ZN-c3 WEE1 Data Review KOL Event - April 12, 2021 - Zentalis ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ZN-c3 WEE1 Data Review KOL Event
April 12, 2021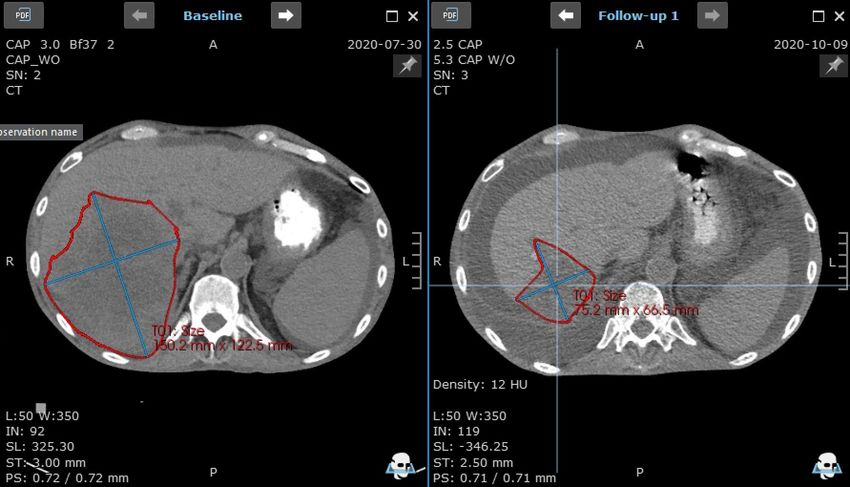
Forward-Looking Statements and Disclaimer Zentalis Pharmaceuticals, Inc. (“we,” “us,” “our,” “Zentalis” or the “Company”) cautions that this presentation (including oral commentary that accompanies this presentation) contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. All statements contained in this presentation that do not relate to matters of historical fact should be considered forward-looking statements, including without limitation statements regarding our future financial or business performance, plans, prospects, trends or strategies, objectives of management, competition and other financial and business matters, the potential, safety, efficacy, and regulatory and clinical progress of our current and prospective product candidates, plans and timing for the initiation of and release of data from our clinical trials and our ability to meet other key milestones, planned preclinical activities, our current and prospective collaborations, the estimated size of the market for our product candidates, and the timing and success of our development and commercialization of our anticipated product candidates and the market acceptance thereof are forward-looking statements, as well as statements that include the words “expect,” “intend,” “plan,” “believe,” “project,” “forecast,” “estimate,” “may,” “should,” “anticipate” and similar statements of a future or forward-looking nature. These statements are neither promises nor guarantees, but involve known and unknown risks, uncertainties and other important factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements, including, but not limited to, the following: the outbreak of the novel coronavirus disease, COVID-19, has adversely impacted and may continue to adversely impact our business, including our preclinical studies and clinical trials; our limited operating history, which may make it difficult to evaluate our current business and predict our future success and viability; we have and expect to continue to incur significant losses; our need for additional funding, which may not be available; our substantial dependence on the success of our lead product candidate; failure to identify additional product candidates and develop or commercialize marketable products; the early stage of our development efforts; potential unforeseen events during clinical trials could cause delays or other adverse consequences; risks relating to the regulatory approval process or ongoing regulatory obligations; failure to obtain U.S. or international marketing approval; our product candidates may cause serious adverse side effects; interim, initial, “topline”, and preliminary data from our clinical trials that we announce or publish from time to time may change as more patient data become available and are subject to audit and verification procedures that could result in material changes in the final data; inability to maintain our collaborations, or the failure of these collaborations; our reliance on third parties; effects of significant competition; the possibility of system failures or security breaches; risks relating to intellectual property; our ability to attract, retain and motivate qualified personnel; and significant costs as a result of operating as a public company. These and other important factors discussed under the caption “Risk Factors” in our Annual Report on Form 10-K for the year ended December 31, 2020 filed with the U.S. Securities and Exchange Commission (SEC) and our other filings with the SEC could cause actual results to differ materially from those indicated by the forward-looking statements made in this presentation. Any such forward-looking statements represent management’s estimates as of the date of this presentation. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. While we may elect to update these forward-looking statements at some point in the future, we assume no obligation to update or revise any forward-looking statements except to the extent required by applicable law. Although we believe the expectations reflected in such forward-looking statements are reasonable, we can give no assurance that such expectations will prove to be correct. Accordingly, readers are cautioned not to place undue reliance on these forward-looking statements. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements. This presentation also contains estimates and other statistical data made by independent parties and by us relating to market size and other data about our industry. This data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such data and estimates. In addition, projections, assumptions and estimates of our future performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk. Neither we nor our affiliates, advisors or representatives makes any representation as to the accuracy or completeness of that data or undertake to update such data after the date of this presentation. Data of Fulvestrant, RAD1901, Abemaciclib, Alpelisib, AZD1775, Venetoclax and Osimertinib presented in this presentation is based on evaluation of comparable proxy chemical compounds purchased from commercial sources rather than the pharmaceutical company commercializing or developing, as applicable, the compound. 2
Broad Oncology Pipeline Designed to Improve Patient Outcomes
IND Enabling Phase 1/2 Phase 3 Collaborator (1)
ZN-c5: Oral SERD
Monotherapy
Breast Cancer
Combinations
ZN-c3: WEE1 Inhibitor
Monotherapy
Solid Tumors
Combinations
ZN-d5: BCL-2 Inhibitor
AML or Non-Hodgkin’s
Lymphoma Monotherapy
Breast Cancer Combination with ZN-c5
ZN-e4: EGFR
NSCLC
(1) Zentalis is currently evaluating ZN-c5 in combination with palbociclib (Ibrance®), as part of a clinical research collaboration with Pfizer, evaluating ZN-c5 in combination with abemaciclib (Verzenio®), as part of a clinical research
collaboration with Lilly. Zentalis intends to evaluate ZN-c3 in combination with niraparib (ZEJULA®), as part of a clinical research collaboration with GlaxoSmithKline. Zentalis maintains full ownership of ZN-c5 and ZN-c3 in each
such collaboration. SciClone has development and commercial rights to ZN-e4 in Greater China (including Macau and Hong Kong), South Korea, Taiwan and Vietnam. Zentera, our majority-owned joint venture, has development
3 and commercial rights to ZN-c5, ZN-c3 and ZN-d5 in select Asian countries (including China). Zentera submitted INDs in China for each of ZN-c5 and ZN-c3 and intends to submit an IND in China ZN-d5 in 2021.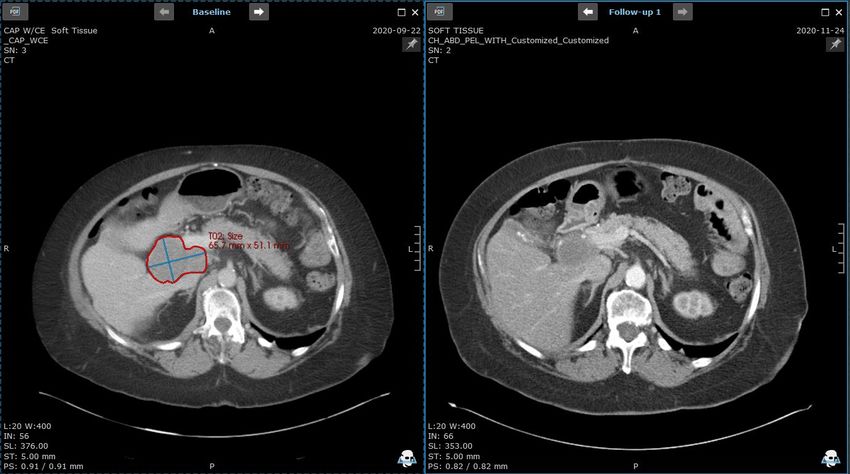
ZN-c3: WEE1 Inhibitor 4
ZN-c3: A DNA Damage Response (DDR) Drug Candidate
ZN-c3
• WEE1 is a protein kinase expressed at high levels in many cancer types that prevents entry into mitosis in response to
DNA damage by regulating the G2 checkpoint
• WEE1 inhibition causes cancer cells to proceed to mitosis without repairing DNA damage, resulting in premature
mitotic entry and apoptosis
• ZN-c3 has demonstrated significant growth inhibition and induced apoptosis in vitro and anti-tumor activity in vivo
5 Source: Drawing based on Targeting WEE1 Kinase in Cancer. Matheson CJ, et al. Trends Pharmacol Sci. 2016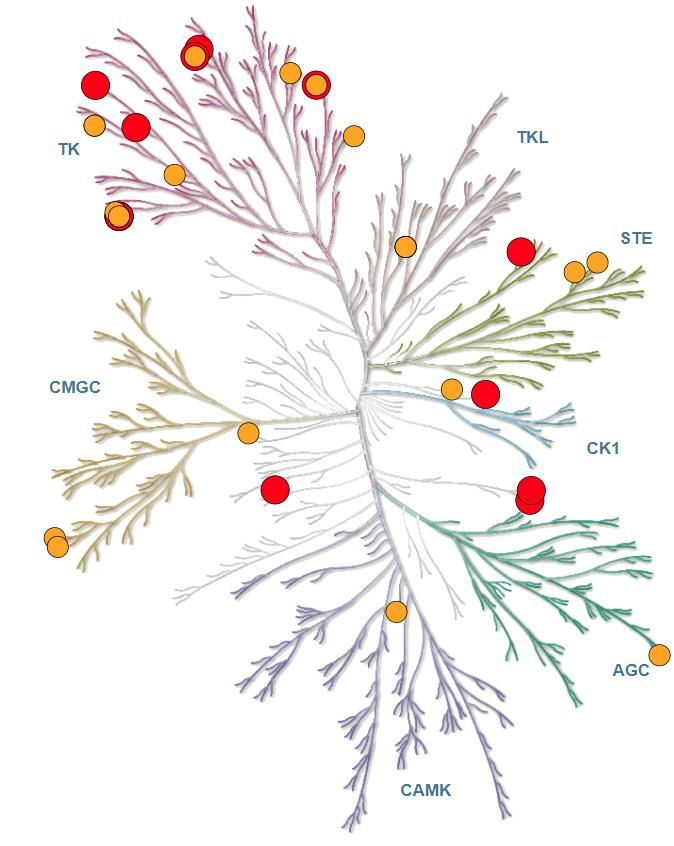
WEE1 Inhibitors Show Strong Preclinical Activity and Clinical Responses
Combination of WEE1 and PARP Phase II Study of WEE1 Inhibitor Plus Phase II Trial of WEE1 Inhibitor in
Inhibitors Showed Improved Anti- Gemcitabine for Platinum-Refractory Recurrent recurrent Uterine Serous
Tumor Activity Compared to the Use of Ovarian Cancer: Double-Blind, Randomized, Carcinoma (USC) (3,4)
Each as Monotherapy (1) Placebo-Controlled(2)
AZD1775
AZD1775
AZD1775
AZD1775
(1) Fang, Y. Cancer Cell (2019). A total of 2 x 106 OVCAR8 ovarian cancer cells were injected subcutaneously (s.c.) and grown for 2 weeks in nude mice. Mice were randomized with six in
each group and treated as indicated. Average tumor volume ± SEM are displayed. p value: one-way ANOVA. **p < 0.01
(2) Lheureux S., Lancet (2021). Addition of a WEE1 to Gemcitabine shows a statistically significant improvement in mOS over Gemcitabine with placebo (HR=0.56, P=0.017)
(3) Liu, J.F. AZD1775 SGO Presentation (2020)
6 (4) An aggressive subtype of endometrial carcinoma characterized by frequent TP53 mutations (>90%)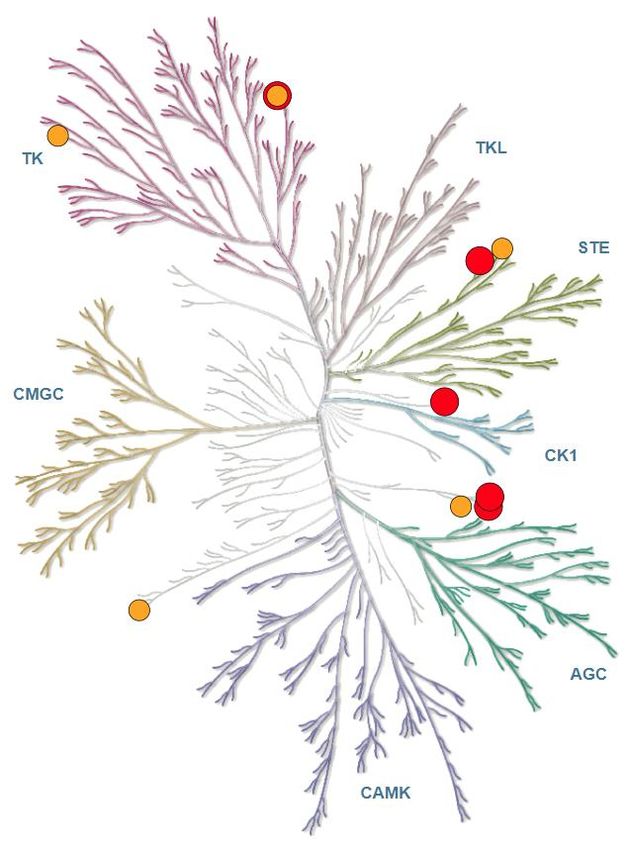
ZN-c3: Excellent Potency, PK and Preclinical Activity
ZN-c3 Anti-Proliferative Activity in a Panel of Cell Lines
Compound CTG IC50(nM)
ID
NSCLC SCLC TNBC Ovarian cancer cells ZN-c3 Induced Prolonged Tumor Growth Delay
NCI-H23 A-427 DMS-53 NCI- MDA- HCC OVCAR3 UWB A427 Human NSCLC Tumor Xenograft Model
H1048 MB-231 1806 1.289
ZN-c3 124 88 118 92 190 95 69 54
AZD1775
AZD1775(1) 108 94 130 97 233 94 124 57
Improved Tumor Concentration in Preclinical Models
Study
ZN-c3 AZD1775 (1)
(A-427 NSCLC)
Dose
20 40 80 20 40 80
(mg/kg/day)
Cmax (ng/mL) 1,167 1,997 5,100 635 2,460 4,703
ZN-c3
Tmax (hr) 1 1 1 1 1 1
AUC0-24hr (ng.hr/mL) 4,863 17,088 39,722 1,494 6,313 13,408
Tumor Conc. (ng/mL) 10.5 48.0 811 BQL(2) BQL 6.95
(1) AZD1775 data based on evaluation of comparable proxy chemical compound purchased from commercial sources
rather than obtained from the pharmaceutical company developing the compound.
(2) BQL: Below Quantifiable Level
7 Note: ZN-c3 has excellent thermodynamic solubility of 2132 µM (vs. 60 µM for AZD1775) based on internal data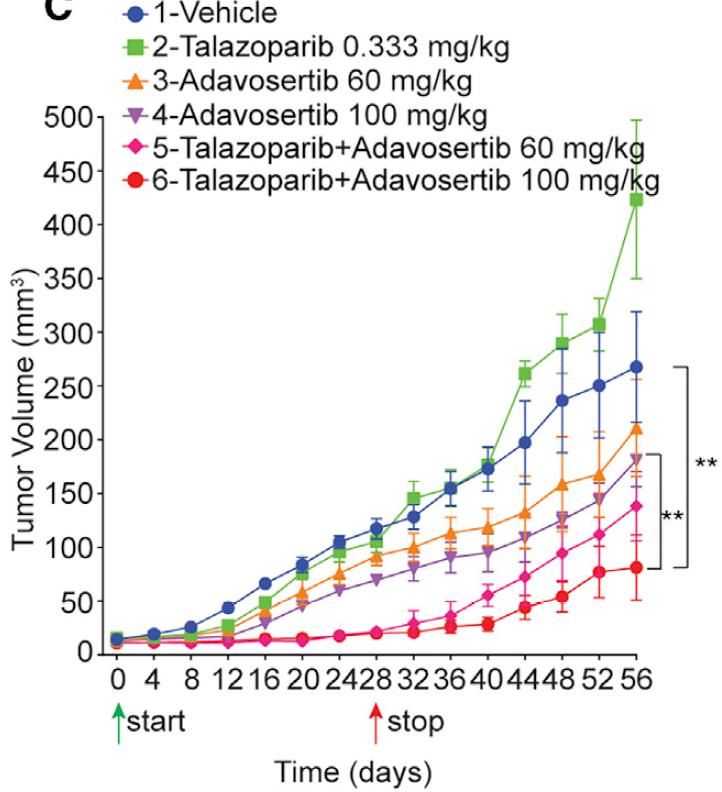
ZN-c3: Differentiated Selectivity Profile in >470 Kinase Screening Panel
AZD1775 (1) ZN-c3
% Inhibition (@ 1µM) % Inhibition (@ 1µM)
90+ 13 kinases 90+ 5 kinases
75-89 24 kinases 75-89 5 kinases
(1) AZD1775 data based on evaluation of comparable proxy chemical compound purchased from commercial sources rather than obtained from the pharmaceutical company developing the compound
8 (2) Illustrations reproduced courtesy of Cell Signaling Technology, Inc. (www.cellsignal.com)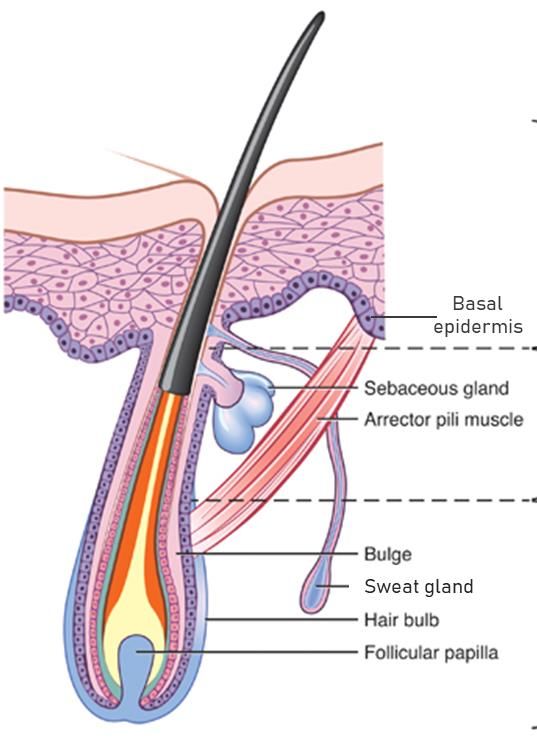
ZN-c3: Comprehensive Clinical Development Plan
Ongoing and Planned Clinical Programs Overview
Phase 1 Phase 2 • Initial Phase 1 monotherapy
dose escalation data
reported at AACR 2021
Solid Tumors: Monotherapy Dose Uterine Serous Carcinoma
Escalation Monotherapy Ph 2 Study • ZN-c3 was safe and well-
Initial data presented at AACR 2021 Expected Initiation 3Q 2021 tolerated as a single agent
• RP2D for ZN-c3 determined
Ovarian Cancer
Chemo Combination Ph 1b Study • ZN-c3 showed Exceptional
Initiated 4Q 2020 Additional Clinical Studies Responses in heavily
pretreated subjects with
Osteosarcoma advanced solid tumors
ZN-c3 + gemcitabine Ph 1/2 Study
Expected Initiation 3Q 2021 • Corresponding studies with
Monotherapy Study Zentera in Greater China
Ovarian Cancer Combination Study
ZN-c3 + niraparib Ph 1/2 Study
Expected Initiation 2H 2021
9
Initial Results of ZN-c3 Phase 1 Monotherapy
Dose Escalation Trial
10ZN-c3 Study: Schema and Endpoints
Dose Escalation Dose Expansion
Dose escalation of Dose Expansion in
ZN-c3 QD plus MTD/RP2D subjects with Uterine
Subjects with
Solid Tumors
1 - 2 additional dosing Serous Carcinoma (USC)
schedules or Mutations of Interest
(N = up to ~70) (N = up to ~40)
Study Objectives include:
• Safety and tolerability of ZN-c3, determination of maximum tolerated dose
(MTD) based on a CRM model, and recommended Phase 2 dose (RP2D)
• Clinical activity according to RECIST v 1.1: ORR, DOR, PFS, CBR
• Plasma pharmacokinetics (PK) of ZN-c3
• Evaluation of exploratory biomarkers
11ZN-c3 Study: Inclusion / Exclusion Criteria Key Inclusion: • Subjects must have a solid tumor with advanced or metastatic disease, refractory to standard therapy or for whom no standard therapy is available, or the subject is ineligible for standard therapy • Eastern Cooperative Oncology Group (ECOG) performance status ≤2 • Measurable or evaluable disease per RECIST version 1.1 Key Exclusion: • Major surgery within 28 days, radiation therapy within 21 days, stem cell transplant within 3 months, or serious illness/medical condition • Hypersensitivity to any drugs similar to ZN-c3, or prior therapy with a WEE1 inhibitor 12
ZN-c3 Study: Dose Cohorts, Dose Frequency, Number of Subjects
Enrolled and Cancer Types (as of 02/12/2021)
Dosing Cohorts, Gender and Cancer Type
ZN-c3 Dose in mg Males Females Cancer Types (Primary) Dosing Cohorts, Frequency and # of Subjects
25 QD 0 2 Lung (2)
50 QD 1 1 Breast, Colon Median Prior Lines: 4 (1-18)
75 QD Bladder, Breast (2), Colon (3),
(Expansion Cohort) 5 5 Endometrium, Gall Bladder, Pancreas,
Prostate
100 QD 3 1 Breast, Prostate (2), Testis
200 QD Endometrial Serous Carcinoma,
1 2
Rectum, Prostate
300 QD Ampulla of Vater, Breast, Colon (2),
(Expansion Cohort) 6 6 Kidney, Lung, Ovary, Prostate (2),
Retroperitoneum, Uterus (2)
175 BID Ampullary Invasive, Breast, Colon,
2 4
Ovary, Pancreas, Prostate
350 QD Colon (2), Gastric (2), Pancreas,
3 3
Uterus
400 QD 2 1 Biliary Tract, Colon, Pancreas
450 QD 3 1 Colon (2), Lung, Uterus
RP2D
450 QD Ramp Up 1 2 Lung, Pancreas, Prostate
13Monotherapy Responses for Representative Agents
Untargeted, All-Comer Targeted
• AZD1775 (WEE1 inhibitor) • Larotrectinib (Trk inhibitor)
• Metastatic Solid Tumor study • Metastatic Solid Tumor study
• N=21 • 8/8 PRs (100%) in NTRK fusion(3)
• 2 PRs (9.5%)(1) • Zero responses in 62 patients (0%)
Responses only in BRCA mutants who were NTRK-
Average Expected Expected Response Rates
Response Rates = 6.5%(2) = 18-78%(4)
(1) Do Kh et al. Journal of Clinical Oncology. 2015
(2) Chakiba C et al. Journal of Clinical Oncology. 2016
(3) Hong DS et al. Annals of Oncology. 2019
(4) Gyawali B et al. JNCCN. 2020
14ZN-c3 Study: Initial Waterfall Plot (Updated 03/01/2021)
ZN-c3 Dose Escalation and Expansion Study
Best % Change in Target Lesion Size and Best Overall Response
≥300mg Dose Cohorts (N= 29 (1))
80
≥300mg Cohorts N= 42
Measurable Disease: 37
60 No scans, ongoing: 4
No scans due to withdrawn consent, Inv Dec: 4
Median Prior Lines: 4 (1-18)
40
PD PD ORR evaluable = 29
PD PD ORR: 5/29 (17%) [95%CI: 6%, 36%]
PD
20 PD ORR evaluable (USC only subset) = 5(1)(3)
PD
PD
SD SD+ CPD PD
Inv Dec SD PD USC USC NSCLC(2) CRC (2) Ovarian (2)
CRC CRC LeiomyoS CRC LeiomyS CRC
0 Pancreas Prostate Pancreas CRC SCLC RCC Breast CRC CRC USC CRC USC NSCLC Gastric Pancreas
PD SD
SD
-20
SD+
SD+ PD
-40
uPR+
-43% uPR+ cPR+
cPR
-60 -49% -50%
-51%
cPR+
-65%
-80
(1) 3 subjects with no treatment scans (CRC, USC, Pancreas), and experienced clinical progressive disease (CPD). + denotes treatment ongoing
(2) 3 confirmed Exceptional Responders PRs, including an additional confirmation of Exceptional Responder PR since AACR Presentation Press Release
15 (3) Updated as of 03/15/2021ZN-c3 Study: Exceptional Responders on Single Agent ZN-c3
Initial Results from ZN-c3 Study
• Preliminary evidence of rapid, single agent clinical activity in heavily
pretreated patients generating Exceptional Responses
• PRs also in tumor types not expected with WEE1 monotherapy (e.g., non-USC
or BRCA1/2 WT patients)
• At the time of the data cutoff on March 1, 2021, 5 subjects with best overall
response of Partial Response (PR) by RECIST v1.1:
• 3 confirmed Exceptional Responder PRs(1) in multiple tumor types (ovarian
cancer, CRC, NSCLC)
• 2 unconfirmed PRs in USC
• RP2D 300mg QD with continuous dosing
Exceptional Responses were observed in non-USC patients who had
experienced up to 18 prior lines of treatment and no recent responses
16 (1) Additional confirmation of Exceptional Responder PR since AACR Presentation Press ReleaseExceptional Responders: Who Are They?
Who is an Exceptional Responder? Characteristics of an
Exceptional Response
• Unexpected
• Rapid
• Durable
Exceptional Responses are generally
"NCI selected those that fit specific criteria [for an Exceptional
observed randomly, and the underlying
Responder]: The patient's tumors shrank or disappeared in response driver of response is often unknown
to a drug that worked for less than 10% of patients overall in a
clinical trial. Or the patient had a response that lasted at least three
times longer than it had for a typical patient."
- Harold Varmus, Weill Cornell Medicine
17Exceptional Responders Exhibit Unique Biological Features
Zentalis Predictive Biomarker Approach Confirming Biomarker Profile
Genomic Profiling
(Tissue and Liquid • Zentalis has observed, at this initial stage
Biopsy) of the ZN-c3 study at the time of the
Biology MOA Proteomics data cutoff on March 1, 2021, multiple
Exceptional Responses on single agent
CRISPR/Cas9 screen ZN-c3 (3/3 patients or 100% ORR)
Expression data/IHC
• Activity in tumor types (e.g., CRC) not
previously seen by other WEE1 inhibitors
Unique and Predictive • In addition: Partial Responses seen in
Biomarker Profile USC patients
• Prospective Identification • Zentalis Predictive Biomarker approach
of “Exceptional Responders” used to confirm unique, novel and
• Addresses High Unmet Clinical
Need and Meaningful Patient
predictive profile
Populations
• Indication Agnostic
• Straightforward Development of
Companion Diagnostic
18Summary of Relevant Genomic Backgrounds
CCNE1
TP53 BRCA1/2
amplification
Amp
MUT
All subjects WT
(n=43)
MUT WT WT
Amp
Partial
MUT WT
Responders (1)
(n=5) WT
19 (1) Includes 3 Exceptional Responder cPRs (one additional confirmation of Exceptional Responder PR since AACR Presentation Press Release) and 2 USC uPRsExceptional Responder #1: First PR seen in ≥3 lines
Exceptional Responder #1 Summary
• 63-year-old White male, Stage IV CRC, metastases to
the liver, lymph nodes, and pleura. ECOG PS 1 Previous Therapy Experience
• Heavily pretreated with 5 prior lines of therapy (see Best
table) Intent of Regimen Start Stop
response
Treatment
• ZN-c3 starting dose: 450 mg QD on August 18th, 2020 Advanced / Bev / 5FU / LV 20/Jun/2018 28/May/2019 Unknown
Metastatic
• Dose reduced to 300 mg QD on D32 due to Gr 3
Advanced / Irinotecan / 24/Jul/2019 31/Dec/2019 Unknown
neutropenia, then 200 mg QD (5/2) on D77 due
Metastatic 5FU / LV / Bev
Gr 2 nausea, vomiting and Gr 1 diarrhea
Advanced / MK0482 30/Jan/2020 12/Mar/2020 PD
• TP53 mutant. BRCA1/2 negative. CCNE1 amp negative Metastatic
Advanced / ABBV181 / 15/Apr/2020 13/May/2020 PD
• Duration on study: 169 days (5.6 months), off study Metastatic ABBV151 27/May/2020
now due to progressive disease
Advanced / AGEN2373 1/Jul/2020 1/Jul/2020 PD
Metastatic
Confirmed PR with 51% reduction overall
Bev: Bevacizumab, 5FU: Fluorouracil, LV: Leucovorin, PD: Progressive disease
(updated 03/01/21); AGEN2373: anti-CD137 AB, ABBV181: PD-1 inhibitor, ABBV151: GARP- TGF-β1 MAB
First PR seen in ≥3 lines
20Exceptional Responder #1: Unexpected, Dramatic and Durable
Decrease of Tumor Marker within Weeks of First ZN-c3 Administration
CEA Tumor Marker
Start of ZN-c3
• CEA tumor marker typically
used in CRC
• Patient experienced rapid CEA
decrease from 327 ng/mL at
PD1i + Bispecific GARP-TGF-β1 baseline toExceptional Responder #1: Baseline and Follow-up Liver Imaging and
Tumor Markers with 51% Partial Response (Updated 03/01/21)
Baseline: 07/30/2020 1st Assessment: 10/09/2020
22Exceptional Responder #2: Experienced 18 prior lines and first
response seen in over two years with ZN-c3
Exceptional Responder #2 Summary Intent of
Treatment
Regimen Start Stop Best
Response
• 72-year-old White female, Stage IV ovarian cancer, metastases Adjuvant Carboplatin / 8/Sep/2011 10/Nov/2011 Unknown
to the pleura, peritoneum and retroperitoneum. ECOG PS 1 Paclitaxel
Adjuvant Letrozole 27/Apr/2012 25/Oct/2013 PD
• Heavily pretreated with 18 prior lines of therapy, 11 of which
were in the advanced/metastatic setting (see table) Adjuvant Carboplatin / 7/Nov/2013 20/Feb/2014 SD
Paclitaxel
• ZN-c3 starting dose: 175 mg BID on October 7th, 2020 Adjuvant Carboplatin / 17/Apr/2014 29/May/2014 Unknown
• Dose was reduced to 300 mg QD on D13 due to Gr 3 Taxol
diarrhea and Gr 2 dehydration, further modified to 200 Adjuvant Zejula UNK/UNK/20 20/Jul/2014 Unknown
mg QD (5/2) on D69 due to persistent Gr 1-2 dizziness 14
Tolerating 5 days on 2 days off weekly Adjuvant Arimidex 20/Mar/2015 5/Jun/2015 Unknown
• CA-125 dropped from 610 kU/L at baseline to 125 kU/L within Adjuvant Aromasin Total 18 Prior Lines14/Aug/2015
13/Jun/2015 Unknown
4 weeks after first dose and normalized 3 weeks later Advanced/
Advanced APG115 (MDM2
Paraplatin / 27/Feb/2019
8/Jan/2016 05/Aug/2019–
23/Jun/2016 NASD
(not
/Metastatic
Metastatic inh)
Avastin / UNK – applicable)
• TP53 mutant. BRCA1/2 negative. CCNE1 amp positive / Pembrolizum
Gemzar 28/Apr/2016
ab
• Duration on study. 186 days (6.2 months) and remains on Advanced /
Advanced
Avastin
ABBV-155
28/Jul/2016
09/Sep/2019
8/Sep/2016
09/Sep/2019
SD
PD
Metastatic
study / Metastatic (CD275 ADC)
Advanced / Avelumab 10/Nov/2016 16/Mar/2017 SD
Advanced
Metastatic NC318
(MSB0010718 16/Oct/2019 23/Dec/2019 SD
Confirmed PR with 65% reduction overall (updated / Metastatic (Siglec-15
C) AB)
03/01/21) with 18 prior lines and first response seen in Advanced
Advanced SM08502
Liposomal 13/Feb/2020
13/Apr/2017 9/Apr/2020
31/Aug/2017 PD
PD
// Metastatic (CLK inhibitor)
over two years; Remains on study Metastatic Doxorubicin
23Exceptional Responder #2: Unexpected, Dramatic and Durable
Decrease of Tumor Marker within Weeks of First ZN-c3 Administration
CA-125 Tumor Marker
Start of ZN-c3
CLK inhibitor
• CA-125 tumor marker typically
used in ovarian cancer
• CA-125 dropped from 610 kU/L
Siglec-15 mAb at baseline to 125 kU/L within
4 weeks after first dose
and normalized 3 weeks later
• Patient remains on study and
tumor marker remains down
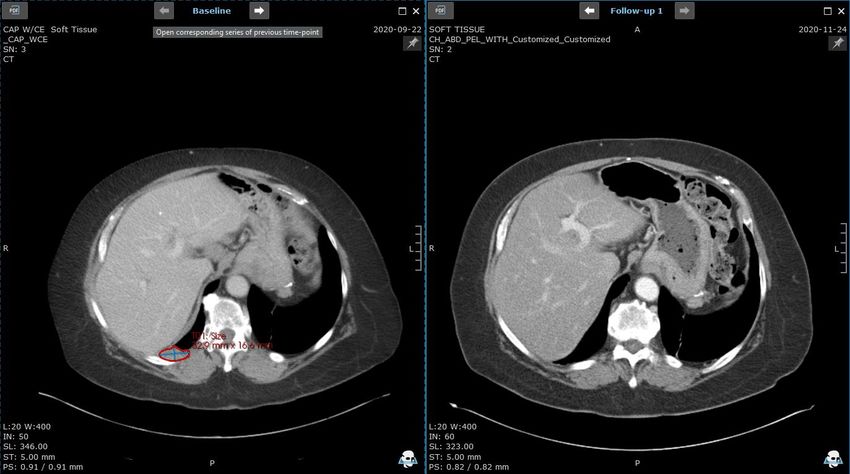
24Exceptional Responder #2: Baseline and Follow-up Porta Hepatis
Lymph Node; Overall 65% Partial Response (Updated 03/01/21)
Baseline: 09/22/2020 1st Assessment: 11/24/2020
25Exceptional Responder #2: Baseline and Follow-up Pleural Lesion
with Complete Regression
Baseline: 09/22/2020 1st Assessment: 11/24/2020
26Exceptional Responder #3: No responses seen prior to ZN-c3
Exceptional Responder #3 - Summary
Previous Therapy Experience
• 61-year-old White male, Stage IV NSCLC, Intent Regimen Start Stop Best
metastases to lung, liver, ECOG PS 0 of Treatment Response
• 3 prior lines of therapy in the advanced/metastatic Neoadjuvant Carboplatin/ 27/Nov/2018 05/Feb/2019 SD
Paclitaxel
setting
Adjuvant Durvalumab UNK/Feb/2019 UNK/Jul/2019 PD
• ZN-c3 starting dose: 350 mg QD on November 17th,
2020, no dose reduction Advanced Carboplatin/ UNK/Jul/2019 23/Oct/2019 PD
/ Metastatic Pemetrexed
• TP53 mutant. BRCA1/2 negative. CCNE1 amp Advanced Atezolizumab UNK/Jan/2020 UNK/Mar/2020 PD
negative / Metastatic
Advanced Docetaxel UNK/Apr/2020 20/Sep/2020 PD
• Duration on study: 145 days (4.8 months) and / Metastatic
remains on study
Confirmed PR with 50% reduction overall at
first evaluation; Remains on study
27Exceptional Responder #3: Baseline and Follow-up Lung Mass
Imaging with 50% Partial Response
Baseline: 11/10/2020 1st Assessment: 01/18/2021
28USC Partial Response #1
USC Partial Response #1 - Summary
Previous Therapy Experience
• 72-year-old, White female, Stage IV USC; metastases to
peritoneum and lymph nodes, ECOG PS 1 Intent of Regimen Start Stop Best
Treatment Response
• 1 prior line of therapy in the advanced/metastatic Adjuvant Carboplatin 10/Dec/2018 27/Mar/2019 Unknown
setting / Paclitaxel
Advanced / Paclitaxel / 06/Dec/2019 27/Mar/2020 Unknown
• Starting dose: 350 mg QD on December 9th, 2020 Metastatic Avastin
• Dose reduced to 300 mg QD on D55 due to Gr 3 Maintenance Avastin 24/Apr/2020 30/Oct/2020 Unknown
fatigue
• Tumor marker CA 125:
• December 8th, 2020: 35.8 U/mL
• February 10th, 2021: 16 U/mL
• TP53 mutant. BRCA1/2 negative. CCNE1 amp negative
Unconfirmed PR of 49%; Remains on Study
29USC Partial Response #2
USC Partial Response #2 - Summary
• 69-year-old, African American female, Stage IV USC,
metastases to lymph node and lung, ECOG PS 1 Previous Therapy Experience
Intent of Regimen Start Stop Best
• 4 prior lines of therapy in the advanced/metastatic Treatment Response
setting Advanced / Carboplatin / Taxol 13/Sep/2019 22/Nov/2019 PD
Metastatic / Avastin
• Starting dose: 300 mg QD on January 13th, 2021
Advanced / Trastuzumab 24/Feb/2020 07/Apr/2020 PD
• Dose modified to 300 mg QD (5/2) on D44 due to Gr Metastatic (Herceptin)
2 nausea Advanced / Pembrolizumab / 30/Apr/2020 21/May/2020 PD
Metastatic Lenvatinib
• Further reduced to 200 mg QD on D51 due to Gr 2
fatigue, nausea and anorexia Advanced / Doxorubicin 24/Jun/2020 12/Nov/2020 PD
Metastatic Liposomal
• Tumor marker CA-125:
• Baseline: 440.4 U/mL
• D63: 46.4 U/mL
• TP53 mutant. BRCA1/2 negative. CCNE1 amp negative
Unconfirmed PR of 43%, Remains on Study
30RP2D Shows Highest AUC Between 25 mg and 400 mg Doses
Interim Plasma Pharmacokinetics
20000
Day1 (QD)
Day15 (QD) • Greater than dose proportional
AUClast (ng•hr/mL)
Day1 (BID) exposure up to 450 mg (not
15000
Day15 (BID) plotted)
• 1.87 to 2.50-fold accumulation
10000 at 200-350 mg dose
• No additional increase of
5000 exposure occurs beyond Day 15
(up to Cycle 6)
• ZN-c3 shows ~30% more
0
0 100 200 300 400 exposure than AZD1775 300 mg
RP2D dose(1)
Dose (mg)
25 & 50 mg: n=2 200 mg: n=3 400 mg: n=3
75 mg: n=10/8 300 mg: n=16/9 175 mg BID: n=7/5
100 mg: n=4 350 mg: n=10/9
31 (1) Cancer Chemotherapy and Pharmacology (2020) 86:97–108Decreases in p-CDK1 Show Target Engagement for WEE1 Inhibition
1. CDK1 phosphorylation by WEE1
Confirmation of WEE1i Target Engagement in Surrogate Tissue
1. CDK1 phosphorylation (p-CDK1) is mediated by WEE1 ZN-c3 WEE1
2. Inhibition of WEE1 therefore will lead to inhibition of p-CDK1
3. Skin biopsies were performed at baseline (C1D1) and on-
treatment (C1D15) to verify p-CDK1 levels, and hence level of target 1.
2. p-CDK1 inhibition
engagement of WEE1
p-CDK1 = Brown Staining (subject with cPR) Y15
CDK1
3. Skin Biopsy
Basal C1D1
epidermis
C1D15
Hair bulb
40x
-99% -100%
32 Source: Drawing adapted from Servier Medical Art Hair bulb Basal epidermisPK/PD Correlation Shows Active Target Engagement at RP2D
WEE1 Target Engagement
100
More WEE1 Target Engagement
• Inhibition of p-CDK1
50 demonstrates WEE1 target
p-CDK1 (% inhibition)
engagement
0 • Increase in dose / drug
exposure directly relates to
WEE1 target engagement
-50
Average drug
exposure at RP2D • Data supportive of RP2D
-100
0 5000 10000 15000 20000
AUC0-24 hr (ng*h/mL)
Higher Drug Exposure
33Interim Adverse Events (≥3 events) of All Patients (as of 02/12/2021)
Nausea 63.6 5.4 5.4 49
Diarrhea 43.6 3.6 3.6 32.7 N = 55
Fatigue 41.8 5.4 5.4 29
Vomiting 34.5 1.8 1.8 29
Decreased appetite 23.6 1.8 10.9
Anemia 14.5 9 5.4 7.2
Constipation 10.9 7.2
Dehydration 10.9 5.4
Edema peripheral 10.9 0
Abdominal pain 9 1.8 5.4
Dizziness 9 5.4
Hypertension 9 5.4 1.8
Platelet count decreased 9 3.6 3.6 7.2
White blood cell count decreased 9 3.6 3.6 7.2
Alanine aminotransferase increased ALL AEs 7.2 1.8 1.8 5.4 Related AEs
Blood alkaline phosphatase increased 7.2 1.8 3.6
Dyspnea 7.2 1.8 1.8
Hypophosphatemia 7.2 3.6
Hypotension 7.2 1.8 1.8
Pyrexia 7.2 0 All Grades (All AEs)
Weight decreased 7.2 3.6
Abdominal distension 5.4 1.8 All Grades (Related AEs)
Ascites 5.4 0
Confusion state 5.4 1.8 1.8 Grade ≥ 3 (Related AEs)
Headache 5.4 3.6
Hepatic enzyme increased 5.4 3.6 3.6 Grade ≥ 3 (All AEs)
Neutrophil count decreased 5.4 1.8
Tumor pain 5.4 0
-75 -50 -25 0 25 50 75
34Interim AEs (all events): ZN-c3 ≥300 mg versus Adavosertib 300 mg(1)
N = 34 N = 34
• ≥300 mg QD • 300 mg QD for days
continuously for 21 1-5, then days 8-12
days of 21-day cycle of 21-day cycle
• 6.3 grams dosed (published)
in cycle • 3.0 grams dosed
in cycle
Adverse Events (%)
Source: Liu JF et al. J Clin Oncol. 2021 Mar 11:JCO2003167
35 (1) Non-head-to-head comparison. Results of a head-to-head comparison may differ significantly from those set forth herein. In addition, because our Phase 1 clinical trial for ZN-c3 and
the Adavosertib clinical trials were separate trials, differences between the results of the trials may not be statistically or clinically meaningfulZN-c3 Exhibits Meaningfully Reduced Hematological Toxicities
versus Adavosertib(1)
Chart Title TRAEs at ≥RP2D
Interim Grade ≥3 Hematological
35
32.3
30
25 23.5
63% Less
91% Less Despite continuous
20 Neutropenia
dosing delivering twice
% of Subjects
Anemia for
For ZN-c3
ZN-c3
14.6
the drug load, ZN-c3
15
induces markedly less
60% Less
Thrombocytopenia hematological toxicity
10 8.8 For ZN-c3
5.8
5
2.9
0
Anemia Neutropenia Thrombocytopenia
Adavosertib 300mg Intermittent ZN-c3 ≥ 300mg QD Continuous
Source: Liu JF et al. J Clin Oncol. 2021 Mar 11:JCO2003167
36 (1) Non-head-to-head comparison. Results of a head-to-head comparison may differ significantly from those set forth herein. In addition, because our Phase 1 clinical trial for ZN-c3
and the Adavosertib clinical trials were separate trials, differences between the results of the trials may not be statistically or clinically meaningfulOther ZN-c3 Studies 37
ZN-c3 Phase 2 Monotherapy Study in USC
Overview of Uterine Serous Carcinoma (USC) USC Represents High Unmet Medical Need
• Type II endometrial cancer
Comprises 10% of Endometrial Cancers with Highest Mortality
• Not hormonally mediated
All Endometrial Cancer
• Approx. 70% of USC present with Stage III or IV disease New Cases and Deaths (2020 Estimated)
at diagnosis 100%
All Other
• Poor survival rates; only 30-50 %, even if confined to Endometrial
uterus Cancer 7,680
• >90% of USCs have TP53 mutation 50%
59,058
• Recurrence rates are 29-80% post-surgery
• ~6k new cases and ~4.5k deaths in U.S. per year 4,910
6,562 USC
• Current standard of care: comprehensive surgery, 0%
New Cases Deaths
adjuvant chemotherapy and adjuvant vaginal cuff
brachytherapy
Zentalis Initiating Phase 2 Monotherapy Trial for
Patients with USC in 3Q 2021
38 Source: Gynecologic Oncology 115 (2009) 142-153, David Boruta et al.; National Cancer Institute, SEER 2020 DataZN-c3 + Gemcitabine: Novel Combination Approach for Osteosarcoma
ZN-c3 + Gemcitabine SJSA-1 Sarcoma Tumor Model Clinical Unmet Need in Osteosarcoma
3600 Vehicle control (1d off, 6d on) × 2 cycles
ZN-c3 30 mg/kg (1d off, 6d on) × 2 cycles + qd × 3 days
Gemcitabine 100 mg/kg qw × 3 • Approximately 1,000 new cases in the US(1)
3000 ZN-c3 30 mg/kg (1d off, 6d on) × 2 cycles + qd × 5 days p.o. + Gemcitabine 100 mg/kg qw × 3 i.p.
• Up to 90% have sequence mutations or
structural variants in TP53 and are often
Tumor Volume (mm3)
2400
enriched in relapsed or refractory cases,
portending resistance to chemotherapy(2)
1800
• No significant advances over the last 10 plus
years(3)
1200
• Overall survival rate for patients with
metastatic or recurrent disease isZN-c3 + Zejula (niraparib) Collaboration with GSK
Zentalis and GSK Collaboration Agreement
• Announced April 12, 2021
• Zentalis will evaluate the combination of
WEE1 inhibition (ZN-c3) and PARP inhibition
(niraparib) in patients with advanced
epithelial ovarian cancer
• ZN-c3’s tolerability profile shows promise for
future combinations with niraparib and other
drugs
• Zentalis/Zentera retain full ownership of ZN-c3
• Details of the study will be disclosed on
www.clinicaltrials.gov
Initiating Phase 1b in 2H 2021
40ZN-c3 Market Opportunities 41
Versatility of WEE1 Inhibition Could Unlock Large Addressable
Populations Across Solid Tumors
Potential Market Opportunities for WEE1
Combination
Predictive Therapy Settings
Biomarker
Driven
Orphan
Settings
Setting
Drug Setting Single Agent Single Agent Combination
Biomarker Identified PARP Related (Early, Adjuvant, Late Lines)
Representative Uterine Serous
“Exceptional Responders” Chemo Related (Ovarian, NSCLC, CRC, Osteosarcoma)
Indication(s) Carcinoma
Across Tumor Types Novel Related (Undisclosed)
Response ~30% 50% plus Indication Specific
Expectations
Population
~6,500 (US Only)(1) 10,000 – 30,000 (US only) Large
Incidence(s)
42 (1) Gynecologic Oncology 115 (2009) 142-153, David Boruta et al.; National Cancer Institute, SEER 2020 DataZN-c3 Summary
• ZN-c3 has strong evidence for clinical activity: Exceptional Responders in heavily
pretreated populations, as well as PRs in USC patients
• ZN-c3 appeared safe and well-tolerated with a wide therapeutic window
• Zentalis declared RP2D with continuous (not intermittent) dosing at 300 mg QD
• Zentalis confirming Unique Predictive Biomarker for the Exceptional Responder patient
population
• ZN-c3 may offer treatment to diverse solid tumor indications:
AS SINGLE AGENT IN COMBINATIONS
• Uterine Serous • PARP Related
Carcinoma
• Chemo Related
• Exceptional
Responder Population • Novel Related
ZN-c3 has the Potential to be
Best-in-Class WEE-1 Inhibitor in the Clinic
43Questions? 44
Key Milestones
Expected Expected
Event Event
Timing Timing
ZN-c5 (Oral SERD) ZN-d5 (BCL-2 Inhibitor)
✓ Phase 1 topline results from monotherapy dose ◼ Achieved ✓ IND Clearance ◼ April ‘20
escalation study July ‘20
✓ Initiate Phase 1 trial in AML and Non-Hodgkin’s Lymphoma ◼ Achieved
✓ Initiate Phase 1b combination study with abemaciclib ◼ Achieved
4Q ’20
b 4Q ‘20
◼ Phase 1 topline results from Window of Opportunity study ZN-e4 (EGFR Inhibitor)
◼ 1H 2021
◼ Initial results from dose escalation study ◼ 2021
◼ Initiate Phase 2 monotherapy study ◼ 1H 2021
◼ Evaluate potential for use in combinations for treatment of ◼ 2021+
◼ Initiate Phase 2 combination study with palbociclib ◼ 1H 2021 lung cancer
A
◼ Initiate Phase 1b combination study with ZN-d5 ◼ 2021
Integrated Discovery Engine
◼ Initiate Phase 2/3 monotherapy in earlier-stage patients ◼ 2021 (1)
◼ Submit 5th IND ◼ 2021
ZN-c3 (WEE1 Inhibitor)
Zentera
✓ Initiate Phase 1b combination dose escalation study with ◼ Achieved
◼ Submit ZN-c5 and ZN-c3 INDs in China ◼ Achieved
chemotherapy in ovarian cancer b 4Q ‘20 ✓ 1Q ‘21
✓
◼ Phase 1 initial results from dose escalation study in ◼ AACR
advanced solid tumors 2021 a ◼ Submit ZN-d5 INDs in China ◼ 2021
◼ Initiate Phase 2 monotherapy in uterine serous carcinoma ◼ 3Q 2021
◼ Initiate Phase 1/2 chemotherapy combo in osteosarcoma ◼ 3Q 2021
45 ◼ Initiate Phase 1/2 niraparib combo in ovarian cancer ◼ 2H 2021 ✓AchievementsContact Us
Anthony Sun, M.D., Melissa Epperly,
CEO and Chairman CFO
asun@zentalis.com mepperly@zentalis.com
(212) 433-3780 (215) 290-7271
Corporate Office Science Center
530 Seventh Ave 10835 Road to the Cure
Suite 2201 Suite 205
New York, NY 10018 San Diego, CA 92121
46You can also read

















































