American College of Endocrinology Position Statement on the Insulin Resistance Syndrome
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
American College of Endocrinology
Position Statement on the Insulin Resistance Syndrome*
*By the American College of Endocrinology Task Force on the Insulin Resistance Syndrome.
Presented at the National Press Club, Washington, DC, August 27, 2002.
Reprinted from Endocr Pract. 2003;9(No. 3):236-252.
ENDOCRINE PRACTICE Vol 9 (Suppl 2) September/October 2003 5Executive Summary
INTRODUCTION members at risk, treatment for individual components as
soon as cut points are crossed, enrollment into research
Daniel Einhorn, MD, FACP, FACE studies and, possibly, prevention of the disease conse-
quences of IRS. The potential role of pharmacology was
The work presented in this Endocrine Practice report reviewed, and remains one of the more challenging
reflects the commitment of the American Association of questions.
Clinical Endocrinologists (AACE) and the American Due to the complex and rapidly evolving nature of
College of Endocrinology (ACE) to provide leadership this field, the Task Force recognized it could not issue
and guidance on public health issues that involve clinical definitive clinical “guidelines” in the usual sense until
endocrinology. This material was originally presented at more data were available. Therefore, as a complement to
the National Press Club in Washington, DC, on August the Position Paper, a Conference on the Insulin Resistance
27, 2002. Syndrome was convened in Washington, DC, August 25-
The Position Paper presents the official position of 26, 2002. The proceedings of that conference will be
AACE/ACE, authored by the members of the Task Force published separately; the presenters and participants are
appointed by the AACE President. Faced with an listed in the Appendix.
absence of definitive studies, the Task Force used the best Special thanks to Drs. Gerald Reaven and Earl Ford
available evidence to make its recommendations. for providing leadership in development of the paper, and
The National Cholesterol Education Program (NCEP) Dr. Yehuda Handelsman for organization of the
Adult Treatment Panel (ATP III) definition of the Conference.
Metabolic Syndrome has been extremely successful in pop- Finally, the Task Force acknowledges a great debt to
ularizing the concept of the clustering of blood pressure, the many colleagues and friends of AACE/ACE who gave
lipid, glycemic and obesity risk factors and the implications informal advice, and who have helped advance the under-
of this cluster. The Task Force adopted the blood pressure standing of insulin resistance.
and lipid criteria. However, the Task Force suggested mod-
ifications to other parts of the definition, including:
– recognizing the limitations of the fasting glucose EXECUTIVE SUMMARY
– recognizing the value of the 2 hour post-chal-
lenge glucose Question 1. What is the Insulin Resistance Syndrome
– adding BMI as a measure of obesity (IRS)?
– classifying obesity as a risk factor rather than a IRS describes a condition that is characterized by
criterion decreased tissue sensitivity to the action of insulin, leading
– adjusting obesity criteria for ethnicity to a compensatory increase in insulin secretion. This meta-
– expanding the list of individuals considered at risk bolic dysfunction leads to a cluster of abnormalities with
– expanding the list of associated disorders. serious clinical consequences, including cardiovascular
disease and type 2 diabetes, polycystic ovary syndrome
The 2 hour post-challenge glucose is recommended (PCOS), nonalcoholic fatty liver disease (NAFLD), and
when individuals at risk (Table 2 of the Position Paper) do other illnesses.
not meet sufficient other criteria for IRS (Table 3) and a
more sensitive test may be needed. It is not suggested for Question 2. What is the clinical impact of the Insulin
use in mass screenings or in every individual at risk. Resistance Syndrome?
There were numerous issues beyond the scope of the One in three to four American adults has IRS; most
Task Force. For example, is there any evidence for treat- are able to produce enough insulin to maintain non-
ment of the IRS beyond treating individual components, diabetic glucose levels. Some of these individuals will go
e.g. elevated blood pressure, dyslipidemia, etc.? Should on to develop overt type 2 diabetes. The majority will not
the cut points for treatment of individual components be develop diabetes, but yet will remain at significant
lower when IRS is present? Should treatment strategies for increased risk for cardiovascular disease and other dis-
individual components be different if IRS is present? eases. Over 90% of the 16 million Americans who have
What might be the implications for an individual’s health type 2 diabetes are insulin resistant. One in ten women
or life insurance if they carried a “diagnosis” of IRS? Are have PCOS, another manifestation of IRS. The current
there any promising new diagnostic tools for IRS? What epidemic of obesity among children and adolescents puts
surrogate markers are of value in IRS? them at increased risk for IRS and its complications.
The Task Force agreed that there was important clin-
ical value in identifying an individual at risk for IRS. The Question 3. Who is at risk to have the Insulin
potential benefits include: early and more aggressive Resistance Syndrome?
lifestyle intervention with nutrition and fitness, closer and The more risk factors an individual has, the greater
more focused medical follow-up, identification of family the likelihood of having IRS.
6 ENDOCRINE PRACTICE Vol 9 (Suppl 2) September/October 2003ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2) 7
• Overweight: a Body Mass Index (BMI) >25 or a Question 5. What is a reasonable approach to manag-
waist circumference of >40 inches for men, >35 ing the Insulin Resistance Syndrome in clinical
inches for women (10-15% lower for non- practice?
Caucasians) A discussion of treatment considerations for patients
• A sedentary lifestyle with IRS must begin by differentiating between efforts
• Age >40 years focused on improving insulin sensitivity itself and those
• Non-Caucasian ethnicity (e.g., Latino/Hispanic aimed at treatment of any of the specific manifestations of
American, African American, Native American, IRS.
Asian American, Pacific Islander)
• A family history of type 2 diabetes, hypertension Efforts to improve insulin sensitivity
or cardiovascular disease There is consensus that individualized lifestyle modi-
• A history of glucose intolerance or gestational fication is appropriate for all patients who are considered
diabetes at risk to have IRS. The panel encourages research into
• Acanthosis nigricans other approaches, including pharmacologic therapies, to
• Polycystic ovary syndrome address insulin resistance directly.
• Nonalcoholic fatty liver disease
Treatment of the components
Question 4. How can the Insulin Resistance Syndrome Evidence-based guidelines exist which support the
be detected in clinical practice? appropriate use of pharmacologic agents to treat the indi-
Individuals at risk for having IRS can be identified by vidual components of IRS. Individuals identified as being
history, physical examination and laboratory evaluation. at risk should be treated as soon as thresholds are met and
The following are the characteristic abnormalities of the then followed closely, in anticipation of development of
IRS (Table A). There is no single definitive test for insulin the other components of the syndrome.
resistance available for use in clinical practice.
Standardized assays for plasma insulin are not available Question 6. What should be the priorities for the
for routine use. Note that the post-glucose challenge future?
plasma glucose provides a more sensitive indicator of The panel identified four key areas of particular
insulin resistance than fasting plasma glucose measure- interest.
ment. 1. Development of a better diagnostic test for
The “diagnosis” of IRS should be considered in any insulin resistance.
individual with risk factors and abnormalities from Table 2. Targeted testing for individuals and families at
A, and we did not want to focus on an arbitrary numerical risk.
scoring system until there are data to justify it. For epi- 3. Research into pharmacologic therapies to
demiological purposes, however, we concluded that 2 or improve insulin sensitivity.
more abnormalities from Table A (corresponding to Table 4. Convening a conference to gather leading
3 in the Position Paper) in an individual with risk factors researchers and clinicians to establish the best
(Table 2 in the Position Paper) constituted the IRS. current understanding of IRS (Appendix).
SUMMARY
Table A The Insulin Resistance Syndrome Task Force
Characteristic Abnormalities of Insulin attempted to provide a means of understanding the Insulin
Resistance Syndrome
Resistance Syndrome and a practical clinical approach to
Plasma glucose identifying and managing individuals at risk. By necessi-
Fasting 110 - 125 mg/dL ty, we had to limit discussion to outline form only, espe-
120 min post-glucose challenge (75 g) 140 - 200 mg/dL cially with regard to treatment. While we have accepted
the lipid and blood pressure guidelines from NCEP ATP
Triglycerides* > 150 mg/dL III, we do recommend certain differences to identify
HDL cholesterol* individuals with IRS. These differences may be summa-
Men < 40 mg/dL rized as follows:
Women < 50 mg/dL 1) The Insulin Resistance Syndrome is used to
describe the cluster of abnormalities that are more
Blood pressure* > 130/85 mm Hg likely to occur in insulin resistant/hyperinsuline-
* Levels based upon NCEP/ATP III Guidelines, JAMA, mic individuals.
May 16, 2001. 2) The Insulin Resistance Syndrome is differentiat-
ed from type 2 diabetes.8 ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2)
3) BMI, as well as waist circumference, is used as consisting of many small incremental steps, of which the
the index of obesity, and viewed as a physiologi- work of our Task Force is but one.
cal variable that increases insulin resistance,
rather than as a criterion for diagnosis of the INSULIN RESISTANCE SYNDROME TASK
Insulin Resistance Syndrome. Any measure of FORCE
obesity must be adjusted for ethnicity.
4) Ethnicity is introduced as an important risk factor Daniel Einhorn, MD, FACP, FACE, Co-Chair IRS Task
for insulin resistance, and non-Caucasian ances- Force, Scripps Whittier Institute for Diabetes
try identified as increasing risk of the Insulin Gerald M. Reaven, MD, Co-Chair IRS Task Force,
Resistance Syndrome. Stanford University
5) Other factors have been identified that increase Rhoda H. Cobin, MD, FACE, AACE Immediate Past
the risk of developing the Insulin Resistance President, ACE Chancellor
Syndrome, including a family history of type 2 Earl Ford, MD, MPH, Centers for Disease Control
diabetes, hypertension, CVD, as well as a person- Om P. Ganda, MD, FACE, Joslin Clinic, AACE Board
al history of CVD, PCOS, gestational diabetes, of Directors
and acanthosis nigricans. Yehuda Handelsman, MD, FACP, FACE
6) Fasting plasma glucose concentration is used Richard Hellman, MD, FACP, FACE, University of
primarily to identify individuals with type 2 Missouri/Kansas City School of Medicine
diabetes. The plasma glucose concentration 2 Paul S. Jellinger, MD, FACE, University of Miami
hours after a 75-g oral glucose load is introduced David Kendall, MD, International Diabetes Center
as a more sensitive measure of risk for the Insulin Ronald M. Krauss, MD, Lawrence Livermore
Resistance Syndrome. Laboratories/Berkeley
Naomi D. Neufeld, MD, FACE, AACE Board of
We are supportive of current concepts in medically Directors
supervised therapeutic lifestyle change, efforts directed to Steven M. Petak, MD, JD, FACE, AACE Board of
the treatment of obesity, and strategies for increasing Directors
physical activity. Further research into pharmacologic Helena W. Rodbard, MD, FACE, ACE Immediate Past
interventions for the treatment of the Insulin Resistance President
Syndrome appears very promising. We fully concur that John A. Seibel, MD, MACE, AACE Board of Directors
the emergence of the Insulin Resistance Syndrome is Donald A. Smith, MD, MPH, FACP, Mount Sinai
among the most pressing problems of public health in the School of Medicine
developed world, and many diverse talents and resources Peter W. F. Wilson, MD, Boston University School of
will need to work together to meet this challenge. As the Medicine
Position Paper states, this is an area of rapid evolutionACE Position Statement
INTRODUCTION In the absence of a straightforward diagnostic test or
definitive clinical trials, identification and treatment of a
The clinical consequences of insulin resistance and syndrome as complex as this one is require thoughtful
compensatory hyperinsulinemia, the Insulin Resistance evaluation of the best available evidence and consensus
Syndrome, are increasingly appreciated as posing a major among researchers and clinicians. Our task force was
public health problem. Currently recognized clinical man- created by AACE and the American College of
ifestations of the Insulin Resistance Syndrome include Endocrinology (ACE) to work toward this consensus and
atherosclerotic cardiovascular disease (CVD), hyperten- so to provide guidance to clinicians and the many others
sion, polycystic ovary syndrome (PCOS), and nonalco- involved in and affected by the Insulin Resistance
holic steatohepatitis, and the list continues to expand. Syndrome. This is an area in rapid evolution, so progress
Despite the recognition of the importance of this syn- will consist of many small incremental steps, of which the
drome, identifying individuals who have the Insulin efforts of our task force are but one.
Resistance Syndrome is difficult, as there is no simple
clinically available test to diagnose it. Important contribu- 1. Differentiation between the Insulin Resistance
tions have been made by the National Cholesterol Syndrome and type 2 diabetes
Education Program (NCEP) Adult Treatment Panel III
(ATP III) in their publication of criteria for diagnosing the Sensitivity to insulin-mediated glucose disposal
“Metabolic Syndrome.” The explosion of research and varies widely in the population at large (1). When insulin
educational material on the “Metabolic Syndrome” attests resistant individuals cannot maintain the degree of hyper-
to the recognition of its importance by clinicians. The insulinemia needed to overcome the resistance, type 2 dia-
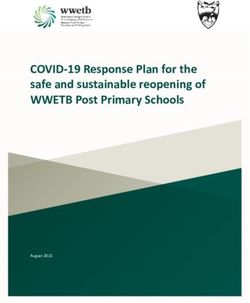
American Association of Clinical Endocrinologists betes develops (Fig. 1). However, even when insulin
(AACE) championed the creation of the new ICD-9 Code resistant individuals secrete enough insulin to remain non-
277.7 for the “Dysmetabolic Syndrome” and, with other diabetic, they remain at increased risk to develop a cluster
groups, is leading efforts to enable clinicians to screen and of abnormalities that have been given many names, but
treat individuals at risk. For reasons outlined below, we which we suggest is best described as the Insulin
will use the term Insulin Resistance Syndrome to describe Resistance Syndrome. The primary reason for selecting
the consequences of insulin resistance and compensatory this name is to focus explicitly on the central role of
hyperinsulinemia, thereby focusing on the underlying insulin resistance with compensatory hyperinsulinemia in
pathophysiology that unites the cluster of related abnor- the pathogenesis of the associated cluster of abnormalities.
malities. Use of alternative labels such as “the metabolic
Insulin Resistance
“Inadequate” Compensatory
Insulin Response Hyperinsulinemia
Type 2 Diabetes Insulin Resistance
Syndrome
CVD
Retinopathy Hypertension
Stroke
Nephropathy
PCOS
Neuropathy NAFLD
Fig. 1. Differentiation between the Insulin Resistance Syndrome and type 2
diabetes.
ENDOCRINE PRACTICE Vol 9 (Suppl 2) September/October 2003 910 ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2)
syndrome” or the “dysmetabolic syndrome” relies on an type 2 diabetes. In addition to representing the abnormali-
unclear definition of “metabolic,” and these terms are like- ties generally accepted as belonging to the Insulin
ly to become even less appropriate as the abnormalities Resistance Syndrome, the changes listed in Table I have
associated with insulin resistance and compensatory also been shown to increase the likelihood of an individual
hyperinsulinemia continue to expand. Furthermore, use of developing type 2 diabetes and/or CVD (5-26). It should
these labels usually leads to a descriptive compilation of be noted that the conditions associated with insulin resist-
clinical findings that tend to cluster within an individual, ance/compensatory hyperinsulinemia continue to expand,
without implying any mechanistic explanation for why and there is increasing evidence that nonalcoholic steato-
this happens. In contrast, the Insulin Resistance Syndrome hepatitis (NASH), and perhaps even several forms of can-
offers a clear statement of the presumed pathogenesis of cer, are more likely to occur in individuals with the Insulin
the syndrome, is based on evidence that insulin resistance Resistance Syndrome (27,28).
and compensatory hyperinsulinemia significantly increase Not all insulin resistant/hyperinsulinemic individuals
the likelihood of an individual developing a cluster of will develop the entire cluster of abnormalities that cur-
related abnormalities, and provides a broad umbrella rently make up the Insulin Resistance Syndrome (Table 1).
under which all of the abnormalities related to insulin At the simplest level, the number of manifestations present
resistance with compensatory hyperinsulinemia can be in an insulin resistant individual will vary with the criteria
gathered. used to separate normal from abnormal. In addition, nei-
As depicted in Fig. 1, some individuals with the ther insulin resistance nor the plasma insulin concentration
Insulin Resistance Syndrome will eventually develop dia- is the sole regulator of the abnormalities listed in Table 1.
betes because they lose the ability to secrete the large For example, two individuals can be equally insulin resist-
amount of insulin needed to overcome the insulin resist- ant or hyperinsulinemic, with a comparable increase in
ance (2). However, while the majority of insulin resistant hepatic triglyceride (TG) secretion, but differ in terms of
individuals do not become frankly diabetic, they remain at their ability to remove TG-rich lipoproteins from plasma.
increased risk (2) to develop CVD and all of the other clin- As a consequence, one subject will have a TG concentra-
ical consequences of insulin resistance/compensatory tion of 140 mg/dL, while the other will have a concentra-
hyperinsulinemia. Since CVD is also the major cause of tion of 180 mg/dL.
morbidity and mortality in patients with type 2 diabetes The situation is even more complicated in the case of
(3), and because the vast majority of individuals with CVD essential hypertension. Even though insulin resistance/
and/or type 2 diabetes are also insulin resistant (2), it could hyperinsulinemia is likely to be responsible for increased
be argued that the differentiation between the two clinical blood pressure in no more than 50% of patients with
syndromes outlined in Fig. 1 is inappropriate. However, essential hypertension (17), the fact remains that the eleva-
the diagnosis of type 2 diabetes is relatively straightfor- tion of blood pressure in a substantial proportion of
ward and based primarily upon the degree of hyper- patients with essential hypertension is one of the manifes-
glycemia that increases risk of diabetic microangiopathy tations of the Insulin Resistance Syndrome.
(4). An approach to identifying those individuals who do Insulin resistance is not a disease in and of itself, but
not have diabetes, but who do have the Insulin Resistance rather a physiological abnormality that increases the risk
Syndrome, is not so simple and is the primary goal of this of developing one or more of the abnormalities listed in
report. This decision is not meant to deny the many simi- Table 1. Not all insulin resistant individuals develop these
larities between the Insulin Resistance Syndrome and type abnormalities, nor is their appearance confined to insulin
2 diabetes, but only to develop a construct that recognizes resistant individuals. On the other hand, the presence of
the clinical importance of insulin resistance and compen- any one of them indicates that the individual may be
satory hyperinsulinemia in the absence of frank hyper- insulin resistant and increases the possibility that the other
glycemia. abnormalities will be present. The more insulin resistant
A secondary goal is to outline briefly the therapeutic an individual, and the greater the degree of compensatory
approaches to prevent, or attenuate, the pathophysiological hyperinsulinemia, the more likely the person is to have the
consequences of the Insulin Resistance Syndrome. Insulin Resistance Syndrome. However, in order to
emphasize that the abnormalities listed in Table 1 can also
2. What are the disease-related consequences of occur independently of insulin resistance and compensa-
insulin resistance/compensatory hyperinsulinemia tory hyperinsulinemia, they are listed separately.
(the Insulin Resistance Syndrome)? In the remainder of this section we will explore the
relationships between insulin resistance/hyperinsulinemia
Insulin-mediated glucose disposal by muscle varies and currently recognized components of the Insulin
approximately 10-fold in healthy, nondiabetic, normoten- Resistance Syndrome listed in Table 1.
sive individuals (1). The more insulin resistant the muscle,
the more insulin needs to be secreted in order to maintain 1) Glucose tolerance—The majority of persons with
normal glucose homeostasis. Table 1 presents a list of the the Insulin Resistance Syndrome will have a
changes that are more likely to occur in insulin resistant “normal” fasting plasma glucose (FPG) concen-
individuals who are able to maintain the degree of com- tration (ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2) 11
Table 1
Components of the Insulin Resistance Syndrome
1. Some degree of glucose intolerance
• Impaired fasting glucose
• Impaired glucose tolerance
2. Abnormal uric acid metabolism
• Plasma uric acid concentration
• Renal uric acid clearance
3. Dyslipidemia
• Triglycerides
• HDL-C
• LDL-particle diameter (small, dense LDL-particles)
• Postprandial accumulation of TG-rich lipoproteins
4. Hemodynamic changes
• Sympathetic nervous system activity
• Renal sodium retention
• Blood pressure (~50% of patients with hypertension are insulin resistant)
5. Prothrombotic factors
• Plasminogen activator inhibitor-1
• Fibrinogen
6. Markers of inflammation
• C-reactive protein, WBC, etc.
7. Endothelial dysfunction
• Mononuclear cell adhesion
• Plasma concentration of cellular adhesion molecules
• Plasma concentration of asymmetric dimethylarginine
• Endothelial-dependent vasodilatation
individuals with either “impaired fasting glucose” lesterol (HDL-C) concentration are common
(FPG concentration >110 and12 ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2)
5) Hemostasis and 6) Inflammation—Plasma con- hyperinsulinemic. Finally, a prior diagnosis of glucose
centrations of plasminogen activator inhibitor-1 intolerance suggests that insulin resistance may be present.
are frequently increased in insulin resistant/ Ethnicity is also a powerful predictor of insulin resist-
hyperinsulinemic individuals. The presence of ance/hyperinsulinemia (34), and manifestations of the
increased fibrinogen levels has been a less consis- Insulin Resistance Syndrome are increased in essentially
tent finding and may be more likely a manifesta- every group of non-Caucasian ancestry in which compar-
tion of an acute-phase reaction associated with isons have been made. Furthermore, these differences per-
inflammation of the vascular wall in patients with sist when adjustments are made for the impact of lifestyle
the Insulin Resistance Syndrome. In this context, variables known to lead to insulin resistance.
there is evidence that other markers of inflamma- The most powerful modulators of insulin action are
tion are present in the Insulin Resistance differences in degree of obesity and physical activity, and
Syndrome, e.g. C-reactive protein and higher there is evidence in both Pima Indians and Caucasians that
white blood cell counts. Whether these latter approximately 50% of the variability in insulin-mediated
changes are simply an epiphenomenon, increased glucose disposal can be attributed to variations in degree
because of the enhanced atherogenesis in insulin of obesity and physical fitness (35). The two variables
resistant individuals, or play a causal role in the were approximately equally powerful, and it is quite like-
development of CVD, remains to be determined. ly that at least a portion of the untoward effect of obesity
7) Endothelial dysfunction—Mononuclear cells iso- on insulin resistance is due to the fact that overweight indi-
lated from insulin resistant/hyperinsulinemic viduals are often physically inactive. Degree of physical
individuals bind with greater adherence to cul- fitness is not routinely quantified, but body weight is. We
tured endothelium, associated with increases in suggest that body mass index (BMI, weight in kg/height in
plasma concentrations of cellular adhesion mole- meters squared) be used as the criterion for defining a per-
cules and asymmetric dimethylarginine (an son as being overweight/obese, and that a BMI >25.0
endogenous inhibitor of nitric oxide synthase). kg/m2 identifies individuals at increased risk to have the
Functionally, endothelium-dependent vasodilata- Insulin Resistance Syndrome. It is recognized that using a
tion is decreased in insulin resistant/hyperinsu- BMI value of 25 or more to identify individuals at
linemic individuals. increased risk to have the Insulin Resistance Syndrome
may be too high for ethnic groups in whom the prevalence
3. Identification of individuals at risk for the Insulin of insulin resistance/hyperinsulinemia is more common.
Resistance Syndrome On the other hand, inclusion of ethnicity as a risk factor
minimizes the lack of definitive ethnic-specific data con-
The prevalence of insulin resistance is increased in cerning the relationship between adiposity and insulin
nondiabetic individuals with diagnosed CVD, essential resistance.
hypertension, or acanthosis nigricans as shown in Table 2. Age, per se, has relatively little effect on insulin
Women with PCOS (26), or a history of gestational dia- resistance (35), but body weight tends to increase, and
betes (30), are likely to be insulin resistant, and at physical activity decrease, as persons get older. Thus,
increased risk to develop one or more of the clinical although somewhat arbitrary, it seems reasonable to eval-
components of the Insulin Resistance Syndrome. Insulin uate all individuals >40 years of age for manifestations of
resistance has been shown to be a familial characteristic the Insulin Resistance Syndrome. On the other hand, it
(31-33), and a family history of type 2 diabetes, hyperten- must be emphasized that manifestations of the Insulin
sion, or CVD increases the likelihood of an individual Resistance Syndrome can occur at any age.
being insulin resistant. In contrast to the CVD risk associ- Finally, it should be emphasized that obesity and
ated with a high LDL-C concentration, there is no physical inactivity are variables that not only significantly
evidence that the earlier the history of CVD in the family, increase the likelihood of an individual being insulin
the more likely the individual is to be insulin resistant/ resistant, but also represent predictors of the Insulin
Table 2
Factors That Increase the Likelihood of the Insulin Resistance Syndrome
• Diagnosis of CVD, hypertension, PCOS, NAFLD, or acanthosis nigricans
• Family history of type 2 diabetes, hypertension, or CVD
• History of gestational diabetes or glucose intolerance
• Non-Caucasian ethnicity
• Sedentary lifestyle
• BMI >25.0 kg/m2 (or waist circumference >40 inches in men, >35 inches in women)
• Age >40 yearsACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2) 13
Resistance Syndrome that can be modified by changes in circumference was used as the estimate of obesity in the
lifestyle. The importance of weight loss and increased 3300 individuals in the NHANES III database in whom
physical activity in treatment of the insulin resistance syn- these measurements were made (37). Finally, BMI and
drome will be discussed subsequently. abdominal circumference were closely related, with corre-
lation coefficients of approximately r=0.9 in the 15,271
4. Obesity and the Insulin Resistance Syndrome participants in the NHANES III study, irrespective of gen-
der or ethnicity. For all of these reasons, it has been sug-
The relationship between obesity and the Insulin gested that BMI be used as the marker to identify individ-
Resistance Syndrome outlined in this document differs in uals that should be evaluated for the Insulin Resistance
two respects from many other published considerations of Syndrome. On the other hand, there would not be a great
this topic. In the first place, descriptions of the Insulin deal to lose if an increase in abdominal circumference
Resistance Syndrome often include obesity, usually (>40 inches for men and >35 inches for women) was used
abdominal obesity, as one of the features of the syndrome, instead of (or in addition to) BMI as a way to identify indi-
rather than as a lifestyle factor that, because of its adverse viduals at increased risk to have the Insulin Resistance
effect on insulin-mediated glucose disposal, increases the Syndrome.
risk of the Insulin Resistance Syndrome. The decision to
view obesity in this latter manner was based upon the fol- 5. “Diagnosing” the Insulin Resistance Syndrome
lowing considerations. Obesity is not a consequence of
insulin resistance/hyperinsulinemia, but a physiological Recognition of the importance of insulin resistance/
variable that decreases insulin-mediated glucose disposal. hyperinsulinemia as increasing risk of CVD has led to the
Furthermore, not all insulin resistant individuals are over- publication of criteria for diagnosing what was referred to
weight/obese, nor are all overweight/obese individuals as the “Metabolic Syndrome (38)” and the creation of an
insulin resistant. For clarity of the physiological construct ICD-9 code 277.7 for the “Dysmetabolic Syndrome X.”
of the Insulin Resistance Syndrome, it is important that Unfortunately, the experimental evidence available does
obesity be viewed as contributing to the insulin resist- not exist that can be translated into simple criteria for diag-
ance/hyperinsulinemia, rather than being a consequence of nosing the Insulin Resistance Syndrome. The Insulin
the abnormal insulin metabolism. This view of the rela- Resistance Syndrome is not a specific disease, any more
tionship between obesity and insulin resistance/hyperinsu- than insulin resistance is, but rather a group of abnormali-
linemia should not be construed as minimizing the impor- ties that tend to cluster together, occur with greater preva-
tant role that the current epidemic of obesity plays in lence in insulin resistant/hyperinsulinemic persons, and
increasing the incidence of both type 2 diabetes and the identify individuals at increased risk to develop type 2 dia-
Insulin Resistance Syndrome. betes and CVD. Consequently, it seems useful to provide
Secondly, it is proposed that BMI, rather than abdom- the means, using the relatively simple tests described in
inal circumference, be used to identify individuals at the next section, to identify individuals who are likely to
increased risk to have the Insulin Resistance Syndrome. be insulin resistant/hyperinsulinemic because they display
This decision was based on the following considerations. at least one of the components of the Insulin Resistance
Height and weight are simple and routine measurements Syndrome as summarized in Table 1. The more the num-
that are easily quantified, in contrast to estimates of ber of components an individual has, and the more severe
abdominal circumference, which are neither routinely per- the magnitude of the abnormality, the more likely that
formed nor is its quantification as well standardized. In individual is to have the Insulin Resistance Syndrome, and
addition, BMI has been widely used to define obesity also to be at increased risk to develop type 2 diabetes
status in the U.S. and Europe, and the classification of nor- and/or CVD.
mal weight, overweight, and obesity is based on use of
BMI, as are current guidelines for the appropriate use of 6. Criteria for predicting the Insulin Resistance
pharmacological treatment of obesity. Furthermore, avail- Syndrome
able evidence does not demonstrate that measurements of
abdominal circumference provide a superior estimate of The abnormalities listed in Table 3 are increased in
insulin resistance than does BMI. For example, the rela- prevalence in insulin resistant/hyperinsulinemic individu-
tionship between insulin-mediated glucose disposal as als and predict the development of type 2 diabetes and/or
measured by the euglycemic clamp technique and obesity CVD. However, the relationship is far from perfect, and
based on the results of >1100 subjects studied by the each of these changes can occur independently of insulin
European Group for the Study of Insulin Resistance was resistance. Furthermore, the actual numerical values are, at
not increased when abdominal circumference replaced best, approximations. For example, defining a plasma TG
BMI as the marker of obesity (36). Additional support for concentration >150 mg/dL as evidence of the Insulin
this decision came from the observation that the relation- Resistance Syndrome may be reasonable, but there is no
ship between obesity and plasma glucose and insulin con- evidence that using a TG concentration of 175 mg/dL as a
centrations, before and 120 min after a standard oral glu- cut point would be any less useful. In the absence of
cose load, was identical when either BMI or abdominal rigorous criteria, we propose, for the sake of consistency14 ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2)
Table 3
Identifying Abnormalities of the Insulin Resistance Syndrome
1. Triglycerides >150 mg/dL
2. HDL cholesterol
Men < 40 mg/dL
Women < 50 mg/dL
3. Blood pressure >130/85 mm Hg
4. Glucose
Fasting 110-125 mg/dL
120 min post-glucose challenge 140-200 mg/dL
and in recognition of the important contribution made by concentrations to differentiate insulin resistant from
the National Cholesterol Education Program, to use the insulin sensitive individuals. This information is based on
values suggested by the Adult Treatment Panel III (ATP analysis of the results in a large population of apparently
III) for identifying the dyslipidemic and blood pressure healthy, nondiabetic individuals, in whom specific meas-
characteristics of the Insulin Resistance Syndrome (38). urements of insulin action were available (1,40).
However, the plasma glucose concentration criterion has Measurements of insulin-mediated glucose disposal in
been modified to focus on the response to a 75-g oral glu- these 490 individuals demonstrated that this variable was
cose challenge, with a plasma glucose concentration 120 distributed continuously throughout the population, mak-
min after the glucose load >140 mg/dL (and < 200 mg/dL) ing it impossible to create rigid criteria for identifying an
replacing a fasting plasma glucose concentration of >110 individual as being either insulin resistant or insulin sensi-
mg/dL. It should be emphasized again that the Insulin tive. However, there are prospective data available
Resistance Syndrome, as defined, excludes patients whose demonstrating that in a population without obvious dis-
degree of hyperglycemia fulfills the diagnostic criteria for ease at baseline that CVD and type 2 diabetes developed
type 2 diabetes. to a significant degree in the most insulin resistant tertile,
The decision to use a post-glucose challenge measure- and did not occur in the most insulin sensitive tertile
ment to identify insulin resistant individuals is not in con- (41,42). Thus, for the analysis in Table 4, we divided the
flict with the recommendation of the American Diabetes 490 volunteers in whom specific measurements of insulin
Association that determination of FPG be used to diagnose action were available into tertiles, and calculated the abil-
diabetes (18). The use of FPG to identify patients with ity of several plasma glucose concentrations to identify
type 2 diabetes is an effort to provide a practical approach individuals as being in the third of the population that was
to identify individuals who are sufficiently hyperglycemic either the most insulin sensitive or the most insulin resist-
to be at risk for the microvascular complications of dia- ant. The fasting plasma glucose criterion recommended
betes. If the focus is shifted to provide a more sensitive by the ATP III (FPG >110 and 126 mg/dL, in whom there plasma glucose concentrations are even less helpful than
were values for plasma glucose concentrations before and the cut point suggested by the ATP III in distinguishing
120 min after a 75-g oral glucose challenge. In this popu- between insulin resistant and insulin sensitive individuals.
lation, approximately 10% had fasting glucose concentra- Based upon the NHANES results discussed above,
tions 110-126 mg/dL, whereas about 25% had a glucose and the data in Table 4, it appears that the extra effort
concentration >140 andACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2) 15
Table 4
Number of 490 Nondiabetic Volunteers Identified as Being Insulin Resistant or
Insulin Sensitive on the Basis of Plasma Glucose Measurements
Variable Total number Insulin sensitive Insulin resistant
FPG >90 mg/dL 277 63 112
FPG >100 mg/dL 100 14 61
FPG >110140 mg/dL 71 4 54
plasma glucose concentration 120 min after the oral glu- (r=~0.6) and post-glucose challenge (r=~0.8) plasma
cose challenge could be limited to those individuals who insulin concentrations (1). However, they have not been
had a fasting plasma glucose concentration16 ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2)
Table 5
Prevalence of the 4 Abnormalities of the Insulin Resistance Syndrome in NHANES III*
Variable Prevalence (%)
TG> 150 mg/dL 35
Low HDL-C 36
Hypertension 44
120 min glucose >140 mg/dL 26
*The population includes 3280 individuals, aged 40-74, without diabetes by history or a fasting plasma
glucose concentration >126 mg/dL.
function of BMI. The results of this analysis are seen in tion with the epidemic of obesity in developed countries, it
Table 6, and demonstrate that being classified as of normal is also clear that the incidence is not lagging that far
weight (BMI30.0 kg/m2 having 2 abnormalities, and 3 components with the components of the Insulin Resistance Syndrome,
being present in 30% of this subgroup. as well as a relatively simple approach to identify persons
Table 7 presents the prevalence of the individual with the Insulin Resistance Syndrome. This information
abnormalities by themselves, and their appearance in should not serve as the sole means to “rule out” the Insulin
combination with the other 3 abnormalities. It can be seen Resistance Syndrome. Indeed, at this time, that “either/or”
from these data that all theoretical combinations occur to decision has the potential to do more harm than good.
some extent, although some more often than others. However, the information presented provides evidence-
Whether or not some of these will be more useful than based criteria to identify individuals most likely to have
others in predicting clinical outcome is an issue worth the Insulin Resistance Syndrome, and those so identified
pursuing. can then be considered for the most appropriate therapeu-
tic intervention. As described above, our purpose is to pro-
9. Clinical utility of recognizing the Insulin vide information that is both simple, so it will be used, and
Resistance Syndrome sensitive, so that individuals at risk can be confidently
screened.
The purpose of this position paper is, in part, to
acquaint heath-care professionals with the major role that 10. Treatment of the Insulin Resistance Syndrome
the Insulin Resistance Syndrome plays in what are often
referred to as “diseases of Western civilization.” Although A discussion of treatment considerations for patients
the prevalence of these diseases is increasing in associa- with the Insulin Resistance Syndrome must begin by
Table 6
Age-Adjusted Prevalence of the 4 Abnormalities of the Insulin Resistance Syndrome as a Function of BMI*
Abnormalities
1 2 3 4
Total population (n=3280) 71% 42% 17% 4.5%
BMI
30 kg/m2 (n=917) 86% 62% 30% 9.1%
*The population includes 3280 individuals, aged 40-74, without diabetes by history or a fasting plasma glucose
concentration >126 mg/dL.ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2) 17
differentiating between efforts focused on improving interest in that they are capable of improving
insulin sensitivity itself and those aimed at treatment of insulin sensitivity. However, TZD compounds are
any of the specific manifestations of the insulin resistant currently approved by the FDA for the treatment
syndrome. of hyperglycemia only in patients with type 2 dia-
betes, and at the present time there are no com-
A. Efforts to improve insulin sensitivity pelling experimental data that establish their clin-
1) Lifestyle—As discussed previously, both adipos- ical utility in nondiabetic individuals with the
ity and level of physical activity are powerful Insulin Resistance Syndrome. The potential
modulators of insulin-mediated glucose disposal. benefits of this class of drugs are being intensive-
More importantly, in contrast to the other factors ly evaluated at this time, and it is highly likely
that affect insulin action, they are modifiable by that a clearer view of their role in treatment of the
safe, straightforward lifestyle changes. Thus, Insulin Resistance Syndrome will soon be
weight loss of 5-10% of body weight in over- apparent.
weight/obese individuals, who are also insulin
resistant, will significantly enhance insulin sensi- Although metformin does not seem to act by directly
tivity, lower ambient plasma insulin concentra- improving insulin sensitivity, it may also offer potential
tions, and improve the manifestations of the benefit for treatment of the Insulin Resistance Syndrome.
Insulin Resistance Syndrome (43). It has been used worldwide for the treatment of type 2 dia-
betes, has an outstanding safety record, and has been
An increase in physical activity in insulin resistant shown to be effective in treatment of PCOS (47). In
individuals is also of considerable utility, and provides addition, although not as effective as weight loss and
two benefits. At the simplest level, any increase in energy increased physical activity, metformin also decreased pro-
expenditure will help insulin resistant individuals maintain gression to type 2 diabetes in patients with impaired glu-
or lose weight. The greater the magnitude of the increase cose tolerance (45). Finally, there is evidence that met-
in energy expenditure, the greater will be the benefit to the formin administration can lower circulating insulin levels
individual. It is also possible to enhance insulin sensitivity and improve glucose and lipid metabolism in patients with
directly if an individual is able to exercise aerobically characteristics of the Insulin Resistance Syndrome (48).
for approximately 30-40 min, 4 times/week. Given the importance that obesity plays in the devel-
Perhaps the most dramatic evidence of the beneficial opment of insulin resistance in susceptible individuals,
effects of lifestyle intervention is the evidence from recent pharmacological treatment of obesity may play an impor-
prospective intervention studies showing that the combina- tant role in the management of overweight individuals
tion of weight loss and increased physical activity can with the Insulin Resistance Syndrome. If overweight/
significantly decrease the development of type 2 diabetes obese patients with the Insulin Resistance Syndrome
in high-risk individuals (44,45). cannot lose weight with simple caloric restriction, both
Before ending the discussion of the clinical benefits orlistat and sibutramine have been shown to be more effec-
of weight loss, three additional points must be empha- tive than diet alone in the treatment of obesity.
sized: 1) Not all overweight/obese individuals are insulin Furthermore, administration of both drugs to appropriate-
resistant, or have manifestations of the Insulin Resistance ly selected individuals has been shown to result in attenu-
Syndrome, and weight loss does not lead to significant ation of the manifestations of the Insulin Resistance
enhancement of insulin sensitivity in these individuals Syndrome (43,49).
(43). 2) There is no persuasive evidence that obese, insulin
resistant individuals have any more difficulty in losing B. Efforts to treat the manifestation of the Insulin
weight in response to energy-restricted diets than do Resistance Syndrome
equally overweight persons who are not insulin resistant 1) Lifestyle—Although macronutrient composition
(43). 3) It does not appear that the ability to lose weight in of the diet, by itself, has little or no direct effect
response to energy-restricted diets varies as a function of on insulin-mediated glucose disposal, a variety of
the macronutrient composition of the diet (46). studies have shown that it certainly can impact on
the manifestations of the Insulin Resistance
2) Pharmacological—Given the difficulty in chang- Syndrome in the absence of weight loss (50). In
ing lifestyle, and the probable limits of its effica- this context, some general principles should be
cy in many individuals, it could be argued that kept in mind when treating insulin resistant
treatment of the Insulin Resistance Syndrome persons with manifestations of the Insulin
would be a drug(s) that could significantly Resistance Syndrome. Of greatest importance is
enhance insulin sensitivity, as well as the other the avoidance of low fat-high carbohydrate diets
manifestations of the Insulin Resistance unless weight loss is also occurring. The more
Syndrome. In this context, the use of thiazolidine- insulin resistants individual are, the more insulin
dione (TZD) compounds, either agents cur- they must secrete in order to maintain normal glu-
rently available or future ones, is of particular cose homeostasis. As a consequence, in the18 ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2)
absence of weight loss, manifestations of the tions of the Insulin Resistance Syndrome, i.e.
Insulin Resistance Syndrome will be accentuated hypertension, dyslipidemia, etc., that persist
when insulin resistant persons increase the despite appropriate changes in lifestyle. It is not
amount of carbohydrate in their diet (50). A sim- appropriate within the context of this document to
ple alternative, and one consistent with efforts to discuss extensively the pros and cons of the vari-
minimize the intake of saturated fat, would be to ous pharmacological approaches that can help to
replace saturated fat with unsaturated fat, rather ameliorate the manifestations of the Insulin
than with carbohydrate, thus maintaining a mod- Resistance Syndrome, but it is totally relevant
erate carbohydrate intake. Parenthetically, this that a thorough search be made to both identify
dietary manipulation is as effective as low fat- and initiate appropriate drug treatment for any of
high carbohydrate diets in lowering LDL-C con- the manifestations of the Insulin Resistance
centrations (51,52). Although this general Syndrome that have not responded to lifestyle
approach will have the greatest benefit in mini- modifications. There are no evidence-based
mizing the untoward manifestations of the Insulin guidelines to provide therapeutic targets for treat-
Resistance Syndrome, additional benefit may be ment of the central manifestations of the Insulin
gained by increasing intake of soluble dietary Resistance Syndrome, but efforts to obtain values
fiber, as well as by decreasing intake of highly for the lipid, glucose, and blood pressure cut
refined carbohydrates. points outlined in Table 3 seem reasonable.
2) Pharmacological intervention—In the absence of Finally, although a high LDL-C concentration is
evidence that there is one drug capable of not part of the Insulin Resistance Syndrome, it
addressing the entire cluster of abnormalities also seems reasonable to treat hypercholes-
associated with insulin resistance/hyperinsuline- terolemia aggressively, possibly to the same
mia, pharmacological treatment at this point is by degree as is recommended for patients with type
necessity directed to the individual manifesta- 2 diabetes (53).
CONCLUSIONS
Table 7 This document has attempted to provide a means of
Prevalence of Combinations of the 4 understanding the Insulin Resistance Syndrome and a prac-
Metabolic Abnormalities* of the tical clinical approach to identifying and managing individ-
Insulin Resistance Syndrome† uals at risk. By necessity, we had to limit discussion to out-
line form only, especially with regard to treatment. While
Prevalence (%) we have accepted the lipid and blood pressure guidelines
One abnormality from ATP III, we do suggest certain differences from earli-
BP 11.4 er excellent efforts to identify individuals who are insulin
HDL-C 9.1 resistant and hyperinsulinemic, and at increased risk to
TG 5.2 develop type 2 diabetes and CVD. These differences may
Glucose 3.0 be summarized as follows: 1) The Insulin Resistance
Two abnormalities Syndrome is used to describe the cluster of abnormalities
TG, HDL-C 7.2 that are more likely to occur in insulin resistant/hyperinsu-
BP, glucose 5.4 linemic individuals. 2) The Insulin Resistance Syndrome is
BP, TG 4.6 differentiated from type 2 diabetes. 3) BMI, rather than
BP, HDL-C 4.1 waist circumference, is used as the index of obesity, and
HDL-C, glucose 2.0 viewed as a physiological variable that increases insulin
TG, glucose 1.4 resistance, rather than as a criterion for diagnosis of the
Three abnormalities Insulin Resistance Syndrome. 4) Ethnicity is introduced as
TG, HDL-C, BP 5.8 an important risk factor for insulin resistance, and non-
TG, BP, glucose 3.1 Caucasian ancestry identified as increasing risk of the
TG, HDL-C, glucose 2.4 Insulin Resistance Syndrome. 5) Other factors have been
HDL-C, BP, glucose 1.5 identified that increase the risk of developing the Insulin
Four abnormalities Resistance Syndrome, including a family history of type 2
TG, HDL-C, BP, glucose 4.6 diabetes, hypertension, CVD, as well as a personal history
of CVD, PCOS, gestational diabetes, and acanthosis nigri-
*Values defining an abnormality are shown in Table 3. cans. 6) Fasting plasma glucose concentrations are used to
†The population includes 3280 individuals, aged 40-74, identify individuals with type 2 diabetes, and the plasma
without diabetes by history or a fasting plasma glucose glucose concentration 2 hours after a 75-g oral glucose
concentration >126 mg/dL. load is introduced as a more sensitive measure of risk for
the Insulin Resistance Syndrome.ACE Position Statement on the Insulin Resistance Syndrome, Endocr Pract. 2003;9(Suppl 2) 19
We are supportive of current concepts in medically disease: studies in the postprandial state. Arterioscler
supervised therapeutic lifestyle change, including con- Thromb. 1992;12:1336-1345.
cerns about high carbohydrate diets, efforts directed to the 15. Facchini FS, Stoohs A, Reaven GM. Enhanced sympa-
thetic nervous system activity. The linchpin between
treatment of obesity, and strategies for increasing physical insulin resistance, hyperinsulinemia, and heart rate. Am J
activity. Further research into pharmacologic interventions Hypertens. 1996;9:1013-1017.
for the treatment of the Insulin Resistance Syndrome 16. DeFronzo RA, Cooke CR, Andres R, Faloona GR,
appears very promising. We fully concur that the emer- David PJ. The effect of insulin in renal handling of sodi-
gence of the Insulin Resistance Syndrome is among the um, potassium, calcium and phosphate in man. J Clin
most pressing problems of public health in the developed Invest. 1975;55:845-855.
17. Zavaroni I, Mazza S, Dall’Aglio E, Gasparini P, Passeri
world, and many diverse talents and resources will need to M, Reaven GM. Prevalence of hyperinsulinaemia in
work together to meet this challenge. patients with high blood pressure. J Intern Med. 1992;231:
235-240.
REFERENCES 18. American Diabetes Association. Standards of medical
care for patients with diabetes mellitus. Diabetes Care.
1. Yeni-Komshian H, Carantoni M, Abbasi F, Reaven 2002;25(Supp 1):S21-24.
GM. Relationship between several surrogate estimates of 19. Jeppesen J, Hein HO, Suadicani P, Gyntelberg F. High
insulin resistance and quantification of insulin-mediated triglycerides and low HDL cholesterol and blood pressure
glucose disposal in 490 healthy, nondiabetic volunteers. and risk of ischemic heart disease. Hypertension.
Diabetes Care. 2000;23:171-175. 2000;36:226-232.
2. Reaven GM. Role of insulin resistance in human disease. 20. Juhan-Vague I, Thompson SG, Jeppesen J, on behalf of
Diabetes. 1988;37:1595-1607. the ECAT Angina Pectoris Study Group. Involvement of
3. Wingard DL, Barrett-Connor E. Heart disease in dia- the hemostatic system in the insulin resistance syndrome.
betes. In: Diabetes in America. 2nd ed. Bethesda, MD: Arterioscler Thromb. 1993;13:1865-1873.
National Institutes of Health, National Institute of Diabetes 21. Meigs JB, Mittleman MA, Nathan DM, et al.
and Digestive and Kidney Diseases, NIH publication no. Hyperinsulinemia, hyperglycemia, and impaired home-
95-1468, 1995;429-448. ostasis. The Framingham Offspring Study. JAMA. 2000;
4. American Diabetes Association. Report of the Expert 283:221-228.
Committee on the Diagnosis and Classification of Diabetes 22. Chen N-G, Abbasi F, Lamendola C, McLaughlin T,
Mellitus. Diabetes Care. 2002;25(Suppl 1):S5-S20. Cooke JP, Tsao PS, Reaven GM. Mononuclear cell adher-
5. Fuller JH, Shipley MJ, Rose G, Jarrett RJ, Keen H. ence to cultured endothelium is enhanced by hypertension
Coronary-heart disease and impaired glucose tolerance: the and insulin resistance in healthy nondiabetic volunteers.
Whitehall Study. Lancet. 1980;1:1373-1376. Circulation. 1999;100:940-943.
6. Lillioja S, Mott DM, Spraul M, et al. Insulin resistance 23. Chen N-G, Holmes M, Reaven GM. Relationship
and insulin secretory dysfunction as precursors of non- between insulin resistance, soluble adhesion molecules,
insulin dependent diabetes mellitus. N Engl J Med. and mononuclear cell binding in healthy volunteers. J Clin
1993;329:1988-1992. Endocrinol Metab. 1999;84:3485-3489.
7. Facchini F, Chen YD-I, Hollenbeck CB, Reaven GM. 24. Stuhlinger MC, Abbasi F, Chu JW, Lamendola C,
Relationship between resistance to insulin-mediated glu- McLaughlin TL, Cooke JP, Reaven GM, Tsao PS.
cose uptake, urinary uric acid clearance, and plasma uric Relationship between insulin resistance and an endogenous
acid concentration. JAMA. 1991;266:3008-3011. nitric oxide synthase inhibitor. JAMA. 2002;287:1420-
8. Laws A, Reaven GM. Evidence for an independent rela- 1426.
tionship between insulin resistance and fasting plasma 25. Baron AD. Vascular reactivity. Am J Cardiol. 1999;84:
HDL-cholesterol, triglyceride and insulin concentrations. J 25J-27J.
Int Med. 1992;231:25-30. 26. Dunaif A. Insulin resistance and the polycystic ovary syn-
9. Castelli WP, Garrison RJ, Wilson PWF. Abbott RD, drome: mechanism and implications for pathogenesis.
Kalousdian S, Kannel WB. Incidence of coronary heart Endocr Rev. 1997;18:774-800.
disease and lipoprotein cholesterol levels: the Framingham 27. Sanyal AJ, Campbell-Sargent C, Mirashi F, et al.
Study. JAMA. 1986;256:2835-2838. Nonalcoholic steatohepatitis: association of insulin resist-
10. Austin MA, Hokanson JE, Edwards KL. Hypertrigly- ance and mitochondrial abnormalities. Gastroenterology.
ceridemia as a cardiovascular risk factor. Am J Cardiol. 2001;120:1183-1192.
1998;81(4A):7B-12B. 28. Argiles JM, Lopez-Soriano FJ. Insulin and cancer. Int J
11. Reaven GM, Chen Y-DI, Jeppesen J, Maheux P, Krauss Oncol. 2001;18:683-687.
RM. Insulin resistance and hyperinsulinemia in individuals 29. Jeppesen, J, Hein HO, Suadicani P, et al. Low triglyc-
with small, dense, low density lipoprotein particles. J Clin erides-high high-density lipoprotein cholesterol and risk of
Invest. 1993;92:141-146. ischemic heart disease. Arch Intern Med. 2001;161:361-
12. Austin MA, Breslow JL, Hennekens CH, Buring JE, 366.
Willett WS, Krauss RM. Low-density lipoprotein sub- 30. O’Sullivan JB, Mahan CM. Criteria for the oral glucose
class patterns and risk of myocardial infarction. JAMA. tolerance test in pregnancy. Diabetes. 1964;13:278.
1988;260:1917-1921. 31. Warram JH, Martin BC, Krowlewski AS, et al. Slow
13. Jeppesen J, Hollenbeck CB, Zhou, M-Y, Coulston AM, glucose removal rate and hyperinsulinemia precede the
Jones C, Chen Y-DI, Reaven GM. Relation between development of type II diabetes in the off-spring of the
insulin resistance, hyperinsulinemia, postheparin plasma diabetic parents. Ann Intern Med. 1990;113:909-915.
lipoprotein lipase activity, and postprandial lipemia. 32. Facchini F, Chen Y-DI, Clinkingbeard C, Jeppesen J,
Arterioscler Thromb Vasc Biol. 1995;15:320-324. Reaven GM. Insulin resistance, hyperinsulinemia, and
14. Patsch JR, Miesenbock G, Hopferwieser T, et al. dyslipidemia in nonobese individuals with a family history
Relation of triglyceride metabolism and coronary artery of hypertension. Am J Hypertens. 1992;5:694-699.You can also read