Acute Vestibular Syndrome in Cerebellar Infarction: A Case Report
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
International Journal of Research and Review
DOI: https://doi.org/10.52403/ijrr.20210906
Vol.8; Issue: 9; September 2021
Website: www.ijrrjournal.com
Case Report E-ISSN: 2349-9788; P-ISSN: 2454-2237
Acute Vestibular Syndrome in Cerebellar
Infarction: A Case Report
Diayanti Tenti Lestari1, Hanik Badriyah Hidayati2
1
Department of Neurology, 2Department of Neurology,
Faculty of Medicine, Airlangga University, Surabaya, Indonesia
Corresponding Author: Diayanti Tenti Lestari
ABSTRACT Keywords: acute vestibular syndrome, vertigo,
cerebellum, HINTS
Introduction: Acute vestibular syndrome
(AVS) is characterized by rapid onset of vertigo, INTRODUCTION
nausea and vomiting, and gait unsteadiness in Acute vestibular syndrome is
association with head motion intolerance and characterized by the sudden onset of
nystagmus, lasting days to weeks. Although the dizziness/vertigo, nausea and vomiting, and
majority of AVS patients have acute peripheral
unsteadiness that lasts from days to weeks.
vestibulopathy, some may also have brainstem
or cerebellar strokes. Cerebellar infarctions This syndrome causes static and dynamic
sometimes only cause vertigo. The Head imbalances in the vestibular system on one
Impulse Test, skew deviation, and nystagmus or both body sides.(1) The occurrence of
testing provide for great sensitivity and dizziness/vertigo due to central lesions
specificity in distinguishing between peripheral usually occurs in association with other
vestibular impairment and stroke. neurological signs and symptoms, and the
Case: A 41-year-old male patient suffered from diagnosis of vertigo is isolated from lesions
acute-onset vertigo and dizziness about 5 hours of the brainstem and cerebellum. (1)
before admission, which started when he started Dizziness/vertigo is the most common
doing his morning routine. Patients also feel gait symptom of the posterior circulation
unsteadiness and almost fall to the left side.
ischemia. Based on literature, 62% patients
There was no weakness in extremities, skew
face or slurred speech. Patient's neurological with vertigo due to vertebrobasilar
status showed the cerebellar examination was infarction had at least one episode of vertigo
positive left dysmetria, left dysdiadochokinesia, and 19% patients presented vertigo as the
the Romberg test open eye fell to the left, initial symptom. (1) Acute vestibular
normal Head Impulse Test (HIT), with syndrome due to stroke is mostly due to
horizontal bidirectional nystagmus and negative lesions in the posterior inferior cerebellar
skew deviation test. Cerebellum infarction was artery (PICA) region of cerebellum. (2)
discovered using computed tomography Cerebellum lesions cause variety of
imaging. After passing through the acute stroke audiovestibular symptoms and nystagmus.
period, patients are offered symptomatic therapy (2) Nystagmus is caused by damage to the
in the form of betahistine, antiplatelet
intercalate nucleus and paramedian tract
medication, and vestibular rehabilitation
planning. On the tenth day after the onset, the (PMT) cell group. (2)
patient's symptoms began to improve. Dizziness and vertigo assemble for
Conclusion: Proper diagnosis of acute 4.0% of visits to the emergency department
vestibular syndrome will guide the necessary and associated stroke in 3.2–4.0% of cases.
tests. The HINTS oculomotor test at the bedside (2,3) Data show that approximately 15000
can detect acute vestibular stroke. to 25000 cases have a morbidity due to
misdiagnoses at the time of initial
International Journal of Research and Review (ijrrjournal.com) 29
Vol.8; Issue: 9; September 2021
Diayanti Tenti Lestari et.al. Acute vestibular syndrome in cerebellar infarction: a case report.
admission. (4) Twenty-five percent of The prevalence of the causes of
patients with vascular risk factors who vertigo/dizziness Cerebrovascular in acute
present to emergency department with vestibular syndrome group was 10.0 % of
isolated severe vertigo, nystagmus, and strokes and transitory ischemic attack (TIA),
postural instability, turned out to have this is higher when compared to the
cerebellar infarction in the region of the occurrence of cerebrovascular causes among
medial posterior inferior cerebellar artery vertigo/dizziness patients who are not acute
PICA (mPICA) region. (5) Dizziness/ vestibular syndrome as much as 3.6%. (3)
vertigo caused by acute vestibular syndrome This paper is intended to aid in the study of
have three times higher risk of dizziness or sudden vertigo in posterior
cerebrovascular causes than dizziness circulation strokes, particularly cerebellar
without the syndrome of vestibular acute. infarction.
CASE REPORT
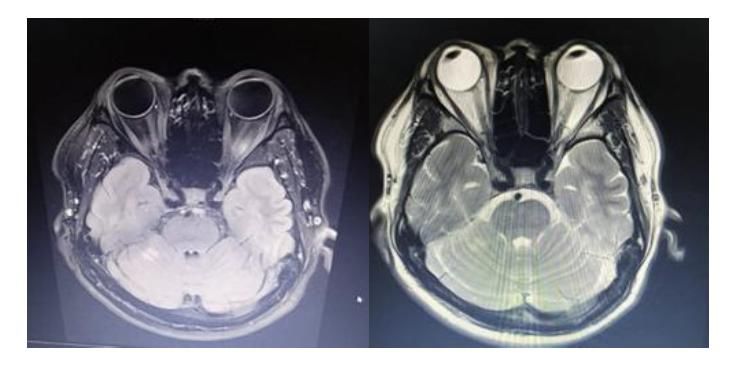
Figure 1. Computed Tomography CT scan of the head without contrast, axial section; acute infarction of the cerebellum
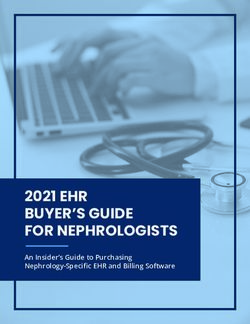
Figure 2. Magnetic Resonance Imaging (MRI) of the Head; Restricted diffusion on Diffuse weight Imaging (DWI), cerebellar
hyperintense on T2 Fluid Attenuates Inversion Recovery FLAIR
A 41-year-old man suffered from patient described that the head is floating as
acute-onset vertigo and dizziness about 5 if it is light and everything around him
hours before admission, which started when seemed to be moving. The symptoms were
he started doing his morning routine. The not prompted by changes in his head, and
International Journal of Research and Review (ijrrjournal.com) 30
Vol.8; Issue: 9; September 2021Diayanti Tenti Lestari et.al. Acute vestibular syndrome in cerebellar infarction: a case report.
they did not improve with sleep. The percent. Cerebellar infarct, hypodense
patient stated that he would want to fall to region in the cerebellum, can be seen on a
his left side. The patient's hands and feet are CT scan of the head without contrast.
unaffected. On the route to the hospital, the After the initial phase of the stroke,
patient vomits, his head jerks, and he patients were given betahistine 24 mg every
becomes uneasy. He denied any previous 12 hours, Amlodipine 10 mg every 24
headaches, tingling, visual field hours, Domperidone 1 tablet every 12 hours
abnormalities, double vision, swallowing or as required, Acetyl Salicylic Acid 100 mg
difficulties, convulsions, or fever. The every 24 hours, Simvastatin 20 mg every 24
patient's previous medical history includes hours, and Cawthorne-Cooksey exercise.
hypertension from 5 to 6 years ago, which
was not routinely treated, and no previous DISCUSSION
stroke, tumor, or lump elsewhere, which the Acute vestibular syndrome (AVS) is
patient disputed. Traditional medicine was characterized by acute onset of prolonged
used previously, and no painkillers were vertigo (days to weeks) with spontaneous
used. Patient has been a 15-year smoker nystagnation, postural instability and
who smokes 5-10 cigarettes per day and autonomic symptoms such as nausea or
does not drink alcohol. There are no vomiting. (1,4,5) Eleven percent of patients
relatives with hypertension, heart disease, with cerebellar infarction showed clinically
diabetes mellitus, or stroke in the family isolated vertigo and most (96%) had medial
history. Blood pressure was 210/150 branch PICA territory infarction, including
mmHg, pulse was 98 beats per minute, nodules. (6) Cerebellar stroke will cause
respiratory rate was 18-20x/minute, severe ataxia, visual disturbances, headache,
temperature 36.6° Celsius on general and vertigo. However, about 10% of
examination. Bidirectional horizontal patients with cerebellar infarction
nystagmus without hearing loss, excellent experience only vertigo or nausea and
motor function, and normal exteroceptive vomiting. (7)
and proprioceptive sensory were discovered Pathophysiology of acute vestibular
on neurological examination. Both sides of syndrome on cerebellum lesions is
the extremities have normal deep tendon associated with vestibular pathway and
reflexes, with no abnormal or primitive vascularisation into the vestibular system.
reflexes. Dysmetria on the left side, left The cerebellum receives projections from
dysdiadochokinesia, positive Romberg's the vestibular labyrinth, vestibular nerve,
test, and a fall to the left side were the and vestibular nucleus in the brainstem and
cerebellar signs. The Head Impulse HIT test the projections back to the vestibular
revealed a bidirectional horizontal nucleus to control oculomotor and postural
nystagmus and no ocular deviation, which reflexes. The cerebellum is also involved in
were both within normal ranges. Fasting the visual suppression of ocular vestibular
glucose readings were 113 mg/dl, responses, including nystagmus caused by
postprandial blood sugar was 150 mg/dl; acute vestibular dysfunction. (8) The blood
urea was 15 mg/dl; serum creatinine was supply to the peripheral vestibular labyrinth,
1.57 U/L; albumin was 4.5 g/L; SGOT was vestibular nerve, the vestibular nucleus in
18 U/L; SGPT was 16 U/L; CRP was 9.4; the brainstem and cerebellum originates
WBC was 13,200/l; Hb was 1 5.2 g/dl; from the vertebrobasilar artery system. (8,9)
platelets were 425,000/l. HbA1C levels 5.7 The internal auditory arteries branch is a
percent, lipid profile: cholesterol 245 mg/dl, branch of the AICA's Anterior Inferior
triglycerides 110 mg/dl, HDL 42 mg/dl, Cerebellar Artery, supplying the vestibular
LDL 89 mg/dl, electrolyte levels sodium and cochlear labyrinths. Branches of the
145 mmol/L, potassium 4.0 mmol/L, vertebral and basilar arteries supply the
chloride 103 mmol/L, HbA1C values 5.7 vestibular nuclei in the brainstem. (6,8) The
International Journal of Research and Review (ijrrjournal.com) 31
Vol.8; Issue: 9; September 2021Diayanti Tenti Lestari et.al. Acute vestibular syndrome in cerebellar infarction: a case report.
posterior and anterior cerebellar arteries Diyan et al, 2020 and Kim Ah, 2012,
provide blood supply to the inferior described the most common causes of
cerebellum and the flocculonodular lobe posterior circulation infarcts are posterior
which are parts of the cerebellum that are inferior cerebellar artery (PICA) and
closely related to the vestibular system. superior cerebellar artery (SCA) compared
(6,8) to the anterior inferior cerebellar artery
(AICA). Patients with cerebellar infarction
have clinical features of vertigo, nausea and
vomiting, horizontal nystagmus, limb
ataxia, unbalanced gait, and headache, may
be in the occipital, frontal, or upper cervical
region. Frequently, the clinical picture of
cerebellar artery infarction results from
infarction of the lateral medulla or pons, and
does not involve the cerebellum. These
clinical features include trigeminal and
spinothalamic sensory deficits or Horner's
syndrome. (5,6) The patient we reported
also presented with acute vertigo, head
discomfort, such as floating sensation
accompanied by a feeling of tumbling at the
acute onset and may lead to acute-onset
Figure 3: Magnetic Resonance Imaging MRI of right inferior limb ataxia and associated vascular risk
cerebellar infarction. Pathophysiological vascularization
illustration posterior inferior cerebellar artery (PICA) and
factors.
anterior inferior cerebellar artery (AICA). (8) Also mentioned by Hotson and
Baloh, 1998; The sudden onset of isolated
The pathophysiology of acute vertigo lasting for minutes in a person with
vestibular syndrome also occur through risk factors for stroke suggests an ischemic
involvement of the structures of the attack in the vertebrobasilar system or
vestibular nucleus, root entry zone of cranial transient ischemia of the vestibular
nerve VIII at the border of the pontomedula, labyrinth. Transient ischemic attacks often
dorsolateral or caudolateral rostral medulla, last for less than 30 minutes. Isolated
paramedian pons or mesencephalon transient vertigo may precede a stroke in a
tegmentum, and inferior cerebellar branch of the vertebrobasilar artery that
peduncle. (6) Cerebellar vestibular ocular presents with similar symptoms over a span
reflex (VOR) function and associated of weeks or months. (8) In acute vestibular
vestibular abnormalities. Purkinje Cell of syndrome, factors that lead to stroke should
vestibulocerebellum have an inhibitory be considered, such as; age over 60 years,
effect, usually in the ipsilateral vestibular history of hypertension or diabetes mellitus,
nucleus. Damage of these Purkinje cells accompanying symptoms refer to the central
tend to increase the tonic activity of nervous system, spontaneous and acute
ipsilateral vestibular nucleus, causing onset of symptoms for the first time. (11)
spontaneous cerebellar nystagmus on the Bed side examination of acute
lesion side. However, patients with floccular vestibular syndrome is important to
lesions exhibit much stronger spontaneous establish the diagnosis, even considered
nystagmus in response to abnormal head sensitive and specific for acute vestibular
impulses, suggesting that the flocculus has a syndrome, it’s hard to differentiate vascular
much more important role in controlling vertigo isolated from peripheral
VOR than does the cerebellar tonsil. (10) vestibulopati acute. As described by Kim JS
and Choi KD, 2013, indicates that bed side
International Journal of Research and Review (ijrrjournal.com) 32
Vol.8; Issue: 9; September 2021Diayanti Tenti Lestari et.al. Acute vestibular syndrome in cerebellar infarction: a case report.
examination of oculomotor has three steps postural instability that is severe enough to
for hints: Head impulse test, nystagmus and fall during a vertigo attack, the doctor can
Test of Skew Deviation consists of a head easily detect that the vertigo stems from
Impulse Test HIT, nystagmus, and the central vestibular dysfunction. (5) An
deviation of the eye is more sensitive to examination protocol that combines the
stroke while scheduling definitive imaging. Head Impulse test HIT with looking for
(1,2) nystagmus that changes direction in
If a patient shows any signs of eccentric gaze or skew deviation is 100%
central vestibular dysfunction such as sensitivity and 96% specificity for stroke
vertical nystagmus in usual position, identification, whereas diffusion weighted
nystagmus due to head shaking movements, DWI Magnetic Resonance Imaging MRI
asymmetric oculomotor dysfunction, or can be missed in 12% of cases. (5,12)
Table 1. Characteristics of the clinical presentation of acute unilateral vestibulopathy, stroke in the posterior inferior cerebellar
artery PICA and stroke in the anterior inferior cerebellar artery AICA (13)
Acute Unilateral Vestibulopathy Stroke (PICA) Stroke (AICA)
Nystagmus Spontaneous horizontal unidirectional Central form of Central form of nystagmus
nystagmus
Qualitative Head Impuls Test Abnormal to one side, fast phase Normal bilateral Abnormal on the side of the
nystagmus lesion
Quantitative Head impuls Test Ipsilateral;0.2-0.4 Ipsilateral;0.7-0.8 Ipsilateral;0.3-0.4
(gain) Contralateral: 0.6-1.0 Contralateral:0.7-0.8 Contralateral: 0.5-0.6
Skew deviation - There's a possibility There's a possibility
Vascular Risk Low Risk High Risk High Risk
Hearing disorders probability does not exist - Often there
HINTs examination is useful to 12 hours of the beginning of the event, the
reduce misdiagnosis of stroke or acute sensitivity of CT for ischemic stroke is just
vestibular syndrome and should be studied 39%. With a sensitivity of 99 percent,
in head-to-head for the comparative cost- Magnetic Resonance Imaging (MRI) with
effectiveness of the neuroimaging by MRI sequence Diffusion Weight Imaging (DWI)
DWI. (13) The research of Kattah et al, is significantly more accurate. Another
2009 and Choi et al, 2017 also proves that study discovered that the sensitivity of MRI
finding one of the 3 dangerous oculomotor is reduced in minor lesions, stroke at the
signs (normal Head Impulse Test HIT or ni fossa posterior region, and if the MRI is
horizontal stagmus that changes direction in conducted within 24 hours of the beginning
eccentric gaze or skew deviation) is more of symptoms rather than within 2 to 4 hours.
sensitive than the presence of other The DWI MRI procedure might be to blame
neurologic signs to identify if the acute for some of the decreased accuracy. (13)
vestibular syndrome is caused by stroke. However, a recent meta-analysis indicated
(14,15) The patient in this case report that, whereas only 6.8% of patients with
showed 2 out of 3 HINTS examination ischemic stroke had negative DWI MRI
results that lead to stroke, namely normal on findings, posterior circulation strokes had
the Head Impulse Test (HIT) and the this outcome five times more frequently.
presence of bidirectional horizontal Concurrent clinical evaluation and vascular
nystagmus, plus a deficit in the cerebellar imaging (CT or MR angiography to detect
system such as acute limb ataxia and the relevant occlusion or stenosis) may be
cerebellar signs, dysmetria. useful in determining a diagnosis. (9)
A computed tomography (CT) scan In most cases, only CT is performed,
of the head is routinely done in individuals although in fact MRI is a better method for
with acute vestibular dysfunction. CT is a visualizing pathology in the posterior
fairly reliable diagnostic for cerebral cranial fossa as demonstrated by the higher
bleeding; however, when conducted within diagnostic yield of MRI in this and other
International Journal of Research and Review (ijrrjournal.com) 33
Vol.8; Issue: 9; September 2021Diayanti Tenti Lestari et.al. Acute vestibular syndrome in cerebellar infarction: a case report.
studies. The use of CT as the only vestibular patients, isolated vascular vertigo
diagnostic investigation has several reasons, is not recommended for thrombolysis.
including; limited medical resources, Patients with an NIHSS score of more than
unreasonable fears or concerns of patients four were evaluated for intravenous
(false sense) and prevention of exposure to thrombolysis or urgent endovascular
ionizing radiation. It is important to be more surgery. In the case of acute vestibular
selective when selecting patients for syndrome, conservative therapy will be
neuroradiological treatment, and in larger effective. (16) Symptomatic therapy may be
cases MRI can be used instead of CT administered in the event of a labyrinth,
because of the higher sensitivity for cerebellum, or brainstem infarction.
posterior fossa pathology. (3) Ideally, Exercise-based vestibular therapy is
patients with acute dizziness require necessary as soon as feasible. There may be
imaging. MRI is preferred over CT scan in some improvement after therapy, but it is
the majority of cases. In certain cases, it is not usually complete. Patients with infarcts
important to exclude bleeding prior to should be closely monitored to minimize
thrombolysis or to detect vertebral artery brainstem compression caused by cerebellar
dissection using CT angiography. (4) The edema. (17) The patient in our case report
timing of MRI is also very important, got symptomatic therapy for vertigo and
because of the risk of false negatives in the dizziness in the form of Betahistine
first 48 hours. In some cases, it is necessary Hydrochloride 24 mg every 12 hours,
to perform a repeat MRI if the HINTS test however thrombolysis could not be done
results suggest a central process but the because it had been more than 4.5 hours
MRI results do not show any significance. from the beginning when the patient arrived
(4) Imaging performed on our patient was a at the neurology department.
head-CT scan, which was performed at the Prognosis for Acute vestibular
time the patient was admitted to the syndrome will improve with time and will
emergency department, 5 hours of onset and necessitate vestibular therapy. (13) Because
found a suspected cerebellar infarction of central structural damage, dizziness or
according to Fig. 1, then on the sixth day of vertigo might linger for months. Patients
treatment, the patient underwent MRI of the may also have discomfort in their heads or
Head and was found to have infarction in eyesight, which may seem unsteady, as well
the cerebellar region as per Fig. 2 with as spontaneous nystagmus and impairment
Magnetic Resonance Angiography (MRA) to the central vestibular and cerebellar
results within normal limits. These imaging circuits. (17)
results support the diagnosis of acute Antihistamines betahistine
vestibular syndrome in this patient. hydrochloride 24 mg every 12 hours for 14
The treatment of acute vestibular days, Acetyl Salicylic Acid 10 mg every 24
syndrome is based on treating acute stroke; hours, Amlodipine 10 mg every 24 hours
however, because this is linked with starting upon this fifth day after onset,
intravenous thrombolysis, it must be Simvastatin 20 mg every 24 hours were
modified to the time and severity of the prescribed to our patient as symptomatic
disease according to the National Institute of treatment. On the tenth day, the patient's
Health Stroke Scale (NIHSS) when the symptoms improved, and his vertigo was
patient arrives. (16) About 4% of patients significantly reduced by around 50-60%,
with dizziness or vertigo and clinical and his postural disturbances were reduced
symptoms indicative of a posterior as well, allowing him to walk more steadily.
circulation stroke arrive to the emergency The patient was then taught how to perform
room, but most have past the 4.5-hour time Cawthorne Cooksey vestibular therapy at
window for intravenous thrombolysis home.
therapy. If the score is low in acute
International Journal of Research and Review (ijrrjournal.com) 34
Vol.8; Issue: 9; September 2021Diayanti Tenti Lestari et.al. Acute vestibular syndrome in cerebellar infarction: a case report.
CONCLUSION 7. Volgger V, Gürkov R. Acute vestibular
Acute vestibular syndrome is closely syndrome in cerebellar stroke. HNO.
related to the posterior circulation and can 2017;65(07 march 2017):149–52.
be caused by cerebellar infarction. 8. John R. Hotson , M.D., And Robert W.
Pathophysiology according to cerebral Baloh MD. Acute Vestibular Syndrome. N
Engl J Med. 1998;volume 339:9–14.
blood circulation disorders that occur. 9. Banerjee G, Stone SP, Werring DJ.
Clinical features of patients with cerebellar Posterior circulation ischaemic stroke. BMJ.
lesions may include vertigo, nausea and 2018;361(April):1–7.
vomiting, horizontal nystagmus, limb ataxia 10. Kim SH, Park SH, Kim HJ, Kim JS.
or postural disturbances. The Bedside Isolated central vestibular syndrome. Ann N
HINTS oculomotor examination is sensitive Y Acad Sci. 2015;1343(1):80–9.
for acute vestibular stroke. Management 11. Strupp M, Dlugaiczyk J, Ertl-Wagner BB,
Pharmacological therapy in the form of Rujescu D, Westhofen M, Dieterich M.
symptomatic and non-pharmacological in Vestibular disorders: Diagnosis, new
the form of vestibular rehabilitation. classification and treatment. Dtsch Arztebl
Investigations can be followed by CT or Int. 2020;117(17):300–10.
12. Chen L, Lee W, Chambers BR, Dewey HM.
MRI of the head. The prognosis for acute Diagnostic accuracy of acute vestibular
vestibular syndrome is good. syndrome at the bedside in a stroke unit. J
Neurol. 2011;258(5):855–61.
Acknowledgement: None 13. Kerber KA. Acute Vestibular Syndrome.
Semin Neurol. 2020;40(1):059–66.
Conflict of Interest: None 14. Kattah JC, Talkad A V., Wang DZ, Hsieh
YH, Newman-Toker DE. HINTS to
Source of Funding: None diagnose stroke in the acute vestibular
syndrome: Three-step bedside oculomotor
REFERENCES examination more sensitive than early MRI
1. Kim SH, Kim HJ, Kim JS. Isolated diffusion-weighted imaging. Stroke.
vestibular syndromes due to brainstem and 2009;40(11):3504–10.
cerebellar lesions. J Neurol. 2017;264:63–9. 15. Choi JY, Lee SH, Kim JS. Central vertigo.
2. Choi KD, Lee H, Kim JS. Vertigo in Curr Opin Neurol. 2018;31(1):81–9.
brainstem and cerebellar strokes. Curr Opin 16. Machner B, Choi JH, Neumann A,
Neurol. 2013;26(1):90–5. Trillenberg P, Helmchen C. What guides
3. Ljunggren M, Persson J, Salzer J. Dizziness decision-making on intravenous
and the Acute Vestibular Syndrome at the thrombolysis in acute vestibular syndrome
Emergency Department: A Population- and suspected ischemic stroke in the
Based Descriptive Study. Eur Neurol. posterior circulation? J Neurol [Internet].
2018;79(1–2):5–12. 2020;(0123456789). Available from:
4. Putra IBK, Adrian F. Dizziness dan Vertigo https://doi.org/10.1007/s00415-020-10134-9
Dengan Keterkaitan Sistem Vertebrobasiler. 17. Sri Sutarni,Rusdy Gazali Malueka AG.
Callosum Neurol. 2019;2(1):19–27. Bunga Rampai Vertigo. In: Wibowo S,
5. Kim HA, Lee H. Recent advances in central editor. Yogyakarta: ugmpres.ugm.ac.id;
acute vestibular syndrome of a vascular 2018. p. 73–88.
cause. J Neurol Sci [Internet]. 2012;321(1–
2):17–22. Available from: How to cite this article: Lestari DT, Hidayati
http://dx.doi.org/10.1016/j.jns.2012.07.055 HB. Acute vestibular syndrome in cerebellar
6. Diyan Anita Sari, Sri Sutarni IS. Stroke infarction: a case report. International Journal
Iskemik Dengan Manifestasi of Research and Review. 2021; 8(9): 29-35.
Dizziness/Vertigo Terisolasi. Neurona. DOI: https://doi.org/10.52403/ijrr.20210906
2020;volume 37(2 Maret 2020):3–9.
******
International Journal of Research and Review (ijrrjournal.com) 35
Vol.8; Issue: 9; September 2021You can also read