A review of microsampling techniques and their social impact
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Biomedical Microdevices (2019) 21: 81
https://doi.org/10.1007/s10544-019-0412-y
A review of microsampling techniques and their social impact
Benson U. W. Lei 1,2 & Tarl W. Prow 1,2
Published online: 15 August 2019
# The Author(s) 2019
Abstract
Conventional skin and blood sampling techniques for disease diagnosis, though effective, are often highly invasive
and some even suffer from variations in analysis. With the improvements in molecular detection, the amount of
starting sample quantity needed has significantly reduced in some diagnostic procedures, and this has led to an
increased interest in microsampling techniques for disease biomarker detection. The miniaturization of sampling
platforms driven by microsampling has the potential to shift disease diagnosis and monitoring closer to the point
of care. The faster turnaround time for actionable results has improved patient care. The variations in sample
quantification and analysis remain a challenge in the microsampling field. The future of microsampling looks
promising. Emerging techniques are being clinically tested and monitored by regulatory bodies. This process is
leading to safer and more reliable diagnostic platforms. This review discusses the advantages and disadvantages of
current skin and blood microsampling techniques.
Keywords Microsampling . Skin biopsy . Blood sampling . Minimally invasive . Point-of-care device . Microneedle
1 Introduction requirements that may subsequently delay clinical deci-
sion-making. The simplification of skin sample collec-
Microsampling is a procedure for capturing minute sam- tion via microsampling has the potential to improve the
ples (usually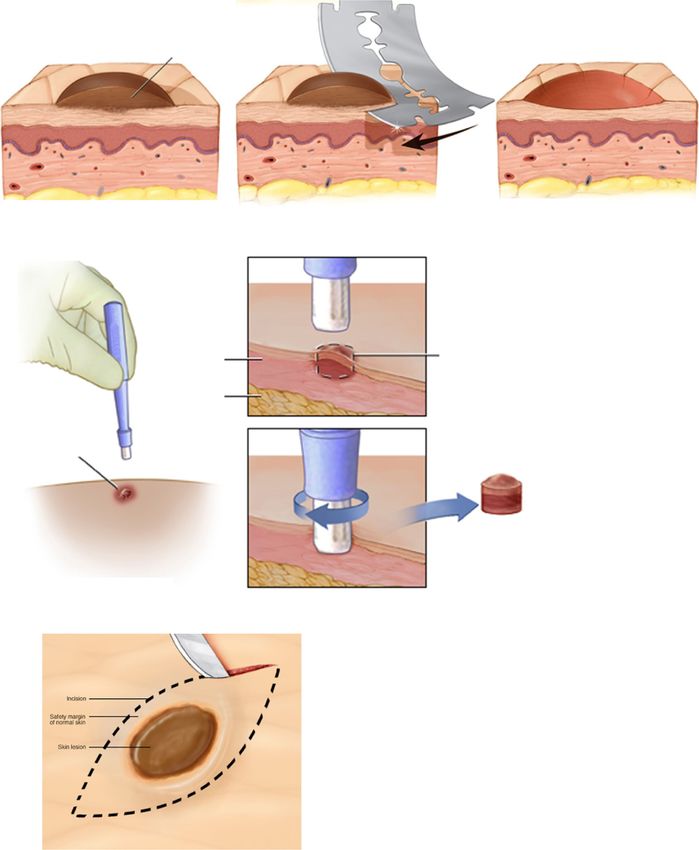
81 Page 2 of 30 Biomed Microdevices (2019) 21: 81
2 Blood sampling as the technique is considered an invasive procedure (Freeman
et al. 2018).
2.1 Conventional blood sampling approach and its
limitations 2.2 Blood microsampling
The use of whole blood sample for biomarker detection is one With improvements in molecular analysis techniques, the de-
of the most commonly used procedures in disease diagnosis, mand for sample size in disease diagnosis has significantly
with an estimated global market size of U$55bn in 2017 reduced. In the case of blood, a microsample generally refers
(Global Blood Testing Market Size & Share | Industry to a sample size of 1 mL in phlebot-
Report, 2018–2024 n.d.). The current standard for whole omy (Nys et al. 2017). A smaller sample demand addresses
blood sampling necessitates a phlebotomist to collect a rela- the limitations in conventional techniques by expanding the
tively large volume of blood (>0.1–1 mL) intravenously using potential for a quicker, cost-effective and less invasive diag-
a hypodermic needle connected to an evacuation tube nostic procedure (Table 1). It is also well recognized that re-
(Freeman et al. 2018) (Fig. 1). Various types of evacuation peated and large-volume sampling is undesirable for patients,
tubes can be used based on the risk of contamination and especially for patients with chronic disease who require regu-
coagulation, such as an EDTA pre-filled tube that prevents lar sampling or when maintaining blood volume is critical
clotting (Banfi et al. 2007). Venipuncture is often performed (Chapman et al. 2014). Most microsampling approaches are
on the volar forearm of the patient in the sampling process, less painful and stressful and often have fewer requirements
and a tourniquet can be used to restrict blood flow. Once the on handling and storage. Therefore the benefits of blood
sample is collected in the evacuation tube, it can be delivered microsampling has the potential to increase the patient’s ac-
to a central diagnostic laboratory for analysis under appropri- cessibility to a blood test (Chapman et al. 2014).
ate storage and delivery conditions (Tsai et al. n.d.).
Although the technique can provide accurate diagnosis, it 2.2.1 Dried blood spot
is often considered a costly and time-consuming procedure
due to the consumables, personnel and storage/logistical re- An approach that bridges the gap between small blood sam-
quirements (Freeman et al. 2018). For example, in a central pling and analysis is dried blood spot (DBS). DBS was first
testing laboratory setting, the turnaround time of blood testing developed for large-scale screening of the metabolic disease,
ranges from hours to days depending on the sample/result phenylketonuria, on neonates in 1963 (Guthrie and Susi
delivery between the clinic and the central laboratory 1963). Since then, it has been used for detection of sickle cell
(Cohen et al. 2014; Jones et al. 2007). A central laboratory disorders and human immunodeficiency virus infection
might require more than double the amount of time to process (Parker and Cubitt 1999). The technique involves the use of
a sample as compared to a POC test for some basic blood tests, a blood lancet and a sample collection card. After performing
such as cell count and glucose level analysis (Tsai et al. n.d.). a finger-prick on the patient with the lancet, a few drops of
Another limitation of the conventional approach stems from blood, usually 0.1–1 mL of blood for biomarker
sample quantification and analysis due to technical errors
analysis. Picture retrieved from https://www.butlertech.org/event/ and biological fluctuations, such as hematocrit (Hall et al.
phlebotomy-program-starts/ 2015) (HCT). When spotting a fixed volume of blood sample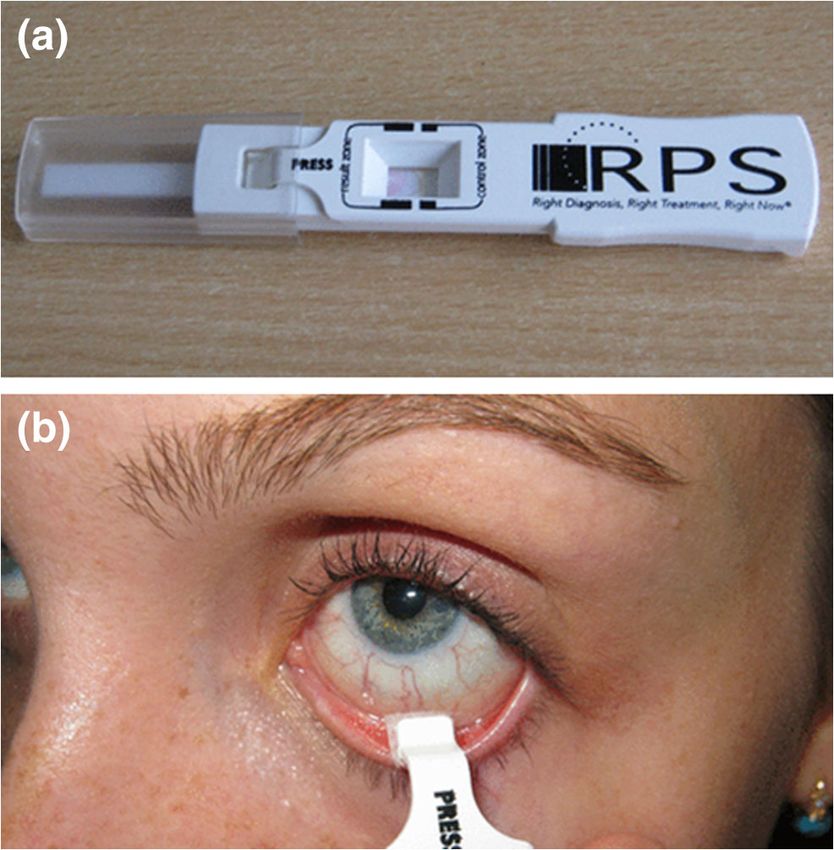
Biomed Microdevices (2019) 21: 81 Page 3 of 30 81
(a) (b)
Specimen sufficient for analysis (minimum 70 μL spots)
Specimen with 40 μL spots
Specimen with 30 μL spots
Specimen insufficient for analysis (less than 30 μL spots)
10 mm
(c) Whatman 903TM Lot: 6940712 W113
Whatman 903TM Lot: 6940712 W113
(d)
QC identification LLOQ Low QC Mid QC High QC
Nominal concentration (µg/mL) 0.50 1.50 20.00 75.00
DBS
Mean (μg/mL) 0.47 1.64 21.13 75.15
% CV (%) 5.3 5.1 2.3 4.2
% Nominal (%) 93.0 109.2 105.6 100.2
PCDBS
Mean (μg/mL) 0.48 1.52 20.89 71.82
% CV (%) 2.8 3.1 1.2 1.0
% Nominal (%) 95.4 101.5 104.4 95.8
Fig. 2 Dried blood spot (DBS) is the most common blood microsampling top sample was 0.35 and the bottom was 0.5. d) Youhnovski et al.
approach. It involves using a collection card to collect a sample of blood compared the precision and accuracy of DBS and PCDBS. PCDBS
via finger-prick. Due to its low sample demand, it is often performed on showed higher precision (%CV) and accuracy (%nominal). Pictures
infants (panel a). b) The volume of blood needs to be standardized in DBS retrieved/adopted from http://www.ewbbu.com/mobile-health.html,
for downstream analysis. Because of the strict requirement on sample Govender et al. 2016, Wilhelm et al. 2014 and Youhnovski et al. 2011.
volume, a technician is usually required to perform the technique. c) All figures are under a Creative Commons Attribution 2.0. Full terms at
The hematocrit (HCT) level can lead to variations in analysis and can http://creativecommons.org/licenses/by/2.0
sometimes be distinguished by the color of sample. The HCT level of the
on the sample collection card, the HCT affects the resultant this technique, the entire spot of collected sample is analyzed to
size of spot (Fig. 2b, c). A high HCT tends to give a smaller minimize the impact of HCT on sample analysis. This method
spot, conversely a low HCT provides a bigger spot. The HCT retains almost all advantages of DBS while overcoming the
effect can introduce variation in analysis, such as the amount impact of HCT. Youhnovski et al. reported using the PCDBS
of analytes in the sample (Hall et al. 2015; Fallah and technique with a 3-mm disk punched out from DBS card for
Peighambardoust 2012). fixed volume blood absorption. Liquid chromatography/
On the other hand, a pre-cut dried blood spot (PCDBS) is a electrospray ionization tandem mass spectrometry was then
variation of DBS that aims to address the HCT issue in DBS. In performed to determine the naproxen concentration in the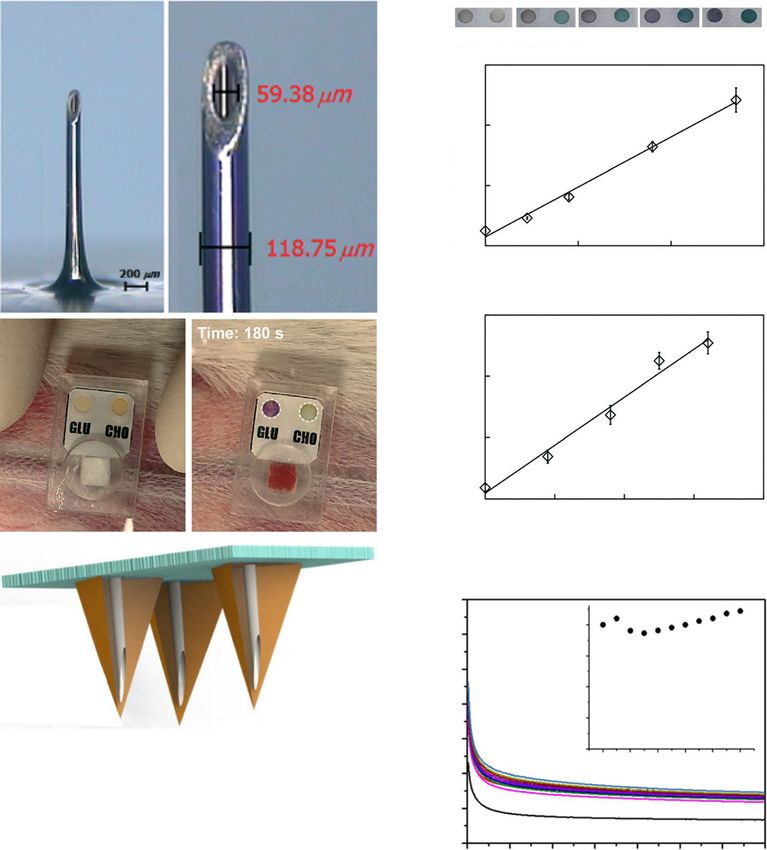
81 Page 4 of 30 Biomed Microdevices (2019) 21: 81
sample. The main objective of PCDBS was to tackle the HCT In this study, the plasma extraction card was used to quan-
effect and drug distribution issue encountered in general DBS tify the amount of Vitamin D in whole blood sample with LC-
(Youhnovski et al. 2011). As compared to the general DBS MS/MS, and the result was compared with the conventional
approach, the PCDBS technique displayed lower variations plasma separation approach of liquid-liquid extraction across
in precision (%CV ≤3.1%) and higher accuracy (%nominal an HCT range of 21% to 70%. The result suggested that the
value: 95.4–104.4%) across the HCT range of 25% to 75%. coefficients of variation were 4.4 for the plasma extraction
Although the PCDBS technique partially overcame the HCT card and 1.8% for liquid-liquid extraction (Fig. 3b). The mea-
impact, the sampling process required a precise and accurate sured values of Vitamin D concentration were also similar
volume of blood, making it unsuitable for self-sampling with- (19.8 ng/mL vs 22.2 ng/mL). This showed that the results of
out extensive training (Fig. 2d). the three-layer plasma collection card and centrifugation were
comparable.
Plasma sampling via the plasma extraction card method has
2.2.2 Plasma microsampling the potential to change the way diagnostic services are per-
formed in resource-poor areas as a result of the reduced need
Plasma microsampling involves collecting a small for specialized laboratory equipment. Although this technique
amount of plasma for quantitative analysis of biomole- can also overcome the HCT effect on the whole blood sample,
cules. A patient is first finger-pricked and < 100 μL of potential widespread adoption for applications could be re-
blood sample is collected into a capillary tube or a stricted due to the limited biological information that the plas-
plastic device (Li et al. 2012). The sample is then cen- ma sample may provide.
trifuged, so the plasma can be isolated and analyzed
directly with techniques such as liquid chromatography 2.2.3 Volumetric absorptive microsampling
- tandem mass spectrometry (Parker et al. 2015a) (LC-
MS/MS). Parker et al. has reported a dried plasma spot Volumetric absorptive microsampling (VAMS) is a novel
(DPS) technique in which a small volume of harvested approach that permits the collection of a fixed volume
plasma sample was spotted onto cellulose cards for sub- of whole blood. The technique involves the use of a
sequent quantitative analysis of fosfomycin with LC- sampler with a porous hydrophilic tip that enables the
MS/MS (Parker et al. 2015a). The results displayed a collection of small, accurate and precise blood volumes
high accuracy (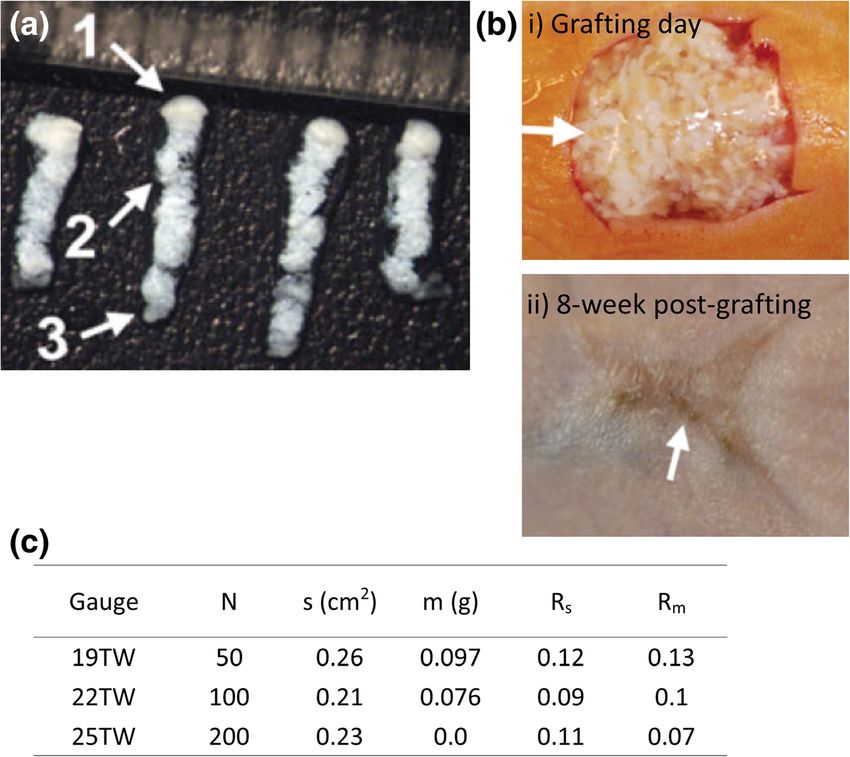
Table 1 Selected publications of current blood and skin microsampling techniques
Sample Technology Target Application Analytical Additional information Potential Sample amount Reference
target model method for
system self-
sampling
Blood Dried blood spot Human Drug detection and LC/ESI-MS/MS - Use of pre-cut filter paper No ~100 μL of whole blood Youhnovski et al. 2011
quantification to overcome hematocrit (HCT)
impact
- Less than ±3% of variations
Biomed Microdevices (2019) 21: 81
in volume
- A precise volume of blood is
necessary
Human Drug detection and LC-MS/MS - Use of conventional filter paper No ~100 μL of whole blood Koster et al. 2013
quantification card
- Presence of HCT impact
Human Virus detection PCR - Use of conventional filter paper No >70 μL of whole blood Govender et al. 2016
card
- Presence of HCT impact
Plasma Human Protein detection and LC-MS/MS - Use of three-layer sample separation Yes 2.5 μL of plasma from Kim et al. 2013
microsampling quantification card 25 μL of whole blood
- Lab setting is not necessary
- Absence of HCT impact, but biological
information is limited
Human Drug detection and LC-MS/MS - Use of centrifugation in plasma separation No 25 μL of plasma Li et al. 2015a, b
quantification - Lab setting is necessary
- Absence of HCT impact, but biological
information is limited
Human Drug detection and LC-MS/MS - Use of centrifugation in plasma separation No 5–30 μL of plasma from Parker et al. 2015a, b
quantification - Lab setting is necessary 2 mL of whole blood
- Absence of HCT impact, but biological
information is limited
VAMS Human Drug detection and LC-MS/MS - Fixed volume sampling Yes 10 μL of whole blood Denniff and Spooner 2014
quantification - HCT impact can potentially be ignored
- Less than ±5% of variations in volume
- Sample collection within 2–4 s
- Convenient sample storage
Human Drug detection and LC-MS/MS - Fixed volume sampling Yes 10 μL of whole blood Mano et al. 2015
quantification - Biased drug levels at low and high HCT
levels
- Sample collection within 2–4 s
- Convenient sample storage
Rat Drug detection and LC–MS/MS - Fixed volume sampling Yes 10 μL of whole blood Kita et al. 2018
quantification - Biased drug levels at low HCT level
- Sample collection within 2–4 s
- Convenient sample storage
hemaPen Human Fixed volume sampling of N/A - Fixed volume sampling Yes N/A https://www.trajanscimed.
whole blood - HCT impact can potentially be ignored com/pages/hemapen
- Absence of clinical data
- Overall collection duration less than 20 s
Page 5 of 30 81
Table 1 (continued)
Sample Technology Target Application Analytical Additional information Potential Sample amount Reference
target model method for
system self-
81 Page 6 of 30
sampling
- Convenient sample storage
Skin/Blood Microneedle Mouse Biomolecule detection ELISA - Use of solid microneedle arrays No N/A Bhargav et al. 2012
and quantification - For disposable use only
- Variations in sample capturing
Mouse Drug level monitoring Electrochemistry - Use of hollow microneedle arrays No N/A Mohan et al. 2017
- For continuous monitoring
- Integrated diagnostic platform
Mouse Biomolecule level Colorimetric - Use of single hollow microneedle Yes 30 μL of whole blood Li et al. 2015a, b
quantification assay - For disposable use only
- Integrated diagnostic platform
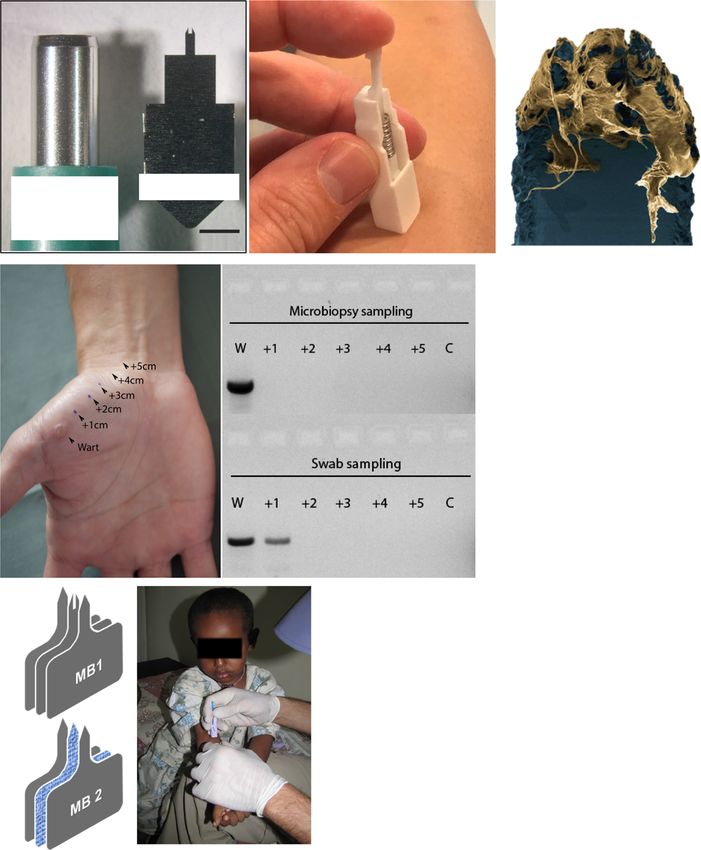
Human Skin sampling qPCR - Use of single hollow microneedle Yes 3–12 μg of skin sample Lin et al. 2013
- For disposable use only
- Low cost and simple design
Mouse Body fluid sampling N/A - Use of absorbent microneedle arrays Yes ~3 μL of body fluid Samant and Prausnitz 2018
- For disposable use only
- Low cost and simple design
- Use of external pressure to improve
yield
Human Virus detection PCR - Use of hollow microneedle arrays Yes 3–12 μg of skin sample Tom et al. 2016
- For disposable use only
- Low cost and simple design
- Spatial and repeated sampling
capabilities
Human Parasite detection PCR - Use of single absorbent microneedle Yes 1.5–3 μL of blood; Kirstein et al. 2017
- For disposable use only unclear for skin.
- Low cost and simple design
- Capability to sample both skin and
blood
Skin Abrasion Human Skin disease diagnosis Bacterial - Use of various culturing conditions No N/A Pachtman et al. 1954
culture to distinguish bacteria
Human Skin disease diagnosis PCR - Inconsistent genotypic results between No N/A Hernandez et al. 2006
physician- and self-collected sampled
Tape stripping Human Protein level quantification BCA - Great inter-individual variances in No 11 μg of protein/cm2 Clausen et al. 2016
protein content
Human Melanoma diagnosis Microarray - Use of 17-gene classifier to distinguish No N/A Wachsman et al. 2011
melanoma
- 100% sensitivity and 88% specificity
(melanomas vs naevi)
Human Melanoma diagnosis qPCR - Use of only 2 genes to distinguish No N/A Gerami et al. 2017
melanoma
- 91% sensitivity and 69% specificity
(melanomas vs naevi)
- Short turnaround time
Swine Skin grafting Not applicable - Use of modified hypodermal needle No 10–100 mg/skin column Tam et al. 2013
Biomed Microdevices (2019) 21: 81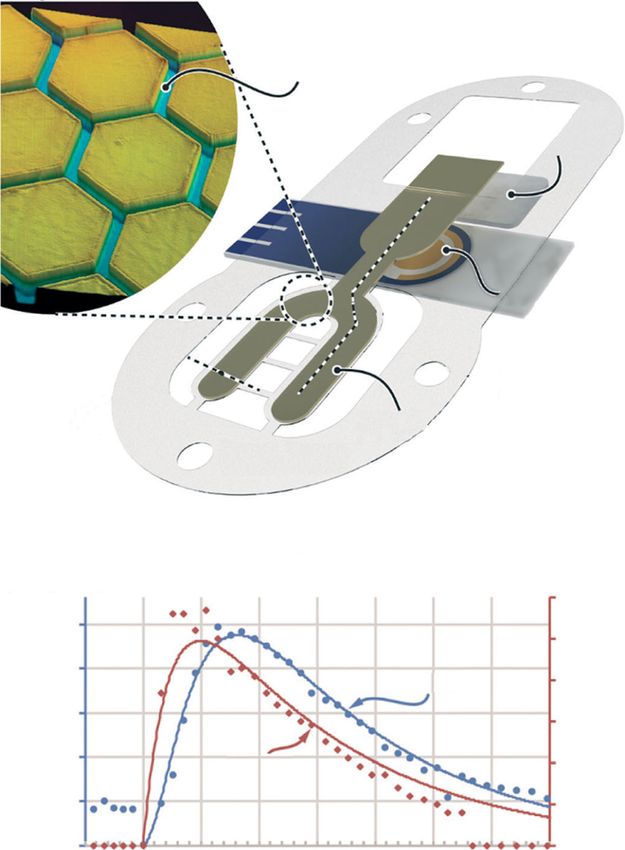
Table 1 (continued)
Sample Technology Target Application Analytical Additional information Potential Sample amount Reference
target model method for
system self-
sampling
Fractional skin - Potential for other applications,
harvesting such as tissue sampling for
histopathological analysis
Other bodily Reverse Human Glucose level Electrochemistry - Inconsistent extraction rate Yes 20–60 nmol/cm2*h Diabetes Research in Children
Biomed Microdevices (2019) 21: 81
fluids iontophoresis monitoring - Unsuitable for real-time monitoring Network (DIRECNET) Study
due to reading delay Group 2003
- Low accuracy when the analyte
concentration
is low
Human Glucose level Electrochemistry - Lower variability as compared to Yes N/A Lipani et al. 2018
monitoring GlucoWatch
- Pixel density needs to align
with follicle density
Nanopore Human Glucose and asparagine Electric signal - Highly sensitive Yes Glucose: 2 μL for sweat Galenkamp et al. 2018
level monitoring - Application can be limited 15 μL for saliva 10 nL
for blood
Oral rinse Human HPV diagnosis PCR - Saliva sampling No N/A Qureishi et al. 2018
- Use of 1 biomarker for HPV
screening
Passive drooling Human Subclinical malaria Immunoassay - Saliva sampling No 2 mL Tao et al. 2019
diagnosis - High sensitivity and specificity
- Low cost
Wearable sweat Human Ethanol level Electrochemistry - Continuous sweat sampling Yes 100 nL/cm2 Hauke et al. 2018
biosensor monitoring - Low cost and simple design
- Suitable for low-resource areas
AdenoPlus Human Adenoviral Immunoassay - Disease-specific tear sampling No N/A Sambursky et al. 2013
conjunctivitis diagnosis - Shot turnaround time
Page 7 of 30 81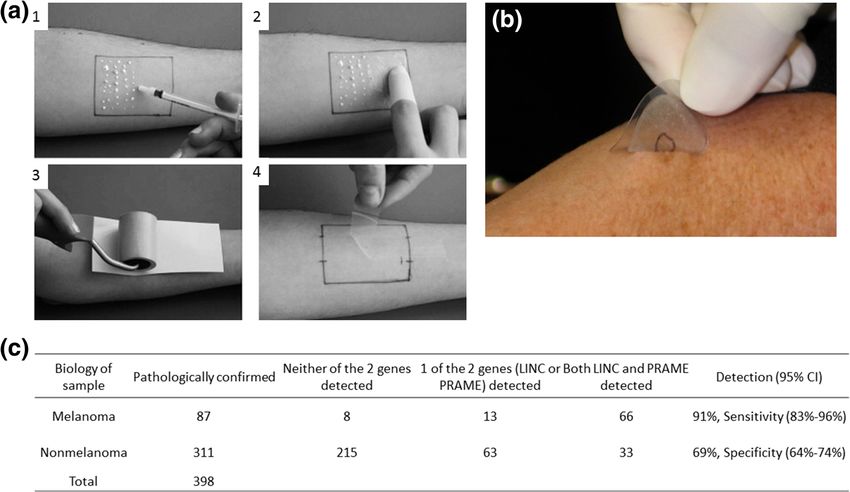
81 Page 8 of 30 Biomed Microdevices (2019) 21: 81
(a)
Control spot Whole blood
application
Overlay
Spreading
layer
Separation
membrane
Plasma collection Plasma
resevoir
Isolation
Base card screen
(b)
Ratio Measured
d6-25OHVD3 Average concentration of % CV of
Donor 1 (2.57 μL of plasma Analyte peak IS peak area (analyte/ 25OHVD3 (ng/
a (pg on Collection Disc) analyte (ng/mL) replicates
from finger-stick) area (counts) (counts) IS) mL)
Plasma extraction card, 5.07 × 1003 2.63 × 1003 1.93 28.0 20.8
replicate 1
Plasma extraction card, 5.00 × 1003 2.74 × 1003 1.82 28.0 19.6
replicate 2
Plasma extraction card, 5.11 × 1003 2.89 × 1003 1.77 28.0 19.1 19.8 4.4
replicate 3
Ratio Measured
Donor 1 (100 μL serum Analyte peak IS peak area (analyte/ d6-25OHVD3 (pg 25OHVD3 (ng/ Average concentration of % CV of
from venipuncture) area (counts) (counts) IS) in a tube) mL) analyte (ng/mL) replicates
LLE, replicate 1 2.83 × 1005 8.83 × 1004 3.20 700 22.2
LLE, replicate 2 2.79 × 1005 8.88 × 1004 3.14 700 21.8
LLE, replicate 3 3.52 × 1005 1.08 × 1005 3.26 700 22.6 22. 1.8
Fig. 3 Plasma microsampling involves sampling whole blood and extraction card and conventional liquid-liquid extraction. Reprinted
separating plasma out for analysis. a) The plasma collection card was (adapted) with permission from Kim et al. 2013. Copyright 2018
designed to separate plasma from whole blood without centrifugation. American Chemical Society
b) The coefficients of variation (%CV) were similar for both the plasma
however, it has also been reported that the analyte recovery volume inaccuracy and HCT effect in DBS (hemaPEN -
varies as the HCT level changes. For example, in two separate Trajan Scientific and Medical n.d.) (Fig. 4c). The device
pharmacokinetic studies, Parker et al. and Mano et al. both contains end-to-end capillaries with pre-punched DBS pa-
suggested that the drug recovery levels of analytes, per for blood collection and dispensing. The purpose of
fosfomycin and tacrolimus, were inversely correlated with the device is to provide an easy and convenient sampling
HCT levels (Parker et al. 2015b; Mano et al. 2015). Both experience. Upon performing a finger-prick, the device
studies examined the analyte recovery at three different HCT uses a capillary collection mechanism to dispense an ac-
levels across the range of 20 to 65%. The recoveries of curate volume of blood onto filter paper. The sample in-
analytes were shown to be higher at a lower HCT level (20– tegrity is ensured at every stage of the process via the
30%) for both analytes. However, the main reason that led to integrated compartments in the device.
this inverse relationship is still unclear. These studies sug- Following sampling, the device can be sent to a diagnostic
gested that challenges remain for analyzing drug concentra- laboratory for analysis. Since the hemaPEN is still under de-
tion with VAMS. Although the technique provides a conve- velopment, the next key step for a device like this is to dem-
nient way to sample an accurate volume of blood, the relation- onstrate the reliability with clinical data. While the feasibility
ship between HCT and analyte needs to be thoroughly inves- and reliability of both VAMS and hemaPEN still require fur-
tigated before it can be used as a routine sampling tool. ther validation, the importance of accurate sampling volume
Similar to VAMS, the hemaPEN (Trajan Medical and and reducing the HCT impact are two of many issues both
Scientific) is a sampling platform that aims to tackle devises are aiming to address.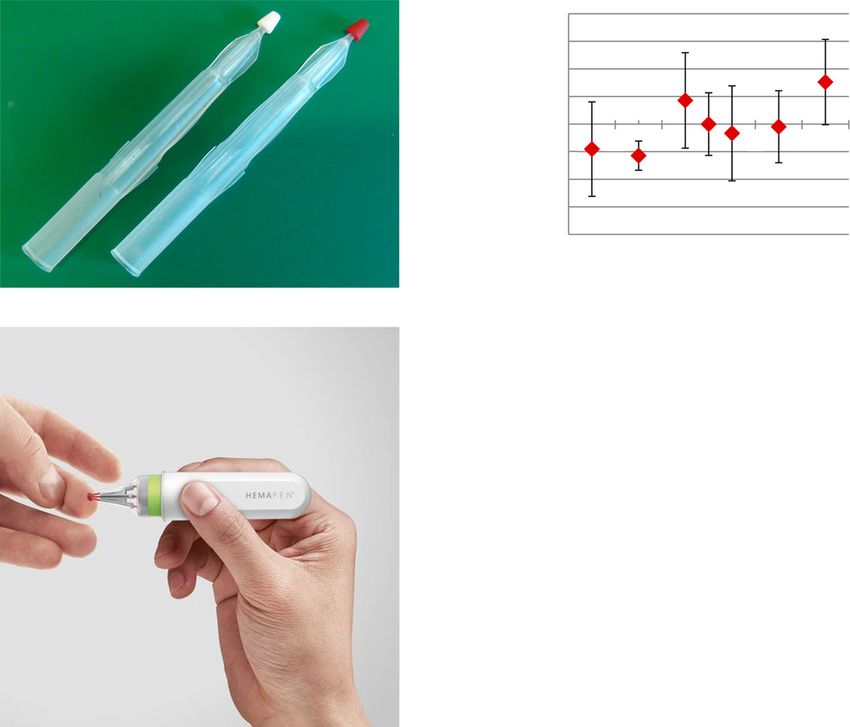
Biomed Microdevices (2019) 21: 81 Page 9 of 30 81
Fig. 4 Blood microsampling with (a) (b)
Volume difference from
volumetric absorptive 8%
microsampling (VAMS) and 6%
hemaPEN are emerging 4%
45% HCT
techniques for facilitating 2%
0%
convenient and accurate
-2%
sampling. a) VAMS sticks before
-4%
(left) and after (right) sampling. b) -6%
Blood sample recovered from -8%
VAMS tip displayed less than 5% 15 25 35 45 55 65 75
volumetric variation when Hematocrit
compared to pipetting across the (c)
HCT range of 20 to 70%. c) The
application of hemaPEN
following finger-prick. Pictures
retrieved from Denniff and
Spooner 2014 and https://www.
trajanscimed.com/pages/hemapen
2.2.4 Microneedle Earlier studies have already demonstrated that the MPA de-
vice was able to penetrate the dermal tissue and capture spe-
Unlike other established techniques, microneedles are capable cific circulating biomarkers when applied to the skin of live
of penetrating the skin and sampling at the same time without mice (Crichton et al. 2010, 2011).
the use of a blood lancet. Early microneedle designs usually In the study, the impact of protein immobilization
possessed a solid body and were primarily designed for cos- conditions on biomarker capturing efficiency was inves-
metic or therapeutic purposes, such as drug delivery Kim et al. tigated, and two groups of MPAs were designed for this
2012). Recent advances in rapid prototyping techniques, for purpose: one group involved the use of 1-Ethyl-3-(3-
example 3D printing and laser cutting, has enabled dimethylaminopropyl) carbodiimide (EDC) and N-
microsampling with microneedles for clinical research pur- hydroxysuccinimide (NHS) in the immobilization proce-
poses (Lin et al. 2013; Samant and Prausnitz 2018). dure of ovalbumin on MPAs, and the other group did
The dimensions and geometries of microneedles can vary not use EDC/NHS. The purpose of the EDC/NHS treat-
and can have an impact on needle penetration and pain. ment was to improve probe surface density and orienta-
Reported microneedle penetration can range from 1 to 2 mm tion. The resulting ovalbumin-immobilized MPA device
(Iriarte et al. 2017; Römgens et al. 2014). The range was was applied on ovalbumin-vaccinated mice to detect α-
sometimes comparable to blood lancet penetration depths, ovalbumin-IgG antibodies 21 days after vaccination.
which usually range between 0.85 mm on newborns to Upon application, an enzyme-linked immunosorbent as-
2.2 mm on adults (Fruhstorfer et al. 1999; Kocher et al. say was performed to determine the capturing efficiency
2009). The penetration depth allows the microneedle to by- of the antibody. The result showed that the EDC/NHS
pass the stratum corneum and sample the biomarkers/ treatment improved the capturing efficiency of ovalbu-
biological fluids directly. min by 18-fold in vivo and 140-fold in vitro (Fig. 5d).
There are three major types of microneedle; solid However, most solid microneedle designs, including
microneedle, hollow microneedle and absorbent microneedle. MPAs, suffered from variations in capturing efficiency
Most solid microneedle designs were primarily created for and were not an ideal technology for sample quantifica-
drug delivery (Jenkins et al. 2012; Crichton et al. 2010), how- tion purposes (Ventrelli et al. 2015).
ever, they can also create micropores on the skin and extract Hollow microneedles have a channel/hollow structure for
fluid/biomarkers through the resulting pores. Bhargav et al. blood extraction (Kim et al. 2012). One benefit of the hollow
reported a silicon chip containing an array of cone-like pro- microneedle is the potential for real-time or automated biomark-
jections called microprojection arrays (MPAs) for selective er monitoring in a minimally invasive manner when paired with
biomarker capturing (Bhargav et al. 2012) (Fig. 5a-c). a wearable device. There are some wearable devices that have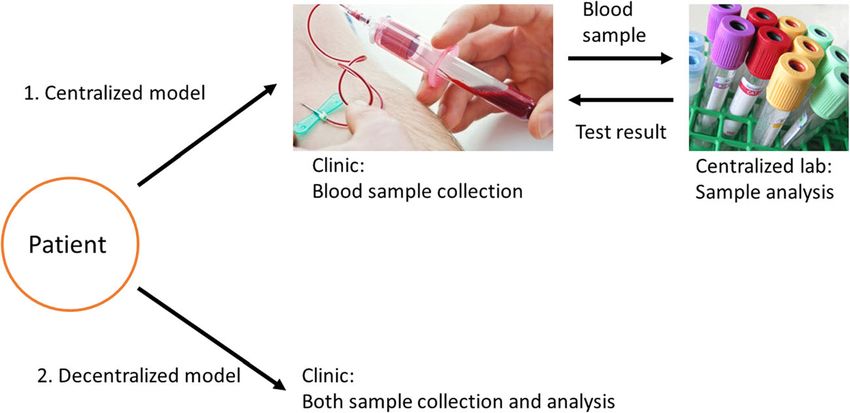
81 Page 10 of 30 Biomed Microdevices (2019) 21: 81
MFI (AF647-OVA)
Fig. 5 Microprojection arrays, a
(a) (d)
solid microneedle-based device, 2000
was used to capture biomarkers in **
the skin of live mice as reported 1500
by Bhargav et al. a-c) The surface
of microprojection arrays imaged 1000 **
with SEM. d) Surface
modifications with EDC/NHS 500
improved the capturing
efficiency. The fluorescence 0
intensities of EDC/NHS-treated (b) (c)
Au
H Au
H Au
MPAs showed an 18-fold
ED P )
S)
S
/N -
/N -
C EG
C EG
increase. Pictures retrieved from
Bhargav et al. 2012
ED P
(+
(-
integrated diagnostic functionality for improved patient experi- Most hollow microneedle designs suffered from some com-
ence (Norman et al. 2014; Li et al. 2015b). In a recent study from mon technical issues, such as channel blockage and needle
Li et al., a single stainless-steel hollow microneedle with an deformation (Kim et al. 2012; Reed et al. 1998). Given these
outer diameter of 120 μm was combined with a paper-based technical challenges, the majority of the current designs have
sensor for glucose and cholesterol concentration measurement only been performed on animals instead of humans. Another
(Li et al. 2015b) (Fig. 6a and b). major limitation is that these designs often require the use of
Once the device was fixed to the skin of a live rabbit, the some advanced fabrication technologies and therefore are not
device could be activated by applying pressure at the back of scalable in most cases (Kim et al. 2018; Lutton et al. 2015).
the microneedle. About 30 ± 5 μL of blood sample could be In contrast, Lin et al. reported an alternative type of hollow
collected by the hollow microneedle on a rabbit model in microneedle, the skin microbiopsy, that was fabricated with
3 min. The separation membrane, an asymmetric polysulfone relatively low-tech equipment, such as a laser cutter, for skin
layer, then transferred the sample through absorption to the reac- sampling (Lin et al. 2013). In the study, the skin microbiopsy
tion zones, which contained colorimetric assays. Color change of was fabricated with three layers of medical-grade steel sheet
the reaction zones indicated the concentration of sample, and the (Fig. 7a, b). The skin microbiopsy penetrated the skin approx-
color change was quantified by image analysis (Fig. 6b). Upon imately 500 μm deep, and the channel in the middle of the
comparing different sample concentrations, the result of intensity microneedle was able to sample tiny pieces of skin tissue like
analysis showed linear correlation coefficients (R2) of 0.99 for a claw (Lin et al. 2013) (Fig. 7c). The puncture site created by
glucose and 0.98 for cholesterol, suggesting a reliable detection the skin microbiopsy only spanned 0.2 ± 0.1 mm wide (Tom
of sample concentration (Fig. 6c). Another advantage of the de- et al. 2016). The minimally invasive nature of the device also
vice was the use of low-cost materials, such as PDMS, which enabled spatial-temporal sampling and facilitated molecular
made the device ideal for disposable use. However, the technique profiling of skin diseases (Tom et al. 2016; Tan et al. 2015).
is still at an early stage and it has only been tested on the skin of a In a separate study in 2016, Tom et al. demonstrated the
rabbit model. detection of spatial presence of human papillomavirus (HPV)
Instead of one single microneedle, a growing number of stud- with a skin microbiopsy by sampling cutaneous warts (Tom
ies has reported using hollow microneedle arrays for real-time et al. 2016). After applying the skin microbiopsy with a
monitoring of biomarkers in blood. In most cases, a patch filled spring-loaded applicator, 1–2 ng of DNA was extracted from
with microneedles was applied to the skin, and blood samples the patient. The DNA gel electrophoresis result suggested that
were continuously extracted through microfluidic channels to the the skin microbiopsy provided a more accurate spatial detection
back of the patch for analysis. Mohan et al. reported a hollow of HPV DNA when compared to the conventional swab sam-
microneedle array coated with alcohol oxidase in the pling approach, which displayed an HPV positive result for a
microcavities (channels) for alcohol concentration detection sample collected from healthy skin 1 cm away from the lesion
(Mohan et al. 2017) (Fig. 6d). Upon enzymatic reaction with (Fig. 7d). Although the skin microbiopsy does not have the
alcohol, platinum and silver wires within the microcavities of ability to draw blood like other hollow microneedles, the device
needles enabled electrochemical signal measurement. The device has been tested on humans and has the potential to facilitate
demonstrated the ability to monitor an alcohol level of 0–80 mM molecular detection of skin diseases in dermatological research.
for 100 min with a relative standard deviation ofBiomed Microdevices (2019) 21: 81 Page 11 of 30 81
Fig. 6 Hollow microneedles were
combined with sensors for real-
(a) (c)
time biomarker monitoring. a)
Gl Ch Gl Ch Gl Ch Gl Ch Gl Ch
The dimension of hollow 1.5
microneedle reported in Li et al.
b) The absorption of blood led to
color change in the reaction 1.0
k/s
zones. The color change was used
to determine the concentrations of 0.5
glucose and cholesterol. c) The
calibration curves for glucose and
cholesterol measured by using the 0.00 100 200 300
one-touch hollow microneedle
device. Both measurements Glucose (mg/dL)
showed linear correlation
0.6
coefficients (0.99 and 0.98). d) (b)
Schematic representation of the
hollow microneedle array from 0.4
Mohan et al. e) Real-time alcohol
k/s
detection of 30 mM alcohol in
artificial interstitial fluid 0.2
(20.1 mg/mL BSA) for 100 min.
The artificial interstitial fluid was
located in a reservoir under a 0.0
piece of excised mouse skin and 0 100 200 300
was sampled by the microneedle Cholesterol (mg/dL)
array after penetrating the skin.
(d)
Pictures retrieved from Li et al. (e)
2015a, b and Mohan et al. 2017 35
100
current, %
Relative
i, nA
15
0
0 t, s 100
0
0 35
t, s
mixture (Kirstein et al. 2017). Instead of simply pulling out reported in animal studies for dermal interstitial fluid sam-
skin tissue with the microneedle, the absorbent microbiopsy pling. Samant et al. reported an absorbent microneedle-based
consisted of an absorbent layer, a layer of filter paper, in the device for interstitial fluid sampling on pig and mouse skin
middle to sample blood (Fig. 7e, f). In the study, the device called microneedle patch(Samant and Prausnitz 2018). The
was used to facilitate the diagnosis of Leishmaniasis, a para- design of the microneedle patch was similar to the absorbent
sitic skin condition. After applying on the lesion sites of pa- microbiopsy described above, with two layers of stainless-
tients, the absorbent microbiopsy collected about 1.5–3 μL of steel cover sandwiching an absorbent paper (Fig. 8a, b).
blood. Patients with histories of Leishmaniasis were sampled However, the microneedle patch contained an array of
by both the absorbent microbiopsy and conventional finger- microneedles, instead of just one single needle. After applying
prick approach for comparison. Quantitative real-time kineto- the patch on the skin, the patch stayed on the skin and a
plast DNA PCR data suggested that the absorbent transverse pressure of 10 lbf was applied around the applica-
microbiopsy was able to collect both blood and skin samples tion site to increase the fluid extraction rate. At the end of the
at the same time and showed a 3-fold increase (101 vs 32 20-min experiment, approximately 3 μL of interstitial fluid
patients) in accuracy in diagnosing Leishmaniasis, including was sampled by the patch (Fig. 8c).
asymptomatic patients (Fig. 7g). Absorbent microneedle-based devices such as the ab-
In addition to the absorbent microbiopsy reported by sorbent microbiopsy and the microneedle patch are pri-
Kirstein et al., absorbent microneedles have also been marily designed for single use. Although the absorbent81 Page 12 of 30 Biomed Microdevices (2019) 21: 81
Fig. 7 Microneedle-based
microbiopsies were used in skin
(a) (b) (c)
and blood microsampling. a) A
side-by-side comparison between
conventional punch biopsy and
the skin microbiopsy. b) The
spring-loaded applicator used in
microbiopsy application. c) After
application, the microneedle
captured pieces of skin tissue in 3 mm Microbiopsy
the channel. d) Spatial detection conventional
of HPV by sampling cutaneous
warts. Skin microbiopsy provided
punch biopsy
2 mm
a more accurate spatial detection
as demonstrated by DNA gel
electrophoresis. e) Designs of
(d)
skin (top) and absorbent Microbiopsy sampling
microbiopsies (bottom). The main
difference between the two W +1 +2 +3 +4 +5 C
designs was the middle absorbent +5cm
+4cm
layer. f) The absorbent +3cm
microbiopsy was used to sample +2cm
patients with Leishmaniasis in +1cm
rural areas. g) The PCR data Wart
suggested the absorbent Swab sampling
microbiopsy was able to detect
Leishmaniasis more accurately W +1 +2 +3 +4 +5 C
than the finger-prick method.
Pictures retrieved from Lin et al.
2013, Tom et al. 2016 and
Kirstein et al. 2017. All figures
are under a Creative Commons (e) (f) (g) FP+ Np. (%) FP+ Np.(%)
Attribution 2.0. Full terms at 1st Study
http://creativecommons.org/ MB+ 22 (12.1) 79(43.6)
licenses/by/2.0
MB- 10 (5.5) 70 (38.7)
2nd Study
MB+ 2 (2.8) 18 (26.0)
MB- 6 (8.6) 43 (62.3)
microneedle does not offer the continuous monitoring 3 Skin sampling
function like the hollow microneedle, the fabrication pro-
cess is usually much simpler, and thus the cost of the 3.1 Conventional and invasive skin sampling
device is much lower comparatively. For the case of the techniques
absorbent microbiopsy, the fabrication process only in-
volved the use of laser cutting and low-cost materials, Another main area of microsampling is skin sampling. In skin
such as filter paper and stainless-steel sheet (Lin et al. sampling, there are a larger variety of functional techniques
2013; Kirstein et al. 2017). Furthermore, the absorbent due to the easier access of samples. Different techniques have
microneedle has the potential to facilitate clinical research their own unique features, and they are often tailored for spe-
by reducing the use of reagents and the use of animals cific disease conditions. Similar to blood, most conventional
when compared to other conventional sampling ap- approaches are invasive and expose patients to potential risk
proaches. Nevertheless, the sampling variation is a huge of complications.
obstacle as there are a variety of factors that might affect The skin biopsy is one of the most essential techniques in
the needle penetration and sample absorption amount, in- dermatology for diagnosis of skin conditions through histo-
cluding skin thickness and microneedle dimension. pathological assessment. In Australia alone, the cost MedicareBiomed Microdevices (2019) 21: 81 Page 13 of 30 81
Fig. 8 The microneedle patch (a)
reported by Samant et al. utilized
absorbent microneedles to sample Stainless steel cover
interstitial fluid from animal
Adhesive
models. a Schematic of the
microneedle patch. b The bottom Absorbent paper
view of the device, showing the
absorbent paper was sandwiched Adhesive
by stainless steel covers. c Stainless steel cover
Extraction of interstitial fluid
from rat skin in vivo. Reproduced
from Samant and Prausnitz 2018
with permission from the Royal
Society of Chemistry (b) 5
Fluid eluted through rat skin over time
upon application of pressure (n=3)
Amount of fluid eluted (μl)
4
3
2
1
0
0 5 10 15 20
Time (min)
spent on 750,000 skin biopsies in 2016 was approximately the removal of the entire suspicious spot, irrespective of the
A$150 M, assuming that the minimum cost of skin biopsy size, which prevents any follow-up treatments or diagnosis.
and laboratory evaluation combined was A$200 per procedure Another conventional technique of skin sampling is suction
(Skin cancer - Cancer Council Australia n.d.; Biopsy by a blistering which involves using a chamber with a vacuum
Dermatologist for moles and skin cancer n.d.). The procedure pump to extract body fluid for diagnosis of skin conditions.
involves the removal of suspicious skin lesions followed by The extracted sample can be used to identify and quantify
examination under the microscope. There are three major biomarkers. The fluid obtained with this technique is largely
types of skin biopsies; punch biopsy, shave biopsy and exci- derived from interstitial fluid, which is the place where many
sional biopsy (Alguire and Mathes 1998) (Fig. 9a). All three important biomarkers are expected to be found. Suction blis-
types of biopsies are highly invasive and can cause discomfort tering is much less invasive than a skin biopsy and can be used
to patients. to detect drugs and several skin conditions such as epidermal
For instance, in punch biopsy, a doctor uses a sharp and necrolysis (Paquet et al. 1998), and scleroderma (Juhlin et al.
circular tool for cutting into the top layer of fat beneath the 1986). However, the technique requires time (>2 h) for the
skin (epidermis, dermis and superficial fat) and removing the blistering process and may alter the biomarker structure dur-
suspicious site for examination. Due to the invasive nature of ing the procedure.
the technique, a suture is often needed to close the wound. The
procedure needs to be performed by trained personnel, such as 3.2 Skin microsampling
dermatologists. A skin punch biopsy procedure typically takes
about 15 min in total. The sample may need to be sent off to a 3.2.1 Abrasion techniques
laboratory for analysis depending on the subsequent tests
involved. Skin microsampling has advanced tremendously in recent
Although a skin punch biopsy combined with histopatho- years due to the lower sample demand. Some of these “new”
logical study is the gold standard for diagnosis of skin lesions, minimally invasive techniques are in fact modifications from
the procedure requires local anesthesia and sutures, and gen- their predecessors, such as the abrasion technique. As one of
erally does not permit molecular analysis due to the use of the earliest minimally invasive skin sampling techniques, the
formalin (Gerami et al. 2017). The procedure also requires abrasion technique was first reported by Pachtman et al. in81 Page 14 of 30 Biomed Microdevices (2019) 21: 81
(a)
Shave biopsy
(b) Punch biopsy
Skin Lesion
Fat
Lesion
Lesion
removed
(c) Excision biopsy
Incision
Margin
Lesion
Fig. 9 Skin biopsy is the current standard for skin conditions diagnosis. removing the suspicious location for analysis by a trained medical
The three main types of skin biopsies are shave (a), punch (b), and professional. Pictures adopted from https://www.mayoclinic.org/tests-
excision (c) biopsy. All three types of skin biopsies are conducted bu a procedures/skin-biopsy/about/pac-20384634 & https://myhealth.alberta.
trained medical professional and the biopsy is sent for dermatopathology ca/Health/pages/conditions.aspx?hwid=hw234496
diagnosis in most cases. b The procedure for punch biopsy involvesBiomed Microdevices (2019) 21: 81 Page 15 of 30 81 1954. The team utilized a wood scraper with a diameter of address a larger population. One representative example is 23 mm to scrape the skin for sample collection from patients the non-invasive skin biopsy tape from DermTech with Seborrheic dermatitis, an inflammatory disease, for col- (Wachsman et al. 2011) (Fig. 10b). The technology is based ony counts (Pachtman et al.1954). The suspicious location of on tape-stripping and is designed for the diagnosis of deadly infection was abraded for >20 times before the sample was melanoma. Conventional approaches for melanoma diagnosis subsequently transferred for culturing and colony counting. include the use of 4–6 mm diameter punch biopsy or a deep The study utilized alkaline and aerobic/anaerobic environment shave biopsy, and the technique is highly invasive. In contrast, to control the culturing conditions in order to identify different DermTech’s adhesive tape biopsy permits minimally invasive types of bacteria. Although the study was unable to find a sampling of cells from the surface of a patient’s skin. After connection between the presence of Seborrheic dermatitis sampling, the tape can be stored and sent to DermTech’s lab- and number/type of bacteria on the culture plate, the sampling oratory for analysis. RNA extracted from the sample can be methodology was adopted by the main stream specifically in analyzed for the 17 genes that form the genetic signature for clinical research settings Pachtman et al. 1954). melanoma. The approximate turnaround time from sampling After Pachtman’s study, there had been a number of to result delivery to the doctor/clinic is three days (Ferris et al. modified abrasion techniques for different purposes re- 2015). ported, including pathological studies and environmental Out of the 17-gene classifiers that separate melanoma and toxin studies (Coman et al. 2014; Weldon and Du Preez non-melanoma, LINC0518 (Long Intergenic Non-Protein 2006). However, most of these studies suffered from var- Coding RNA 518) and PRAME (preferentially expressed antigen iations in analysis. For instance, Hernandez et al. demon- in melanoma) were one of the best performing gene pairs in strated that samples collected via the abrasion technique identifying melanoma (Gerami et al. 2017). Gerami et al. report- by patient and physician showed inconsistent genotypic ed using the pair of target genes combined with DermTech’s results (Hernandez et al. 2006). In the study, patients ei- adhesive tape biopsy to distinguish melanoma from non- ther self-sampled or were sampled by a physician for the melanoma samples. The study was designed with 157 training detection of genital HPV via the abrasion technique, and sets and 398 validation sets of adhesive tape biopsy. After non- the results were compared between the two groups. In the invasive sampling with the adhesive tape biopsy, the lesions were study, the collected samples were tested with PCR to de- sampled with conventional biopsy for comparison with the val- tect the presence of HPV DNA. The PCR results from the idation sets of adhesive tape biopsy. Out of the 398 validation two groups showed
81 Page 16 of 30 Biomed Microdevices (2019) 21: 81
Fig. 10 Tape stripping is a non-invasive technique for skin sampling. a technician at a clinic, and the tape was sent to a laboratory for analysis.
The typical procedure of conventional tape stripping. 1) The penetration c Performance of LINC00518 and/or PRAME preferentially expressed
formulation was applied on the surface of the skin. 2) The formulation antigen in melanoma detection in the validation sets suggested a 91%
was spread across the sampling area. 3 & 4) The tape was applied and sensitivity and 69% specificity. Both numbers were higher than using a
subsequently removed for downstream analysis. b The tape stripping dermoscopy alone. Pictures retrieved from Lademann et al. 2009 and
biopsy kit from DermTech. The technique was performed by a Gerami et al. 2017
91% and a specificity of 69% (Fig. 10c). Both sensitivity and negative pressure, and the sample is transferred to a collection
specificity were higher than dermoscopy (Ferris et al. 2015). basket for subsequent skin grafting. The purpose of the device
Although DermTech’s adhesive tape biopsy needs to be was to harvest and transfer hundreds of microscopic skin tissue
performed by medical professionals, the training requirement columns directly into a skin wound.
is much lower than conventional biopsies due to its ease-of- In a later study, the device was tested on human skin for
use and non-invasive nature, making melanoma diagnostics sample collection (Tam et al. 2017) (donor). The collected
more accessible to the public. In addition, the technique al- skin columns (Fig. 11a) were grafted on the dorsal skin of a
lows for repeated diagnosis and simpler disease progression mouse (recipient). The healing responses of both donor site
monitoring. These advantages are ideal for melanoma man- and recipient site were observed over time. After grafting, the
agement as melanoma in some instances can be curable if donor site healed by tissue remodeling without scarring as the
detected and treated early without going through any removal wound sites were much smaller than the conventional split-
procedure(Gerami et al. 2017). thickness skin graft technique. However, the FSH technique
led to inferior cosmetic outcome on the recipient as the skin
3.2.3 Fractional skin harvesting wound healed resembling a ‘fishing net’ (Fig. 11b panel i &
ii). The sample size of FSH was also compared with the con-
There are also skin microsampling techniques that are designed ventional approach (Fig. 11c). Depending on the choice of
for medical purposes other than diagnosis. A recent study from needle, FSH was able to sample about 10–100 mg of skin
Tam et al. reported a needle-based technique called fractional sample with similar penetration as split-thickness skin graft
skin harvesting (FSH) for skin grafting (Franco et al. 2014). while preserving the sample structure and viability. Both sur-
FSH consists of two main parts: a standard hypodermal needle face areas and masses of FSH samples were at least 8-fold
for harvesting and a fluidic device for sample collection. The smaller than split-thickness skin graft samples. This demon-
harvesting needle is produced by honing a standard needle to strated the lower level of invasiveness of FSH. The FSH tech-
fabricate two cutting edges. Once the needle is inserted into the nique also has other potential applications, such as tissue sam-
skin, a column of microscopic skin tissue can be extracted. A pling for histopathological analysis or tissue removal for drug
fluidic device attached to the other end of the needle is then delivery through the fractional channels (Franco et al. 2014;
utilized to remove the sample from the harvesting needle with Tam et al. 2013).Biomed Microdevices (2019) 21: 81 Page 17 of 30 81
Fig. 11 Fractional skin harvesting (FSH) was designed for skin grafting. thickness wound on the dorsal skin of a mouse; arrow highlights the
a Full-thickness skin columns harvested with a 19-gauge coring needle epidermal head of one skin column. ii) The recipient site formed a
from the donor. (Cohen et al. 2014) Epidermis; (Graber et al. 2017) ‘fishing net’ in the middle (arrow) after recovery. c The FSH resulted in
dermis including adnexal structures; (Global Point Of Care Diagnostics samples with smaller surface area and mass than conventional split-
Market will reach USD 40.50 Billion by 2022: Zion Market Research thickness skin graft. Rσ = surface area ratio; Rm = mass ratio. Pictures
n.d.) subcutaneous fat. Each mark on the ruler in the photograph spans retrieved/adopted from Tam et al. 2017. All figures are under a Creative
1 mm. b The recipient site i) before and ii) after the 8-week recovery time. Commons Attribution 2.0. Full terms at http://creativecommons.org/
i) Human skin columns were applied in random orientation to a full- licenses/by/2.0
4 Sampling of other bodily fluids and other patch is transmitted wirelessly to a separate watch-like device
technologies that delivers the glucose level reading (Ackerman et al. 1999).
Several major problems exist with the device, including time
4.1 Reverse iontophoresis delay and disruption by sweating (Diabetes Research in Children
Network (DIRECNET) study group, T. D. R. in C. N. (DirecNet)
Reverse iontophoresis utilizes an electric current to remove mol- S, 2003). In a report from Diabetes Research in Children
ecules and interstitial fluid through the skin for analysis Network (DirecNet) Study Group, the functionality and reliabil-
(Fig. 12a). The technique involves applying a low-level electrical ity of GlucoWatch were examined (Diabetes Research in
current, which increases the permeability of the skin. As a result, Children Network (DIRECNET) study group, T. D. R. in C. N.
molecules are transported across the stratum corneum by electro- (DirecNet) S 2003). On one hand, 60% of the sensor glucose
phoresis and electro-osmosis. The transport of molecules is usu- values were within 20% of the serum glucose, suggesting an
ally measured in units of chemical flux. The technique was first acceptable level of accuracy (data not shown). On the other hand,
described by Glikfeld et al. for extracting glucose, theophylline the measurement was less accurate at low glucose level. As
and clonidine (Glikfeld et al. 1989). It was later combined with a shown in Fig. 12c, for a glucose level lower than 70 mg/dL, only
glucose sensor in a real-time monitoring device called 32% of the readings met the International Organization for
GlucoWatch Biographer (Ackerman et al. 1999) (Cygnus, Inc., Standardization (ISO) criteria (Diabetes Research in Children
Fig. 12b). Network (DIRECNET) study group, T. D. R. in C. N.
GlucoWatch is a wearable and non-invasive glucose mon- (DirecNet) S 2003) (±20%). This indicated that the device might
itoring device that tracks the glucose level in adults. The de- only be sufficient for identifying the trends of glucose level in
vice requires the user to apply a plastic patch on the skin for hyperglycemia patients unless a highly sensitive analytical meth-
periodic sample collection through reverse iontophoresis. od is used, which is usually difficult to achieve on a wearable
Upon sample extraction, the electrochemical signal from the device.81 Page 18 of 30 Biomed Microdevices (2019) 21: 81
Fig. 12 Reverse iontophoresis (a) Reverse iontophoresis
was utilized in glucose Constant current source
monitoring. a In reverse
iontophoresis, an electrical
current is applied on skin to
electro-osmotically drive
Cathode Electrolyte Anode
interstitial fluid, which usually
contains targeting analytes,
through the epidermis to the skin
surface for analysis or sample
collection. b The GlucoWatch Na+
was one of the reversion
iontophoresis-based diagnostic
Cl-
platforms for glucose level
monitoring. The device was
separated into two pieces, a watch
Net convective solvent flow
(panel i) and an electrode
assembly (panel ii). c
GlucoWatch model GW2B (b) GlucoWatch
accuracy test across a range of
glucose concentrations. The
medium relative absolute
difference (RAD) value at the
Working electrode
lowest glucose concentration
(≤70 mg/dL) was the highest Counter/Iontophoresis
among all testing concentrations. electrode
Only 32% of the data collected
met the ISO criteria (±20%).
Pictures retrieved/adopted from Reference electrode
Potts et al. 2002 and the Diabetes
Research in Children Network
(DirecNet) Study Group (b) GlucoWatch accuracy test
Number of paired RAD ISO criteria
data points (median) met (%)
Serum glucose
level (mg/dL)
≤70 334 38% 32%
71-120 926 18% 55%
121-180 963 14% 66%
181-240 776 14% 66%
>240 673 13% 67%
Hypoglycemia test 482 20% 52%
Hyperglycemia test 417 15% 66%
Another major disadvantage of GlucoWatch is the calibra- volumes of the pixels, sensors could operate on an individual
tion procedure. A drop of finger-prick blood was required for hair follicle. The dilution factor of the extracted glucose was
regular calibration due to the variations caused by large sam- constant. Therefore, the inter- and intra-skin variabilities were
pling area (>3cm2 and sample dilution (Sieg et al. 2004). reduced without the use of blood.
Lipani et al. reported an alternative reverse iontophoresis- Figure 13b illustrated a 2 × 2 array strapped to the vol-
based glucose monitoring platform without the need for reg- unteer’s forearm. An in vivo experiment was performed on
ular blood calibration (Lipani et al. 2018). The device two healthy volunteers for comparing the glucose level
consisted of hydrogel, electrochemical glucose sensor and tracking ability of the array with a commercial glucose
miniaturized electrodes (Fig. 13a). The platform exploited meter. The experiment monitored the glucose level over
the fact that most of the electroosmotic flow during the reverse the course of 6-h, which included lunch and snack periods.
iontophoresis process follows low-resistance pathways asso- The interstitial fluid glucose profile collected with the ar-
ciated with hair follicles. Using the graphene-based pixel ar- ray closely followed that of the blood glucose data obtain-
rays in the design, the interstitial fluid was extracted along the ed with the glucose meter (Fig. 13c). There was also an
hair follicle pathway into a separate, small-volume pixel. The expected 15-min lagging time. This suggested the ap-
subsequent reaction with glucose oxidase was detected in the proach was able to effectively track the glucose level
pixel by electrochemical sensors. By fixing the area and through interstitial fluid without any calibration.Biomed Microdevices (2019) 21: 81 Page 19 of 30 81
Fig. 13 The use of follicular (a) Folicular pathway sampling
pathway in bodily fluid sampling
provided a calibration-free Graphene sensors
glucose monitoring platform. a
Schematic illustration of the
Transducer
glucose preferential pathway (hair
follicles). b A screen-printed Hydrogel
array fixed onto a volunteer’s Stratum corneum
forearm. The array was connected
to a potentiostat. c The platform Epidermis
enabled good tracking of the
blood glucose as compared to
Hair Dermis
commercial platform. Pictures
retrieved from Lipani et al. 2018
follicle
Subcutaneous
Blood vessel l (hypodermis)
Hair follicle Intercellular Transcellular
pathway pathway pathway
(b) 2x2 folicular sampling array
(c) Glucose profile
Extracted, pixel A Blood 18
32 Extracted, pixel B
16
28
Blood glucose (mM)
14
Current (nA)
24 12
10
20 Snack
8
Lunch
16 6
In vivo 4
12
0 50 100 150 200 250
Time (min)81 Page 20 of 30 Biomed Microdevices (2019) 21: 81
The technique provides a more user-friendly experience when In a recent study, Galenkamp et al. reported using
compared to GlucoWatch. One main future challenge for the nanopores to detect glucose and asparagine on a real-time
platform is to ensure each pixel only interrogates one follicle. basis (Galenkamp et al. 2018) (Fig. 14a). The study utilized
When there is more than one follicle per pixel, it may lead to specific metabolite-binding proteins, glucose-binding protein
the variability issue observed in GlucoWatch (Sieg et al. 2004). and a substrate-binding domain that recognizes asparagine,
This can potentially be achieved by adjusting the array density. within the nanopore cavity for binding glucose and aspara-
However, it is crucial to keep in mind that the follicle density gine, respectively. The glucose data was compared with the
varies depending on individuals (Sinclair et al. 2005). The array commercial glucose meter data, and the asparagine data was
density may need to be adjusted accordingly. compared with the HPLC data.
The measurement of glucose concentration with nanopores
was similar to the commercial glucose meter, with less than
4.2 Nanopores 5% of difference across most biological samples (sweat, urine
and blood samples; Fig. 14b). For the case of asparagine, the
Most electronic POC biosensors rely on the oxidation of a measurement with nanopores was not as close to its
target biomarker to generate an electric signal (Bayley benchmarking technique HPLC. However, it was crucial to
2015). However, oxidase enzymes may not be readily avail- note that the nanopore approach was more sensitive than
able for some analytes. Nanopore is an emerging technology HPLC and was able to detect an asparagine concentration of
that can address the problem. These pores are nanometer-sized 1.36 ± 0.22μM in saliva sample.
water conduits spanning biological or artificial membranes The nanopore technique is highly sensitive due to its
(Bayley 2015). The technology also involves the use of single-molecule nature of the sensor. Another recent study
analyte-binding protein. The binding of analyte causes a utilized the sensitivity of nanopore and combined the tech-
change in conformation and a current passing through the nique with artificial intelligence for detecting the electrical
nanopores. When an electronic sensor is attached to the signature of virions and facilitate influenza detection(Arima
nanopore membrane, biological signals are converted into et al. 2018). One of the biggest weaknesses of this technique is
electrical signals for the direct quantification of analytes. the need for identifying the appropriate binding proteins for
(a) Nanopore glucose sensor
Ionic current
Current (pA)
Nanopore –80
Glucose binding protein
Open + Glucose Closed IB
cis
A IO
–140
– Glucose 20 s
trans
Lipid bilayer
(b) Methods comparison
Glucose Asparagine
Nanopore
Sampled Commercial Nanopore Sampled LC assay
volume assay volume
Sweat 105±9 μM 2 μL 105±7 μM 94.6±5.0 μM 5 μL 90.9±4.1 μM
Urine 368±7.5 μM 200 nL 381±6 μM 35.4±2.8 μM 4 μL 89.7±3.6 μM
Saliva 5.71±0.48 μM 15 μL 10.4±7.9 μM 1.36±0.22 μM 30 μL ND
Blood sample 1 5.09±0.88 mM 10 nL 5.3 mM 10.2±0.20 μM 5-15 μL 6.7±0.2 μM
Blood sample 2 4.91 mM 10 nL 4.9 mM
Blood sample 3 4.21 mM 10 nL 4.4 mM
Fig. 14 Nanopore biosensor for detecting analytes in bodily fluids. a glucose meter in general. The asparagine measurement was less similar to
Schematic illustration of the nanopore technique. The binding of the benchmarking technique HPLC but demonstrated a higher sensitivity
analyte (glucose in this case) caused conformational change. The in saliva sample. Pictures retrieved from Galenkamp et al. 2018. All
passing of proteins through the nanopore led to a change in current. b figures are under a Creative Commons Attribution 4.0. Full terms at
The glucose quantification with nanopore was similar to the commercial http://creativecommons.org/licenses/by/4.0You can also read