Unmatched: Repairing the U.S. Medical Residency Pipeline - Robert Orr - Niskanen ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Unmatched: Repairing the U.S. Medical Residency Pipeline Robert Orr September 2021

The Niskanen Center is a nonpartisan 501(c)(3)
think tank that works to promote an open society.
Niskanen Center
820 1st Street NE, Suite 675
Washington, D.C. 20002
NiskanenCenter.org
Unmatched:
Repairing the U.S. Medical Residency Pipeline
Robert Orr
September 2021
NISKANEN CENTER
Contents
5 Introduction
7 The three eras of the modern U.S. residency system
7 1945–1980: The era of expansion and abundance
10 1981–2000: The era of modernization, federal retrenchment and downsizing
14 1997–present: Cumulative and persistent imbalances
16 Quantifying the residency bottleneck
20 Our broken, convoluted system of GME financing
25 Additional barriers to primary care residents
27 Policy recommendations
27 Consolidate and standardize federal GME payments
28 Reorganize GME funding
28 Abolish institution-level FTE caps on residency support
30 Vary federal payments to teaching institutions based on program size
30 Increase payments based on the share of PG-1 residents
31 End support for training beyond the 5th year of residency
32 Ensure federal GME payments are geographically uniform
33 Give states flexibility to target Medicaid GME payments
33 Plan for an organized transition to the new system
34 Establish a health care resources development bank
35 Conclusion
36 Appendix 1: Using NRMP data
38 Appendix 2: GME funding sources
39 Appendix 3: Hypothetical funding schedules
About the Author
Robert Orr is a poverty and welfare policy analyst at the Niskanen Center. He earned his BA at Skidmore
College and his MA in Economics at George Mason University. His research focuses on welfare, health
care, and economic development.
For media inquiries, please contact Louisa Tavlas at ltavlas@niskanencenter.org
NISKANEN CENTER
Introduction
“To become a doctor, you spend so much time in the tunnels of preparation —
head down, trying not to screw up, trying to make it from one day to the next
— that it is a shock to find yourself at the other end, with someone shaking
your hand and asking how much money you want to make.”
— Atul Gawande
Piecework, The New Yorker, 2005
P
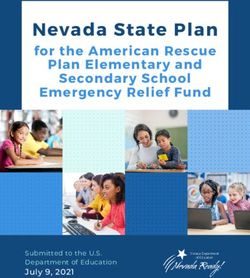
hysicians are the cornerstone of any health care delivery system. Nonetheless, the United
States employs substantially fewer of these professionals than most other developed
countries. Given that the number of physicians per person is a reasonable proxy for the
number of service access points within a health system, the United States therefore faces
greater challenges in delivering basic, accessible care to its citizens compared to other developed
countries.12
At the most abstract level, this lack of physicians is a puzzle. The combined cost of a medical
degree and postgraduate residency training is many multiples smaller than the expected lifetime
earnings of those who complete residency and become a licensed physician. This raises the question:
If the financial incentives are there, why do we have so few doctors?
The key reason for our physician shortfall is that substantial bottlenecks exist in the training and
education pipeline, with the most significant of these being the medical residency system. These
bottlenecks were initially encouraged by policymakers based upon the misguided belief that limiting
physician supply would control rising health care costs.3 Yet these attempts to constrain physician
supply growth beginning in the 1980s have been an utter policy failure, leading to no noticeable
reduction in health care costs.4 Savings have failed to materialize because when physicians are
scarce, the money simply gets spent elsewhere in the health system. All the indications are that
squeezing physician supply is much like squeezing a balloon — the costs largely migrate rather than
disappear altogether. Because physicians are the U.S. health care system’s primary access point, the
health system has effectively been encouraged to pursue high-intensity, low-access care. This shift
has been harmful because provision of the most basic medical services is generally recognized to
have the greatest marginal impact on population-level health.5 The United States’ failure to allocate
1 Robin Osborn, David Squires, Michelle M. Doty, et al., “In New Survey of Eleven Countries, US Adults Still Struggle With Access
to and Affordability of Health Care,” Health Affairs Vol. 35, No. 12 (December 2016): Page 2328.
2 Health Resources and Services Administration, “MUA Find,” 2021.
3 Robert Orr, “The Planning of U.S. Physician Shortages,” Niskanen Center, September 8, 2020.
4 Robert Orr, “The U.S. Has Much to Gain from More Doctors,” Niskanen Center, August 4, 2021.
5 Victor Fuchs, “More variation in use of care, more flat-of-the-curve medicine,” Health Affairs Vol. 23 No. 2 (2004) Var 104–107.
NISKANEN CENTER
Unmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 6
health resources effectively helps explain why our health outcomes fall short of what we would
expect given our country’s exceptional level of health spending.6 The United States thus has little to
lose and much to gain from increasing the supply of physicians across the board.7 The most effective
course of action to achieve this would be to reform and modernize federal support for the physician
residency system.
Figure 1: The U.S. has fewer physicians per-capita than most OECD countries
Source: OECD
This report unpacks the policy failures currently plaguing the residency system in the United
States and proposes how we might solve them. The first section provides an overview of the history
of graduate medical education (GME) from the standpoint of both the public and private institutional
actors. The second section examines the residency pipeline, confirming the existence of an undesirable
bottleneck in the current system. The third section analyzes the shortcomings that result from the
current mechanisms of GME financing. The final section focuses on how our GME system might be
reformed in order to resolve these issues over the long term.
6 Nancy Fullman, Jamal Yearwood, Solomon Abay, et. al, “Measuring performance on the Healthcare Access and Quality Index
for 195 countries and territories and selected subnational locations: a systematic analysis from the Global Burden of
Disease Study 2016,” The Lancet Vol. 391 Issue 10136 (June 2018): Pages 2236–2271.
7 Robert Orr, “The U.S. Has Much to Gain from More Doctors,” Niskanen Center, August 4, 2021.
NISKANEN CENTER
Unmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 7
The three eras of the modern U.S. residency system
Knowing the history of U.S. graduate medical education (GME) is critical to a full understanding of
our current predicament. Consequently, this section introduces the key players in GME,and sheds
light on their interests and ideas; explains the role of the federal government, in particular; and
reveals how our system has been developed in a patchwork fashion. The system supporting GME
in our country has ultimately achieved policymakers’ misguided top-line goal of limiting physician
supply, but along the way, it has encouraged misallocation of health care resources and entrenched
geographic inequities. The current overview will only cover the period following World War II, both
because the recognizable outlines of the residency system were still taking shape and because the
role of federal policymaking was minimal up to that point.
1945–1980: The era of expansion and abundance
Federal involvement in GME emerged during an era of rapid transformation of the American
residency system and the health system more broadly. Following World War II, booming medical
school enrollment (financed in part by the Servicemen’s Readjustment Act of 1944, also known
as the G.I. Bill, and later by the Health Professions Educational Assistance Act of 1963), on top of
increased interest in specialty training among established physicians, resulted in surging demand
for postgraduate medical training — that is, additional training beyond the MD level.8 At the same
time, federal matching funds provided through the Hill–Burton Act of 1946 led to a substantial
expansion in hospital construction in communities across the country.9 The resulting confluence of
supply- and demand-side support effectively cemented the teaching hospital as the primary venue
for postgraduate medical training in the U.S., a distinction it retains to the present day.10
The rapid expansion of the U.S. health system during this period created fierce competition among
hospitals for labor in the form of medical interns and residents. As a result, hospitals began pressuring
medical students to sign commitment contracts earlier and earlier in their medical school tenures,
eventually pushing the need for a decision into their second year. The National Intern Matching
Program (later renamed the National Resident Matching Program, and colloquially known as “The
Match”) was established as a centralized nonprofit clearinghouse to put an end to this rat race.11
When The Match was first established in 1952, there were only 5,800 medical graduates available
to fill roughly 10,500 positions.12 In other words, the supply of potential residents was exceedingly
scarce relative to the demand from hospitals.
With the establishment of Medicare in 1965, the federal government began providing direct
payments to cover the hospitals’ teaching costs. Medicare made payments to hospitals to cover its
8 Kenneth M. Ludmerer, Let Me Heal: The Opportunity to Preserve Excellence in American Medicine (Oxford: Oxford University
Press, 2014): Page 154.
9 Ibid., Page 170.
10 Ibid., Page 169.
11 Ibid., Page 172.
12 F.J. Mullin and J.M. Stalnaker, “The Matching Plan for Internship Appointment,” Journal of Medical Education, Vol. 26, No. 5
(September 1951): Pages 341–346.
NISKANEN CENTER
Unmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 8
Figure 2: In the early 1970s, Residency Review Committees eliminated pathways
for starting a general practice without undergoing a 3 year residency program.
Source: American Board of Internal Medicine
patients’ share of overall operating costs, submitted retrospectively each fiscal year based upon incurred
costs, with teaching costs included in these payments. The intent was to replace similar payments
that private insurers had previously been making on behalf of elderly patients who were now covered
by Medicare. These payments had grown considerably due to both the increasing complexity of care
and the growing demands by interns and residents for salaries and fringe compensation.13 In these
early years of the Medicare program, cost control was largely nonexistent, resulting in substantial
financial support for medical training and education programs.14 It also resulted in wide disparities in
federal support across institutions, mostly stemming from disparities in the cost of training programs
as well as from the institutions’ having an incentive to report higher costs in order to maximize their
Medicare payments.15 However, despite growing costs, the overriding preoccupation of policymakers
was to ensure the sufficiency of health provider capacity in the face of rapidly growing demand
for health care services. In addition to the funding delivered through Medicare, some states began
contributing federally matched GME funding through the concurrently established Medicaid health
13 Ludmerer, “Let Me Heal,” Page 169.
14 Committee on Implementing a National Graduate Medical Education Trust Fund, On Implementing a National Graduate
Medical Education Trust Fund, (Washington D.C: National Academy Press, 1997), Pages 54–64.
15 udmerer, “Let Me Heal,” Page 169.
NISKANEN CENTER
Unmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 9
insurance program for low-income Americans.16 However, no formal arrangement was ever put in
place to earmark GME contributions from private insurers, so the residency system gradually became
reliant upon government support, delivered overwhelmingly through Medicare.
Concurrent with the increasing flows of federal dollars into the residency system came calls to
regularize and raise training standards. At the time, the disparate residency programs were governed
by numerous autonomous Residency Review Committees (RRCs) in the individual specialties and
subspecialties. In 1972, the American Medical Association, Association of American Medical Colleges,
American Board of Medical Specialties, American Hospital Association, and Council of Medical
Specialty Societies came together to create the Liaison Committee for Graduate Medical Education
(later reorganized as the Accreditation Council on Graduate Medical Education) to oversee the RRCs.17
Three years later, the option to pursue a single-year rotating internship as a pathway to general
practice was eliminated.18 From that point onward, physicians looking to pursue a more generalist
practice would need to spend at least three years in residency programs, often via internal medicine
or the newly created family medicine specialty.19 The sole point of entry into physician practice was
now through specialist residency training (Figure 2).
Beginning in 1974, successive attempts were made to curtail cost growth in Medicare through
the placement of limits on per-patient reimbursements to hospitals, initially excluding GME from
cost controls, as policymakers also sought to maintain the government’s commitment to training
physicians.20 Thus, even as cost limits continued to tighten, exceptions were eventually established
for the financing of GME, two of which continue to inform the basis of Medicare GME financing even
today. The first, in 1979, established an exclusion from reimbursement cost limits for all direct costs
of teaching at hospitals.21 The second, established in 1980, increased the general reimbursement
cost limits based on a hospital’s ratio of interns and residents to hospital beds, in order to provide
compensation for the higher indirect costs of care at teaching hospitals.22 Even after Medicare phased
out cost-based reporting during the 1980s, reimbursement of hospitals based on this conceptual
distinction between “Direct Medical Education” (DME) and “Indirect Medical Education” (IME)
continued, remaining in roughly the same form up to the present day.23
16 im M. Henderson, “Medicaid’s Role In Financing Graduate Medical Education,” Health Affairs Vol. 19, No. 1 (January 2000):
Page 227.
17 Ludmerer, “Let Me Heal,” Page 319.
18 Ludmerer, “Let Me Heal,” Page 319.
19 Ludmerer, “Let Me Heal,” Page 319.
20 Committee on Implementing a National Graduate Medical Education Trust Fund, On Implementing a National Graduate
Medical Education Trust Fund.
21 House of Representatives, Ninety-ninth Congress, First Session “Medicare’s Prospective Payment System: Hearings Before
the Task Force on Health of the Committee on the Budget,” September 30, October 7 and 21, 1985: Page 223.
22 Ibid., Page 224.
23 Continued cost growth in Medicare prompted its transition to the Prospective Payment System (PPS) for acute-care
hospitals in 1983, replacing the old system of cost-based reimbursement. The IME and DME funding streams for residency
training were formalized and considerably revamped in the process. Indirect Medical Education (IME) was converted into
an add-on adjustment to the new PPS system, boosting payments per discharge on the basis of a hospital’s intern-and-
resident-to-bed ratio (IRB). For Direct Medical Education (DME), the direct training costs reported in 1984 were carried over
in the form of a Per Resident Amount (PRA). As with the initial iteration of DME, Medicare’s support was scaled in line with
the hospital’s share of Medicare patients.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 10
1981 to 2000: The era of modernization, federal
retrenchment and downsizing
The tide turned decisively in the 1980s and 1990s, as the conventional wisdom on physician supply
swung from shortage to surplus. The federal government retrenched its support of GME through
Medicare while nongovernmental bodies overseeing the medical training pipeline began to
promulgate policies aimed at curbing the growth in the number of U.S. physicians.
In 1981, a federally sponsored report by the Graduate Medical Education National Advisory
Committee (GMENAC) concluded that the United States was on the verge of a massive physician
surplus.24 Motivated chiefly by cost concerns, the committee reached this conclusion through
estimating the physician workforce needed to meet the country’s projected medical needs.25 The report
recommended immediate action to curtail both the domestic training of physicians and the admittance
of those trained outside of the country. Support for both medical schools and medical students was
thus sharply scaled-back.26 These moves coincided with a broader skepticism of government during
the “Reagan Revolution” of the 1980s, resulting in a retrenchment of federal support for investment
in the health system. Around the same time, federal support for the construction of hospitals, the
sites in which residency training takes place, was totally cut off (Figure 3).27
Robert Graham, the administrator of the Health Resources and Services Administration, concisely
summed up the attitudes of the era toward physician supply when he stated in 1981:28
“I believe that the Administration’s position can be interpreted as follows: (1) The general supply
of health professionals is adequate or the capacity of the U.S. health professionals schools to
produce the needed supply is perceived to be adequate, (2) there will be a minimum federal role
for investment in terms of health professions education whether we are talking about direct project
grants, institutional assistance, student aid, or other support, and (3) competition will sort out the
major issues of distribution, specialty choice, and workforce mix.”
The cause of reducing physician numbers was often taken up with great fervor by members of
24 Graduate Medical Education National Advisory Committee, Volume 1: GMENAC Summary Report, Summary Report of the
Graduate Medical Education National Advisory Committee (Washington, D.C: Department of Health and Human Services,
September 30, 1980).
25 Physician workforce forecasts models have historically been influential in shaping the conventional wisdom around
physician workforce sufficiency, both in the United States as well as abroad. 1) The methods involved in these forecasts
have evolved considerably, from rather crude projections based on indicators of workforce size and health care demand
to today’s more sophisticated approaches integrating considerations such as productivity and the substitution of tasks
between various health professions. 2) Not only has the accuracy of the inputs to the forecasts been demonstrated to
be limited in practice, but they also rest upon significant assumptions about the sufficiency of care of the status quo.
3) Important considerations such as the quality of care or provider market power remain outside the scope of these
forecasts. 1) Sabine Stordeur and Christian Léonard, “Challenges in physician supply planning: the case of Belgium,” Human
Resources for Health Vol. 8 No. 28 (December 2010); 2) Mário Amorim Lopes, Álvaro Santos Almeida, and Bernardo Almada-
Lobo, “Handling healthcare workforce planning with care: where do we stand?,” Human Resources for Health Vol. 13 No.
38 (May 2015); 3) Dominique Roberfroid, Christian Leonard, and Sabine Stordeur, “Physician supply forecast: better than
peering in a crystal ball?,” Human Resources for Health Vol. 7 No. 10 (February 2009).
26 A.W. Nichols and G. Silverstein, “Financing medical care for the underserved in an era of Federal retrenchment: the health
service district,” Public Health Reports Vol. 102 No. 6 (November 1987): Pages 686–691.
27 S. Ryan Greysen, Candice Chen, and Fitzhugh Mullan, “A History of Medical Student Debt: Observations and Implications for
the Future of Medical Education,” Academic Medicine Vol. 86, No. 7 (July 2011): Pages 840–845.
28 Barbara Barzansky and Norman Gevitz, Beyond Flexner: Medical Education in the Twentieth Century (United States: Praeger,
1992), Page 119.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 11
Figure 3: Federal support for hospital construction ended in the mid-1980s.
Source: OMB, “Table 9.6—Composition of Outlays for Grants for Major Public Physical Capital Investment: 1941-2021”
the profession, partly out of fear that a failure to reduce numbers would invite greater government
control over the profession. As Charles Evarts, the president of the American Orthopaedic Association
and a Residency Review Committee member, put it in a 1985 speech:29
“Manpower control is mandatory. The size of medical schools must be diminished; there must be a
strict limit upon foreign medical school graduates. Certain programs need to reduce their numbers,
others must consolidate, and others need to terminate voluntarily or be terminated — not the easiest of
actions. Currently there are no official agencies to directly mandate numbers. However, the impending
decrease in funding for graduate medical education will directly influence the numbers. Before our
destiny is controlled for us, we must step into the breach and exercise considerable leadership. Many
pressures will be brought to bear against those who decide to decrease the numbers of orthopedic
residents in training. Yet, there is no other choice. We cannot succumb to the temptation of increasing
numbers. We must slowly decrease the numbers and continue to increase the quality.”
The physician pipeline’s various nongovernmental accrediting and oversight bodies responded
by taking swift action to reduce numbers. In 1980, the MD-granting medical schools agreed to a
voluntary freeze on new slots as well as to the construction of additional medical schools.30
The accrediting boards also took action. The Accreditation Council on Graduate Medical Education
— the successor to the Liaison Committee for Graduate Medical Education — and many of its affiliated
RRCs raised the standards for teaching hospitals. The intent was to make residency programs harder
to establish and less financially attractive to operate.31 The accreditors’ actions frequently resulted
29 C. McCollister Evarts, “Leaders and Leadership: Tomorrow’s American Orthopaedic Association,” The Journal of Bone and
Joint Surgery Vol. 67 No. 8 (October 1985): Pages 1298–1302.
30 Robert Orr, “The Planning of U.S. Physician Shortages.”
31 A quote from obstetrics–gynecology illustrates these intentions: The Residency Review Committee (RRC) for obstetrics–
gynecology has, as do many of the RRC’s, new and more stringent special requirements, the rules and regulations under
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 12
Figure 4: In 1980, medical schools implemented a freeze on new MD slots.
Sources: Census Bureau, AAMC
in a lowering of the caps on the number of residents in approved programs and outright eliminated
programs deemed to be of insufficient quality.32 A side-effect of these retrenchment measures was a
doubling down on technical education rather than the vocational aspects of the residency experience,
an emphasis that continues to define the U.S. system to the present day.
The growing adoption of health maintenance organizations (HMOs) and other forms of managed
care added to the pressure to curb physician supply. HMOs were tightly managed, vertically integrated
health-service networks that required central approval for many procedures and doctor visits, with
the ultimate goal of curbing health care utilization. Managed care spread rapidly during the 1980s
and 1990s, with the majority of Americans being insured under such an arrangement by 1995.33 In
light of this, between 1988 and 2000, the congressionally authorized Council on Graduate Medical
Education repeatedly endorsed the need to constrain physician numbers in order to avoid a “surplus”
in its annual reports.34 35 36
which residency programs are approved. Because of stricter scrutiny of residency education programs and because of
financial constraints on hospitals, the coming decade will see, at the best, a continued plateau in resident numbers. What
is more likely is a decline in the number of approved residency programs and a slow decline in the number of residents
per year.
32 David A. Asch and Jack Ende, “The Downsizing of Internal Medicine Residency Programs,” Annals of Internal Medicine Vol.
117 No. 10 (November 1992): Pages 839–844.
33 Jon Gabel, “Marketwatch: Ten Ways HMOs Have Changed During the 1990s,” Health Affairs Vol. 16, No. 3 (May 1997): Pages
134–145.
34 Council on Graduate Medical Education, Volume I, First Report of the Council, (Washington D.C.: Department of Health and
Human Services, July 1, 1988).
35 Council on Graduate Medical Education, Fifteenth Report: Financing Graduate Medical Education in a Changing Health
Care Environment, (Washington D.C.: Department of Health and Human Services, December 2000).
36 This exuberance toward the prospects of curbing costs through managed care, which tightly manage services offered by
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 13
Figure 5: Residency bottlenecks incentivized an explosion in subspecialities.
Source: ACGME Program Accreditation Data
But even as high-level administrators sought to control the supply of physicians, new and
distinct RRCs governing the specialties and subspecialties proliferated and created new pipelines
for interns and residents. The result was to make limiting overall physician numbers more difficult
than anticipated while producing an imbalance in the make-up of the physician workforce: too many
specialists, too few primary care doctors.37 While the conventional wisdom over this period remained
ardent that the nation was on the verge of an overall “physician surplus,” the rapidly declining share
of primary care physicians had begun to raise alarm in some quarters.38
Aiming to preempt government action, the Accreditation Council for Graduate Medical Education
(ACGME) enacted a 2-year moratorium on the recognition of new subspecialty RRCs between 1992 and
1993.39 Yet this didn’t stop the Clinton administration’s failed Health Security Act from proposing that
the federal government take direct control over the approval of federally funded residency programs.40
Ultimately, though, Congress ended up merely freezing Medicare’s GME inflation adjustments for
non-primary care specialties, which lasted for two years.41
physicians is further illustrated by workforce modeling by the federal Health Resources and Services Administration of
Health Professions in 1989. Leonard Greenberg and James M. Cultice, “Forecasting the Need for Physicians in the United
States: The Health Resources and Services Administration’s Physician Requirements Model,” HSR: Health Services Research
Vol. 31 No. 6 (February 1997): Pages 723–737.
37 P.O. Kohler, “Specialists/primary care professionals: striking a balance,” Inquiry: a Journal of Medical Care Organization,
Provision, and Financing Vol. 31 No. 3 (Fall 1994): Pages 289–295
38 John Z. Ayanian, “The Prospect of Sweeping Reform in Graduate Medical Education,” The Milbank Quarterly Volume 72,
Issue 4 (December 1994): Pages 701–704.
39 L.R. Faulkner, D. Juul, R.M. Pascuzzi, et al., “Trends in American Board of Psychiatry and Neurology specialties and neurologic
subspecialties,” American Academy of Neurology Vol. 75 No. 12 (September 2010): Pages 1110–1117.
40 H.R. 3600, Health Security Act of 1993, 103rd Congress.
41 107 Statute 312 – Agricultural Reconciliation Act of 1993.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 14
This trend of retrenchment of federal support for GME culminated with the 1997 Balanced Budget
Act (BBA). The BBA impacted Medicare funding for medical residencies in two important ways. First,
the legislation reduced the generosity of the formula through which hospitals that have residents
receive increased Medicare reimbursement. Second, and most famously, it capped Medicare’s number
of funded residency slots, adjusted for inflation, at 1996 levels. Because GME funding is allocated on
a hospital-specific basis, the introduction of the cap largely froze the geographic distribution of these
slots.42 Residency programs could continue to add slots above the cap, but would receive no Medicare
funding for doing so.
1997 to present: Cumulative and persistent imbalances
Recent years have seen the culmination of various trends that had been building over the previous
two decades, and a gradual shift toward expanding physician supply. Starting in the late 1980s,
increasing competition and declining profit margins made it harder for private insurers to pass on the
higher costs associated with residency training to consumers through their premiums.43 The implicit
understanding when Medicare’s GME funding stream was established was that it would replace
merely the contributions that would have been made otherwise by private insurers had Medicare
never existed, yet there was never any mechanism devised to ensure that private reimbursements
would be earmarked for training, with the result that medical residency funding became increasingly
reliant upon Medicare.44 Yet since this funding stream was scaled based on a hospital’s Medicare-
patient load, it created a bias against the training of pediatric specialists in children’s hospitals.
In response, Congress established the Children’s Hospital Graduate Medical Education (CHGME)
program in 1999.45
By the late 1990s, the constraints on physician numbers had translated into increasing market
power, granting doctors leverage over managed care plans.46 Physicians increasingly felt empowered
to stay out of plans that limited utilization, resulting in narrower provider networks for those plans.
The tight labor markets at the turn of the new century delivered the finishing blow to what had,
up until then, been heralded as the “managed-care revolution.”47 Employers, intent on attracting
and retaining employees under conditions of low unemployment, became willing to accept large
health insurance premium increases. Limits on access to services and choice among providers largely
reverted to how they had been in the pre-managed care days.
42 Legislation enacted in the years following the BBA have since increased DGME’s cap for rural hospitals and redistributed
some unused slots, and created a mechanism for reallocating slots that would have otherwise been lost following the
closure of resident training programs.
43 James Reuter, The Financing of Academic Health Centers: A Chart Book, (Washington, D.C.: Institute for Health Care Research
and Policy, 1997).
44 M.E. Whitcomb, W.O. Cleverly, “Financial performance of academic medical center hospitals,” Academic Medicine Vol. 68 No.
10 (October 1993): Pages 729–731.
45 The act also established a floor and ceiling on per-resident funding of 70 percent and 140 percent of the national average
per resident. Prior to that point, per-resident funding ranged between approximately $10,000 and $240,000. See: Daniel
Guss, Ann L. Prestipino, and Harry E. Rubash, “Graduate medical education funding: a Massachusetts General Hospital case
study and review,” The Journal of Bone and Joint Surgery Vol. 94 No. 4 (February 2012).
46 Cara S. Lesser, Paul B. Ginsburg, and Kelly J. Devers, “The end of an era: what became of the “managed care revolution” in
2001?,” Health Services Research Vol. 38 (February 2003): Pages 337– 355.
47 Ibid., Pages 337–355.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 15
Figure 6: The “managed-care revolution” in the ‘90s slowed health care spending.
Source: Census Bureau, CMS
The rate of health care consumption growth accelerated, swiftly converging with its pre-managed
care trajectory. Thus, ironically, the effort to accommodate the transition toward tightly managed
HMO care by restricting the entry of physicians into the profession had instead helped to facilitate
its unraveling.
By this time, the balance of power in the residency pipeline had shifted completely from
residents to hospitals. Hospitals effectively utilized their power as gatekeepers into the supply-
constrained profession, resulting in sluggish resident wage growth despite the long hours. Growing
dissatisfaction among residents resulted in organized action against the institutions governing entry
into the profession. Opposition among medical students to the National Resident Matching Program’s
algorithm led to its design being shifted from program-optimal to applicant-optimal in 1997. In 2002,
an antitrust lawsuit was filed alleging anti-competitive collusion between the ACGME, The Match, and
various medical associations.48 Congress responded by passing a law in 2002 exempting matching
programs from antitrust action, but still, the message had been received.49 In 2003, ACGME instituted
new duty-hour restrictions on residents. Under the new rule, the hours of clinical and educational
activity conducted by medical residents would be capped at 80 hours per week, with specialty boards
able to petition for an additional 8 hours.50
While Medicare GME cutbacks continued into the middle of the decade, the perceived wisdom
on physician supply had begun to evolve. By the early 2000s, awareness began to grow that prior
48 Jack R. Bierig, “Jung v. Association Of American Medical Colleges: the lawsuit challenging our system of graduate medical
education,” Journal of the American College of Radiology Vol. 1 Issue 1 (January 2004): Pages 40–47.
49 Richard Weinmeyer, “Challenging the Medical Residency Matching System through Antitrust Litigation,” AMA Journal of
Ethics Vol. 17 No. 2 (February 2015); Pages 147–151.
50 Patient Safety Network, “Duty Hours and Patient Safety,” September 7, 2019.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 16
projections of physician surpluses were misguided.51 In 2005, the Association of American Medical
Colleges began to sound the alarm of an impending “physician shortage,” calling for a 10 percent
expansion in medical school enrollment and raising the recommendation to 30 percent the following
year.52 After two and half decades, the moratorium on allopathic medical enrollment was effectively
lifted, resulting in substantial growth in the number of medical school graduates each year.
The various physician associations that had supported and lobbied on behalf of Medicare’s cap
on graduate medical education slots, such as the American Medical Association (AMA), began to
gradually flip their position on the topic.53 And by 2009, legislation to repeal the cap on Medicare
GME was introduced in Congress; now with the support of the organizations that had originally
supported the cap.54
Federal policy gradually became more accommodative of GME funding. The Affordable Care Act
established the Teaching Health Center Graduate Medical Education program in order to increase
funding for primary care training programs operating in community-based ambulatory settings. Like
the children’s hospital GME funding program before it, the new program’s impetus responded to
biases in Medicare’s GME funding, which had provided an indirect-medical-expense adjustment solely
for hospital inpatient care. Yet over the intervening years, the share of care provided in outpatient
settings had increased considerably.
The most recent change came with the enactment of the Consolidated Appropriations Act of 2021,
which added 1,000 new Medicare GME slots, distributed over the upcoming years, with 40 percent
reserved for hospitals meeting certain criteria, such as being in a rural area. The law also made various
minor fixes, such as allowing hospitals that had inadvertently established a low reimbursement rate
for residency training to have another shot. But as discussed next, these incremental changes fall far
short of what is needed to solve our physician shortage.
Quantifying the Residency Bottleneck
The United States’ dearth of physicians per capita relative to peer countries is not because of lower
interest, less capable citizens, or less generous remuneration. The United States has fewer physicians
because of the remarkable degree to which its physician pipeline filters out entrants into the
profession. While medical schools are once again admitting more graduates, the extent to which they
can do so is ultimately constrained by the supply of residencies.
Medical residencies are an odd institution from an economic standpoint due to the manner in
which they blur the line between education and employment. On the one hand, a residency forms
51 Richard A. Cooper, “There’s a Shortage of Specialists: Is Anyone Listening?,” Academic Medicine : Journal of the Association
of American Medical Colleges Vol. 77 No. 8 (August 2002); Pages 761–766.
52 Da’Shia Davis, Michael Dill, Projected Shortage of Physicians through 2030, AAMC Workforce Studies Data Snapshot
(United States: Association of American Medical Colleges, May 2018).
53 James E. Dalen, “The Moratorium on US Medical School Enrollment, from 1980 to 2005: What Were We Thinking?,” The
American Journal of Medicine Vol. 121 No. 2 (February 2008): Pages e1–e2.
54 Kevin B. O’Reilly, “Federal funding for Medicaid program should not be capped: AMA,” American Medical Association, June
16, 2017.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 17
a crucial step in a physician’s professional education. Residency programs allow medical graduates
to gain valuable hands-on experience that isn’t sufficiently imparted during medical school in a
supervised fashion. Residents also take part in significant amounts of classroom learning, particularly
during the initial year. Much as in university, this includes a specified curriculum and performance
evaluations watched over by full-time program administrators, as stipulated by the ACGME and its
affiliated RRCs. These requirements place substantial financial demands on teaching institutions,
both in terms of the direct expenditures and the opportunity costs imposed on teaching physicians
who could otherwise be providing additional services.
Yet unlike other teaching institutions, teaching hospitals pay residents, rather than the other way
around. At the most basic level, a resident exchanges their labor for the educational experience and
pathway to eventual licensure provided by the hospital, on top of any financial compensation. In
return, residents contribute substantial hours of labor to the hospital and are paid relatively modestly
compared to their enormous prior investment in education.
If the marginal resident’s direct labor contribution isn’t sufficient to motivate the creation of
an additional slot, then that slot won’t be created. As a result, the number of aspiring physicians
who are capable of entering and subsequently completing a residency is ultimately determined
by the financial costs and benefits of such programs at individual teaching hospitals. And despite
the earnings premium on attaining physician licensure being so great that many would take out a
student loan in order to obtain a residency placement, this opportunity to internalize the educational
costs of residency training in order to eventually reap the benefits does not presently exist – nothing
analogous to student loans exists for financing one’s residency training. Instead, if the costs of an
additional residency slot exceed the benefits, hospitals will not add the residency unless subsidized
by third-party payers to do so, such as through Medicare.
At least a year of residency training is required for physician licensure in all 50 states and in the
District of Columbia. If newly minted MDs cannot get that training, they are effectively locked out
of the profession they have spent years preparing for. Data released by The Match illustrate this
bottleneck and how it has tightened over time.55 The figures below attempt to accurately capture the
outlook across time for an American medical school graduate in terms of the graduate entering the
profession, adjusting for both the changing composition of medical graduates as well as isolating the
outcomes for U.S. citizens. Correcting for this involves grouping allopathic and osteopathic graduates
as well as creating a separate measure that also includes Americans who attend medical school
abroad. A more detailed description of these choices is available in Appendix 1.
When looked at in terms of raw numbers, we can see that thousands of U.S. medical school graduates
remain unmatched each year. Yet even properly categorizing residency applicants to account for the
changing composition of medical school degrees still results in a picture of the residency pipeline that
is likely too rosy. The Match only includes “active applicants,” a metric that omits certain applicants
who either dropped out or didn’t get a single interview offer. Most of the applicants who dropped
out likely received a match through minor matching services, such as the independent and highly
55 Also known as the National Resident Matching Program. See the appendix for an explanation of the author’s calculations.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 18
Figure 7: Thousands of U.S. medical school graduates go unmatched each year.
Source: Author’s calculations using data from the National Resident Matching Program.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 19
competitive Urology Match or Military Match. However, the omission of applicants who didn’t receive
an interview leads to a meaningful overstatement of medical school graduates’ career prospects.
Estimates accounting for this suggest that The Match overstates applicant success rates by half a
percent for allopathic degree holders, 2 percent for osteopathic degree holders, and a whopping 13
percent for U.S. citizen holders of degrees from foreign medical schools.56
The residency bottleneck for entry into the physician profession results in an enormous waste of
persons and talent. Though unmatched applicants can reapply, residency applications are expensive
and those applying after their senior year of medical school face tough odds to succeed. Those medical
graduates who fail to obtain a residency placement generally find they lack a smooth path toward a
career that will allow them to apply their clinical skill in a manner commensurate with their training
and education. Despite four years of postgraduate education, including two years in clinical settings,
unmatched medical graduates cannot simply become a physician assistant (PA) or nurse practitioner
(NP) without first going back to school. Yet that’s exactly what many unmatched medical graduates
do, obtaining three more years of education, including one year of clinical experience, to become an
NP or PA.57 Others pursue certifications in various technician roles or seek employment as liaisons or
analysts for the medical device industry or pharmaceutical industry.
The status quo results in tragedy on a personal level as well. Even putting aside the cost of
pursuing additional training, failure to ultimately obtain a physician’s income after slogging through
all the intermediate steps up to residency placement can be financially crippling.58 The median
medical school debt upon graduation is over $200,000, according to the Association of American
Medical Colleges, excluding any debt accumulated in pursuit of the preceding bachelor’s degree.59
And that’s on top of what generally amounts to tens of thousands of dollars spent on licensing exams,
residency application fees, traveling for residency interviews, and other physician pipeline-related
expenses. Many unmatched graduates end up with burdensome monthly interest payments and face
a high risk of default.60
This state of affairs is not normal. Neighboring Canada is instructive here, owing to the similarity
of its physician training pipeline. It utilizes both its own matching system for residencies and a
dual undergraduate-plus-medical-degree educational track for entry into the residency system.
Canada also followed the U.S. lead in pursuing policies aimed at reducing the physician supply, such
as freezing medical school enrollment.61 Yet when Canada reversed course, once again pursuing
expansion of its physician workforce, the residency system did not prove to be the same bottleneck
that it has in the United States. The match rate for Canadian graduates is 97 percent, surpassing even
56 Bryan Carmody, “What’s the Real Match Rate,” The Sheriff of Sodium, December 5, 2019.
57 Melissa Bailey, “After Earning an MD, She’s Headed Back to School — to Become a Nurse,” Stat News, November 28, 2016.
58 Emma Goldberg, “‘I Am Worth It’: Why Thousands of Doctors in America Can’t Get a Job,” New York Times, February 19, 2021.
59 James Youngclaus and Julie A. Fresne, 2012 Update, Physician Education Debt and the Cost to Attend Medical School,
(Washington D.C.: Association of American Medical Colleges, February 2013).
60 Emma Goldberg, “‘I Am Worth It’: Why Thousands of Doctors in America Can’t Get a Job,” New York Times, February 19, 2021.
61 Benjamin T.B. Chan, From Perceived Surplus to Perceived Shortage: What Happened to Canada’s Physician Workforce in the
1990s?, Canadian Institute for Health Information (Ottawa: Canadian Institute for Health Information, June 2002).
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 20
the 93 percent success rate for the elite subset of U.S. allopathic graduates in The Match.62
Looking beyond North America, the strangeness of the U.S. practice of locking thousands of
medical graduates out of the profession each year is even more apparent. Access to some form of
postgraduate training for medical school graduates essentially operates as something close to an
entitlement throughout most of Europe. So long as an individual is able to pass their respective
country’s licensing exam, they can be confident that their investment in medical school won’t be
wasted.
Our broken, convoluted system of GME financing
The primary reason why the American residency system is so dysfunctional is that it is tilted against
medical graduates. In contrast to when the residency system was in its infancy and hospitals competed
for medical graduates, today, medical graduates compete for hospitals. The implementation of
increasingly stringent program requirements combined with tightening public funding have made
it the case that the training of residents has increasingly become a net cost to hospitals. And, as
discussed in the earlier history section, this reversal in bargaining leverage is a product of intentional
design, an attempt to dissuade Americans from becoming physicians out of the mistaken fear of an
impending “physician surplus.”
The primary goal for reforming the residency system should be to increase the demand for medical
graduates among teaching hospitals. The diminished pay experienced by physicians in teaching
institutions relative to those in private or hospital settings helps to illustrate the perverse dynamics
currently facing the physician training pipeline. A 2017 survey found the average annual salary cut
experienced by physicians in academic settings to be worth $123,000 relative to their counterparts
in non-academic settings.63 This gap would be even larger if the fact that academic facilities are
disproportionately located in higher-cost areas in the American North East were accounted for.
After decades of failing to adequately support physician training, their services are now in such
high demand that expanding one’s precious time on teaching doesn’t make financial sense for most
physicians. The stark imbalance in remuneration between medical services and physician training is
impacting not only residency programs but medical schools as well. And a secondary consequence of
this remuneration gap that’s worth noting is the financial disincentives it imposes on physicians who
would otherwise be interested in pursuing medical research. This reliance of our physician training
and education pipeline upon an altruistic “calling” has created a gap that will require additional
spending to close.
Still, attributing workforce bottlenecks in the residency system solely to insufficient funding levels
fails to take seriously the structural deficiencies in the current financing arrangement. Indeed, despite
cutbacks to federal funding enacted in the 1980s and 1990s, many residency programs remain
62 John Gallinger, Michel Ouellette, Eric Peters, Lisa Turriff, “CaRMS at 50: Making the match for medical education,” Canadian
Medical Education Journal Vol. 11 No. 3 (July 15, 2020): Pages e133–e140.
63 Medical Group Management Association, “MGMA Data Finds Non-Academic Hospital System Physicians Earn As Much As
$123,000 More Than Their Academic Counterparts,” CISION PR Newswire, November 29, 2017.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 21
Figure 8: Public sources of GME funding
Sources: See Appendix 2
well-funded, with the subsidies for some bordering on lavish. In 2018, the public subsidies for GME
totaled approximately $21 billion across all federal programs and Medicaid.64 Spending for that year
worked out at almost $150,000 for each of the approximately 140,000 residents and fellows.65 The
current overall amount of public spending likely isn’t too far short of what would be needed to put
the residency system on a substantially better footing — however, the current organization of GME
financing is just too poorly structured for doing so effectively.
Over two-thirds of GME subsidies are delivered through Medicare. However, this funding stream
has substantial problems. For instance, hospital subsidies are scaled based upon a hospital’s Medicare
patient load. This design choice is a product of the false assumption at the time that all insurers
would contribute their fair share of funding. As a result, the overwhelming alignment of GME funding
with the elderly Medicare population creates funding biases, not only in geographic terms, but also
in terms of the specialty mix. And yet a more appropriate alignment of funds around a nationally
unrepresentative patient load is merely the tip of the iceberg.
The most straightforward source of federal support for GME is Medicare’s Direct Graduate
Medical Education (DME). It’s a total mess though, based largely upon fossilized funding formulas
and levels derived from Medicare’s cost-based reimbursement system from roughly 40 years ago.
For most facilities, the reimbursement per resident was carried over from Medicare’s cost-based
reimbursement system when it was retired. Due to changes in the relative cost of living across
64 See Appendix 2 for a detailed breakdown.
65 ACGME News, “ACGME Releases 2018-2019 Statistics on Graduate Medical Education Programs and Resident Physicians,”
Accreditation Council for Graduate Medical Education, September 30, 2019.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 22
Figure 9: The structure of public financing for medical residency programs
the country over the last 40 years and the fact that the originally established values were often
subject to limited oversight, the present subsidies bear only a hazy resemblance to the costs a given
facility faces today. Reimbursement based on the reported costs is sort of a silly exercise because the
expenditures reported on paper can easily bear no resemblance to the actual economic incidence
of GME funding support being described. And this is particularly true when teaching institutions
face a minimal threat of having their prospective medical residents (and associated federal funding)
migrate elsewhere, as is often the case due to the cap on Medicare-funded slots.
The largest channel through which Medicare funds residencies is actually indirect medical
education (IME). IME works by magnifying reimbursements to hospitals made through Medicare’s
Prospective Payment System (PPS), which operates on predetermined prices based on a patient’s
medical diagnosis. Within IME, there are two separate funding streams: operating and capital. These
are based upon the ratio of residents to hospital beds and to the average daily number of patients,
respectively — a difference that’s largely an artifact of the staggered transition from cost-based
reimbursement to the PPS in the 1980s, with the designers deciding that an adjustment based upon
patients was actually superior by the time the capital PPS was rolled out.66 Indeed, the IME operating
adjustment, which uses the ratio between residents and beds, is essentially no longer functioning
as originally intended due to a hospital-specific cap on IME payments instituted in 1997 as part
of the Balanced Budget Act of that year. Hospitals that reduce beds or add interns no longer gain
any additional payment, thus rendering the payment adjustment that hospitals receive today fairly
arbitrary.
66 Comptroller General of the United States, Flawed Data Add Millions to Teaching Hospital Payments, Report GAO/IMTEC-
91-31 (Washington: U.S. General Accounting Office; Jun, 1991).
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 23
Figure 10: Medicare residency funding is highly concentrated in the Northeast.
Source: ACGME; CMS; author’s calculations.
The caps imposed in 1997 largely froze in place the facilities eligible to receive Medicare GME
funding. However, the resulting reimbursement disparities are far beyond what can be defended
based on inherent or necessary cost differentials between teaching hospitals. Medicare will add 1,000
funded slots, which will be distributed over five years starting in 2023 under the 2021 Consolidated
Appropriations Act.67 Even putting aside the direct limitations on funding imposed by the cap, the
existing system does a poor job of facilitating the creation of new residency programs for other
reasons. Funded slots through Medicare are sometimes made available through reallocation as
facilities close down.68 Establishing a residency program involves significant fixed costs and there’s
67 McDermot+ Consulting, “Summary of Key Health Provisions in the Consolidated Appropriations Act, 2021,” December 31,
2020.
68 Though nearby hospitals are prioritized when this occurs.
NISKANEN CENTERUnmatched: Repairing the U.S. Medical Residency Pipeline September 2021 | 24
Figure 11: Medical residencies are heavily concentrated in the Northeast.
Source: ACGME.
also a significant risk involved in inadvertently establishing an insufficiently generous per-resident
rate of reimbursement. This is because, perversely, Medicare reimbursement rates for residency
programs, in almost all cases, are set over an infinite time horizon with no possibility of revision.
Currently, medical residents are trained disproportionately in low-population-growth, high-cost
states and metropolitan areas in the Northeast. These residents are, in turn, expected to disperse
throughout the rest of the country. Considering investments in the residency system from the
standpoint of cost-effectiveness, it makes more sense to do the exact opposite. Owing to differences
in the cost of living, a dollar spent to train a medical resident in Georgia goes much further than
in New York state, yet New York trains more than 3 times as many medical residents per person as
Georgia.
Another issue with the current allocation is simply the mismatch between residents and the demand
for additional medical services. This is because medical residents implicitly finance a portion of their
NISKANEN CENTERYou can also read