ABO Genotype, "Blood-Type" Diet and Cardiometabolic Risk Factors
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ABO Genotype, “Blood-Type” Diet and Cardiometabolic
Risk Factors
by
Jingzhou Wang
A thesis submitted in conformity with the requirements
for the degree of Master of Science (M.Sc.)
Graduate Department of Nutritional Sciences
University of Toronto
© Copyright by Jingzhou Wang 2014ABO Genotype, “Blood-Type” Diet and Cardiometabolic
Risk Factors
Jingzhou Wang
Master of Science
Graduate Department of Nutritional Sciences
University of Toronto
2014
Abstract
The ‘Blood-Type’ diet advises individuals to eat according to their ABO blood group to optimize
health without the support of science evidence. The objective of this study was to determine
whether consumption of a diet in accordance with an individual’s ABO genotype is associated
with various biomarkers of cardiometabolic health. Study subjects (n=1,455) were participants of
the Toronto Nutrigenomics and Health study. Dietary intake was assessed using a one-month,
196-item food frequency questionnaire and a diet score was calculated to determine relative
adherence to each of the four blood type diets. ABO blood group was determined by genotyping
rs8176719 and rs8176746 in the ABO gene. The results show that adherence to the Type-A,
Type-AB, and Type-O diets were associated with favourable profile of certain cardiometabolic
risk factors (PAcknowledgments
I would not have reached this stage without the help of others. Here, I want to express my
sincere gratitude to the people who made my life in the department truly enjoyable.
First of all, I want to thank my supervisor, Dr. Ahmed El-Sohemy for his excellent
support throughout my Master’s training. His passion in the field of nutrigenomics attracts me to
pursue this graduate degree and his brilliant ideas allow me to work on an interesting project.
With his approachability and patience, I was able to learn and improve my thinking, writing,
speaking skills significantly. His generosity and flexibility has also enabled me to discover career
opportunities and to develop my soft skills in other settings. It was truly my honour to be a
student for Ahmed. I am very grateful for all the opportunities and knowledge he has offered. I
cannot imagine a better mentor.
Second, I would like to thank Dr. Richard Bazinet and Dr. Elena Comelli for offering
wonderful support as my committee members. Their critical feedback and constructive advice
have helped me to further develop my critical thinking and to mature as a graduate student. It was
also a privilege to have two of my most admiring undergraduate professors to serve on my
advisory committee. I have also benefited tremendously from the teaching of Dr. Paul Corey and
Dr. Tony Hanley. Their high levels of expertise in statistics and epidemiology have helped me
build a solid foundation in my research project. I also want to specifically thank Dr. Harvey
Anderson, who has played a significant role in my undergraduate training. Without his guidance,
I would not fall in love with research. His consistent support, even after I leave the lab, has been
invaluable.
Third, I want to thank all the past and present members in the El-Sohemy team. The thesis
would not be completed in a timely manner without the effort of all past students. I am also very
iiigrateful to receive the support from Bibiana Garcia-Bailo, Daiva Nielsen, Ouxi Tian, Andre Dias,
Nanci Guest and Joseph Jamnik in both academic and social circumferences. The quality of my
research project improved significantly thanks to their input. It was a pleasure to be a part of the
big family.
Fourth, I would like to thank all the staff members and students in the department. Louisa
Kung and Emeliana D'Souza were always there to give an extra hand. Clara Cho and Diana
Sanchez-Hernandez were my first mentors in the research field and have taught me a significant
amount of knowledge and skills that are useful in my future career. I am also equally grateful for
the experiences and encouragement offered by my colleagues and teammates in the departmental
student union and volleyball team. The assistances of all these fellows have no doubt facilitated
the completion of my research project.
I also gratefully acknowledge the funding sources that made this thesis possible: the
Ontario Graduate Scholarship program and the Advanced Foods and Materials Network. In addition,
I was fortunate to be able to attend an international conference thanks to the generous support from
Dr. Ahmed El-Sohemy and School of Graduate Studies at University of Toronto.
My last gratitude goes to my family. My parents have offered invaluable guidance in my
entire life. Without the support of my father, Song Wang, I would not have had the opportunity to
study aboard. I want to specifically thank for my mother, Yu Liu, who passed away from liver
cancer when I was 15 years old. Watching Animal Planet with my mother made me fall in love
with biology when I was young; losing my closest person due to cancer led me to pursue a career
in life sciences. To her I dedicate this thesis.
Thank you all!
iv“In a group of three people, there is always something I can learn from. Choose to follow the
strengths of others, use the shortcomings to reflect upon ourselves."
Confucious, 500 BC
vTable
of
Contents
TABLE
OF
CONTENTS
VI
LIST
OF
TABLES
IX
LIST
OF
FIGURES
X
LIST
OF
APPENDIX
XI
Chapter
1:
Introduction
and
Literature
Review
1.1
INTRODUCTION
1
1.2
“BLOOD-‐TYPE”
DIET
1
1.3
ABO
BLOOD
GROUP
2
1.3.1
ABO
SYSTEM
2
1.3.2
ABO
BLOOD
GROUP
AND
DISEASES
3
1.3.3
BLOOD
GROUPS
AND
NUTRITION
4
1.4
CARDIOMETABOLIC
DISEASES
6
1.4.1
PREVALENCE
AND
ETIOLOGY
6
1.4.2
BIOMARKERS
OF
RISK
6
1.4.3
RISK
FACTORS
9
1.5
SUMMARY
AND
RATIONALE
10
1.6
HYPOTHESIS
AND
ORGANIZATION
OF
THESIS
11
Chapter
2:
Effect
of
ABO
Genotype
on
Cardiometabolic
Risk
Factors
2.1
ABSTRACT
12
2.2
INTRODUCTION
13
2.3
METHODS
14
vi2.3.1
STUDY
DESIGN
AND
PARTICIPANTS
14
2.3.2
ABO
GENOTYP
IDENTIFICATION
14
2.3.3
CARDIOMETABOLIC
RISK
FACTOR
ASSESSMENT
15
2.3.4
STATISTICAL
ANALYSIS
16
2.4
RESULTS
16
2.5
DISCUSSION
22
Chapter
3:
Effect
of
"Blood-‐Type"
Diet
on
Cardiometablic
Risk
Factors
3.1
ABSTRACT
23
3.2
INTRODUCTION
24
3.3
MATERIAL
AND
METHODS
27
3.3.1
STUDY
DESIGN
AND
PARTICIPANTS
27
3.3.2
DIETARY
ADHERENCE
SCORE
ASSESSMENT
27
3.3.3
CARDIOMETABOLIC
RISK
FACTOR
ASSESSMENT
28
3.3.4
STATISTICAL
ANALYSIS
28
3.4
RESULTS
29
3.5
DISCUSSION
38
Chapter
4:
Effect
of
matching
ABO
genotype
to
"Blood-‐Type"
Diet
on
Cardiometabolic
Risk
Factors
4.1
ABSTRACT
41
4.2
INTRODUCTION
42
4.3
MATERIAL
AND
METHODS
42
4.3.1
STUDY
DESIGN
AND
PARTICIPANTS
42
4.3.2
ABO
GENOTYPE
IDENTIFICATION
43
vii4.3.3
DIETARY
ADHERENCE
SCORE
ASSESSMENT
43
4.3.4
CARDIOMETABOLIC
RISK
FACTOR
ASSESSMENT
43
4.3.5
STATISTICAL
ANALYSIS
43
4.4
RESULTS
44
4.5
DISCUSSION
54
Chapter
5:
Overview
and
General
Discussion
5.1
OVERVIEW
56
5.2
LIMITATIONS
58
5.3
FUTURE
DIRECTIONS
60
5.4
IMPLICATION
61
REFERENCE
62
APPENDIX
70
viiiList of Tables
TABLE
2-‐1:
SUBJECT
CHARACTERISTICS
BY
ABO
GENOTYPE
19
TABLE
3-‐1A:
THE
"TYPE-‐A
"
DIET
CHARACTERISTICS
34
TABLE
3-‐1B:
CARDIOMETABOLIC
RISK
FACTORS
BY
TERTILES
OF
“TYPE-‐A”
DIET
SCORE
34
TABLE
3-‐2A:
THE
"TYPE-‐AB"
DIET
CHARACTERISTICS
35
TABLE
3-‐2B:
CARDIOMETABOLIC
RISK
FACTORS
BY
TERTILES
OF
“TYPE-‐AB”
DIET
SCORES
35
TABLE
3-‐3A:
THE
"TYPE-‐B"
DIET
CHARACTERISTICS
36
TABLE
3-‐3B:
CARDIOMETABOLIC
RISK
FACTORS
BY
TERTILES
OF
"TYPE-‐B"
DIET
SCORES
36
TABLE
3-‐4A:
THE
"TYPE-‐O"
DIET
CHARACTERISTICS
37
TABLE
3-‐4B:
CARDIOMETABOLIC
RISK
FACTORS
BY
TERTILES
OF
"TYPE-‐O"
DIET
SCORES
37
TABLE
4A:
CARDIOMETABOLIC
RISK
FACTORS
BY
"TYPE-‐A"
DIET
SCORES
AND
ABO
GENOTYPE
47
TABLE
4B:
CARDIOMETABOLIC
RISK
FACTORS
BY
"TYPE-‐AB"
DIET
SCORES
AND
ABO
GENOTYPE
50
TABLE
4C:
CARDIOMETABOLIC
RISK
FACTORS
BY
"TYPE-‐B"
DIET
SCORES
AND
ABO
GENOTYPE
52
TABLE
4D:
CARDIOMETABOLIC
RISK
FACTORS
BY
"TYPE-‐O"
DIET
SCORES
AND
ABO
GENOTYPE
53
ixList of Figures
FIGURE
2-‐1:
ABO
BLOOD
TYPE
ASSESSMENT
BY
GENOTYPING
SINGLE
NUCLEOTIDE
POLYMORPHISMS
15
FIGURE
2-‐2:
ABO
BLOOD
GROUP
DISTRIBUTION
IN
THE
ENTIRE
TNH
COHORT
(A)
AND
BY
ETHNOCULTURAL
GROUPS
(B)
17
FIGURE
2-‐3:
LEVELS
OF
FASTING
GLUCOSE
IN
INDIVIDUALS
WITH
DIFFERENT
ABO
BLOOD
GROUPS
20
FIGURE
2-‐4:
LEVELS
OF
FASTING
INSULIN
IN
INDIVIDUALS
WITH
DIFFERENT
ABO
BLOOD
GROUPS
21
FIGURE
3-‐1:
TOTAL
NUMBER
OF
RECOMMENDED
ITEMS
TO
EAT
(A)
OR
AVOID
(B)
IN
FOUR
MAJOR
FOOD
GROUPS
LISTEDIN
THE
FFQ
FOR
EACH
"BLOOD-‐TYPE"
DIET
30
FIGURE
3-‐2:
DIET
SCORE
DISTRIBUTION
FOR
EACH
"BLOOD
TYPE”
DIET
31
FIGURE
4-‐1:
NUMBER
OF
INDIVIDUALS
WITH
MATCHED
AND
UNMATCHED
BLOOD
GROUPS
ACROSS
THE
TERTILE
TERTILE
OF
EACH
“BLOOD-‐TYPE”
DIET
SCORE
45
FIGURE
4-‐2:
THE
ASSOCIATION
BETWEEN
TERTILES
OF
“TYPE-‐A”
DIET
SCORES
AND
FASTING
INSULIN
IN
SUBJECTS
WITH
BLOOD
TYPE
A
AND
THE
OTHERS
48
FIGURE
4-‐3:
THE
ASSOCIATION
BETWEEN
TERTILES
OF
“TYPE-‐A”
DIET
SCORES
AND
FASTING
GLUCOSE
IN
SUBJECTS
WITH
BLOOD
TYPE
A
AND
THE
OTHERS
49
FIGURE
4-‐4:
THE
ASSOCIATION
BETWEEN
TERTILES
OF
“TYPE-‐AB”
DIET
SCORES
AND
FASTING
GLUCOSE
IN
SUBJECTS
WITH
BLOOD
TYPE
A
AND
THE
OTHERS
51
xList of Appendix
TABLE:
FOOD
ITEMS
INCLUDED
IN
THE
"BLOOD-‐TYPE"
DIET
SCORE
CALCULATION
65
xiChapter 1: Introduction and Literature Review
1.1 Introduction
The “Blood-Type” diet is a set of nutritional guidelines that advocate people to eat
according to their blood group. Although popular with the public, the diet remains controversial
because no scientific research has examined its validity. The proposed study will be the first
observational study to investigate whether consumption of a diet in accordance with one's blood
group is associated with favourable health outcomes.
1.2 “Blood-Type” Diet
The connection between blood group and diet was first suggested by P.J. D’Adamo, a
naturopathic physician, in his book “Eat Right For Your Type” published in 1996 [1]. The
“Blood-Type” diet theory has thereafter gained widespread attention from the public. With more
than 7 million copies sold in over 60 languages, this book was a New York Times bestseller [2].
Based on his perceptions of the blood group evolution and the action of lectins, D’Adamo
postulates that the ABO blood group reveals the dietary habits of our ancestors and people with
different blood groups process food differently; thus, adherence to a diet specific to one’s blood
group could improve health and decrease risk of chronic diseases such as cardiovascular disease.
Based on the “Blood-Type” diet theory, group O is considered the ancestral blood group in
humans, so their optimal diet should resemble the high animal protein diets typical of the hunter-
gatherer era. In contrast, those with group A should thrive on a vegetarian diet as this blood
12
group was believed to have evolved when humans settled down into agrarian societies. Following
the same rationale, individuals with blood group B are considered to benefit from consumption of
dairy products because this blood group was believed to originate in nomadic tribes. Finally,
individuals with an AB blood group are believed to benefit from a diet that is intermediate to
those proposed for group A and group B. The “Blood-Type” diet also proposes that lectins,
which are sugar-binding proteins found in certain foods [3], could cause agglutination if they are
not compatible with an individual’s ABO blood group. However, there has been no scientific
research conducted to either support his explanations or validate the “Blood-Type” diet, making
this popular theory controversial.
1.3 ABO Blood Group
1.3.1 ABO System
Although little is known about the effectiveness of the “Blood-Type” diet, the ABO blood
group itself is well understood. A blood group is a classification of blood based on the presence
or absence of surface antigenic substance on red blood cells. Depending on the blood group
system, these antigens can be proteins, carbohydrates, glycoproteins or glycolipids. To date, 30
human blood groups are recognized by the International Society of Blood Transfusion [4].
Among them, the ABO blood group is the most important one in transfusion medicine and has
been studied extensively. Group O, A, B, and AB are the four subgroups within the ABO system,
which is estimated to account for 44%, 35%, 16% and 5% of global population, respectively [5].
The distinction of ABO blood group relies on the structural variation of a carbohydrate antigenic
substance, called H-antigen, found on red blood cells. Such variation is a result of different
23
enzymatic activities determined by the alleles of the ABO gene locus. Specifically, the IA allele
encodes a glycosyltransferase that attaches α-N-acetylgalactosamine to H-antigen, producing the
A antigen. The IB allele encodes a glycosyltransferase that bonds α-D-galactose to the H antigen,
creating the B antigen. In contrast, the i allele does not produce any functional enzyme due to a
frameshift mutation that results in premature termination of the translation, so H antigen remains
intact in this case [6]. Because the IA and IB alleles are co-dominant to each other and both are
dominant over allele i, different combinations of IA, IB and i can produce different ABH antigens
on human red blood cells. For example, people with blood group AB will have genotype IAIB,
whereas those with blood group A can have either IAIA or IAi [7]. The discovery of the ABO
blood group not only was a major breakthrough in transfusion medicine, but also draws attention
to the potential importance of blood group in health and disease risk management.
1.3.2 ABO Blood Group and Diseases
As one of the first recognizable genetic variants in humans, the ABO system has been
studied for its association with a variety of diseases, including cardiometabolic syndromes,
cancer and microorganism infections. As for cardiometabolic diseases, research has shown that
people with group O on average had 25% lower level of von Willebrand factor (VWF), which is
a critical protein involved in haemostasis [8]. Considering the fact that higher VWF levels could
increase the risk of ischemic stroke [9], a lower expression of VWF may explain the observation
that people with blood group O had a reduced risk of venous thromboembolism [10]. Although
blood group O demonstrates some degree of protection against thrombosis, it may increase the
risk of diabetes. One study has shown that blood group B was associated with a decreased risk of
type 2 diabetes compared to blood group O (OR = 0.44, 0.27-0.70) [11], suggesting that the
association between ABO blood group and cardiometabolic diseases is disease-specific.
34
Regarding its association with cancers, people with blood group O may have lower risks of
pancreatic cancer [12] and gastric cancer [13], but a higher risk of non-melanoma skin cancer
[14]. Gates et al. have also found that the presence of the B antigen on the red blood cells was
positively associated with ovarian cancer incidence [15]. Thus, certain ABO groups may be
associated with different risks in different types of cancers. Besides its associations with
cardiometabolic diseases and cancers, the ABO blood group may also alter the incidences of
malaria and cholera. In a matched case-control study of 567 Malian children, Rowe et al. found
that group O was correlated with a 66% reduction in the odds of developing severe malaria
compared to the non-O blood groups. The difference in group O may be caused by the inhibition
of Plasmodium falciparum resetting, which is a parasite virulence phenotype associated with
severe malaria [16]. As for cholera, an observational study in Bangladesh found that both the
incidence and severity of diarrhea were higher in group O, but lower in group AB [17]. Overall,
the existing research suggests that ABO blood type may play a role in modifying an individual’s
susceptibility to certain diseases.
1.3.3 Blood Groups and Nutrition
To date, research on the association between blood groups and nutrition is limited.
Nonetheless, the results from several published studies have suggested that blood groups might
indeed alter the relationship between diet and physiological outcomes to some extent. For
example, in a study on high-fat diet and intestinal phosphatase published in 1960s, Langman et
al. found that people with group A not only had the lowest level of enzyme activity at baseline,
but also had lowest increase of activity after giving a high-fat diet.[18] Because phosphatase
negatively regulates fat absorption in the gut [19], a lower enzyme activity may explain why
people with blood group A had higher levels of serum cholesterol in another study [20]. Although
45
the findings suggested that ABO blood group might alter a metabolic pathway related to nutrient
absorption, the interpretation of the results is limited because no statistical analysis was
performed in these two early studies. In addition to the potential to influence nutrient absorption,
a Finnish group has demonstrated that ABO blood group might have an impact on the human gut
microbiota composition. Compared to individuals with the B antigen (blood group B and AB),
people with non-B antigens were shown to have lower diversity of the Eubacterium rectale-
Clostridium coccoides (EREC) and Clostridium leptum (CLEPT) –groups [21]. The linkage
between ABO blood group and microbiota has been further substantiated in recent studies. For
example, both Helicobacter pylori [22] and Lactobacillus spp. [23] have been shown to use ABO
antigens as adhesion receptors. Furthermore, research has shown that different species may have
different binding affinities to ABH antigen [23] and host ABO genotype can affect the enzyme
secretion and metabolism of gut microbiota [24]. Considering the role of gut microbiota on
nutrient breakdown and absorption [25], the results of these studies further imply that ABO blood
group could be a genetic host factor that modulates the relationship between diet and health.
Besides the ABO system, research on another glycoprotein-based blood group system, known as
MNS, has found that individuals with blood group NN tended to have a greater reduction in low
density lipoprotein (LDL) cholesterol in response to a low-fat diet compared to individuals with
MN and MM blood groups. [26] However, because ABO and MNS blood group systems are
functionally distinct, the generalization of the MNS finding on the current project is limited.
Overall, several studies have suggested that a potential interaction may exist among blood
groups, diet and health. However, the evidence, particularly for the ABO system, remains scarce.
56
1.4 Cardiometabolic Diseases
1.4.1 Prevalence and Etiology
Cardiometabolic diseases, including Type 2 diabetes (T2D) and cardiovascular diseases
(CVD), are the leading causes of mortality and morbidity globally [27]. Patients with this type of
disease usually exhibit hypertension, hyperglycemia, dyslipidemia, inflammation and obesity
[28]. In Canada, over 3 million and 1.3 million of people suffer from T2D and CVD respectively
[29,30]. As a huge burden on the health care system, T2D is expected to cost the Canadian
healthcare system $16.9 billion a year by 2020 [31], and CVD alone costs Canadian more than
20.9 billion each year [29].
The development of cardiometabolic diseases commonly involves excess accumulation of
body fat and insulin resistance in adipose, hepatic and muscle tissues [32]. Visceral and central
adiposity are known to increase the level of free fatty acids in the circulation [33,34]. High levels
of free fatty acids can cause hepatic gluconeogenesis and lead to excess secretion of glucose,
triglycerides and very low-density lipoprotein (VLDL). This process is usually accompanied by a
reduction in high-density lipoprotein (HDL) cholesterol secretion and elevation of low-density
lipoprotein (LDL) cholesterol. Eventually, these physiological states lead to dysglycemia and
dyslipidemia, which are early signs of cardiometabolic disorders [35].
1.4.2 Biomarkers of risk
In order to prevent and manage T2D and CVD, a number of serum biomarkers along with
the anthropometric measurements are usually monitored during clinical visits to indicate the risk
of these two common diseases. These biomarkers are usually associated with glucose and fat
metabolism that are important in the disease pathology. Regarding glucose metabolism, insulin
67
regulates the cellular uptake of glucose from blood when its level is high after a meal, and
glucagon promotes gluconeogenesis and glycogenolysis in the liver when the level of glucose is
low [36]. In patients with insulin resistance, higher levels of insulin are required to maintain glucose
uptake in peripheral tissues [37]. Pancreatic β-cells produce and secrete more insulin in response,
resulting in the individual becoming hyperinsulinemic [38]. This process continues until β-cells
cannot meet the increased need of insulin secretion, which results in elevation of blood glucose
[39,40]. Therefore, high levels of glucose and insulin are strong predictors of the development of
T2D [36]. A number of approaches have been developed to monitor and indicate insulin resistance
and β-cell dysfunction. In epidemiologic studies, the homeostasis model assessment of insulin
resistance (HOMA-IR) and β-cell dysfunction (HOMA-Beta) is a method commonly used to
indicate the function of glycemic regulation. HOMA is based on the levels of fasting insulin and
glucose, which are indicators of the balance between insulin secretion and glucose maintenance in the
liver [41]. The equation of calculating HOMA is shown below.
HOMA-IR = (fasting plasma insulin x fasting plasma glucose) / 22.5
HOMA-Beta = (20 x fasting plasma insulin) / (fasting plasma glucose - 3.5), where insulin is
measured in mU/L and glucose is measured in mmol/L [42].
Results from the HOMA method have been proven to correlate well (r>0.7) with the traditional
hyperglycemic clamp method [43,44].
As for biomarkers of cardiometabolic diseases in lipid metabolism, high levels of serum
cholesterol and triglycerides are common indicators of dysregulation in lipid metabolism, which
is a main feature of cardiometabolic diseases. Although serum total cholesterol level is associated
with cardiometabolic risk, the lipoprotein carriers of cholesterol actually play a larger role in the
pathologic process [45]. Lipoprotein particles consist of triglycerides, cholesterol, phospholipids
78
and apolipoproteins. Based on the composition of apolipoproteins and the relative density of
triglycerides and cholesterol, lipoprotein particles can be classified into several categories [45].
Low-density lipoprotein (LDL) and high-density lipoprotein (HDL) are the two that are highly
related to cardiometabolic risk. The main role of LDL is to transport triglycerides and cholesterol
to tissues, whereas HDL is involved in returning cholesterol back to liver for excretion [46].
Elevated levels of LDL coupled with reduced levels of HDL are known to promote the formation
of atherosclerotic plaques and thus the development of the CVD [45,46]. The atherosclerotic
process begins when high amounts of LDL enter the vascular endothelium and become oxidized,
which attracts macrophages that engulf the extra lipids and form foam cells. Meanwhile, the
activated macrophages release high levels of pro-inflammatory cytokines, such as IL-6. This
attracts platelets to attach to the site of injury and promotes the proliferation of smooth muscle
cells. The process is also accompanied by an elevation of C-reactive protein (CRP) secretion,
which plays a critical role in the phagocytosis by macrophages [47]. As a well-established
biomarker of inflammation, CRP has been consistently associated with T2D and CVD [48].
Compared to healthy individuals, people with cardiometabolic diseases tend to have levels of
CRP that are two- to four-fold higher [48]. The effects of CRP and other pro-inflammatory
cytokines all perpetuate the accumulation of foam cells and smooth muscle cells at the plaque. As
a result, blood vessel narrows down and blood flow is diminished, which can lead to stroke and
myocardial infarction [46]. In contrast, high levels of HDL can inhibit the deposition of
cholesterol and prevent the formation of atherosclerotic plaques by transporting triglycerides and
cholesterol back to the liver [49]. In addition to LDL and HDL, serum triglyceride (TG)
concentration is another biomarker that strongly correlates with cardiometabolic diseases [50,51].
High levels of TG are known to both impede the scavenging capacity of HDL [52,53] and
promote the formation of small, dense LDL particles, which are more easily oxidized and thus
89
more atherogenic than their normal-sized counterpart [54]. In summary, the levels of biomarkers
involved in glucose and fat metabolism all play critical roles in the pathologic process of
cardiometabolic diseases and thus are often used as surrogate indicators during disease screening
[55,56].
1.4.3 Risk Factors
Sex, age, family history, ethnicity are all known to alter the risk of cardiometabolic
diseases [32,57]. For example, South Asian individuals have a higher prevalence of CVD in
Canada compared to Caucasian or East Asian [57]. In addition to these demographic factors,
smoking, exercise and diet represent other risk factors that can be modified through lifestyle
habits [58,59]. As one of the most important modifiable risk factors, diet has been consistently
shown to alter the risk of cardiometabolic diseases. Regarding specific nutrients, consumption of
foods rich in dietary fiber [60,61], magnesium [62,63], and vitamin D [64,65], may be beneficial
in preventing the development of T2D and CVD. In contrast, diets with a high intake of dietary
cholesterol and high ratio of saturated /polyunsaturated fat can increase the risk of both T2D and
CVD [66,67,68]. As for general dietary patterns, diets high in fruit and vegetable intakes are
known to significantly reduce cardiometabolic disease risk. For example, in a recent landmark
study. the Mediterranean diet, which is characterised by a high intake of olive oil, nuts, fruits and
vegetables, a moderate intake of fish and poultry, and a low intake of dairy and red meat, has
been shown to substantially reduce the incidence of major cardiovascular events by 30% [69].
Overall, research suggests that a healthy diet is a significant modifiable lifestyle factor in the
prevention and management of cardiometabolic diseases.
910
1.5 Summary and Rationale
In summary, both ABO blood group and dietary habits have been shown to alter the risk
of cardiometabolic diseases in previous research. The associations of these diseases with diet, as
well as with blood group, may imply that a potential interaction exists between diet and blood
group on subsequent cardiometabolic disease risk. Considering the popularity of the “Blood-
Type” diet and its lack of scientific evidence, it will thus be worthwhile to investigate whether
the effects of dietary intake on diseases are dependent on an individual’s blood group. The results
of this research has the potential to either substantiate or reject the health claims of the “Blood-
Type” diet, so that evidence-based recommendations can be made by health professionals in the
future.
1011
1.6 Hypothesis and Organization of Thesis
Hypothesis
Adherence to a diet specific to one's blood group is associated with a reduced disease risk profile.
Objectives
1. To determine the effect of ABO genotype on cardiometabolic risk factors.
2. To determine the effect of “Blood-Type” diet on cardiometabolic risk factors.
3. To determine the effect of matching ABO genotype and “Blood-Type” diet on
cardiometabolic biomarkers.
11Chapter 2: Effect of ABO Genotype on Cardiometabolic Risk
Factors
2.1 Abstract
Background: Previous research has suggested that ABO blood group is associated with a variety
of chronic diseases, such as cancer, thrombosis and Type 2 diabetes. However, the results on
some of these linkages, such as the one with T2D risk, have largely remained inconsistent and
inconclusive. The objective of this chapter is to examine the relationship between ABO blood
group and cardiometabolic risk factors, which can further elucidate some of these linkages from a
biomarker perspective.
Methods: Subjects (n=1,455) were participants of the Toronto Nutrigenomics and Health study.
ABO blood group was determined by genotyping rs8176719 and rs8176746 in the ABO gene.
Overnight 12-hour fasting blood samples were collected to measure serum cardiometabolic
biomarkers by high performance liquid chromatography. ANCOVA, with age, sex, ethnicity, and
energy intake as covariates, was used to compare anthropometric measurements and biomarkers
of cardiometabolic health across different blood groups
Results: Subjects with blood group O had lower levels of serum insulin, HOMA-IR, and
HOMA-Beta compared to blood groups A and B (p13
2.2 Introduction
The “Blood-Type” diet advises people to eat based on their blood group to optimize
health outcome. For each blood group, the recommended diet represents as a distinct dietary
pattern. For example, the Type-A diet is similar to a vegetarian diet, whereas the Type-O diet
resembles the low-carbohydrate diet that has high animal protein intake. Before examining
whether people with certain blood group may benefit more from following the corresponding
“Blood-Type” diet, it is critical to investigate the effect of different ABO genotypes on
cardiometabolic risk factors.
As a well-known genetic variant among individuals, ABO blood group is not only
critical in blood transfusion, but may also alter the risk of a variety of diseases, including
cardiometabolic syndromes, cancers and microorganism infections [11,13,17]. Regarding
cardiometabolic diseases, research has shown that people with group O may have a reduced risk
of venous thromboembolism due to their lower level of von Willebrand factor [8], which is a
critical protein involved in blood clotting [10]. Although blood group O may confer some degree
of protection against thrombosis, it may increase the risk of diabetes. By using the data from the
Nurses’ Health Study, Qi et al. have shown that ABO blood group is not only associated with the
serum level of E-Selectin, a well-known risk factor for T2D, but also found that blood group O
was associated with an increased risk of Type 2 diabetes compared to blood group B [11].
However, the results on the some of these linkages, such as the one with T2D risk, have remained
inconsistent. For example, the higher risk of T2D in people with blood group O was reported in
two studies [11,70], but not replicated in others [71,72,73]. In order to address this
inconsistency, this study intends to elucidate the linkage between ABO blood group and
cardiometabolic disease risk in a young multiethnic population. This would allow us to further
1314
investigate the etiological relationship upstream before disease onset and to study the role of
ethnicity in the linkage between ABO blood group and cardiometabolic serum biomarkers.
2.3 Material and Methods
2.3.1 Study Design and Participants
Subjects (n=1,639) were participants of the Toronto Nutrigenomics and Health (TNH)
Study, which is a cross-sectional examination of young adults aged 20 to 29 years. All subjects
were recruited between October 2004 and December 2010 and completed a general health and
lifestyle questionnaire, which included information on age, sex, ethnocultural group and other
subject characteristics. Subjects who were likely under-reporters (less than 800 kcal per day) or
over-reporters (more than 3,500 kcal per day for females or 4,500 kilocalories per day for males)
of energy intake were excluded from the analyses. Subjects were also excluded if they had
missing data for any of the biomarkers of interest or ABO genotype (n=184). After exclusions,
1,455 subjects (993 women and 462 men) remained. Individuals were categorized into four major
ethnocultural groups: White (n=703), East Asians (n=491), South Asians (n=155), and others
(n=106).
2.3.3 ABO Genotype Identification
The Sequenom MassArray® multiplex method was used to determine the blood group of
study participants by genotyping two single nucleotide polymorphisms (SNPs)
(rs8176719Del>G; rs8176746A>C) in the ABO gene. The rs8176719 SNP indicates O-allele-
specific 261delG while rs8176746 determines the galactose specificity of the encoded A/B
1415
transferases and thus the expression of A and B alleles [7]. Previous studies have taken
advantages of the genetic information to infer blood type from single nucleotide polymorphism
(SNP), which can be more accurate and efficient compared to the traditional blood typing that is
based on antibody assay [11,74]. Figure 2.1 depicts the exact relationship between these SNPs
and ABO blood type assessment.
Figure 2-1: ABO blood group assessment by genotyping SNPs.
2.3.3 Cardiometabolic Risk Factor Assessment
Anthropometric measurements including height, weight, blood pressure and waist
circumference were determined as previously described [75]. Body mass index (BMI; kg/m2) was
calculated and physical activity was measured by questionnaire and expressed as metabolic
equivalent (MET)-hours per week, as described previously [75,76]. Overnight 12-hour fasting
blood samples were collected to measure serum biomarkers of cardiometabolic disease, including
triglycerides, free fatty acids, C-reactive protein, fasting glucose, fasting insulin, and total-, HDL-
and LDL-cholesterol, as described previously [77]. After converting insulin concentrations from
pmol/L to IU/mL, the homeostasis model of insulin resistance (HOMA-IR) was calculated by
1516
using the formula: (insulin * glucose)/22.5, and the homeostasis model of beta-cell function
(HOMA-Beta) was calculated by using the formula: (20 * insulin)/(glucose - 3.5).
2.3.5 Statistical Analysis
Statistical analyses were performed using the Statistical Analysis Systems (SAS)
Software program (version 9.2; SAS Institute Inc., Cary, North Carolina). The a error was set at
0.05 and reported p-values are 2-sided. Subject characteristics were compared across different
ABO blood groups by using chi-square tests for categorical variables and analysis of variance
(ANOVA) for continuous variables. Analysis of covariance (ANCOVA) was used to compare
means of cardiometabolic biomarkers among different ABO blood groups. Variables that were
not normally distributed were either loge or square root transformed prior to analysis, but the
mean values and standard errors are displayed without transformation to facilitate interpretation.
Means compared between groups were adjusted for multiple comparisons using the Tukey-
Kramer procedure. Age, sex, ethnicity were used as covariates in the ANCOVA analysis.
2.4 Results
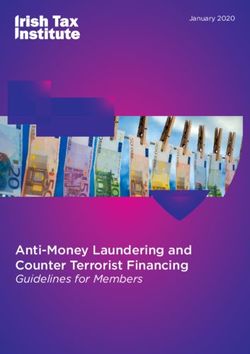
As for blood group determination, SNPS rs8176719 and rs8176746 were genotyped to
infer the ABO blood group of study subjects. Figure 2-2A shows that Group O, A, B and AB
represented 37%, 38%, 19% and 6% of the population, respectively. The frequency of each blood
group was different across ethnocultural groups (P17
A
O
A
B
AB
B
Caucasian
East
Asian
Others
South
Asian
O
A
B
AB
Figure 2-2: ABO blood group distribution in the entire TNH cohort (A) and by ethnocultural
groups (B).
1718
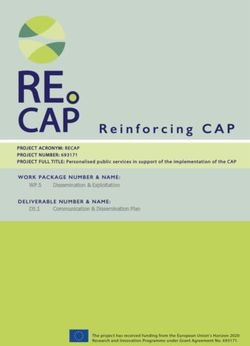
Subject characteristics based on the ABO blood group are summarized in Table 2-1. After
adjusting for age, sex, and ethnocultural group, subject characteristics were similar across ABO
blood groups, except for insulin, HOMA-IR and HOMA-Beta. Group O individuals had lower
levels of fasting insulin, HOMA-IR and HOMA-Beta compared to group A or B. Although the
overall association between blood group and total cholesterol was significant (p=0.043), no
difference was observed among specific ABO blood group. Figure 2-3 and Figure 2-4
respectively show the levels of fasting glucose and insulin in individuals with different ABO
blood groups.
1819
Table 2-1: Subject Characteristics by ABO Genotypea
Genotype
Characteristic O A B AB P value
Subjects [n (% of total)] 543 (37) 544 (38) 277 (19) 91 (6)
b
Age (y) 22.7 ± 2.5 22.8 ± 2.5 22.4 ± 2.3 22.5 ± 2.6 0.13
Sex [n (%)] 0.31
Female 358 (36) 387 (39) 187 (19) 61 (6)
Male 185 (40) 157 (34) 90 (19) 30 (7)
Ethnocultural group [n (%)]20
5
4.9
4.8
Fas`ng
Glucose
(mmol/L)
4.7
4.6
4.5
4.4
4.3
4.2
4.1
4
O
A
B
AB
Figure 2-3: Levels of fasting glucose in individuals with different ABO blood groups.
2021
60
b
b
55
ab
50
a
Fas`ng
Insulin
(pmol/L)
45
40
35
30
O
A
B
AB
Figure 2-4: Levels of fasting insulin in individuals with different ABO blood group
212.5 Discussion
Regarding the determination of ABO blood group, the reported frequency of blood group
distribution in our study population is similar to the frequency reported previously for Canada
[78], in which group O and A being the most common two blood groups. The higher frequency
of blood group B observed in people from Asian ethnocultural backgrounds is also consistent
with previous findings [5]. The consistency of our results with existing knowledge therefore
confirms the validity of our blood-typing method.
An examination of the relationship between the ABO blood group and levels of
cardiometabolic risk factors showed no association for most of the biomarkers, except for fasting
insulin and the derived assessment of insulin resistance and beta-cell function. The lower levels
of these risk factors in subjects with blood group O were consistently shown in both men and
women and across different ethnocultural groups (data not shown). This finding is in line with
previous research suggesting that an association may exist between the blood groups and diabetes
risk [11,70,71,72,73]. However, it is not clear which ABO blood group is at higher risk. Some
studies reported that individuals with blood group O were at higher risk [11,70], but this was not
replicated in others [71,72,73]. The inconsistent results from these studies may be partly
explained by ethnicity, sample sizes and other unadjusted covariates. By investigating in a
multiethnic population, our study indicates that the linkage between ABO blood group and
diabetes risk exist consistently across ethnicities. The observed difference in fasting insulin levels
in healthy young adults also indicates that may indeed play a role in the development of insulin
resistance and the aetiology of T2D development and contribute to diabetes risk later in life.
Larger prospective studies will be helpful to further confirm the etiological relationship between
ABO blood group and T2D, which has the potential facilitate T2D screening and prevention.
2223
Chapter 3: Effect of “Blood-Type” Diet on Cardiometabolic Risk
Factors
3.1 Abstract
Background: Each of the four “Blood-Type” diets represents a distinct dietary pattern.
Promoting high vegetable and fruits consumption, the Type-A diet resembles to a vegetarian diet.
Recommending moderate intake of fish and dairy consumption, the Type-AB and Type B diets
are closely related to the well-known Mediterranean diet. As the only “Blood-Type” diet that
allows high intake of animal proteins, the Type-O diet is similar to a low-carbohydrate diet.
Before examining whether people with certain blood group may benefit more from following the
corresponding “Blood-Type” diet, it is critical to investigate the overall dietary effects in people
regardless of their ABO blood groups, which is the objective of this chapter.
Methods: Subjects (n=1,455) were participants of the Toronto Nutrigenomics and Health study.
Overnight 12-hour fasting blood samples were collected to measure serum cardiometabolic
biomarkers through by high performance liquid chromatography. Dietary intake was assessed
using a one-month, 196-item food frequency questionnaire and a diet score was calculated to
determine relative adherence to each of the four “Blood-Type” diets. ANCOVA, with age, sex,
ethnicity, and energy intake as covariates, was used to compare anthropometric measurements
and biomarkers of cardiometabolic health across tertiles of each blood type diet score.
Results: Adherence to the Type-A diet was associated with lower BMI, waist circumference,
blood pressure, serum cholesterol, triglycerides, insulin, HOMA-IR and HOMA-Beta (P24 (P
25
diet. Therefore, each of the four “Blood-Type” diets is similar to some existing dietary patterns
that have been shown to reduce the disease risk and promote health.
As for the Type-A diet pattern, vegetarian diets contain no meat, more grains, legumes,
vegetables and fruits, which therefore is associated with lower dietary intake of total fat, saturated
fat, and cholesterol and higher intake of fiber [79]. Consuming a vegetarian diet has been shown
to reduce the risk of hospital admission [80], cataract [81], cancers [82,83], T2D [84,85],
hypertension [86], ischemic heart disease [87], and all-cause mortality [88]. As for
cardiometabolic diseases specifically, people who follow a vegetarian diet are known to have
higher insulin sensitivity, lower blood pressure and LDL-cholesterol, which contribute to a lower
risk of diabetes [89] and ischemic heart disease [80] compared to non-vegetarians.
As for dietary pattern that resembles to the Type-AB and Type-B diets, the Mediterranean
diet is characterized by a high consumption of whole grains, fruits and vegetables, legumes and
olive oil, and a moderate consumption of fish, dairy and wine [90]. This popular diet has recently
received wide attention from the public as many studies have demonstrated its health-promoting
effects [90]. Adherence to a Mediterranean diet has been shown to decrease the risk of preterm
delivery [91], gestational diabetes [92], Alzheimer’s Disease [93], Parkinson’s Disease [94], and
pancreatic [95], colorectal [96], breast [97,98], and esophageal cancers [98]. Regarding to
cardiovascular diseases and diabetes, research has shown that adhering to the Mediterranean diet
could have long-term beneficial effects on insulin sensitivity and blood pressure management,
which could lead to lower risks of Type 2 diabetes and cardiovascular diseases [69,99]. It has
been suggested that the observed beneficial effect may be attributed to higher intakes of anti-
oxidants, n-3 fatty acids, and fibre from the Mediterranean diet [69]. Therefore, as evident from
2526
the aforementioned studies, following a Mediterranean diet may be beneficial for preventing
chronic diseases, such as cardiovascular diseases and Type 2 diabetes.
As the “Blood-Type” diet that restrains the intake of grains and promotes the
consumption of animal products, the Type-O diet resembles to the low-carbohydrate diet and the
high-protein diet. With carbohydrate content contribute to 15%-40% of total energy intake, low-
carbohydrate diets have been shown to promote weight loss and enhance glycemic control
[100,101]. High-protein diets typically are characterized by 20-30% or more of total daily
calories coming from proteins [102]. High intakes of proteins have been suggested to enhance
appetite suppression [103] and insulin sensitivity [104]. Nonetheless, with its recommendation
for animal protein consumption, especially red meat, the Type-O diet also shares some similarity
with the high-fat diet, which is known to cause extra abdominal fat accumulation [105,106],
hyperphagia [107], and insulin resistance [108]. Therefore, the Type-O diet may represent as the
only non-healthy “Blood-Type” diet.
Based on findings of these previous studies on different dietary patterns, it is interesting
to examine whether each of the four “Blood-Type” diets can influence serum biomarker profile in
our study population. The examination of this association requires the quantification of the
relative adherence to the “Blood-Type” diet based on the existing data from the Food Frequency
Questionnaire (FFQ). Considering the fact that the “Blood-Type” diet recommends the
consumption or avoidance of specific food items, the diet adherence score system needs to be
based on these items, instead of the general food group. Furthermore, because the
recommendations of the “Blood-Type” diet does not specify the exact amount of consumption for
each food item [1], the score system would assign points based on actual quantity of consumption
for each food item and assumes that higher consumption indicates closer adherence. Based on the
2627
food item and their quantities of consumption provided by the Food Frequency Questionnaire, the
scoring system aimed to generate a continuously scaled grade to capture relative diet adherence
of each individual. By examining the effect of “Blood-Type” diets in a population regardless of
ABO blood group, the goal of this chapter was to investigate whether following “Blood-Type”
diets is associated with a healthier biomarker profile in the general population.
3.3 Material and Methods
3.3.1 Study Design and Participants
Refer to Chapter 2 (pages 14).
3.3.2 Dietary Adherence Score Assessment
Dietary intake was assessed by a one-month, Toronto-modified Willet 196-item semi-
quantitative food frequency questionnaire (FFQ) as described previously [77]. Briefly, each
subject was given instructions on how to complete the FFQ by using visual aids of portion sizes
to improve the measurement of self-reported food intake. Subject responses to the individual
foods were converted into daily number of servings for each item. In order to quantify the
adherence to each of the four “Blood-Type” diets, four different diet scores were given to each
subject regardless of his or her own blood group. Based on the food items listed in the “Blood-
Type” diet [1], subjects received one positive point for consuming one serving of each
recommended food item and one negative point for consuming one serving of an item on the list
of foods to avoid. Foods that are listed as “Neutral” were not included in the equation and do not
contribute to the final score. The equation of calculating the diet score is attached below.
2728
“Blood-Type” Diet Score = Σ (Recommended Food Groups to Eat * Servings) – Σ
(Recommended Food Groups to Avoid * Servings)
The lists of recommended foods to eat or avoid for each ABO blood group are shown in the
Appendix. Subjects were then grouped into tertiles based on their scores for each diet, with the
top tertile representing those whose diet most closely resembles the corresponding blood type
diet.
3.3.3 Cardiometabolic Risk Factor Assessment
Refer to Chapter 2 (page 15).
3.3.4 Statistical Analysis
Statistical analyses were performed using the Statistical Analysis Systems (SAS)
Software program (version 9.2; SAS Institute Inc., Cary, North Carolina). The a error was set at
0.05 and reported p-values are 2-sided. Subject characteristics were compared across ABO blood
groups by using chi-square tests for categorical variables and analysis of variance (ANOVA) for
continuous variables. Analysis of covariance (ANCOVA) was used to compare means of
biomarkers of cardiometabolic disease risk across tertiles of diet scores. Variables that were not
normally distributed were either loge or square root transformed prior to analysis, but the mean
2829
values and standard errors are displayed without transformation to facilitate interpretation. Means
compared between groups were adjusted for multiple comparisons using the Tukey-Kramer
procedure. Age, sex, ethnocultural group and energy intake were used as covariates in the
ANCOVA analysis. Physical activity and smoking were also considered; however, they did not
materially alter the results and were not included in the final model.
3.4 Results
Regarding the diet adherence assessment, the method used in this study was able to
generate scores that are continuously scaled and have a normal distribution. Figure 3-1A and
Figure 3-1B demonstrate the total number of recommended items to eat or avoid respectively in
four major food groups listed in the FFQ for each "Blood-Type” diet. Briefly, the Type-A diet
recommends high consumption of grains, fruits, and vegetables. The Type-B diet recommends
high intake of dairy products and moderate intakes of other food groups. The Type-AB diet is
similar to the Type-B diet in terms of recommended food groups, but has more restrictions on
specific food items. For example, only eggs and fish are recommended as sources of meat for
group AB individuals. The Type-O diet encourages high consumption of meats and avoidance of
grain products. In order to quantify the adherence to these four blood type diets, four different
scores were calculated for each subject, regardless of his or her own ABO genotype. Figure 3-2
shows the score distribution. All four scores were normally distributed and did not require any
transformation.
29You can also read