RISK BENEFIT INSIGHTS - GROUP - Hot Topics I March 2019 - Alexander Forbes
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

GROUP RISK BENEFIT INSIGHTS Hot Topics I March 2019

Contents Page
1. Global perspective on death and disability 1
2. Local perspective on death and disability claims 7
3. Proactive claims management 13
4. Group risk benefit design 17
5. Group risk benefit solutions 23
People we can thank for writing this workbook are:
Myrna Sachs
Vickie Lange
Belinda Sullivan
The issues surrounding trustee duties are complex and depend entirely on the particular circumstances facing each fund. Trustees must in all
cases take their own decision on issues based on their particular fund’s circumstances at the time. It is for this reason that trustees can’t simply
rely on what we’ve discussed here today, neither should they regard our discussions as advice. Trustees should get specific assistance where they
are uncertain of the consequences or reasonableness of any contemplated action.
The information in this document belongs to Alexander Forbes. You may not copy, distribute or modify any part of this document without the
express written permission of Alexander Forbes.
Alexander Forbes Financial Services is a licensed financial services provider (FSP 1177).
Alexander Forbes Investments Limited (FSP711 and registration number 1997/000595/06)
Alexander Forbes Health (Pty) Ltd (FSP 33471 and registration number ORG 00064)
Taking action based on information provided
While care has been taken to present correct information, Alexander Forbes and its directors, officers and employees take no responsibility for any
actions taken based on this information, all of which require financial advice.
For further details of our services please contact our office in Johannesburg:
Telephone: +27 (0)11 269 1800
Email: info@aforbes.com
1
Global perspective
on death and
disability
Global perspective on
death and disability
Background Causes of death globally
Understanding the leading causes of death and According to research issued by WHO, about 56.9 million
disability around the world, and in particular at country people died in 2016. To put this into perspective, it’s
level, is extremely important. These statistics assist estimated that the world’s population is 7.7 billion.
health authorities in designing health programmes and
Estimates on the leading causes of death in 2016:1
interventions to address the major areas of concern and
the biggest risks facing a country’s citizens. With resources ■■ Ischaemic heart disease and stroke are the world’s
being limited, it’s important that they are channelled to biggest killers, claiming 15.2 million lives, and have
address relevant health priorities. Understanding how remained the leading causes of death in the 15 years
diseases and injuries affect people is essential in assessing up to 2016.
the effectiveness of a country’s health system. Access ■■ Lung cancer, including tracheal and bronchial cancers,
to good medical care and appropriate health and risk caused 1.7 million deaths.
protection continues to be a challenge for low- to middle- ■■ Diabetes claimed 1.6 million lives.
income countries. ■■ Dementia is the fifth leading cause of death (deaths
from dementia more than doubled between 2000
More generally, we have seen the World Health and 2016).
Organization (WHO) help drive specific initiatives to ■■ Lower respiratory infection is the deadliest
address the major risks facing our global citizens. communicable disease.
These initiatives play an important role in addressing the ■■ One million people died from HIV-related diseases,
which reduced from 1.5 million in 2000. For this
health needs of millions of people and improving their
reason, HIV Aids is no longer one of the world’s top 10
quality of life.
causes of death.
■■ Road injuries killed 1.4 million people, 74% of whom
Health, disability and death are interconnected. were males.
1
World Health Organization, The top 10 causes of death, 24 May 2018
2|
HOT TOPICS I 2019
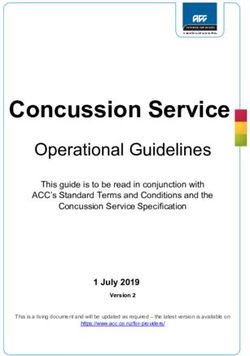
Top 10 global causes of deaths, 2016
Deaths (millions)
0 2 4 6 8 10
Ischaemic heart disease
Stroke
Chronic obstructive pulmonary disease
Lower respiratory infections
Alzheimer’s disease and other dementias
Cause group
Tracheal, bronchial and lung cancers
Communicable, maternal,
Diabetes mellitus
neonatal and nutritional
Road injury conditions
Noncommunicable diseases
Diarrhoeal diseases
Injuries
Tuberculosis
Source: Adapted from World Health Organization, Global Health Estimates 2016: Deaths by Cause, Age, Sex by Country and by
Region 2000–2016, 2018
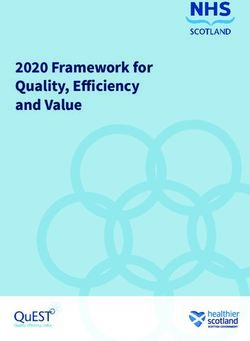
Top 10 global causes of deaths, 2000
Deaths (millions)
0 2 4 6 8 10
Ischaemic heart disease
Stroke
Lower respiratory infections
Chronic obstructive pulmonary disease
Diarrhoeal diseases
Cause group
Tuberculosis
Communicable, maternal,
HIV Aids
neonatal and nutritional
Preterm birth complications conditions
Noncommunicable diseases
Tracheal, bronchial and lung cancers
Injuries
Road injury
Source: Adapted from World Health Organization, Global Health Estimates 2016: Deaths by Cause, Age, Sex by Country and by
Region 2000–2016, 2018
|3
ALEXANDER FORBES
Noncommunicable (chronic) diseases (NCDs) caused 71% of deaths globally; however, in low-income countries 7 out of the top
10 causes of death were the result of communicable diseases. HIV Aids is the fourth biggest killer in low-income countries.
Deaths as a result of NCDs include:2
cardiovascular disease cancer respiratory diseases diabetes
17.9 million 9 million 3.9 million 1.6 million
NCDs can be attributed to several factors: genetic, in the proactive management of NCDs is critical, as
physiological, environmental and behaviours. For interventions provided early to patients reduce the need
example, lack of physical activity, tobacco use, harmful for more expensive treatment. This is therefore a sensible
use of alcohol and unhealthy diets increase the risk of economic investment.
premature death.
Stress, depression, anxiety and other
The forces driving the increase in deaths from NCDs
include: urbanisation, globalisation of unhealthy lifestyles
health conditions are interconnected
and ageing populations.
Stress is considered to be one of the greatest health
challenges facing our global citizens. If stress is not
Despite anti-tobacco laws and monitoring systems, tobacco
managed appropriately, it can lead to mental disorders
use (including non-smokers who are exposed to second-
such as depression and anxiety, as well as other physical
hand smoke) results in over 7.2 million deaths every year
health conditions. It’s estimated that globally more than
and is expected to increase in the future. Tobacco use has
300 million6 people suffer from depression – and it affects
actually declined in some countries, but global population
all ages. Each year, about 800 000 people die as a result
growth means the absolute number of tobacco users is
of suicide. Suicide is the second leading cause of death in
likely to increase.3 These premature deaths cause financial
15- to 29-year-olds.
difficulties for the families and increase healthcare costs.
Tobacco use can also lead to permanent disabilities before
According to a mental health study done in Britain and
death. Smoking tobacco is attributed to 25% of heart
commissioned by the Mental Health Foundation, long-term
disease deaths and 75% of lung disease deaths.4 It’s
conditions, such as cancer, diabetes and heart disease
anticipated that flavoured tobacco will be the next public are risk factors for stress.7 And long-term stress can affect
health threat among young people. sleep, memory and eating habits and increase the risk of
developing physical health conditions such as stomach
About 6.5 trillion cigarettes are sold globally each year. ulcers and heart disease. People who are stressed are more
Only about 20% of the world’s population is protected by likely to respond by over-eating, drinking alcohol, or using
comprehensive national smoke-free laws.5 Research has drugs or tobacco. This in turn leads to being at risk for
found that bans on tobacco advertising could decrease developing certain NCDs. It’s a vicious circle.
tobacco use by about 7% on average. It has also been
found that tax increases that increase the price of tobacco According to the study, another common cause of high
products by 10% can decrease tobacco use by 4% to 5%. stress levels are workplace issues, including working
outside normal hours and poor work–life balance. In
Monitoring trends and the risks of NCDs assists in guiding addition, 22% of respondents said that financial problems,
health policies and priorities. A multi-stakeholder approach especially debt, is a trigger for increased stress. After a
is required to promote interventions to prevent and control review into mental health in the workplace, some British
these diseases. Planning these interventions includes companies are implementing mental health plans at work,
several sectors: health, finance, transport, education, creating awareness and monitoring health and well-being.
agriculture and others. WHO suggests that investing
2
World Health Organization, Noncommunicable diseases, 1 June 2018
3
World Health Organization, WHO report on the global tobacco epidemic, 2017
4
Verywell Mind, Smoking statistics from around the world, Terry Martin, 6 November 2018
5
World Health Organization, Tobacco, 9 March 2018
6
World Health Organization, Depression, 22 March 2018
7
The Guardian, Three in four Britons felt overwhelmed by stress, survey reveals, Denis Campbell, 14 May 2018
4|
HOT TOPICS I 2019
Causes of disability globally A few trends in global risk benefit
design
The causes of death globally are interlinked with the
causes of disability. According to the World Report on Top priorities, identified by Australian employers, for their
Disability, disability prevalence is high and is growing. benefit programmes is to focus on changing benefit designs to
It’s estimated that over a billion people worldwide manage costs (78% of employer respondents) and influence
are living with a disability, of whom 200 million employee behaviours (74% of employer respondents).
experience significant difficulties in functioning in their 9
Importantly, employers have recognised that a narrow
environments.8 strategy of cost containment cannot be effective, and that
employer and employee behaviour itself can be a cost driver.
Disability includes physical, intellectual or sensory Employers are aiming to get a better sense of the drivers for
impairments. The greater the impairment the greater the engagement and behaviour change so that they can better
disadvantage experienced. People living with disabilities connect with employees’ wants and needs. These employers are
experience attitudinal, physical and financial barriers implementing ways to measure the needs of their workforce.
such as:
Although traditional benefits, such as retirement benefits, life
■■ inadequate healthcare insurance and healthcare benefits, continue to be viewed as
■■ lack of rehabilitation services most important to Australian employees, their employers are
■■ low employment opportunities planning to expand on the provision of non-traditional benefits.
■■ lack of access to transport, buildings and information In particular, well-being benefits, including solutions to address
■■ financial challenges from high healthcare expenses financial well-being, are on the rise. In addition, providing
family-friendly programmes, such as additional maternity
leave, and being able to buy or sell leave are gaining popularity.
‘Disability is part of the human condition. Almost Many employers are considering implementing plan designs
every one of us will be permanently or temporarily that provide their employees with choice in their benefits. In
disabled at some point in life.’ – Dr Margaret Chan, addition, effective communication and appropriate decision-
Director-General of WHO support tools are being developed to help employees make
choices that best suit their personal and family needs.
Prevalence of disability is increasing due to: It’s anticipated that up to 74% of Australian employer’s well-
being programmes will be enhanced to better support managing
■■ ageing populations globally, as there is higher risk of stress and mental health over the next three years.
disability in older people
■■ the global increase in chronic health conditions, such Closer to home, a 2017 benefit trend survey,10 showed that
as diabetes, cardiovascular disease, cancer and mental companies in North Africa, Sub-Saharan Africa and South
health disorders Africa are prioritising certain health and well-being benefit
improvements over three years. These priorities include:
Depression is a leading cause of disability globally and
is becoming a major factor in productivity issues in the ■■ behavioural or emotional health management
workplace. Depression is caused by a complex interaction ■■ chronic disease management
of social, psychological and biological factors. Challenges ■■ fitness or activity-based benefits
to effective care include: ■■ lifestyle risk management
■■ lack of resources Behavioural and emotional health management is the main
■■ lack of trained healthcare providers (resulting focus for South African companies. There is a general shift
in misdiagnosis and ineffective care or medical from wellness to well-being, which aims to improve financial
treatments) and emotional health. The Alexander Forbes Benefits
■■ social stigma relating to mental disorders Barometer research publications have shown over the years
how financial stress and health conditions (including mental
The main causes of disability at country level are affected disorders) are interconnected.
by trends in:
As with Australian employers, South African employers have
■■ health conditions, including mental health also been enhancing their benefit offerings by including more
■■ environmental and other factors, for example road choice for employees. A broader range of benefit options to
traffic injuries, natural disasters, conflict, unhealthy employees needs be offered, together with a way for employees
eating habits and substance abuse to assess which benefit options provide the greatest value
to them and their families. The intention is for well-being
Research has shown that disability is more common among programmes to facilitate better decision-making by providing a
women, older people and poorer households. guidance and educational framework.11
8
World Health Organization, World report on disability, 2011
9
Willis Towers Watson, Benefit strategies for tomorrow’s workforce, Insights from the 2017/2018 Australia Benefits Trends Survey
10
Willis Towers Watson, Health and well-being benefits, 2017 Benefits Trends Survey
11
Alexander Forbes, Benefits Barometer, 2017
|5
ALEXANDER FORBES
A closer look at a few global risk 6. Emerging risks:
factors
Climate risk
There are many risks facing the insurance landscape:12 This is one of the most concerning risks facing
global populations as a result of climate change
or global warming, creating new risks and assets
1. Cybersecurity and cybercrime threats
to protect. It was reported that global insured
Dealing with system vulnerabilities and continuously
natural catastrophe losses in 2017 amounted to
staying ahead of cybercriminals is challenging. There
US$135 billion.13 These were the largest losses
is a rising need and regulatory requirements are
ever and were 3.9 times the 30-year average.
increasing to implement effective risk management
The impact was mostly concentrated in North
practices for cyber and data security. America, which suffered 93% of these losses
from hurricanes, wildfires and earthquakes.
2. Fraudulent claims
These continue to remain a big risk for insurance The overall losses were over US$330 billion,
companies. including uninsured losses. Although local
insurers were affected, the reinsurers remained
3. Tech gap resilient with less than a 10% capital impact,
Significant amounts are being invested into insurtech owing to high capital reserves. Evidence of this
(insurance and technology), dealing with blockchain growing risk is the increase in insured loss per
and artificial intelligence for example. year, over the last 10 years as a result of the
effects of climate change. Insurers may have to
4. Higher-than-normal frequency and severity of claims shift their focus from risk management to risk
This has significant impact on the sustainability of prevention. However, this will be a challenging
risk pools in terms of funding levels. task when dealing with the complexities of
climate risk.
5. Traditional approaches don’t meet client needs
Client needs evolve and so should the insurance
industry evolve to meet these new or changing needs. Natural resources
Needs of younger people need to be better met, but With growing global populations, natural
because of increasing global life expectancy there is resources are under threat, in particular fresh
likely to be higher demand for retirement, long-term water and clean air. This also poses new risks
care and longevity products. that need to be managed and assets that need
to be protected.
A general trend across the globe is a shifting of financial responsibility and financial risks from the state to
companies and individuals. And with the emergence of these new risks, it may be that companies and individuals
need to consider how they will protect themselves, potentially through some form of self-insurance, where
uninsurable risks exist.
12
Willis Towers Watson, Midyear update: Most dangerous risks for insurers, July 2018
13
EY, Global insurance trends analysis, June 2018
6|
2
Local perspective on
death and disability
claims
ALEXANDER FORBES
Local perspective on death
and disability claims
Background General claims experience in
perspective
Because group insurance is compulsory, it gives members
who may not normally have access to cover the ability to ASISA (Association for Savings and Investment South
protect their family and themselves. The economies of Africa) confirmed in September 2018 that South African
scale and the cross-subsidy within a group arrangement are life insurers paid R63.7 billion in claims relating to death,
not the only appeal. Depending on the size of the scheme, disability or critical illness over the 12 months ending 30
all members or employees enjoy cover up to the set free June 2018. Claims against employer disability schemes
cover limit without having to provide evidence of good increased by 21% over this period.
health, unlike individual insurance.
In an environment where the only growth is seemingly
While this benefits the individual in the group scheme, the the cost of living and unemployment, employers are
insurer has to assume the type of risk they may be taking under pressure since growth does not meet expectations.
on and price cover accordingly. They take the following into Employees are also under pressure as a result of financial
account: stress and uncertainty. Together, these pressures ultimately
feed into the claims experience through disease, for
■■ Industry example stress-related cardiovascular, psychiatric or
■■ Demographics suicide claims. While this is not directly measurable, the
■■ Age reports indicate more claims have been lodged over the
■■ Gender last three years.
■■ Earnings
■■ Claims experience (where the membership is over 400) Although a number of other benefits are used to meet
■■ Current claimants for disability income needs, this article focuses on group life and disability
income insurance and the claim trends that we
As the claims experience plays out at scheme level, the see generally.
insurer may need to adjust their rates to ensure their
product offering is sustainable long term and the scheme What are South Africans dying of?
is affordable for all stakeholders (members, employees,
the fund and the employer). This approach is followed for Statistics South Africa (Stats SA) presented the mortality
all group insurance, including but not limited to group life and causes of death in South Africa to the media in 2018
assurance, disability income, lump-sum disability, critical based on 456 612 recorded deaths in 2016. Business
illness (dread disease) or funeral cover. Insider1 summarised the top natural killers in South Africa
based on this report.
It is critical when implementing a scheme that the
conditions for cover (for example free cover limits, pre-
existing conditions and any exclusions) are communicated
clearly to scheme members.
1
Business Insider, These are now the top natural killers in South Africa, Phillip de Wet, 27 March 2018
8|HOT TOPICS I 2019
These are set out below by percentage for 2016 covering all age groups compared with 2015.2
Cause of death 2015 2016
1. Tuberculosis 33 063 29 513
2. Diabetes 25 070 25 255
3. ‘Other’ heart disease 22 215 23 515
4. Cerebrovascular disease 22 879 23 137
5. HIV 21 926 21 830
6. Hypertensive disease 19 443 19 960
It should be highlighted that while there is evidence of a decline in some conditions, death as a result of cancer has not been
specifically documented in the report. The larger portion of the natural deaths is noted as ‘Other natural causes’. In 2015
this was recorded as 202 840, which is 44% of the total number of recorded deaths at this time. Although we cannot state
categorically that this number is specifically cancer related, we would expect that a large proportion does relate to cancer. The
2016 number for ‘Other natural causes’ was not provided, but with ‘unnatural causes’ totalling 51 242, we could estimate this
number, which has been climbing over the last three years, to be in excess of 200 000. Bear in mind that the statistics apply to
people of all ages.
The World Health Rankings3, however, have identified the spread of cancer in South Africa by type relative to the rest of the world
as follows:
South Africa cancer rank by type
Age-standardised death rate per 100 000 population
GOOD POOR
Rate World rank
1. Prostate cancer 35.07 21
2. Cervical cancer 20.99 32
3. Lung cancers 20.75 57
4. Breast cancer 20.75 51
5. Oesophagus cancer 10.53 15
6. Colon-rectum cancers 10.45 72
7. Lymphomas 8.06 15
8. Pancreatic cancer 6.04 51
9. Ovarian cancer 5.65 48
10. Liver cancer 5.60 87
11. Stomach cancer 4.69 113
12. Skin cancers 4.48 4
13. Oral cancers 3.92 69
14. Leukemia 3.76 101
15. Uterine cancer 2.31 82
16. Bladder cancer 2.27 77
2
Stats SA, Mortality and causes of death in South Africa, 2015: Findings from death notification
3
Word Life Expectancy website, world health rankings page (www.worldlifeexpectancy.com), 13 February 2019 (online)
|9ALEXANDER FORBES
Cancer is personal for most of us, where we have either In addition, in March 2015, the tax treatment of disability
been personally affected or have a family member, friend income benefits changed, allowing for the monthly
or colleague battling this disease. This has led to a greater benefit to be paid tax free to the claimant. This applied
demand for critical illness (dread disease) benefits to to existing claims in payment as well as new claims. The
be provided on a group basis to complement death and concern has been that there is no longer an incentive
disability cover. With greater awareness4 of health, early for claimants to rehabilitate, as they could be better off
detection and treatment of cancer and other critical disabled than working, which is contrary to the general
illnesses, there has been a rise in the take-up of this principles of disability insurance. Coupled with the poor
type of cover to pay for treatment costs where there are economy, a disabled employee who previously would have
shortfalls. SwissRe’s 2017 survey5 showed an increase of been accommodated in the workplace would now apply
58% in take-up compared to 2015. for disability.
Stats SA notes that deaths related to HIV have declined in While we noted that it is not directly measurable, disability
the medium to long term, which demonstrates the positive income claims tend to increase when the economy is under
effect of early intervention and the introduction of and strain. The impact of potential job losses and increases in
accessibility to antiretroviral treatment. However, on the the cost of living results in financial stress, which could
disability income side, we still see HIV Aids as a significant lead to physical or mental illnesses or both. As highlighted,
(although declining) contributor to the claims experience. ASISA found that claims against employer disability
schemes increased by 21%.
Most insurers noted that while they were seeing an
increase in the number of claims, there was also an SwissRe6 also found that the average benefit for disability
increase in respect of higher income earners claiming, income increased over the period. Most insurers have
resulting in an increase in the average size of the death reported that both the number of claims since 2015 and
benefit paid. Potential key drivers here being stress and the number of higher income earners applying for disability
lifestyle-related diseases. have increased.
Disability: protecting your income The current state of the economy makes it difficult to
correlate the higher claims directly to the change in the
when you are no longer able to work
tax treatment of the benefit. Most insurers believe that it
relates to a combination of factors, including:
Disability income benefits offer employees a lifeline
when they are unable to work as a result of illness or
■■ greater awareness of benefits
injury, whether this is temporary or permanent. This
■■ an increase in lifestyle-related illnesses
benefit insures for loss of income based on the terms and
■■ the economy
conditions of the policy until the claimant recovers, dies
■■ tax changes
or reaches company retirement age, whichever occurs
first. The merits of this benefit as a long-term solution for
Although income tax relief has been noted as one of the
employees are significant.
contributing factors to increases in disability claims, it’s
important to remember that, for most companies, the
The liability of providing this income sits on the insurers’
disability income benefit is about 75% of pensionable
balance sheet. The increase in not only the number of
salary. Pensionable salary is normally less than 100% of
claims but also the value of claims is now at a critical
total earnings. Most South African employers use about
state, threatening to affect the long-term sustainability of
70% to 75%, as a percentage of total earnings, as the
this product offering and the product itself. This does not
most common pensionable salary. This means that the
mean that there are no assets to pay the insured claims,
disability income benefits for many members average
but the pressure of future claims on a book that is already
around 52% to 60% of total earnings which seems low
under pressure could have major ramifications, such as
even considering the tax treatment. Where companies
increased premiums. The struggle is a reality for group
have inappropriately high disability income benefits,
insurance business, where almost all insurers reported
these should be revised, taking the change in tax
losses, decreased profitability or both as a result of higher
treatment into account.
claims experience on their group business.
4
Sanlam, The Sanlam Benchmark Survey, Research summary, A disabled economy, Michele Jennings, 2018
5
SwissRe, Group Volume Survey, 2017
6
SwissRe, Group Volume Survey, 2017
10 |HOT TOPICS I 2019
Capital Alliance noted that, in general, it is difficult to positions are available in the open labour market given
rehabilitate claimants back into the workplace for the the current economic conditions.
following reasons: ■■ Earning potential
There is minimal motivation to return to work if we
■■ Incapacity procedures compare earning potential after having been declared
Once admitted as a valid claim, many companies end disabled with the untaxed disability income benefit
the individual’s employment as a result of incapacity. amount.
■■ Broad unemployment
It becomes difficult to assist individuals in finding Ultimately, claimants remain on disability for much longer
alternative placement, especially at their own employer, than in the past, with little chance of rehabilitation, the
during the initial period where their employment has longer the claim remains in payment.
been ended as a result of incapacity. In addition, few
What are the main causes?
Musculoskeletal disease and cancer are common threads across the insurers’ data. While there are still a high number of claims
for HIV Aids, there are areas where the stats are improving. Psychiatric claims are more subjective, but in the world of increased
financial pressure and general levels of stress the number of claims is increasing.
An analysis on the Alexander Forbes group insurance book with Momentum7 provided some observations over the 2010 to 2018
period on the top three causes of disability:
Industry classes 2010 to 2018 2010 to 2014
Cause Cause
1 2 3 1 2 3
Financial services
Banking Psychological Neurological Psychological Neurological
Cancer Cancer
Law firms illness illness illness illness
Engineering (off site)
IT and telecoms administration
Musculoskeletal Psychological Musculoskeletal Psychological
Professional and administrative Cancer Cancer
disease illness disease illness
services
Health and welfare – private
hospitals
Musculoskeletal Respiratory Musculoskeletal Respiratory
Nursing and residential care Cancer Cancer
disease illness disease illness
Entertainment and hospitality
Education
Transport – logistics
Agriculture – farming on site Musculoskeletal Musculoskeletal
Cancer HIV Aids Cancer HIV Aids
Manufacturing – brewery, disease disease
chemicals and allied products
General construction labour
Manufacturing – machinery
and heavy equipment Neurological Musculoskeletal Neurological Musculoskeletal
Cancer Cancer
Fishing factories and trawlers illness disease illness disease
Government and state organs –
municipal workers
Musculoskeletal Neurological Musculoskeletal
Heavy mining Spinal injury HIV Aids Cancer
disease illness disease
From the above, it is evident that there has not been much change in the top three causes of disability in each industry class over
both periods.
7
Momentum, Income disability insights – Alexander Forbes’s Momentum Client Book
| 11ALEXANDER FORBES
The causes highlighted on the Alexander Forbes book with This is consistent with findings from Maredza and Chola,
Capital Alliance over the five-year period ending 2015 20168 in their research on major causes of disability in
related mostly to musculoskeletal disease, HIV Aids and South Africa and the experience that we see from other
cancer. On the whole, these are similar to the main causes insurers:
highlighted in the Momentum data.
■■ musculoskeletal illness (arthritis)
Old Mutual conducted a survey in 2017, where the ■■ cardio-vascular and cerebral-vascular illness (stroke)
respondents ranged from insurers to intermediaries, ■■ cancer
reinsurers and corporates. Based on this, consensus was
that the disabilities on the increase were: Globally these concerns are similar.
stress-related or stress-induced illness Premiums will continue to increase to balance the liability
relative to the benefit and the trends of the:
■■ increasing number of claims
psychological illness ■■ higher value of claims
■■ difficulty of incentivising and rehabilitating claimants
where there is seemingly no opportunity for
musculoskeletal illness employment
What can be done by our industry
and corporate South Africa to reduce
lifestyle-related disease – diabetes, heart disease,
obesity claims?
There is no easy solution. Early intervention, however, is
key. Having an overarching financial well-being philosophy
cancers that not only looks after physical health but also recognises
and addresses financial stressors will go a long way in
ensuring physically and mentally healthy people at work.
8
Disability Gauteng website, Major causes of disability in South Africa, May 2017 newsletter (www.disabilitygauteng.org), 13 February 2019 (online)
12 |HOT TOPICS I 2019
3
Proactive claims
management
| 13ALEXANDER FORBES
Proactive claims management
How can an employer proactively According to John Greenwood, Corporate Adviser, 7
manage potential claims? February 2019, more than a fifth of British businesses
say they lack the expertise to manage sickness absence
effectively, with the proportion even higher for small
‘A spike in disability claims has hit the profits of all SA’s
businesses. This is no different in South Africa. According
life assurers hard over the past year, with claims experience
to a study by Zurich Insurer, employers could be leaving
deteriorating across the industry because of the economic themselves exposed to losing skilled employees and
downturn and a change to tax rules.’ – Hilary Joffe dealing with reduced productivity. This has an impact
(Business Day), 13 March 2017 on the bottom line, through extended and unmanaged
sickness absence.
In 2018 insurance companies once again saw an increase
in disability claims. Many of these claims were for Organisations can play a role through early identification
psychiatric as well as musculoskeletal conditions such as and management of potential mental and behavioural
fractures, backache and spinal conditions. conditions. The first signs can be observed in absenteeism
trends and extended sick leave. Through sick leave
Alexander Forbes Health Management Solutions has management, short frequent absences should trigger
reported mental and behavioural conditions, including a red flag and prompt early investigation to provide
stress-related conditions, as the leading reasons for our necessary support.
clients’ long-term disability cases from 2016 to 2018.
Close monitoring is required, especially within the
These conditions were followed by musculoskeletal
extended sick leave period of 14 days or more, as this
conditions and cancer-related conditions, which are on
will indicate the potential for prolonged absenteeism from
the rise. Mental and behavioural conditions make up work, which may lead to a disability claim.
24% of all long-term incapacity and disability cases while
musculoskeletal conditions account for about 16%. Instead of effectively managing the disability process,
employers rush to settle cases within the legislated
Cancer-related conditions and circulatory conditions make period, handing disabled employees over to their insurers
up nearly 12% of all cases submitted. The concern is for income replacement benefits or the payment of a
that employees claiming for cancer-related conditions are lump sum. As a result of new tax legislation on disability
getting younger. Organisations face increased pressure benefits, there is now less incentive to return to work after
to ensure that well-designed wellness programmes are in a short period on an income replacement benefit.
place as support for employees.
As a result of the above, claims experience increases and
With greater work pressure, high inflation, a growing rate of the cost to the fund increases. Boarding a 43-year-old
unemployment and the increasing cost of living, individuals male with a monthly salary of R8 494 costs the company’s
group benefit scheme R1.3 million. So, ‘successfully
find themselves burdened by debt and societal pressures.
retraining the same employee, and others like him, into
This, in turn, leads to high stress levels.
a suitable alternative occupation will save the company
scheme approximately R1.3 million per case,’ says
Disability claims, however, cannot be seen in Anton Engelbrecht, Business Development and Strategic
isolation. They need to be looked at together with Consultant, Alexander Forbes Health.
sickness absence and incapacity in the workplace.
14 |HOT TOPICS I 2019
Employee wellness programmes that emphasise case issues from the employee wellness programme. A holistic
management and face-to-face counselling sessions are integrated approach involving all the service providers
beneficial if they are started early and during treatment. needs to be used to ensure that employees are motivated
Early management of psychiatric disorders is critical to and productive in the workplace.
limit time away from work. It becomes a challenge for an
employee to return to work after a prolonged absence.
This will allow the company to understand:
Employees who have access to support through their
employer’s group benefits (for example employee ■■ the health and well-being issues that employers
assistance programmes, absenteeism and incapacity and employees are grappling with and their
management or a rehabilitation benefit) tend to return to impact on the health and well-being of the
work sooner and more successfully than those who don’t. organisation
■■ the impact of the organisation’s policies, culture
Organisations worldwide have largely accepted the merits and environment on the health and well-being of
of employee wellness. The interrelatedness of employee its employees
health and organisational well-being is acknowledged. ■■ short-term and long-term strategic objectives
Healthy employees are generally more productive, have around employee health and organisational well-
lower rates of absenteeism and are more engaged. They’re being
also better able to manage stress and change, enjoy higher ■■ where targeted interventions are required
job satisfaction and have positive morale. ■■ where benefit offerings are duplicated, which
will help the organisation identify greater cost
Workplace incapacity that is not managed quickly and efficiencies within the well-being programmes.
effectively can result in financial and reputational risk
for the company as well as an increase in disability
claims. Poor realignment and performance management Many companies face a lack of data integration, which
can result in an employee suffering multiple relapses often leads to their well-being programmes not being used
of their condition, requiring longer periods off work. effectively. For example, medical scheme wellness reports
This, ultimately, can lead to a disability claim. Early provide data on many aspects of employees’ physical
management allows for adequate case management if an and lifestyle health. However, without organisations
employee does require time off work or accommodations understanding the impact that those aliments are having
in the workplace, or even a period on an income protection on the business (and the correlation with sickness absence
benefit. This allows realignment into another occupation data and disability data), very little is done with the
earlier, which also reduces claims experience. information provided.
Another way to manage the increase in claims is through Alexander Forbes Health Management Solutions has found
an effective absenteeism management programme. This through many interventions that high-risk employees can
aims to reduce the adverse effects of absenteeism, such be proactively managed to reduce the impact of reported or
as increased costs, low employee morale and employees actual medical conditions on their vocational functioning.
taking on extra work. An absenteeism management This, in turn, reduces their use of sick leave. It also helps
programme should involve a thorough analysis of to identify employees with genuine medical conditions
absenteeism data to highlight trends and any pertinent compared with employees who may be misusing sick leave.
Organisations that focus on employee well-being seek to reap the rewards associated
with a healthy workforce:
lower absenteeism All this contributes
to a competitive
fewer workers’ compensation claims and sustainable
organisation and
reduced disabilities fewer disability
claims.
greater workplace safety, productivity and performance
| 15ALEXANDER FORBES
By actively managing incapacity in the workplace, the
employer can also be confident that they have fulfilled their
legal obligation of investigating each disability claim in line To summarise, the potential intervention strategies
with the Labour Relations Act, Schedule 8. that can be considered by employers, insurers
and group scheme arrangements may include the
Organisations may not realise the saving initially when following:
managing sick leave actively. However, results have shown
a reduction in the costs and increase in productivity in ■■ Early intervention by identifying high-risk
the workplace. An example of this can be seen in one of employees through sickness absenteeism
Alexander Forbes Health Management Solutions’ larger management programmes, extended sick leave
national clients, where a reduction of the sickness absence and early referral for interventions
ratio went from 5.8% to 1.4% over a four-year period. This ■■ Managing expectations of employees
is a significant saving to the bottom line and a reduction in and managers in maintaining employees’
the disability risk pool. productivity even during temporary incapacity
■■ Ensuring the provision of skills development
Taking all this information into account, there are different and further training at the time of incapacity
approaches and empowering methodologies for helping to consider alternative employment routes and
employers to manage employees who have been affected career advancement opportunities
by personal or medical challenges. The aim is to empower ■■ Ensuring that all human resources policies
managers to handle employee issues fairly and equitably comply with relevant legislation: the
in relation to the impact of the medical condition on the Employment Equity Act, the Labour Relations
employee’s performance. One way of doing this is through Act and the Code of Best Practice
health risk management workshops, which equip managers ■■ Providing a disabled-friendly environment that
with the skills to manage wellness issues in the workplace is physically accessible as well as socially and
and ensure compliance with all legislative requirements. professionally accommodating
■■ Providing active case management, clinically
The Code of Best Practice of Key Aspects of Disability and vocationally, to enable employees
in the Workplace issued by the Department of Labour with disabilities to return to their place of
provides a guideline for employers, employees and their employment or find alternative income-
representatives to develop, implement and refine disability generating opportunities
equity policies and programmes to suit the needs of their
respective workplaces.
While the intention of the legislation is that such practice Apart from being the right thing to do, getting this process
becomes internalised within organisations, the truth is right sees a reduction in the costs of disability claims on
that human resources skills, practice and capacity in many group benefit schemes and ensures legislative compliance
South African organisations is limited when it comes to while retaining skills within the business.
managing this process within the tight deadlines imposed
by legislation.
An alternative is to outsource the design of an
organisation’s disability management strategy. This will
not only allow the strategy to meet legislative requirements
while assisting the employer to become ‘an employer of
choice’, but also help to retain skills while saving costs for
the group benefit scheme.
16 |HOT TOPICS I 2018
4
Group risk benefit
design
| 17Group risk benefit design
Background Why are group benefits so important?
The goal has always been to maximise as much towards Employees rely on their employer to provide benefits in
retirement savings as possible, with risk benefits the event of death or disability. Providing targeted benefits
structured to target an average benefit offering for the through the employee benefit programme not only meets
cheapest premium. the needs and expectations of employees, but also enables
the employer to provide a cost-efficient and meaningful
Looking at risk benefits from a different angle, and in the benefit programme. Most employees rely solely on these
context of supporting individuals throughout their lives, benefits and don’t have the financial means to add to these
the goal should be to optimise exposure to benefits as life benefits in their personal capacity.
dynamics change. For most, the benefit design needs to
be done within the cost and contribution constraints of a To illustrate this point: True South Actuaries and
fund. However, flexibility, and the opportunity to give the Consultants calculated the insurance gap by referring to
individual access to more, does exist within the confines of the financial impact on South African households when
a group arrangement. an active earner in a household dies or becomes disabled.
They conducted this study1 for the Association of Savings
Why? Group insurance provides cross-subsidy of rates, and Investment South Africa (ASISA). The gap considers
economies of scale and, importantly, access to cover group and individual insurance and assesses what is
without providing evidence of good health within needed as opposed to what is covered. The significant
certain limits. levels of underinsurance for both life and disability benefits
were confirmed as follows:
A well-constructed risk benefit offering not only gives
members the ability to target their personal holistic needs,
but also strengthens the overall employee value proposition Underinsurance
(EVP) for the employer.
Life insurance
2010 R7.3 trillion
Currently, benefits are mostly structured on a ‘one-size
fits all’ approach based on the average member. There
is, however, growing interest in providing a more flexible 2013 R9.3 trillion
approach to benefits and introducing other benefits to
complement the current offering, for example critical 2016 R12.9 trillion
illness (dread disease).
Disability income
Disability benefits allow for less flexibility on a group basis. 2010 R11.1 trillion
However, these benefits can be reviewed to better meet
outcomes and gaps. 2013 R14.7 trillion
Additional group benefits do come at a cost, so it’s
important to consider how these are priced and funded to 2016 R15.9 trillion
ensure sustainability.
1
ASISA. 2016. The South African insurance gap (2016). A study by True South Actuaries and Consultants
18 |HOT TOPICS I 2019
Group risk is important and if we are able to better meet The benefit offering needs to balance wealth accumulation
the needs of individuals within the confines of the group and wealth protection throughout the individual’s journey.
arrangements, we can promote better coverage. Here’s why:
With the retirement–risk trade-off, risk benefits should
■■ Group risk is compulsory cover and is often the only not be considered in isolation. The design and review
cover individuals (and therefore their families) have. should be in the context of the fund offering and the
■■ Individuals tend to have an aversion to insurance: EVP, which would guide where these benefits sit, how
• Need additional disposable income to pay for cover they can be funded and how they complement the overall
• Cover takes time to implement and may require value proposition.
medicals at the outset
• Cover is costed on rate per age and may be more Everyone has individual needs
expensive.
■■ There is usually little or no financial planning outside Everyone has their own specific needs and different time
the fund and employee benefit programme. horizons, while most benefits are based on an average.
■■ Ultimately, employees rely on the employer. An
underinsured disabled employee puts pressure on the An extended offering to individuals within a group allows
employer and, in the event of death, the employee’s for benefits to be provided cost efficiently. It also gives
family would likely approach the employer for them access to benefits that they would perhaps not have
assistance or benefits. considered or had access to as individuals.
Reviewing the benefit offering and assessing whether the Understanding the membership and how and what
current design is suitable is also supported by Treating is available for providing benefits clears the way to
Customers Fairly (TCF), which is embedded into the new assess underlying needs of members and matching
policyholder protection rules (PPR). The design therefore appropriate solutions.
must provide:
■■ products and services to meet customers’ needs
■■ good advice that suits customers’ circumstances
Identifying needs
To review the offering and provide an appropriate solution in a needs-based framework,
the following will need to be considered:
Financial
Time horizon: Needs-based
Financial Risk sophistication
Sector age profile of the benefit
constraints appetite and the level of
membership framework
education
■■ Member’s needs ■■ Equity
■■ Type of job ■■ Age cross-subsidies
■■ Earnings ■■ Simplicity
■■ Remuneration structure (total cost to company, ■■ Practicality of implementation
basic plus)
■■ Associated costs
■■ Labour relations issues
Current employee value proposition (EVP)
| 19ALEXANDER FORBES
Gap analysis
While most benefit design is done with the board of trustees or management committees, additional information is needed from
the employer to ensure that the offering does not contradict, but rather supports and complements, the current EVP. For example,
are there stated benefits, funeral benefits through a union or medical aid scheme, or a sick fund? This provides an ideal way to
consider any gaps or overlaps as well as to identify possible benefit improvements to ensure a holistic benefit offering.
Benefit design
Death benefits
The actual death benefit (insured multiple and accumulated fund credit) provided to members can be compared against a
‘benchmark need’. This is assumed to be the capital expected to be enough to provide for a targeted spouse’s pension of 60% of
pensionable salary on death.
The table below shows the total shortfall against the benchmark need by age and service. The average shortfall can be presented
as follows:
Required
Adjusted multiple of salary Actual multiple of
Age band multiple of Shortfall
including 'savings' salary
salary
20 to 25 13.5 13.5 3.7 9.8
25 to 30 13.0 13.4 3.6 9.8
30 to 35 12.5 12.9 3.6 9.3
35 to 40 11.7 11.4 3.5 7.9
40 to 45 10.5 9.5 3.4 6.1
45 to 50 9.2 7.2 3.3 3.9
50 to 55 7.7 4.6 3.2 1.4
55 to 60 6.2 2.0 3.0 (1.0)
> 60 4.8 0.3 3.1 (2.8)
Source: Benefits Barometer
Defined benefit versus defined contribution
Most death benefits are structured on defined benefit risk rather than on affordability.
R
Defined contribution risk Defined benefit risk
The amount of money available to spend on benefits The level of cover is fixed and defined in the policy.
is set. The benefit selection is then limited to what The premium will vary based on the cost of providing
can be afforded. As a result, the cover will vary from the benefit for a particular membership group.
time to time depending on affordability. An approved
fund will need to make sure that the fund rules
accommodate a varying level of cover.
20 |HOT TOPICS I 2019
Is there an optimum design?
Benefit structures with full flexibility
Increasing risk
of individual Appropriate solution lies
shortfall or excess between the two extremes
Increasing risk of if you have appropriate
behavioural factors support mechanisms
influencing choices
Fixed benefit structures
It is important to go through the process of assessing the The following must be considered in reviewing the
various risk benefit structures and what is suitable, given appropriateness of the design and structure of the benefit:
the data gathered from the fund and employer. Each
alternative can be measured against a set of criteria to ■■ Remuneration structure – key to establishing if there
get a better feel for what is being assessed and what is will be any benefit capping on the disability income
needed: side
■■ Incapacity procedure
■■ Needs ■■ What has been contracted with the individual and
■■ Simplicity stated in the individual’s contract of employment?
■■ Cost
■■ Equity The needs-based framework, financial constraints, and so
■■ Age cross-subsidies on, all contribute to the decisions taken in deciding which
■■ Practicality benefit is most suitable for members.
Disability benefit choices Let’s have a look at a few ways of setting up cover.
Identifying the intention of the benefit will assist in Typical benefit structures
identifying the appropriate solution. Is the disability benefit
required to: Death
While the current approach provides for an average benefit
■■ cover total and permanent disability? structure, would a customised solution to help individuals
■■ cover temporary disability, total and permanent balance their needs throughout their working lifetime be
disability or both? more appropriate? In designing a death benefit offering,
■■ provide replacement of income during disability? there are a number of solutions to consider:
■■ provide a lump sum to pay once-off and to retire the
disabled individual as a result of ill-health? ■■ Flat multiple of cover
• Spouse’s benefits or critical illness benefits, for
What do the members need or which type of structure example, may be a flat multiple and then limited to
would be most beneficial for the members? a flat rand maximum benefit
■■ Age-related benefits
In assessing the structure and level of the disability ■■ Lifecycle risk approach
benefit, engagement with the employer is critical as design ■■ Flexible risk benefits
or changes in this benefit may have an impact on the • Full flexibility within a range
employer–employee relationship and even the contract of • Flat core level of cover with voluntary buy-up
employment. ■■ Top-up cover – voluntary
■■ Tax replacement cover
■■ Accidental death cover
| 21ALEXANDER FORBES
Disability benefits In short, the difference between the tax treatment is as
Firstly, the benefit type would need to be selected follows:
based on the intention and need identified. The level of
benefit and waiting period would then also need to be Approved Unapproved
established, taking into account the employer’s incapacity
procedure. Consider potential limitations of benefits since No fringe benefit tax on
the income benefit is tax free. This means considering Fringe benefit tax on premium
premium
the benefit relative to the total guaranteed package and
where a claimant could potentially be better off disabled Benefit proceeds are
than working. taxed in terms of the Benefit proceeds are paid tax
legislated benefit tax free
Currently there is no room for individual flexibility in the scale
level of benefit. However, there may be a mix of benefits,
Fund-owned policy: Employer-owned policy:
for example an income benefit and a lump-sum benefit,
that are compulsory for employees or categories of ■■ Group life
employees. The waiting periods for these benefits can vary, ■■ Critical illness (dread
along with a number of ‘add-on’ benefits, such as employer disease)
waiver, health premium waiver, and so on. ■■ Disability income benefit
■■ Group life ■■ Temporary and total
The disability definition really sets the basis for the ■■ Lump-sum disability disability (TTD)
disability application and assessment, for example the ■■ Funeral
definition may be ‘own’ occupation or job with ‘own’ ■■ Lump-sum disability
employer for the first two years, thereafter, ‘own or any’ ■■ Spouse’s cover
occupation or job with ‘any’ employer. It is important to ■■ Education benefit
note that the definition of job compared with occupation
can also have different interpretations. Understanding Where the potential tax payable in the event of a claim
the definitions relative to the benefit that is needed, and is raised as an issue, introducing tax replacement cover
communicating this effectively to members, is critical. is a way to mitigate the tax that would be payable on an
approved insured death benefit. However, it is important to
Consider the following disability benefit structures: understand that the tax legislation at the time of the claim
determines the calculation of the benefit in this instance.
■■ Disability income benefit or permanent health The calculation only takes into account the insured benefit
insurance: and not the member’s fund credit. This benefit is priced on
• Flat scale of 75% of income the potential liability as determined based on the insured
• Scaled benefit cover only.
■■ Managed disability income – rehabilitation and re-
integration is key For some, the tax treatment or the avoidance of paying
• Flat scale of 75% of income tax on the end benefit becomes a discussion on approved
• Scaled benefit versus unapproved. Although this does provide for the tax-
■■ Temporary and total disability (TTD) free payment of the death benefit, it changes the overall
• Limited-term disability income benefit normally structure and intent of the benefit. From a cost point
coupled with a lump-sum disability benefit of view, the increase in the premium to provide the tax
■■ Lump-sum disability or permanent and total disability replacement cover can be measured against the level of
• Flat multiple of salary fringe benefit tax applicable should the benefit move to an
• Flat rand amount unapproved basis.
• Fund-owned benefit or employer-owned benefit –
there are practical implications for how and why
Concluding remarks
this may be structured this way.
It is important to review and ensure that the design of
Tax status the benefits, within the context of the fund itself, still
meets the fund’s overall long-term objectives. There is
The tax status of the death benefit offering can be based scope, along with solutions, to design an employee benefit
on whether benefits are approved (a fund-owned policy) or package not only for the average group through appropriate
unapproved (employer-owned policy). Depending on how smart defaults, but to give the individual member greater
this is structured, there will be an impact on the treatment flexibility.
of the premium and benefit for tax purposes. Whether this
is a fund-owned or employer-owned policy will also impact The discussion on the design of the benefits and the
on how the benefit can be distributed at the date of death. different types of benefits available is extensive. While
we’ve tried to cover as much as possible in this article,
All other policies (disability income, spouses cover, critical not all variables have been included. Please speak to your
illness, funeral benefits) are unapproved benefits, while consultant to learn more about any aspect of your risk
lump-sum disability benefits can be structured on a fund- insurance.
owned or employer-owned basis.
22 |You can also read