2021 OPEN ENROLLMENT GUIDE - Coke Florida Wellness
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2021 OPEN ENROLLMENT GUIDE

Coke Florida is committed to providing our Associates with a benefits program that is both
comprehensive and competitive. Our benefits program offers health care, dental and
vision coverage, as well as other voluntary benefits to our Associates and their families. This
guide provides a general overview of your benefit choices and enrollment information to
help you select the coverage that is right for you.
ELIGIBILITY
If you are a full-time Associate working 30 or more hours per Adult dependent children 26 years old or older, who are
week, the chart below lists the benefits you may be eligible for supported primarily by you, and incapable of self-sustaining
after meeting each plan’s eligibility requirements. The eligibility employment by reason of mental or physical handicap (proof of
waiting period for benefits listed below is first of the month their condition and dependence must be submitted) may also
following 60 days of continuous employment: be eligible.
• Medical/Prescription
MAKING CHANGES
• Supplemental Life and AD&D
• Voluntary Dental • Short-Term Disability
• Voluntary Vision
• Basic Life
• Flexible Spending Acocunts (FSAs)
• 401(k)
DURING THE YEAR
Choose your benefits carefully. Medical,
• Employee Assistance Program
dental, vision, and flexible spending account contributions are
The eligibility waiting period for Long-Term Disability is first of the made on a pre-tax basis and IRS regulations state that you
month following 90 days of continuous employment. cannot change your pre-tax benefit options during the year
unless you have a qualified life event. Qualified life events
DEPENDENT ELIGIBILITY include:
You can enroll your dependents in plans that offer dependent • Marriage or divorce;
coverage. Eligible dependents are defined as your legal spouse • Death of your spouse or dependent;
and eligible children who reside in your household and depend
primarily on you for support. This includes: your own children, • Birth or adoption of a child;
legally adopted children, stepchildren, a child for whom you • Your spouse terminating or obtaining new employment (that
have been appointed legal guardian, and/or a child for whom affects eligibility for coverage);
the court has issued a Qualified Medical Child Support Order • You or your spouse switching employment status from full-
(QMCSO) requiring you or your spouse to provide coverage. time to part-time or vice versa (that affects eligibility for
coverage);
MEDICAL PLAN DEPENDENT • Significant cost or coverage changes; or
COVERAGE • Your dependent no longer qualifies as an eligible dependent.
You must contact Coke Florida Benefits Hotline at
Under health care reform, you may cover your eligible
dependent children up to age 26, regardless of marital or 877.340.0929 and submit the appropriate forms within 31
student status (this does not include spouses of adult children). days of the event. The Benefits Administrator will review your
request and determine whether the change you are requesting
Other plans offering dependent coverage (Dental, Vision, and
is allowed. Only benefit changes which are consistent with the
Life) will cease for your covered dependent children at the end
qualified life event are permitted.
of the month in which an eligible dependent reaches age 26,
regardless of student status, if the dependent is unmarried.
ENROLLMENT PERIODS
NEW ASSOCIATES ANNUAL ENROLLMENT
As a new full-time Associate of Coke Florida, you become As a benefits-eligible Associate, you have the opportunity
eligible for benefits on the first of the month following 60 to enroll in or make changes to your benefit plans during
days of continuous employment. Our benefits plan year our annual enrollment period. Annual enrollment is usually
runs from January through December. held in the Fall with benefit elections effective January 1.
2
ADVANTAGES OF TELADOC
Teladoc® gives you access to a national network of U.S. board-
A HEALTH SAVINGS certified doctors by phone, video, or mobile app who are
available anywhere, 24/7/365 to treat many of your medical
ACCOUNT (HSA) issues. Teladoc doctors can treat many medical conditions.
A welcome kit will be mailed to your home with instructions
If you’re enrolled in the high-deductible health plan such as the for setting up your Teladoc account, completing your medical
HSA Choice Plus HDHP Plan, you’re also eligible to contribute history and requesting a consult. Once you’re set up, a Teladoc
on a pre-tax basis to an HSA (if you’re not eligible for Medicare). doctor is always just a call or click away!
Coke Florida also contributes to your HSA. NEW for 2021! Mental Health Care and Dermatology services
are now also available through Teladoc (copays apply). Use the
YOUR ACCOUNT, YOUR MONEY! Teladoc app or go online to review these new available services
in more detail.
You can use your HSA to pay for eligible health care expenses—
PAYING FOR YOUR
or choose to pay out-of-pocket instead and let your HSA
balance grow over time. It works like a personal savings account,
but with more advantages:
Use it today or save for tomorrow. Your HSA is an account
in your name; you own it and you decide how to get the most
BENEFITS
from it. Some benefits are provided to you at no cost, such as basic life
insurance, short-term disability, and core long-term disability.
Money rolls over each year. Lose the worry of having to spend The cost of other benefits, such as medical, dental, and vision
it all before the end of the year. With the HSA, the balance rolls
is shared by you and Coke Florida. Additional benefits, such
over year after year so you can let it grow over time.
as supplemental life insurance and supplemental long-term
Get triple tax advantages. Not only do you contribute pre-tax disability are paid for by you at discounted group rates. Having
money, but your account can grow tax-free and you can use your benefit options available means you can build a benefits
HSA to pay for eligible health care expenses tax-free. Bottom
program that meets your needs and your lifestyle.
line, you save money in three ways with an HSA.
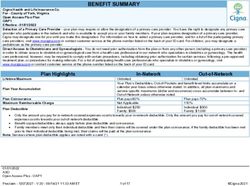
WHO
Take it with you. Your HSA is yours to keep, even if you retire BENEFIT TAX BASIS
CONTRIBUTES?
or leave the company.
Medical/Prescription You and Coke Florida Pre-tax
It’s convenient. If you choose, contributions are automatically
deducted from your paycheck. You can change or stop Dental You and Coke Florida Pre-tax
contributions at any time. Vision You and Coke Florida Pre-tax
Associates can contribute up to a maximum of $3,600 to an Basic Life
HSA account for individual coverage, and up to a maximum of Imputed income is required by the You may pay
$7,200 for family coverage. The maximum contribution amount Internal Revenue code on employer imputed
Coke Florida
includes employer funding. Please keep employer funding in mind paid life insurance over $50,000. The income
when electing your maximum contribution amount. Associates amount is age based and typically (After-tax)
age 55+ are allowed to make an additional $1,000 in catch up low in cost.
contributions. Supplemental Life and
You After-tax
AD&D
MEDICAL BENEFITS Short-Term Disability Coke Florida After-tax
Coke Florida seeks to provide the best possible medical benefits Core Long-Term Disability Coke Florida Pre-tax
at a reasonable cost. Associates are provided with two medical Supplemental LTD You After-tax
plans that include prescription drug coverage.
FSAs You Pre-tax
Please refer to the chart on the next page for a comparison of
medical plan benefits. You with a Coke
Retirement Savings 401(k) Florida Match
Pre-tax
Voluntary (Accident, Hospital
You Pre-tax
Indemnity)
Voluntary (Critical Illness,
You Post-tax
Legal)
3
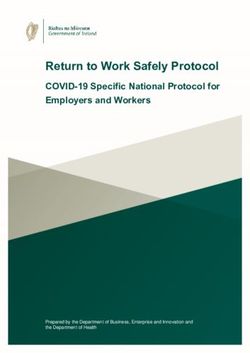
MEDICAL BENEFITS AT-A-GLANCE AND COST OF COVERAGE
The information below is a summary of medical coverage only. Please log on to MDFCokeflorida@ceridian.com, our enrollment
platform, for plan summaries detailing coverage information, limitations, and exclusions.
Any deductibles and copays shown in the chart below are amounts for which you are responsible.
CHOICE PLUS VALUE PLAN CHOICE PLUS HDHP PLAN WITH HSA
KEY FEATURES
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
HSA Fund
Associate only N/A $200
Family $400
Annual Calendar Year Deductible Embedded Non-Embedded
Associate only $1,000 $2,000 $1,900 $3,800
Family $2,000 $4,000 $3,800 $7,600
Out-of-Pocket Maximum* Embedded Non-Embedded
Individual (includes deductible) $4,000 $8,000 $3,550 $7,100
Family (includes deductible) $10,667 $21,333 $7,100 $14,200
Lifetime Maximum None None None None
Coinsurance (portion you pay) 80% 60% 80% 60%
Physician Services
Office Visit 20% after ded. 40% after ded. 20% after ded. 40% after ded.
Specialist Visit 20% after ded. 40% after ded. 20% after ded. 40% after ded.
Preventive Care No Charge No Charge No Charge No Charge
Lab and X-ray Services 20% after ded. 40% after ded. 20% after ded. 40% after ded.
Hospital Services
Inpatient (per admission) 20% after ded. 40% after ded. 20% after ded. 40% after ded.
Emergency Treatment
Urgent Care Copay 20% after ded. 40% after ded. 20% after ded. 40% after ded.
Emergency room Copay (waived if admitted) $250 $250 20% after ded. 20% after ded.
Annual Prescription Drug Deductible Combined with Combined with
None None Medical Medical
PRESCRIPTION DRUGS
Retail Prescriptions (30-day supply)
Generic $15 Not Covered $5 Not Covered
Preferred brand 20% up to $50 max Not Covered 25% after ded. Not Covered
Non-preferred brand 35% up to $100 max Not Covered 25% after ded. Not Covered
Mail Order Prescriptions (90-day supply)
Generic $30 Not Covered $10 Not Covered
Preferred brand 20% up to $125 max Not Covered 25% after ded. Not Covered
Non-preferred brand 35% up to $250 max Not Covered 25% after ded. Not Covered
ASSOCIATE CONTRIBUTIONS NON-TOBACCO USER / TOBACCO NON-TOBACCO USER / TOBACCO
(PER PAYCHECK) USER / SPOUSE TOBACCO USER USER / SPOUSE TOBACCO USER
Associate Only $88.60 / $111.68 $33.33 / $56.40
Associate + Spouse $295.77 / $318.84 / $341.92 $137.89 / $160.97 / $184.05
Associate + Child(ren) $206.50 / $229.58 $85.28 / $108.35
Associate + Family $371.70 / $394.78 / $417.86 $175.94 / $199.02 / $222.10
*Includes all copays.
Note: Deductibles, copays and coinsurance accumulate toward the out-of-pocket maximums. Usual, Customary and Reasonable (UCR) charges apply for all out-of-
network benefits.
Embedded Deductible and Out-Of-Pocket - For associate only coverage, the amounts represented as single coverage. For family coverage, the plan actually has two deductible
amounts. Each covered individual within the family will not exceed the applicable individual amount listed and the total family deductible is satisfied once 3 family members
meet the individual amount. For example, if only one individual in the family is receiving medical services, they only have to meet the individual deductible and individual OOP
maximum. However, if there are 5 members in the family and 3 members meet their individual deductibles, then all family members are deemed to have satisfied the family
deductible.
Non-Embedded Ded and OOP (cumulative) - For associate only coverage, the amounts are represented as single. For family coverage, the plan requires the family deductible
and family out-of-pocket amount maximum to be met in full by one or more members. If only one individual is receiving medical services, they still have to meet the family
deductible and family OOP maximum. In a family coverage situation, this may put more financial risk for payment of medical bills if only one member of the family is receiving
medical services than an embedded deductible.
4
PREVENTIVE AND VOLUNTARY DENTAL BENEFITS
NON-PREVENTIVE Dental coverage is key to your overall health. Coke Florida offers Associates one
dental plan through Delta Dental. Your dental plan offers coverage for four main
SERVICES types of expenses:
Preventive care services are those that are • Preventive and diagnostic services like routine exams and cleanings, fluoride
treatments, sealants, and X-rays
generally linked to routine wellness exams.
Non-preventive services are those that are • Basic services such as simple fillings and extractions, root canals, oral surgery,
and gum disease treatment
considered treatment or diagnosis for an illness,
• Major services such as crowns and dentures
injury, or other medical condition. There may be
limits on how often you can receive preventive • Orthodontia
care treatments and services. You should Note: When going out-of-network, higher charges/balance billing may apply.
ask your health care provider whether your visit
is considered preventive or non-preventive
care. Examples of preventive care include:
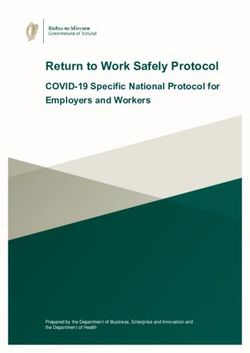
DENTAL BENEFITS AT-A-GLANCE AND COST
• Annual routine physicals OF COVERAGE
• Bone-density tests, cholesterol screening KEY FEATURES DENTAL PPO
Annual Calendar Year Maximum $1,500 per person
• Immunizations, mammograms, Pap smears,
pelvic exams, PSA exams Calendar Year Deductible
Individual / Family $50 per person / $150 per family
• Sigmoidoscopies, colonoscopies
Preventive Services (no deductible) No Charge
Basic Services 20% In-Network / 50% Out-of-Network
COPAYMENTS AND Major Services 50% In-Network / 60% Out-of-Network
COINSURANCE Orthodontia (children up to age 19)
Lifetime maximum $2,000 In-Network / $1,000 Out-of-Network
A copayment (copay) is the fixed dollar amount
ASSOCIATE CONTRIBUTIONS (PER PAYCHECK)
you pay for certain in-network services. In some
cases, you may be responsible for coinsurance Associate Only $7.11
after a copay is made. Associate + Spouse $13.76
Coinsurance is the percentage of covered Associate + Child(ren) $16.02
expenses shared by the Associate and the plan. In Associate + Family $23.02
some cases, coinsurance is paid after the insured Note: ID Card will not be provided. Please visit the Delta Dental website.
meets a deductible. For example, if the plan pays
VISION BENEFITS
90% of an in-network covered charge, you pay
10%.
Coke Florida offers Associates a vision plan through Vision Service Plan (VSP) that
IN-NETWORK ADVANTAGE includes coverage for eye exams, eyeglasses and/or contact lenses.
Within some of the medical, dental and vision
plans, you have the freedom to use any provider.
However, when you use an in-network provider, the
VISION BENEFITS AT-A-GLANCE AND COST
percentage you pay out-of-pocket will be based on OF COVERAGE
a negotiated fee, which is usually lower than the
KEY FEATURES IN-NETWORK FREQUENCY
actual charges of care. If you use a provider who is
outside of the network, you may be responsible to Exam $20 Every 12 months
pay for the difference of the Usual, Customary and Lenses Combined with exam Every 12 months
Reasonable (UCR) charges and what the provider Copay combined with
Every 24 months for adults
charges. You may also need to submit claim forms. Frames exam, up to $150
Every 12 months for child(ren)
allowance available
OUT-OF-POCKET Contact Lenses Instead of Glasses
Conventional/Disposable/
MAXIMUM Medically Necessary
$150 allowance Every 12 months
Our medical/prescription plans feature an out- ASSOCIATE CONTRIBUTIONS (PER PAYCHECK)
of-pocket maximum, which limits the amount
Associate Only $1.91
of coinsurance you will pay for eligible health care
expenses. Once you reach that maximum, the Associate + Spouse $4.70
plan begins to pay 100% of eligible expenses. Associate + Child(ren) $3.83
There may be separate in- and out-of-network Associate + Family $6.66
annual out-of-pocket maximums. Copays,
Note: ID Card not required for vision services.
deductibles and coinsurance accumulate towards
your out-of-pocket maximum.
5
INCOME PROTECTION FLEXIBLE SPENDING
BASIC LIFE ACCOUNTS
Coke Florida provides Associates with basic life insurance Flexible Spending Accounts (FSAs) help Associates save
coverage in the amount of 1.5 times your basic annual earnings money by allowing you to pay for certain types of health
to a maximum of $400,000. care and dependent care expenses on a pre-tax basis. You
decide how much money to contribute each pay period to
SUPPLEMENTAL LIFE AND AD&D cover these expenses.
Associates can purchase supplemental life and Accidental Death This amount is then divided by the remaining calendar
& Dismemberment coverage for you and your family. You can year pay periods and deducted on a before tax basis and
elect additional life and AD&D insurance for: deposited into your FSA. When you need money to cover
an eligible expense, you can get reimbursed using a variety
Choice of 1x, 2x, 3x, 4x, or 5x your basic
of reimbursement methods. Remember to always keep
annual earnings to $1,600,000 (AD&D to a
Yourself: your receipts.
maximum amount of the lesser of 5x your
basic annual earnings to $1,000,000) HEALTH CARE SPENDING ACCOUNT
Increments of $5,000 up to 50% of your Eligible Associate or family health care
Supplemental Life Benefit or $100,000 (AD&D expenses such as medical, dental, or
Your Spouse: Use for:
vision plan deductibles, copays, and/or
is an amount equal to 40% of your AD&D
coinsurance, as well as for prescription drugs
insurance to a maximum of $700,000)
Annual Annual Minimum: $120
Choice of $5,000 or $10,000 (AD&D is an
contribution: Annual Maximum: $2,750
Your Child(ren): amount equal to 10% for each child of your
AD&D Insurance to a maximum of $200,000) DEPENDENT CARE SPENDING ACCOUNT
Eligible child and elder care expenses so you
You pay 100% of the cost for this supplemental life and AD&D Use for:
(and your spouse) can work or go to school
coverage. Please refer to the plan summaries for additional Annual Annual Minimum: $120
details. A statement of Health (SOH) application may be contribution: Annual Maximum: $5,000
required if you elect coverage over the Guaranteed Issue
amount or if you enroll after your initial eligibility period. Age
reductions may apply to life insurance amounts. IMPORTANT: USE IT OR LOSE IT!
According to IRS rules, any money remaining in a health
WHAT’S DOES GUARANTEED ISSUE MEAN? care or dependent care spending account after the
Guaranteed issue refers to the amount of insurance you may deadline for filing claims will be forfeited. However, the
buy without the insurance company requiring you to provide Plan shall provide for a carryover of $500 of any amount
remaining unused in the health FSA as of the end of the
evidence of insurability (EOI), or proof of your good health.
Plan year. Such carryover amount may be used to pay
or reimburse medical expenses under the health FSA
SHORT-TERM DISABILITY incurred during the entire Plan year to which it is carried
over.
Associates are eligible to receive short-term disability (STD)
benefits for a qualified non-work related illness or injury that
prevents you from working for a period longer than 7 days
(1 day for salaried Associates). The total amount of benefits
paid depends on if you are hourly or salaried at the time your
ADDITIONAL INSURANCE OPTIONS
disability occurs. Hourly Associates may receive 75% of your To provide you and your family additional financial security,
weekly pay up to a maximum of 26 weeks. Salaried Associates you can elect additional coverage:
may receive 100% of your weekly pay for weeks 1-8 and 75% for • Accident Insurance pays cash benefits in the event of an
the remainder of the 26 week period. Coke Florida pays the full accident to help with the costs associated with out-of-
cost of this coverage. pocket expenses and bills
• Critical Illness helps with the treatment costs of covered
critical illnesses. You receive cash benefits directly. (Please
LONG-TERM DISABILITY refer to MetLife benefit summaries for more detail.)
Associates are eligible for employer paid long-term disability (LTD) • Legal coverage through MetLife provides you with access
to legal services at a discounted price. You can get help
insurance which provides a monthly benefit in the event you cannot with real estate, wills, traffic tickets, and more.
work because of a long-term illness or injury. LTD benefits provide
you with 50% of your monthly salary, after 26 weeks of a qualified • Hospital Indemnity helps you with hospital costs by
reimbursing you for your out of pocket expenses.
non-work related illness or injury.
• Pet Insurance helps you with pet healthcare costs by
reimbursing you for your out of pocket expenses.
VOLUNTARY LTD
Supplemental LTD coverage is available for purchase and will
provide Associates with an additional 10% or 20% of your monthly
earnings, up to a $20,000 monthly maximum.
6
RETIREMENT SAVINGS 401(k)
As an Associate of Coke Florida on the 60th day of continuous employment, you are eligible to participate in the Retirement Savings 401(k)
Plan.
The 401(k) plan allows you to invest up to 100% of your regular earnings on a pre-tax basis through automatic regular payroll deductions.
In addition, for any contributions up to 6% of your pay, Coke Florida will match $1.00 for each dollar you invest for the first 1% and $.50 for
every dollar for the next 5%.
For additional information regarding any of the plan provisions, please consult the 401(k) guidebook available through the Benefits Administrator.
Our 401(k) Plan administrator is Wells Fargo. You may contact them at 800.728.3123 or visit their website at www.wellsfargo.com.
BENEFITS ADMINISTRATOR INFORMATION
If you have any questions regarding eligibility, benefit plans or enrollment periods or would like additional information, you may
contact the appropriate vendor directly or contact Coke Florida’s Benefits Hotline.
REFERENCES AND RESOURCES FOR
ADDITIONAL INFORMATION
FOR QUESTIONS ABOUT CONTACT CALL VISIT/EMAIL PLAN/GROUP ID
Coke Florida’s
Benefits 877.340.0929 MDFCokeflorida@ceridian.com N/A
Benefits Hotline
Medical/Virtual Visits:
Aetna Medical: 888.699.1005 Medical: 868660
Medical/Prescription Drug www.aetna.com
CVS Caremark Pharmacy: 855.383.9428 Pharmacy: 1586
Pharmacy: www.caremark.com
Dental Delta Dental 800.521.2651 www.deltadentalins.com 17681
Vision VSP 800.877.7195 www.vsp.com 30057528
Life Insurance MetLife 800.638.6420 www.metlife.com 160264
Short-Term Disability UNUM 866.779.1054 www.unum.com 951689
Long-Term Disability UNUM 866.779.1054 www.unum.com 951688
Flexible Spending Accounts WageWorks 877.924.3967 www.wageworks.com N/A
EAP Compsych 888.664.6512 www.guidanceresources.com Member ID: CCBF
401(k) Savings Plan Wells Fargo 800.728.3123 www.wellsfargo.com N/A
HSA Payflex 888.678.8242 www.payflex.com N/A
Business Travel Accident MetLife 800.638.6420 www.metlife.com 160378
Accident MetLife 800.GETMET8 www.metlife.com 160264
Critical Illness MetLife 800.GETMET8 www.metlife.com 160264
Legal MetLife 800.GETMET8 www.metlife.com 160264
Hospital Indemnity Aetna 800.607.3366 www.myaetnasupplemental.com 802425
Pet Insurance Nationwide 877.738.7874 www.nationwide.com TBD
ABOUT THIS GUIDE
This guide highlights all Associate benefits. Official plan and insurance documents govern your rights and benefits under each
plan.
For more details about your benefits, including covered expenses, exclusions, and limitations, please refer to the individual
summary plan descriptions (SPDs), plan document or certificate of coverage for each plan. If any discrepancy exists between
this guide and the official documents, the official documents will prevail.
7IMPORTANT NOTICES
About This Guide Newborns’ and Mothers’ Health
This guide highlights your benefits. Official plan and insurance Protection Act Disclosure
documents govern your rights and benefits under each plan. For Group health plans and health insurance issuers generally may not,
more details about your benefits, including covered expenses, under Federal law, restrict benefits for any hospital length of stay in
exclusions, and limitations, please refer to the individual summary connection with childbirth for the mother or newborn child to less
plan descriptions (SPDs), plan document, or certificate of coverage than 48 hours following a vaginal delivery, or less than 96 hours
for each plan. If any discrepancy exists between this guide and the following a cesarean section. However, Federal law generally does
official documents, the official documents will prevail. Coke Florida not prohibit the mother’s or newborn’s attending provider, after
reserves the right to make changes at any time to the benefits, costs, consulting with the mother, from discharging the mother or her
and other provisions relative to benefits. newborn earlier than 48 hours (or 96 hours as applicable). In any case,
plans and issuers may not, under Federal law, require that a provider
Reminder of Availability of Privacy Notice obtain authorization from the plan or the issuer for prescribing a
This is to remind plan participants and beneficiaries of the Coke length of stay not in excess of 48 hours (or 96 hours).
Florida Health and Welfare Plan (the “Plan”) that the Plan has issued a
Health Plan Privacy Notice that describes how the Plan uses and USERRA
disclosed protected health information (PHI). You can obtain a copy Your right to continued participation in the Plan during leaves of
of the Coke Florida Health and Welfare Plan Privacy Notice upon your absence for active military duty is protected by the Uniformed
written request to the Human Resources Department, at the Services Employment and Reemployment Rights Act (USERRA).
following address: Accordingly, if you are absent from work due to a period of active
Coke Florida, Human Resources duty in the military for less than 31 days, your Plan participation will
10117 Princess Palm Avenue, Suite 400 not be interrupted and you will continue to pay the same amount as if
Tampa, FL 33610 you were not absent. If the absence is for more than 31 days and not
more than 24 months, you may continue to maintain your coverage
If you have any questions, please contact the Coke Florida Human
under the Plan by paying up to 102% of the full amount of premiums.
Resources Office at 813.327.7289.
You and your dependents may also have the opportunity to elect
COBRA coverage. Contact Coke FL Human Resources Manager for
Women’s Health and Cancer Rights Act more information.
If you have had or are going to have a mastectomy, you may be
entitled to certain benefits under the Women’s Health and Cancer Also, if you elect not to continue your health plan coverage during
Rights Act of 1998 (WHCRA). For individuals receiving mastectomy- your military service, you have the right to be reinstated in the Plan
related benefits, coverage will be provided in a manner determined upon your return to work, generally without any waiting periods or
in consultation with the attending physician and the patient, for: pre-existing condition exclusions, except for service connected
illnesses or injuries, as applicable.
• All stages of reconstruction of the breast on which the mastectomy
was performed;
• Surgery and reconstruction of the other breast to produce a This guide contains important
symmetrical appearance;
• Prostheses; and
information about the Medicare Part D
• Treatment of physical complications of the mastectomy, including creditable status of your prescription
lymphedema. drug coverage on page 9.
These benefits will be provided subject to the same deductibles and
coinsurance applicable to other medical and surgical benefits
provided under this plan. If you would like more information on
WHCRA benefits, call your plan administrator Aetna at 888.699.1005.
8MEDICARE PART D NOTICE OF CREDITABLE
COVERAGE
Your Options When will you pay a higher premium
Please read this notice carefully and keep it where you can find it. (penalty) to join a Medicare Drug Plan?
This notice has information about your current prescription drug You should also know that if you drop or lose your current coverage
coverage with Coke Florida and about your options under with Coke Florida and don’t join a Medicare drug plan within 63
Medicare’s prescription drug coverage. This information can help continuous days after your current coverage ends, you may pay a
you decide whether or not you want to join a Medicare drug plan. If higher premium (a penalty) to join a Medicare drug plan later.
you are considering joining, you should compare your current
coverage, including which drugs are covered at what cost, with the If you go 63 continuous days or longer without creditable
coverage and costs of the plans offering Medicare prescription drug prescription drug coverage, your monthly premium may go up by at
coverage in your area. Information about where you can get help to least 1% of the Medicare base beneficiary premium per month for
make decisions about your prescription drug coverage is at the end every month that you did not have that coverage. For example, if you
of this notice. go nineteen months without creditable coverage, your premium may
consistently be at least 19% higher than the Medicare base
There are two important things you need to know about your current beneficiary premium. You may have to pay this higher premium (a
coverage and Medicare’s prescription drug coverage: penalty) as long as you have Medicare prescription drug coverage. In
1. Medicare prescription drug coverage became available in 2006 to addition, you may have to wait until the following October to join.
everyone with Medicare. You can get this coverage if you join a
Medicare Prescription Drug Plan or join a Medicare Advantage For more information about this notice or
Plan (like an HMO or PPO) that offers prescription drug coverage.
All Medicare drug plans provide at least a standard level of
your current prescription drug coverage:
Contact the person listed below for further information. NOTE: You’ll
coverage set by Medicare. Some plans may also offer more
get this notice each year. You will also get it before the next period
coverage for a higher monthly premium.
you can join a Medicare drug plan, and if this coverage through Coke
2. Coke Florida has determined that the prescription drug coverage Florida changes. You also may request a copy of this notice at any
offered by CVS Caremark is, on average, for all plan participants, time.
expected to pay out as much as standard Medicare prescription
drug coverage pays and is therefore considered Creditable
Coverage. Because your existing coverage is Creditable
For more information about your options
Coverage, you can keep this coverage and not pay a higher under Medicare Prescription Drug
premium (a penalty) if you later decide to join a Medicare drug coverage:
plan. More detailed information about Medicare plans that offer
prescription drug coverage is in the “Medicare & You” handbook.
When Can You Join A Medicare Drug You’ll get a copy of the handbook in the mail every year from
Plan? Medicare. You may also be contacted directly by Medicare drug
You can join a Medicare drug plan when you first become eligible for plans. For more information about Medicare prescription drug
Medicare and each year from October 15th through December 7th. coverage:
However, if you lose your current creditable prescription drug • Visit www.medicare.gov
coverage, through no fault of your own, you will also be eligible for a
• Call your State Health Insurance Assistance Program for
two (2) month Special Enrollment Period (SEP) to join a Medicare
personalized help. See the inside back cover of your copy of the
drug plan.
“Medicare & You” handbook for their telephone number.
• Call 800.MEDICARE (800.633.4227) TTY users should call
What Happens to Your Current Coverage 877.486.2048
if You Decide to Join a Medicare Drug • If you have limited income and resources, extra help paying for
Plan? Medicare prescription drug coverage is available. For information
If you decide to join a Medicare drug plan, your current Coke Florida about this extra help, visit Social Security on the web at:
coverage will not be affected. Coca-Cola Beverages Florida, LLC’s • www.socialsecurity.gov
current prescription drug plan under CVS/Caremark is a $15 • or call: 800.772.1213 (TTY: 800.325.0778)
copay (Value Plan) and $5 copay (HDHP) for tier 1 drugs, 20% up
to $50 max (Value Plan) and 25% after deductible (HDHP) for tier Remember: Keep this Creditable Coverage notice. If you
2 drugs and 35% up to $100 max (Value Plan) and 25% after decide to join one of the Medicare drug plans, you may
deductible (HDHP) for tier 3 drugs. There is also a mail order be required to provide a copy of this notice when you join
benefit for maintenance prescriptions that costs $30 copay (Value to show whether or not you have maintained creditable
Plan) and $10 copay (HDHP) for tier 1 drugs, 20% up to $125 max coverage and, therefore, whether or not you are required
(Value Plan) and 25% after deductible (HDHP) for tier 2 drugs and to pay a higher premium (a penalty).
35% up to $250 max (Value Plan) and 25% after deductible
(HDHP) for tier 3 drugs for a 90-day supply. If you do decide to join
Date: 10/02/2020
a Medicare drug plan and drop your current coverage, be aware that
Name of Entity/Sender: Coke Florida
you and your dependents may not be able to get this coverage back.
Contact: Leroy Whitaker
Coke Florida
Address: 10117 Princess Palm Avenue, Suite 400, Tampa, FL 33610
Phone Number: 813.327.7289 9YOUR ERISA RIGHTS
As a participant in the Coke Florida benefit plans, Enforce Your Rights
you are entitled to certain rights and protections If your claim for a benefit is denied or ignored, in whole or in part,
under the Employee Retirement Income Security you have a right to:
Act of 1974 (ERISA), as amended. ERISA provides • Know why this was done;
that all plan participants shall be entitled to • Obtain copies of documents relating to the decision without
receive information about their plan and benefits, charge; and
continue group health plan coverage, and enforce • Appeal any denial.
their rights. ERISA also requires that plan All of these actions must occur within certain time schedules. Under
fiduciaries act in a prudent manner. ERISA, there are steps you can take to enforce your rights. For
instance, you may file suit in a federal court if:
Receive Information About Your Plan and • You request a copy of plan documents or the latest annual report
Benefits from the plan and do not receive them within 30 days, you may file
You are entitled to: suit in a federal court. In such a case, the court may require the
plan administrator to provide the materials and pay you up to $110
• Examine, without charge, at the plan administrator’s office, all plan a day until you receive the materials, unless the materials were not
documents—including pertinent insurance contracts, trust sent because of reasons beyond the control of the administrator;
agreements, and a copy of the latest annual report (Form 5500
• You have followed all the procedures for filing and appealing a
Series) filed by the plan with the U.S. Department of Labor and
claim (as outlined earlier in this summary) and your claim for
available at the Public Disclosure Room of the Employee Benefits
benefits is denied or ignored, in whole or in part. You may also file
Security Administration;
suit in a state court.
• Obtain, upon written request to the plan’s administrator, copies of
• You disagree with the plan’s decision or lack thereof concerning
documents governing the operation of the plan, including
the qualified status of a domestic relations order or a medical child
insurance contracts and copies of the latest annual report (Form
support order; or
5500 Series), and updated summary plan description. The
administrator may make a reasonable charge for the copies. • The plan fiduciaries misuse the plan’s money, or if you are
discriminated against for asserting your rights. You may also seek
• Receive a summary report of the plan’s annual financial report. The
assistance from the U.S. Department of Labor.
plan administrator is required by law to furnish each participant
with a copy of this Summary Annual Report. The court will decide who should pay court costs and legal fees. If
you are successful, the court may order the person you have sued to
Continued Group Health Plan Coverage pay these costs and fees. If you lose, the court may order you to pay
You are entitled to: these costs and fees. This should occur if the court finds your claim
frivolous.
• Continued health care coverage for yourself, spouse, or
dependents if there is a loss of coverage under the plan as a result
of a qualifying event. You or your dependents may have to pay for
Assistance with Your Questions
If you have questions about how your plan works, contact the Human
such coverage. Review this summary plan description governing
Resources Department. If you have any questions about this
the plan on the rules governing your COBRA continuation
statement or your rights under ERISA, or if you need assistance in
coverage rights.
obtaining documents from the plan administrator, you should
• Reduce or eliminate exclusionary periods of coverage for pre- contact the nearest office listed on EBSA’s website:
existing conditions under your group health plan, if you have https://www.dol.gov/agencies/ebsa/about-ebsa/about-us/regional-
credible coverage from another plan. You should be provided a offices
certificate of credible coverage, free of charge, from your group
health plan or health insurance issuer when: Or you may write to the:
Division of Technical Assistance and Inquiries
– You lose coverage under the plan;
Employee Benefits Security Administration
– You become entitled to elect COBRA continuation coverage; U.S. Department of Labor
– You request it up to 24 months after losing coverage. 200 Constitution Avenue, NW
Washington, DC 20210
Prudent Actions by Plan Fiduciaries You may also obtain certain publications about your rights and
In addition to creating rights for plan participants, ERISA imposes
duties upon the people who are responsible for the operation of the responsibilities under ERISA by calling the Employee and Employer
plans. The people who operate your plans are called “fiduciaries,” Hotline of the Employee Benefits Security Administration at:
and they have a duty to act prudently and in the interest of you and 866.275.7922. You may also visit the EBSA’s web site on the Internet
other plan participants and beneficiaries. No one, including your at: http://www.dol.gov/ebsa.
employer or any other person, may fire you or otherwise discriminate
against you in any way to prevent you from obtaining a benefit or
exercising your rights under ERISA.
10CONTINUATION COVERAGE RIGHTS UNDER COBRA
Introduction Your dependent children will become qualified beneficiaries if they
You are receiving this notice because you have recently become lose coverage under the Plan because any of the following qualifying
covered under a group health plan (the Plan). This notice contains events happen:
important information about your right to COBRA continuation • The parent-employee dies;
coverage, which is a temporary extension of coverage under the • The parent-employee’s hours of employment are reduced;
Plan. This notice generally explains COBRA continuation
• The parent-employee’s employment ends for any reason other
coverage, when it may become available to you and your family,
than his or her gross misconduct;
and what you need to do to protect the right to receive it.
• The parent-employee becomes entitled to Medicare benefits (Part
The right to COBRA continuation coverage was created by a federal A, Part B, or both);
law, the Consolidated Omnibus Budget Reconciliation Act of 1985
• The parents become divorced or legally separated; or
(COBRA). COBRA continuation coverage can become available to
you when you would otherwise lose your group health coverage. • The child stops being eligible for coverage under the plan as a
“dependent child.”
It can also become available to other members of your family who
are covered under the Plan when they would otherwise lose their When is COBRA Coverage Available?
group health coverage. For additional information about your rights The Plan will offer COBRA continuation coverage to qualified
and obligations under the Plan and under federal law, you should beneficiaries only after the Plan Administrator has been notified that
review the Plan’s Summary Plan Description or contact the Plan a qualifying event has occurred. When the qualifying event is the end
Administrator. of employment or reduction of hours of employment, death of the
You may have other options available to you when you lose group employee, or the employee’s becoming entitled to Medicare
health coverage. For example, you may be eligible to buy an benefits (under Part A, Part B, or both), the employer must notify the
individual plan through the Health Insurance Marketplace Plan Administrator of the qualifying event.
(www.healthcare.gov). By enrolling in coverage through the
Marketplace, you may qualify for lower costs on your monthly You Must Give Notice of Some Qualifying
premiums and lower out-of-pocket costs. Additionally, you may Events
qualify for a 30-day special enrollment period for another group For the other qualifying events (divorce or legal separation of the
health plan for which you are eligible (such as a spouse’s plan), even employee and spouse or a dependent child’s losing eligibility
if that plan generally doesn’t accept late enrollees. for coverage as a dependent child), you must notify the Plan
Administrator within 60 days after the qualifying event occurs. You
What is COBRA Continuation Coverage? must provide this notice to: Coke Florida Human Resources or
COBRA continuation coverage is a continuation of Plan coverage COBRA Administrator.
when coverage would otherwise end because of a life event known
as a “qualifying event.” Specific qualifying events are listed later in How is COBRA Coverage Provided?
this notice. After a qualifying event, COBRA continuation coverage Once the Plan Administrator receives notice that a qualifying event
must be offered to each person who is a “qualified beneficiary.” You, has occurred, COBRA continuation coverage will be offered to each
your spouse, and your dependent children could become qualified of the qualified beneficiaries. Each qualified beneficiary will have an
beneficiaries if coverage under the Plan is lost because of the independent right to elect COBRA continuation coverage. Covered
qualifying event. Under the Plan, qualified beneficiaries who elect employees may elect COBRA continuation coverage on behalf of
COBRA continuation coverage must pay for COBRA continuation their spouses, and parents may elect COBRA continuation coverage
coverage. on behalf of their children. Any qualified beneficiary who does not
If you are an employee, you will become a qualified beneficiary if you elect COBRA within the 60-day election period specified in the
lose your coverage under the Plan because either one of the election notice will lose his or her right to elect COBRA.
following qualifying events happens: COBRA continuation coverage is a temporary continuation of
• Your hours of employment are reduced, or coverage that generally lasts for 18 months due to employment
• Your employment ends for any reason other than your gross termination or reduction of hours of work. When the qualifying event
misconduct. is the death of the employee, the employee’s becoming entitled to
Medicare benefits (under Part A, Part B, or both), your divorce or
If you are the spouse of an employee, you will become a qualified
legal separation, or a dependent child’s losing eligibility as a
beneficiary if you lose your coverage under the Plan because any of
dependent child, COBRA continuation coverage lasts for up to a
the following qualifying events happens:
total of 36 months. When the qualifying event is the end of
• Your spouse dies; employment or reduction of the employee’s hours of employment,
• Your spouse’s hours of employment are reduced; and the employee became entitled to Medicare benefits less than 18
• Your spouse’s employment ends for any reason other than his or months before the qualifying event, COBRA continuation coverage
her gross misconduct; for qualified beneficiaries other than the employee lasts until 36
months after the date of Medicare entitlement. For example, if a
• Your spouse becomes entitled to Medicare benefits (under Part A,
covered employee becomes entitled to Medicare 8 months before
Part B, or both); or
the date on which his employment terminates, COBRA continuation
• You become divorced or legally separated from your spouse. coverage for his spouse and children can last up to 36 months after
the date of Medicare entitlement, which is equal to 28 months after
the date of the qualifying event (36 months minus 8 months).
Otherwise, when the qualifying event is the end of employment or
reduction of the employee’s hours of employment, COBRA
11CONTINUATION COVERAGE RIGHTS UNDER COBRA
Disability extension of 18-month period Other Coverage Options
of continuation coverage Instead of enrolling in COBRA continuation coverage, there may be
If you or anyone in your family covered under the Plan is determined other coverage options for you and your family through the Health
by the Social Security Administration to be disabled and you notify Insurance Marketplace, Medicaid, or other group health plan
the Plan Administrator in a timely fashion, you and your entire family coverage options (such as a spouse’s plan) through what is called a
may be entitled to receive up to an additional 11 months of COBRA “special enrollment period.” Some of these options may cost less
continuation coverage, for a total maximum of 29 months. The than COBRA continuation coverage. You can learn more about many
disability would have to have started at some time before the 60th of these options at www.healthcare.gov.
day of COBRA continuation coverage and must last at least until the
end of the 18-month period of continuation coverage. If You Have Questions
Questions concerning your Plan or your COBRA continuation
The disability extension is available only if you notify the Plan
coverage rights should be addressed to the contact or contacts
Administrator in writing of the Social Security Administration’s
identified below. For more information about your rights under
determination of disability within 60 days after the latest of the date
ERISA, including COBRA, the Health Insurance Portability and
of the Social Security Administration’s disability determination; the
Accountability Act (HIPAA), and other laws affecting group health
date of the covered employee’s termination of employment or
plans, contact the nearest Regional or District Office of the U.S.
reduction in hours; and the date on which the qualified beneficiary
Department of Labor’s Employee Benefits Security Administration
loses (or would lose) coverage under the terms of the Plan as a result
(EBSA) in your area or visit the EBSA website at www.dol.gov/ebsa.
of the covered employee’s termination or reduction in hours. You
(Addresses and phone numbers of Regional and District EBSA
must also provide this notice within 18 months after the covered
Offices are available through EBSA’s website.)
employee’s termination or reduction in hours in order to be entitled
to this extension.
Keep Your Plan Informed of Address
Second qualifying event extension of Changes
In order to protect your family’s rights, you should keep the Plan
18-month period of continuation Administrator informed of any changes in the addresses of family
coverage members. You should also keep a copy, for your records, of any
If your family experiences another qualifying event while receiving 18 notices you send to the Plan Administrator.
months of COBRA continuation coverage, the spouse and
dependent children in your family can get up to 18 additional months Plan Contact Information
of COBRA continuation coverage, for a maximum of 36 months, if For further information regarding the plan and COBRA continuation,
notice of the second qualifying event is properly given to the Plan. please contact:
This extension may be available to the spouse and any dependent
Coke Florida Benefits Supervisor
children receiving continuation coverage if the employee or former
10117 Princess Palm Avenue, Suite 400, Tampa, FL 33610
employee dies, becomes entitled to Medicare benefits (under Part A,
813.327.7289
Part B, or both), or gets divorced or legally separated, or if the
dependent child stops being eligible under the Plan as a dependent
child, but only if the event would have caused the spouse or
dependent child to lose coverage under the Plan had the first
qualifying event not occurred.
SUMMARIES OF BENEFITS AND COVERAGE (SBCS)
As required by the Affordable Care Act, Summaries of Benefits and Coverage (SBCs) are available at MDFCokeflorida@ceridian.com. If you
would like a paper copy of the SBCs (free of charge), you may also call Coke Florida benefits hot-line at 877.340.0929.
Coke Florida is required to make SBCs available that summarize important information about health benefit plan options in a standard
format, to help you compare across plans and make an informed choice. The health benefits available to you provide important protection
for you and your family and choosing a health benefit option is an important decision.
12PREMIUM ASSISTANCE UNDER MEDICAID AND THE
CHILDREN’S HEALTH INSURANCE PROGRAM (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and
health coverage from your employer, your state may have a premium you think you or any of your dependents might be eligible for either of these
assistance program that can help pay for coverage, using funds from their programs, contact your State Medicaid or CHIP office or dial 877.KIDS.NOW
Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your
or CHIP, you won’t be eligible for these premium assistance programs but you state if it has a program that might help you pay the premiums for an
may be able to buy individual insurance coverage through the Health employer-sponsored plan.
Insurance Marketplace. For more information, visit www.healthcare.gov.
If you or your dependents are eligible for premium assistance under Medicaid
If you or your dependents are already enrolled in Medicaid or CHIP and you or CHIP, as well as eligible under your employer plan, your employer must
live in a State listed below, contact your State Medicaid or CHIP office to find allow you to enroll in your employer plan if you aren’t already enrolled. This is
out if premium assistance is available. called a “special enrollment” opportunity, and you must request coverage
within 60 days of being determined eligible for premium assistance. If you
have questions about enrolling in your employer plan, contact the Department
of Labor at www.askebsa.dol.gov or call 866.444.EBSA (3272).
If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is
current as of July 31, 2020. Contact your State for more information on eligibility –
1. ALABAMA – Medicaid KCHIP Website:https://kidshealth.ky.gov/Pages/index.aspx 24. NORTH DAKOTA – Medicaid
Website: http://myalhipp.com/ Phone: 1-877-524-4718 Website: http://www.nd.gov/dhs/services/medicalserv/
Phone: 1-855-692-5447 Kentucky Medicaid Website: https://chfs.ky.gov medicaid/
2. ALASKA - Medicaid 12. LOUISIANA – Medicaid Phone: 1-844-854-4825
The AK Health Insurance Premium Payment Program Website: www.medicaid.la.gov or www.ldh.la.gov/lahipp 25. OKLAHOMA – Medicaid and CHIP
Website: http://myakhipp.com/ Phone: 1-888-342-6207 (Medicaid hotline) or Website: http://www.insureoklahoma.org
Phone: 1-866-251-4861 1-855-618-5488 (LaHIPP) Phone: 1-888-365-3742
Email: CustomerService@MyAKHIPP.com 13. MAINE – Medicaid 26. OREGON – Medicaid
Medicaid Eligibility: http://dhss.alaska.gov/dpa/Pages/ Enrollment Website: Website: http://healthcare.oregon.gov/Pages/index.aspx
medicaid/default.aspx https://www.maine.gov/dhhs/ofi/applications-forms http://www.oregonhealthcare.gov/index-es.html
3. ARKANSAS - Medicaid Phone: 1-800-442-6003 TTY: Maine relay 711 Phone: 1-800-699-9075
Website: http://myarhipp.com/ Private Health Insurance Premium Webpage: 27. PENNSYLVANIA – Medicaid
Phone: 1-855-MyARHIPP (855-692-7447) https://www.maine.gov/dhhs/ofi/applications-forms Website: https://www.dhs.pa.gov/providers/Providers/
4. CALIFORNIA – Medicaid Phone: 1-800-977-6740 TTY: Maine relay 711 Pages/Medical/HIPP-Program.aspx
Website: https://www.dhcs.ca.gov/services/Pages/TPLRD_ 14. MASSACHUSETTS – Medicaid and CHIP Phone: 1-800-692-7462
CAU_cont.aspx Website: http://www.mass.gov/eohhs/gov/departments/ 28. RHODE ISLAND – Medicaid and CHIP
Phone: 916-440-5676 masshealth/ Website: http://www.eohhs.ri.gov/
5. COLORADO – Health First Colorado (Colorado’s Medicaid Phone: 1-800-862-4840 Phone: 1-855-697-4347, or 401-462-0311 (Direct RIte Share
Program) & Child Health Plan Plus (CHP+) Health First 15. MINNESOTA – Medicaid Line)
Colorado Website: https://www.healthfirstcolorado.com/ Website: https://mn.gov/dhs/people-we-serve/seniors/ 29. SOUTH CAROLINA – Medicaid
Health First Colorado Member Contact Center: health-care/health-care-programs/programs-and-services/ Website: https://www.scdhhs.gov
1-800-221-3943/ State Relay 711 other-insurance.jsp Phone: 1-888-549-0820
CHP+: https://www.colorado.gov/pacific/hcpf/ Phone: 1-800-657-3739
30. SOUTH DAKOTA - Medicaid
child-health-plan-plus 16. MISSOURI – Medicaid Website: http://dss.sd.gov
CHP+ Customer Service: 1-800-359-1991/ State Relay 711 Website: http://www.dss.mo.gov/mhd/participants/pages/ Phone: 1-888-828-0059
Health Insurance Buy-In Program (HIBI): hipp.htm
https://www.colorado.gov/pacific/hcpf/health-insurance- 31. TEXAS – Medicaid
Phone: 573-751-2005
buy-program HIBI Customer Service: 1-855-692-6442 Website: http://gethipptexas.com/
17. MONTANA – Medicaid Phone: 1-800-440-0493
6. FLORIDA – Medicaid Website: http://dphhs.mt.gov/
Website: https://www.flmedicaidtplrecovery.com/ 32. UTAH – Medicaid and CHIP
MontanaHealthcarePrograms/HIPP
flmedicaidtplrecovery.com/hipp/index.html Medicaid Website: https://medicaid.utah.gov/
Phone: 1-800-694-3084
Phone: 1-877-357-3268 CHIP Website: http://health.utah.gov/chip
18. NEBRASKA – Medicaid Phone: 1-877-543-7669
7. GEORGIA – Medicaid Website: http://www.ACCESSNebraska.ne.gov
Website: https://medicaid.georgia.gov/health-insurance- 33. VERMONT– Medicaid
Phone: 1-855-632-7633
premium-payment-program-hipp Website: http://www.greenmountaincare.org/
Lincoln: 402-473-7000
Phone: 1-678-564-1162 ext 2131 Phone: 1-800-250-8427
Omaha: 402-595-1178
8. INDIANA – Medicaid Healthy Indiana Plan for low-income 34. VIRGINIA – Medicaid and CHIP
19. NEVADA – Medicaid
adults 19-64 Website: https://www.coverva.org/hipp/
Medicaid Website: http://dhcfp.nv.gov
Website: http://www.in.gov/fssa/hip/ Medicaid Phone: 1-800-432-5924
Medicaid Phone: 1-800-992-0900
Phone: 1-877-438-4479 CHIP Phone: 1-855-242-8282
20. NEW HAMPSHIRE – Medicaid
All other Medicaid 35. WASHINGTON – Medicaid
Website: https://www.dhhs.nh.gov/oii/hipp.htm
Website: https://www.in.gov/medicaid/ Website: https://www.hca.wa.gov/
Phone: 603-271-5218
Phone 1-800-457-4584 Phone: 1-800-562-3022
Toll free number for the HIPP program: 1-800-852-3345, ext
9. IOWA – Medicaid and CHIP (Hawki) 5218 36. WEST VIRGINIA – Medicaid
Medicaid Website: https://dhs.iowa.gov/ime/members Website: http://mywvhipp.com/
21. NEW JERSEY – Medicaid and CHIP
Medicaid Phone: 1-800-338-8366 Toll-free phone: 1-855-MyWVHIPP (1-855-699-8447)
Medicaid Website: http://www.state.nj.us/humanservices/
Hawki Website: http://dhs.iowa.gov/Hawki 37. WISCONSIN – Medicaid and CHIP
dmahs/clients/medicaid/
Hawki Phone: 1-800-257-8563 Website: https://www.dhs.wisconsin.gov/
Medicaid Phone: 609-631-2392
10. KANSAS-Medicaid CHIP Website: http://www.njfamilycare.org/index index. badgercareplus/p-10095.htm
Website: http://www.kdheks.gov/hcf/default.htm html CHIP Phone: 1-800-701-0710 Phone: 1-800-362-3002
Phone: 1-800-792-4884 38. WYOMING – Medicaid
22. NEW YORK – Medicaid
11. KENTUCKY-Medicaid Website: https://www.health.ny.gov/health_care/medicaid/ Website: https://health.wyo.gov/healthcarefin/medicaid/
Kentucky Integrated Health Insurance Premium Payment Phone: 1-800-541-2831 programs-and-eligibility/
Program (KI-HIPP) Phone: 1-800-251-1269
23. NORTH CAROLINA – Medicaid
Website: https://chfs.ky.gov/agencies/dms/member/Pages/
Website: https://medicaid.ncdhhs.gov/
kihipp.aspx - Phone: 1-855-459-6328
Phone: 919-855-4100
Email: KIHIPP.PROGRAM@ky.gov
To see if any other states have added a premium assistance program since July 31, 2020, or for more information on special enrollment rights, contact either:
U.S. Department of Labor U.S. Department of Health and Human Services
Employee Benefits Security Administration Centers for Medicare & Medicaid Services
www.dol.gov/agencies/ebsa www.cms.hhs.gov
866.444.EBSA (3272) 877.267.2323, Menu Option 4, Ext. 61565
13You can also read