A WHOLE CLOTTA MYSTERY: DOSING ANTICOAGULANTS IN OBESITY - ANDREW ZWERLEIN, PHARMD & CORRIE BLACK, PHARMD PGY1 PHARMACY RESIDENTS PROVIDENCE ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
A WHOLE CLOTTA MYSTERY:
DOSING ANTICOAGULANTS
IN OBESITY
Andrew Zwerlein, PharmD & Corrie Black, PharmD
PGY1 Pharmacy Residents
Providence Alaska Medical Center
AKPhA Annual Convention- February 13, 2021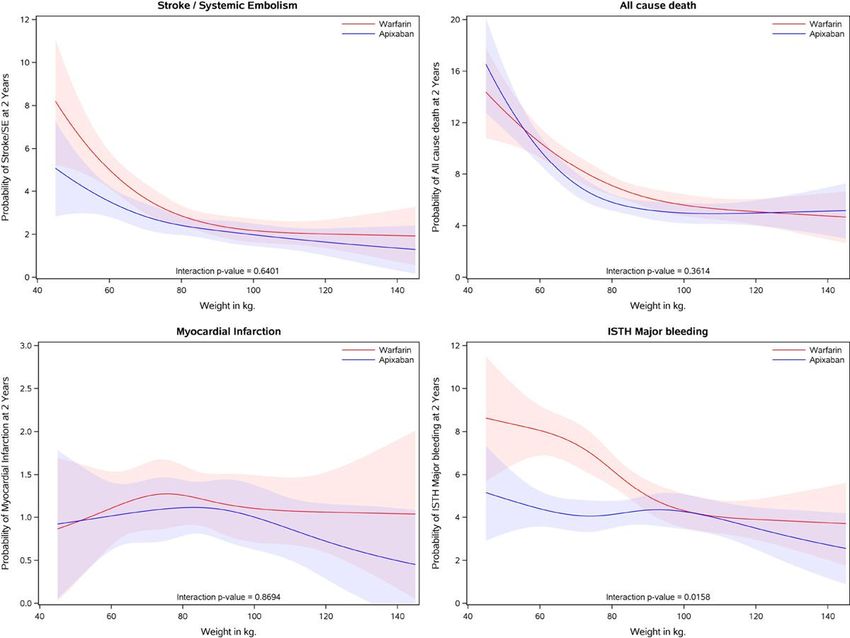
Disclosures • No disclosures from either of the presenters
Learning Objectives
By the end of the presentation, technicians should be able to:
• Define obesity according to the World Health Organization
• List possible risks to the patient associated with sub- or supratherapeutic dosing of
anticoagulants
By the end of the presentation, pharmacists should be able to:
• Describe pharmacokinetic changes in obesity
• Summarize current literature for anticoagulants in obese populations
• Apply appropriate dosing strategies and monitoring plans for oral and parenteral
anticoagulants in obesity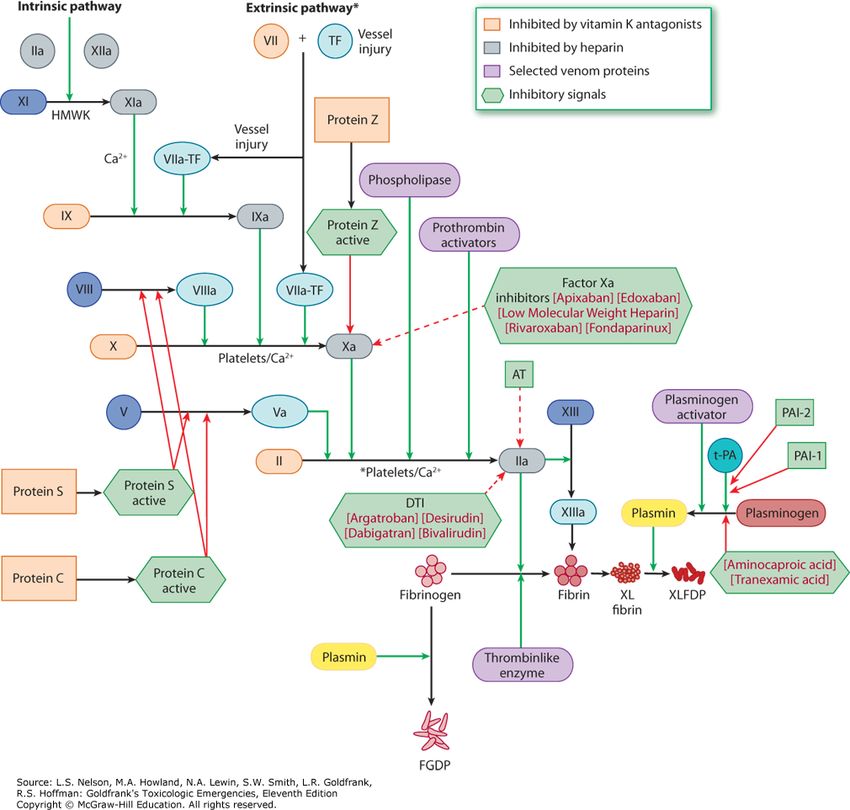
Outline
Pre-test questions
Define obesity
Overview of anticoagulants
Describe pharmacokinetic/pharmacodynamic changes
Review parenteral anticoagulation and obesity literature
Review direct oral anticoagulation and obesity literature
Post-test questions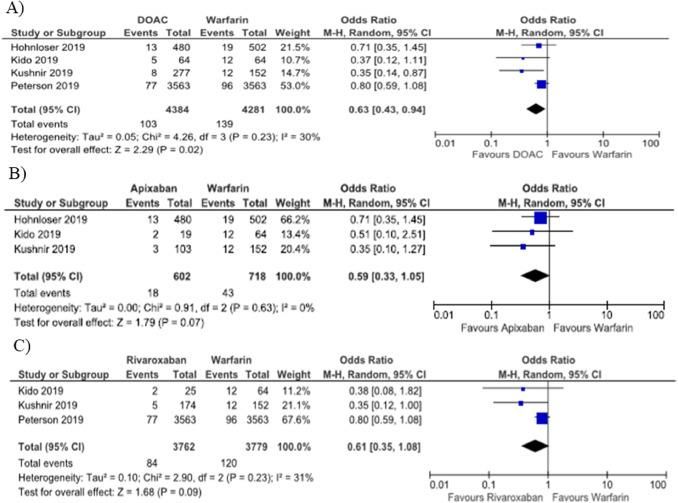
Question 1 How does the World Health Organization define obesity? a. >150 lbs b. >120 kg c. BMI >40 d. BMI >30
Question 2 What pharmacokinetic property/ies change in obese patients compared to normal weight patients? a. Vd tends to be smaller if drug is lipophilic b. Clearance is increased for renally cleared drugs c. Drug absorption is increased d. All the above
Question 3 Given patients with obesity may display altered pharmacokinetics, what is the risk of anticoagulation that is supra-therapeutic? (select all that apply) a. Intracranial hemorrhage b. Death c. GI bleed d. Stroke
Question 4 Which of the following anticoagulants may need dose adjustments in obese patients? a. Apixaban b. Aspirin c. Enoxaparin d. Dabigatran
Question 5 Thromboprophylaxis high dose unfractionated heparin (i.e. 7,500 units q8h) may be associated with increased ______ risk when used in obese patients. a. Recurrent thrombosis b. Bleed c. Treatment failure d. Kidney injury
Question 6 Which anticoagulation
regimen should not be
J.M. 37yof, 161 kg, 5'0.5", BMI 70 used for this patient?
PMH: asthma, obesity, PCOS
a. Enoxaparin 150 mg twice daily
cc: Chest pain
BP 150/110, HR 144, RR 38, O2 sat 99% RA b. Enoxaparin 1.5 mg/kg once daily
CT angiogram: pulmonary emboli with c. Heparin bolus and drip adjusted
severe right heart strain via a weight-based nomogram
D-dimer: 16.8, SCr 0.66 d. Enoxaparin 0.8 mg/kg twice dailyINTRODUCTION TO
OBESITY
Definition of Obesity
Pharmacokinetic changes
Subtherapeutic vs supratherapeutic vs therapeuticBODY MASS INDEX BMI RANGE
(BMI) CATEGORY
Underweight < 18.5 kg/m2
World Health
Organization Normal 18.5 – 24.9 kg/m2
(WHO)
Overweight 25 – 29.9 kg/m2
Definition
Class I Obese 30 – 34.9 kg/m2
Class II Obese 35 – 39.9 kg/m2
Body mass index – BMI. WHO.
https://www.euro.who.int/en/health-topics/disease-
prevention/nutrition/a-healthy-lifestyle/body-mass-
Class III Obese ≥ 40 kg/m2
index-bmiDose Adjustment Equations
Total Body Weight (TBW) = Actual measured weight
BMI = TBW (in kg) / height (m2)
Lean Body Weight (LBW) – Male = [1.1 x TBW (kg)] – [0.0128 x BMI x TBW (kg)]
LBW – Female = [1.07 x TBW (kg)] – [0.0148 x BMI x TBW (kg)]
Ideal Body Weight (IBW) – Male = 50 kg + 2.3 [height (in) – 60]
IBW – Female = 45.5 kg + 2.3 [height (in) – 60]
Adjusted Body Weight (AdjBW) = IBW + 0.4 (TBW – IBW)
Shank B, Zimmerman D. Demistifying Drug Dosing in Obese Patients. ASHP. 2016Pharmacokinetic Changes in Obesity
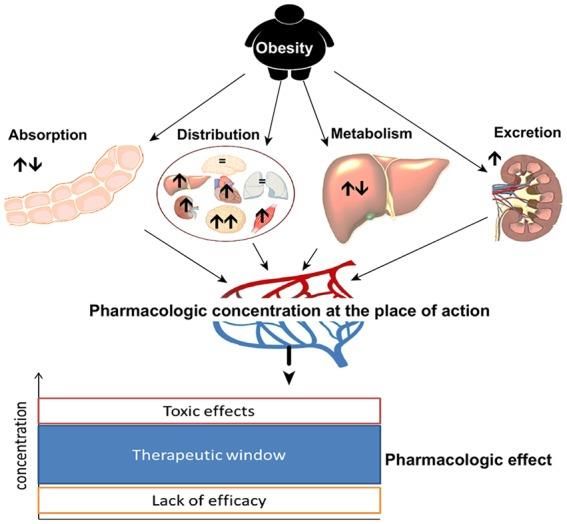
• Absorption
• Not much evidence
• Distribution
• Lipophilicity
• Polarity
• Plasma protein binding
• Metabolism
• Mixed data
• Excretion
• Increased clearance
• Nonlinear with TBW
• Cockcroft-Gault
May, et al. Ther Adv Endocrinol Metab 2020, Vol. 11: 1–19Challenges and Considerations with
Anticoagulation in Obesity
• Patients with severe forms of obesity are often excluded
or underrepresented in clinical trials
• Differing definitions of “obese” patients included in trials
• Pharmacokinetics among drugs may vary
• Medication dosing may require different weight-based
strategies
• Managing the therapeutic window
• Consequences with subtherapeutic/supratherapeutic
levelsClotting Cascade • Pathway of clot formation • Anticoagulants inhibit this pathway • Inappropriate medication concentrations could lead to unwanted effects
Risks and Benefits of Anticoagulation
• Risks of being subtherapeutic
• Stroke
• Myocardial infarction
• Death
• Risks of being supratherapeutic
• Minor/major bleeds
• Bleeding requiring hospitalization
• Death
• Benefits
• Stabilizes an active clot
• Prevents future clot formationPARENTERAL
ANTICOAGULANTS
Heparin (UFH) & Low Molecular Weight Heparin (LMWH)
Corrie Black, PharmD
PGY1 Resident at Providence Alaska Medical CenterPulmonary Embolism HEPARIN VTE/PE PROTOCOL
Bolus: 80 units/kg x1 (10,000 units max)
(PE) Case Infusion: 18 units/kg/hr, INITIAL RATE MAX 1,500 units/hr
Goal: aPTT 60-90 seconds
J.M. 37yof, 161 kg, 5'0.5", BMI 70 aPTT Nomogram for ADJUSTING heparin
PMH: asthma, obesity, PCOS aPTT < 50 seconds:
Bolus 5,000 units & increase rate by 150 units/hr
cc: Chest pain Repeat aPTT 6 hr after change
BP 150/110, HR 144, RR 38, O2 sat 99% RA
CT angiogram: pulmonary emboli with RECEIVED
severe right heart strain
Heparin 10,000 u bolus
D-dimer: 16.8, SCr 0.66 Baseline aPTT- 28 seconds
Heparin 1,500 units/hour started
6 hr aPTT- 30 seconds
Heparin 5,000 u bolus then infusion changed to
1,650 units/hour
12 hr aPTT- 27 secondsHeparin Pharmacokinetics
High protein binding & low Vd
• Stays in vasculature
Rapid saturable and slow first
order clearance
Blood volume increases with
increasing body weight
• Moderate dose increase needed
in obesity
Clin Pharmacokinet. 1980;5(3):204-220 Chest. 1995;108(4)(suppl):258S-275S Chest. 2012;144(2):( suppl):e24S-e43STherapeutic Anticoagulation When achieved in
Heparin Weight-Based Nomogram
Weight based group: 97% reached
therapeutic threshold within 24
hours vs 77% in standard group
Higher doses given in weight-
based group:
• Without more major bleeds
• Reduced recurrent thrombosis
Ann Intern Med 1993;119(9):874 – 881Heparin Weight-Based Nomogram
Standard dose adjustment nomogram
aPTT Adjustment Cardiac/ACS
< 50 Bolus 5,000 units & increase rate by 150 units/hr Starting heparin IV bolus: 60 units/kg x1 dose (MAX 4000 units)
Starting heparin IV infusion rate: 12 units/kg/hr (MAX 1,000 units/hr)
50-59 Bolus 2,000 units & increase rate by 100 units/hr
60-90 No change VTE/PE
Starting heparin IV bolus: 80 units/kg x1 dose
91-100 Decrease rate by 50 units/hr Starting heparin IV infusion rate: 18 units/kg/hr (MAX 1,500 units/hr)
101-120 Stop infusion 30 minutes & decrease by 100 units/hr
121-170 Stop infusion 60 minutes & decrease rate by 150 units/hr
> 170 Stop infusion 60 minutes & decrease rate by 200 units/hr
Weight based dose adjustment nomogram
aPTT Adjustment
< 50 Bolus 80 units/kg, max 10,000 units & increase rate by 4 units/kg/hr
50-59 Bolus 40 units/kg, max 10,000 units & increase rate by 2 units/kg/hr
60-90 No change
91-100 Decrease rate by 1 unit/kg/hr
101-120 Stop infusion 30 minutes & decrease by 2 units/kg/hr
121-170 Stop infusion 60 minutes & decrease rate by 3 units/kg/hr
Ann Intern Med 1993;119(9):874 – 881Which Body
Weight to Use?
Hours to
Bleed
One study found higher major bleed therapeutic
BMI event n
rates when TBW (10.5%) was used in aPTT, p= 0.506
obese vs non-obese (1.1%) p=0.01, no (%)
difference when AdjBW used (9.1% vs
12.2%, p=0.66) 100 kg with a BMI >30, time
UFH dosed with AdjBW if TBW was >120% of IBW
to therapeutic anti-coagulation is
(TBW used otherwise)- found comparable time to
comparable whether dosed by TBW
therapeutic aPTT amongst BMI groups (table above)
or AdjBW
Am J Health Syst Pharm 2016;73:1512-1522 J Thromb (2020) 49:206–213 Ann Pharm 2017; 51(9) 768-773PE Case
J.M. 37yof, 161 kg, 5'0.5", BMI 70
PMH: asthma, obesity, PCOS
cc: Chest pain
BP 150/110, HR 144, RR 38, O2 sat 99% RA RECEIVED
CT angiogram: pulmonary emboli with Heparin 10,000 u bolus
severe right heart strain Baseline aPTT- 28 seconds
D-dimer: 16.8, SCr 0.66 Heparin 1,500 units/hour started
6 hr aPTT- 30 seconds
Heparin 5,000 u bolus then infusion changed
to 1,650 units/hour
12 hr aPTT- 27 secondsEnoxaparin Pharmacokinetics
Compared to Heparin: In obese patients:
• More predictable • Dose reduction likely
anticoagulation response needed (TBW)
• Predominantly renally cleared • Recommended to
• GFR increases with body monitor anti-Xa levels
weight • Twice daily dosing is
superior to once daily
dosing
Chest. 2012;144(2):( suppl):e24S-e43S Eur J Clin Pharmacol 2015;71(01):25–34 Ann Intern Med 2001;134 (03):191–202Enoxaparin < 1 mg/kg BID?
Average therapeutic doses by BMI
mg/kg
BMI Class q12h IQR
40-50 0.97 0.79-1.0
50-60 0.70 0.64-0.93
>60 0.71 0.58-0.98
Clin Drug Inves (2020) 40:33–40Enoxaparin ~0.7-1 mg/kg BID
Hospitalized cohort, BMI >40:
• Average therapeutic dose: 0.83 mg/kg BID Case Reports
• Average weight 138 kg • 0.85 mg/kg BID, 263 kg
• 0.62 mg/kg BID, BMI 114,
Australian cohort, >100 kg: 0.75-0.85 mg/kg BID 322 kg
• 14% subtherapeutic (0.74 mg/kg)
• 62% therapeutic (0.82 mg/kg)
• 24% supratherapeutic (0.89 mg/kg)
• Average weight 128 kg
Clin Appl Thromb Hemost 2015 Sep;21(6):513-20 J Thromb (2019) 48:387–393 Hosp Pharm 2019;54:371-7 Am J Health Syst Pharm 2017;74:977-80PE Case
J.M. 37yof, 161 kg, 5'0.5", BMI 70
PMH: asthma, obesity, PCOS
What dosing
cc: Chest pain strategy do you
BP 150/110, HR 144, RR 38, O2 sat 99% RA
CT angiogram: pulmonary emboli with
recommend for
severe right heart strain
D-dimer: 16.8, SCr 0.66
enoxaparin?Take Home Points-
Parenteral Treatment Dosing
Heparin Enoxaparin
• For BMI ≥ 40, use AdjBW • Higher bleed risk with standard
dosing is suspected
• Weight based dosing nomogram
achieves therapeutic anticoagulation • Therapeutic anti-Xa levels in obese
quicker patients is associated with
enoxaparin 0.7-1 mg BID
• Insufficient evidence suggestive that
dose capping prevents bleeds in • Consider lower doses in more
obese patients extreme weight (in addition to other
considerations, e.g. age, renal
function, clot vs bleed risk)
• Limited data with doses >150 mgThromboembolism Prophylaxis
Bariatric surgery registry “High dose” vs standard prophylaxis,
hospitalized cohort with BMI>40:
Large registry found lower VTE rates with
LMWH vs UFH • High dose: enoxaparin 40 mg BID or UFH 7,500
TID
• OR 0.34 (0.19–0.62)
• Standard dose: enoxaparin 40 mg QD or UFH
5,000u BID-TID
• VTE rate: 0.77% vs 1.48%, OR 0.52 (0.27-1.00)
Another cohort, average BMI 50: • Bleed rate OR 0.84 (0.66-1.07)
• Enoxaparin 40 mg BID: 0.6%
• vs 30 mg BID: 5.4% VTE rate,pHeparin Prophylaxis Dosing in Obesity
Retrospective cohort,
hospitalized
Hospitalized patients >100 kg,
UFH 7,500 or 5,000u q8h • All received UFH 5,000 units q8h
• VTE rates: 0.6% vs 0.7% (BMI
• Similar VTE rates
>30 vs 40
demonstrated poor association
with BMI>30 and VTE (OR 1.4,
0.7-3.0)
• Bleed rates comparable
Pharmacother; 2016 36(7):740-748 Throm Res; 2018 169:159-156Enoxaparin Prophylaxis Dosing
Risk stratified dosing algorithm
0.5 mg/kg q12h, goal anti-Xa: 0.2-0.6 • Very high risk: 0.5 mg/kg q12h
• Moderate-high risk: 0.5 mg/kg q24h
Surgical ICU patients, average BMI 46 • 86% achieved goal level
• 91% achieved goal level • Average BMI 45.6
• No bleeds noted
General medicine patients
Trauma patients, average BMI 35 • 0.5 mg/kg/day achieved goal level vs
0.4 mg/kg/d or 40 mg/d
• 86% achieved goal level
• Average BMI >60
Pharmacother 2011;45:1356-62 Am J Surg 2013;206:847-51 J Pharm Technol 2015;31:282-8 Am J Hematol 2012;87:740-3Take Home Points- Prophylaxis Dosing
Heparin Enoxaparin*
• UFH 5,000 q8h recommended • 40 mg BID appropriate in
patients with BMI >40
• Higher doses may be associated
with increased bleed risk, • Larger doses may be necessary
further data needed in more extreme obesity or with
higher VTE risk
• 60 mg BID or ~0.4-0.5 mg/kg
twice daily if BMI >50
*Normal renal functionDIRECT-ACTING ORAL
ANTICOAGULANTS
(DOAC)
Apixaban, Dabigatran, Edoxaban, Rivaroxaban
Andrew Zwerlein, PharmD
PGY1 Resident at Providence Alaska Medical CenterThe DOACs in Question
• Medications
• Direct Thrombin Inhibitor
• Dabigatran
• Factor Xa Inhibitors
• Apixaban
• Edoxaban
• Rivaroxaban
• Indications
• Ischemic stroke prevention in non-valvular atrial fibrillation (NVAF)
• Guideline suggests DOAC > warfarin
• Venous thromboembolism (VTE)
• Guideline suggests in patients with VTE and no cancer, DOAC > warfarin
January C, et al. Circulation. 2019;140:e125–e151 Kearon C, et al. CHEST 2016; 149(2):315-352Quantitative Assessments for DOAC
• Diluted thrombin time • Anti-Xa Levels
• Dabigatran • Apixaban
• Edoxaban
• Rivaroxaban
Eikelboom J, et al. JAMA Cardiology. 2017;2(5):566-574Pharmacokinetics After Apixaban 10 mg
• Body weight has little
impact
• Caution with severe renal
impairment
• Cmax~31% lower (90% CI:
18-41%) than reference
• AUC~23% lower (90% CI:
9-35% than reference
• Anti-Xa activity was linear
with plasma concentration
regardless of body weight Upreti V, et al. Br J Clin Pharmacol
. 2013 Dec;76(6):908-16.Pharmacokinetics After Rivaroxaban 10 mg
Kubitza D, et al. J Clin Pharmacol
. 2007 Feb;47(2):218-26.Dabigatran and Edoxaban
Pharmacokinetics
• RE-LY - Dabigatran • Edoxaban
• Weight ≥ 100 kg has 53% higher • Pharmacokinetic evidence in obesity is
concentration than weight < 50 kg not well-studied
• Wide therapeutic range for 110 mg and • Body weight affected nonrenal clearance
150 mg strengths
• Safety and efficacy correlated with
plasma concentrations
• Renal function and age are important
factors
Reily P, et al. J Am Coll Cardiol Yin O, et al. Eur J Clin Pharmacol
. 2014 Feb 4;63(4):321-8. . 2014 Nov;70(11):1339-51.International Society of Thrombosis and
Haemostasis (ISTH) Guidance
• Recommendations
• Standard dosing of DOAC in patients with a BMI ≤ 40 kg/m2 and weight ≤ 120 kg
• Avoid DOAC with a BMI > 40 kg/m2 or weight > 120 kg
• If using DOAC in patients with a BMI > 40 kg/m2 or weight > 120 kg, check drug-
specific peak and trough level
J Thromb Haemost. 2016 June ; 14(6): 1308–1313Recent Literature
• NVAF • VTE
• Phase 3 Trial Post-Hoc Data • Retrospective Studies
• ARISTOTLE • Kushnir, et al 2019
• ENGAGE-TIMI 48 • Spyropoulos, et al 2019
• RE-LY • Coons, et al 2020
• ROCKET-AF
• Retrospective Studies
• Kido, et al 2019
• Kushnir, et al 2019
• Peterson, et al 2019NVAF LITERATURE
ARISTOTLE “Obesity Paradox”
• All-cause mortality
• Overweight: HR 0.67 (95% CI 0.59-
0.78)
• Obese: HR 0.63 (95% CI 0.54-
0.74), P < 0.0001]
• Composite endpoint
• Overweight: HR 0.74 (95% CI 0.65-
0.84)
• Obese: HR 0.68 (95% CI 0.60-0.78)
P < 0.0001
• Higher BMI was associated with
lower risk of all-cause mortality
and lower stroke, systemic
embolism (SE), myocardial
infarction, or all-cause
mortality than normal BMI
Sandhu R, et al. Eur Heart J
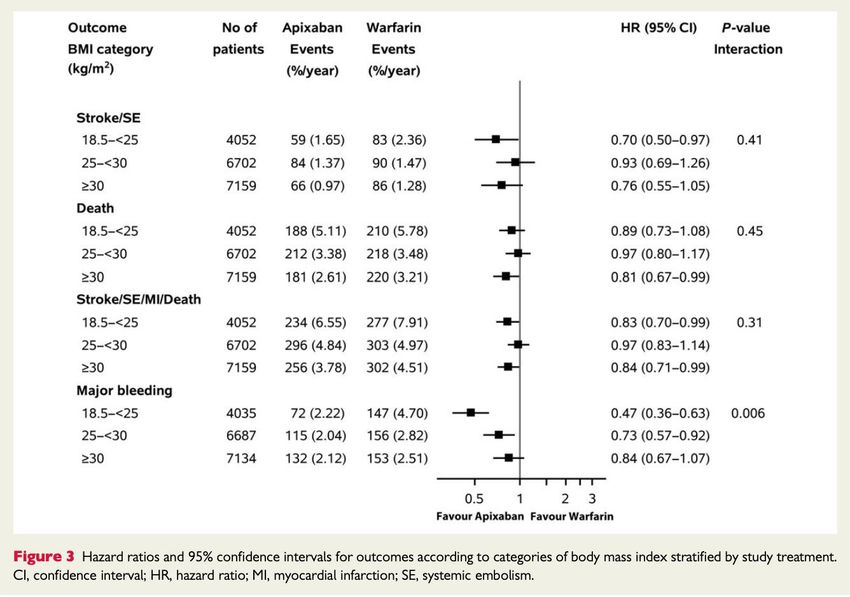
. 2016 Oct 7;37(38):2869-2878.ARISTOTLE (Apixaban)
• No significant interactions between 3
weight cohorts (< 60 kg, 60-120 kg, >
120 kg) for composite stroke/SE
outcome
• Major bleeding or clinically relevant
non major bleeding (CRNM) had
reductions > 120 kg
• Subanalysis of 121-140 kg vs > 140 kg
had wide confidence intervals and
small samples
• Stroke/SE: HR 2.35 (95% CI 0.21-
25.95)
• Major bleeding or CRNM: HR 1.21
(95% CI 0.42-3.46)
Hohnloser S, et al. Circulation
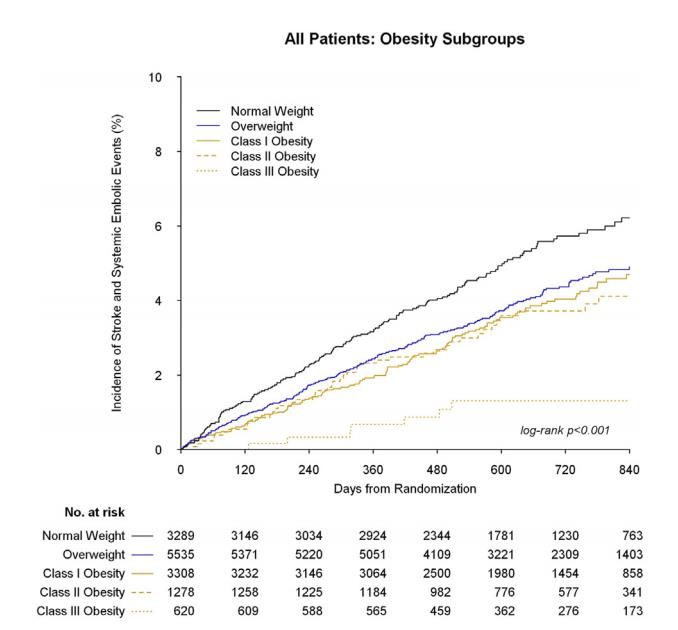
. 2019 May 14;139(20):2292-2300ROCKET-AF (Rivaroxaban)
• Population
• Normal weight (n = 3289)
• Overweight (n = 5535)
• Obese (n = 5206)
• Class II/III obesity protective
association with stroke risk
compared with normal weight
• Overweight: HR 0.78 (95% CI 0.64 to
0.96, p = 0.02
• Class II/III obese patients: HR 0.54,
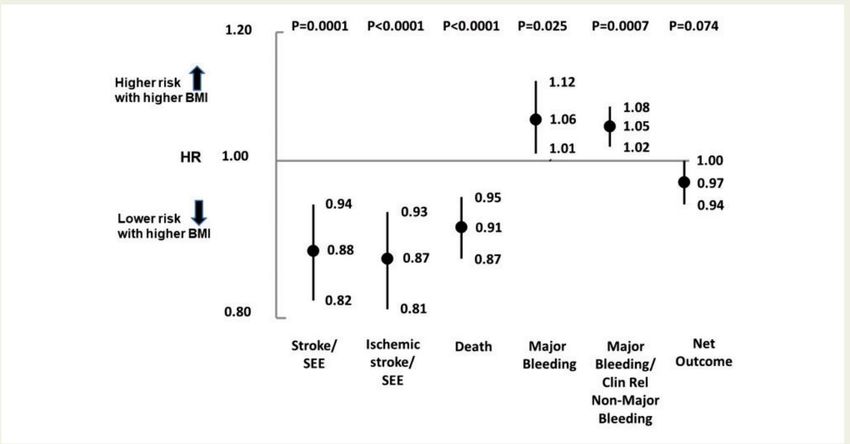
(95% CI 0.40 to 0.73, pENGAGE-TIMI 48 (Edoxaban)
• Increased BMI had
better survival, lower
stroke/SE risk, but
increased risk of
bleeding
• Net outcome not
favorable
• Anti-Xa trough stayed
the same across all
BMI groups
Boriani, et al. Eur Heart J
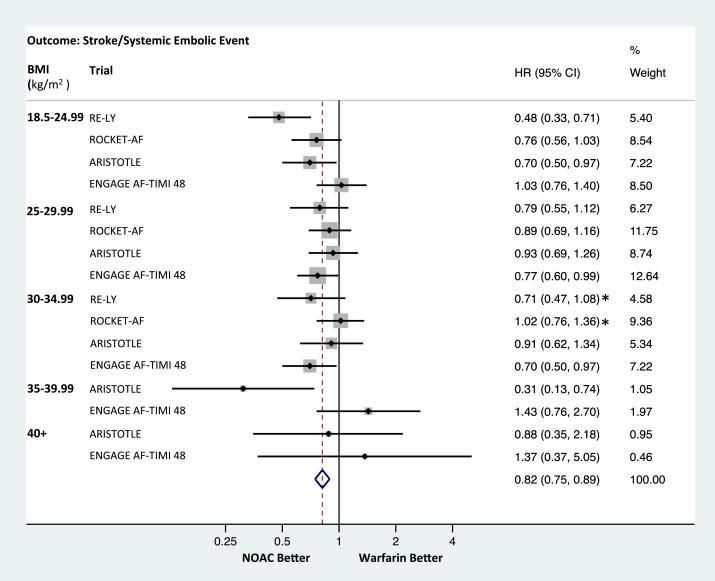
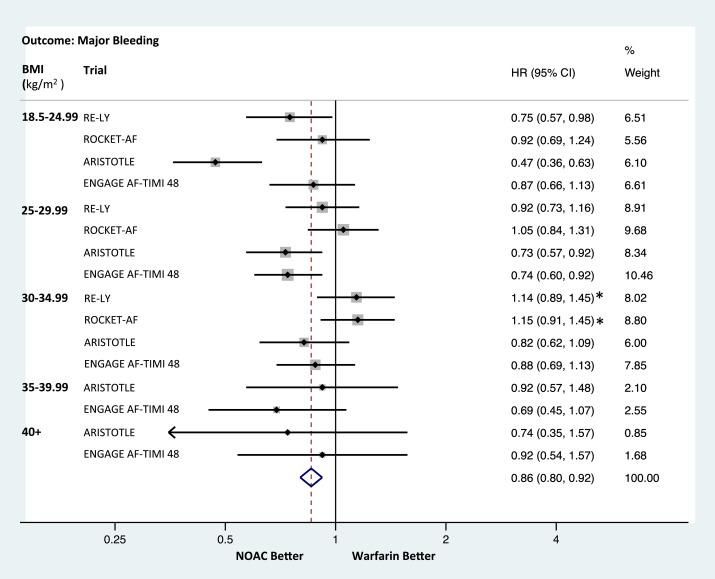
. 2019 May 14;40(19):1541-1550.Analysis of the Major NVAF Clinical Trials Wang, et al. Am J Cardiol
. 2020 Jul 15;127:176-183.DOAC and Obesity with Stroke or SE
Kido, et al. Am J Cardiol
. 2020 Jul 1;126:23-28.DOAC and Obesity with Major Bleeding
Kido, et al. Am J Cardiol
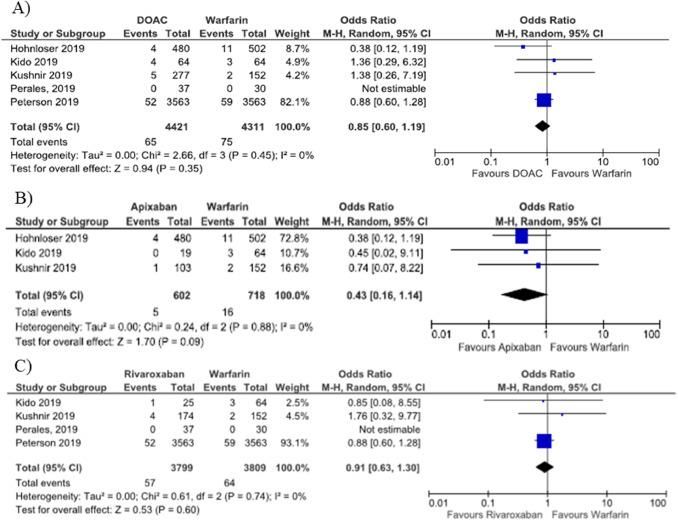
. 2020 Jul 1;126:23-28.VTE TREATMENT LITERATURE
VTE Treatment – Rivaroxaban vs.
Warfarin
• Retrospective Cohort Study - Spyropoulos A, et al
• BMI based on diagnosis code
• < 1% received an anti-Xa level
• Efficacy
• Risk of Recurrent VTE: 8.1% (rivaroxaban) vs. 8.6% (warfarin)
• OR 0.93 (95% CI: 0.77-1.12), p = 0.4338
• Safety
• Risk of major bleeding: 1.4% (rivaroxaban) vs. 1.8% (warfarin)
• OR 0.75 (95% CI: 0.47-1.19), p = 0.2266
• Total health care cost (including pharmacy)
• $43,034 (rivaroxaban) vs $44,565 (warfarin)
• Driven by hospitalization costs
Spyropoulos A, et al. Thromb Res
. 2019 Oct;182:159-166.VTE Treatment DOAC vs. Warfarin
• Retrospective Cohort Study – Coons J, et al
• Dabigatran, apixaban, or rivaroxaban (n = 632) vs.
warfarin (n = 1208)
• Weight 100-300 kg
• Outcomes
• Recurrence of VTE within 12 months
• 6.5% (DOAC) vs 6.4% (warfarin), p=0.93
• Deep vein thrombosis (DVT)
• 3% (DOAC) vs 3.5% (warfarin), p=0.56
• PE
• 3.7% (DOAC) vs 3.8% (warfarin), p=0.94
• Bleeding
• 1.7% (DOAC) vs. 1.2% (warfarin), p = 0.31
Coons J, et al. Pharmacotherapy
. 2020 Mar;40(3):204-210.PE Case
J.M. 37yo F, 161 kg, 5'0.5", BMI 70
PMH: asthma, obesity, PCOS
What oral
cc: Chest pain
anticoagulation
BP 150/110, HR 144, RR 38, O2 sat
do you
99% RA, SCr: 0.82, CrCl~141 ml/min recommend
CT angiogram: pulmonary emboli
with severe right heart strain upon discharge?
D-dimer: 16.8DOAC and Obesity Recommendations
• Apixaban: No dose adjustment needed for AF and VTE
• Up to BMI of 50 kg/m2 for AF
• Up to 300 kg for VTE
• Consider alternative anticoagulation
• Dabigatran: Follow ISTH recommendation and consider alternative anticoagulation
• Edoxaban: Follow ISTH recommendation and consider alternative anticoagulation
• Rivaroxaban: No dose adjustment needed for AF and VTE
• Up to BMI of 50 kg/m2 for AF
• Up to 300 kg for VTE
• Consider alternative anticoagulationQuestion 1 How does the World Health Organization define obesity? a. >150 lbs b. >120 kg c. BMI >40 d. BMI >30
Question 1 How does the World Health Organization define obesity? a. >150 lbs b. >120 kg c. BMI >40 d. BMI >30
Question 2 What pharmacokinetic property/ies change in obese patients compared to normal weight patients? a. Vd tends to be smaller if drug is lipophilic b. Clearance is increased for renally cleared drugs c. Drug absorption is increased d. All the above
Question 2 What pharmacokinetic property/ies change in obese patients compared to normal weight patients? a. Vd tends to be smaller if drug is lipophilic b. Clearance is increased for renally cleared drugs c. Drug absorption is increased d. All the above
Question 3 Given patients with obesity may display altered pharmacokinetics, what is the risk of anticoagulation that is supra-therapeutic? (select all that apply) a. Intracranial hemorrhage b. Death c. GI bleed d. Ischemic Stroke
Question 3 Given patients with obesity may display altered pharmacokinetics, what is the risk of anticoagulation that is supra-therapeutic? (select all that apply) a. Intracranial hemorrhage b. Death c. GI bleed d. Ischemic Stroke
Question 4 Which of the following anticoagulants may need dose adjustments in obese patients? a. Apixaban b. Aspirin c. Enoxaparin d. Dabigatran
Question 4 Which of the following anticoagulants may need dose adjustments in obese patients? a. Apixaban b. Aspirin c. Enoxaparin d. Dabigatran
Question 5 Thromboprophylaxis high dose unfractionated heparin (i.e. 7,500 units q8h) may be associated with increased ______ risk when used in obese patients. a. Recurrent thrombosis b. Bleed c. Treatment failure d. Kidney injury
Question 5 Thromboprophylaxis high dose unfractionated heparin (i.e. 7,500 units q8h) may be associated with increased ______ risk when used in obese patients. a. Recurrent thrombosis b. Bleed c. Treatment failure d. Kidney injury
Question 6 Which anticoagulation
regimen should not be
J.M. 37yof, 161 kg, 5'0.5", BMI 70 used for this patient?
PMH: asthma, obesity, PCOS a. Enoxaparin 150 mg twice daily
cc: Chest pain b. Enoxaparin 1.5 mg/kg once daily
BP 150/110, HR 144, RR 38, O2 sat 99% RA
c. Heparin bolus and drip adjusted
CT angiogram: pulmonary emboli with via a weight-based nomogram
severe right heart strain
d. Enoxaparin 0.8 mg/kg twice daily
D-dimer: 16.8, SCr 0.66Question 6 Which anticoagulation
regimen should not be
J.M. 37yof, 161 kg, 5'0.5", BMI 70 used for this patient?
PMH: asthma, obesity, PCOS a. Enoxaparin 150 mg twice daily
cc: Chest pain b. Enoxaparin 1.5 mg/kg once daily
BP 150/110, HR 144, RR 38, O2 sat 99% RA
c. Heparin bolus and drip adjusted
CT angiogram: pulmonary emboli with via a weight-based nomogram
severe right heart strain
d. Enoxaparin 0.8 mg/kg twice daily
D-dimer: 16.8, SCr 0.66A WHOLE CLOTTA
MYSTERY: DOSING
ANTICOAGULANTS IN
OBESITY
Any Questions?
Andrew.Zwerlein@providence.org
Corrie.Black2@providence.orgYou can also read