WELLBEING FIRST QUEENSLAND ALLIANCE FOR MENTAL HEALTH JULY 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

QUEENSLAND ALLIANCE FOR MENTAL HEALTH
WELLBEING
FIRST JULY 2021
Wellbeing First imagines a future
state where everyone has access
to locally designed wellbeing
supports and where the nation’s
growth is measured not just in
economic terms but also in its
mental wellbeing.
2 QUEENSLAND ALLIANCE FOR MENTAL HEALTH
QUEENSLAND ALLIANCE
FOR MENTAL HEALTH
Queensland Alliance for Mental Health (QAMH) is the peak body for
the Community Mental Wellbeing Sector in Queensland. We represent
more than 100 organisations and stakeholders involved in the delivery
of Community Mental Wellbeing Services across the state.
Our role is to reform, promote and drive community mental wellbeing service delivery for all
Queenslanders, through our influence and collaboration with our members and strategic partners.
At a federal level, we collaborate with Community Mental Health Australia. We work alongside
our members to add value to the sector and act as a strong advocate on issues that impact
their operations in Queensland communities.
ACKNOWLEDGEMENTS DISCLAIMER
This report is informed by eight months of The views or opinions in this report do not
research and exploration. The research was necessarily reflect all the stakeholders that
led by CEO Jennifer Black with guidance from were consulted during the life of the project.
Jose Ramos (Action Foresight) and Helen Glover
Many of the service examples that have been
(Enlightened Consultants).
showcased throughout the document have been
The work was supported by the staff of the chosen because their values and frameworks
Queensland Alliance for Mental Health. align with the vision articulated. QAMH has
not formally evaluated the efficacy of these
A range of workshops and consultations were
approaches but has provided references for
held with QAMH members and key stakeholders
the further interest of readers.
across the mental health system within
Queensland and across the nation. We thank Every effort has been made to ensure this
all of those who participated. document is accurate, reliable, and up to date
at the time of publication. QAMH does not accept
AVAILABILITY any responsibility for loss caused by reliance on
this information and makes no representation or
The report is available online at
warranty regarding the quality or appropriateness
www.qamh.org.au.
of the data or information.
QAMH CONTACT DETAILS
Address: 433 Logan Road, Stones Corner QLD 4120
For any further information please contact:
Jennifer Black
Chief Executive Officer
Email: jblack@qamh.org.au
Tel: (07) 3394 8480
WELLBEING FIRST 3GLOSSARY
ACRONYMS:
QAMH Queensland Alliance for Mental Health
CMHA Community Mental Health Australia
ABS Australian Bureau of Statistics
HHS Hospital and Health Services
MBS Medicare Benefit Schedule
NDIS National Disability Insurance Scheme
LGBTIQ+ Lesbian, gay, bisexual, transgender, intersex, and queer/questioning, and
the + represents other identities not captured in the letters of the acronym
PHN Primary Health Network
MHCT Mentally Health Cities Townsville
WHO World Health Organisation
KEY TERMS
A model that emphasises medication-based treatments and
Biomedical model
monitoring to reduce mental illness symptoms.
A state of high wellbeing. Flourishing states have a high presence
Flourishing
of psychological, emotional and social wellbeing indicators.
A state of low wellbeing. Languishing states have low levels
Languishing
of emotional, social and psychological wellbeing indicators.
An approach that places the person experiencing mental ill-health
Person-centred
at the centre of the service.
An approach that responds to the person as the leader of their
life in ways that foster personal agency and the capacity to
Person-led
manage challenges. Person-led approaches require providers
to be accountable to the person.
Individualised supports that create opportunities for people
Psychosocial to better respond to their needs, such as social connection,
supports relationships, self-care and economic participation. Also
called “wellbeing supports” for the purposes of this report.
4 QUEENSLAND ALLIANCE FOR MENTAL HEALTHCONTENTS
Queensland Alliance for Mental Health 3
Acknowledgements 3
Glossary 4
Foreword from the CEO 6
Executive Summary 7
Part 1: The mental health crisis 8
1.1 The current public mental health crisis 8
1.2 The impacts of COVID-19 10
1.3 The response required 12
Part 2: The argument for change 14
2.1 Personal experience and outcomes 14
2.2 The Economics of mental wealth 16
2.3 Reduce the burden on acute services 16
2.4 Culture and stigma 17
2.5 Limitations of the current mental health ecosystem 17
2.6 The identity of the Community Mental Wellbeing Sector 18
2.7 The challenge of actioning reform 20
Part 3: Emerging opportunities for the Community Mental Wellbeing Sector 21
3.1 A focus on mental wealth 21
3.2 Pivot from mental illness to wellbeing 22
3.3 The potential of the Queensland Community Mental Wellbeing Sector 24
3.4 Use of technology 25
Part 4: The preferred future 26
4.1 The future scope of the Community Mental Wellbeing Sector 26
4.2 The characteristics of community wellbeing service design 29
4.3 Mental wellbeing program characteristics to be resisted 33
Part 5: QAMH leading into the future 34
5.1 Lead and influence the unique value of the sector 34
5.2 Modelling service design 34
5.3 Strengthening workforce wellbeing capability 35
5.4 Build a collection of mental wellbeing resources 35
Methodology 36
References 38
WELLBEING FIRST 5JENNIFER BLACK
FORWARD
FROM THE CEO
Since the global pandemic hit, we have all been faced with significant
disruption to our lives and a prolonged period of uncertainty. It has
been a blow to the mental health of the nation.
For those of us who work in the mental health This vision is not a wish list, but the result of
sector, it has once again shone light on a system deep consideration by the members of QAMH
desperately in need of change. and key representatives of the broader mental
health system. You may notice this report refers
The pandemic came just after the release of
to the community managed sector as the
the draft report of the Productivity Commission’s
Community Mental Wellbeing Sector. This
inquiry into Mental Health (2019). While there
is deliberate, in that it underlines the unique
has been a plethora of reviews and reports
contribution of the sector and the preferred
over the past two decades, the Productivity
change of direction articulated in this report.
Commission - the nation’s key economic advisory
body - confirmed that the mental health system Our preferred future has been formulated using
is in crisis. Compellingly, it stated that the right strategic foresight thinking, processes and
services are often not available when needed, scanning mechanisms. It is set within the
leading to wasted health resources and missed political, economic, social, technological, legal,
opportunities to improve lives. At the beginning and environmental horizons of the next five
of 2020, a new Human Rights Act also came to ten years.
into force in Queensland and the idea that our
system was failing to improve the lives of the “Strategic foresight is the ability to create
people it was set up to help, was hard to absorb. and sustain a variety of high-quality forward
The Queensland Alliance for Mental Health views and to apply emerging insights in
(QAMH) is the peak body for community organisationally useful ways.”
managed mental health organisations - those (Slaughter, 2018, p 11)
organisations that provide much practical support
to people in mental distress in our community. We know integration within the system and
During the pandemic, we witnessed a surging across systems is crucial and that the Community
need for these services. In response, the sector Mental Wellbeing Sector needs to embrace
rapidly developed innovative models of care, its unique offering in the context of the broader
showing strength, resilience and agility. system to be most effective. We also acknowledge
that a range of responses will always be required
It struck the QAMH team that this crisis could
to meet community needs. While the preferred
be the burning platform to finally effect real
future outlined in this report has been configured
change in the system.
largely for the Community Mental Wellbeing
To this end, QAMH has collaborated with futurist Sector, we believe many of the ideas could have
Jose Ramos (Action Foresight) and mental broader application.
health innovator Helen Glover (Enlightened
Wellbeing First is a call to fundamentally shift
Consultants), to paint a vision for the future.
the focus of our sector from managing illness
to actively supporting wellbeing.
Jennifer Black
6 QUEENSLAND ALLIANCE FOR MENTAL HEALTHEXECUTIVE SUMMARY
This report examines the urgent and compelling • For decades, people with lived experience
need for change in the mental health system. have been calling for new approaches, and
many report their most positive experiences
This is based on three key points:
have been with community mental wellbeing
• The current system has been repeatedly services.
identified as one which is struggling with
• In this report, QAMH argues that only when
demand, fragmented, siloed and difficult for
a range of alternatives to medical intervention
the public to navigate.
can be accessed, will the system be truly
• This vexed system is now facing unprecedented trauma informed and recovery oriented.
pressure from the mental health impacts of the
The vision outlined in Wellbeing First would
COVID-19 pandemic.
have life-changing benefits.
• Human distress does not always need a
For the individual, this approach will build social
medical response. For this reason, we need
and economic participation. For clinical mental
to move beyond current models of care, and
health services, it will alleviate many of the current
pivot to a contemporary whole of community
demand pressures. It will increase community
approach that places Wellbeing First.
resilience to life challenges. And for the nation,
In this report, the Queensland Alliance for Mental it will foster mental wealth.
Health (QAMH) calls for fundamental changes to
Mental Wealth is defined as the collective
the way we fund and position community mental
cognitive and emotional resources of citizens.
wellbeing services in Queensland.
It includes people’s mental capital, their mental
There are several clear reasons to do this: health and wellbeing which underpins the ability
• The Community Mental Wellbeing Sector is to work productively, creatively and build and
an under-utilised element of the mental health maintain strong positive relationships with others.
ecosystem with huge potential to provide a Wellbeing First imagines a future state where
practical, early intervention approach. everyone has access to locally designed well-
• The pandemic has taught us that mental being supports and where the nation’s growth
wellbeing supports are no longer considered is measured not just in economic terms but
relevant only to a small proportion of people also in its mental wellbeing.
living with disadvantage. There is growing
demand to recognise them as economic,
social and health necessities for everyone.
”
In this report, the Queensland Alliance for Mental Health
(QAMH) calls for fundamental changes to the way we
fund and position community mental wellbeing services
in Queensland.
WELLBEING FIRST 7PART 1:
THE MENTAL HEALTH CRISIS
KEY POINTS
• The COVID-19 pandemic has raised • People are demanding a different
public discourse about the importance experience from mental health care.
of wellbeing. • The Community Mental Wellbeing
• The pandemic will have significant Sector is ready to provide broader
impacts on the mental health of a wellbeing services.
broad sweep of the population.
• The responses so far to the mental
health crisis focus on acute treatment
rather than wellbeing supports.
The COVID-19 pandemic has significantly 1.1 The current public mental health crisis
disrupted our lives, fundamentally changing
Our mental health models are principally
the way we live, work, love, and play. For many
designed to be reactive, crisis-driven and focus
people, the impact on their mental health has
on those with severe and persistent mental ill
been significant and the notion of actively
health. Care is often experienced as coercive,
working on their own wellbeing has been
traumatising or re-traumatising, creating
a new experience.
unintended harm to those who most need help.
Never have we seen such widespread public
The mental health system is notoriously difficult
discourse about the importance of our collective
for people to navigate, particularly when in
wellbeing. The prevalence of diagnosed mental
distress, leaving no alternative but to go to a
health issues such as depression and anxiety
hospital emergency department. In 2018 the
have been steadily increasing and COVID-19
Australasian College of Emergency Medicine
has increased all the known risk factors. The
concluded that the current mental health
enormity of the situation has identified the gaps
system fails individuals, families, and health
in available supports and highlighted the
services, and that the strain on emergency
challenges for traditional mental health services
departments as well as patients and families
to adapt to the rapidly changing needs of the
is unsustainable (Duggan, 2020). People with
population. There is an urgent and compelling
lived experience have outlined the distress of
need to change how we design, access, and
overcrowding, noise, long waits and the use of
provide mental wellbeing supports that are
restrictive practices in emergency departments.
responsive and meet a whole of population need.
Despite this, emergency departments are still
the primary access point for people in distress
and will remain so until sustainable community
alternatives are established and supported.
8 QUEENSLAND ALLIANCE FOR MENTAL HEALTHAlarmingly, there is also a large number of people Although well intended, many community mental
the Productivity Commission calls the ‘missing health services have simply transposed a
middle’. This cohort is considered to be too unwell biomedical model of care into community
to be treated in the primary care system but are settings. The Community Mental Wellbeing
not deemed sick enough to be treated by acute Sector is well-placed to provide an alternative
services. They fall between the cracks of federal but is often limited by a lack of resources and
and state funding and cannot necessarily afford by prescribed models of care designed to reduce
to access private support (Australia. Productivity the burden on the medical system.
Commission, 2020). Post COVID-19, they are
likely to be left languishing in greater levels
of distress. Even if the ‘missing middle’ are
eventually found, it is likely to be through a
medical model.
The Existing Mental Health Ecosystem Most primary mental health care is provided
Mental health services in Queensland are by GPs and the most common intervention
funded at both a federal level through primary is medication. In 2019-20 there were 40.7
care initiatives and the National Disability million mental health-related prescriptions
Insurance Scheme (NDIS), and at a state provided to 4.4 million people, with an
level by Queensland Health through the average of nine prescriptions per person
Hospital and Health Services (HHS) and (Australia. Australian Institute of Health and
community-based services. Additional Welfare, 2021). In the preceding year,
services can be accessed through the 1.3 million people received MBS-rebated
private health system but primarily by those psychological therapy and the PHNs com-
who can afford the out-of-pocket expenses. missioned 70,000 sessions. 60,000 young
people received help through headspace
Primary Care centres and about 4,000 used supported
Primary health services such as GPs, health online treatment (Australia. Productivity
nurses and allied health professionals often Commission, 2020).
act as the entry point into the mental health
In addition to these services there are a
system and provide services to those
range of online and telephone-based sup-
not requiring emergency care. These may
ports, for example: Lifeline, Kids Helpline,
be people seeking help for the first time,
Sane Australia Helpline, Beyond Blue,
receiving assistance for mild to moderate
Parent line, PANDA and Diverse Voices.
mental illness, or managing their serious
mental health issues with support. Hospital-Based Care and Specialist
Mental Health Services
Funding primarily comes from the Federal
Government through Medicare rebates and The state funds specialist mental health
at a local level through the Primary Health services or clinical services, either as
Networks (PHNs), which have a major role outpatient or residential and bed-based
in developing and commissioning a range acute services. These are provided by the
of mental health and suicide prevention HHS and are designed to provide support
services within their local regions. to those with a more severe or complex
mental illness or those in crisis.
WELLBEING FIRST 9...Continued from previous page Psychosocial Programs
The 1300 MH Call access line is another The non-government or not-for-profit
key entry point into public mental health sector, supported by a mix of state and
services. This mental health telephone federal funding, has been the main source
triage service: “can provide support, of psychosocial services in Queensland.
information, advice and referral; provide However, the psychosocial support landscape
advice and information in a mental health shifted significantly with the introduction of
emergency or crisis; is staffed by trained the NDIS. The NDIS now funds support for
and experienced professional mental health thousands of people who have a significant
clinicians; will provide a mental health triage psychosocial disability through individual
and refer to acute care teams where support packages.NDIS statistics indicate
appropriate” (Queensland Government, that in the July to September 2020 quarter,
2020). there were 7,067 participants with psy-
Emergency Care chosocial disability in Queensland, who
had an individually funded plan under the
The entry point into the clinical mental
NDIS (NDIS, 2020). Since its introduction,
health system is often through hospital
the scheme has been criticised about its
emergency departments. Due to the lack
accessibility and its ability to respond to
of alternatives available in the community,
participants with mental illness.
people in crisis either turn up themselves
or are brought in by emergency services The Queensland government continues
and the police. There are some interesting to fund other local supports through the
programs, providing community triaging non-government sector. Many of these
points with an element of lived experience, operate in conjunction with clinical services
but they generally lack the resources to and often require a clinical referral. This
provide effective 24-hour assistance. In means they are not readily available to
Queensland there are eight new crisis support the public as an early intervention or
spaces being trialled which are in various self-management option.
stages of development.
1.2 The impacts of COVID-19 Forecasting the lasting impacts on the nation’s
mental health is particularly challenging without
The problems of the system are not new, but the
knowing the duration of the pandemic, and
pandemic has amplified them. The full impacts
without any similar scenarios to draw upon.
of COVID-19 have not yet been realised and are
What is clear, is that in the long term there is likely
difficult to predict. What we do know is that the
to be a significant increase in the number and
psychological distress is widespread, stemming
severity of mental health issues requiring a
largely from the immediate impacts of the virus
response from the mental health system.
and the consequences of physical isolation and
separation from and/or death of loved ones. The Black Dog Institute reports up to a 40
In addition, many people have lost or are at risk per cent increase in calls to support lines like
of losing their income and livelihoods, creating Beyond Blue and Lifeline and online supports.
uncertainty about the future. We know that there In a recent Australian study 78 per cent of
is strong evidence that employment has a respondents indicated their mental health had
positive relationship with mental health and that worsened since the beginning of the pandemic,
with every 1 per cent increase in unemployment, with a significant impact on the mental health
there is a comparable increase in suicide rates of those with a pre-existing mental health issue.
(Christensen, 2020).
10 QUEENSLAND ALLIANCE FOR MENTAL HEALTHGiven that loneliness, social isolation, and (Christensen, 2020). Australian Bureau of
financial stress are significant risk factors for Statistics data released in May 2020 suggested
mental distress and suicidal ideation, it is that 76 per cent of Australians with children
particularly concerning that 80 per cent of in their household kept them at home during
people have reported moderate to extreme that period. In order to care for their children
loneliness and worries about finances (Newby, 38 per cent of people worked from home, 22
2020). The onset of COVID-19 has also led per cent worked reduced hours or changed
to an increase in alcohol consumption with their working hours and 13 per cent took leave
55 per cent of Australians reported to be (Australia. Australian Bureau of Statistics, 2020).
drinking at levels hazardous to their health The added stress within relationships and the
(Christensen, 2020). restrictions on movement has correlated with a
30 per cent increase in violence towards women,
In the past year, investment into acute mental
adding yet another level of consequence to
health services has increased to deal with surging
the public health actions (Christensen, 2020).
demand, suggesting more people are asking for
help for the first time. In its December 2020 Older people are also at increased risk not only
budget, the Queensland government allocated from the life-threatening complications of
an extra $743,488 million to the state’s health COVID-19 but also from the stress of accessing
budget. The detail of this was closely linked to care for other physical and mental health issues.
hospital demand with the announcement of new Loneliness is a major risk factor for mortality
hospitals, ambulance stations and health facilities. in older adults and they are more likely to be
impacted by social isolation while physical
The demand has come from a broad sweep
restrictions are in place.
of the community.
The health workforce is likely to be adversely
Emotional difficulties among children and young
affectedby the stress of heavier workloads,
people have been exacerbated by increasing
the risks of becoming infected, of passing the
stress and anxiety, including within their families.
infection to their own families and communities,
The pandemic has led to social isolation, more
as well as observing higher rates of death in
family violence and disrupted schooling at
their care.
critical points in the emotional development
of young people. Research from headspace The economic fallout is also likely to exacerbate
indicates 74 per cent of young people have existing health care disparities. This will result
experienced poorer mental health than before in a disproportionate impact on those already
the pandemic. Many feel that COVID-19 has socially disadvantaged including those with
had an adverse impact on their confidence in serious mental illness, disabilities, Aboriginal
achieving future goals. Interestingly, their most and Torres Strait Islander people, the LGBTIQ+
frequently used coping strategy has been talking community and those from culturally diverse
to family and a reliance on natural supports backgrounds.
(see headspace, 2020).
In Queensland, there are additional difficulties
The mental health impacts experienced by associated with the state’s size and geographical
women are expected to be harsh, judging by diversity. In regional and remote areas, the
employment figures alone. Almost 200,000 known risk factors include isolation as well
women have lost their jobs and 110,000 have as recurring natural disasters such as bushfires,
left the workforce altogether since March floods, and drought. Very few mental health
2020. At the peak of the COVID-19 restrictions services are available, leading to long waiting
more than one million women had no work at times and significant travel to receive treatment.
all. Women in the workforce are more likely to Sadly, suicide rates in very remote regions are
be doing most childcare and household work, more than twice the national average (Australia.
as well as home schooling during lockdowns Australian Institute of Health and Welfare, 2021).
WELLBEING FIRST 11In 2019, suicide rates in Queensland were With a philosophy and approach that focusses
significantly higher than the national average on wellbeing rather than illness, community
(Australia. Australian Bureau of Statistics, 2020). organisations could support people experiencing
It is the primary cause of death in Queenslanders mental health difficulties before they reach
aged between 15 and 44 and the rate of suicide crisis point, early in the trajectory of their
in Queensland’s Aboriginal and Torres Strait distress. Access points and entry pathways
Islander population is double that of the general to these wellbeing supports away from clinical
population (Queensland Mental Health gateways must also be created.
Commission, 2019).
For the individual, early intervention will build
Without timely and active responses to distress social and economic participation. For com-
the rates of mental illness and suicide will munities, it will increase resilience to common
inevitably rise. life challenges. For clinical mental health services,
it will alleviate many of the current demand
1.3 The response required pressures. And for the nation, it will foster
This widespread impact has prompted demands mental wealth.
for more help across the population. This requires Governments around the globe are considering
a whole of government approach to put the ways to foster mental wealth, in part prompted
mental wealth of the nation at the forefront by the effects of the pandemic. The final report
of all decision making. from the Productivity Commission Mental
There is a better way to provide mental health Health Inquiry outlined an economic argument
care in the community. for investment in the mental wellbeing of the
nation (Australia. Productivity Commission,
In September 2020, QAMH consulted key
2020). It found the economic benefits from
stakeholders including CEOs of prominent
following its recommendations would amount
mental health organisations. There was
to as much as $18 billion a year.
consensus that not all distress needs a
medical intervention. Prioritising mental wealth would reap significant
economic and societal rewards. But it requires
We know that the most successful public health
investment in the mental wellbeing of everyone
strategies in times of crisis have been highly
– a whole of population wellbeing approach.
practical in nature, as exemplified by responses
to various natural disasters. The Community
Mental Wellbeing Sector is ready to deliver
practical support in this crisis.
12 QUEENSLAND ALLIANCE FOR MENTAL HEALTHIndividual benefits Mental health ecosystem benefits
• Improved mental wellbeing due to earlier • Reduced demand on emergency
intervention departments and acute bed-based
• Increased satisfaction that services can services
respond to needs • Reduced need for more expensive
• Decreased friction points to access support crisis intervention responses
• Reduced number of people using the
Community benefits Health and Hospital System to access
• Increased community wellbeing and support
mental wealth • Reduced demand on assessment
• Increased economic engagement and and treatment services
productivity • Free up space within clinical systems
• Increased liveability of care to focus on those that require
• Access to services are normalised and clinical interventions
encouraged, helping to reduce stigma • Reduced number of referrals from clinical
• Increased levels of community access, to community mental wellbeing services
engagement, and participation • Improved clarity about the unique
• Meet community expectations of acces- contribution of the Community Mental
sibility and locally designed initiatives Wellbeing Sector
• Reduced duplication and competition
between services
Mentally Healthy City Townsville groups to build local wellbeing capacity
to create, improve and grow community
Townsville was the first city in Australia to
resources. The MHCT website offers
take up the Mentally Healthy Cities challenge
information about local mental health and
to support population-wide wellbeing.
wellbeing supports, including online sites
Mentally Health Cities Townsville (MHCT)
and apps. Similar approaches have been
is auspiced by the Tropical Brain & Mind
successfully implemented in London and
Foundation to take action to support the
Philadelphia.
communities within the Townsville City
Council area to achieve a balance of mental
Find out more:
health and wellbeing that enables our citizens
to cope with the normal stresses of life, https://www.mentallyhealthycitytowns-
realise their abilities, participate in, and ville.com.au
belong to community, and work productively.
MHCT engages with the Townsville City
Council, Townsville Hospital and Health
Service, the MHCT Champions, the
corporate and business sectors, community
mental health sector and broader community
WELLBEING FIRST 13PART 2:
THE ARGUMENT FOR CHANGE
KEY POINTS
• Despite multiple calls for change in • Poor mental health has broad
the mental health ecosystem, there economic costs
has been no significant reform
• The Community Mental Wellbeing
• The system is fragmented, siloed, Sector can foster wellbeing outcomes
difficult to navigate and designed to that help build the mental wealth
gatekeep demand for clinical resources of the nation
• A focus on early care in an episode
or illness is crucial to ease the pressure
on acute services
2.1 Personal experience and outcomes Alarmingly, at a time when there is emerging
discourse around the protection of human
For decades, the voice of lived experience has
rights, the mental health system has been
told us they want services that help them stay
described by the very people who seek help
well and regain control of their lives. The voice
within it as traumatising and retraumatising.
of lived experience has driven much of the
contemporary reform agenda, articulating the The Community Mental Wellbeing Sector has
need for a focus on wellbeing, greater self- provided a welcome point of difference. People
determination and less restrictive care. with lived experience of our sector, often report
their best experiences as those which challenge
People with lived experience of care have
them to try new things, learn new skills and
described a system which is coercive and
engage in full community life (Biringer, 2017;
entrenched in a culture of discrimination leading
Myers et al., 2016). Services that adapt to meet
to stigmatised responses from health care
the needs of participants rather than offering
professionals. This implicit discrimination leads
a one-size-fits-all approach can achieve even
to low expectations placed on those accessing
greater results.
services and dependence on the system, limiting
their own ability to manage distress, drive their The Community Mental Wellbeing Sector would
care, and lead contributing lives (Carrotte, 2019; benefit by continuing to challenge itself to work
Edwards, 2017). People with lived experience with people in different ways and ensure its
have detailed the power imbalance in the current workforce is equipped to help individuals
mental health system; how they have limited drive their own care and outcomes.
choice and control of their own treatment; how
that treatment relies heavily on medication to
alleviate distress, but which, in some cases,
impairs their quality of life.
14 QUEENSLAND ALLIANCE FOR MENTAL HEALTHGift of Gallang to each week’s session. The program
was developed by Mission Australia’s
The Gift of Gallang ‘Healing of the Mind,
Cultural Connect worker Roxanne Ware,
Body & Spirit’ is a suicide prevention school
a Bundjalung woman of Northern NSW,
-based program specifically developed for
who was born and raised in the community
Aboriginal and Torres Strait Islander children
of Inala. Ms Ware consulted with community,
in Brisbane’s Inala region (grades 4-6). The
key indigenous organisations, and experts
program is also currently delivered in the
over a three-year period. The Gift of Gallang
Logan and Beaudesert regions.
is community-driven, developed and owned
The program aims to provide children with by the Aboriginal and Torres Strait Islander
tools to support and nurture their resilience community. Training was also undertaken
while providing a safe environment. Its to ensure the appropriate and sensitive
development was prompted by several components of the program would meet the
deaths by suicide of Aboriginal and Torres needs of young ones and youth, delivering
Strait Islander children and young people in the core message of healing and resilience.
the community. The community recognised
the significant impact of these deaths on Find out more:
the well-being of individuals, families and https://www.facebook.
communities. com/434251400094091/vid-
Children are immersed in cultural age-old eos/904179850055259/
traditional ceremonies, practices and https://www.missionaustralia.com.au/pub-
spirituality to strengthen their identity lications/research/children-and-families
and give them a sense of belonging and
connection. These are seen as crucial
factors in enabling the children to weather
obstacles and adversity in life. Children The program aims to provide
are provided and taught strategies using children with tools to support
different mediums to manage their own and nurture their resilience while
social and emotional well-being. Aboriginal providing a safe environment.
and Torres Strait Islander members of the
community or those with strong cultural
ties to the area facilitate the 11-14 week
program, with a psychologist attached
WELLBEING FIRST 152.2 The Economics of mental wealth Given we know that 1 in 5 Australians already
experience mental ill health in any given year
Poor mental health has economic consequences
(Australia. Department of Health, 2021), we
beyond health care, with costs incurred in the
can safely assume that this ratio will increase
justice system, aged care, housing, and
the longer the pandemic continues. A response
education.
which simply strives to get more people into
The Productivity Commission indicated that in face-to-face care with health professionals
2018-2019 the annual cost to the economy of is expensive and not necessarily accessible,
mental ill health and suicide in Australia was as relevant, responsive, or effective.
much as $70 billion. This is made up of direct
expenditure of $16 billion on mental health care, 2.3 Reduce the burden on acute services
calculating the annual cost of lower economic The mental health ecosystem is designed to
participation and lost productivity at $39 billion respond to the impacts of mental illness, and
and $15 billion in replacing the support provided the most resource intensive systems of care
by family and/or friends. It went on to say that are in the crisis space. While there is widely
the cost of disability and premature death due accepted evidence that early intervention is the
to mental illness, suicide and self-inflicted way of the future, much of the focus to date has
injury was equivalent to a further $151 billion been on early intervention in life, rather than ear-
per year (Australia. Productivity Commission, ly intervention in illness or episode. This means
2020). These numbers make a compelling the system has been geared towards acute
economic argument for change. care providing mainly biomedical solutions.
Between November 2006 and June 30, 2019, It is well recognised that busy emergency
general practitioners wrote 31 million mental departments are over-stimulating and unsuitable
health care plans costing $2.75 billion, clinical environments for people in mental distress, but,
psychologists provided sessions costing without realistic alternatives, they remain the
$2.45 billion and registered psychologists primary entry point for receiving care (Duggan,
provided sessions costing $2.6 billion 2020). Mental health presentations to emergency
(Rosenberg, 2020). These figures would be far departments have increased by 70% over the
greater if all those who needed these services past 15 years (Commonwealth of Australia, 2020).
could afford them and were able to access The acute system is consequently struggling
them. Even so, there is little evidence to suggest with demand. The hospital has to act as
this investment has decreased the prevalence gatekeeper of its limited resources and many are
of mental illness. left without care. Those who do make it through
The system is costly for the taxpayer and simply the doors are at greater risk of untimely or
not producing the outcomes desired for the unplanned discharge and relapse, subsequently
health and wellbeing of the nation. Many increasing hospital readmission rates.
countries, such as the United Kingdom and There must be a pivot towards mental wellbeing.
New Zealand, have begun to realise the impact
of wellbeing on the economy and are moving The Community Mental Wellbeing Sector could
to a policy language which articulates the value play a crucial role in reducing this burden on the
of mental wealth and a stronger emphasis on acute system, by delivering services which
early intervention in both life and episode or focus on wellbeing and flourishing and provide
illness (New Zealand. Ministry of Health, 2020). active intervention early in an episode of mental
distress. This will provide better outcomes for
16 QUEENSLAND ALLIANCE FOR MENTAL HEALTHthe individual and provide alternative avenues 2.5 Limitations of the current mental
for help other than the local hospital emergency health ecosystem
department. We are not suggesting that there
is no need for acute services. But enlisting Many of the reports into the mental health
the Community Mental Wellbeing Sector to system in Australia describe a system which
provide early interventions would enable acute is fragmented, siloed, difficult for the public to
services to concentrate on those who absolutely navigate and designed to gatekeep the limited
require them. resources at the clinical end.
This is a considered economic and wellbeing Many people in distress miss out entirely. Those
strategy to provide the right resources, at the who do not meet the entry criteria for accessing
right time in the right place. State Funded Mental Health Services or the
National Disability Insurance Scheme but require
2.4 Culture and stigma more support than can be accessed through
a GP or PHN, are often referred to as the
The overwhelming barrier to change within
“missing midle”.
the mental health ecosystem is its own culture.
Culture is formed by the explicit and implicit The Productivity Commission estimated a
values and customs of how we collectively do staggering 690,000 people would likely benefit
things. The mental health system’s culture is from access to psychosocial support services
the ‘elephant in the room’ when examining the if they were available. However, only 34,000
failure to embrace reform. people currently receive NDIS psychosocial
support (which is only just over 50% of those
The current culture stems from a paternalistic
expected to be eligible when the scheme is fully
model of caring which ultimately values the
rolled out). In addition, 75,000 people receive
expertise of the clinical professional over the
support directly from other government-funded
experience of the person living with an illness.
programs. The gap is massive. The report also
People with lived experience of the system
acknowledged that many others without a
talk about a culture that promotes fear and
formal diagnosis may benefit from psychosocial
powerlessness and low expectations placed
support but would currently need to enter a
on their recovery.
medical pathway to receive any. It surmised that
A similar power imbalance is experienced by as many as one million Australians are missing
different services in the mental health ecosystem, out (Australia. Productivity Commission, 2020).
stemming from entrenched beliefs about what
Despite the significant efforts of PHNs to promote
different parts of the system can and should
a mix of community services to people, they are
contribute. For the Community Mental Wellbeing
regularly undersubscribed. Activities include
Sector, there are low expectations from other
peer support and services with a focus on
elements of the system of its professionalism
building resilience and wellbeing. However, one
and ability to manage risk and support com-
of the most difficult challenges for these services
plexity. This is due to its evolution and limited
is a lack of awareness and recognition of the
resources, and despite the positive outcomes
value of these supports by GPs. The Productivity
being achieved by many community services.
Commission states that it is common practice
for GPs in Australia to prescribe medication
for mental distress (Australia. Productivity
Commission, 2020). Referral to existing services
is limited and when they do, they continue
to refer people to clinical supports. This is
through a Mental Health Care Plan for people
to access Medicare-funded clinical services,
though most will be required to pay a “gap”.
WELLBEING FIRST 17This “gap” payment can sometimes mean The public knows very little about the Community
the difference between receiving help and Mental Wellbeing Sector. Most mistakenly
languishing without. believe community mental health care is actually
private therapy accessed through a GP. The
Despite many reports articulating the need for
public is largely unaware about the support
person-centred care, there is still limited focus
that could be provided by the Community Mental
on personal recovery and wellbeing models
Wellbeing Sector and is therefore unable to
with early intervention at the episode or illness
advocate effectively for this.
level. Trauma-informed care and recovery-
oriented practice are widely used concepts that Although some providers run multimillion dollar
describe a human centred way to work with national organisations, the sector is made up
individuals in distress. But despite pockets of of many small and large organisations that
good practice, the reality is that the change have often grown around a unique offering in
in language has not deeply altered the methods a particular region. This evolution has resulted
in practice. Many people still report experi- in inconsistent expectations of what the sector
encing care as coercive and traumatising and its workforce can deliver. As such, the
or retraumatising. specialisation and unique contribution of
the Community Mental Wellbeing Sector to
2.6 The identity of the Community Mental individuals, communities and the wider mental
Wellbeing Sector health ecosystem is not well articulated and
The Community Mental Wellbeing Sector has undoubtedly underutilised.
largely emerged and grown in response to the Traditionally, wellbeing services are regarded by
high demands placed on acute services. It has people receiving care as a welcome alternative
been funded primarily to provide aftercare to to clinical intervention, because they offer
people diagnosed with a moderate to severe practical support, coaching and life skills. Many
mental illness with a focus on preventing services have developed models based on
relapse or readmission. consultation with participants.
An artificial tension has developed between
clinical and non-clinical settings, with an
historical misconception that the Community
Mental Wellbeing Sector can provide support
only under the guidance of clinical services.
This keeps the wellbeing sector firmly in the
realm of managing illness rather than supporting
mental wellbeing. The sector also suffers from
limited funding and short funding cycles, creating
barriers to attracting, retaining and developing a
skilled workforce. Despite this, some services
have shown expertise in providing clinical
services themselves – and often with a
wellbeing and early intervention framework.
18 QUEENSLAND ALLIANCE FOR MENTAL HEALTHToowoomba Clubhouse, During their time with Momentum Mental
now Momentum Mental Health Health, participants are coached, either
online, over the phone or in person. Among
Toowoomba Clubhouse provides a
the many group activities and programs
supportive environment for its members
participants can join, are sessions which
to develop valuable life skills and receive
offer practical help with budgeting, sleep
mental health support. The clubhouse
hygiene and exercise, and a Job Club.
was established 25 years ago, after its
Momentum takes a collaborative, inclusive
founders noted a shortage of community
approach, ensuring there is less of a power
-based assistance for those living with a
imbalance than in most traditional mental
mental illness in the area. CEO Deborah
health services. It also uses a number of
Bailey describes the service as “not a
methods to receive feedback from members,
traditional clubhouse” as it offers one-
using that feedback to ensure Momentum
on-one coaching to meet the needs of
remains relevant in its community.
individuals. Given the dynamic nature of
the service, the organisation is adopting a Find out more: https://www.toowoom-
new name – Momentum Mental Health. baclubhouse.org.au
Along with the new name, the service
has significantly changed the way it
offers support. One change that has
won strong community backing is that
Momentum Mental Health will no longer
require a diagnosis to access its services.
“If someone wants to work on their mental
health and they can access the service
how it’s intended, they are welcome,”
said Deborah. Another change is that
participants will set out their goal on entry,
plan how they want to achieve it, how
they will celebrate when they reach their
goal, and what their situation will look
like when they are ready to exit the service.
WELLBEING FIRST 192.7 The challenge of actioning reform The Productivity Commission acknowledges
the findings of its report are not new and that
Why have we been unable to effect the
many reform documents release earlier have
change recommended by multiple inquiries?
failed to trigger change. The publication Croakey
Unfortunately, the system is stuck in a cycle,
provides an insight into the system’s stagnation,
holding on to the core belief that medical
stating that there is thirty years of evidence
intervention is the main solution to the problem.
that official inquiries into mental health have
While medical responses can be valuable for
rarely led to major change; there were thirty-two
many, it is not the only strategy to manage
of these reports between 2006 and 2012 alone
distress and mental wellbeing.
(Doggett, 2020).
The Productivity Commission suggests that
its recommendations would address cultural
There is a myth that drives many change
barriers to change.
initiatives into the ground: that the
organisation needs to change because However, the reality is that enacting the rec-
it is broken. The reality is that any social ommendations would require shifting resources
system is the way it is because the people from acute care to alternative co-designed
in that system (at least those individuals models. This would be expensive in the short
and factions with the most leverage) want term, until the value of these alternatives could
it that way. In that sense, on the whole, on be evaluated and proven. To date, it has seemed
balance, the system is working fine, even cheaper and easier to tweak the current system
though it may appear to be dysfunctional or invest in more of the same.
in some respects to some members and
There is a role for a range of services to make
outside observers, and even though it faces
up the mental health ecosystem. Providing
danger just over the horizon. There is no
practical early intervention responses early
such thinking as a dysfunctional organisation
in distress, would allow the more expensive
because every organisation is perfectly
medical interventions to be used where they
aligned to achieve the results it currently
are most needed and most effective.
gets. (Heifetz, 2009)
Human distress does not always need a medical
response.
20 QUEENSLAND ALLIANCE FOR MENTAL HEALTHPART 3:
EMERGING OPPORTUNITIES
FOR THE COMMUNITY MENTAL
WELLBEING SECTOR
KEY POINTS
• Focus on the sector’s ability • Develop prevention and early
to contribute to Queensland’s intervention frameworks to become
mental wealth the main entry point to the system
• Pivot to a wellbeing framework • Further embrace technology to expand
acknowledging the wellbeing service reach and reduce stigma
continuum
3.1 A focus on mental wealth
Mental wealth is an emerging concept that is A nation’s Mental Wealth is defined as the
gaining traction across Australia and the world. collective cognitive and emotional resources
Nations have been challenged to use mental of citizens. It includes people’s mental capital,
wealth as an indicator of economic and social their mental health and well-being which
prosperity (Beddington, 2008). The economic underpins the ability to work productively,
benefits of pursuing policies that are driven creatively and build and maintain strong
by wellbeing include increased individual positive relationships with others.
productivity, reduced mental illness related
How a nation nurtures mental capital, mental
Disability Adjusted Life Years1, increased
health and wellbeing, through adequate
economic security, greater economic prosperity,
education, economic security, housing,
and increased collective community resilience.
healthcare, psychological and cultural safety,
It is only through harnessing citizens’ cogni-
and through equal access to opportunity,
tive resources that nations will prosper both
will have a significant effect on its economic
economically and socially. Early interventions
competitiveness and prosperity, and the
are key to this endeavour.
collective wellbeing and resilience of
communities.
1
One Disability Adjusted Life Year represents the loss of the equivalent of one year of full health (WHO, 2000).
WELLBEING FIRST 213.2 Pivot from mental illness to wellbeing The mixed language often places mental
wellbeing and mental illness opposite each
The United Nations has called for countries
other on a single continuum. However, good
around the world to use the current focus on
mental health or mental wellbeing is not simply
mental health to propel reforms that finally
the absence of mental illness and is not
shift care away from institutions towards a
necessarily achieved through the treatment
community approach. The United Nations
of mental illness alone.
says resources should be made available for
community-based initiatives to activate and The wellbeing continuum
strengthen local and natural supports and
Mental wellbeing and mental ill-health are two
encourage a spirit of community self-help.
different constructs, which move along two
(United Nations, 2020).
discrete but related continuums with clear
This time of crisis represents an opportunity valid indicators articulating their differences
for community-managed mental health ser- (Keyes, 2005).
vices to embrace a wellbeing approach. This
would provide a distinct yet complementary
response to the crisis, that would also be
At any given time, you can have:
sustainable.
• Low, moderate, or high levels
Now is the time to finally redesign the sys-
of mental wellbeing, AND
tem, with a real understanding that respond-
ing to mental illness does not automatically • None, some, or all the symptoms
create states of wellbeing. of a particular mental illness.
Wellbeing can only be achieved within an
ecosystem, that is underpinned by a flour-
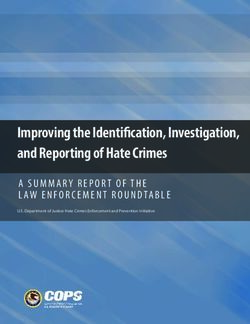
ishing framework responsive to all levels of Mental wellbeing exists on a continuum, ranging
human distress. Three critical and central from floundering to flourishing [figure 1]. A dual
tenets are necessary to guide the design and focus on both the mental illness continuum
delivery of contemporary community mental and the wellbeing continuum will ultimately
wellbeing programs; (i) wellbeing opportu- provide the best outcomes. The mental illness
nities, (ii) strengthening capacity to function continuum requires the expertise of the clinical
well, and (iii) promoting community wellbeing sector, while the Community Mental Wellbeing
(Westerhof & Keyes, 2010). Sector provides the expertise along the flour-
ishing continuum.
The terms ‘mental illness’, ‘mental health’ and
‘mental wellbeing’ are used interchangeably The impact of languishing or poor mental
but they are significantly different constructs. wellbeing is as expensive and detrimental as
The World Health Organisation (WHO) de- the experience of serious mental illness. Keyes
clares mental health as, “a state of well-being (2005) stresses that only 20 per cent of the
in which the individual realizes his or her own population experience states of flourishing at
abilities, can cope with the normal stresses of any one time, making early intervention key
life, can work productively and fruitfully, and to improving quality of life and economic and
is able to make a contribution to his or her social participation.
community” (WHO, 2004). A mental illness is
a health problem that significantly affects how
a person feels, thinks, behaves, and interacts
with others. It is also diagnosed according to
standardised criteria (Australia. Department
of Health, 2021).
22 QUEENSLAND ALLIANCE FOR MENTAL HEALTHHigh presence and experience of wellbeing indicators
Mental Health & Wellbeing Continuum
SS CO
NE MP
ILL LE
AL TE
E NT M
High presence of mental illness symptoms
Low presence of mental illness symptoms
EN
M
TE
TA
LE
L
HE
MP
ALT
INCO
H
STRUGGLING FLOURISHING
Mental Illness Continuum
FLOUNDERING LANGUISHING
INCO
ESS N
M
ILL
PL
AL
TE E
NT
M
E
EN
M TA
E T L
LE P HE
ALT
COM H
Low presence and experience of wellbeing indicators
Figure 1: Dual Mental Illness – Mental Health Continuum (adapted from Keyes, C 2005)
We can all experience mental wellbeing Many of the wellbeing challenges that people
challenges. A mental wellbeing challenge should experience, including those with an existing
not be considered any less distressing than a mental illness, are not necessarily symptoms
mental illness. Left unaddressed, challenges of a mental illness, yet often are responded
to our mental wellbeing will leave most of us to as such.
languishing, severely impacting our ability to
A mental wealth approach which values the
live well, work productively, and contribute
wellbeing of citizens will take seriously all levels
positively to community life.
of human distress, addressing it early with the
Mental wellbeing challenges usually result from expectation that will prevent chronic and costly
loss, poor liveability, social disconnectedness states of languishing. The dual continuum of
and inequity. This impact is compounded when mental illness and mental health clearly articulates
we have exhausted our personal resources: the valued and diverse contributions necessary
a loss of opportunities, loss of roles, changes within the mental health ecosystem. Reducing
in relationships, loss of purpose, experiencing the burden of mental ill health and maximising
racism or sexism, discrimination, loss of economic the potential of people’s mental wellbeing are
means, economic instability, inability to con- essential service responses required to attain
tribute, loss of autonomy, and personal agency. high levels of community mental wealth.
WELLBEING FIRST 233.3 The potential of the Queensland than its historical role of providing aftercare
Community Mental Wellbeing Sector and should be repositioned as a vital adjunct
to clinical treatment.
Creating mental wellbeing requires a different
design with a different endpoint in mind. Services We know that just one per cent of public health
that lead to a connected and contributing life funding is spent on prevention (Christensen,
in the community are more likely to produce 2020). In the mental health context, most of this
the outcomes articulated by the Productivity goes to early intervention in life as opposed
Commission. to early intervention in illness or episode.
However, early intervention in episode would
The Queensland Community Mental Wellbeing
ensure better outcomes for people with severe
Sector is an underutilised resource. There are
and complex issues and for those described
a range of organisations, employing wellbeing
as the “missing middle”. It would also prevent
specialists, adhering to a mental wellbeing
the bottle necks and demand that currently
philosophy, that could play a much greater role
plague the acute system (Table 1).
in our communities. The sector can do far more
FLOUNDERING LANGUISHING STRUGGLING FLOURISHING
Moderate to low Moderate to low Moderate to high Moderate to high
states of wellbeing states of wellbeing states of wellbeing states of wellbeing
with moderate to with moderate to with moderate to with moderate to
high mental Illness low mental Illness high mental Illness low mental Illness
symptoms symptoms symptoms. symptoms
In the current system In the current system In the current system This is a small
these people are these are the people these people are percentage of
the most likely that are most likely likely to be managing people who are
to be admitted to be accessing their own mental living well are resilient
to acute mental primary care or no illness symptoms group but have
health services services. They may well and getting on incorporated
and accessing be experiencing with other aspects wellbeing strategies
community-based early-medium in of their life. They into their daily
mental health episode distress may be experiencing lifestyle. They
services. levels. The lan- early-in episode are unlikely to
guishing group distress levels. be accessing any
could be considered Likely only to access formal helping
some of the ‘missing minimal treatment services.
middle’ that current for mental illness.
programs are not
designed for (largest
% of population)
Table 1: Describing “Floundering” to “Flourishing” cohorts of people across the wellbeing continuum.
24 QUEENSLAND ALLIANCE FOR MENTAL HEALTHYou can also read