A clinical study of peripherally inserted central catheter related venous thromboembolism in patients with hematological malignancies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
www.nature.com/scientificreports
OPEN A clinical study of peripherally
inserted central catheter‑related
venous thromboembolism
in patients with hematological
malignancies
1,2 1,2 1* 1 1 1 1
Jing Yue , Ya Zhang , Fang Xu , Ai Mi , Qiaolin Zhou , Bin Chen & Lin Shi
This study aimed to explore the risk factors of peripherally inserted central catheter (PICC)-related
venous thromboembolism (CRT) in patients with hematological malignancies and the predictive ability
of the thrombotic risk assessment models (RAMs). The clinical data of the 117 eligible patients with
hematological neoplasms at Mianyang Central Hospital with PICC from May 2018 to May 2020 were
analyzed in this retrospective study. Thrombosis risk scores were calculated in patients with image-
confirmed PICC-related thromboembolism. CRT occurred in 19 cases. Compared to the CRT-free group,
the CRT group was older and showed higher body mass index (BMI), leukocyte count level, and the
prevalence of diabetes mellitus. Multivariable logistic regression analysis showed that BMI (P = 0.03)
was a significant risk factor for CRT. The area under the receiver operating characteristic curve for the
Caprini scale (P = 0.01) was higher than that of the modified Wells scale (P = 0.94), the revised Geneva
scale (P = 0.83), Padua scale (P = 0.59), and Michigan scale (P = 0.80). The sensitivity and specificity for
the Caprini scale, Padua scale, modified Wells scale, the revised Geneva scale, and Michigan risk score
were 63.3%/73.7%, 100%/0.00%, 95.9%/5.3%, 31.6%/73.7%, and 1.0%/99.0%, respectively. Caprini
RAM had a better predictive ability for CRT in patients with hematological malignancies. Michigan risk
score may not be better than Caprini RAM in this population.
A peripherally inserted central catheter is widely used for patients with hematologic malignancies due to sim-
ple insertion procedures, long dwell time, and easy maintenance protocol. It is a safe, convenient, economical,
and less painful infusion method. A PICC is suitable for infusion of chemotherapeutic agents, nutrition, blood
products, high concentration medicine, and other cytotoxic agents to avoid peripheral blood vessel impairment,
tissue necrosis, or local phlebitis caused by drug e xtravasation1–3. One of the foremost complications related to
PICC is catheter-related vein thrombosis (CRT)4, with an incidence of 0%–71.9%3,5,6. In addition to pain and
discomfort related to the c atheter7, CRT may result in extra financial burden, treatment delay or interruption,
and fatal c onsequences8. For now, however, there is no generally accepted risk prediction model for CRT. For
patients with hematological malignancies, biological characteristics of tumors are baseline factors leading to CRT.
Compared to solid tumors, concomitant severe thrombocytopenia, coagulopathy, and bone marrow suppression
make the application of prophylactic measures challenging for CRT. Therefore, the risk prediction of CRT in
hematologic malignancy patients is rather complicated. Thus, it is necessary to investigate the CRT-related risk
factors and prediction models for hematology patients.
This retrospective study reviewed hemato-oncology patients with PICC insertion and explored the risk fac-
tors of CRT in hematological cancer patients and examined the predictive value of the traditional thrombotic
risk assessment models for CRT.
1
Department of Hematology, Mianyang Central Hospital, School of Medicine, University of Electronic Science and
Technology of China, Mianyang 621000, China. 2These authors contributed equally: Jing Yue and Ya Zhang. *email:
147377807@qq.com
Scientific Reports | (2022) 12:9871 | https://doi.org/10.1038/s41598-022-13916-5 1
Vol.:(0123456789)www.nature.com/scientificreports/
Methods
Study population. This retrospective study of 117 patients with hematological malignancies having PICC
insertion at Mianyang Central Hospital (Mianyang, China) from May 2018 to May 2020. The malignancies,
including leukemia, malignant lymphoma, myelodysplastic syndrome, and multiple myeloma, were confirmed
through auxiliary examinations, such as bone marrow morphology, bone marrow flow cytometry, and lymph
node biopsy. The inclusion criteria were as follows: diagnosed with a hematological tumor and needed PICC
catheterization. The exclusion criteria were as follows: patients aged < 14-years-old and lost to during the fol-
low-up. The study was approved by the Ethics Committee of Mianyang Central Hospital (approval number:
S2021077). Written informed consent was obtained from parents or guardians of the participants who are less
than 16 years old involved in the study.
Data collection. Patient-related characteristics at baseline and several potential risk factors of CRT reported
in the literature were collected: general conditions (gender, age, and body mass index (BMI)), disease states and
comorbidities (hematological tumor type, smoking, drinking, diabetes, hyperlipidemia, infection status, and
history of thrombosis), biochemical indexes (platelets, fibrinogen concentration, prothrombin time, activated
partial thromboplastin time, and kidney function), catheter-related data (vein entry and laterality), exposure to
blood products and special medications (blood component, human serum albumin, plasma fibrinogen, erythro-
poietin, and parenteral nutrition). These were classified as CRT groups and no CRT groups based on whether or
not PICC-related venous thromboembolism was formed.
Thrombosis risk assessment scales for reference. Several risk scoring tools9–13 were applied to assess
the thrombosis risk before PICC catheterization in all participants, and the cumulative score for each patient
was then calculated.
Detecting venous thrombosis. This research defined CRT as thrombosis involving the peripherally
inserted central catheter-associated upper extremity deep vein thrombosis and mural thrombosis. Symptoms
include redness, swelling, heat, and pain at the catheter arm, intravenous transfusion obstacle, or the catheter
indwelling time for over a year. CRT was confirmed by vascular ultrasound.
PICC insertion and maintenance. All PICC catheterizations had been operated on under ultrasound
guidance by an experienced and qualified professional nurse. All PICCs used in this study were single-lumen
catheters (PowerPICC, Bard Access Systems, Inc., Salt Lake City, Utah, USA) with a model of 4-French and were
routinely maintained by PICC specialist nurses using sterile technique weekly. A 45% catheter-to-vein ratio
limit was used when inserting PICC devices. All the procedures were performed in accordance with the PICC
specifications. PICC tip position at the cavoatrial junction is all confirmed via X-ray.
Statistical analysis. Categorical variables were expressed as frequencies and percentages and compared
between the groups using the chi-square test. Continuous variables were presented as mean ± standard devia-
tion. An independent-sample t-test or Mann–Whitney U test was used to compare the difference between the
groups. A binary logistic regression model was utilized to examine the association between risk factors and
CRT . Receiver operating characteristic (ROC) curves were plotted according to the sensitivity and specificity of
RAMs, and the area under the curve (AUC) and 95% confidence interval (CI) were also calculated. P < 0.05 was
considered statistically significant. Statistical analysis was done with SPSS software (IBM Corp, Released 2016,
IBM SPSS Statistics for Windows, version 24.0, Armonk, NY, USA).
Ethical approval and consent to participate. Written informed consent prior to and regarding the
treatment protocol was obtained from all patients analyzed in the present study. The procedures used in this
study adhere to the tenets of the Declaration of Helsinki.
Consent for Publication. Informed consent was obtained from all individual participants included in the
study.
Results
General characteristics of CRT and no CRT cases. A total of 117 participants, including 63 men
(53.4%) and 54 women (45.8%), with a median age of 54 (range: 15–90 years), were included in this study. 19/117
(16.2%) patients were verified as developing PICC-related venous thromboembolism. Of these cases, 14 were
mural thrombosis and 5 were deep venous thrombosis. Compared to no CRT patients, CRT patients presented
significant differences in median age(P = 0.04), the prevalence of diabetes mellitus(P = 0.04), BMI(P = 0.007),
white blood cell count(P = 0.04), and prothrombin time(P = 0.03). On the other hand, no differences were
detected in gender, disease states, comorbidities, biochemical indexes, catheter-related data, exposure to blood
products, and special medications (Table 1).
Multivariate correlations between risk factors and CRT. Univariate analysis showed that age, BMI,
white blood cell count, prothrombin time, the prevalence of diabetes mellitus, the incidence of hypertension,
and the rates of grade 3 or 4 infections were potential predictive risk factors. These factors were entered in a
binary logistic regression analysis. Results showed that BMI (OR = 1.315, 95% CI: 1.033–1.674, P = 0.03) and pro-
thrombin time (OR = 0.279, 95% CI: 0.097–0.802, P = 0.02) were the independent risk factors for CRT (Table 2).
Scientific Reports | (2022) 12:9871 | https://doi.org/10.1038/s41598-022-13916-5 2
Vol:.(1234567890)www.nature.com/scientificreports/
Patients without CRT Patients with CRT
Variables (n = 98) (n = 19) P-value
Age, years 51.2 ± 17.6 60.2 ± 15.0 0.039*
Gender (Male/Female), n 54/44 9/10 0.536
BMI, kg/m2 22.6 ± 4.2 25.68 ± 4.1 0.007*
Cancer
Acute leukemia, n (%) 50 (51.00) 8 (42.10) N/A
Lymphoma, n (%) 37 (37.80) 9 (47.40)
Plasma cell disease, n (%) 4 (4.10) 2 (10.50)
Other hematological malignancies, n (%) 7 (7.10) 0 (0.00)
Cell origin
Myeloid, n (%) 42 (42.9) 5 (26.3) 0.335
B cell, n (%) 49 (50.0) 13 (68.4)
T/NK cell, n (%) 7 (7.1) 1 (5.3)
Smoking, n (%) 20 (20.4) 3 (15.8) 0.762
Drinking, n (%) 12 (12.2) 2 (10.5) 1.000
Hypertension, n (%) 6 (6.1) 4 (21.1) 0.056
Diabetes, n (%) 8 (8.2) 5 (26.3) 0.037*
Hyperlipidemia, n (%) 4 (4.1) 1 (5.3) 1.000
infection(grade ≥ 3) , n (%) 55 (56.1) 6 (31.6) 0.050
Blood products transfusion, n (%) 83 (84.7) 14 (73.7) 0.315
Erythropoietin use, n (%) 4 (4.1) 0 (0.0) 1.000
Parenteral nutrition support, n (%) 49 (50.0) 7 (36.8) 0.293
Catheter placement(left/right), n 45/53 9/10 1.000
Vessel puncture
Basilic vein, n (%) 81 (82.7) 14 (73.7) N/A
Median cubital vein, n (%) 13 (13.3) 4 (21.1)
Saphenous vein, n (%) 4 (4.1) 1 (5.3)
Biochemical indexes of PICC catheterization
WBC count, × 109/L 16.58 ± 44.49 24.20 ± 33.55 0.042*
Platelet, × 109/L 118.5 ± 105.5 133.5 ± 69.9 0.566
Fibrinogen, g/L 3.3 ± 1.4 3.3 ± 1.29 0.950
PT, s 12.6 ± 1.2 12.0 ± 1.5 0.025*
APTT, s 29.7 ± 6.5 27.2 ± 3.9 0.141
Creatinine, mmol/L 68.7 ± 81.7 75.3 ± 52.3 0.744
Glomerular filtration rate, mL/min/1.7 74.1 ± 22.5 74.1 ± 27.2 0.994
Creatinine clearance, mL/min 106.4 ± 41.3 96.3 ± 30.6 0.356
Table 1. Clinical features of hematological malignancy patients with and without CRT. BMI Body mass
index, PICC Peripherally inserted central catheter, CRTPeripherally inserted central catheter -related venous
thromboembolism, WBC White blood cell, PT Prothrombin time, APPT Activated partial thromboplastin
time. *Statistically significant.
OR 95% CI P-value
Age 1.032 0.964–1.105 0.361
BMI 1.315 1.033–1.674 0.026
Diabetes 0.306 0.039–2.397 0.260
Hypertension 0.188 0.012–2.858 0.229
Infection (grade ≥ 3) 1.538 0.325–7.284 0.588
WBC count 0.998 0.985–1.010 0.707
Prothrombin time 0.279 0.097–0.802 0.018
Table 2. Risk Factors associated with PICC-associated venous thromboembolism (multivariate logistic
regression analysis). BMI Body mass index, PICC Peripherally inserted central catheter, WBC White blood
cell. Variables that had a P-value < 0.10 (age, BMI, diabetes, hypertension, PICC-related infections, WBC) in
univariable analysis were selected for inclusion in the multivariable model.
Scientific Reports | (2022) 12:9871 | https://doi.org/10.1038/s41598-022-13916-5 3
Vol.:(0123456789)www.nature.com/scientificreports/
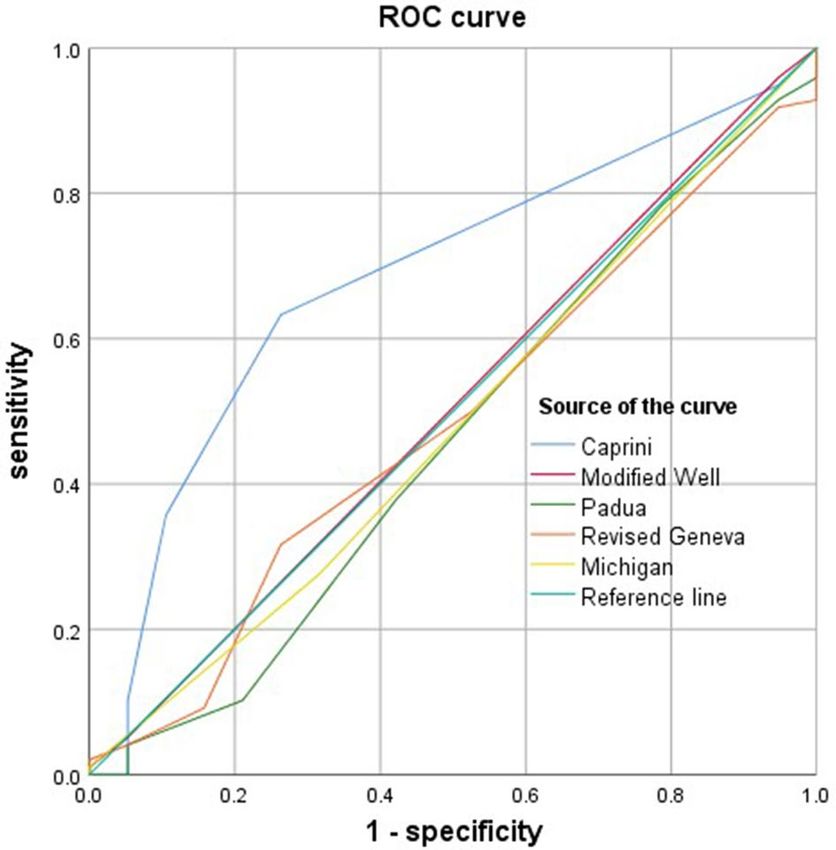
Figure 1. ROC curves of the five different thrombosis risk assessment scales.
Scales AUC Sensitivity (%) Specificity (%) Youden index (%)
Caprini 0.557–0.808 63.3 73.7 37.0
Padua 0.312–0.610 100.0 0.0 0.0
Modified Wells 0.362–0.649 95.9 5.3 1.2
Revised Geneva 0.345–0.624 31.6 73.7 5.3
Michigan 0.338–0.625 1.0 99.0 1.0
Table 3. Comparison of the five different thrombosis risk assessment scales in predicting the occurrence risk
of CRT in patients with hematological cancers.
Predictive capability of different risk assessment scales for CRT. Patients’ risk scores were cal-
culated using the Caprini scale, Padua scale, modified Wells scale, revised Geneva scale, and Michigan risk
score. Subsequently, the ROC curves were plotted and used to assess the validity of different thrombosis risk
assessment scales of CRT. The AUC value for Caprini scale (0.683, 95% CI: 0.557–0.808, P = 0.01) was higher
than that for modified Wells scale (0.505, 95% CI: 0.362–0.649, P = 0.94), revised Geneva scale (0.485, 95% CI:
0.345–0.624, P = 0.83), Padua scale (0.461, 95% CI: 0.312–0.610, P = 0.59), and Michigan scale (0.481, 95% CI:
0.338–0.625, P = 0.80) (Fig. 1). The sensitivity and specificity for Caprini scale, Padua scale, modified Wells scale,
the revised Geneva scale, Michigan risk score were 63.3%/73.7%, 100%/0.00%, 95.9%/5.3%, 31.6%/73.7%, and
1.0%/99.9%, respectively. Interestingly, the Caprini assessment scale was more accurate than the Padua scale,
modified Wells scale, the revised Geneva scale, and Michigan risk score for predicting CRT; 5.5 was the best
cutoff point for Caprini, with a sensitivity of 0.633 and a specificity of 0.737 (Table 3).
Discussion
CRT is defined as a blood clot formed around the external portion of the catheter or internal portion of the vas-
cular walls. Consequently, the risk of VTE may be higher for hematological malignancy patients than for those
with solid tumors; this phenomenon could be attributed to multiple factors, such as the nature of neoplasm,
aging population, and co-morbidities. Hematologic tumor patients are more likely to have CRT than solid
tumors, with a rate of 1.9–18.7%1,14,15. In this research, 12.0% of patients were the peripherally inserted central
catheter-associated mural thrombosis and 4.2% were deep venous thrombosis, which is consistent with the
findings from previous studies. CRT could lead to phlebitis, vascular stenosis, pulmonary embolism, and could
even be life-threatening16. On the other hand, CRT in hemato-oncology patients has specific characteristics.
The practical implementation of the thromboprophylaxis measures for CRT is complicated in hematological
cancer patients, who have a high risk of hemorrhage resulting from thrombocytopenia, coagulopathy, or bone
marrow suppression.
The present study explored the CRT-related clinical risk factors. Advanced age, BMI, history of diabetes
mellitus, hypertension history, leukocyte count, prothrombin time, and grade 3 or 4 infections were identi-
fied as putative risk factors for patients with hematologic tumors. Various studies supported different clinical
Scientific Reports | (2022) 12:9871 | https://doi.org/10.1038/s41598-022-13916-5 4
Vol:.(1234567890)www.nature.com/scientificreports/
features to be CRT related risk factors. Some studies reported that high BMI, high PLT count, non-O blood
group, high level of triglycerides, catheter to vein ratio > 0.45, more than one attempt for PICC insertion, and
fluoropyrimidine containing chemotherapy are potential risk factors for CRT e vents17–21. However, all of the
above studies mainly focused on the solid tumor p opulation22. Also, there was a lack of reliable evidence from
hemato-oncology patients. Scrivens et al. demonstrated that PICC type was associated with the incidence and
rate of PICC-associated venous thromboembolism in hematologic malignancies22. Another study reported that
no feature was predictable for a high risk of catheter-related thrombotic complications in hematology patients1.
Univariate analysis showed that age, BMI, the prevalence of diabetes mellitus and hypertension, prothrombin
time, leukocyte count, and infections > grade 3 or 4 severity were potential predictive risk factors in hematological
cancer patients in this study. However, multivariate logistic regression analysis showed that BMI and prothrombin
time were the independent risk factors for CRT. Notably, the prothrombin time was within the normal range
in both groups. The clinical significance for CRT in patients with hematological malignancies was limited. This
finding is consistent with the previously reported clinical investigations that B MI19,23 may be a crucial risk pre-
dictor for CRT in patients with hematological cancer. Considering blood hypercoagulation and slow blood flow,
cardiovascular diseases may occur in obese patients. Thus, adopting close vascular monitoring, positive exercises,
diet intervention, and antithrombotic prophylaxis is necessary for obese patients to reduce the risk of CRT.
Herein, no specific thrombotic risk assessment model was applied to stratify the risk of CRT in patients with
hematological malignancy. Classic VTE assessment scales include Caprini, Padua, modified Wells, and the revised
Geneva score. The conclusive scores were obtained from patients from General Surgery, Internal Medicine,
outpatients, or intensive care unit (ICU), respectively9,11,12,24. Few studies have attempted to apply the classic
VTE risk models to assess the thrombosis risk of PICC25,26. The Michigan risk score is the first risk model for
CRT prediction in recent years. Nonetheless, the model also encompassed patients admitted to the General
Medicine ward or ICU as the main research subjects. This study compared the potential predictive power of CRT
risk in hemato-oncology patients, using Caprini, Padua, modified Wells, the revised Geneva and Michigan risk
score. Firstly, in this study, the Michigan model was not superior to the other four classic models in this study.
The predictor variables in the Michigan risk score include the presence of another CVC when index PICC is
placed, WBC count at the time of PICC insertion, active cancer, number of PICC lumens, and history of venous
thromboembolism13. Herein, only a single-lumen catheter was used. Supposedly, in hematologic malignancy
patients, WBC count may be affected by many factors. Hence, WBC count may not be a predictive variable sen-
sitive in the hematology patient as in the General Medicine ward or the ICU patients. Also, the Michigan risk
score was obtained from the Western populations. This might indicate that the characteristics and risk model of
CRT may be different based on the underlying diseases. Secondly, the current study identified that the Caprini
assessment scale had a greater predictive value in the assessment of CRT than other models. This finding was
consistent with that of Feng et al., wherein the Caprini scale was used for high-risk screening of the CRT in cancer
patients, and the AUC value was 0.636 (95% CI: 0.590–0.680; P < 0.001)25. Unlike Feng et al., this study compared
the predictive value of five different risk assessment scales simultaneously. Compared to the Padua scale, the
modified Wells scale, the revised Geneva, and Michigan risk scale, the Caprini scale has better sensitivity and
specificity in the risk prediction of CRT in patients with hematology tumors.
Nevertheless, the present study has several limitations. First, it was a retrospective study. Second, the study
was conducted at a single research institution, and the population size was small. All PICCs used in this study
were single-lumen catheters. Due to the small number of patients, the authors were unable to evaluate the puta-
tively related risk factors reported in the literature, such as PICC brand, the type of PICC, and chemotherapy
regimen. Thus, large, multicenter, prospective studies are necessary to substantiate these findings in the future.
Finally, some patients with PICC-related asymptomatic venous thromboembolism during the study period were
not included. A prospective study assessing the asymptomatic CRT samples by a regular vascular examination
is essential.
Conclusion
BMI is a significant risk factor for CRT in patients with hematological cancer. It is necessary to strengthen
monitoring and intervention to reduce the risk of CRT for patients with high BMI. Caprini thrombosis risk
assessment model has a better predictive value for CRT than other tools and could be used as an effective risk
prediction tool in patients with hematologic malignancies.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reason-
able request.
Received: 13 December 2021; Accepted: 30 May 2022
References
1. Morano, S. G. et al. Catheter-associated bloodstream infections and thrombotic risk in hematologic patients with peripherally
inserted central catheters (PICC). Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 23, 3289–3295 (2015).
2. Jaffray, J. et al. Peripherally inserted central catheters lead to a high risk of venous thromboembolism in children. Blood 135,
220–226 (2020).
3. Balsorano, P. et al. Peripherally inserted central catheter-related thrombosis rate in modern vascular access era-when insertion
technique matters: a systematic review and meta-analysis. J. Vasc. Access 21, 45–54 (2020).
4. Kang, J. R. et al. Peripherally inserted central catheter-related vein thrombosis in patients with lung cancer. Clin. Appl. Thromb./
Hemost. Off. J. Int. Acad. Clin. Appl. Thromb. /Hemost. 23, 181–186 (2017).
Scientific Reports | (2022) 12:9871 | https://doi.org/10.1038/s41598-022-13916-5 5
Vol.:(0123456789)www.nature.com/scientificreports/
5. Chen, Y. et al. Patterns and risk factors of peripherally inserted central venous catheter-related symptomatic thrombosis events in
patients with malignant tumors receiving chemotherapy. J. Vasc. Surg. Venous Lymphat. Disord. 8, 919–929 (2020).
6. Chen, P., Zhu, B., Wan, G. & Qin, L. The incidence of asymptomatic thrombosis related to peripherally inserted central catheter
in adults: a systematic review and meta-analysis People’s. Nurs. Open 8, 2249–2261 (2021).
7. McKeown, C. et al. A prospective study of the use of central venous catheters in patients newly diagnosed with acute myeloid
leukemia treated with induction chemotherapy. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 30, 1673–1679
(2022).
8. Pu, Y. L. et al. Complications and costs of peripherally inserted central venous catheters compared with implantable port catheters
for cancer patients: a meta-analysis. Cancer Nurs. 43, 455–467 (2020).
9. Caprini, J. A. Risk assessment as a guide to thrombosis prophylaxis. Curr. Opin. Pulm. Med. 16, 448–452 (2010).
10. Wells, P. S. et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the
models utility with the SimpliRED D-dimer. Thromb. Haemost. 83, 416–420 (2000).
11. Le Gal, G. et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann. Intern. Med.
144, 165–171 (2006).
12. Barbar, S. et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism:
the Padua prediction score. J. Thromb. Haemost. JTH 8, 2450–2457 (2010).
13. Chopra, V. et al. The Michigan risk score to predict peripherally inserted central catheter-associated thrombosis. J. Thromb. Hae-
most. JTH 15, 1951–1962 (2017).
14. Tran, H. et al. Deep venous thromboses in patients with hematological malignancies after peripherally inserted central venous
catheters. Leuk. Lymphoma 51, 1473–1477 (2010).
15. Schears, G. J., Ferko, N., Syed, I., Arpino, J. M. & Alsbrooks, K. Peripherally inserted central catheters inserted with current best
practices have low deep vein thrombosis and central line-associated bloodstream infection risk compared with centrally inserted
central catheters: a contemporary meta-analysis. J. Vasc. Access 22, 9–25 (2021).
16. Kang, J., Sun, W., Li, H., Ma, E. & Chen, W. Variable D-dimer thresholds in predicting peripherally inserted central catheter-related
vein thrombosis in patients with hematological malignancies: a pilot study. Thromb. Res. 190, 8–10 (2020).
17. Jones, D. et al. The risk of venous thromboembolism associated with peripherally inserted central catheters in ambulant cancer
patients. Thromb. J. 15, 25 (2017).
18. Li, X. et al. The incidence, risk factors, and patterns of peripherally inserted central catheter-related venous thrombosis in cancer
patients followed up by ultrasound. Cancer Manag. Res. 13, 4329–4340 (2021).
19. Al-Asadi, O., Almusarhed, M. & Eldeeb, H. Predictive risk factors of venous thromboembolism (VTE) associated with peripher-
ally inserted central catheters (PICC) in ambulant solid cancer patients: retrospective single Centre cohort study. Thromb. J. 17, 2
(2019).
20. Sharp, R. et al. Catheter to vein ratio and risk of peripherally inserted central catheter (PICC)-associated thrombosis according
to diagnostic group: a retrospective cohort study. BMJ Open 11, e045895 (2021).
21. Wang, G. et al. Association between ABO blood group and venous thrombosis related to the peripherally inserted central catheters
in cancer patients. J. Vasc. Access 22, 590–596 (2021).
22. Scrivens, N., Sabri, E., Bredeson, C. & McDiarmid, S. Comparison of complication rates and incidences associated with different
peripherally inserted central catheters (PICC) in patients with hematological malignancies: a retrospective cohort study. Leuk.
Lymphoma 61, 156–164 (2020).
23. Kang, J. et al. Peripherally inserted central catheter-related complications in cancer patients: a prospective study of over 50,000
catheter days. J. Vasc. Access 18, 153–157 (2017).
24. Bo, H. et al. Assessing the risk for development of deep vein thrombosis among chinese patients using the 2010 caprini risk assess-
ment model: a prospective multicenter study. J. Atheroscler. Thromb. 27, 801–808 (2020).
25. Feng, Y. et al. Assessing the thrombosis risk of peripherally inserted central catheters in cancer patients using Caprini risk assess-
ment model: a prospective cohort study. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 29, 5047–5055 (2021).
26. Lin, Y. et al. The Caprini thrombosis risk model predicts the risk of peripherally inserted central catheter-related upper extremity
venous thrombosis in patients with cancer. J. Vasc. Surg. Venous Lymphat. Disord. 9, 1151–1158 (2021).
Acknowledgements
This work is supported by a research project from Mianyang Central Hospital (grant no.2021YJ014).
Author contributions
Y.Z., A.M. and L.S. researched data. J.Y. and F.X. contributed to the study design and discussion. J.Y., Y.Z. and
F.X. performed statistical analyses. J.Y., Y.Z. and Q.L.Z. was responsible for conceiving the idea and drafting of
the manuscript. B.C. and F.X. revised the manuscript. F.X. was responsible for collecting funds. Both authors
contributed to literature search and in the approval of final manuscript.
Competing interests
The authors declare no competing interests.
Additional information
Correspondence and requests for materials should be addressed to F.X.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations.
Scientific Reports | (2022) 12:9871 | https://doi.org/10.1038/s41598-022-13916-5 6
Vol:.(1234567890)www.nature.com/scientificreports/
Open Access This article is licensed under a Creative Commons Attribution 4.0 International
License, which permits use, sharing, adaptation, distribution and reproduction in any medium or
format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the
Creative Commons licence, and indicate if changes were made. The images or other third party material in this
article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the
material. If material is not included in the article’s Creative Commons licence and your intended use is not
permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from
the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
© The Author(s) 2022
Scientific Reports | (2022) 12:9871 | https://doi.org/10.1038/s41598-022-13916-5 7
Vol.:(0123456789)You can also read

















































