A Longitudinal Study of Psychiatric Disorders in Offspring of Parents With Bipolar Disorder From Preschool to Adolescence
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NEW RESEARCH
A Longitudinal Study of Psychiatric Disorders in
Offspring of Parents With Bipolar Disorder From
Preschool to Adolescence
Boris Birmaher, MD, John Merranko, MA, Danella Hafeman, MD,
Benjamin I. Goldstein, MDPhD, Rasim Diler, MD, Jessica C. Levenson, PhD,
Kelly Monk, BSNRN, Satish Iyengar, PhD, Mary Beth Hickey, BA, Dara Sakolsky, MD,
David Axelson, MD, Tina Goldstein, PhD
Objective: To compare the prevalence of psychopathology, particularly bipolar disorder (BD), between preschool offspring of parents with BD and
community controls.
Method: A total of 116 offspring of BD-I/II parents and 98 controls (53 parents with non-BD psychopathology and 45 healthy parents) were recruited
at ages 2 to 5 years and followed on average 9.6 years (on average: 25: 1.6 times; after age 5: 4 times) (average ages at intake/last follow-up: 3.8/13.4,
retention: 98%). Participants were evaluated with standardized instruments blinded to parental diagnoses.
Results: After adjusting for confounders, offspring of BD parents only showed more attention-deficit/hyperactivity disorder (ADHD) during
ages 2 to 5 years than the other 2 groups. After age 5, offspring of BD parents did not differ from offspring of parents with non-BD psycho-
pathology, but they had more anxiety, ADHD, and behavior problems than offspring of healthy parents. Only offspring of BD parents devel-
oped BD-I/II: 3.4% (n = 4) and BDnot-otherwise-specified (BD-NOS): 11.2% (n = 13), with mean onset ages 11.4 and 7.4, respectively.
About 70% of offspring with BD had non-BD disorders before BD. Only ADHD, diagnosed before age 6 years, and early-onset parental BD
were significantly associated with BD risk.
Conclusion: Most offspring of BD parents did not develop BD, but they were at specific high risk for developing BD, particularly those with preschool
ADHD and early-onset parental BD. BD symptoms were scarce during the preschool years and increased throughout the school age, mainly in the form
of BD-NOS, a disorder that conveys poor prognosis and high risk to develop BD-I/II. Developing early interventions to delay or, ideally, to prevent its
onset are warranted.
Key words: bipolar disorder, preschoolers, offspring, psychopathology, high-risk
J Am Acad Child Adolesc Psychiatry 2021;60(11):1419−1429.
ffspring of parents with bipolar disorder (BD) are The few studies of preschool offspring of parents with BD
O at high risk for developing bipolar spectrum dis-
orders, an illness that significantly affects psycho-
social functioning and increases risk for suicidality, legal
show higher rates of disinhibition, fidgetiness, hyperactivity,
aggression, hostility, disruptive behaviors, and depressive
symptoms during observed interactions with peers and
difficulties, substance abuse, and physical illnesses.1 Identifi- unknown adults when compared with offspring of control
cation of factors that specifically predict development of BD parents.12-19 Results from the only 2 longitudinal studies of
among these high-risk offspring will enable early identifica- preschool offspring to date indicate that disruptive behaviors
tion and treatment that may delay onset and/or progression and/or depressive symptoms persist or increase over time.16,19
of the illness and, optimally, prevent it altogether. However, these studies have methodological limitations
Most of the existing studies evaluating the risk of BD such as small samples (maximum sample size = 44), short
development in offspring of parents with BD have been con- follow-up duration, no controls or only healthy control
ducted among school-aged offspring.2-9 However, the study of parents and their offspring, not adjusting for confounding
preschool-aged offspring holds great promise, as preventive factors that may account for the increased psychopathology
interventions delivered during the earlier stages of development in offspring of parents with BD, and/or assessors not
may help preserve a normative developmental trajectory.10,11 blinded to parental diagnosis.
Journal of the American Academy of Child & Adolescent Psychiatry www.jaacap.org 1419
Volume 60 / Number 11 / November 2021BIRMAHER et al.
At the urging of parents enrolled in the Pittsburgh Bipolar from all parents and assent from the offspring when they
Offspring Study (BIOS) of school-age children,2-5 we recruited became 6 years of age.
of 121 preschool offspring (aged 25 years) of parents with For all parents who participated as probands and for
BD and 102 offspring of 65 demographically matched control 66 (49%) of the 134 biological co-parents, psychiatric
parents (45% healthy and 55% with non-BD psychopathol- disorders were ascertained face-to-face using the Struc-
ogy).20 A prior cross-sectional analysis of this sample showed tured Clinical InterviewDSM-IV (SCID),22 plus items
that after adjusting for confounding factors (eg, parental non- from the Schedule for Affective Disorders and Schizo-
BD psychopathology), compared to offspring of the control phrenia for School-Age ChildrenPresent and Lifetime
parents, offspring of parents with BD had significantly more Version (K-SADS-PL)23 for ADHD, disruptive behavior,
attention-deficit/hyperactivity disorder (ADHD) and opposi- and separation anxiety disorders. The SCID kappa (k)
tional defiant disorder (ODD). Regarding mood symptom- values were ≥0.8. Psychosocial functioning was mea-
atology, among the 121 preschool offspring of parents with sured using the Global Assessment of Functioning
BD, 2 exhibited subthreshold manic symptoms, 1 had depres- (GAF).24
sive disorder not-otherwise-specified (NOS), and 1 had adjust- The Family History-Research Diagnostic Criteria
ment disorder with depressed mood. Independent of method25 (plus ADHD, separation anxiety, and disruptive
categorical psychopathology, preschool offspring of parents behavior disorder items) was used to ascertain psychiatric
with BD showed significantly greater aggression, mood dysre- history regarding siblings, second-degree relatives, and
gulation, sleep disturbances, and somatic complaints compared biological co-parents who were not seen for face-to-face
to offspring of control parents.21 Having characterized the life- interviews.
time psychopathology of BIOS preschoolers at study intake, For offspring aged 25 years, only parents were inter-
we set out to prospectively (every other year over nearly 10 viewed about their preschoolers for the presence of lifetime
years) compare the cumulative prevalence of lifetime psychiat- psychiatric disorders using the K-SADS-PL for establishing
ric disorders between offspring of parents with BD and the off- psychiatric diagnoses in preschoolers.20,26-32 The methods
spring of control parents. In addition, we evaluated factors and psychometrics of the KSADS-PL for preschoolers used
associated with risk to develop bipolar spectrum disorders in this study were described in detail in a prior publica-
among offspring. tion.20,27 The language used to asses each symptom in the
KSADS-PL was modified as needed to ensure developmen-
tal appropriateness. Furthermore, to be counted as diagnos-
METHOD tic symptoms, cognitive, behavioral, and emotional
The methods for the BIOS preschool sample have been pre- experiences had to exceed those expected from a typically
sented in detail in a prior publication.20 Briefly, parents with developing preschool-aged child. All evaluations were pre-
DSM-IV BD-I/II who had offspring aged 2 to 5 years were sented to a child psychiatrist/psychologist who ultimately
recruited mainly through advertisement (60%) and followed decided whether a child fulfilled DSM-IV criteria for any
every other year. Exclusion criteria included lifetime schizo- particular disorder; in the event of ambiguity, the inter-
phrenia, autism spectrum disorders, intellectual disability, viewer called parents again to obtain further information
and mood disorders secondary to other conditions. Control and/or clarification.
parents grouped-matched by age, sex, and neighborhood Lifetime (past, intake, and during follow-up) pharmaco-
were recruited from the community via telephone using ran- logical treatment was ascertained using the respective sec-
dom dialing. The exclusion criteria for the control parents tion in the KSADS.
were the same as those for the parents with BD, with the In keeping with procedures for research studies includ-
addition that biological parents and first- or second-degree ing school-aged children, after age 5 years, parents (about
relatives could not have BD. However, other psychiatric dis- their offspring) and offspring were directly interviewed
orders were permitted. Thus, control parents consisted of using the KSADS-PL. As the KSADS-PL did not include
healthy parents and parents with no-BD psychopathology. disruptive mood dysregulation disorder (DMDD), the diag-
Except for children with a condition that impeded their nosis of this disorder was conducted using modified criteria
participation in the study (eg, intellectual disability), all pre- derived from the KSADS-PL and described elsewhere.33
school offspring from each family were included. With the exception of an operationalized criterion for BD-
NOS derived from the Course and Outcome of Bipolar
Procedures Youth study (Table S1, available online),34 all diagnoses
The study was approved by the University of Pittsburgh were made using the DSM-IV. The k values for all disorders
Institutional Review Board. Informed consent was obtained ranged from 0.80 to 0.90.
1420 www.jaacap.org Journal of the American Academy of Child & Adolescent Psychiatry
Volume 60 / Number 11 / November 2021OFFSPRING OF BIPOLAR PARENTS
Approximately 75% of the assessments were conducted psychopathology and 45 offspring of 28 healthy parents)
in the subjects’ homes. Interviewers and investigators were with at least 1 follow-up were included. These 214 off-
blinded to parental diagnoses. spring, representing 95.5% of the original sample, were fol-
Socioeconomic status (SES) was ascertained using the lowed on average for 9.6 § 2.8 years (1.1 § 1.2 years
Hollingshead scale.35 between ages 2 and 5 years; 6.5 § 2.7 years after age 6
years; mean age at intake at last follow-up: 3.8 § 1.3 and
Statistical Analyses 13.4 § 3.1, respectively) and interviewed on average 5.5 §
Between-group comparisons of demographic and clinical 1.4 times (1.6 § 0.7 times between ages 2 and 5 years; 4.0
characteristics were evaluated using t tests, x2 tests, Fisher § 1.3 times during ages 6+ years). The retention rate at the
exact tests, analysis of variance, and linear mixed models (fit- last follow-up was 98%.
ting random intercept to account for within-subject correla-
tion across outcomes with repeated measures). Satterthwaite Biological Parents’ Demographic and Clinical
approximation was used in linear models to account for Characteristics
unequal group variances where applicable. BD and Control Parents. Parents with BD and parents
Group contrasts were first designed to compare parents with non-BD psychopathology had significantly lower SES
with BD, parents without BD, and healthy parents. Subse- than the healthy parents, and parents with non-BD psycho-
quently, offspring groups were compared on the risk to pathology were less likely to be married than were healthy
develop psychiatric disorders during follow-up via parents (Table S2, available online). All 3 parental groups
KaplanMeier survival analyses, then via Cox proportional significantly differed in psychosocial functioning (as mea-
hazards regression accounting for within-family correlation sured by the GAF) at intake and across follow-up (parents
via random intercept (ie, frailty modeling) and covarying for with BD lowest, healthy highest). Prevalence of each psychi-
demographic variables that showed group differences at a p atric disorder was significantly greater in parents with BD
value ofBIRMAHER et al.
TABLE 1 Demographic and Clinical Comparisons Among Preschool Offspring (25 Years of Age) of Parents With Bipolar
Disorder (BD), Preschool Offspring of Parents With Non-BD Psychopathology, and Preschool Offspring of Healthy Parents
Offspring of parents
Offspring of with non-BD Offspring of
parents with BD psychopathology healthy parents
Intake variables (n = 116) (n = 53) (n = 45) Statistic p
Age 3.8 §1.3 3.8§1.3 3.6 (1.2) F = 0.71 .5
Sex, male, % (n) 48.3 (56) 56.6 (30) 53.3 (34) x2 = 1.10 .6
Ethnicity, White, % (n) 81.0 (94) 69.8 (37) 88.9 (40) x2 = 5.72 .06
Living with both natural parents, % (n) 69.8 (81)z 66.0 (35)z 91.1 (41)x x2 = 9.45 .009
Mother's age at offspring’s birth 28.9 § 5.5z 28.4 § 6.6z 31.5 § 4.6x F = 4.39 .01
Father's age at offspring’s birth 31.2 § 6.7z,x 29.9 § 7.8z 33.8 § 6.7x F = 3.76 .02
Psychiatric disorders between ages 2 and 5 years, % (n) Fisher's exact test p
Any axis-I disordera 34.5 (40)z 13.2 (7)x 2.2 (1)xOFFSPRING OF BIPOLAR PARENTS
TABLE 2 Demographic and Clinical Comparisons Among Offspring of Parents With Bipolar Disorder (BD), Offspring of Parents
With Non-BD Psychopathology, and Offspring of Healthy Parents After They Became More Than 5 Years of Age (619 Years of
Age)
Offspring of parents
Offspring of with non-BD Offspring of
parents with BD psychopathology healthy parents
(n = 116) (n = 53) (n = 45)
Variables at last follow-up Statistic p
Age 13.0 § 3.5 13.9 § 2.9 13.8 § 2.3 F = 1.78 .2
Living with both natural parents, % (n) 38.8 (45)z 56.6 (30)z,x 71.1 (32)x x2 = 14.77 .0006
Duration of follow-up 9.2 § 3.1z 10.0 § 2.4z 10.2 § 2.0z F = 3.05 .05
Psychiatric disorders after age 5 years, % (n) Kaplan-Meier estimation
log-rank x2 p
Any axis-I disordera 69.8 (81)z 66.0 (35)x 31.1 (14)║ 29.89BIRMAHER et al.
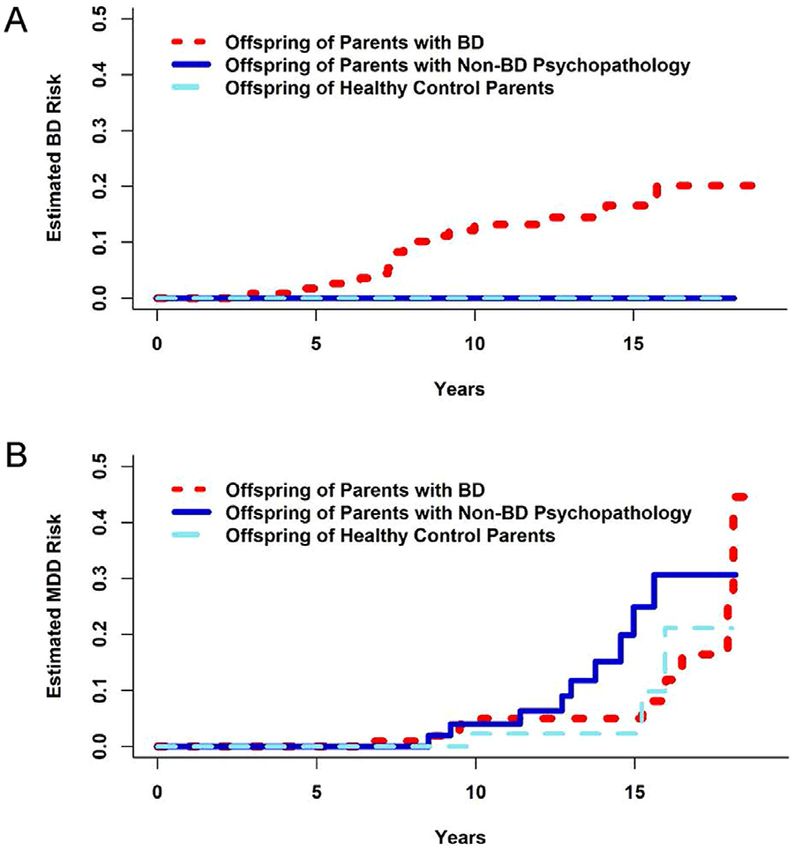
FIGURE 1 Cumulative Lifetime Risk of Developing (A) Regarding the pharmacological treatments after age 5
Bipolar Disorder (BD) and (B) Major Depressive Disorder years, for the entire sample, 26.2% (n = 56) received any
(MDD) in Offspring of Parents With BD and Community lifetime (past, intake, and follow-up) pharmacological treat-
Controls
ment, without significant differences among the 3 groups
(Table S4, available online). For specific medications, the
only significant finding was that the offspring of parents
with BD (9.5%, n = 12) were treated with more Second
Generation of Antipsychotics (SGAs) than the offspring of
healthy controls (0%, n = 1). There were no differences in
treatment with SGAs between offspring of parents with BD
and offspring of parents with non-BD psychopathology.
Factors Associated With Increased Risk for Developing
BD in Offspring of Parents With BD
Parental Factors. First, demographic and clinical differen-
ces between parents with BD whose offspring developed
BD versus parents with BD whose offspring did not develop
BD were analyzed to evaluate whether these differences
could account, at least in part, for the increased risk for their
offspring to develop BD. In comparison with parents with
BD with offspring who did not develop BD, parents with
BD with offspring with BD had significantly earlier age of
mood disorder onset and were significantly younger at
Note: Seventeen (14.3%) offspring of parents with BD developed BD with a mean intake (Table S5, available online). Furthermore, mothers
onset age = 8.3 § 3.2 years of age (log-rank x2 = 16.74, p = .0002). Ten (8.6%) off-
spring of parents with BD, 9 (17.0%) offspring of parents with non-BD psychopa-
and fathers of offspring with BD were both significantly
thology, and 3 (6.7%) offspring of healthy parents developed MDD with mean younger at the time of their offspring’s births than of non-
onset ages of 12.8 § 4.3, 12.6 § 2.5, and 13.6 § 3.4 years of age, respectively BD offspring’s births (p ≤ .04). There were no between-
(x2 = 2.75, p = .3). Please note color figures are available online.
group differences in any other parent/co-parent demo-
graphic and clinical characteristics.
Offspring Factors. In comparison with offspring of parents
future diagnosis of MDD. Of note, within the offspring of with BD who did not develop BD, those who did develop
non-BD parent group, those offspring of parents with BD had more any lifetime (before intake, intake, and
MDD (37 offspring of 23 parents) specifically had more follow-up) Axis-I disorders, ADHD, and ODD/DMDD
than 8 times the estimated hazard of developing MDD (all p valuesOFFSPRING OF BIPOLAR PARENTS
TABLE 3 Demographic and Clinical Characteristics in Offspring With and Without Bipolar Disorder (BD) of Parents With BD
Offspring with Offspring without
BD (n = 17) BD (n = 99)
Intake variables Statistic p
Age 4.3 § 1.2 3.7 § 1.3 t = 1.52 .1
Sex, male, % (n) 41.2 (7) 49.5 (49) x2 = 0.40 .5
Ethnicity, White, % (n) 70.6 (12) 82.8 (82) x2 = 1.41 .2
Living with both natural parents, %(n) 52.9 (9) 72.7 (72) x2 = 2.70 .1
Mother’s age at offspring's birth 26.4 § 5.2 29.4 § 5.5 t = 2.04 .04
Father’s age at offspring's birth 27.5 § 7.1 31.8 § 6.5 t = 2.41 .02
Psychosocial Functioning 60.4 § 12.3 72.4 § 14.1 t = 3.26 .002
Follow-up variables Statistic p
Duration of follow-up 10.1 § 2.2 9.1 § 3.3 t = 1.21 .2
Living with both natural parents at 64.7 (11) 73.7 (73) x2 = 0.59 .4
some point during follow-up, % (n)
Psychiatric disorders over follow-up, % (n) KaplanMeier estimation Cox proportional hazards regressiona
Log-rank x2 p Hazard ratio (95% CI) p
Any axis-I disorderb 100 (17) 66.7 (66) 14.75 .0001 2.67 (1.29, 5.50) .005
Depression 47.1 (8) 27.3 (27) 1.74 .2 1.19 (0.51, 2.76) .7
Any anxiety 58.8 (10) 33.3 (33) 3.62 .06 1.51 (0.63, 3.66) .3
ADHD 94.1 (16) 40.4 (40) 26.00BIRMAHER et al.
TABLE 4 Factors Predicting Bipolar Disorder (BD) Risk those in high-risk studies that recruited school-aged off-
Among Offspring of Parents With BD spring of parents with BD.2,3,5-8
After age 5 years, after adjusting for confounders, off-
Hazard ratio
Predictor (95% CI) Wald x2 p spring of parents with BD had more lifetime Axis-I psychi-
Sex, male 0.73 (0.28−1.92) 0.40 .5 atric disorders, BD, any anxiety disorders, ADHD, and
Ethnicity, White 0.47 (0.16−1.33) 2.04 .2 ODD/DMDD than offspring of healthy parents. However,
Living with both natural 0.43 (0.17−1.13) 2.95 .09 with the exception of BD and the observation that offspring
parents of parents with BD tended to develop disorders such
Mother’s age at 0.58 (0.34−1.00) 3.89 .05 ADHD and ODD earlier than offspring of non-BD
offspring’s birtha parents, there were no other differences between of these 2
Father’s age at 0.90 (0.82−0.98) 5.95 .02 groups of offspring. Interestingly, there were no between-
offspring’s birtha group differences in rates of offspring MDD, which was 8-
Socioeconomic statusa 0.53 (0.29−0.98) 4.09 .04
fold more common in offspring of parents with unipolar
Parental mood disorder 0.43 (0.22−0.83) 6.39 .01
depression. Similar to the literature, the above results indi-
onset agea,b
Parental functioninga 1.35 (0.74−2.45) 0.96 .33
cate the specificity of risk for BD development among off-
Any anxiety disorder 1.57 (0.36−6.87) 0.35 .6 spring of parents with BD.2-4,6-8
Attention-deficit/ 6.52 (2.47−17.22) 14.30 .0002 More specifically for BD, during an average of 9.2 years
hyperactivity disorderb of follow-up, offspring of parents with BD showed a cumu-
Oppositional defiant 3.74 (1.37−10.19) 6.63 .01 lative rate of BD of 14.7% (n = 17/116), which, taking into
disorder account the average age at last assessment (age 13 years), is
comparable to rates among the BIOS youths who were
Note: Boldface type indicates significant p values.
a
Estimated hazard ratios are standardized for continuous predictors. school-aged at intake.2,3,5 Most offspring BD were BD-
b
Attention-deficit/hyperactivity disorder and parental mood disorder NOS, which onset mainly during childhood and very rarely
onset age and were the only significant factors (p = .0009 and .04, before age 6 years, whereas BD-I/II onset mainly during
respectively) retained in combined model after backward selection (pOFFSPRING OF BIPOLAR PARENTS
ADHD, a finding similar to cross-sectional studies of BD from the symptoms of BD; this may lead to inappropriate
youth showing an age effect in rates of comorbid ADHD, psychosocial and/or pharmacological treatment, some of
with school-aged BD children having more ADHD (up to which may trigger the onset of BD.1 This highlights the
90%) as compared with adolescents and adults.40,41 need for a comprehensive assessment and close longitudinal
Of all the above factors, final models show that only follow-up to observe mood and behavioral fluctuations and
early parental mood onset and ADHD, particularly if it was clusters of hypomanic of manic symptoms above and
diagnosed before age 6 years, predicted BD. More specifi- beyond the symptoms of other psychopathology, which
cally, and consistent with the literature, offspring of parents may indicate BD.
whose age at mood disorder onset was 1 SD below the Regarding medications, as expected, the exposure to any
mean were estimated to have more than double the hazard medication increased with age (17.8%, 38/214) of the com-
of BD development.1 Of note, in our study, 75% (56/75) bined sample before age 5 years, and 26.2%, 56/214, after
of parents reported mood disorder onset before age 22 age 5), with most medications prescribed being stimulants.
years, and 24% (18/75) reported mood disorder onset Before and after age 5 years, there were no between-group
before age 12 years—rates that are very similar to those differences in any lifetime pharmacological treatments. For
reported in the BIOS study3 and in adult BD studies.42 specific medications, there were no between-group differen-
Other small, mainly cross-sectional studies in preschool ces before age 5 years. After age 5, except for offspring of
offspring of parents with BD also report higher rates of parents with BD having more lifetime treatment with SGAs
impulsivity and inattention when compared to offspring of in comparison with the offspring of healthy controls, there
controls.12-19 In the BIOS school-aged offspring study, off- were no other differences.
spring of parents with BD showed significantly increased Within the offspring of parents with BD, overall off-
risk for ADHD; however, this effect was nonsignificant after spring diagnosed with BD received more pharmacological
adjusting for covariates.2 Similar findings were reported in treatment than offspring without BD. However, in these
other longitudinal high-risk studies that included adoles- and the medication comparisons noted above, the number
cents and young adults of parents with BD.6,7,43 This infor- of offspring treated with medications, even after 9 years of
mation suggests that only ADHD symptomatology that follow-up, was too small for inferences to be made regarding
onsets during the preschool years is associated with pharmacological treatment. Moreover, the study was natu-
increased risk for developing BD among offspring of parents ralistic and subject to “confounds by indication.”
with BD. Whether these symptoms are indeed ADHD or The results of this study should be considered in light of
prodromal symptoms of BD deserves further investigation. the following limitations. Although this is a prospective lon-
Investigations that evaluate whether youths diagnosed gitudinal study, the diagnoses and estimates of onset age
with ADHD are at risk for developing BD can also inform were made retrospectively for the interval between assess-
our understanding of the association between these 2 ments. From age 2 to 5 years, offspring were evaluated
disorders. However, results from such studies are through parental information and not direct observation.
inconsistent.2,44,45 For example, the Multimodal Treatment Most of the sample were White, reflecting the demographics
Study did not find that ADHD is associated with increased of the area where the study was conducted. In addition, off-
risk for developing BD but that it is associated with the spring were not through the peak age of risk for developomg
development of some manic symptoms. 45 In contrast, a mood disorders. As most parents with BD had early-onset
recent longitudinal study reported higher incidence rates of BD, the results of this study may not pertain to parents
BD among individuals with history of ADHD.46 Also, a with BD with late-onset BD. Finally, because only 17 off-
study of 13,532 twin pairs (912 years of age) found that spring developed BD, Cox regression analyses were gener-
ADHD and hypomanic symptoms were associated with ally underpowered, and addition of variables such as
shared genetic factors.47 Of note, most longitudinal ADHD parental non-mood disorders to the predictive analysis was
studies have not examined whether having a family history not possible. However, no parental non-mood disorders
of BD increases the risk of BD in youths with ADHD. were significant univariate predictors of offspring BD risk.
Except for SUD, about 71% (12/17) of the non-BD In conclusion, having a parent with psychopathology
disorders (mainly ADHD, followed by ODD/DMDD, anx- generally increased offspring risk for psychiatric disorders
iety, and dysthymia/depression-NOS) predated the onset of from an early age, particularly ADHD, ODD, and anxiety
BD, and these disorders onset earlier than in the other 2 disorders. However, although a relatively small group devel-
control groups. This is a clinically relevant finding, because oped BD, only offspring of parents with BD demonstrated
some symptoms of other disorders, especially ADHD and increased rates of BD, in particular those offspring of
other behavioral disorders, may be difficult to differentiate parents with BD who were more than 6 years of age who
Journal of the American Academy of Child & Adolescent Psychiatry www.jaacap.org 1427
Volume 60 / Number 11 / November 2021BIRMAHER et al.
showed symptoms of ADHD during the preschool years Author Contributions
Conceptualization: Birmaher, B. Goldstein, Diler, Monk, Iyengar, Axelson, T.
and whose parents had early-onset BD. Symptoms of BD Goldstein
were scarce among offspring during the preschool years, but Data curation: Birmaher, Merranko, Monk, Hickey, Axelson
Formal analysis: Birmaher, Merranko, Hafeman, B. Goldstein, Diler, Levenson,
increased throughout the school-age period, mainly in the Iyengar, Axelson, T. Goldstein
form of BD-NOS. However, as all subtypes of BD are asso- Funding acquisition: Birmaher, Monk, Axelson
Investigation: Birmaher, Merranko, Hafeman, B. Goldstein, Diler, Monk, Sakol-
ciated with poor psychosocial functioning and increased sky, Axelson, T. Goldstein
Methodology: Birmaher, Monk, Iyengar, Hickey, Axelson, T. Goldstein
risk for suicidality and substance abuse, and as BD-NOS Project administration: Birmaher, Monk, Axelson
conveys high risk for BD-I/II, developing early interven- Resources: Birmaher, Monk, Axelson
Software: Merranko, Hickey
tions to delay or, in the best of cases, prevent its onset are Supervision: Birmaher, Hafeman, Monk, Sakolsky, Axelson, T. Goldstein
warranted.1,34,48,49 As in the literature, offspring of parents Validation: Birmaher, Merranko, Hafeman, B. Goldstein, Diler, Monk, Sakol-
sky, Axelson, T. Goldstein
with BD also had other non-BD disorders, especially Visualization: Birmaher, Merranko, Hafeman, B. Goldstein, Diler, Monk, Sakol-
ADHD and ODD, that usually predated the onset of BD1,2 sky, Axelson, T. Goldstein
Writing − original draft: Birmaher, Axelson
and that also require identification and treatment, as well as Writing − review and editing: Birmaher, Merranko, Hafeman, B. Goldstein,
fostering of research regarding the most appropriate phar- Diler, Levenson, Monk, Iyengar, Hickey, Sakolsky, Axelson, T. Goldstein
macological management to avoid triggering mania/ The authors would like to thank the studies’ participants and their families, the
research assistants, and Rita Scholle, BA, of the University of Pittsburgh Medi-
hypomania.48,50,51 Moreover, BD youths are at high risk cal Center, for preparation of the manuscript. The authors would also like to
for developing SUD, thus providing a window of opportu- acknowledge Stacia Friedman-Hill, PhD, of NIMH, for her continued encour-
agement and support.
nity to prevent this disorder.52 Finally, as consistently
Disclosure: Dr. Birmaher has received grants from NIMH, during the conduct
reported in the adult literature,53 parents with BD had other of the study, and royalties from Random House, UpToDate, and Lippincott,
psychiatric disorders that, in addition to BD, required iden- Williams, and Wilkins, outside of the submitted work. Dr. Hafeman has
received grants from NIMH and the Brain and Behavior Research Foundation.
tification and treatment. This is important, because success- Dr. B. Goldstein has received grant funding from Brain Canada, the Canadian
ful treatment of parental psychopathology not only helps Institutes of Health Research, the Heart and Stroke Foundation of Canada,
NIMH, and the departments of psychiatry of Sunnybrook Health Sciences
parents but improves the prognosis in their offspring.51 Centre and the University of Toronto. Dr. Diler has received research support
from NIMH. Dr. Levenson has received grant support from the Eunice Ken-
nedy Shriver National Institute of Child Health and Human Development, the
Accepted February 19, 2021. National Institute on Drug Abuse, and the University of Pittsburgh and royal-
Drs. Birmaher, Hafeman, Diler, Levenson, Sakolsky, Goldstein, Mr. Merranko, ties from American Psychological Association Books. Dr. Sakolsky has
and Mss. Monk and Hickey are with Western Psychiatric Hospital, University of received grant support from NIMH. Dr. Axelson has received grants from
Pittsburgh School of Medicine, Pennsylvania. Dr. Goldstein is with the Center NIMH, during the conduct of the study, and royalties from Wolters-Kluwer /
for Addiction and Mental Health, University of Toronto Faculty of Medicine, UpToDate, outside the submitted work. Dr. T. Goldstein has received grants
Ontario, Canada. Dr. Iyengar is with the University of Pittsburgh, Pennsylvania. from NIMH, the American Foundation for Suicide Prevention, the University
Dr. Axelson is with Nationwide Children’s Hospital and The Ohio State Col- of Pittsburgh Clinical and Translational Science Institute (CTSI), and the Brain
lege of Medicine, Columbus. and Behavior Foundation and royalties from Guilford Press, outside the sub-
mitted work. Dr. Iyengar, Mr. Merranko, and Mss. Monk and Hickey have
This paper was supported by National Institute of Mental Health (NIMH) grant reported no biomedical financial interests or potential conflicts of interest.
RO1 MH060952. The work was completed at Department of Psychiatry, Western
Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine. This Correspondence to Boris Birmaher, MD, Western Psychiatric Hospital, 3811
manuscript represents original material that has never been published before, is O’Hara Street, Bellefield Towers − Room 612, Pittsburgh, PA 15213; e-mail:
not under consideration for publication elsewhere, and has been approved by birmaherb@upmc.edu
each author. 0890-8567/$36.00/© 2021 American Academy of Child & Adolescent Psychia-
Dr. Merranko served as the statistical expert for this research. try. Published by Elsevier Inc. All rights reserved
https://doi.org/10.1016/j.jaac.2021.02.023
REFERENCES 7. Preisig M, Strippoli MF, Castelao E, et al. The specificity of the familial aggregation of
early-onset bipolar disorder: a controlled 10-year follow-up study of offspring of parents
1. Birmaher B. Bipolar disorders. In: Martin A, Volkmar FR, eds. Lewis's Child and Adolescent
with mood disorders. J Affect Disord. 2016;190:26-33.
Psychiatry: A Comprehensive Textbook. 5th ed.Philadelphia: Wolters Kluwer; 2018.
8. Van Meter AR, Burke C, Youngstrom EA, Faedda GL, Correll CU. The bipolar pro-
2. Axelson D, Goldstein B, Goldstein T, et al. Diagnostic precursors to bipolar disorder in
drome: meta-analysis of symptom prevalence prior to initial or recurrent mood episodes.
offspring of parents with bipolar disorder: a longitudinal study. Am J Psychiatry.
J Am Acad Child Adolesc Psychiatry. 2016;55(7):543-555.
2015;172:638-646.
9. Zwicker A, Drobinin V, MacKenzie LE, et al. Affective lability in offspring of parents
3. Birmaher B, Axelson D, Monk K, et al. Lifetime psychiatric disorders in school-aged off-
with major depressive disorder, bipolar disorder and schizophrenia. Eur Child Adolesc
spring of parents with bipolar disorder: the Pittsburgh Bipolar Offspring study. Arch Gen
Psychiatry. 2020;29:445-451.
Psychiatry. 2009;66:287-296.
10. Luby JL, Barch DM, Whalen D, Tillman R, Freedland KE. A randomized controlled
4. Duffy A, Horrocks J, Doucette S, Keown-Stoneman C, McCloskey S, Grof P. The devel-
trial of parent-child psychotherapy targeting emotion development for early childhood
opmental trajectory of bipolar disorder. Br J Psychiatry. 2014;204:122-128.
depression. Am J Psychiatry 2018. appiajp201818030321.
5. Hafeman DM, Merranko J, Axelson D, et al. Toward the definition of a bipolar pro-
11. Uher R, Cumby J, MacKenzie LE, et al. A familial risk enriched cohort as a platform for
drome: dimensional predictors of bipolar spectrum disorders in at-risk youths. Am J Psy-
testing early interventions to prevent severe mental illness. BMC Psychiatry.
chiatry. 2016;173:695-704.
2014;14:344.
6. Mesman E, Nolen WA, Reichart CG, Wals M, Hillegers MH. The Dutch bipolar off-
12. Dilsaver SC, Akiskal HS. Preschool-onset mania: incidence, phenomenology and family
spring study: 12-year follow-up. Am J Psychiatry. 2013;170:542-549.
history. J Affect Disord. 2004;82(Suppl 1):S35-S43.
1428 www.jaacap.org Journal of the American Academy of Child & Adolescent Psychiatry
Volume 60 / Number 11 / November 2021OFFSPRING OF BIPOLAR PARENTS
13. Hirshfeld-Becker DR, Biederman J, Henin A, Faraone SV, Cayton GA, Rosenbaum JF. 33. Sparks GM, Axelson DA, Yu H, et al. Disruptive mood dysregulation disorder and
Laboratory-observed behavioral disinhibition in the young offspring of parents with chronic irritability in youth at familial risk for bipolar disorder. J Am Acad Child Adolesc
bipolar disorder: a high-risk pilot study. Am J Psychiatry. 2006;163:265-271. Psychiatry. 2014;53:408-416.
14. Hirshfeld-Becker DR, Biederman J, Henin A, et al. Psychopathology in the young 34. Axelson DA, Birmaher B, Strober MA, et al. Course of subthreshold bipolar disorder in
offspring of parents with bipolar disorder: a controlled pilot study. Psychiatry Res. youth: diagnostic progression from bipolar disorder not otherwise specified. J Am Acad
2006;145:155-167. Child Adolesc Psychiatry. 2011;50:1001-1016.e1003.
15. Luby J, Belden A. Defining and validating bipolar disorder in the preschool period. Dev 35. Hollingshead A. Index of Social Status. In: Mangen DJ, PW, eds. Research Instuments in
Psychopathol. 2006;18:971-988. Social Gerontology. Vol 2. Minneapolis, MN: University of Minnesota Press; 1982.
16. Radke-Yarrow M, Nottelmann E, Martinez P, Fox MB, Belmont B. Young children of 36. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing
affectively ill parents: a longitudinal study of psychosocial development. J Am Acad Child risk. J Am Stat Assoc. 1999;94:496-509.
Adolesc Psychiatry. 1992;31:68-77. 37. Axelson D, Findling RL, Fristad MA, et al. Examining the proposed disruptive mood
17. Tumuluru RV, Weller EB, Fristad MA, Weller RA. Mania in six preschool children. dysregulation disorder diagnosis in children in the Longitudinal Assessment of Manic
J Child Adolesc Psychopharmacol. 2003;13:489-494. Symptoms study. J Clin Psychiatry. 2012;73:1342-1350.
18. Zahn-Waxler C, Chapman M, Cummings EM. Cognitive and social development 38. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Obser-
in infants and toddlers with a bipolar parent. Child Psychiatry Hum Dev. 1984;15: vational Studies in Epidemiology (STROBE): explanation and elaboration. Int J Surg.
75-85. 2014;12:1500-1524.
19. Zahn-Waxler C, Mayfield A, Radke-Yarrow M, McKnew DH, Cytryn L, Davenport YB. 39. Egger HL, Angold A. Common emotional and behavioral disorders in preschool children:
A follow-up investigation of offspring of parents with bipolar disorder. Am J Psychiatry. presentation, nosology, and epidemiology. J Child Psychol Psychiatry. 2006;47:313-337.
1988;145:506-509. 40. Axelson D, Birmaher B, Strober M, et al. Phenomenology of children and adolescents
20. Birmaher B, Axelson D, Goldstein B, et al. Psychiatric disorders in preschool offspring of with bipolar spectrum disorders. Arch Gen Psychiatry. 2006;63:1139-1148.
parents with bipolar disorder: the Pittsburgh Bipolar Offspring Study (BIOS). Am J Psy- 41. Singh MK, DelBello MP, Kowatch RA, Strakowski SM. Co-occurrence of bipolar and
chiatry. 2010;167:321-330. attention-deficit hyperactivity disorders in children. Bipolar disorders. 2006;8:710-720.
21. Maoz H, Goldstein T, Axelson DA, et al. Dimensional psychopathology in pre- 42. Perlis RH, Dennehy EB, Miklowitz DJ, et al. Retrospective age at onset of bipolar disor-
school offspring of parents with bipolar disorder. J Child Psychol Psychiatry. der and outcome during two-year follow-up: results from the STEP-BD study. Bipolar
2014;55:144-153. Disord. 2009;11:391-400.
22. Spitzer RL, Williams JB, Gibbon M, First MB. The Structured Clinical Interview for 43. Duffy A, Goodday S, Keown-Stoneman C, Grof P. The emergent course of bipolar disor-
DSM-III-R (SCID). I: history, rationale, and description. Arch Gen Psychiatry. der: observations over two decades from the Canadian High-Risk Offspring Cohort. Am
1992;49:624-629. J Psychiatry. 2019;176:720-729.
23. Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophre- 44. Arnold LE, Van Meter AR, Fristad MA, et al. Development of bipolar disorder and other
nia for School-Age ChildrenPresent and Lifetime Version (K-SADS-PL): initial reliabil- comorbidity among youth with attention-deficit/hyperactivity disorder. J Child Psychol
ity and validity data [See comment]. J Am Acad Child Adolesc Psychiatry. 1997;36:980- Psychiatry. 2020;61:175-181.
988. 45. Elmaadawi AZ, Jensen PS, Arnold LE, et al. Risk for emerging bipolar disorder, variants,
24. Endicott J, Spitzer RL, Fleiss JL, Cohen J. The Global Assessment Scale. A procedure for and symptoms in children with attention deficit hyperactivity disorder, now grown up.
measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry. 1976;33:766-771. World J Psychiatry. 2015;5:412-424.
25. Andreasen NC, Endicott J, Spitzer RL, Winokur G. The family history method using 46. Meier SM, Pavlova B, Dalsgaard S, et al. Attention-deficit hyperactivity disorder and anx-
diagnostic criteria. Reliability and validity. Arch Gen Psychiatry. 1977;34:1229-1235. iety disorders as precursors of bipolar disorder onset in adulthood. Br J Psychiatry.
26. Birmaher B, Ehmann M, Axelson DA, et al. Schedule for Affective Disorders and Schizo- 2018;213:555-560.
phrenia for School-age Children (K-SADS-PL) for the assessment of preschool children 47. Hosang GM, Lichtenstein P, Ronald A, Lundstrom S, Taylor MJ. Association of genetic
—a preliminary psychometric study. J Psychiatr Res. 2009;43:680-686. and environmental risks for attention-deficit/hyperactivity disorder with hypomanic
27. Henin A, Biederman J, Mick E, et al. Psychopathology in the offspring of parents with symptoms in youths. JAMA Psychiatry. 2019;76:1150-1158.
bipolar disorder: a controlled study. Biol Psychiatry. 2005;58:554-561. 48. Miklowitz DJ, Chang KD. Prevention of bipolar disorder in at-risk children: theoretical
28. Kashani JH, Allan WD, Beck Jr. NC, Bledsoe Y, Reid JC. Dysthymic disorder in clinically assumptions and empirical foundations. Dev Psychopathol. 2008;20:881-897.
referred preschool children. J Am Acad Child Adolesc Psychiatry. 1997;36:1426-1433. 49. Sullivan AE, Judd CM, Axelson DA, Miklowitz DJ. Family functioning and the course of
29. Keenan K, Wakschlag LS. Are oppositional defiant and conduct disorder symptoms nor- adolescent bipolar disorder. Behav Ther. 2012;43:837-847.
mative behaviors in preschoolers? A comparison of referred and nonreferred children. Am 50. Goldstein TR, Merranko J, Krantz M, et al. Early intervention for adolescents at-risk for
J Psychiatry. 2004;161:356-358. bipolar disorder: a pilot randomized trial of Interpersonal and Social Rhythm Therapy
30. Kim-Cohen J, Arseneault L, Caspi A, Tomas MP, Taylor A, Moffitt TE. Validity of (IPSRT). J Affect Disord. 2018;235:348-356.
DSM-IV conduct disorder in 41/2-5-year-old children: a longitudinal epidemiological 51. Weissman MM, Pilowsky DJ, Wickramaratne PJ, et al. Remissions in maternal depres-
study. Am J Psychiatry. 2005;162:1108-1117. sion and child psychopathology: a STAR*D-child report. JAMA. 2006;295:1389-1398.
31. Luby JL, Mrakotsky C, Heffelfinger A, Brown K, Hessler M, Spitznagel E. Modification 52. Goldstein BI, Strober M, Axelson D, et al. Predictors of first-onset substance use
of DSM-IV criteria for depressed preschool children. Am J Psychiatry. 2003;160:1169- disorders during the prospective course of bipolar spectrum disorders in adolescents.
1172. J Am Acad Child Adolesc Psychiatry. 2013;52:1026-1037.
32. Scheeringa MS, Peebles CD, Cook CA, Zeanah CH. Toward establishing procedural, cri- 53. Post RM, Leverich GS, Kupka R, et al. Increased parental history of bipolar disorder in
terion, and discriminant validity for PTSD in early childhood. J Am Acad Child Adolesc the United States: association with early age of onset. Acta Psychiatr Scand. 2014;129:
Psychiatry. 2001;40:52-60. 375-382.
Journal of the American Academy of Child & Adolescent Psychiatry www.jaacap.org 1429
Volume 60 / Number 11 / November 2021You can also read