In Children and Adolescents - TECHNICAL REPORT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

TECHNICAL REPORT
Diagnosis, Evaluation, and
Management of High Blood Pressure
in Children and Adolescents
Carissa M. Baker-Smith, MD, MS, MPH, FAAP, FAHA,a Susan K. Flinn, MA,b Joseph T. Flynn, MD, MS, FAAP,c David C.
Kaelber, MD, PhD, MPH, FAAP, FACP, FACMI,d Douglas Blowey, MD,e Aaron E. Carroll, MD, MS, FAAP,f Stephen R. Daniels,
MD, PhD, FAAP,g Sarah D. de Ferranti, MD, MPH, FAAP,h Janis M. Dionne, MD, FRCPC,i Bonita Falkner, MD,j Samuel S.
Gidding, MD,k Celeste Goodwin,l Michael G. Leu, MD, MS, MHS, FAAP,m Makia E. Powers, MD, MPH, FAAP,n Corinna Rea,
MD, MPH, FAAP,o Joshua Samuels, MD, MPH, FAAP,p Madeline Simasek, MD, MSCP, FAAP,q Vidhu V. Thaker, MD, FAAP,r,s,t
Elaine M. Urbina, MD, MS, FAAP,u SUBCOMMITTEE ON SCREENING AND MANAGEMENT OF HIGH BP IN CHILDREN
Systemic hypertension is a major cause of morbidity and mortality in
abstract
adulthood. High blood pressure (HBP) and repeated measures of HBP,
hypertension (HTN), begin in youth. Knowledge of how best to diagnose,
manage, and treat systemic HTN in children and adolescents is important aDivision of Cardiology, Department of Pediatrics, School of Medicine,
University of Maryland, Baltimore, Maryland; bConsultant, Washington,
for primary and subspecialty care providers. District of Columbia; cDivision of Nephrology, Department of Pediatrics,
University of Washington and Seattle Children’s Hospital, Seattle,
OBJECTIVES: To provide a technical summary of the methodology used Washington; Departments of dDivision of General Internal Medicine,
to generate the 2017 “Clinical Practice Guideline for Screening and Pediatrics and Population and Quantitative Health Sciences, Case
Western Reserve University and Center for Clinical Informatics
Management of High Blood Pressure in Children and Adolescents,” an update Research and Education, The MetroHealth System, Cleveland, Ohio;
to the 2004 “Fourth Report on the Diagnosis, Evaluation, and Treatment of
eUniversity of Missouri-Kansas City, Children’s Mercy Kansas City,
Children’s Mercy Integrated Care Solutions, Kansas City, Missouri;
High Blood Pressure in Children and Adolescents.” fDepartment of Pediatrics, School of Medicine, Indiana University,
Indianapolis, Indiana; gDepartment of Pediatrics, School of Medicine,
DATA SOURCES: Medline, Cochrane Central Register of Controlled Trials, and University of Colorado, Children’s Hospital Colorado, Aurora,
Colorado; hPreventive Cardiology Clinic, oPrimary Care at Longwood,
Excerpta Medica Database references published between January 2003 and and rDepartment of Medicine, Boston Children’s Hospital, Harvard
July 2015 followed by an additional search between August 2015 and July Medical School, Harvard University, Boston, Massachusetts; iDivision
of Nephrology, Department of Pediatrics, University of British
2016. Columbia and BC Children’s Hospital, Vancouver, British Columbia,
Canada; Departments of jMedicine and Pediatrics, Thomas Jefferson
STUDY SELECTION: English-language observational studies and randomized University, Philadelphia, Pennsylvania; kCardiology Division, Nemours
Cardiac Center, A. I. duPont Hospital for Children and Department
trials. of Pediatrics, Sidney Kimmel Medical College, Thomas Jefferson
University, Philadelphia, Pennsylvania; lNational Pediatric Blood
METHODS: Key action statements (KASs) and additional recommendations Pressure Awareness Foundation, Prairieville, Louisiana; Departments
regarding the diagnosis, management, and treatment of HBP in youth were of mPediatrics and Biomedical Informatics and Medical Education,
University of Washington, University of Washington Medicine
the product of a detailed systematic review of the literature. A content Information Technology Services, and Seattle Children’s Hospital,
outline establishing the breadth and depth was followed by the generation of Seattle, Washington; nDepartment of Pediatrics, Morehouse School of
Medicine, Atlanta, Georgia; Departments of pPediatrics and Internal
4 patient, intervention, comparison, outcome, time questions. Key questions Medicine, McGovern School of Medicine, University of Texas, Houston,
Texas; qDepartment of Pediatrics, UPMC Shadyside Family Medicine
addressed: (1) diagnosis of systemic HTN, (2) recommended work-up of
systemic HTN, (3) optimal blood pressure (BP) goals, and (4) impact of high
BP on indirect markers of cardiovascular disease in youth. Once selected, To cite: Baker-Smith CM, Flinn SK, Flynn JT, et al. Diagnosis,
references were subjected to a 2-person review of the abstract and title Evaluation, and Management of High Blood Pressure in
Children and Adolescents. Pediatrics. 2018;142(3):e20182096
followed by a separate 2-person full-text review. Full citation information,
Downloaded from www.aappublications.org/news by guest on September 4, 2018
PEDIATRICS Volume 142, number 3, September 2018:e20182096 FROM THE AMERICAN ACADEMY OF PEDIATRICS
population data, findings, benefits and harms of the findings, as well as other
key reference information were archived. Selected primary references were
then used for KAS generation. Level of evidence (LOE) scoring was assigned
for each reference and then in aggregate. Appropriate language was used to
generate each KAS based on the LOE and the balance of benefit versus harm
of the findings. Topics that could not be researched via the stated approach
were (1) definition of HTN in youth, and (2) definition of left ventricular
hypertrophy. KASs related to these stated topics were generated via expert
opinion.
RESULTS: Nearly 15 000 references were identified during an initial literature
search. After a deduplication process, 14 382 references were available for
title and abstract review, and 1379 underwent full text review. One hundred
twenty-four experimental and observational studies published between 2003
and 2016 were selected as primary references for KAS generation, followed
by an additional 269 primary references selected between August 2015 and
July 2016. The LOE for the majority of references was C. In total, 30 KASs and 27
additional recommendations were generated; 12 were related to the diagnosis
of HTN, 13 were related to management and additional diagnostic testing, 3
to treatment goals, and 2 to treatment options. Finally, special additions to
the clinical practice guideline included creation of new BP tables based on
BP values obtained solely from children with normal weight, creation of a
simplified table to enhance screening and recognition of abnormal BP, and a
revision of the criteria for diagnosing left ventricular hypertrophy.
CONCLUSIONS: An extensive and detailed systematic approach was used to
generate evidence-based guidelines for the diagnosis, management, and
treatment of youth with systemic HTN.
INTRODUCTION who carefully evaluated the existing before assigning a recommendation
published literature. However, since strength.2
The 2017 “Clinical Practice Guideline the publication of the Fourth Report,
for Screening and Management of there has been a notable increase Systemic HTN is 1 of 7 markers of
High Blood Pressure in Children and in the number of peer-reviewed poor cardiovascular health, according
Adolescents” serves as an update primary references, review articles, to the American Heart Association.3
to the 2004 “Fourth Report on the and systematic reviews (SRs) related The presence of systemic HTN in
Diagnosis, Evaluation, and Treatment to high blood pressure (HBP) and childhood and adolescence is 1 of the
of High Blood Pressure in Children systemic hypertension (HTN) in key risk factors predictive of HTN
and Adolescents” (Fourth Report).1 youth. Hence, the CPG was developed and cardiovascular disease (CVD)
The Fourth Report was sponsored not only by including experts but also in adults.4– 6 Systemic hypertension
by the National Heart, Lung, and by using a reproducible, systematic in youth has been associated with
Blood Institute (NHLBI), whereas search and reference archival increased left ventricular mass
the 2017 Clinical Practice Guideline process, detailed study design (LVM), greater carotid intima-media
(CPG) is sponsored by the American evaluation, and evidence strength thickness (cIMT),5 stiffer arteries,7
Academy of Pediatrics (AAP) and determination. In developing the reduced endothelial function,8 and
has been endorsed by the American 30 key action statements (KASs) of renal9 as well as neurocognitive
College of Cardiology and by the the 2017 CPG, the subcommittee impairments.10 HBP in children has
American Heart Association. The members assessed the individual been shown to track into
authors of the Fourth Report relied and aggregate evidence quality adulthood,11,12 and HTN in adulthood
primarily on summary statements and incorporated the balance of is a leading cause of morbidity and
created by a panel of expert clinicians benefits and harms of the findings mortality.13– 15 For these reasons,
Downloaded from www.aappublications.org/news by guest on September 4, 2018
2 FROM THE AMERICAN ACADEMY OF PEDIATRICSappropriate diagnostic, management, 2. greater clarity for primary care and treatment/time (PICOT)
and treatment strategies should providers regarding the utility of questions, organized the literature
be used in children. However, the BP assessment and management search, structured the article review
diagnosis of HTN can be challenging of HTN in the pediatric population. and selection process, assisted with
and is often missed.16,17
archiving all selected references,
The request proposed a modification
Estimates of the prevalence of drafted the evidence table (ET)
to the screening process and
elevated blood pressure (BP) and and the technical report (TR).
safeguards against both under-
HTN in children are largely based on Kymika Okechukwu, MPA, was the
and overdiagnosis of HTN. New
analyses of weighted samples from the AAP staff representative for the
normative BP tables based on BP
NHANES.18 Analyses of more recent project. Susan K. Flinn, MA, was the
values obtained in children with
NHANES (1999–2012) data, as well as professional medical editor, who
normal BMI were proposed.25
other cross-sectional and prospective drafted and edited the text of the
Furthermore, given increasing
study data, suggest a strong CPG and assisted with editing the
evidence to support the use
association between obesity and HBP TR. Two librarians, knowledgeable
of ambulatory blood pressure
in youth,19,20
such that the prevalence in the process of SR, Kimberly Yang
monitoring (ABPM) for more
of childhood HTN is higher among and Emilie Ludeman, assisted the
accurately assessing BP, it was
children with overweight and obese epidemiologist in identifying search
proposed that the revision expand
status.21 Children and adolescents terms and conducting the literature
on the indications for ABPM.26 The
with specific chronic diseases, such search for reference selection in
new CPG was intended to specifically
as chronic kidney disease (CKD), Medline, Cochrane Central Register
incorporate methods for screening
also have an increased prevalence of of Controlled Trials (CENTRAL), and
and diagnosing target organ damage
elevated BP and HTN. According to Excerpta Medica dataBASE (Embase).
(TOD), to include data from the
the Chronic Kidney Disease (CKD) in pediatric antihypertensive clinical All subcommittee members played
Children study, 37% of youth with trials published since 2004, and an active role in the process of title
CKD had elevated systolic blood to provide additional information and abstract review, article retrieval
pressure (SBP) or diastolic blood regarding screening for secondary and storage in Mendeley,27 reference
pressure (DBP) (>90th percentile), causes of HTN. review, KAS generation, ET generation,
and 14% are hypertensive (based on and editing of the CPG document
In spring 2014, the AAP Executive
repeated BP assessment), with either sections. All conflicts of interests
Committee authorized the formation of
a SBP and/or DBP greater than or were disclosed at the beginning of the
the Screening and Management of High
equal to the 95th percentile.22– 24
process and updated throughout the
Blood Pressure in Children Clinical
Practice Guideline Subcommittee of process. Reported conflicts of interest
Stated Objective of the AAP the Council on Quality Improvement can be found at the end of this TR.
Regarding the Preparation of
and Patient Safety (henceforth, “the The subcommittee met face-to-
Updated “Clinical Practice Guideline
for Screening and Management of subcommittee”). face in June 2015 and March 2016.
High Blood Pressure in Children and Conference calls occurred every 2
Composition of the Subcommittee
Adolescents” to 4 weeks, along with frequent and
Members and Meetings
regular e-mail correspondence. These
On February 6, 2014, members of
The subcommittee comprised meetings, calls, and e-mails were used
the AAP Sections on Nephrology,
individuals with expertise in the to assess the evidence and to draft
Nutrition, and Cardiology and Cardiac
field of systemic HTN in youth, the CPG content. Given the broad
Surgery made a formal request to
including representatives from a range of representation and expertise,
the Executive Committee of the AAP
variety of relevant AAP committees. potential biases were managed
to sponsor a new pediatric HTN
The subcommittee was cochaired through group discussion and review
CPG focused on the evaluation and
by a pediatric nephrologist, Joseph of the data throughout the process.
management of HBP in children and
Flynn, MD, MS, FAAP, and a general
adolescents. Arguments made to Definitions
pediatrician, David Kaelber, MD,
support the generation of an updated
PhD, MPH, FAAP. Carissa Baker- •• Children and adolescents: youth 1
guideline included the following:
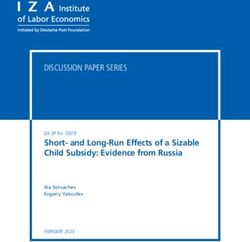
Smith, MD, MPH, MS, FAAP, FAHA, toFIGURE 1
Process flow map used for creation of the 2017 “Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and
Adolescents.”
CHANGES IN THE DEFINITION OF FORMULATION AND ARTICULATION OF Content Outline
HYPERTENSION IN YOUTH THE QUESTIONS ADDRESSED BY THE
CPG SUBCOMMITTEE The epidemiologist created a general
According to the Fourth Report and topic outline. The original content
its predecessors, the diagnosis of The process of creating the outline included 16 main topics
HTN in youth is purely a statistical CPG involved ensuring that key and a total of 100 subtopics that
determination based on the topics related to HTN in youth determined the breadth of topics to
distribution of BP values obtained were addressed, ensuring that the be addressed in the updated CPG.
in youth. Unfortunately, BPs used literature search was complete Agreement regarding outline content
for developing BP percentiles in and unbiased in identifying was obtained from all subcommittee
the Fourth Report were obtained the most relevant references, members. Some of the originally
from children with both normal ensuring that data were extracted selected topics were ultimately
and unhealthy weight, skewing and analyzed correctly, and that excluded because of lack of sufficient
the mean. In addition, it was also the selected references were evidence, and other topics were
appreciated that at approximately 13 summarized fully and accurately. combined to generate a more concise
years of age, the 90th percentile for The subcommittee also sought to CPG.
BP is ∼120/80 mm Hg. Previously, ensure that the process of KAS
it was possible for youth, entering generation was transparent and
SR Process
adult care at 18 years of age, to based on the available evidence
have a “normal” pediatric BP, but, and that the language used The SR was conducted in accordance
unchanged, an “abnormal” adult to describe a particular with the Preferred Reporting
BP categorization. As a result, the KAS corresponded to the Items for Systemic Reviews and
definition of HTN was revised in recommendation strength, level of Meta-Analysis guidelines.29 The
the 2017 CPG to reflect statistical evidence (LOE), and benefits versus epidemiologist carefully drafted
definitions for HTN in children harms of the published findings.28 4 PICOT questions to guide the
younger than 13 years and to use A process flow map of the steps literature search. These questions
adult cutoff values for youth 13 years taken to generate the CPG can be addressed how the diagnosis of
of age and older. found in Fig 1. systemic HTN should be made in
Downloaded from www.aappublications.org/news by guest on September 4, 2018
4 FROM THE AMERICAN ACADEMY OF PEDIATRICSinfants, children, and adolescents; An ET was created for storage of hypertrophy (LVH) were also not
the recommended clinical and data from references selected for searched via a PICOT format (see
laboratory-based approach for inclusion in the CPG. The following Supplemental Table 5). These topics
identification of potential causes of information was entered for were individually researched, and
systemic HTN (eg, evaluation for each reference in the ET: PICOT expert opinion was used to create
secondary causes); the target BP to number, citation number in the CPG, statements relevant to these topics.
be achieved with treatment; and the original search reference number
impact of BP severity on indirect (identification number within the PICOT 1
markers of CVD in youth. Outcome PICOT 1–4 spreadsheet), author(s), How should systemic HTN (primary
measures, inclusion and exclusion relevant KAS number, relevant CPG HTN, renovascular HTN) be
criteria, and comparison groups were section number, year of publication, diagnosed in neonates, infants, and
predetermined before the initiation journal of publication, full citation, children (0–18 years of age)? How
of the literature search. The primary LOE assignment for the individual should white coat hypertension
literature search was conducted by reference, type of study (eg, (WCH) and masked hypertension
Emilie Ludeman and Kimberly observational, randomized controlled (MH) be diagnosed in children and
Yang. trial [RCT], etc), primary population, adolescents? What is the optimal
reported sample size, subpopulations approach to diagnosing HTN in
A line-by-line description of the of interest, method of BP assessment children and adolescents?
search strategy is presented in (eg, manual, oscillometric, ABPM),
Supplemental Appendix A, including intervention (if applicable), quality PICOT 2
the dates of the primary search of BP measurements (at least 3
for each PICOT. At the time of KAS measurements made during a single What is the recommended workup
generation, between August 2015 and visit), study findings, identified for evaluating children and
July 2016, subcommittee members benefits of the study findings, adolescents with suspected or
conducted additional searches. The potential harms related to the confirmed systemic HTN? How do
epidemiologist was not directly study findings, benefit versus harm we best identify the underlying
involved in these additional literature analysis, and potential limitations of etiologies of secondary HTN in
searches but requested that search the study. children and adolescents, including
criteria, date, and time of each search renal-, endocrine-, environment-,
PICOT Questions Generation medication-, and obesity-related
be stored. All selected citations,
including those identified during the Once the CPG subcommittee causes? When should providers
initial and subsequent searches, were members agreed on the topics suspect a monogenic form of
entered into 4 separate spreadsheets to be covered, 4 PICOT questions systemic HTN among children and
by PICOT (eg, PICOT 1, PICOT 2, PICOT were created (see below). Nearly adolescents?
3, PICOT 4). Originally identified 80% of the topics included in the
PICOT 3
references, selected on the basis of the outline were amenable to a PICOT
SR, were numbered. Added references, search strategy and included in What is the optimal goal SBP and/
selected between August 2015 and the PICOT formatted search (see or DBP for children and adolescents?
July 2016, were labeled not with a Supplemental Tables 1 through 4 What nonpharmacologic and
number but as “added.” All selected for outline topics addressed by the pharmacologic therapies are
references, either chosen on the 4 PICOT questions); 20% were not. available for the treatment of HTN in
basis of title and abstract review or Topics that were not amenable to the children and adolescents?
later chosen on the basis of separate PICOT search format included the
PICOT 4
searches conducted by subcommittee following: strategies for prevention,
members during the KAS generation challenges in the implementation In children and adolescents 1 to 18
phase, were downloaded as a PDF of pediatric hypertension years of age, how does the presence
from the Internet and then uploaded guidelines, economic impact of BP and the severity of systemic HTN
into Mendeley, a commercially management, patient perspective, influence indirect markers of CVD
available reference management parental perspective, evidence gaps, and vascular dysfunction (eg, flow-
software, used for reference storage and proposed future directions. mediated dilation [FMD], cIMT),
and deduplication. Mendeley served Definition of HTN in neonates (0–1 and how does HTN in children
as the subcommittee’s central month), infants (1–12 months of impact long-term risk of HTN into
reference repository for easy access age), children (1–13 years of age), adulthood? Among children and
to selected articles during the article adolescents (13–18 years of age), adolescents with systemic HTN,
review and appraisal process.27 and the definition of left ventricular how does the presence and the
Downloaded from www.aappublications.org/news by guest on September 4, 2018
PEDIATRICS Volume 142, number 3, September 2018 5•• non–English language studies;
•• letters;
•• commentaries; and
•• references related to topics that
were not included in the CPG.
The citation information and any
reasons for study exclusion were
recorded by the methodologist.
Review articles, meta-analyses,
and most SRs were included for
background. Adult studies were
excluded from KAS generation
but may have been included for
background or table content.
Studies that took place outside
of the United States were included
only when US data regarding
the topics were not available
or were limited.
Evidence Review and Selection
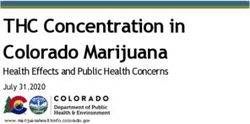
Analysis of Available Evidence,
FIGURE 2 Assignment of LOE, Assignment of
Integrating evidence quality appraisal with anticipated benefits versus harms27: individual references Grade Strength
were graded, benefits versus harms of the findings were assessed, and the aggregate evidence AAP policy stipulates that the
quality was used to generate a strong, moderate, or weak recommendation.
evidence in support of each KAS be
prospectively identified, appraised,
severity of systemic HTN influence •• male and female sex; and summarized and that an explicit
comorbidities such as dyslipidemia, link between the LOE and grade
•• all races and/or ethnicities;
obstructive sleep apnea syndrome of recommendation be defined. A
(OSAS), and cognition? •• RCTs and observational studies summary of the available grades is
(eg, cross-sectional, retrospective described in Fig 2.28
Search Strategy cohort, and prospective cohort);
and Strong Recommendation
The epidemiologist and 2 librarians
created a list of appropriate search •• case series for rare conditions for A strong recommendation is the
terms and strategies (see Appendix which large population studies highest level of recommendation,
A). Search terms included keywords were unavailable. reserved for recommendations
and database-specific terminology supported by evidence with
Exclusion criteria included the
(eg, medical subject headings terms, grade A or B that demonstrates
following:
Emtree). The primary literature review a preponderance of benefit over
for all PICOT questions was limited to •• abstract only; harm. Interventions based on
studies published between 2003 and •• adult-only population (especially level X evidence might also be
2015. PubMed, CENTRAL, and Embase when relevant pediatric studies categorized as “strong” on the
database searches were conducted were available); basis of their risk-benefit profile.
on September 1, 2015, for PICOT 1; A strong recommendation in favor
September 2, 2015, for PICOT 2; •• duplicate studies (in some cases, of a particular action is made
September 15–16, 2015, for PICOT 3; the same data were presented in when the anticipated benefits of
and September 17, 2015 for PICOT 4. another reference, and submitted the recommended intervention
to a different journal); clearly exceed the harms (as a
Inclusion criteria (see Supplemental
•• primary population was non- strong recommendation against an
Table 6) included the following:
United States (unless there were an action is made when the anticipated
•• neonates, infants, children, and insufficient number of US studies harms clearly exceed the benefits)
adolescents; to address the key question); and the quality of the supporting
Downloaded from www.aappublications.org/news by guest on September 4, 2018
6 FROM THE AMERICAN ACADEMY OF PEDIATRICSevidence is excellent. In some clearly recommendations for the 2017 CPG the particular topic. In addition to
identified circumstances, strong is depicted in Fig 2. the creation of KAS writing teams,
recommendations are made when expert work groups were established
high-quality evidence is impossible Evidence Selection Process to address (1) the revision of the
to obtain and the anticipated A 3-step process was used to select HTN definition (members were
benefits strongly outweigh the references for review. The first step Flynn, Kaelber, Giddings, Falkner,
harms. The implication for clinicians included the selection of references and Urbina) and (2) defining LVH
is that they should follow a strong from 3 databases (eg, Medline, (members were Giddings, Urbina, De
recommendation unless a clear CENTRAL, Embase). References Ferranti, and Baker-Smith).30
and compelling rationale for an were deduplicated. Next, by using
alternative approach is present. preestablished written criteria for Building Recommendations in a
article selection for each PICOT, Developer’s Guideline Editor
Moderate Recommendation
references were selected on the
A moderate recommendation is made basis of title and abstract review. The language used for each KAS
when the anticipated benefit exceeds When the 2 reviewers disagreed, was specifically chosen to reflect
the harms but the methodology used the epidemiologist provided the the strength of recommendation by
to generate the evidence is not sound. deciding vote on whether to include a using Building Recommendations
Moderately recommended KASs are particular reference. A third and final in a Developer’s Guideline Editor
to be supported by grade B or grade step involved full reference review. (BRIDGE-Wiz),31 an interactive
C evidence. Level X evidence may clinical software application that
A final search of articles published
also be used to support a moderate has been adopted by the AAP to aid
between August 2015 and July 2016
recommendation depending on CPG authors. This application leads
was completed at the time of KAS
risk-benefit considerations. A guideline writing teams through a
generation to identify any additional
recommendation in favor of a series of questions intended to create
relevant references. Subcommittee
particular action is made when the clear, transparent, and actionable
teams also had the option of
anticipated benefit exceeds the KASs. BRIDGE-Wiz incorporates
incorporating additional background
harm but the quality of evidence LOE and benefit-harm assessment
references into the text preceding
is not as strong. In some clearly into a final determination of each
each KAS. Additional references
identified circumstances, moderate recommendation strength. BRIDGE-
were selected on the basis of expert
recommendations are made when Wiz provides safeguard against
opinion and familiarity with the
high-quality evidence is impossible creating vague and/or underspecified
literature. Background references
to obtain but the anticipated benefits recommendations. This software
selected for inclusion in the final
outweigh the harms. The implication was used to generate KASs during an
document were also achieved in the
for clinicians is that they should be in-person meeting held at the AAP
ET.
prudent when following a moderate headquarters on March 21, 2016.
recommendation but should remain Generation of KASs BRIDGE-Wiz was also used to help
alert to new information and generate the text for KASs generated
KASs were actionable statements, after the March 21, 2016, meeting.
sensitive to patient preferences.
drafted on the basis of the assembled
Weak Recommendation and No evidence, intended to guide clinical Generation of Recommended KAS
Recommendation practice. Writing teams consisting of After considering the available LOE
When published evidence is 2 or more subcommittee members and recommendation grades, the
lacking, and/or when the limited were established to generate KASs subcommittee formulated 30 KASs.32
evidence available demonstrates for each selected topic. The clinical Each KAS included the following:
an equivocal risk-benefit profile, no expertise of subcommittee members
was used during the KAS generation •• an aggregate evidence quality
recommended key action is offered.
phase. Subcommittee members with score;
No recommendation indicates that
there is a lack of pertinent published expertise in the topic were selected •• a list of the potential benefit(s) of
evidence and that the anticipated to either review the references the proposed KAS;
balance of benefits and harms is relevant to a particular topic or serve •• a description of the risks, harms,
presently unclear. The implication as primary author(s) of the KAS and costs of the proposed KAS;
for clinicians is that they should be relevant to their clinical expertise. In
alert to new published evidence other cases, authors for the KAS were •• a benefit-harm assessment;
that clarify the balance of benefit selected on the basis of previous •• a description of any intentional
versus harm. The classification of involvement in article selection for vagueness;
Downloaded from www.aappublications.org/news by guest on September 4, 2018
PEDIATRICS Volume 142, number 3, September 2018 7•• a description of the role of patient for BP are based on auscultatory BP diagnosing HTN among youth.
preference; measurements for normal-weight Challenges associated with use
•• any exclusions; children. Unchanged from the Fourth of a complex table may lead to
Report, defining abnormal BP in lack of recognition.44 However,
•• an assessment of the strength of youth 1 tohypertensive emergency and require lifestyle modifications can have a Heart Study, and the Muscatine
more immediate management and significant and positive impact on BP Study, the strength of association
intervention.52 management.57 Furthermore, since between the presence of childhood
the enactment of the 1997 Food and risk factors for premature CVD and
PICOT 3 Drug Administration Modernization the presence of cIMT is dependent on
What is the optimal goal SBP and/ Act and passage of the Best Drugs for age of onset of elevation in SBP in 6-
or DBP for children and adolescents? Children Act,58 the path for assessing to 18-year-olds, whereas elevations
What nonpharmacologic and the pharmacokinetics, dose-effect, in DBP were not associated with
pharmacologic therapies are and safety of antihypertensive abnormal cIMT.5
available for the treatment of HBP in therapy in children has been
children and adolescents? cleared. The goals of PICOT 3 and General Results From Full Search
its associated KASs were to both A total of 14 763 references were
The optimal goal SBP and DBP for identify effective therapies (eg, selected after the initial PICOT
children and adolescents remain lifestyle, noninvasive therapies, and search. After deduplication, 14 382
unknown. However, data from a antihypertensive therapies) and to references were available for title
recent survey study indicate that evaluate response to therapy. and abstract review. The 2-person
compared with normotension,
abstract and title review resulted
elevated BP can be associated PICOT 4
in a total of 1379 references for full
with the development of TOD in
In children and adolescents 1 to 90th percentile) and TOD in
and vascular dysfunction (eg, FMD, were selected for inclusion during
youth.7 Thus, the CPG recommends
cIMT), and how does HTN in children the expanded search.
a target BP ofetiologies of secondary hypertension review led to the selection of 631 and vascular dysfunction (eg, FMD,
in the pediatric population? references for full reference review cIMT), and how does hypertension
The literature search for PICOT 2 was and data extraction. A total of 59 in children impact long-term risk of
focused on the diagnostic approach references were initially selected for hypertension into adulthood?
for identifying renal, renovascular, inclusion in KAS generation. Some
A total of 3857 references were
cardiac, endocrine (including of the references were excluded
selected after a deduplication
pheochromocytoma), medication- because the topics covered were
process was conducted in Mendeley.
related, and genetic causes of HTN. beyond the scope of the CPG (eg,
Abstract and title review led to the
A total of 1567 references were RCTs of the use of dark chocolate,
selection of 3744 references for
selected on the basis of initial cocoa, beetroot juice, dietary fiber,
full review and data extraction. In
search terms (see Supplemental dietary protein, diet rich in fish,
total, 219 references were selected
Table 7). After the deduplication or garlic to treat hypertension in
for full review (see Supplemental
process, a total of 1565 references children),59– 66
(see Supplemental
Table 7), and 196 were excluded for
were selected. Abstract and title Table 12 for the excluded PICOT 3
the following reasons: 1 abstract
review led to the exclusion of 196 references), and other references
only, 10 non-English language and/
references after full reference review. were excluded because they
or non-US population, 110 adult-
See Supplemental Table 10 for the pertained to a particular subset
only population, and 98 for other
excluded PICOT 2 references. of children with hypertension
reasons (eg, review article, duplicate
(eg, pharmacologic management
Of a total of 225 references selected, reference, etc; see Supplemental
of hypertension in children with
86 references (see Supplemental Table 14).
CKD).67,68 There were many trials in
Table 11), 9 were selected for KAS which combination therapy in the After the updated search, a total
generation. Seventy-two additional adult population was addressed. of 23 references were selected for
references that were added during Such topics were not explored in the inclusion in PICOT 4. The majority
the search conducted between CPG,69– 74
and such references were of selected references were cross-
August 2015 and July 2016 were ultimately excluded. Some references sectional studies or retrospective
also used to generate KASs related to considered to be duplicates (eg, cohort studies.
PICOT 2. reports of the pediatric candesartan
Of the selected references used to trial) were excluded.75,76 In total,
SPECIAL ADDITIONS TO THE CPG
generate PICOT 2–related KASs, 4 587 references were excluded (see
were LOE B and 24 were LOE C. Supplemental Table 12). Creation of New BP Tables
Eight background references were
After the updated search and KAS The subcommittee engaged Bernard
selected at the discretion of the KAS
generation, 45 additional references Rosner, PhD, the statistician
authors.
were selected for inclusion for a total previously consulted by the NHLBI
Primary Literature Search, PICOT 3 of 60 references (see Supplemental on past pediatric BP guidelines, to
Table 13). The majority of selected generate new normative BP tables on
The primary questions used to
references were cross-sectional the basis of values obtained only in
conduct the literature search for
studies. A total of 60 primary children with normal BMI. The goal
PICOT 3 were as follows: What
references were used to generate was to eliminate the effects of obesity
is the optimal goal SBP and/or
KASs for PICOT 3: 10 were LOE A, on the normative values, which
DBP for children and adolescents?
11 were LOE B, 31 were LOE C, and was a criticism of the normative
What nonpharmacologic and
none were LOE D/EO. In addition, BP tables published in the Fourth
pharmacologic therapies are
5 background references and 3 SRs Report. Methods used to generate
available for the treatment of HBP in
were selected for inclusion and KAS these tables have previously been
children?
generation. published.25
A total of 6958 references were Data included in this updated
Primary Literature Search, PICOT 4
selected on the basis of initial search analysis were already presented in
terms (see Supplemental Table 7). The primary question used to the National High Blood Pressure
A minimum therapeutic follow-up conduct the literature search for Education Program NHLBI database
period of 3 months was required PICOT 4 was as follows: In children and consisted of 11 pediatric BP
for inclusion of a study. After a and adolescents 0 to 18 years of studies conducted between 1976 and
deduplication process conducted in age, how does the presence and the 2000.77–86
For the new normative BP
Mendeley, a total of 6710 references severity of systemic hypertension table, only subjects with BMIDisease Control and Prevention age- both specification of the regression that may need further evaluation
and sex-specific BMI growth charts function for a specific quantile and either by the nurse himself or herself
were used. Separate sex-specific allowance for separate regression or by the clinician. For adolescents
analyses were performed for SBP and equations for different quantiles. ≥13 years of age, a threshold of
DBP. Of note, the heights used in the 120/80 mm Hg was used in the
Complete tables for the 90th
new tables are those for children of simplified table regardless of sex
percentile are available in Table
x years, 6 months, and therefore may to align with adult guidelines for
4 of Rosner et al,87 along with
differ from height values found in detection of elevated BP.90
the regression equations used to
standard growth charts.
generate each of the quantiles(s)
To remove study effects, a restricted in the restricted cubic spline in New Definition of LVH
cubic spline linear regression addition to a macro that ran 99
model was run of BP on study quantile regressions for s = 0.01, Echocardiography is used to assess
age, height z score, and weight z 0.99 (0.01) and estimated the closest the presence of left ventricular target
score, represented as 10 dummy quantile that agrees with a child’s organ injury related to hypertension
variables. Height and height z scores given BP, age, sex, and height. These in children.1 The basis for this
corresponding to height at age x percentiles, both in tabular form assessment is (1) the relationship of
years+ 6 months and not the CDC for assessment of BP of individual LVM to BP,91 (2) the independent and
height percentiles, were used. The children and in a SAS macro for strong relationship of LVH to adverse
study effects from the regression assessment of BP percentiles in batch CVD outcomes in adults,92–94
and (3)
model were used to compute mode for larger numbers of children, the fact that a significant percentage
“adjusted BP” (eg, BP_adj), which are available online.88 of children and adolescents with
was the BP that would be obtained hypertension demonstrate a degree
Information regarding how to
if a subject came from an average of LVH associated with adverse
incorporate 2017 CPG BP definitions
study. A second restricted cubic outcomes in adults.95– 97
into the EHR can be found in
spline regression was then run of the
Supplemental Appendix B.87
adjusted BP on age, height, and age × The left ventricle (LV) structure in
height, with knots at the fifth, 27.5th, the CPG is stratified into 4 groups
50th, 75th, and 95th percentiles and Simplified BP Table on the basis of LVM (normal or
residuals that were assumed to be hypertrophied) and relative LV wall
The CPG also includes a new,
normally distributed. thickness (normal or increased). The
simplified table for initial BP
screening based on the 90th 4 stratified groups proposed for LVM
A cubic spline was used because it include (1) normal geometry with
is considered to be more flexible percentile BP for age and sex for
children at the fifth percentile for normal LVM and normal relative
than a single ordinary polynomial wall thickness (RWT), (2) concentric
regression over the entire age and/ height. This gives the BP values in the
simplified table a negative predictive geometry with normal LVM and
or height z score. The cubic spline increased RWT, (3) eccentric LVH
is a concatenation of separate value of more than 99%.89 The
simplified table was designed for use with increased LVM and normal
cubic polynomials with smooth RWT, and (4) concentric LVH with
intersections at the knots. The only as a screening tool to identify
children and adolescents who need both increased LVM and increased
restricted cubic spline model RWT98,99
(see Supplemental
assumes normal residuals, which further BP evaluation.
Table 15).
implies that the effects of age and It is not intended that one will use the
height are the same for all quantiles simplified table to diagnose elevated Because the heart increases in size in
of BP. To relax this assumption, BP or hypertension but rather to relation to body size, indexing LVM is
quantile regression methods were determine when a BP measurement required.100
used. With quantile regression, mean should be repeated. To diagnose For the 2017 CPG, the following
BP was modeled by using restricted elevated BP or hypertension, it is definitions for LV target organ
cubic spline. However, a separate important to use the actual BP values injury were chosen regarding
set of regression coefficients was in the complete BP tables because hypertrophy, RWT, and ejection
obtained for each quantile (s = 0.01, these may be as much as 9 mm Hg fraction (EF). These definitions
0.05, 0.10, 0.25, 0.50, 0.75, 0.90, 0.95, higher than those in the simplified are based on published guidelines
and 0.99). The quantile regression table, depending on the child’s age from the American Society of
approach, using separate restricted and length or height. A typical use Echocardiography and associations
cubic splines for each quantile, case for this simplified table is for of thresholds for indexed LVM with
offers the most flexibility in terms of nursing staff to quickly identify BP adverse outcomes in adults92,93,
98,
100
:
Downloaded from www.aappublications.org/news by guest on September 4, 2018
PEDIATRICS Volume 142, number 3, September 2018 11•• LVH is defined as left ventricular ACKNOWLEDGMENTS Aaron Carroll, MD, MS, FAAP, Partnership for
mass, indexed >51 g/m2.7 or LVM Policy Implementation
We thank Kimberly Yang, Emilie Stephen R. Daniels, MD, PhD, FAAP, Committee on
>115 g/body surface area (BSA) Ludeman, and Bernard Rosner, PhD. Nutrition
for boys and LVM >95 g/BSA for Sarah D. de Ferranti, MD, MPH, FAAP, Committee
girls. (Note that the values for LVH on Cardiology & Cardiac Surgery
LEAD AUTHORS
are well above the 95th percentile Michael G. Leu, MD, MS, MHS, FAAP, Council on
Carissa M. Baker-Smith, MD, MS, MPH, FAAP, FAHA Quality Improvement and Patient Safety
for distributions of LVM in children
Susan K. Flinn, MA Makia Powers, MD, MPH, FAAP, Committee on
and adolescents.98 The clinical Joseph T. Flynn, MD, MS, FAAP Adolescence
significance of values between the David C. Kaelber, MD, PhD, MPH, FAAP, FACP, FACMI Corinna Rea, MD, MPH, FAAP, Section on Early
95th percentile of a population- Douglas Blowey, MD Career Physicians
based distribution and these Aaron E. Carroll, MD, MS, FAAP Joshua Samuels, MD, MPH, FAAP, Section on
thresholds is uncertain.101) Stephen R. Daniels, MD, PhD, FAAP Nephrology
Sarah D. de Ferranti, MD, MPH, FAAP Madeline Simasek, MD, FAAP, Quality Improvement
•• An LV RWT >0.42 indicates Janis M. Dionne, MD, FRCPC Innovation Networks
concentric geometry. LV wall Bonita Falkner, MD Vidhu Thaker, MD, FAAP, Section on Obesity
thickness >1.4 cm is abnormal.102 Samuel S. Gidding, MD Elaine Urbina, MD, FAAP, American Heart
Celeste Goodwin Association, Atherosclerosis, Hypertension, &
•• Decreased LV EF is a valueResidency, University of Pittsburgh Medical Center, Children’s Hospital of Pittsburgh and School of Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania; sDivision of Molecular
Genetics, Department of Pediatrics, Columbia University Irving Medical Center, Columbia University, New York, New York; tBroad Institute, Cambridge, Massachusetts; and uPreventive
Cardiology, Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio
This document is copyrighted and is property of the American Academy of Pediatrics and its Board of Directors. All authors have filed conflict of interest statements with the American
Academy of Pediatrics. Any conflicts have been resolved through a process approved by the Board of Directors. The American Academy of Pediatrics has neither solicited nor accepted
any commercial involvement in the development of the content of this publication.
The guidance in this report does not indicate an exclusive course of treatment or serve as a standard of medical care. Variations, taking into account individual circumstances, may be
appropriate.
All technical reports from the American Academy of Pediatrics automatically expire 5 years after publication unless reaffirmed, revised, or retired at or before that time.
DOI: https://doi.org/10.1542/peds.2018-2096
Address correspondence to Carissa M. Baker-Smith. Email: cbaker-smith@som.umaryland.edu
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2018 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. National High Blood Pressure Determinants of Adult Health Study, 11. Bao W, Threefoot SA, Srinivasan SR,
Education Program Working Group on the Bogalusa Heart Study, and the Berenson GS. Essential hypertension
High Blood Pressure in Children and Muscatine Study for the International predicted by tracking of elevated blood
Adolescents. The fourth report on the Childhood Cardiovascular Cohort pressure from childhood to adulthood:
diagnosis, evaluation, and treatment (i3C) Consortium. Circulation. the Bogalusa Heart Study. Am J
of high blood pressure in children and 2010;122(24):2514–2520 Hypertens. 1995;8(7):657–665
adolescents. Pediatrics. 2004;114(2
6. Shen W, Zhang T, Li S, et al. Race and 12. Theodore RF, Broadbent J, Nagin
suppl 4th report):555–576
sex differences of long-term blood D, et al. Childhood to Early-Midlife
2. American Academy of Pediatrics pressure profiles from childhood and Systolic Blood Pressure Trajectories:
Steering Committee on Quality adult hypertension: the Bogalusa Heart Early-Life Predictors, Effect Modifiers,
Improvement and Management. Study. Hypertension. 2017;70(1):66–74 and Adult Cardiovascular Outcomes.
Classifying recommendations for Hypertension. 2015;66(6):1108–1115
7. Urbina EM, Khoury PR, McCoy C, Daniels
clinical practice guidelines. Pediatrics.
SR, Kimball TR, Dolan LM. Cardiac 13. Chen X, Wang Y. Tracking of blood
2004;114(3):874–877
and vascular consequences of pre- pressure from childhood to adulthood:
3. Benjamin EJ, Blaha MJ, Chiuve SE, et al; hypertension in youth. J Clin Hypertens a systematic review and meta-
American Heart Association Statistics (Greenwich). 2011;13(5):332–342 regression analysis. Circulation.
Committee and Stroke Statistics
8. Garanty-Bogacka B, Syrenicz M, 2008;117(25):3171–3180
Subcommittee. Heart disease and
stroke statistics-2017 update: a report Syrenicz A, Gebala A, Lulka D, Walczak 14. Theodore RF, Broadbent J, Nagin
from the American Heart Association M. Serum markers of inflammation D, et al. Childhood to early-midlife
[published correction appears and endothelial activation in systolic blood pressure trajectories:
in Circulation. 2017;135(10):e646; children with obesity-related early-life predictors, effect modifiers,
Circulation. 2017;136(10):e196]. hypertension. Neuroendocrinol Lett. and adult cardiovascular outcomes.
Circulation. 2017;135(10):e146–e603 2005;26(3):242–246 Hypertension. 2015;66(6):1108–1115
4. Sun SS, Grave GD, Siervogel RM, 9. Lubrano R, Travasso E, Raggi C,
15. Chobanian AV, Bakris GL, Black HR,
Pickoff AA, Arslanian SS, Daniels SR. Guido G, Masciangelo R, Elli M. Blood
et al; Joint National Committee on
Systolic blood pressure in childhood pressure load, proteinuria and renal
Prevention, Detection, Evaluation, and
predicts hypertension and metabolic function in pre-hypertensive children.
Treatment of High Blood Pressure;
syndrome later in life. Pediatrics. Pediatr Nephrol. 2009;24(4):823–831
National Heart, Lung, and Blood
2007;119(2):237–246 10. Adams HR, Szilagyi PG, Gebhardt L, Institute; National High Blood Pressure
5. Juonala M, Magnussen CG, Venn A, Lande MB. Learning and attention Education Program Coordinating
et al. Influence of age on associations problems among children with Committee. Seventh report of the Joint
between childhood risk factors and pediatric primary hypertension. National Committee on Prevention,
carotid intima-media thickness in Pediatrics. 2010;126(6). Available at: Detection, Evaluation, and Treatment
adulthood: the Cardiovascular Risk www.pediatrics.org/cgi/content/full/ of High Blood Pressure. Hypertension.
in Young Finns Study, the Childhood 126/6/e1425 2003;42(6):1206–1252
Downloaded from www.aappublications.org/news by guest on September 4, 2018
PEDIATRICS Volume 142, number 3, September 2018 1316. Hansen ML, Gunn PW, Kaelber DC. monitoring: indications and 2017;140(6):e20173035]. Pediatrics.
Underdiagnosis of hypertension in interpretations. J Clin Hypertens 2017;140(3):e20171904
children and adolescents. JAMA. (Greenwich). 2012;14(6):372–382 37. Ostchega Y, Prineas RJ, Nwankwo
2007;298(8):874–879 27. Mendeley [computer program]. New T, Zipf G. Assessing blood
17. Kaelber DC, Liu W, Ross M, et al; York, NY: Elsevier; 2008 pressure accuracy of an aneroid
Comparative Effectiveness Research sphygmomanometer in a national
28. American Academy of Pediatrics
Through Collaborative Electronic survey environment. Am J Hypertens.
Steering Committee on Quality
Reporting (CER2) Consortium. 2011;24(3):322–327
Improvement and Management.
Diagnosis and medication treatment Classifying recommendations for 38. Podoll A, Grenier M, Croix B, Feig DI.
of pediatric hypertension: a clinical practice guidelines. Pediatrics. Inaccuracy in pediatric outpatient
retrospective cohort study. Pediatrics. 2004;114(3):874–877 blood pressure measurement.
2016;138(6):e20162195 Pediatrics. 2007;119(3). Available at:
29. Preferred reporting items for
18. Din-Dzietham R, Liu Y, Bielo MV, www.pediatrics.org/cgi/content/full/
systematic reviews and meta-analyses
Shamsa F. High blood pressure trends 119/3/e538
(PRISMA) web site. Available at: www.
in children and adolescents in national prisma-statement.org/. Accessed April 39. Mourad A, Carney S. Arm position and
surveys, 1963 to 2002. Circulation. 24, 2018 blood pressure: an audit. Intern Med J.
2007;116(13):1488–1496 2004;34(5):290–291
30. Flynn JT, Kaelber DC, Baker-Smith
19. Skinner AC, Perrin EM, Moss LA, CM; Subcommittee on Screening 40. Flynn JT, Pierce CB, Miller ER III, et al;
Skelton JA. Cardiometabolic risks and Management of High Blood Chronic Kidney Disease in Children
and severity of obesity in children Pressure in Children, et al. Clinical Study Group. Reliability of resting
and young adults. N Engl J Med. practice guideline for screening and blood pressure measurement and
2015;373(14):1307–1317 management of high blood pressure in classification using an oscillometric
20. Graf C, Rost SV, Koch B, et al. Data from children and adolescents [published device in children with chronic kidney
the StEP TWO programme showing the correction appears in Pediatrics. disease. J Pediatr. 2012;160(3):434–
effect on blood pressure and different 2017;140(6):e20173035]. Pediatrics. 440.e1
parameters for obesity in overweight 2017;140(3):e20171904 41. Daley MF, Sinaiko AR, Reifler LM, et al.
and obese primary school children. 31. BRIDGE-Wiz. Available versions of Patterns of care and persistence after
Cardiol Young. 2005;15(3):291–298 BridgeWiz. Available at: http://gem. incident elevated blood pressure.
21. Falkner B. Recent clinical and med.yale.edu/BRIDGE-Wiz/ . Accessed Pediatrics. 2013;132(2). Available at:
translational advances in pediatric April 24, 2018 www.pediatrics.org/cgi/content/full/
hypertension. Hypertension. 132/2/e349
32. BRIDGE-Wiz. Available versions of
2015;65(5):926–931 BridgeWiz. Available at: http://gem. 42. Becton LJ, Egan BM, Hailpern
22. Flynn JT, Mitsnefes M, Pierce C, med.yale.edu/BRIDGE-Wiz/. Accessed SM, Shatat IF. Blood pressure
et al; Chronic Kidney Disease in April 24, 2018 reclassification in adolescents based
Children Study Group. Blood pressure on repeat clinic blood pressure
33. Picone DS, Schultz MG, Otahal P, et al.
in children with chronic kidney measurements. J Clin Hypertens
Accuracy of cuff-measured blood
disease: a report from the Chronic (Greenwich). 2013;15(10):717–722
pressure: systematic reviews and
Kidney Disease in Children study. meta-analyses. J Am Coll Cardiol. 43. Chiolero A, Cachat F, Burnier M,
Hypertension. 2008;52(4):631–637 2017;70(5):572–586 Paccaud F, Bovet P. Prevalence of
23. Samuels J, Ng D, Flynn JT, et al; hypertension in schoolchildren
34. Kent AL, Chaudhari T. Determinants
Chronic Kidney Disease in Children based on repeated measurements
of neonatal blood pressure. Curr
Study Group. Ambulatory blood and association with overweight.
Hypertens Rep. 2013;15(5):426–432
pressure patterns in children with J Hypertens. 2007;25(11):2209–2217
chronic kidney disease. Hypertension. 35. Dionne JM, Abitbol CL, Flynn JT.
44. Bijlsma MW, Blufpand HN, Kaspers GJ,
2012;60(1):43–50 Hypertension in infancy: diagnosis,
Bökenkamp A. Why pediatricians fail to
management and outcome [published
24. Shatat IF, Flynn JT. Hypertension diagnose hypertension: a multicenter
correction appears in Pediatr Nephrol.
in children with chronic kidney survey. J Pediatr. 2014;164(1):173–177.
2012;27(1):159–160]. Pediatr Nephrol.
disease. Adv Chronic Kidney Dis. e7
2012;27(1):17–32
2005;12(4):378–384 45. Chaudhry B, Wang J, Wu S, et al.
36. Flynn JT, Kaelber DC, Baker-Smith CM,
25. Rosner B, Cook N, Portman R, Daniels Systematic review: impact of health
et al; Subcommittee on Screening
S, Falkner B. Determination of blood information technology on quality,
and Management of High Blood
pressure percentiles in normal-weight efficiency, and costs of medical care.
Pressure in Children. Clinical
children: some methodological issues. Ann Intern Med. 2006;144(10):742–752
practice guideline for screening and
Am J Epidemiol. 2008;167(6):653–666 46. Shojania KG, Jennings A, Mayhew A,
management of high blood pressure in
26. Flynn JT, Urbina EM. Pediatric children and adolescents [published Ramsay CR, Eccles MP, Grimshaw J.
ambulatory blood pressure correction appears in Pediatrics. The effects of on-screen, point of care
Downloaded from www.aappublications.org/news by guest on September 4, 2018
14 FROM THE AMERICAN ACADEMY OF PEDIATRICSYou can also read