A Renaissance in Moder n and Future Endovascular Stroke Care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
A Re n a i s s a n c e in M o d e r n
a n d Fu t u re En d o v a s c u l a r
S t rok e C a re
Devi P. Patra, MD, MCh, MRCSEda,b,c,
Bart M. Demaerschalk, MD, MSc, FRCP(C)d, Brian W. Chong, MDe,
Chandan Krishna, MDa,b,c, Bernard R. Bendok, MD, MSCIa,b,c,e,f,*
KEYWORDS
Mechanical thrombectomy Stroke Endovascular Stentriever
KEY POINTS
Reducing the time between the stroke symptom onset to intervention is the key to reduce irrevers-
ible brain damage.
Telestroke with integration of AI, Mobile stroke units, Neuro ED, Direct patient transfer to angio suite
are some of the important concepts that are being evaluated to optimize the stroke management
workflow.
Use of perfusion studies are helpful to assess the extent of salvageable brain tissue that might
benefit from reperfusion therapy in patient presenting beyond 6 hours of symptom onset.
Significant advancements in aspiration catheter and stent retriever designs have allowed a faster
and safer reperfusion after mechanical thrombectomy.
Telerobotics is a revolutionary concept with a possibility of mechanic thrombectomy at remote
locations using endovascular robot.
INTRODUCTION medical management in patients presenting early
with large vessel occlusion. These findings have
Stroke intervention with the intention to cure is a rela- resulted in a paradigm shift in acute stroke manage-
tively new concept. Despite the fact that the history ment protocols and paved the way for other clinical
of medicine has spanned many centuries, stroke trials to further refine the standard of care. Although
was considered to be an irreversible pathologic pro- a detailed description is beyond the scope of this
cess until about 3 decades ago, when systemic article, current advancements and breakthrough
thrombolysis showed promising evidence of clot concepts in the endovascular management of
lysis and reversal of neurologic deficits. However, acute ischemic stroke are summarized later in
no incremental progress was made until the early discussion.
twenty-first century when advancement in endovas-
cular access made mechanical thrombectomy (MT)
possible. Despite that, the benefits of MT were not Acute Triage and Transfer to Angiosuite
fully realized until 2015, when 5 landmark random-
Telestroke
ized trials consistently proved that MT significantly
The use of telemedicine in stroke care (Tele-
improves clinical outcome as compared with best
stroke) is a revolutionary concept that allows
neurosurgery.theclinics.com
Conflict of Interest: None.
a
Department of Neurological Surgery, Mayo Clinic, 5777 East Mayo Blvd, Phoenix, AZ 85054, USA; b Precision
Neuro-therapeutics Innovation Lab, Mayo Clinic, Phoenix, AZ, USA; c Neurosurgery Simulation and Innovation
Lab, Mayo Clinic, Phoenix, AZ, USA; d Department of Neurology, Mayo Clinic, 5777 East Mayo Blvd, Phoenix,
AZ 85054, USA; e Department of Radiology, Mayo Clinic, 5777 East Mayo Blvd, Phoenix, AZ 85054, USA;
f
Department of Otolaryngology, Mayo Clinic, Phoenix, AZ, USA
* Corresponding author. Department of Neurosurgery, 5777 E Mayo Blvd, Phoenix, AZ 85054.
E-mail address: bendok.bernard@mayo.edu
Neurosurg Clin N Am 33 (2022) 169–183
https://doi.org/10.1016/j.nec.2021.12.001
1042-3680/22/ÓDescargado
2021 Elsevier Inc. AllMedica
para Biblioteca rightsHospital
reserved.
México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.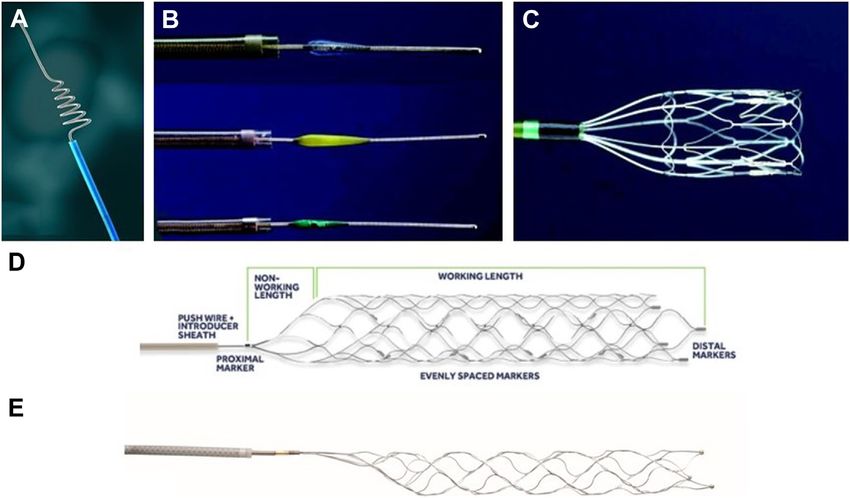
170 Patra et al
high-quality care by health care professionals in Direct transfer to angiosuite
relatively underserved areas guided by a stroke The workflow in stroke care is driven by a common
specialist at remote hospitals through web- theme which is “Time is Brain.” Timely reperfusion
based audiovisual interactions.1 The use of of the brain is an important factor associated with
telestroke has increased by almost 30% of US optimal outcome. In a retrospective study on 6756
hospitals now capable of telestroke. There is a patients, Jahan and colleagues, showed a
higher likelihood of successful reperfusion ther- nonlinear relationship between onset to puncture
apy and lower 30-day mortality in patients with time and outcome at discharge with a steeper
ischemic stroke who are treated in a hospital slope between 30 and 270 minutes as compared
with telestroke capacity.2 The rationale of tele- with more than 270 minutes.9 In the 30 to 270 mi-
stroke is to rapidly identify the patients who would nutes time window, with every 15-min increments
benefit from reperfusion therapy by timely inter- of faster intervention there was higher likelihood of
preting the computed tomogram (CT) or magnetic independent ambulation at discharge. A faster
resonance imaging (MRI) scans by a stroke endovascular treatment has also been shown to
expert over a teleconference. In this regard, be associated with higher rate of successful reper-
recent advancements have been made to use fusion. The individual patient data meta-analysis of
artificial intelligence (AI) in image processing the HERMES group which combined the data of 7
and interpretation through a deep machine randomized trials, showed a relative reduction of
learning algorithm. This allows rapid identification successful reperfusion (TICI 2 b/3) by 22% with
of stroke mimics (intracranial hemorrhage, mass every hour of delay in groin puncture since admis-
lesions), calculation of Alberta Stroke Program sion.10 Therefore, a significant effort has been
Early CT score (ASPECTS), and interpretation of made to reduce the time of transfer from arrival
perfusion imaging. AI has particularly been found to ED to the angiosuite with the development of
to be more accurate than human readers in dedicated stroke bay and strict institutional pol-
detecting ischemic changes in patients present- icies. A direct transfer to angiosuite (DTAS)
ing early (between 1 and 4 hours of stroke onset).3 method has been evaluated for eligible patients
Integration of AI technology in telestroke has a with suspected LVO within 6 hours of symptom
huge potential in improving patient outcome by onset to bypass the delay from initial CT/MR. Pa-
shortening the time delay in instituting IV throm- tients received a cone-beam CT in the angiosuite
bolysis and coordinating inter-facility transfer in before angiogram to rule out hemorrhage. The me-
patients eligible for MT. dian door to groin time was significantly lower in
Mobile stroke units (MSU) bring emergency patients with DTAS as compared with standard
hospital-grade diagnosis and treatment to the pa- workflow patients (16 vs 70 minutes) with a higher
tient instead of the patient to the hospital with rate of favorable clinical outcome in the former
diagnostic capabilities such as point-of-care labo- group at 90 days (41% vs 28%).11 More recently,
ratory tests, computed tomography (CT) scanning, a multicenter trial has been designed, WE-
telemedicine capability, ride-along stroke pro- TRUST trial (workflow optimization to reduce
viders, and telemedicine with the ability to rapidly time to endovascular reperfusion for ultrafast
deliver thrombolytic therapy.4 MSUs have been stroke treatment, NCT04701684) to further eval-
demonstrated to be safe and effective at reducing uate the DTAS approach.
time to thrombolysis and reducing times to therapy
(decision-to treat).5,6 With the chance to confirm Role of tissue plasminogen activator (tPA) in
the diagnosis of stroke in the field, distinguish be- Large vessel occlusion (LVO)
tween hemorrhagic and ischemic stroke, and The use of intravenous thrombolysis (bridging
screen for more severe strokes requiring a supe- therapy) along with MT has been used as the stan-
rior level of stroke care, MSUs can assist with dard therapy in patients with suspected LVO pre-
determining whether direct transport to a compre- senting within 4.5-h window. This approach has
hensive stroke center or thrombectomy capable now been challenged considering the effective
center is best for the patient. With the high and rapid reperfusion achieved with MT alone.
cost and limited numbers of MSUs, alternative op- The individual patient data meta-analysis of the
tions of including telemedicine-capable remote HERMES study showed no difference in functional
ambulance-based NIHSS assessment is feasible independence with bridging therapy versus MT
and has the potential to decrease door-to-needle alone.12 The SKIP trial from Japan was the initial
times by prehospital assessment.7 Prospective randomized trial that evaluated the concept and
trial evidence demonstrates MSUs are capable of failed to demonstrate the noninferiority of MT
reducing stroke-related disability compared with alone compared with standard bridging therapy.13
standard EMS care.8 However, 2 subsequent trials (Direct MT and DEVT
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.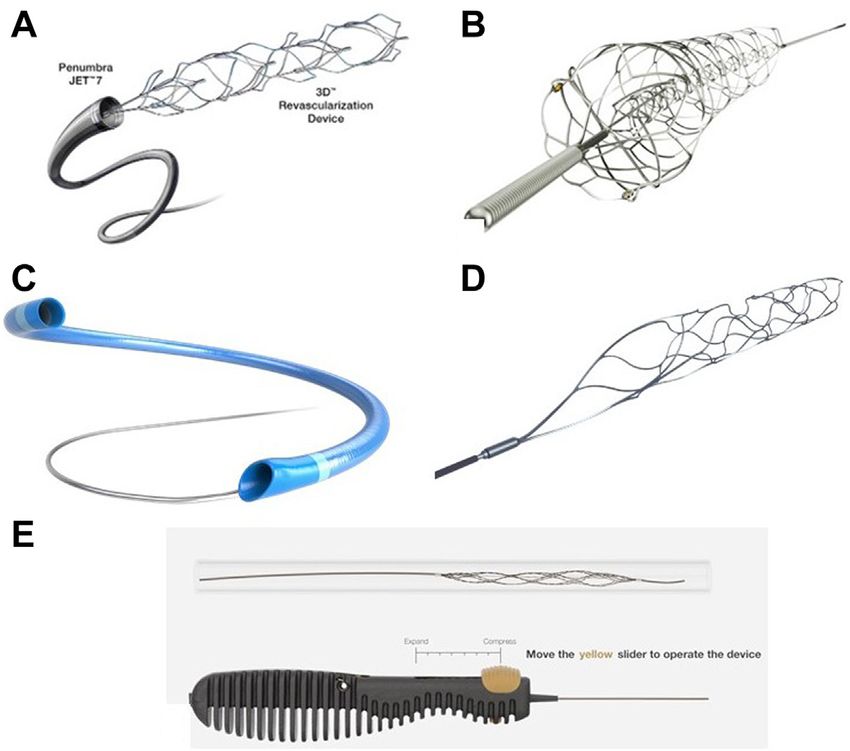
Modern and Future Endovascular Stroke Care 171
trial) being conducted in China could prove the this to be evident in FLAIR sequences. Therefore,
noninferiority of MT alone.14,15 There are now 4 DWI-FLAIR mismatch has been used as a marker
other trials in progress (ESTO, DIRECT SAFE, to differentiate early versus late stroke to guide
SWIFT DIRECT and MR CLEAN NO IV) evaluating reperfusion therapy.17 Because preservation of
the feasibility of MT alone without the use of viability in brain tissue largely depends on the
thrombolysis (Table 1). collateral vascular supply, patients with good col-
laterals can sustain brain perfusion for a longer
Expanding Indications for Mechanical time after a territorial occlusion. Therefore, a sub-
Thrombectomy set of patients may still benefit from MT even after
Role of imaging the 6 hour time window. Perfusion imaging in this
Noncontrast CT is the primary imaging modality in regard has been revolutionary to identify the brain
the evaluation of acute stroke to rule out any intra- parenchyma which is ischemic but without irre-
cranial hemorrhage and to identify the extent of versible damage, hence are salvageable with
stroke seen as areas of hypodensity which are timely reperfusion (penumbra). The CT or MR
determined by the ASPECTS score. The stroke perfusion imaging is based on the calculation of
guidelines in 2015 included ASPECT score 6 three parameters after a bolus of contrast adminis-
as the imaging criteria for patients eligible for tration which are cerebral blood flow (CBF), cere-
MT.16 MRI of the brain is more sensitive and spe- bral blood volume (CBV), and time to peak (TTP).
cific to detect early ischemia which seems as le- Overall, low CBF and CBV in an area implicate irre-
sions with restricted diffusion in DWI sequences versible brain damage (infarct core), whereas
and can be seen as early as few minutes after increased TTP suggests a delay in contrast transit
the stroke onset. Fluid attenuated inversion recov- owing to collateral-predominant filling, leading to
ery imaging (FLAIR) sequences also detect delay in contrast transit in that specific area. A
ischemic changes appearing as hyperintensity in normal CBV/CBF with increased TTP can thus
the images, although it takes several hours for identify penumbra and allow for potential
Table 1
Ongoing trials comparing direct mechanical thrombectomy to current standard of therapy (Bridging
treatment with IV alteplase) in patients with large vessel occlusion
ESTO Direct Safe Swift Direct MR Clean No IV
Continent of North America Australia Europe Europe
origin
Single/ Single Multicenter (33) Multicenter (39) Multicenter (20)
multicenter
Number of 80 780 410 540
patients
Major Inclusion Pts 18–90 y Pts 18 y Pts 18 y Pts 18 y
criteria Within 4.5 h of Within 4.5 h of Within 4.5 h of Within 4.5 h of
onset onset onset onset
NIHSS 6 Occlusion of NIHSS 5 Occlusion of
Occlusion of ICA, M1, M2, or and < 30 ICA, M1, M2
ICA,M1,M2 Basilar artery Occlusion of ICA,
M1
ASPECT score
4
Major Exclusion ASPECTS 1/
3rd MCA
territory
Estimated study December 2021 May 2023 December 2023 April 2022
completion
date
Trial Registration NCT04240470 NCT03494920 NCT03192332 ISRCTN80619088
Number
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.172 Patra et al
therapeutic intervention. Most centers use CBV or findings of these studies proved while time is an
CBF less than 30% of normal hemisphere as the important limiting factor for stroke intervention,
cutoff for core infarct and a TTP threshold of selected patients with preserved ischemic brain
more than 6 seconds as cut-off to define the pen- may benefit from reperfusion even if delayed.
umbra. The core-penumbra mismatch is used to Therefore, in the new AHA/ASA guideline, the indi-
determine the degree of salvageable brain tissue cation of MT has been expanded to include pa-
which might benefit from reperfusion therapy. tients up to 24 hours of stroke onset provided
This was the basis of the recent 2 new trials they meet the DEFUSE-3/DAWN trial criteria.21
(DAWN and DIFFUSE-3) on MT which evaluated There are currently 2 other trials evaluating the
the clinical benefit of MT beyond the 6-h win- role of MT beyond the 6-hour time window
dow.18,19 One of the notable advancements in (Table 2). To date, the benefit of MT beyond the
recent years is the development of automated 24-h window has not been evaluated in any ran-
and semiautomated postprocessing software domized trial. In an ad hoc analysis, the
which provides an immediate CTA and perfusion DEFUSE-3 investigators found that about 20% of
maps and identifies the brain areas with reduced the patients who presented beyond 24 hours of
flow and vessel occlusion. One of the important stroke onset (so not treated with MT) continued
benefits of these tools is the availability of mobile to have mismatch for an additional 24 hours.22
devices across multiple platforms, allowing rapid Only 10% of these patients had a favorable
notification of providers within few seconds of im- outcome at 90 days, suggesting that MT could
age acquisition. These mobile applications run an have been of benefit in these patients. In another
automated algorithm to show the CTA map, the retrospective study, Desai and colleagues
ASPECT score, presence or absence of large reviewed 21 patients who met the DAWN criteria
vessel occlusion, and the likelihood of candidacy but underwent MT beyond 24 hours of last known
for MT. There are several vender specific commer- normal status.23 When compared with the DAWN
cial software programs available at this time; how- intervention arm, these patients had comparable
ever, the most commonly used software in the clinical outcomes in terms of 90-day functional in-
large trials including EXTEND-IA, DEFUSE 3, and dependence and safety (symptomatic intracranial
DAWN trials is the rapid processing of perfusion hemorrhage). Currently, the evidence is insuffi-
and diffusion (RAPID) software (iSchemaView). cient to support MT in patients presenting beyond
24 hours. Randomized trials are needed to further
Leveraging the time window for mechanical investigate the benefits in this patient population
thrombectomy which may allow extension of the eligibility time
A revolutionary change in stroke intervention was window for MT.
witnessed after the success of 5 randomized trials
demonstrating a significant benefit of MT in pa- Implications of large core infarcts at
tients with large vessel occlusion.20 In the initial presentation
guideline proposed by the American Heart Associ- Most of the RCTs evaluating the benefits of MT
ation/American Stroke Association (AHA/ASA), in exclude patients with an ASPECT score less than
2015, the indication of MT in patients with LVO 6 which suggests an already developed large
was limited to 6 hours from the stroke symptom core infarct. The HERMES group meta-analysis
onset.16 With subsequent post hoc analyses of 5 randomized trials shows that lower baseline
from the RCTs and anecdotal reports, the benefit ASPECTs (Less than 6) is strongly associated
of MT was often observed in patients beyond the with lower rates of favorable outcome.12 Similarly,
6-h time window. With the advancement of imag- in the THRACE trial, only 30% of the patients with
ing technology and use of perfusion imaging, it is large core infarct and poor baseline ASPECTS (0–
now possible to identify patients with significant 4), had a good clinical outcome at 3 months.24 On
penumbra even after the standard 6 hours. Two the other hand, a retrospective study analyzing pa-
important randomized trials (DIFUSE-3 and tients with low ASPECTs (6) from the French
DAWN) evaluated the clinical benefit in patients af- Endovascular Treatment in Ischemic Stroke regis-
ter this 6-h time window.18,19 The DEFUSE-3 trial try found an increased rate of favorable outcome
included patients up to 16 hours, whereas the and decreased rate of mortality in patients who
DAWN included patients up to 24 hours from had successful reperfusion with MT as compared
symptom onset and used perfusion mismatch with nonreperfused patients.25 However, the
criteria with maximal allowable core infarct volume benefit was minimal in patients with very low AS-
of 70 mL (DEFUSE-3) and 51 mL (DAWN). Both tri- PECTS (50 cc on CTP) found that MT
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.Modern and Future Endovascular Stroke Care 173
Table 2
Ongoing trials evaluating the role of mechanical thrombectomy beyond 6 h window
RESILIENTExt MR Clean-Late Tension
Continent of origin South America Europe EUROPE
Single/multicenter Multicenter Multicenter Multicenter
Number of patients 376 500 665
Major Inclusion Criteria Within 6–24 h of Within 6–24 h within 12 h of stroke
symptom onset NIHSS 2 onset
Prestroke mRS2 ICA, M1/M2 occlusion NIHSS 90%). However,
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.174
Table 3
Ongoing trials evaluating the role of mechanical thrombectomy in patients with large ischemic core
Patra et al
Rescue-Japan
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
Select 2 Limit Angel-Aspect Tesla Laste
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.
Continent of North America Asia Asia North America EUROPE
origin
Single/ Multicenter Multicenter Multicenter Multicenter Multicenter
multicenter
Number of 560 200 488 300 450
patients
Major Inclusion NIHSS 6 NIHSS 6 Prestroke 0–1 NIHSS >6 Prestroke mRS
criteria Last known well ASPECT 3–5 NIHSS 6–30 Prestroke 0–1 0–1
6–24 h Prestroke 0–1 ASPECT 3–5 ASPECT 2–5 ASPECTS 0–5 (4–
Prestroke mRS Large infarct 5 in 80 yrs)
0–1 core defined as Last known
Large infarct ASPECT 3–5 or normal 6.5 h
core defined as rCBF ofModern and Future Endovascular Stroke Care 175 the rate of favorable outcome, procedural safety, substantial benefit of endovascular therapy over and intracranial hemorrhage were similar. Per- medical management. forming thrombectomies in these situations is challenging as it involves the treatment of proximal Thrombectomy in mild stroke stenosis or occlusion with stenting or angioplasty. The patients presenting with mild stroke score Both an anterograde approach (which involves (NIHSS 0–5) are classically considered to have no stenting/angioplasty of the extracranial ICA fol- large vessel occlusion or have good collateral circu- lowed by distal ICA/MCA thrombectomy) and lation to sustain brain function, therefore, were retrograde approach (initial distal access through excluded as candidates for MT. However, as high the occluded segment and performing thrombec- as 18% of patients with NIHSS score less than 5 tomy of ICA/MCA followed by the subsequent and 39% of patients with NIHSS score 5 to 8 can treatment of the proximal occlusion) have been re- have large vessel occlusion and therefore, may ported, without any significant difference in benefit from thrombectomy.35 However, in a retro- outcome.30 Currently, there is equivocal evidence spective study of 214 patients, Sarraj and col- regarding the use of carotid stenting versus angio- leagues failed to demonstrate any benefit of MT in plasty in acute settings. Proponents of carotid large vessel occlusions with mild strokes (NIHSS stenting argue that stenting allows higher recana-
176 Patra et al
Table 4
Ongoing trials evaluating the role of mechanical thrombectomy in patients with mild strokes
MOSTE ENDOLOW
Continent of Origin Europe North America
Single/Multicenter Single Multicenter
Number of patients 824 200
Major Inclusion Criteria NIHSS 0–5 NIHSS 0–5
ICA, M1, M2 occlusion ICA, M1 or “M1 like” M2
ASPECT 6 occlusion
Infarct coreModern and Future Endovascular Stroke Care 177
Fig. 1. (A) The original Merci device with helicoid loops. (B,C) The original Penumbra aspiration system. (D)
Solitaire-X stentriever. (E). Trevo XP ProVue Stentriever. ([A-E] CopyrightÓ Stryker Neurovascular, Reprinted
with permission. All Rights Reserved; [B,C] Copyright Ó Penumbra Inc. Reprinted with permission. All Rights
Reserved; and [D] Copyright Ó October 2021 Medtronic, Inc. Reprinted with permission-All Rights Reserved.)
separator is passed to fragment the clot that is device (TREVO 2) which again showed a higher
aspirated into the catheter. In one of the index tri- rate of successful recanalization with the Trevo
als using the Penumbra system which included retriever as compared with the Merci Device
125 patients, successful recanalization was (86% vs 60%). In 2013, 3 major trials (MR
demonstrated in 82% (as compared with 69% RESCUE, IMS III, and SYNTHESIS) compared
with Merci device in Multi-MERCI) although with MT to medical management for large vessel occlu-
a similar mortality rate (33%). In the early years, sion, but unfortunately failed to show any benefit of
there was a mixed experience with the use of endovascular management. These trials were
thrombectomy devices. Higher recanalization heavily criticized in the endovascular world
rates were generally associated with good clinical because of inconsistencies in patient selection,
outcomes and failed recanalization leading to device selection, and the treatment workflow.
higher complication rates and higher mortality. Subsequently, in 2015, 5 major trials featured a
There was a persistent enthusiasm over improving streamlined treatment algorithm with the use of
the design and safety of the devices which led to first-generation stent retrievers instead of Merci
the emergence of first-generation stent retrievers. device (MR CLEAN, ESCAPE, EXTEND-IA, SWIFT
The concept of stent retrievers is derived from the PRIME, REVASCT) which consistently showed a
success of expandable stents used in the treat- significant benefit of MT in patients with LVO within
ment of aneurysms and intracranial atheroscle- 6 hours of onset. This finding revolutionized the
rosis, with the difference being the stents used in treatment guidelines for acute ischemic stroke.
thrombectomy are retrievable. The 2 first- Over time, there have been constant attempts to
generation stent retrievers which received FDA improve stent design and delivery mechanisms
clearance are Solitaire FR (MicroTherapeutic Inc, to improve the first pass recanalization rate with
Irvine, CA) and the Trevo Retriever (Concentric the development of second-generation stent re-
Medical, Mountain View, CA). The SWIFT trial in trievers. Currently, there are many stent retrievers
2010 conducted a noninferiority trial comparing on market with unique mechanical advantages
the Solitaire FR and the Merci Retriever and found with each. The newer Solitaire- X (Medtronic,
a far superior rate of recanalization (TIMI scale 2 or Irvine, CA) device offers a unique parametric
3) with the Solitaire device (61% vs 24%). A similar design that allows dynamic clot integration
noninferiority trial was conducted for the Trevo (Fig. 1D. Similarly, the Trevo XP ProVue device
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.178 Patra et al
offers an open-cell design for softness and optimal catheter is advanced in contact with the clot and a
clot integration (Stryker, MI, USA) (Fig. 1E). The contact aspiration is performed. After 1 or 2 failed
other stent retrievers include the 3D revasculariza- attempts, the stent retriever is used as a rescue
tion device (Penumbra Inc, Alameda, California) measure. The advantage of this approach is that
(Fig. 2A); Embotrap retrievable stent (Cerenovus/ it is fast, avoids the manipulation of the vessel
Johnson & Johnson, New Brunswick, New Jersey) with a stent and in addition, more economical if
(Fig. 2B). The 3D device has a unique architecture aspiration is successful without the need of a
of intraluminal chambers to lock and trap clot dur- stent. A single-arm ADAPT FAST study, in 2014,
ing the retrieval process. The Embotrap device is used this technique and reported successful
similarly uniquely designed to have an outer cage revascularization (TICI 2b or 3) in 78% of the cases
and inner cage to secure the clot along with a which improved to 95% when stent retrievers were
distal mesh which helps in retaining the clot during used as rescue.43 Subsequently, 2 RCTs evalu-
the removal process. All these devices have ated the efficacy of ADAPT technique to the stan-
shown promising results in several recent case se- dard stent-retriever first technique. The first trial
ries. With a better understanding of clot was the Contact Aspiration versus Stent Retriever
morphology and their interaction with the vessel for Successful Revascularization (ASTER) which
wall, there is a great expectation of the develop- was designed to prove the superiority of the
ment of newer improved, effective, and safe stent ADAPT technique over the stentreivers.44 Howev-
retrievers. er, the analysis failed to find a significant difference
in the rate of successful reperfusion (mTICI score
Aspiration versus stent 2b) between the 2 techniques (83.1% in ADAPT
The most common technique during a stent vs 85.4% in stent retriever). Subsequently, the
retriever thrombectomy involves the use of aspira- second trial, the COMPASS trial ran a noninferior-
tion during the retrieval process to provide a nega- ity study between the 2 techniques whereby the
tive suction for better grip of the clot in the stent. primary endpoint was functional independence at
Additionally, the negative pressure decreases the 90 days.44 The trial observed 90-days indepen-
forward flow to prevent the distal embolization of dence in 52% of patients with ADAPT as
the disrupted clot. As an alternative to the use of compared with 50% with stent retrievers. Addi-
stent, direct aspiration only has been evaluated tionally, the rate of successful reperfusion (mTICI
and used as a technique for thrombectomy. This score 2b) was comparable between the 2 tech-
approach is called the direct aspiration first pass niques (83% in ADAPT and 81% in stent retriever).
technique (ADAPT) in which a wide bore aspiration The study concluded that the ADAPT technique is
Fig. 2. (A) 3D stentriever (B)
Embotrap Stentriever. (C) MIVI
Q Catheter System. (D) pRESET
stentriever (E) Tigertriever. ([A]
Copyright Ó Penumbra Inc. Re-
printed with permission. All
Rights Reserved; [B] Copyright
Ó CERENOVUS 2021. Reprinted
with permission. All Rights
Reserved; [C] CopyrightÓ MIVI
Neuroscience, Inc. Reprinted
with permission. All Rights
Reserved; [D] Copyright Ó Phe-
nox GmbH, Reprinted with
permission. All Rights
Reserved; and [E] Image cour-
tesy of Rapid Medial – All
rights reserved)
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.Modern and Future Endovascular Stroke Care 179
not inferior to stent retrievers to be used as the first revascularization rate, and functional outcomes.46
pass method for acute large vessel occlusion. Although the transfemoral approach is still the
Currently, the recommendation from American most common access method used in many cen-
Heart Association/American Stroke Association ters, it is now being more evident that the transra-
does not recommend one technique over the dial access could be noninferior to transfemoral
other, but there is a trend among neurointerven- approach for MT.
tionalists to use aspiration as the first pass method Direct trans-cervical carotid access (TCCA) is
for a slightly faster revascularization.21 also an alternate access route for the anterior cir-
culation and has been infrequently reported for
Femoral versus radial versus direct trans- endovascular treatment in strokes. In a reported
carotid approach series of 7 patients, transcarotid puncture was
Transfemoral approach has been the traditional performed after failure of transfemoral access (in
method for endovascular access for MT. This is 6 patients) and as the initial attempt in one patient
the most common approach the stroke interven- (due to tortuosity seen in CT angiogram). Success-
tionalists is trained to use and often is most ful revascularization was achieved in all but one
comfortable with. Due to time-sensitive nature of patient. One complication of neck hematoma not
the MT, the transfemoral approach is most requiring further surgery was noted.47 Another
commonly used. Transradial access is an alterna- report described 6 patients undergoing direct ca-
tive method of vascular access most commonly rotid access whereby successful reperfusion was
adopted in the cardiology world, but has been achieved in all patients. One surgical complication
adopted by neuroendovascular surgeons in a vari- involved a neck hematoma that required surgical
ety of procedures from diagnostic angiograms to removal.48 In a cohort of 7 patients, Scoco and
aneurysm coiling and carotid stenting. Although colleagues reported TCCA in 5 patients in which
difficult femoral access or difficult aortic arch anat- 4 patients achieved TICI 2b reperfusion without
omy is the traditional indication for using a transra- any procedural complications.49 The experience
dial approach, it is being used more frequently as a from all these series suggests that direct transcar-
preferred or first-line approach in some centers. otid access can be used as a reasonable alternate
The benefits of the transradial approach are multi- access when the arch tortuosity or proximal ca-
fold and include shorter recovery time, increased rotid tortuosity is not favorable for transfemoral/
patient comfort, lower access site procedural transradial access.
complication rates, and cost savings by avoiding
closure devices. However, the radial access is
Future Directions
limited by the diameter of the guide catheter that
it may allow and may not be suitable in patients Prehospital triage
with variant arm vascular anatomy or an incom- One of the major challenges in the field is the
plete palmar arch. The utility of the transradial nonavailability of specific imaging to identify pa-
approach has been recently explored in MT. The tients with large vessel occlusions who would
need for rapid intravascular access is one of the benefit from rapid intervention and therefore, rely
challenges; therefore, most reports of MT with on stroke severity scales which often are unreli-
transradial approach are mostly limited to centers able. In this regard, the VIPS device (Volumetric
with vast experience with the technique. In a series Impedance Phase Shift Spectroscopy, Cerebro-
of 375 patients, Phillips and colleagues compared tech, California) has been developed by which
the transradial access to transfemoral access for has the ability to detect LVO based on the differ-
MT and found no difference in terms of time to ence in the water content in 2 hemispheres. This
perfusion (median time from imaging to reperfu- device is worn by the patient which detects the
sion 96.5 mins for transfemoral and 95 min for impendence signals from the hemispheres to see
transradial) and clinical outcome (90-days mRS any asymmetry. In a study of 248 patients
0–2 of 58% with transfemoral vs 67% with transra- including patients with acute stroke, other pathol-
dial).45 Additionally, the rate of major access site ogies, and healthy volunteers, the VIPS device was
complication requiring another procedure was shown to have a sensitivity of 93% and specificity
higher in transfemoral approach (6.5%) versus of 92% in detecting LVOs.50 Similarly, another
none in the transradial approach. Another similar remarkable development is the SONAS device
albeit smaller series that included 51 patients (BURL Concepts, San Diego, California), a
found no difference between transradial versus portable, battery-powered ultrasound device for
transfemoral approach in terms of single-pass brain perfusion assessment. SONAS works in
recanalization rate, average number of passes, combination with intravenously injected micro-
mean access to reperfusion time, successful bubble contrast agents which are used as signal
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.180 Patra et al
tracers. Transducers are positioned on both sides electronic medical record (Intelligent EMR, iEMR)
of the head to detect hemispheric perfusion defi- which allows the extraction of relevant medical his-
cits (Fig. 3A, B). SONAS is CE Mark approved tory or prior treatment to determine candidacy for
and has been tested clinically for safety and feasi- thrombolysis/thrombectomy as well as prognosti-
bility in patients with stroke. cation. With the continued evolution of technology,
the scope of AI is expected to be expanded for the
Improvement of emergency room workflow rapid formulation of a customized treatment plan
Optimization of the emergency room workflow has for an individual patient.
recently been the prime focus to achieve the short-
est door to needle (DTN) and door to groin punc- Endovascular therapy
ture (DTP) time. One of the key advancements in With rapidly evolving technology and a better un-
this regard is the concept and development of a derstanding of clot morphology and biome-
“Neuro ED” which allows a highly coordinated chanics, there have been constant improvements
workflow between the ED to the endovascular in the design and development of stent retrievers.
suite under a highly specialized setup combining One of the new such concepts is the Lazarus Ef-
the resuscitation bay, imaging, and endovascular fect Cover device (Medtronic, Irvine, California)
suite into one hybrid unit.51 which is a novel nitinol mesh cover that wraps
the stentriever during clot retrieval to prevent distal
Role of artificial intelligence embolism. Similarly, the MIVI-Q Catheter system
Machine learning algorithms are being increasingly (MIVI Neurosciences Inc, Prairie, Minnesota) is
used to allow a more automated process and another innovative aspiration catheter system
reduce lag time in treatment initiation. One of the whereby the proximal portion of the catheter is
basic uses is AI-based automated software pro- replaced with a wire, allowing for the increased
cessing of CT/CTA/CTP imaging to rapidly calcu- cross-sectional area to improve the flow rate with
late the ASPECT score, probability of LVO, and aspiration (Fig. 2C). Another stent retriever mar-
the size of penumbra. Another utility of AI is the inte- keted as pRESET 5 to 40 and pRESET LUX (Phe-
gration of natural language processing to read the nox. Bochum, Germany), currently available in
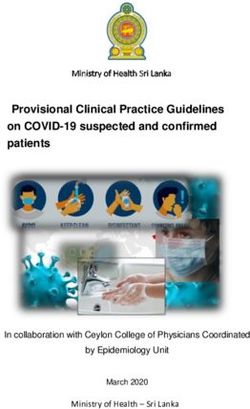
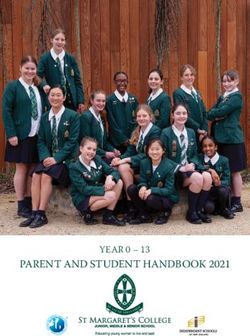
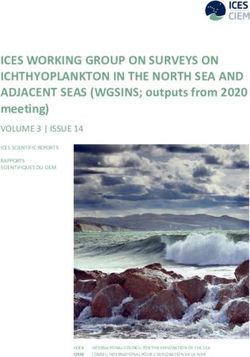
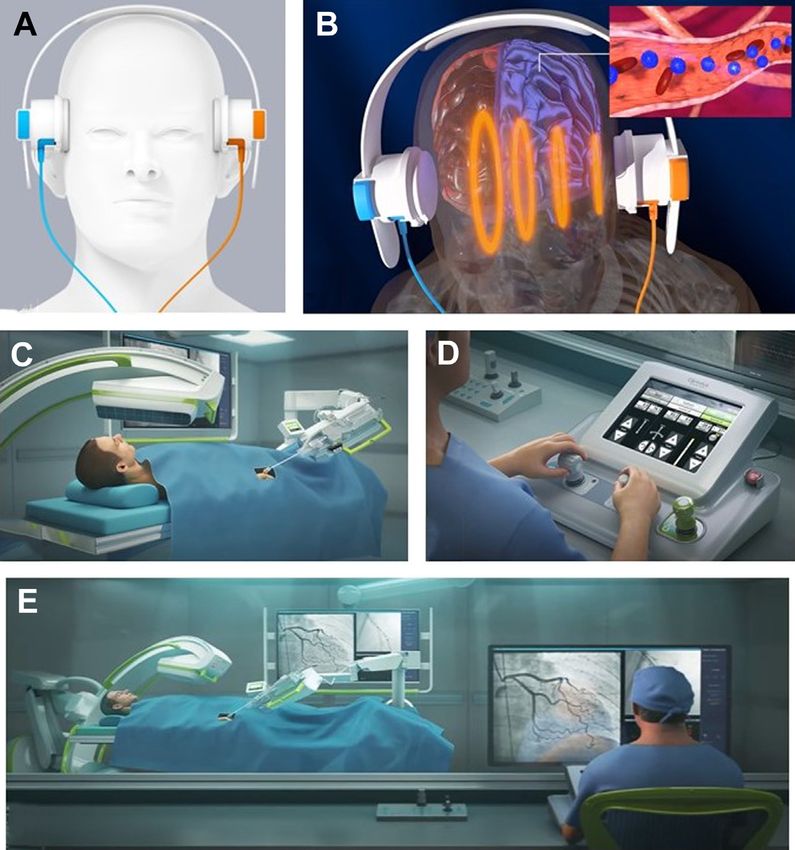
Fig. 3. (A, B) SONAS device.
Illustration showing the detec-
tion of ultrasound waves by
the SONAS device after the in-
jection of contrast bubbles (B).
(C–E): Telerobotics CorPath
GRX system showing the
bedside robotic unit with
extended arm(C), The console
(D), Illustration showing sur-
geon operating the robotic
unit from the console (E). ([A,
B] Copyright Ó Burl Concepts
Inc. Reprinted with permission.
All rights reserved; [C–E] Copy-
right Ó 2021 Corindus, Inc. Re-
printed with permission. All
Rights Reserved.)
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.Modern and Future Endovascular Stroke Care 181
Europe, has a helical slit design to maintain cell benefits from robust industry support and
shape irrespective of the expansion diameter generous funding by foundations and government
(Fig. 2D). Another innovative design is the radially agencies. The last 2 decades have seen rapid and
adjustable stent retriever (Tigertriever, Rapid Med- compelling advances in stroke care. With the inte-
ical) which allows the dynamic manipulation of the gration of imaging, pathology, and clinical data
stent diameter and radial force by the operator into AI platforms, we are not far from the time
with a hand-held slider during the stent deploy- when acute stroke intervention will be an individu-
ment (Fig. 2E). The primary results of the multi- alized approach by man and machine to provide
center TIGER trial have recently been published the best possible outcome.
to show noninferiority of the stent retriever
compared with Trevo and Solitaire devices with a CLINICS CARE POINTS
first pass successful reperfusion of 57.8% and
final successful reperfusion of 95.7%.52
Telerobotics in stroke Mechanical thrombectomy can provide a sig-
The use of teleoperated endovascular robots is nificant improvement in clinical outcome in
one of the revolutionary concepts in modern stroke patients with large vessel occlusion
up to 24 hours from stroke onset
stroke management. Although the concept of ro-
botic MT is relatively new, its utility is now being Optimization of emergency room workflow
increasingly realized. The endovascular robot, to achieve shortest door to needle and door
CorPath GRX system (Corindus, Waltham, MA) to groin puncture time is essential to improve
the clinical outcome after stroke therapy
initially designed for cardiac angioplasty has
now successfully been used in various neuroen- Both aspiration and stent retriever tech-
dovascular procedures including diagnostic an- niques provide comparable successful reper-
giograms, carotid stenting as well as aneurysm fusion rate as well as 90 days independence
rates after mechanical thrombectomy
coiling. The robotic system has 3 components
including the bedside robotic unit with an
extended arm, a single-use cassette with all
endovascular supplies, and a remote physician
workspace with console (Fig. 3C–E). The physi- DISCLOSURE
cian controls the catheter and wire movement at
The authors have nothing to disclose.
the console outside of the operating room using
a joystick, touch screen, and foot pedals. A
high-speed local area network allows rapid trans- REFERENCES
mission of the signal to the robotic arm for precise
and real-time control of the catheter system 1. Demaerschalk BM, Berg J, Chong BW, et al. Amer-
without significant time lag. Telerobotics involves ican Telemedicine Association: Telestroke Guide-
the use of robots at one facility which is controlled lines. Telemed J E Health 2017;23(5):376–89.
by an experienced endovascular surgeon at 2. Wilcock AD, Schwamm LH, Zubizarreta JR, et al.
another facility through high-speed fiber network Reperfusion Treatment and Stroke Outcomes in
system.53 The utility of telerobots has been Hospitals With Telestroke Capacity. JAMA Neurol
recently tested in an ex vivo proof of concept 2021;78(5):527–35.
study whereby robotics endovascular thrombec- 3. Kuang H, Najm M, Chakraborty D, et al. Automated
tomy was successfully performed on an artificial ASPECTS on Noncontrast CT Scans in Patients with
human model by an off-site neurosurgeon at a Acute Ischemic Stroke Using Machine Learning.
location 5 miles away.54 With future use in real pa- AJNR Am J Neuroradiol 2019;40(1):33–8.
tients, such a proficient system is likely to com- 4. Fassbender K, Walter S, Liu Y, et al. Mobile stroke
plement the existing telestroke system by unit" for hyperacute stroke treatment. Stroke 2003;
adding the possibility for intervention at remote 34(6):e44.
locations, thereby considerably optimizing time 5. Fassbender K, Grotta JC, Walter S, et al. Mobile
to treatment. stroke units for prehospital thrombolysis, triage,
and beyond: benefits and challenges. Lancet Neurol
Summary 2017;16(3):227–37.
We are now in a time when the scope of revolution- 6. Walter S, Kostopoulos P, Haass A, et al. Diagnosis
izing acute stroke care is enormous, thanks to and treatment of patients with stroke in a mobile
multi-center collaborations, novel device design, stroke unit versus in hospital: a randomised
and technological breakthroughs. The field also controlled trial. Lancet Neurol 2012;11(5):397–404.
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.182 Patra et al
7. Barrett KM, Pizzi MA, Kesari V, et al. Ambulance- between Deficit and Infarct. N Engl J Med 2018;
based assessment of NIH Stroke Scale with tele- 378(1):11–21.
medicine: A feasibility pilot study. J Telemed Tele- 19. Albers GW, Marks MP, Kemp S, et al. Thrombectomy
care 2017;23(4):476–83. for Stroke at 6 to 16 Hours with Selection by Perfu-
8. Grotta JC, Yamal JM, Parker SA, et al. Prospective, sion Imaging. N Engl J Med 2018;378(8):708–18.
Multicenter, Controlled Trial of Mobile Stroke Units. 20. Demaerschalk BM, Scharf EL, Cloft H, et al. Contem-
N Engl J Med 2021;385(11):971–81. porary Management of Acute Ischemic Stroke
9. Jahan R, Saver JL, Schwamm LH, et al. Association Across the Continuum: From TeleStroke to Intra-
Between Time to Treatment With Endovascular Re- Arterial Management. Mayo Clin Proc 2020;95(7):
perfusion Therapy and Outcomes in Patients With 1512–29.
Acute Ischemic Stroke Treated in Clinical Practice. 21. Powers WJ, Rabinstein AA, Ackerson T, et al. Guide-
JAMA 2019;322(3):252–63. lines for the Early Management of Patients With
10. Bourcier R, Goyal M, Liebeskind DS, et al. Associa- Acute Ischemic Stroke: 2019 Update to the 2018
tion of Time From Stroke Onset to Groin Puncture Guidelines for the Early Management of Acute
With Quality of Reperfusion After Mechanical Throm- Ischemic Stroke: A Guideline for Healthcare Profes-
bectomy: A Meta-analysis of Individual Patient Data sionals From the American Heart Association/Amer-
From 7 Randomized Clinical Trials. JAMA Neurol ican Stroke Association. Stroke 2019;50(12):
2019;76(4):405–11. e344–418.
11. Mendez B, Requena M, Aires A, et al. Direct Transfer 22. Christensen S, Mlynash M, Kemp S, et al. Persistent
to Angio-Suite to Reduce Workflow Times and In- Target Mismatch Profile >24 Hours After Stroke
crease Favorable Clinical Outcome. Stroke 2018; Onset in DEFUSE 3. Stroke 2019;50(3):754–7.
49(11):2723–7. 23. Desai SM, Haussen DC, Aghaebrahim A, et al.
12. Goyal M, Menon BK, van Zwam WH, et al. Endovas- Thrombectomy 24 hours after stroke: beyond
cular thrombectomy after large-vessel ischaemic DAWN. J Neurointerv Surg 2018;10(11):1039–42.
stroke: a meta-analysis of individual patient data 24. Bracard S, Ducrocq X, Mas JL, et al. Mechanical
from five randomised trials. Lancet 2016; thrombectomy after intravenous alteplase versus al-
387(10029):1723–31. teplase alone after stroke (THRACE): a randomised
13. Suzuki K, Matsumaru Y, Takeuchi M, et al. Effect of controlled trial. Lancet Neurol 2016;15(11):1138–47.
Mechanical Thrombectomy Without vs With Intrave- 25. Desilles JP, Consoli A, Redjem H, et al. Successful
nous Thrombolysis on Functional Outcome Among Reperfusion With Mechanical Thrombectomy Is
Patients With Acute Ischemic Stroke: The SKIP Ran- Associated With Reduced Disability and Mortality
domized Clinical Trial. JAMA 2021;325(3):244–53. in Patients With Pretreatment Diffusion-Weighted Im-
14. Yang P, Zhang Y, Zhang L, et al. Endovascular aging-Alberta Stroke Program Early Computed To-
Thrombectomy with or without Intravenous Alteplase mography ScoreModern and Future Endovascular Stroke Care 183
Thrombectomy for Tandem Large Vessel Occlusion ischemic stroke. Results of the multi Mechanical
Strokes. Interv Neurol 2020;8(2–6):92–100. Embolus Removal in Cerebral Ischemia (MERCI)
31. Da Ros V, Scaggiante J, Sallustio F, et al. Carotid trial, part I. AJNR Am J Neuroradiol 2006;27(6):
Stenting and Mechanical Thrombectomy in Patients 1177–82.
with Acute Ischemic Stroke and Tandem Occlusions: 43. Turk AS, Frei D, Fiorella D, et al. ADAPT FAST study:
Antithrombotic Treatment and Functional Outcome. a direct aspiration first pass technique for acute
AJNR Am J Neuroradiol 2020;41(11):2088–93. stroke thrombectomy. J Neurointerv Surg 2014;
32. Zhu F, Hossu G, Soudant M, et al. Effect of emergent 6(4):260–4.
carotid stenting during endovascular therapy for 44. Lapergue B, Blanc R, Gory B, et al. Effect of Endo-
acute anterior circulation stroke patients with tan- vascular Contact Aspiration vs Stent Retriever on
dem occlusion: A multicenter, randomized, clinical Revascularization in Patients With Acute Ischemic
trial (TITAN) protocol. Int J Stroke 2021;16(3):342–8. Stroke and Large Vessel Occlusion: The ASTER
33. Schonewille WJ, Wijman CA, Michel P, et al. Treat- Randomized Clinical Trial. JAMA 2017;318(5):
ment and outcomes of acute basilar artery occlusion 443–52.
in the Basilar Artery International Cooperation Study 45. Phillips TJ, Crockett MT, Selkirk GD, et al. Transradial
(BASICS): a prospective registry study. Lancet Neu- versus transfemoral access for anterior circulation
rol 2009;8(8):724–30. mechanical thrombectomy: analysis of 375 consec-
34. Langezaal LCM, van der Hoeven E, Mont’Alverne FJA, utive cases. Stroke Vasc Neurol 2021;6(2):207–13.
et al. Endovascular Therapy for Stroke Due to Basilar- 46. Chen SH, Snelling BM, Sur S, et al. Transradial
Artery Occlusion. N Engl J Med 2021;384(20): versus transfemoral access for anterior circulation
1910–20. mechanical thrombectomy: comparison of technical
35. Heldner MR, Zubler C, Mattle HP, et al. National In- and clinical outcomes. J Neurointerv Surg 2019;
stitutes of Health stroke scale score and vessel oc- 11(9):874–8.
clusion in 2152 patients with acute ischemic 47. Jadhav AP, Ribo M, Grandhi R, et al. Transcervical
stroke. Stroke 2013;44(4):1153–7. access in acute ischemic stroke. J Neurointerv
36. Sarraj A, Hassan A, Savitz SI, et al. Endovascular Surg 2014;6(9):652–7.
Thrombectomy for Mild Strokes: How Low Should 48. Wiesmann M, Kalder J, Reich A, et al. Feasibility of
We Go? Stroke 2018;49(10):2398–405. combined surgical and endovascular carotid ac-
37. Goyal N, Tsivgoulis G, Malhotra K, et al. Medical cess for interventional treatment of ischemic stroke.
Management vs Mechanical Thrombectomy for J Neurointerv Surg 2016;8(6):571–5.
Mild Strokes: An International Multicenter Study 49. Scoco AN, Addepalli A, Zhu S, et al. Trans-Carotid
and Systematic Review and Meta-analysis. JAMA and Trans-Radial Access for Mechanical Thrombec-
Neurol 2020;77(1):16–24. tomy for Acute Ischemic Stroke: A Systematic Re-
38. Seners P, Ben Hassen W, Lapergue B, et al. Predic- view and Meta-Analysis. Cureus 2020;12(6):e8875.
tion of Early Neurological Deterioration in Individuals 50. Kellner CP, Sauvageau E, Snyder KV, et al. The VI-
With Minor Stroke and Large Vessel Occlusion In- TAL study and overall pooled analysis with the
tended for Intravenous Thrombolysis Alone. JAMA VIPS non-invasive stroke detection device.
Neurol 2021;78(3):321–8. J Neurointerv Surg 2018;10(11):1079–84.
39. Ravindra VM, Alexander M, Taussky P, et al. Endo- 51. Greenberg K, Hedayat HS, Binning MJ, et al. Inno-
vascular Thrombectomy for Pediatric Acute vations in Care Delivery of Stroke from Emergency
Ischemic Stroke: A Multi-Institutional Experience of Medical Services to the Neurointerventional Oper-
Technical and Clinical Outcomes. Neurosurgery ating Room. Neurosurgery 2019;85(suppl_1):
2020;88(1):46–54. S18–22.
40. Al-Mufti F, Schirmer CM, Starke RM, et al. Thrombec- 52. Gupta R, Saver JL, Levy E, et al. New Class of Radi-
tomy in special populations: report of the Society of ally Adjustable Stentrievers for Acute Ischemic
NeuroInterventional Surgery Standards and Guide- Stroke: Primary Results of the Multicenter TIGER
lines Committee. J Neurointerv Surg 2021. https:// Trial. Stroke 2021;52(5):1534–44.
doi.org/10.1136/neurintsurg-2021-017888. 53. Panesar SS, Volpi JJ, Lumsden A, et al. Telerobotic
41. Smith WS, Sung G, Starkman S, et al. Safety and ef- stroke intervention: a novel solution to the care
ficacy of mechanical embolectomy in acute dissemination dilemma. J Neurosurg 2019;132(3):
ischemic stroke: results of the MERCI trial. Stroke 971–8.
2005;36(7):1432–8. 54. Singer J, VanOosterhout S, Madder R. Remote ro-
42. Smith WS. Safety of mechanical thrombectomy and botic endovascular thrombectomy for acute ischae-
intravenous tissue plasminogen activator in acute mic stroke. BMJ Neurol Open 2021;3(1):e000141.
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en abril 04, 2022. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2022. Elsevier Inc. Todos los derechos reservados.You can also read