Nonoperative Management of Appendicitis in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COLLECTIVE REVIEW
Nonoperative Management of Appendicitis in
Adults: A Systematic Review and Meta-Analysis
of Randomized Controlled Trials
John M Findlay, BMedSci, BMBS (hons), MRCS, Jihène el Kafsi, MBBS, FRCS, Clare Hammer, MBChB, MRCS,
Jeffrey Gilmour, MPhil, FRCS, Richard S Gillies, MD, FRCS, Nicholas D Maynard, MS, FRCS
Appendicitis remains the most common intra-abdominal recommended in the US and Europe.10-12 However, these
surgical emergency, with an annual incidence of 250,000 guidelines, reviews, and meta-analyses were published
patients in the US, 50,000 patients in the UK, and a life- before a recent relevant RCT in 2015.13 Although this
time risk of 8%.1,2 The vast majority of these cases are did not demonstrate noninferiority of antibiotics, the sig-
managed by appendectomy, underpinned by the dogma nificant reduction in complications seen with antibiotics
that uncomplicated appendicitis inevitably progresses to has frequently been interpreted as additional evidence
abscess formation, gangrene, and perforation. However, that antibiotics represent a valid alternative to surgery.14,15
more routine use of imaging has improved diagnostic The aim of this study was to perform an up-to-date system-
accuracy and identification of the majority of patients atic review and meta-analysis of primary antibiotic therapy
with uncomplicated appendicitis at admission.3 vs surgery for the management of acute appendicitis.
In parallel, there is increasing recognition that the path-
ogenesis and natural history of appendicitis is variable.
METHODS
Logically, some patients will have an episode that will
not progress or perhaps may even be self-limiting,4 and Literature search
antibiotics alone will sometimes suffice. Indeed, this A literature search was performed of the PubMed, EMBASE,
approach is necessary in remote environments5 and histor- and Cochrane Central Register of Controlled Trials in May
ically antibiotics have been considered the treatment of 2016 by 2 authors (JEK and CH), independently using stan-
choice for delayed presentations with an appendix mass.6 dardized data collection software, in accordance with the
Consequently, a number of randomized controlled trials Preferred Reporting Items for Systematic Reviews and
(RCTs) and attendant meta-analyses have explored the role Meta-Analyses (PRISMA) and Meta-Analysis Of Observa-
of routine nonoperative management with antibiotics. tional Studies in Epidemiology (MOOSE) guidelines.16,17
Some have concluded that it represents an equally valid The following search terms were used: ([antibiotics OR
alternative to surgery for uncomplicated appendicitis, appendectomy OR appendicectomy OR surgery] AND
with an equivalent safety profile and possibly, fewer com- [trial OR randomized] AND [appendicitis OR appendix]).
plications,7,8 although this view was not supported by Bibliographies of retrieved articles were searched. Any
the most recent Cochrane review of 5 RCTs.9 At present, disagreement was resolved by a third author (JMF). Data
appendectomy remains the treatment of choice were extracted and studies similarly assessed by 2 authors
(JMF and JEK). We contacted the corresponding authors
of 3 studies with questions regarding methodology and
Disclosure Information: Nothing to disclose.
requests for data,18-20 although none could be provided.
Disclosures outside the scope of this work: Dr Findlay has previously
received an honorarium for a lecture from Heibling Consulting and Inclusion criteria
Research AG.
We included randomized and quasi-randomized prospec-
Support: Dr Findlay is supported by the NIHR Oxford Biomedical
Research Centre. tive controlled trials, randomizing patients aged 16 and
older to either primary antibiotic therapy or appendec-
Received July 27, 2016; Revised September 13, 2016; Accepted September
13, 2016. tomy for acute appendicitis.
From the Oxford OesophagoGastric Centre, Churchill Hospital (Findlay, el
Kafsi, Gillies, Maynard) and the Department of Emergency Surgery, John
Radcliffe Hospital (Hammer, Gilmour), Oxford University Hospitals NHS Endpoints
Foundation Trust; and NIHR Oxford Biomedical Research Centre (Fin- Successful treatment was defined pragmatically as resolu-
dlay), Churchill Hospital, Oxford, UK. tion of the presenting acute episode of appendicular inflam-
Correspondence address: John M Findlay, BMedSci, BMBS (hons),
MRCS; Oxford OesophagoGastric Centre, Churchill Hospital, Oxford, mation without recurrence: ie removal of the appendix
OX3 7LJ, UK. email: john.findlay@oncology.ox.ac.uk without subsequent inflammation of the stump or ileum/
ª 2016 by the American College of Surgeons. Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jamcollsurg.2016.09.005
All rights reserved. 814 ISSN 1072-7515/16Vol. 223, No. 6, December 2016 Findlay et al Nonoperative Management of Appendicitis 815
due to methodologic and comparison heterogeneity,
Abbreviations and Acronyms although we performed sensitivity analyses using fixed ef-
GRADE ¼ Grading of Recommendations Assessment, fects, and individual studies. For binary variables Mantel-
Development, and Evaluation Haenszel risk ratio (RR) was used. For the 2 studies18,20
ITT ¼ intention to treat
presenting standard error (SEM) rather than standard de-
PP ¼ per protocol
RCT ¼ randomized controlled trial viation (SD), we converted the former to the latter. One
RR ¼ risk ratio study presented length of stay as median and range, rather
than mean and SD13; the latter were estimated.21 Funnel
plots were inspected visually for evidence of asymmetry.
All analysis was performed using Review Manager v5.222
cecum, or significant improvement in clinical/biochemical
and R v3.0.2.23
evidence of inflammation, not requiring further antibiotics
or appendectomy. This was either during the initial episode
or admission, or at 1 year. Recurrent appendicitis was RESULTS
defined as a clinical or radiologic diagnosis. Complicated Literature search
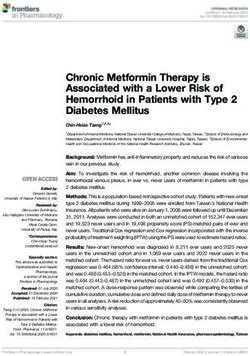
appendicitis was defined as intra-abdominal pus, enteric There were 1,146 studies identified, 69 of which were
contamination, or necrotic/gangrenous appendicitis. For retrieved for full text evaluation (Fig. 1). Seven RCTs
2 studies not stipulating the presence of pus (all categorized were identified. One was excluded due to subsequent
as phlegmonous, gangrenous, or perforated18,19), gangrene retraction.24
or perforation were used.
Complications were as defined in studies. Variable pre- Study characteristics and quality
sentation precluded meaningful synthesis of complications Six RCTs conducted between 1992 and 2012 were
reported by all studies, so we performed pragmatic analyses included (Table 1),13,18-20,25,26 2 with noninferiority de-
for all, minor, and major complications. Minor complica- signs.13,25 A total of 1,724 patients were randomized to
tions included wound infections, presumed adhesional/ antibiotics (n ¼ 837) or surgery (n ¼ 887). Studies varied
wound pain, urinary catheterization at discharge, minor considerably in their interventions, inclusion, exclusion,
anesthetic complications (eg tooth injury), and fungal and diagnostic criteria. All reported a maximum 1-year
infections. Major complications constituted death, follow-up. None were blinded. Randomization was by
intra-abdominal abscess/post-intervention peritonitis, sealed envelope,13,19 computer generation,25 date of
enterocutaneous fistula, major medical complications birth,18 or an unclear method.20,26 One study18 allowed
(eg pneumonia, acute coronary syndrome, pulmonary crossover after randomization, whereby clinicians or sur-
embolism, Clostridium difficile colitis), incisional hernia, geons could alter treatment. All except 1 study19 described
wound dehiscence, or surgery for bowel obstruction. dropouts and withdrawals.
Overall, there were many generic areas of potential bias.
Meta-analysis These included major differences in inclusion, exclusion,
Two analyses were performed for all comparisons: and diagnostic criteria; differences in antibiotics and ther-
intention-to-treat (ITT) and per protocol (PP). For the apy duration; major variability in surgical approach (open
index admission, it was possible to perform a PP analysis procedures being used selectively); follow-up methods;
that included patients crossing over after randomization and definition and reporting of complications.
in 1 study.18 However, this could not be performed at 1
year. For ITT, all patients were included, irrespective of Inclusion, diagnostic, and exclusion criteria
protocol violations and follow-up. For PP, only patients Five studies included patients aged 18 and older; 1 study
completing treatment per protocol and follow-up at the included patients 16 and older.20 Two had upper age
relevant time point were included. For 1 study,13 although limits of 60 years13 and 50 years.19 One included only
a few patients were formally lost to follow-up, the authors male patients.19 Two studies mandated CT diagnosis,13,25
were confident they had identified subsequent appendec- and 3 had clinical diagnosis with or without ultrasound/
tomies. These patients were therefore included in primary CT18 or ultrasound alone alone.26
but not secondary analyses. Overall, exclusion criteria effectively amounted to
radiologic or clinical evidence of perforation or abscess
Statistical analysis formation. Four studies excluded radiologic13,25 or clinical
Heterogeneity was assessed using chi-square (p < 0.05), suspicion of perforation or abscess.19,26 One study18 did
and quantified using I2. We used random effects models not formally exclude such patients, but clinicians could816 Findlay et al Nonoperative Management of Appendicitis J Am Coll Surg
Identification Records identified Records identified Records identified
through PubMed through EMBASE through Cochrane
(n =965) (n =431) (n =508)
Records after duplicates removed
(n =1,146)
Screening
Records screened Records excluded
(n = 1,146) (n = 1,077)
Full-text articles Full-text articles excluded,
assessed for eligibility with reasons
Eligibility
(n = 69)
(n=63)
n=24 not assessing
Studies included in outcome of interest
qualitative synthesis n = 14 review
(n = 6) n= 3 meta-analyisis
n= 12 letter
n=8 non-randomised
Included
n=1 study proposal
n=1 RCT subsequently
Studies included in retracted
quantitative synthesis
(meta-analysis)
(n = 6)
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. RCT, randomized controlled trial.
alter treatments if they felt it was justified. Two also Appendectomy
excluded possible malignancy on CT13,25; 1 excluded All studies except one18 included either open or laparo-
any patient with an appendix >15 mm in diameter.26 scopic procedures, performed at the discretion of the sur-
One study13 excluded patients with a serious systemic geon. One did not present this information18; excluding
illness or the presence of an appendicular fecolith. this, open procedures accounted for 71.4% (584 of
818). No further operative details were provided. For pa-
tients randomized to surgery, antibiotics were limited to a
Primary antibiotic therapy
single prophylactic dose in 3 studies13,18,25 and were not
Five studies involved a variable period of intravenous an- stipulated by 3 studies. Three18,25,26 stipulated an unde-
tibiotics for at least 1,18,25 2,19,26 or 3 days13,20; 1 study25 fined postoperative course in the presence of complicated
used oral antibiotics in the absence of nausea or vomiting. appendicitis; this was unclear in 2,19,20 while 1 did not use
Seven to 10 days of oral antibiotics were used thereafter. postoperative antibiotics.13
Variable combinations of penicillins, cephalosporins, car-
bopenems, or fluoroquinolones were used, in combina-
tions with a nitroimidazole. Criteria for converting to Endpoints
appendectomy varied, but essentially constituted deterio- All studies presented the number of patients randomized
ration or failure to improve within 24 to 48 hours. to antibiotics subsequently treated for failure or recurrentVol. 223, No. 6, December 2016
Table 1. Studies Included
First author,
y Population, n, ITT (PP) Diagnostic Exclusions Antibiotic therapy Operation Potential risks of bias
Salminen,13 Age 18 to 60 y; Finland CT Fecolith; possible Hospital: ertapenem IV Open: 257; lap: 15; AB: x1 Partly incomplete follow-up;
2015 (2009-2012); AB: 257 perforation; abscess; (3 d); discharge: preop dose postop laparoscopy at discretion of
(256); S: 273 (272) possible tumor; levofloxacin þ surgeon; no postoperative
significant systemic metronidazole (7 d) antibiotics, even in presence
illness of contamination;
exclusion: age > 60 y and
significant systemic illness;
incomplete description of
some complications
Vons,25 2011 Age >18 y; France (2004- CT Perforation, abscess, Hospital: co-amoxiclav po/ Open: 41; lap: 78; AB: Laparoscopy at discretion of
2007); AB: 123 (106); possible tumor/ iv (1 d); discharge: co- single preop dose surgeon; oral antibiotics
S: 120 (98) appendix >15 mm amoxiclav po (8 d total) postop unless nauseated or
vomiting
Hansson,18 Age >18 y; Sweden (2006- Clinical US/CT Nil formal; surgeons/ Hospital: cefuroxime þ Open: not specified; lap: Quasi-randomized; cross-over
2009 2007); AB: 202 (102) patients altered metronidazole iv (1 not specified; AB: single after randomization at
(including crossover treatment as thought d); discharge: preop dose postop patient/surgeon request;
115); S: 167 (130) appropriate ciprofloxacin þ laparoscopy at discretion of
(including crossover: metronidazole po (10 surgeon; incomplete and
219) d total) incompletely described
follow-up and data;
Findlay et al
nonstandardized
investigations
Turhan,20 Age >16 y; Turkey (2005- Clinical US and CT Nil formal Hospital: ampicillin þ Open 150; lap: 133; AB: Randomization method
2009 2006); AB: 107 (107); (antibiotic group only) gentamicin þ not specified unclear; significant disparity
S: 183 (183) metronidazole iv (3 d); in patients; allocation
discharge: ampicillin þ concealment: unclear;
metronidazole po (10 d) laparoscopy at discretion of
Nonoperative Management of Appendicitis
surgeon; drop-outs not
specified; use of US/CT
only in AB group, without
reporting negative
appendectomy rate;
postoperative antibiotics
unclear
Styrud,19 2006 Males age 18 to 50 y; Clinical Suspected perforation; C Hospital: cefotaxime þ Open: 116; lap: 8; AB: not Females excluded; incomplete
Sweden (1996-1999); reactive protein 18 y; Sweden (1992- Clinical þ US Generalized peritonitis Hospital: cefotaxime þ Open: 20; AB only if No prophylactic antibiotics
1995 1994); AB: 20 (20); S: tinidazole iv (2 d); perforation/spillage
20 (20) discharge: ofloxacin þ
tinidazole po (8 d)
AB, antibiotics; ITT, intention-to-treat group; lap, laparoscopic; po, per os; postop, postoperative; PP, per protocol group; preop, preoperative; S, surgery; US, ultrasound scan.
817818 Findlay et al Nonoperative Management of Appendicitis J Am Coll Surg
appendicitis. One18 excluded patients undergoing surgery 3.00% to 13.0%) and 9.00% (95% CI 4.00% to
from PP analysis without histologic evidence of appendi- 13.0%), respectively.
citis. However, we included these in the absence of a For patients treated successfully with antibiotics, recur-
similar mechanism for identifying false positives among rence within 1 year necessitating surgery (n ¼ 130) or an-
patients treated with antibiotics, and its reflection of clin- tibiotics (n ¼ 5) occurred in 135 of 759 (ITT 17.8%
ical practice. [95% CI 15.2% to 20.7%]) and 119 of 613 (PP 19.0%
Complications were variably reported and defined, [95% CI 16.5 to 22.7]). On meta-analysis, risks were
with a high risk of reporting bias. One study reported 15.0% (95% CI 8.00% to 22.0%) and 17.0% (95% CI
every complication encountered18; 1 stipulated only 11.0% to 24.0%), respectively.
wound infections.19 The other 4 studies13,18,20,25 reported Cumulatively, at 1 year, meta-analysed risks of antibi-
variable complications including intra-abdominal otics failure were 25.0% (95% CI 12.0% to 35.0%),
abscesses and enterocutaneous fistulae; 3 studies13,18,25 and 29.0% (95% CI 23.0% to 34.0%; p < 0.00001;
also reported wound hernias, postoperative pain/obstruc- Table 2; Fig. 2). Neither study attempting to do so
tive symptoms (subjective and unqualified), with 1 study18 demonstrated noninferiority.13,25 GRADE (Grading of
reporting more extensive minor complications. However, Recommendations Assessment, Development, and Evalu-
it is unclear whether additional complications were seen. ation) levels of evidence were low (PP), and very low (ITT
One study defined wound infection.13 None stratified and PP with crossover [Table 3]).
complication severity.
Risk of complicated appendicitis at surgery
Directness One study18 presenting only data for patients crossing
In addition to introducing bias, many factors above also over was excluded. Overall, there were no significant dif-
limited directness, ie applicability to the population of in- ferences in either index episode or 1-year risk of compli-
terest. These included the over-representation of open cated appendicitis at surgery (Table 4; eFigs. 1 and 2). For
procedures (laparoscopy representing the approach of the index admission, 24 of 632 (3.80%) patients treated
choice in the US and Europe,10-12 with less pain, fewer with antibiotics had complicated appendicitis (ITT),
complications, and shorter length of stay27,28), and varia- compared with 74 of 719 (10.3%) treated with surgery.
tions in inclusion, exclusion, and diagnostic criteria Per-protocol rates were 23 of 618 (3.72%) and 65 of
(such as major comorbidities and routine CT, which 693 (9.38%), respectively. At 1 year, these rates were 40
may not reflect standard practice10). of 632 (6.33%) and 74 of 719 (10.3%), and 36 of 619
(5.98%) and 65 of 593 (9.38%), respectively.
However, for patients in whom antibiotics failed,
Efficacy complicated appendicitis was considerably more likely:
Seventy-five of 834 patients (8.99%; 95% CI 7.49 to PP RR 6.21 (95% CI 1.68 to 23.0; p ¼ 0.006;
11.1) randomized to antibiotics underwent appendec- Table 3; eFig. 3). As a proportion of patients undergoing
tomy during their initial treatment (74 of 720 [10.2%] surgery, 25 of 54 (46.3%; ITT) and 23 of 65 (35.4%; PP)
PP). Antibiotics were less effective than surgery: ITT had complicated appendicitis. At 1 year, significance did
RR 0.92 (95% CI 0.87 to 0.97; p ¼ 0.002), PP (0.91 not persist, with recurrent episodes no more likely to be
[95% CI 0.87 to 0.96]; p ¼ 0.0002), and crossover complicated: 16 of 117 (13.7%; ITT), and 14 of 108
(0.90 [95% CI 0.86 to 0.94]; p < 0.00001; Table 2; (12.7%; PP). Again GRADE levels were low and very
Fig. 2). This constituted failure in 8.00% (95% CI low.
Table 2. Successful Treatment of (Presumed) Appendicitis
Analysis Effect size, RR (95% CI) n I2, % Chi-square p Value Model GRADE quality
Successful treatment at initial episode
ITT 0.92 (0.87e0.97) 6 80 24.42 0.002 Random Very low
PP 0.91 (0.87e0.96) 6 74 19.41 0.0002 Random Low
PP þ crossover 0.90 (0.86e0.94) 6 64 14.08Vol. 223, No. 6, December 2016 Findlay et al Nonoperative Management of Appendicitis 819
Figure 2. One-year efficacy (per protocol analysis).
Risk of complications different scales. Salminen and coworkers13 reported
One study did not present sufficient data to assess minor more pain at discharge and at 1 week with surgery. Eriks-
and major complications individually.19 Another did not son and colleagues29 also found significantly lower visual
provide sufficient data to perform PP meta-analysis.18 analogue scale scores at up to 10 days, associated with
Overall, there were no differences in complications at 1 less morphine consumption.
year (Table 4; eFig. 4). On sensitivity analysis using fixed
effects, antibiotics were associated with fewer complica- Inflammatory response
tions, although random effects were mandated by severe Eriksson and colleagues29 reported a significant reduction
study heterogeneity (I2 >76%), and significance was in white cell count for up to 10 days with antibiotics,
reliant on considerable rates of undefined adhesional/ although C reactive protein levels were not different. A
obstructive symptoms and wound infections after surgery lower temperature was also found on days 1 and 2.
in 1 study.13 Similarly, there were no differences in minor
(eFig. 5) or major complications (eFig. 6; Table 4). The Incidental tumors
GRADE recommendations were of very low quality, In 5 of 843 (0.59%) patients undergoing surgery, for
due to risks of bias and directness discussed earlier, plus whom this outcome was reported, incidental tumors
a lack of definitions of complications and possible selec- were identified: 3 malignancies requiring right hemi-
tive reporting. colectomy, 3 neuroendocrine tumors, and 1 adenoma
with dysplasia.
Length of stay
Antibiotics were associated with a longer length of stay on Cost of treatment
PP analysis: mean difference 0.48 days (95% CI 0.10 to Two studies reported costs of treatment, although for the
0.85 days; n ¼ 4 studies; p ¼ 0.01; Table 5; eFig. 7), primary episode only. Hansson and associates18 reported
but significance was dependent on 1 low quality study20 significantly lower costs with antibiotics vs surgery (17.7%
(GRADE recommendation very low). reduction on ITT; 51.2% on a PP plus cross-over basis).
No difference was reported by Turhan and coauthors.20
Length of sick leave
Antibiotics were associated with a shorter sick leave on ITT
and PP plus crossover analyses (mean difference -2.13 days DISCUSSION
(95% CI -3.85 to -0.41); n ¼ 4 studies; p ¼ 0.020), but There continues to be great interest in nonoperative man-
not on PP analysis (n ¼ 2 studies; p ¼ 0.070; GRADE agement of appendicitis, particularly because 1 recent
recommendation very low; Table 5; eFig. 8). meta-analysis7 and subsequent RCT13 concluded antibi-
otics to be as safe asdif not safer thandsurgery. In this
Post-intervention pain systematic review and meta-analysis of 6 RCTs, we found
Vons and colleagues25 found no differences in the dura- antibiotics to successfully treat the initial episode of un-
tion of pain (visual analogue scale 4), unlike Hansson complicated acute appendicitis in 91% of patients. These
and associates,18 who reported longer duration with sur- patients had a marginally longer length of hospital stay
gery. Meta-analysis was not possible. Two studies assessed (although heavily influenced by 1 low quality study20),
the visual analogue scale at variable time points, using but a quicker return to work and less pain. However,820
Table 3. Grading of Recommendations Assessment, Development, and Evaluation Analysis
Analysis Population Risk of bias Directness Consistency Precision Publication bias Overall quality
Findlay et al
Successful treatment
ITT 6 studies; 1,724 patients High; very serious Serious limitations{,# No limitations No limitations None detected Very low
limitations*,y,z,x,k
PP 6 studies; 1,546 patients Moderate; serious Serious limitations{,# No limitations No limitations None detected Low
(1,440 at 1 y) limitationsy,z,k
PP þ crossover 6 studies; 1,648 patients High; very serious Serious limitationsx,k,{ No limitations No limitations None detected Very low
limitations*,y,z,x,k
Nonoperative Management of Appendicitis
Complicated appendicitis
ITT 6 studies; 1,641 patients High; serious Serious limitations{,# No limitations No limitations None detected Very low
limitationsy,z,k **
PP 6 studies; 1,546 patients Moderate; serious Serious limitations{,# No limitations No limitations None detected Low
(1,440 at 1 y) limitationsy,z,k,**
PP þ crossover 6 studies; 1,648 patients High; very serious Serious limitationsx,k No limitations No limitations None detected Very low
limitations*,y,z,x,k,**
Complications
Overall
ITT 6 studies; 1,724 patients High; very serious Serious limitationsx,{,# No limitations No limitations None detected Very low
limitations*,y,z,x,k,yy
PP 4 studies; 1,229 patients High; serious limitations# Serious limitations{,# No limitations No limitations None detected Very low
Minor and major
complications
ITT 5 studies; 1,468 patients High; very serious Serious limitations{,# No limitations No limitations None detected Very low
limitations*,y,z,x,k,yy,zz
PP 4 studies; 977 patients High; serious Serious limitation{,# No limitations No limitations None detected Very low
limitations*,y,z,x,k,yy
Length of stay and sick
leave
ITT 6 studies; 1,724 patients High; very serious Serious limitationsx,{,# No limitations No limitations None detected Very low
limitations*,y,z,x,k
PP 4 studies; 768 patients High; very serious Serious limitationsx,{,# No limitations No limitations None detected Very low
limitations*,y,z,x,k
*Randomization by date of birth.18
y
Unclear randomization.20
z
Variable/incomplete follow-up.13,18
x
High protocol violations/cross-over/withdrawal rate.18e¼different diagnostic criteria between arms.20
k
Variable diagnostic inclusion criteria.
{
Variable antibiotic therapy.
#
Variable definitions of complicated appendicitis.
J Am Coll Surg
**Undefined complications.
yy
Possible selective reporting of complications.
zz
Likely underlying differences in discharge criteria.Vol. 223, No. 6, December 2016 Findlay et al Nonoperative Management of Appendicitis 821
Table 4. Risk of Complicated Appendicitis at Operation
Analysis Risk ratio (95% CI) n I2 Chi-square p Value Model GRADE quality
Cohort risk
Complicated
appendicitis at
surgery: initial
episode
ITT 0.44 (0.13e1.42); 0.38 (0.24e0.60) 5* 75 15.99 0.170;822 Findlay et al Nonoperative Management of Appendicitis J Am Coll Surg Table 5. Risk of Complications at 1 Year, Length of Stay, and Sick Leave Analysis Risk ratio (95% CI) n I2 Chi-square p Value Model GRADE Cohort risk, all complications (major and minor) ITT 0.53 (0.21e1.33); 0.51 (0.37e0.70) 6 80 24.45 0.170;
Vol. 223, No. 6, December 2016 Findlay et al Nonoperative Management of Appendicitis 823
Beyond the limitations of individual studies, there are REFERENCES
those specific to this meta-analysis. We used an inclusive 1. Hospital Episode Statistics Analysis, Health and Social Care
search strategy in order to identify all relevant articles; Information Centre. Hospital Episode Statistics, Admitted
however, it is possible that some were missed. Statistically, Patient Care - England, 2014-15. Health and Social Care
Information Center; 2015. Available at: http://content.
we used a different endpoint to define “successful” treat- digital.nhs.uk/catalogue/PUB19124.
ment than did other studies. We defined it pragmatically, 2. Addiss DG, Shaffer N, Fowler BS, et al. The epidemiology of
as resolution of the acute episode of presumed inflamma- appendicitis and appendectomy in the United States. Am J
tion without subsequent recurrence. In contrast to other Epidemiol 1990;132:910e925.
meta-analyses, we believed that complications may occur 3. Kim K, Kim YH, Kim SY, et al. Low-dose abdominal CT for
evaluating suspected appendicitis. N Engl J Med 2012;366:
despite complete resolution of the primary ileocecal in- 1596e1605.
flammatory process, while the presence of abdominal 4. Bhangu A, Soreide K, Di Saverio S, et al. Acute appendicitis:
pain or inflammation is similarly complex and may not modern understanding of pathogenesis, diagnosis, and man-
relate to any ongoing ileocecal inflammation. Similarly, agement. Lancet 2015;386:1278e1287.
we did not exclude patients undergoing negative appen- 5. Campbell MR, Johnston SL 3rd, Marshburn T, et al. Nonop-
erative treatment of suspected appendicitis in remote medical
dectomies from analysis because this does not represent care environments: implications for future spaceflight medical
the population of interest on an ITT basis and would care. J Am Coll Surg 2004;198:822e830.
bias analysis against surgery because no such mechanism 6. Senapathi PS, Bhattacharya D, Ammori BJ. Early laparoscopic
exists for identifying false positives in patients treated appendectomy for appendicular mass. Surg Endosc 2002;16:
with antibiotics. 1783e1785.
7. Varadhan KK, Neal KR, Lobo DN. Safety and efficacy of an-
tibiotics compared with appendicectomy for treatment of un-
CONCLUSIONS complicated acute appendicitis: meta-analysis of randomised
We found that overall, nonoperative management of controlled trials. BMJ 2012;344:e2156.
8. Rocha LL, Rossi FM, Pessoa CM, et al. Antibiotics alone
patients with uncomplicated appendicitis was successful versus appendectomy to treat uncomplicated acute appendi-
in the immediate term in 91%, but that this reduced to citis in adults: what do meta-analyses say? World J Emerg
71% at 1 year. The risk thereafter is unknown. In addi- Surg 2015;10:51.
tion, we found that nonoperative management was associ- 9. Wilms IM, de Hoog DE, de Visser DC, et al. Appendectomy
ated with less pain in the first week after treatment and a versus antibiotic treatment for acute appendicitis. Cochrane
Database Syst Rev 2011;[11]:CD008359.
quicker return to work, but would have missed occult 10. Ireland AoSoGBa. Commissioning Guide: Emergency General
tumors in a small number of patients. We found no Surgery (Acute Abdominal Pain). London: Royal College of
convincing evidence of a reduction in complications. Surgeons of England; 2014.
Selective primary antibiotic therapy can be discussed 11. Surgeons SoAGaE. Guidelines for Laparoscopic Appendec-
with patients on this basis, although with the caveat that tomy. Los Angeles: Society of American Gastrointestinal and
Endoscopic Surgeons; 2009.
these data relate primarily to open procedures, and derive 12. Sauerland S, Agresta F, Bergamaschi R, et al. Laparoscopy for
from a poor evidence base overall, with numerous areas of abdominal emergencies: evidence-based guidelines of the Eu-
bias. Laparoscopic appendectomy, therefore, remains the ropean Association for Endoscopic Surgery. Surg Endosc
treatment of choice overall for appendicitis, and has yet 2006;20:14e29.
to be compared with antibiotics by an RCT. Future 13. Salminen P, Paajanen H, Rautio T, et al. Antibiotic therapy vs
appendectomy for treatment of uncomplicated acute appendi-
RCTs should, in addition, focus on standardized outcomes citis: The APPAC randomized clinical trial. JAMA 2015;313:
reporting and study methodology, and investigating mech- 2340e2348.
anisms for more personalized use of antibiotics or surgery. 14. Pollara G, Marks M. Treatment of uncomplicated acute
appendicitis. JAMA 2015;314:1402.
Author Contributions 15. Livingston E, Vons C. Treating appendicitis without surgery.
JAMA 2015;313:2327e2328.
Study conception and design: Findlay, Hammer 16. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items
Acquisition of data: Findlay, Hammer, El Kafsi for systematic reviews and meta-analyses: the PRISMA state-
Analysis and interpretation of data: Findlay, Hammer, El ment. BMJ 2009;339:b2535.
Kafsi, Gilmour, Gillies, Maynard 17. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of
observational studies in epidemiology: a proposal for report-
Drafting of manuscript: Findlay, Hammer, El Kafsi, ing. Meta-analysis Of Observational Studies in Epidemiology
Gilmour, Gillies, Maynard (MOOSE) group. JAMA 2000;283:2008e2012.
Critical revision: Findlay, Hammer, El Kafsi, Gilmour, 18. Hansson J, Korner U, Khorram-Manesh A, et al. Randomized
Gillies, Maynard clinical trial of antibiotic therapy versus appendicectomy as824 Findlay et al Nonoperative Management of Appendicitis J Am Coll Surg
primary treatment of acute appendicitis in unselected patients. 25. Vons C, Barry C, Maitre S, et al. Amoxicillin plus clavulanic
Br J Surg 2009;96:473e481. acid versus appendicectomy for treatment of acute uncompli-
19. Styrud J, Eriksson S, Nilsson I, et al. Appendectomy versus cated appendicitis: an open-label, non-inferiority, randomised
antibiotic treatment in acute appendicitis. a prospective multi- controlled trial. Lancet 2011;377:1573e1579.
center randomized controlled trial. World J Surg 2006;30: 26. Eriksson S, Granstrom L. Randomized controlled trial of
1033e1037. appendicectomy versus antibiotic therapy for acute appendi-
20. Turhan AN, Kapan S, Kutukcu E, et al. Comparison of oper- citis. Br J Surg 1995;82:166e169.
ative and non operative management of acute appendicitis. 27. Sauerland S, Jaschinski T, Neugebauer EA. Laparoscopic
Ulus Travma Acil Cerrahi Derg [Turkish J Trauma Emerg versus open surgery for suspected appendicitis. Cochrane
Surg] 2009;15:459e462. Database Syst Rev 2010;[10]:CD001546.
21. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean 28. Wei B, Qi CL, Chen TF, et al. Laparoscopic versus open
and standard deviation from the sample size, median, range appendectomy for acute appendicitis: a metaanalysis. Surg
and/or interquartile range. BMC Medical Research Methodol- Endosc 2011;25:1199e1208.
ogy 2014;14:135. 29. Eriksson S, Josephson T, Styrud J. A high degree of accuracy is
22. Review Manager (program). 5.3 version. Copenhagen: The possible in the diagnosis of appendicitis. Laboratory tests,
Cochrane Collaboration; 2014. ultrasonography and computerized tomography are of great
23. R Core Team. R: A language and environment for statistical value. Lakartidningen 1999;96:3058e3061.
computing. Vienna, Austria: R Foundation for Statistical 30. Mason RJ, Moazzez A, Sohn H, et al. Meta-analysis of ran-
Computing; 2013. domized trials comparing antibiotic therapy with appendec-
24. Malik AA, Bari SU. Conservative management of acute appen- tomy for acute uncomplicated (no abscess or phlegmon)
dicitis. J Gastrointest Surg 2009;13:966e970. appendicitis. Surg Infect 2012;13:74e84.Vol. 223, No. 6, December 2016 Findlay et al Nonoperative Management of Appendicitis 824.e1
APPENDIX
eFigure 1. Index admission risk of complicated appendicitis (per protocol analysis).
eFigure 2. Two-year risk of complicated appendicitis (per protocol analysis).
eFigure 3. Index admission risk of complicated appendicitis for patients operated on (per protocol analysis).
eFigure 4. One-year complications (per protocol analysis).824.e2 Findlay et al Nonoperative Management of Appendicitis J Am Coll Surg
eFigure 5. One-year risk of minor complications (per protocol analysis).
eFigure 6. One-year risk of major complications (per protocol analysis).
eFigure 7. Length of stay (per protocol analysis).
eFigure 8. Length of sick leave (per protocol analysis).You can also read