizienz (sinkende GFR) durch eingeschränkte
glomeruläre Perfusion
• Glomerulum
→ Proteinurie (bis zu nephrotischem Syndrom) durch Störung der
Podozyten/“Dichtigkeitsverlust“
• Tubulus
→ distal tubuläre Azidose, Polurie/nephrogener Diabetes insipidus, De
Toni-Fanconi-Syndrom
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 26Klinik & Diagnostik
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 27Suspekt ...
• ...nicht-diabetische PatientInnen mit nephrotischem Syndrom
• ...Hepatomegalie und/oder Splenomegalie
• ...nicht-ischämische Kardiomyopathie mit konzentrischer
Hypertrophie im Echokardiogramm (speckled myocardium)
• ...erhöhtem proBNP ohne Herzerkrankung
• ...alkalische Phosphatase ↑
• ...periphere Neuropathie ohne andere Ursache
• ...unklare Petechien (Kopf & Hals, Augenlider)
• ...Makroglossie
• ...Malabsorption ohne gastrointestinale Grunderkrankung
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 28Seltene, aber typische Auffälligkeiten
Abb.5
„bruised eyelids“
petchiale Einblutungen der
Augenlider
(WikiCommons)
Indontie
Abb. 6
Makroglossie
(Hämatologie, Univ.-Spital Zürich)
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 29Labor & Screening
• Screening nach Proteinurie & LABOR
Niereninsuffizienz Serum
- Pat. mit rheumatologischer Erkrankung • BNP
- Pat. mit Periodischen Fiebersyndromen (FMF) • alkalische Phosphatase
• Gesamteiweiß
- MGUS, MM • Albumin
• Kreatinin
- Neoplasien
Harn
• Protein-/Kreatinin-Quotient
• Albumin-/Kreatinin-
Quotient
• Eiweiß & Albumin 24h-
Sammelharn
Be aware!
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 30Serologische Diagnostik
Weiterführend:
• Serum Amyloid-A, (Protein C)
• Quantitative Ig, Freie (!) Leichtketten Serum & Harn,
Serumelektrophorese, Immunfixation (!) Serum & Harn,
β2-Mikroglobulin
• Troponin T, Troponin I, high sensitive Troponin T
• BNP besser als NT-proBNP (bei ESRD)
Nuovolone M & Merlini G, Nephrol Dial Transplant 2016;0:1-10
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 31Bildgebende Verfahren
für renale Affektion geeignet:
• 123I-SAP-Imaging (nur in GB verfügbar)
• sonst...keine valide Bildgebung!
ABER für kardiale, hepatale, ossäre und gastrointestinale
Beteiligung:
• Abdomensonografie (Hepato- & Splenomegalie)
• Echokardiografie (Septumdicke, „speckled myocardium“, HF/pEF)
• MRT des Herzens (late enhancement)
• SPECT-CT
• Tc99-DPD und Tc99-PYP-Scan
Nienhuis HLA, Kidney Dis 2016;2:10-19
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 32Bildgebende Verfahren
Abb. 7
Tc99-PYP-Scan, kardial positiv
(www.revespcardiol.org)
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 33Invasive Verfahren - Biopsie
• Goldstandard
• keine Biopsie – keine Diagnose
• primär betroffenes Organ wählen
f e !
“Die Nierenbiopsie bei Amyloidose-Patienten ist doch riskant!“
sa
Altindal M, Nephron. 2015;131(1):17-21
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 34Silent Site Biopsy
• Aspiration von subkutanem Fettgewebe
• Knochenmarksbiopsie und –aspiration
• Speicheldrüsenbiopsie
• Fettgewebsbiopsie
• Rektumbiopsie Abb. 8
Fettgewebsaspiration
➜ Sensitiviät der Biopsien ist vergleichbar (55-87%)
Merlini GM, Blood 2013;121:5124-30
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 35Histologie
• schwach eosinophil (HE, PAS)
• blau-grau in der Trichrom-Essig-F.
• negativ in der Silberfärbung
• Lachsrot nativ, apfelgrün im Phasenkontrast
(Kongorot)
• Typisch fibrilläre Struktur im
Elektronenmikroskop
Abb. 9
(a) HE
(b) Elektronenmikroskopie
(c) Kongo-Rot
(d) Phasenkontrast
Bridoux F, Kidney Int.,2015;87(4):698-711
Amyloidose aus Sicht des Nephrologen
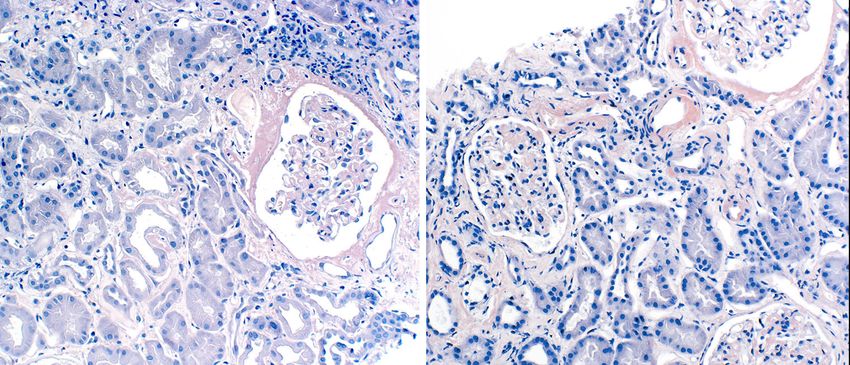
Wien, 21.06.2022 36Die Schnittdicke macht’s!
Abb. 10 renale Amyloidose, Kongorot;
Schnittdicke links - 2 μm Schnittdicke, rechts – 6 μm;
(Kain R., Wien)
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 37Die Schnittdicke macht’s!
Abb. 11 renale Amyloidose, Kongorot;
Schnittdicke links - 2 μm Schnittdicke, rechts – 6 μm;
(Kain R., Wien)
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 38Klassifizierung von Amyloid
• Immunhistochemie
- bei AL-Amyloidose fast nutzlos
• Laser Capture Dissection & Tandem Mass Spectroscopy (LCD/MS)
• Proteomics
Nienhuis HLA, Kidney Dis 2016;2:10-19
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 39Diagnoseweg
Amyloidose?
Systemische Beteiligung
Biopsie
LCD/MS & Proteomics
Immunhistochemie
Diagnose
Nienhuis HLA, Kidney Dis 2016;2:10-19
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 40Therapie
Was nun?
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 41Therapieentscheidung
• Zustand des/der Patienten/Patientin?
- Alter
- Frailty
- Grunderkrankung
- CKD-Stadium
• unterscheidet sich erheblich für die verschiedenen Typen
der Amyloidose
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 422 Säulen der Therapie
• Suppression der Bildung des amyloidogenen Proteins
(Precursor-Product Concept)
und
• Elimination der Amyloiddepots
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 43AA-Amyloidose(n)
Beseitigung der Ursache für die Entzündungsreaktion
• Sanierung des Infektherdes (Tbc, Abszesse,...)
• Kontrolle der Grunderkrankung (CP)
- Biologika, Biosimilars
• Familiäres Mittelmeerfieber
- Colchicin (SAA < 3 mg/dL)
und
- IL-1-Hemmung (Anakinra, Canakinumab), IL-6-Hemmung (Tocilizumab)
Nierentransplantation
Spezifische Therapie
• Eprodisate, Glykosaminoglykanmodifikation (Phase III, NCT01215747)
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 44AL-/AH-/AHL-Amyloidose
• bislang anhand verfügbarer Therapie für MM
• Ziel ist die Reduktion des Paraproteins unter die Nachweisbarkeitsgrenze
• High-Dose Melphalan und Autologe Stammzelltransplantation (ASCT)
oder
• Dexamethason und
• Proteasominhibitoren (Bortezomib, Ixazomib, Carfilzomib) und
• Immunmodulatory drugs (IMiDs) (Thalidomid, Lenalidomid, Pomalidomid)
oder
• Alkylierende Substanzen (Melphalan, Cyclophosphamid)
• Trials mit humanisierten Antikörpern (zB. NEOD001)
Nuvolone M & Merlini, Nephrol Dial Transplant 2016;0:1-10
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 45AL-/AH-/AHL-Amyloidose
• Patienten mit AL-Amyloidose und kompletter
hämatologischer Remission unterscheiden sich im OS
deutlich von Myelom-Patienten
Unterschiedliche Biologie!
Andere Erkrankung!
Dispenzieri A, Bone Marrow
Transplantion 2013;48:1302-1307
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 46AL-Amyloidosen
Therapien – neue Agenten
• Daratumumab
(CD38-Antikörper)
• seit Ende 2020 auch first line
für AL-Amyloidose zugelassen
Kastritis E, N Eng J Med, 2021;385:46-58 (ANDROMEDA)
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 47AL-Amyloidosen
Therapien – Daratumumab
Kastritis E, N Eng J Med, 2021;385:46-58 (ANDROMEDA)
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 48AL-Amyloidosen
Therapien – neue Agenten
• CAEL-101 (mAb 11-1F4)
• Monoklonaler Antikörper
• direkt antifibrillär (AL)
• Amyloid-Depots durch Phagocytose aufgelöst
• Phase Ia/Ib (67% response rate kardial und renal)
Edwards C, Blood, 2021, 138 (25): 2632–2641
Amyloidose aus Sicht eines Nephrologen
Wien, 21.06.2022 49Hereditär bedingte Amyloidosen
• Nur für wenige Proteine steht eine spezifische Therapie zur Verfügung
• Ausnahme: ATTR (-mut/-wt)
- Tafamidis (Vyndaquel®)
- Tolcaptone (NCT02191826)
• Organtransplantion (Leber > Niere)
Nuvolone M & Merlini, Nephrol Dial Transplant 2016;0:1-10
Maurer M, N Engl J Med 2018 Sep 13;379(11):1007-1016
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 50universelle Anti-Amyloid-Therapien
• 4‘-Iodo-4‘Deoxy-Doxorubicin → keine Wirksamkeit nachgewiesen
• Doxycyclin → keine Wirksamkeit nachgewiesen
• Tauroursodesoxycholsäure → keine Wirksamkeit nachgewiesen
• Epigallochatecin-3-gallat (EGCG) → keine Wirksamkeit nachgewiesen
- Inhaltsstoff des Grüntees
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 51Zusammenfassung
• Amyloidose ist eine durch Protein-Fehlfaltung (misfolding disease) verursachte
Erkrankung.
• Amyloidose führt unbehandelt zum Tod.
• Bis zu 60% der Amyloidosen zeigen primär renale Symptomatik
• Es stehen zunehmend Therapien zur Verfügung.
- AA – Stop inflammation!
- AL – Eradicate the clone!
Be aware!
There‘s hope!
Amyloidose aus Sicht des Nephrologen
Wien, 21.06.2022 52You can also read

















































