Understanding Atrial Fibrillation/ Atrial Flutter (AF/AFL)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

U N D E R S TA N D I N G A F / A F L
Understanding Atrial Fibrillation/
Atrial Flutter (AF/AFL)
Please see full Prescribing Information, including Boxed Warning,
and Medication Guide beginning on page 7.
Please see Important Safety Information on page 6.
Understanding AF/AFL
In this brochure, you’ll learn about atrial fibrillation (AF) and atrial flutter
(AFL). You’ll also learn about the options you have for treatment.
[What is arrhythmia?]
An arrhythmia is a medical term for an abnormal heartbeat. Your heart
can beat too slow, too fast, or in an unusual pattern. There are many kinds
of arrhythmias. They can happen in any part of the heart. Here, you’ll learn
about 2 kinds of arrhythmias that happen in parts of your heart called the
atria. The first is called atrial fibrillation. The second is called atrial flutter.
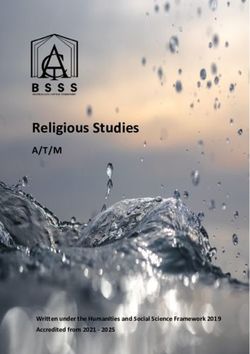
[What are atrial fibrillation and atrial flutter?]
AF and AFL are arrhythmias that happen in parts of your heart called
the atria. Your heart has 4 parts, or “chambers.” The atria are the top 2
chambers. The bottom 2 are called the ventricles. Normally, these chambers
tighten and relax to a regular beat.
Indication
TIKOSYN® (dofetilide) is a medicine for highly symptomatic atrial fibrillation or In AF/AFL, the atria beat very quickly. The beats can be disorganized.
atrial flutter (irregular heartbeats). TIKOSYN may help by converting the irregular The timing of their beat with the ventricles can be off, too.
heartbeats to normal rhythm. It may also help by keeping the normal rhythm for a
longer period of time. It has not been shown to work on certain types of irregular
heartbeats that may come and go on their own. Top Chambers Disorganized
Right Left Signals
Warning Atrium Atrium
To decrease the chance of your getting a different type of dangerous
Left
abnormal heartbeat, TIKOSYN treatment must be started or re-started Right Ventricle
Ventricle
while you are in the hospital. The doctor who prescribed TIKOSYN and
the hospital must have gone through special TIKOSYN training. Feeling
faint, dizziness/lightheadedness, or having fast heartbeats are symptoms Bottom Chambers
of this abnormal heartbeat. Call your doctor or emergency room as soon
as possible if you have any of these symptoms. Chambers of your heart Disorganized and rapid signals in AF
While in the hospital, your kidney function and heart rhythm will be monitored
for a minimum of 3 days. This helps the doctor to choose the right
TIKOSYN dose for you. Only doctors who have gone through TIKOSYN
training will be able to prescribe or refill your TIKOSYN prescription.
Please see full Prescribing Information, including Boxed Warning,
and Medication Guide beginning on page 7.
Please see additional Important Safety Information on page 6.
2
Understanding AF/AFL
[What are the signs of atrial fibrillation and atrial flutter?] [What are the risks of atrial fibrillation and atrial flutter?]
Some of the symptoms you might feel are: In AF/AFL, your heart doesn’t pump blood as well as normal. Blood carries
■ Irregular and rapid pulse ■ Tiring more easily, especially oxygen to your cells. So in AF/AFL, your cells don’t get as much oxygen. This
when exercising can make you feel tired. Also, when your heart doesn’t pump normally, you can
■ Heart palpitations have low blood pressure. This can make you pass out.
■ Dizziness, sweating, and chest ■ Fainting
pain or pressure There are other serious conditions AF/AFL can lead to if not treated.
These include:
■ Shortness of breath or anxiety
■ Chronic fatigue—if you’re not getting enough blood, you may feel tired
The symptoms you feel may come and go. Or they may be constant. If you
have any of these symptoms, your doctor can check your heartbeat using an ■ Heart failure—prolonged AF/AFL can weaken the
electrocardiogram, or ECG, recording. heart, making heart failure more likely
■ Stroke—when your heart doesn’t pump blood normally,
[What are the causes of atrial fibrillation and atrial flutter?] blood can pool in your heart. This can cause clots to form.
If these clots travel to the brain or the lungs, they can stop
Doctors are not quite sure what causes AF/AFL. However, there are the flow of blood. This can cause a stroke in the brain.
some conditions that might make them more likely. These include: This can also lead to a blood clot stuck in the lungs
AF/AFL: (pulmonary embolism). Either of these may lead to death
■ Heart disease, such as ■ Serious illness
congestive heart failure, ■ Chronic lung disease
coronary artery disease,
■ Diabetes
and structural heart disease Selected Safety Information
■ Drinking too much alcohol
■ Thyroid disease Do not take TIKOSYN® (dofetilide) if you have congenital or acquired long QT
syndrome (a disorder of the heartbeat which may be present from birth, or it
AF only: may be acquired as a result of certain medical conditions or from taking certain
■ Older than 60 years of age ■ Infection medications. People with long QT syndrome may have symptoms including an
unusually rapid heartbeat, fainting, and seizures. Sudden cardiac death may also
result from long QT syndrome); have serious kidney problems or are on kidney
dialysis; or are allergic to dofetilide or other ingredients in TIKOSYN.
Please see full Prescribing Information, including Boxed Warning,
and Medication Guide beginning on page 7. Please see additional Important Safety Information on page 6.
3Understanding AF/AFL
[Types of treatment]
Treating underlying conditions and changing lifestyle habits Restoring the rhythm
Before your treatment, your doctor might ask you questions about your With AF/AFL, your doctor may attempt to restore your heartbeat to a
medical history and lifestyle. There might be a disease or habit causing regular and controlled rhythm. This is called normal sinus rhythm.
your AF/AFL. If the disease is treated or the habit changed, the The process of restoring rhythm is called cardioversion. Cardioversion
arrhythmia may go away. can happen in 2 ways:
Preventing stroke ■ Rhythm control medicines
No matter what treatment you receive, you’ll probably also take ■ Direct-current cardioversion—when electricity is applied directly to the heart
anticoagulants or antiplatelets, which help prevent blood clots. This is
Maintaining the rhythm
to reduce your risk of stroke.
After cardioversion, your doctor may prescribe drugs. These help maintain
Treating arrhythmia your normal rhythm. There are several drugs for doing this. The drug you are
Depending on your symptoms, your doctor will discuss your treatment prescribed will depend on what kind of arrhythmia you have. It will also depend
options with you. There are 2 main types of treatment with medicines. on the other conditions you have and the possible side effects of the drug. If the
They are: first drug doesn’t work, your doctor might consider a different medicine. Your
doctor may also try a different approach to treatment.
■ Rhythm control—using drugs to help your heart beat at a
normal rhythm Rate control
■ Rate control—using drugs to control the rate of your heart Depending on your condition, your doctor may use rate-controlling drugs to
Your doctor may also consider certain procedures to restore normal control the rate of your heart. Your doctor may consider cardioversion before
rhythm to your heart. starting these drugs. There are many kinds of medicines that can be used for rate
control. Your doctor may also combine agents in order to increase their effect.
■ Surgical procedures—electrical signals in your heart are
The type of drug you’re prescribed will depend on your symptoms, the kind of
redirected using surgery
AF/AFL, and any other conditions you have.
■ Catheter ablation—a catheter is used to reach the heart and
create scars with radio waves
There are a number of reasons your doctor may choose one treatment Selected Safety Information
over another. Your doctor will consider: Do not take TIKOSYN® (dofetilide) if are taking certain other medicines, including
cimetidine (Tagamet®, Tagamet HB®), verapamil (Calan®, Calan SR®, Covera-HS®,
■ Your medical history Isoptin®, Isoptin SR®, Verelan®, Verelan PM®), ketoconazole (Nizoral®),
■ Your type of arrhythmia trimethoprim alone (Proloprim®, Trimpex®), the combination of trimethoprim
and sulfamethoxazole (Bactrim®, Septra®), prochlorperazine (Compazine®),
■ Other conditions you might have megestrol (Megace®), dolutegravir (Tivicay®) or hydrochlorothiazide alone or
Then your doctor will determine which treatment is right for you. in combination with other medicines (such as Esidrix®, Ezide®, Hydrodiuril®,
Hydro-Par®, Microzide®, or Oretic®).
Listed trademarks are the property of their respective owners.
Please see full Prescribing Information, including Boxed Warning,
and Medication Guide beginning on page 7. Please see additional Important Safety Information on page 6.
4Understanding AF/AFL
[Types of treatment] (cont’d) [More information]
Procedures To learn more about AF, AFL, arrhythmias, or
AF/AFL can sometimes be treated with certain procedures. One type, done heart disease, contact these groups:
using surgery, is called the “maze” procedure:
■ The electrical signals in your heart are slowed by a “maze” American Heart
■ This “maze” is created through small cuts. These cuts are stitched Association
up and allowed to scar over 7272 Greenville Ave
■ The scars redirect electrical signals, slowing them down Dallas, TX 75231
Your doctor may also consider catheter ablation. There are a few steps (800) AHA-USA-1
in this process: www.heart.org
■ A catheter is used to reach the heart to block and correct
electrical signals
CardioSmart
■ Radio waves are sent through the catheter
■ These waves create small scars in specific places on heart tissue Resource Center
American College
■ This blocks electrical signals to help ensure they travel the right way of Cardiology
Catheter ablation can be used in 2 ways: 2400 N Street NW
Washington, DC 20037
■ “Hot spot” ablation—scars are made on areas along the vein that www.cardiosmart.org
carries blood to your lungs
■ Atrioventricular (AV) node ablation—the AV node sends electrical
signals from the atria to the ventricles. In AV node ablation, scars Heart Rhythm Society
are made on the node. A pacemaker, a device used to control your 1400 K Street NW
heartbeat, may then be inserted Suite 500
Washington, DC 20005
(202) 464-3400
www.hrsonline.org
Selected Safety Information
The most common side effects of TIKOSYN® (dofetilide) are headache, chest pain,
and dizziness. TIKOSYN can also cause other side effects. If you are concerned
about these or any other side effects, ask your doctor.
Please see full Prescribing Information, including Boxed Warning,
and Medication Guide beginning on page 7. Please see additional Important Safety Information on page 6.
5Indication TIKOSYN® (dofetilide) is a medicine for highly symptomatic atrial fibrillation or atrial flutter (irregular heartbeats). TIKOSYN may help by converting the irregular heartbeats to normal rhythm. It may also help by keeping the normal rhythm for a longer period of time. It has not been shown to work on certain types of irregular heartbeats that may come and go on their own. Important Safety Information To decrease the chance of your getting a different type of dangerous abnormal heartbeat, TIKOSYN treatment must be started or re-started while you are in the hospital. The doctor who prescribed TIKOSYN and the hospital must have gone through special TIKOSYN training. Feeling faint, dizziness/lightheadedness, or having fast heartbeats are symptoms of this abnormal heartbeat. Call your doctor or emergency room as soon as possible if you have any of these symptoms. While in the hospital, your kidney function and heart rhythm will be monitored for a minimum of 3 days. This helps the doctor to choose the right TIKOSYN dose for you. Only doctors who have gone through TIKOSYN training will be able to prescribe or refill your TIKOSYN prescription. Do not take TIKOSYN if you have congenital or acquired long QT syndrome (a disorder of the heartbeat which may be present from birth, or it may be acquired as a result of certain medical conditions or from taking certain medications. People with long QT syndrome may have symptoms including an unusually rapid heartbeat, fainting, and seizures. Sudden cardiac death may also result from long QT syndrome); have serious kidney problems or are on kidney dialysis; are taking certain other medicines, including cimetidine (Tagamet®, Tagamet HB®), verapamil (Calan®, Calan SR®, Covera-HS®, Isoptin®, Isoptin SR®, Verelan®, Verelan PM®), ketoconazole (Nizoral®), trimethoprim alone (Proloprim®, Trimpex®), the combination of trimethoprim and sulfamethoxazole (Bactrim®, Septra®), prochlorperazine (Compazine®), megestrol (Megace®), dolutegravir (Tivicay®) or hydrochlorothiazide alone or in combination with other medicines (such as Esidrix®, Ezide®, Hydrodiuril®, Hydro-Par®, Microzide®, or Oretic®); or are allergic to dofetilide or other ingredients in TIKOSYN. The most common side effects of TIKOSYN are headache, chest pain, and dizziness. TIKOSYN can also cause other side effects. If you are concerned about these or any other side effects, ask your doctor. Listed trademarks are the property of their respective owners. You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch, or call 1-800-FDA-1088. Please see full Prescribing Information, including Boxed Warning, and Medication Guide beginning on page 7. For more information, please visit www.TIKOSYN.com. TKU630009-01 © 2014 Pfizer Inc. All rights reserved. January 2014
(e.g.,
(e.g.,IKs
IKs
, I, K1
IK1).).AtAtclinically
clinicallyrelevant
relevantconcentrations,
concentrations,dofetilide
dofetilidehas
hasnonoeffect
effectononsodium
sodiumchannels
channels
TIKOSYN®®
TIKOSYN (associated
(associatedwith withClass
ClassI Ieffect),
effect),adrenergic
adrenergicalpha-receptors,
alpha-receptors,ororadrenergic
adrenergicbeta-receptors.
beta-receptors.
(dofetilide)
(dofetilide) Electrophysiology
Electrophysiology
TIKOSYN
TIKOSYN(dofetilide)
(dofetilide)increases
increasesthe
themonophasic
monophasicactionactionpotential
potentialduration
durationinina apredictable,
predictable,
Capsules
Capsules
concentration-dependent
concentration-dependentmanner, manner,primarily
primarilydue
duetotodelayed
delayedrepolarization.
repolarization.This
Thiseffect,
effect,and
andthe
the
related
relatedincrease
increaseinineffective
effectiverefractory
refractoryperiod,
period,isisobserved
observedininthetheatria
atriaand
andventricles
ventriclesininboth
both
resting
restingand
andpaced
pacedelectrophysiology
electrophysiologystudies.
studies.The
Theincrease
increaseininQTQTinterval
intervalobserved
observedononthe thesurface
surface
ToTominimize
minimizethetherisk
riskofofinduced
inducedarrhythmia,
arrhythmia,patients
patientsinitiated
initiatedororre-initiated
re-initiatedononTIKOSYN
TIKOSYN
ECG
ECGisisa aresult
resultofofprolongation
prolongationofofboth
botheffective
effectiveandandfunctional
functionalrefractory
refractoryperiods
periodsininthe
theHis-
His-
should
shouldbebeplaced
placedforfora aminimum
minimumofof33daysdaysinina afacility
facilitythat
thatcan
canprovide
providecalculations
calculationsofofcreatinine
creatinine
Purkinje
Purkinjesystem
systemand andthe
theventricles.
ventricles.
clearance,continuous
clearance, continuouselectrocardiographic
electrocardiographicmonitoring,
monitoring,and andcardiac
cardiacresuscitation.
resuscitation.For
Fordetailed
detailed
instructions
instructionsregarding
regardingdose doseselection, seeDOSAGE
selection,see DOSAGEAND ANDADMINISTRATION.
ADMINISTRATION.TIKOSYN TIKOSYNisis
Dofetilide
Dofetilidediddidnot
notinfluence
influencecardiac
cardiacconduction
conductionvelocity
velocityand
andsinus
sinusnode
nodefunction
functioninina avariety
varietyofof
availableonly
available onlytotohospitals
hospitalsandandprescribers
prescriberswhowhohavehavereceived
receivedappropriate
appropriateTIKOSYN
TIKOSYNdosing dosingand
and
studies
studiesininpatients
patientswith
withororwithout
withoutstructural
structuralheart
heartdisease.
disease.This
Thisisisconsistent
consistentwith
witha alack
lackofofeffect
effect
treatment
treatmentinitiation
initiationeducation;
education;seeseeDOSAGE
DOSAGEAND ANDADMINISTRATION.
ADMINISTRATION.
ofofdofetilide
dofetilideononthe
thePRPRinterval
intervaland
andQRS
QRSwidth
widthininpatients
patientswith
withpre-existing
pre-existingheart
heartblock
blockand/or
and/or
sick
sicksinus
sinussyndrome.
syndrome.
DESCRIPTION
DESCRIPTION InInpatients,
patients,dofetilide
dofetilideterminates
terminatesinduced
inducedre-entrant
re-entranttachyarrhythmias
tachyarrhythmias(e.g.,
(e.g.,atrial
atrial
fibrillation/flutter
fibrillation/flutterand
andventricular
ventriculartachycardia)
tachycardia)and
andprevents
preventstheir
theirre-induction.
re-induction.TIKOSYN
TIKOSYNdoes does
®®
TIKOSYN
TIKOSYN (dofetilide)
(dofetilide)isisananantiarrhythmic
antiarrhythmicdrug
drugwith
withClass
ClassIIIIII(cardiac
(cardiacaction
actionpotential
potentialduration
duration not
notincrease
increasethetheelectrical
electricalenergy
energyrequired
requiredtotoconvert
convertelectrically
electricallyinduced
inducedventricular
ventricularfibrillation,
fibrillation,
prolonging)
prolonging)properties.
properties.ItsItsempirical
empiricalformula
formulaisisCC HH
1919 NN
2727 3O
3O5S
5S2 2and
anditithas
hasa amolecular
molecularweight
weightofof and
andititsignificantly
significantlyreduces
reducesthethedefibrillation
defibrillationthreshold
thresholdininpatients
patientswith
withventricular
ventriculartachycardia
tachycardia
441.6.
441.6.The
Thestructural
structuralformula
formulaisis and
andventricular
ventricularfibrillation
fibrillationundergoing
undergoingimplantation
implantationofofa acardioverter-defibrillator
cardioverter-defibrillatordevice.
device.
Hemodynamic
HemodynamicEffects Effects
NHSO
NHSOCH
CH
2 2 3 3 InInhemodynamic
hemodynamicstudies,
studies,TIKOSYN
TIKOSYNhad hadnonoeffect
effectononcardiac
cardiacoutput,
output,cardiac
cardiacindex,
index,stroke
stroke
volume
volumeindex,
index,ororsystemic
systemicvascular
vascularresistance
resistanceininpatients
patientswith
withventricular
ventriculartachycardia,
tachycardia,mildmildtoto
NN moderate
moderatecongestive
congestiveheart
heartfailure
failureororangina,
angina,and
andeither
eithernormal
normalororlowlowleft
leftventricular
ventricularejection
ejection
CH
CHSO
SOHN
HN H HC C OO
3 3 2 2 3 3
fraction.
fraction.There
Therewaswasnonoevidence
evidenceofofa anegative
negativeinotropic
inotropiceffect
effectrelated
relatedtotoTIKOSYN
TIKOSYNtherapytherapyinin
patients
patientswith
withatrial
atrialfibrillation.
fibrillation.There
Therewaswasnonoincrease
increaseininheart
heartfailure
failureininpatients
patientswith
withsignificant
significant
The
Thechemical
chemicalname
namefor
fordofetilide
dofetilideis:is: left
leftventricular
ventriculardysfunction
dysfunction(see(seeCLINICAL
CLINICALSTUDIES,STUDIES,Safety SafetyininPatients
PatientswithwithStructural
Structural
N-[4-[2-[methyl[2-[4-[(methylsulfonyl)amino]phenoxy]ethyl]amino]ethyl]phenyl]-
N-[4-[2-[methyl[2-[4-[(methylsulfonyl)amino]phenoxy]ethyl]amino]ethyl]phenyl]- Heart
HeartDisease,
Disease,DIAMOND
DIAMONDStudies).Studies).InInthe
theoverall
overallclinical
clinicalprogram,
program,TIKOSYN
TIKOSYNdid didnotnotaffect
affect
methanesulfonamide.
methanesulfonamide. blood
bloodpressure.
pressure.Heart
Heartrate
ratewas
wasdecreased
decreasedbyby4–64–6bpm
bpmininstudies
studiesininpatients.
patients.
Dofetilide
Dofetilideisisa awhite
whitetotooff-white
off-whitepowder.
powder.ItItisisvery
veryslightly
slightlysoluble
solubleininwater
waterand
andpropan-2-ol
propan-2-olandand Pharmacokinetics,
Pharmacokinetics,General General
isissoluble
solubleinin0.1M
0.1Maqueous
aqueoussodium
sodiumhydroxide,
hydroxide,acetone,
acetone,and
andaqueous
aqueous0.1M0.1Mhydrochloric
hydrochloricacid.
acid. Absorption
Absorptionand Distribution:The
andDistribution: Theoral
oralbioavailability
bioavailabilityofofdofetilide
dofetilideisis>90%,
>90%,with
withmaximal
maximal
plasma
plasmaconcentrations
concentrationsoccurring
occurringatatabout
about2–3
2–3hours
hoursininthe
thefasted
fastedstate.
state.Oral
Oralbioavailability
bioavailabilityisis
TIKOSYN
TIKOSYNcapsules
capsulescontain
containthe
thefollowing
followinginactive
inactiveingredients:
ingredients:microcrystalline
microcrystallinecellulose,
cellulose,corn
corn unaffected
unaffectedbybyfood
foodororantacid.
antacid.The
Theterminal
terminalhalf-life
half-lifeofofTIKOSYN
TIKOSYNisisapproximately
approximately1010hours;
hours;
starch,
starch,colloidal
colloidalsilicon
silicondioxide
dioxideand
andmagnesium
magnesiumstearate.
stearate.TIKOSYN
TIKOSYNisissupplied
suppliedfor
fororal
oral steady
steadystate
stateplasma
plasmaconcentrations
concentrationsare areattained
attainedwithin
within2–3 2–3days,
days,with
withananaccumulation
accumulationindex
indexofof
administration
administrationininthree
threedosage
dosagestrengths:
strengths:125
125mcg
mcg(0.125
(0.125mg)
mg)orange
orangeand
andwhite
whitecapsules,
capsules, 1.5
1.5toto2.0.
2.0.Plasma
Plasmaconcentrations
concentrationsarearedose
doseproportional.
proportional.Plasma
Plasmaprotein
proteinbinding
bindingofofdofetilide
dofetilideisis
250
250mcg
mcg(0.25
(0.25mg)
mg)peach
peachcapsules,
capsules,and
and500
500mcg
mcg(0.5
(0.5mg)
mg)peach
peachand
andwhite
whitecapsules.
capsules. 60–70%,
60–70%,isisindependent
independentofofplasma
plasmaconcentration,
concentration,andandisisunaffected
unaffectedbybyrenal
renalimpairment.
impairment.Volume
Volume
ofofdistribution
distributionisis33L/kg.
L/kg.
CLINICAL
CLINICALPHARMACOLOGY
PHARMACOLOGY
Metabolism
Metabolismand Excretion:Approximately
andExcretion: Approximately80% 80%ofofa asingle
singledose
doseofofdofetilide
dofetilideisisexcreted
excretedinin
Mechanism
MechanismofofActionAction urine,
urine,ofofwhich
whichapproximately
approximately80% 80%isisexcreted
excretedasasunchanged
unchangeddofetilide
dofetilidewith
withthe
theremaining
remaining20%20%
consisting
consistingofofinactive
inactiveororminimally
minimallyactive
activemetabolites.
metabolites.Renal
Renalelimination
eliminationinvolves
involvesbothboth
TIKOSYN
TIKOSYN(dofetilide)
(dofetilide)shows
showsVaughan
VaughanWilliams
WilliamsClass
ClassIIIIIIantiarrhythmic
antiarrhythmicactivity.
activity.The
The
glomerular
glomerularfiltration
filtrationand
andactive
activetubular
tubularsecretion
secretion(via
(viathe
thecation
cationtransport
transportsystem,
system,a aprocess
processthat
that
mechanism
mechanismofofaction
actionisisblockade
blockadeofofthethecardiac
cardiacion
ionchannel
channelcarrying
carryingthe
therapid
rapidcomponent
componentofofthe the
can
canbebeinhibited
inhibitedbybycimetidine,
cimetidine,trimethoprim,
trimethoprim,prochlorperazine,
prochlorperazine,megestrol,
megestrol,ketoconazole
ketoconazoleand and
delayed
delayedrectifier
rectifierpotassium
potassiumcurrent,
current,IKr
IKr
. At
. Atconcentrations
concentrationscovering
coveringseveral
severalorders
ordersofofmagnitude,
magnitude,
dolutegravir).InInvitro
dolutegravir). vitrostudies
studieswith
withhuman
humanliver
livermicrosomes
microsomesshow showthat
thatdofetilide
dofetilidecancanbebe
dofetilide
dofetilideblocks
blocksonly
onlyIKrIKrwith
withnonorelevant
relevantblock
blockofofthe
theother
otherrepolarizing
repolarizingpotassium
potassiumcurrents
currents
metabolized
metabolizedbybyCYP3A4,
CYP3A4,but butitithas
hasa alow
lowaffinity
affinityfor
forthis
thisisoenzyme.
isoenzyme.Metabolites
Metabolitesare areformed
formedbyby
7N-dealkylation
N-dealkylationand
andN-oxidation.
N-oxidation.There
Thereare
arenonoquantifiable
quantifiablemetabolites
metabolitescirculating
circulatingininplasma,
plasma,but
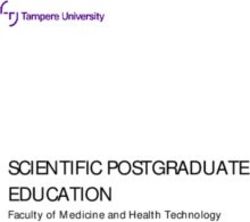
but Figure
Figure1:1:Mean
MeanQTc-Concentration
QTc-ConcentrationRelationship
RelationshipininYoung
YoungVolunteers
VolunteersOver
Over2424Days
Days
55metabolites
metaboliteshave
havebeen
beenidentified
identifiedininurine.
urine. 80
80
Mean Change fromBaseline QTc
Mean Change fromBaseline QTc
DD
ay
ay11
70
70 DD
ay
ay23
23(S
(S
teady
teady
State)
State)
Pharmacokinetics
PharmacokineticsininSpecial SpecialPopulations
Populations
60
60
Renal Impairment:InInvolunteers
RenalImpairment: volunteerswith
withvarying
varyingdegrees
degreesofofrenal
renalimpairment
impairmentand andpatients
patientswith
with
arrhythmias,
arrhythmias,the theclearance
clearanceofofdofetilide
dofetilidedecreases
decreaseswith
withdecreasing
decreasingcreatinine
creatinineclearance.
clearance.As
Asa aresult,
result, 50
50
and
andasasseen
seenininclinical
clinicalstudies,
studies,the
thehalf-life
half-lifeofofdofetilide
dofetilideisislonger
longerininpatients
patientswith
withlower
lowercreatinine
creatinine
(msec)
(msec)
40
40
clearances.Because
clearances. Becauseincrease
increaseininQTQTinterval
intervaland andthe
therisk
riskofofventricular
ventriculararrhythmias
arrhythmiasare are 30
30
directly
directlyrelated
relatedtotoplasma
plasmaconcentrations
concentrationsofofdofetilide,
dofetilide,dosage
dosageadjustment
adjustmentbased
basedon on
20
20
calculated
calculatedcreatinine
creatinineclearance
clearanceisiscritically
criticallyimportant
important(see (seeDOSAGE
DOSAGEAND AND
ADMINISTRATION).
ADMINISTRATION).Patients Patientswith
withsevere
severerenal
renalimpairment
impairment(creatinine
(creatinineclearance
clearance1week
weekduration.
duration.As Asshown,
shown,both boththe
theprobability
probabilityofofa apatient’s
patient’sremaining
remainingininsinussinusrhythm
rhythmatat
Women:AApopulation
Women: populationpharmacokinetic
pharmacokineticanalysis
analysisshowed
showedthat
thatwomen
womenhave
haveapproximately
approximately12– 12– six
sixmonths
monthsandandthe
thechange
changeininQTcQTcfromfrombaseline
baselineatatsteady
steadystate
stateofofdosing
dosingincreased
increasedininanan
18%
18%lower
lowerdofetilide
dofetilideoral
oralclearances
clearancesthan
thanmen
men(14–22%
(14–22%greater
greaterplasma
plasmadofetilide
dofetilidelevels),
levels),after
after approximately
approximatelylinear
linearfashion
fashionwithwithincreasing
increasingdose
doseofofTIKOSYN.
TIKOSYN.Note Notethat
thatininthese
thesestudies,
studies,doses
doses
correction
correctionfor
forweight
weightand
andcreatinine
creatinineclearance.
clearance.InInfemales,
females,asasininmales,
males,renal
renalfunction
functionwas
wasthethe were
weremodified
modifiedbybyresults
resultsofofcreatinine
creatinineclearance
clearancemeasurement
measurementand andin-hospital
in-hospitalQTc QTcprolongation.
prolongation.
single
singlemost
mostimportant
importantfactor
factorinfluencing
influencingdofetilide
dofetilideclearance.
clearance.InInnormal
normalfemale
femalevolunteers,
volunteers,
hormone
hormonereplacement
replacementtherapy
therapy(a(acombination
combinationofofconjugated
conjugatedestrogens
estrogensandandmedroxyprogesterone)
medroxyprogesterone)
did
didnot
notincrease
increasedofetilide
dofetilideexposure.
exposure.
Drug-Drug
Drug-DrugInteractions
Interactions(see
(seePRECAUTIONS)
PRECAUTIONS)
Dose-Response
Dose-Responseand andConcentration
ConcentrationResponseResponsefor forIncrease
IncreaseininQT QTInterval
Interval
Increase
IncreaseininQTQTinterval
intervalisisdirectly
directlyrelated
relatedtotodofetilide
dofetilidedose
doseand
andplasma
plasmaconcentration.
concentration.Figure
Figure11
shows
showsthat
thatthe
therelationship
relationshipininnormal
normalvolunteers
volunteersbetween
betweendofetilide
dofetilideplasma
plasmaconcentrations
concentrationsand and
change
changeininQTc
QTcisislinear,
linear,with
witha apositive
positiveslope
slopeofofapproximately
approximately15–25
15–25msec/(ng/mL)
msec/(ng/mL)afterafterthe
the
first
firstdose
doseand
andapproximately
approximately10–15 10–15msec/(ng/mL)
msec/(ng/mL)atatDay Day2323(reflecting
(reflectinga asteady
steadystate
stateofofdosing).
dosing).
AAlinear
linearrelationship
relationshipbetween
betweenmean meanQTc
QTcincrease
increaseandanddofetilide
dofetilidedose
dosewaswasalso
alsoseen
seenininpatients
patients
with
withrenal
renalimpairment,
impairment,ininpatients
patientswith
withischemic
ischemicheart
heartdisease,
disease,and
andininpatients
patientswith
with
supraventricular
supraventricularand andventricular
ventriculararrhythmias.
arrhythmias.
8Figure
Figure2:2:Relationship
RelationshipBetween
BetweenTIKOSYN
TIKOSYNDose,
Dose,QTc
QTcIncrease
Increaseand
andMaintenance
MaintenanceofofNSR
NSR concomitant
concomitanttherapy,
therapy,including
includingdigoxin
digoxin(over
(over60%),
60%),diuretics
diuretics(over
(over20%),
20%),and
andACE
ACEinhibitors
inhibitors
(over
(over30%).
30%).About
About90%
90%were
wereononanticoagulants.
anticoagulants.
35
35 100
100
QQ
Tc
Tc(95%
(95%
CCI)I)== Acute
Acuteconversion
conversionrates
ratesare
areshown
shownininTable
Table11for
forrandomized
randomizeddoses
doses(doses
(doseswere
wereadjusted
adjustedfor
for
30
30
calculated
calculatedcreatinine
creatinineclearance
clearanceand,
and,ininStudy
Study1,1,for
forQT
QTinterval
intervalororQTc).
QTc).Of
Ofpatients
patientswho
who
PP
robability
robabilityofofNN
SS
RR(95%
(95%
CCI)I)==
25
25 converted
convertedpharmacologically,
pharmacologically,approximately
approximately70% 70%converted
convertedwithin
within24–36
24–36hours.
hours.
QTc Change fromBaseline
QTc Change fromBaseline
Probability of Remaining in NSR
) in NSR
75
75
at Steady State (msec)
at Steady State (msec)
20
20
Table
Table1:1:Conversion
ConversionofofAtrial
AtrialFibrillation/Flutter
Fibrillation/FluttertotoNormal
NormalSinus
SinusRhythm
Rhythm
s (%g
at 6 months (%)
nthainin
15
15
50
50 TIKOSYN
TIKOSYNDoseDose
oem
10
10 125
125mcg
mcg 250
250mcg
mcg 500
500mcg
mcg Placebo
Placebo
R
BID
BID BID
BID BID
BID
ofm
55
at 6
Study1 1
Study 5/82(6%)
5/82(6%) 8/82(10%)
8/82(10%) 23/77(30%)
23/77(30%) 1/84(1%)
1/84(1%)
Probability
25
25 Study2 2
Study 8/135(6%)
8/135(6%) 14/133(11%)
14/133(11%) 38/129(29%)
38/129(29%) 2/137(1%)
2/137(1%)
00
-5-5
Patients
Patientswho
whodid
didnot
notconvert
converttotoNSR
NSRwithwithrandomized
randomizedtherapy
therapywithin
within48–72
48–72hours
hourshad
hadelectrical
electrical
-10
-10 00 cardioversion.
cardioversion.Those
Thosepatients
patientsremaining
remainingininNSR NSRafter
afterconversion
conversionininhospital
hospitalwere
werecontinued
continuedonon
Placebo
Placebo
DD
ofetilid
ofetilid
ee DD
ofetilid
ofetilid
ee DD
ofetilide
ofetilide randomized
randomizedtherapy
therapyasasoutpatients
outpatients(maintenance
(maintenanceperiod)
period)for forupuptotoone
oneyear
yearunless
unlessthey
they
125m
125m
cg
cgBB
ID
ID 250m
250m
cg
cgBB
ID
ID 500m
500m
cg
cgBB
ID
ID experienced
experienceda arecurrence
recurrenceofofatrial
atrialfibrillation/atrial
fibrillation/atrialflutter
flutterororwithdrew
withdrewfor forother
otherreasons.
reasons.
Number
Numberofofpatients
patientsevaluated
evaluatedfor
formaintenance
maintenanceofofNSR:
NSR:503
503TIKOSYN,
TIKOSYN,174174placebo.
placebo.
Number
Numberofofpatients
patientsevaluated
evaluatedfor
forQTc
QTcchange:
change:478
478TIKOSYN,
TIKOSYN,167167placebo.
placebo. Table
Table22shows,
shows,bybyrandomized
randomizeddose,
dose,the
thepercentage
percentageofofpatients
patientsatat66and
and1212months
monthsininboth
bothstudies
studies
who
whoremained
remainedonontreatment
treatmentininNSR
NSRandandthe
thepercentage
percentageofofpatients
patientswho
whowithdrew
withdrewbecause
becauseofof
recurrence
recurrenceofofAF/AFl
AF/AFlororadverse
adverseevents.
events.
CLINICAL
CLINICALSTUDIES
STUDIES
Table
Table2:2:Patient
PatientStatus
Statusatat66and
and1212Months
MonthsPost
PostRandomization
Randomization
Chronic
ChronicAtrial
AtrialFibrillation
Fibrillationand/or
and/orAtrialAtrialFlutter
Flutter
Two
Tworandomized,
randomized,parallel,
parallel,double-blind,
double-blind,placebo-controlled,
placebo-controlled,dose-response
dose-responsetrials trialsevaluated
evaluatedthethe TIKOSYN
TIKOSYNDose
Dose
125
125mcg
mcgBID
BID 250
250mcg
mcgBID
BID 500
500mcg
mcgBID
BID Placebo
Placebo
ability
abilityofofTIKOSYN
TIKOSYN1)1)totoconvert
convertpatients
patientswith
withatrial
atrialfibrillation
fibrillationororatrial
atrialflutter
flutter(AF/AFl)
(AF/AFl)ofof
Study
Study1 1
more
morethan
than11week
weekduration
durationtotonormal
normalsinussinusrhythm
rhythm(NSR)
(NSR)and and2)2)totomaintain
maintainNSR NSR(delay
(delaytime
timetoto Randomized
Randomized 8282 8282 7777 8484
recurrence
recurrenceofofAF/AFl)
AF/AFl)afterafterdrug-induced
drug-inducedororelectrical
electricalcardioversion.
cardioversion.AAtotaltotalofof996
996patients
patientswith
with Achieved
AchievedNSR NSR 6060 6161 6161 6868
a aone
oneweek
weektototwo
twoyear
yearhistory
historyofofatrial
atrialfibrillation/atrial
fibrillation/atrialflutter
flutterwere
wereenrolled.
enrolled.BothBothstudies
studies 6 6months
months
Still
Stillonontreatment
treatmentininNSR
NSR 38%
38% 44%
44% 52%
52% 32%
32%
randomized
randomizedpatients
patientstotoplacebo
placeboorortotodoses
dosesofofTIKOSYN
TIKOSYN125 125mcg,
mcg,250250mcg,
mcg,500 500mcg,
mcg,ororininone
one
D/CD/Cforforrecurrence
recurrence 55%
55% 49%
49% 33%
33% 63%
63%
study
studya acomparator
comparatordrug,
drug,given
giventwice
twicea adayday(these
(thesedoses
doseswerewerelowered
loweredbased
basedononcalculated
calculated D/CD/CforforAEs
AEs 3%
3% 3%3% 8%8% 4%4%
creatinine
creatinineclearance
clearanceand,
and,ininone
oneofofthe
thestudies,
studies,for
forQT
QTinterval QTc).All
intervalororQTc). Allpatients
patientswere
were 1212months
months
started
startedon ontherapy
therapyininaahospital
hospitalwhere
wheretheir
theirECG
ECGwas wasmonitored
monitored(see (seeDOSAGE
DOSAGEAND AND Still
Stillonontreatment
treatmentininNSR
NSR 32%
32% 26%
26% 46%
46% 22%
22%
D/CD/Cforforrecurrence
recurrence 58%
58% 57%
57% 36%
36% 72%
72%
ADMINISTRATION).
ADMINISTRATION). D/CD/CforforAEs
AEs 7%
7% 11%
11% 8%8% 6%6%
Study
Study2 2
Patients
Patientswere
wereexcluded
excludedfromfromparticipation
participationififthey
theyhad
hadhad
hadsyncope
syncopewithin
withinthe
thepast
past66months,
months,AVAV Randomized
Randomized 135
135 133
133 129
129 137
137
block
blockgreater
greaterthan
thanfirst
firstdegree,
degree,MIMIororunstable
unstableangina
anginawithin
within11month,
month,cardiac
cardiacsurgery
surgerywithin
within Achieved
AchievedNSR NSR 103
103 118
118 100
100 106
106
22months,
months,history
historyofofQTQTinterval
intervalprolongation
prolongationororpolymorphic
polymorphicventricular
ventriculartachycardia
tachycardiaassociated
associated 6 6months
months
Still
Stillonontreatment
treatmentininNSR
NSR 41%
41% 49%
49% 57%
57% 22%
22%
with
withuse
useofofantiarrhythmic
antiarrhythmicdrugs,drugs,QT
QTinterval
intervalororQTc
QTc>440
>440msec,
msec,serum
serumcreatinine
creatinine>2.5
>2.5mg/mL,
mg/mL, D/CD/Cforforrecurrence
recurrence 48%
48% 42%
42% 27%
27% 72%
72%
significant
significantdiseases
diseasesofofother
otherorgan
organsystems;
systems;usedusedcimetidine;
cimetidine;ororused
useddrugs
drugsknown
knowntotoprolong
prolongthe
the D/CD/CforforAEs
AEs 9%
9% 6%6% 10%
10% 4%4%
QT
QTinterval.
interval. 1212months
months
Still
Stillonontreatment
treatmentininNSR
NSR 25%
25% 42%
42% 49%
49% 16%
16%
D/CD/Cforforrecurrence
recurrence 59%
59% 47%
47% 32%
32% 76%
76%
Both
Bothstudies
studiesenrolled
enrolledmostly
mostlyCaucasians
Caucasians(over
(over90%),
90%),males
males(over
(over70%),
70%),and andpatients
patients65
65years
years D/CD/CforforAEs
AEs 11%
11% 6%6% 12%
12% 5%5%
ofofage
age(over
(over50%).
50%).Most
Most(>90%)
(>90%)werewereNYHA
NYHAFunctional
FunctionalClass
ClassI IororII.II.Approximately
Approximatelyone-half
one-half Note
Notethatthatcolumns
columnsdodonot notadd
addupuptoto100%
100%due
duetotodiscontinuations
discontinuationsforfor“other”
“other”reasons.
reasons.
had
hadstructural
structuralheart
heartdisease
disease(including
(includingischemic
ischemicheart
heartdisease,
disease,cardiomyopathies,
cardiomyopathies,and andvalvular
valvular
disease)
disease)and
andabout
aboutone-half
one-halfwere
werehypertensive.
hypertensive.AAsubstantial
substantialproportion
proportionofofpatients
patientswere
wereonon
9Figure
Figure4:4:Maintenance
MaintenanceofofNormal
NormalSinus
SinusRhythm,
Rhythm,TIKOSYN
TIKOSYNRegimen
Regimenvs.
vs.Placebo
Placebo(Study
(Study2)2)
Table
Table33and
andFigures
Figures33and
and44show,
show,bybyrandomized
randomizeddose,
dose,the
theeffectiveness
effectivenessofofTIKOSYN
TIKOSYNinin
maintaining
maintainingNSR
NSRusing
usingKaplan
KaplanMeier
Meieranalysis,
analysis,which
whichshows
showspatients
patientsremaining
remainingonontreatment.
treatment.
1.0
1.0
Table
Table3:3:P-Values
P-Valuesand
andMedian
MedianTime
Time(days)
(days)totoRecurrence
RecurrenceofofAF/AFl
AF/AFl
Probability of Remaining in NSR
Probability of Remaining in NSR
TIKOSYN
TIKOSYNDose
Dose 0.8
0.8
125mcg
125 mcgBID
BID 250mcg
250 mcgBID
BID 500mcg
500 mcgBID
BID Placebo
Placebo
Study1 1
Study 500mcg
500mcgBID
BIDDofetilide
Dofetilide
p-valuevs.vs.placebo
p-value placebo P=0.21
P=0.21 P=0.10
P=0.10 P365 2727 0.6
0.6 250mcg
250mcgBID
BIDDofetilide
Dofetilide
Study2 2
Study
p-valuevs.vs.placebo
p-value placebo P=0.006
P=0.006 P365 3434 0.4
0.4
Mediantime
Median timetotorecurrence
recurrenceofofAF/AFl
AF/AFlcould
couldnot notbebeestimated
estimatedaccurately
accuratelyforforthe
the250
250mcg
mcgBID
BIDtreatment
treatmentgroup
groupininStudy
Study2 2and
andthe
the 125mcg
125mcgBID
BIDDofetilide
Dofetilide
500mcg
500 mcgBID BIDtreatment
treatmentgroups
groupsininStudies
Studies1 1and
and2 2because
becauseTIKOSYN
TIKOSYNmaintained
maintained>50% >50%ofofpatients
patients(51%,
(51%,58%,
58%,andand66%,
66%,
p-value
p-valueLog
LogRank
RankTest
Test
respectively)ininNSR
respectively) NSRforforthe
the1212months
monthsduration
durationofofthe thestudies.
studies. 125
125mcg
mcgBID
BIDp=0.006
p=0.006 Placebo
Placebo
0.2
0.2 250
250mcg
mcgBID
BIDpwas
wasininpatients
patientswithwithrecent
recentmyocardial
myocardialinfarction
infarction(DIAMOND
(DIAMONDMI) MI)(of (ofwhom
whom40% 40%had hadNYHA
NYHA these,
these,44cases
casesoccurred
occurredwithin
withinthethefirst
first33days
daysofofdosing
dosingand
and33cases
casesoccurred
occurredbetween
betweenDay Day44and
and
Class
ClassIIIIIIororIV
IVheart
heartfailure).
failure).Both
Bothgroups
groupswerewereatatrelatively
relativelyhigh
highrisk
riskofofsudden
suddendeath.
death.TheThe the
theconclusion
conclusionofofthe
thestudy.
study.InInall,
all,371/749
371/749(50%)
(50%)ofofpatients
patientsononTIKOSYN
TIKOSYNand and419/761
419/761(55%)
(55%)
DIAMOND
DIAMONDtrials trialswere
wereintended
intendedtotodetermine
determinewhether
whetherTIKOSYN
TIKOSYNcould couldreduce
reducethatthatrisk.
risk.The
The ononplacebo
placeborequired
requiredhospitalization.
hospitalization.Of Ofthese,
these,200/749
200/749(27%)
(27%)ofofpatients
patientsononTIKOSYN
TIKOSYNand and
trials
trialsdid
didnotnotdemonstrate
demonstratea areduction
reductionininmortality;
mortality;however,
however,they
theyprovide
providereassurance
reassurancethat,that,when
when 205/761
205/761(27%)
(27%)ononplacebo
placeborequired
requiredhospitalization
hospitalizationbecause
becauseofofworsening
worseningheart
heartfailure.
failure.
initiated
initiatedcarefully,
carefully,inina ahospital
hospitalororequivalent
equivalentsetting,
setting,TIKOSYN
TIKOSYNdid didnot
notincrease
increasemortality
mortalityinin
patients
patientswithwithstructural
structuralheart
heartdisease,
disease,ananimportant
importantfinding
findingbecause
becauseother
otherantiarrhythmics
antiarrhythmics[notably
[notably DIAMOND
DIAMONDPatientsPatientswith
withAtrial
AtrialFibrillation
Fibrillation(the
(theDIAMOND
DIAMONDAF AFsubpopulation).
subpopulation).ThereTherewere
were506506
the
theClass
ClassICICantiarrhythmics
antiarrhythmicsstudied
studiedininthetheCardiac
CardiacArrhythmia
ArrhythmiaSuppression
SuppressionTrial Trial(CAST)
(CAST)and anda a patients
patientsininthe
thetwo
twoDIAMOND
DIAMONDstudies studieswhowhohad
hadatrial
atrialfibrillation
fibrillation(AF)
(AF)atatentry
entrytotothe
thestudies
studies(249
(249
pure
pureClass
ClassIIIIIIantiarrhythmic,
antiarrhythmic,d-sotalol
d-sotalol(SWORD)]
(SWORD)]have haveincreased
increasedmortality
mortalityininpost-infarction
post-infarction randomized
randomizedtotoTIKOSYN
TIKOSYNand and257
257randomized
randomizedtotoplacebo).
placebo).DIAMOND
DIAMONDAF AFpatients
patientsrandomized
randomized
populations.
populations.The TheDIAMOND
DIAMONDtrials trialstherefore
thereforeprovide
provideevidence
evidenceofofa amethod
methodofofsafesafeuse
useofof totoTIKOSYN
TIKOSYNreceived
received250250mcgmcgBID;BID;65%
65%ofofthese
thesepatients
patientshadhadimpaired
impairedrenal
renalfunction,
function,sosothat
that
TIKOSYN
TIKOSYNinina apopulation
populationsusceptible
susceptibletotoventricular
ventriculararrhythmias.
arrhythmias.InInaddition,
addition,the thesubset
subsetofof 250
250mcg
mcgBIDBIDrepresents
representsthe thedose
dosethey
theywould
wouldhave
havereceived
receivedininthetheAF
AFtrials,
trials,which
whichwould
wouldgivegive
patients
patientswithwithAF AFininthe
theDIAMOND
DIAMONDtrials trialsprovide
providefurther
furtherevidence
evidenceofofsafety
safetyinina apopulation
populationofof drug
drugexposure
exposuresimilar
similartotoa aperson
personwith
withnormal
normalrenal
renalfunction
functiongiven
given500
500mcg
mcgBID.
BID.InInthethe
patients
patientswithwithstructural
structuralheart
heartdisease
diseaseaccompanying
accompanyingthe theAF.
AF.Note,
Note,however,
however,thatthatthis
thisAFAF DIAMOND
DIAMONDAF AFsubpopulation,
subpopulation,there therewere
were111
111deaths
deaths(45%)
(45%)ininthe
the249
249patients
patientsininthe
theTIKOSYN
TIKOSYN
population
populationwas wasgiven
givena alower
lower(250
(250mcgmcgBID)BID)dose (seeCLINICAL
dose(see CLINICALSTUDIES,STUDIES,DIAMONDDIAMOND group
groupand
and116116deaths
deaths(45%)
(45%)ininthe the257
257patients
patientsininthe
theplacebo
placebogroup.
group.Hospital
Hospitalreadmission
readmissionratesrates
Patients
Patientswith withAtrial
AtrialFibrillation).
Fibrillation). for
forany
anyreason
reasonwere
were125/249
125/249oror50%50%ononTIKOSYN
TIKOSYNand and156/257
156/257oror61%
61%forforplacebo.
placebo.Of Ofthese,
these,
readmission
readmissionrates
ratesfor
forworsening
worseningheart heartfailure
failurewere
were73/249
73/249oror29%29%ononTIKOSYN
TIKOSYNand and102/257
102/257oror
InInboth
bothDIAMOND
DIAMONDstudies, studies,patients
patientswere
wererandomized
randomizedtoto500
500mcg
mcgBIDBIDofofTIKOSYN,
TIKOSYN,but butthis
this 40%
40%for
forplacebo.
placebo.
was
wasreduced
reducedtoto250250mcg
mcgBIDBIDififcalculated
calculatedcreatinine
creatinineclearance
clearancewas
was40–60
40–60mL/min,
mL/min,ififpatients
patients
had
hadAF,
AF,ororififQT
QTinterval
intervalprolongation
prolongation(>550
(>550msecmsecoror>20%
>20%increase
increasefrom
frombaseline)
baseline)occurred
occurred Of
Ofthe
the506
506patients
patientsininthe
theDIAMOND
DIAMONDstudies
studieswho
whohadhadatrial
atrialfibrillation
fibrillationororflutter
flutteratatbaseline,
baseline,
after
afterdosing.
dosing.Dose
Dosereductions
reductionsfor
forreduced
reducedcalculated
calculatedcreatinine
creatinineclearance
clearanceoccurred
occurredinin47%
47%andand 12%
12%ofofpatients
patientsininthe
theTIKOSYN
TIKOSYNgroup groupand
and2%2%ofofpatients
patientsininthe
theplacebo
placebogroup
grouphadhadconverted
convertedtoto
45%
45%ofofDIAMOND
DIAMONDCHF CHFandandMIMIpatients,
patients,respectively.
respectively.Dose
Dosereductions
reductionsfor
forincreased
increasedQT QT normal
normalsinus
sinusrhythm
rhythmafter
afterone
onemonth.
month.InInthose
thosepatients
patientsconverted
convertedtotonormal
normalsinus
sinusrhythm,
rhythm,79%79%ofof
interval
intervalororQTc
QTcoccurred
occurredinin5% 5%and
and7% 7%ofofDIAMOND
DIAMONDCHF CHFandandMIMIpatients,
patients,respectively.
respectively. the
theTIKOSYN
TIKOSYNgroupgroupand and42%
42%ofofthe
theplacebo
placebogroup
groupremained
remainedininnormal
normalsinus
sinusrhythm
rhythmfor forone
one
Increased
IncreasedQT QTinterval
intervalororQTc
QTc(>550
(>550msec
msecoror>20%
>20%increase
increasefrom
frombaseline)
baseline)resulted
resultedinin year.
year.
discontinuation
discontinuationofof1.8%
1.8%ofofpatients
patientsininDIAMOND
DIAMONDCHF CHFandand2.5%
2.5%ofofpatients
patientsininDIAMOND
DIAMONDMI. MI.
InInthe
theDIAMOND
DIAMONDstudies,studies,although
althoughTorsade
TorsadededePointes
Pointesoccurred
occurredmore
morefrequently
frequentlyininthe
the
InInthe
theDIAMOND
DIAMONDstudies,
studies,all
allpatients
patientswere
werehospitalized
hospitalizedforforatatleast
least33days
daysafter
aftertreatment
treatment TIKOSYN-treated
TIKOSYN-treatedpatients (seeADVERSE
patients(see ADVERSEREACTIONS),
REACTIONS),TIKOSYN, TIKOSYN,givengivenwith
withananinitial
initial
was
wasinitiated
initiatedand
andmonitored
monitoredby bytelemetry.
telemetry.Patients
Patientswith
withQTc
QTcgreater
greaterthan
than460
460msec,
msec,second
secondoror 3-day
3-dayhospitalization
hospitalizationandandwith
withdose
dosemodified
modifiedfor forreduced
reducedcreatinine
creatinineclearance
clearanceand
andincreased
increasedQT QT
third
thirddegree
degreeAVAVblock
block(unless
(unlesswith
withpacemaker),
pacemaker),resting
restingheart
heartrate
rateCONTRAINDICATIONS
CONTRAINDICATIONS Relation
RelationofofQT
QTInterval Dose:The
IntervaltotoDose: TheQTQTinterval
intervalincreases
increaseslinearly
linearlywith
withincreasing
increasingTIKOSYN
TIKOSYN
dose
dose(see
(seeFigures and22ininCLINICAL
Figures11and CLINICALPHARMACOLOGY
PHARMACOLOGYand andDose-Response
Dose-Responseandand
TIKOSYN
TIKOSYNisiscontraindicated
contraindicatedininpatients
patientswith
withcongenital
congenitalororacquired
acquiredlong
longQTQTsyndromes.
syndromes. Concentration
ConcentrationResponse
Responsefor forIncrease
IncreaseininQT
QTInterval).
Interval).
TIKOSYN
TIKOSYNshouldshouldnot
notbebeused
usedininpatients
patientswith
witha abaseline
baselineQT
QTinterval
intervalororQTc
QTc>440
>440msec
msec(500
(500
msec
msecininpatients
patientswith
withventricular
ventricularconduction
conductionabnormalities).
abnormalities).TIKOSYN
TIKOSYNisisalsoalsocontraindicated
contraindicatedinin Frequency
FrequencyofofTorsade
Torsadede Pointes:InInthe
dePointes: thesupraventricular
supraventriculararrhythmia
arrhythmiapopulation
population(patients
(patients
patients
patientswith
withsevere
severerenal
renalimpairment
impairment(calculated
(calculatedcreatinine
creatinineclearance
clearance500 mcg AllDoses
All Doses
megestrol
megestrolshould
shouldnotnotbebeused
usedininpatients
patientsononTIKOSYN.
TIKOSYN. BID
BID BID
BID BID
BID BID
BID
Number
NumberofofPatients
Patients 217
217 388
388 703
703 3838 1346
1346
TorsadededePointes
Torsade Pointes 00 1 1(0.3%)
(0.3%) 6 6(0.9%)
(0.9%) 4 4(10.5%)
(10.5%) 1111(0.8%)
(0.8%)
The
Theconcomitant
concomitantuse
useofofhydrochlorothiazide
hydrochlorothiazide(alone
(aloneororinincombinations
combinationssuch
suchasaswith
withtriamterene)
triamterene)
with
withTIKOSYN
TIKOSYNisiscontraindicated (seePRECAUTIONS,
contraindicated(see PRECAUTIONS,Drug-Drug Drug-DrugInteractions)
Interactions)because
because As
Asshown
shownininTable
Table5,5,the
therate
rateofofTdP
TdPwas
wasreduced
reducedwhen
whenpatients
patientswere
weredosed
dosedaccording
accordingtototheir
their
this
thishas
hasbeen
beenshown
showntotosignificantly
significantlyincrease
increasedofetilide
dofetilideplasma
plasmaconcentrations
concentrationsand
andQTQTinterval
interval
renal
renalfunction (seeCLINICAL
function(see CLINICALPHARMACOLOGY,
PHARMACOLOGY,Pharmacokinetics
PharmacokineticsininSpecial
Special
prolongation.
prolongation.
Populations,
Populations,Renal
RenalImpairment
Impairmentand andDOSAGE
DOSAGEAND ANDADMINISTRATION).
ADMINISTRATION).
TIKOSYN
TIKOSYNisisalso
alsocontraindicated
contraindicatedininpatients
patientswith
witha aknown
knownhypersensitivity
hypersensitivitytotothe
thedrug.
drug. Table
Table5:5:Incidence
IncidenceofofTorsade
TorsadededePointes
PointesBefore
Beforeand
andAfter
AfterIntroduction
IntroductionofofDosing
Dosing
According
AccordingtotoRenal
RenalFunction
Function
Total
Total Before
Before After
After
WARNINGS
WARNINGS Population:
Population: n/N%%
n/N n/N%%
n/N n/N%%
n/N
SupraventricularArrhythmias
Supraventricular Arrhythmias 11/1346(0.8%)
11/1346 (0.8%) 6/193(3.1%)
6/193 (3.1%) 5/1153(0.4%)
5/1153 (0.4%)
Ventricular Arrhythmia:TIKOSYN
VentricularArrhythmia: TIKOSYN(dofetilide)
(dofetilide)cancancause
causeserious
seriousventricular
ventricular DIAMONDCHF
DIAMOND CHF 25/762(3.3%)
25/762 (3.3%) 7/148(4.7%)
7/148 (4.7%) 18/614(2.9%)
18/614 (2.9%)
DIAMONDMI
DIAMOND MI 7/749(0.9%)
7/749 (0.9%) 3/101(3.0%)
3/101 (3.0%) 4/648(0.6%)
4/648 (0.6%)
arrhythmias,
arrhythmias,primarily
primarilyTorsade
TorsadededePointes
Pointes(TdP)
(TdP)type
typeventricular
ventriculartachycardia,
tachycardia,aa DIAMONDAF
DIAMOND AF 4/249(1.6%)
4/249 (1.6%) 0/43(0%)
0/43 (0%) 4/206(1.9%)
4/206 (1.9%)
polymorphic
polymorphicventricular
ventriculartachycardia
tachycardiaassociated
associatedwithwithQTQTinterval
intervalprolongation.
prolongation.QTQT
interval
intervalprolongation
prolongationisisdirectly
directlyrelated
relatedtotodofetilide
dofetilideplasma
plasmaconcentration.
concentration.Factors
Factorssuch
suchasas The
Themajority
majorityofofthe
theepisodes
episodesofofTdP
TdPoccurred
occurredwithin
withinthe
thefirst
firstthree
threedays
daysofofTIKOSYN
TIKOSYNtherapy
therapy
reduced
reducedcreatinine
creatinineclearance
clearanceororcertain
certaindofetilide
dofetilidedrug
druginteractions
interactionswill
willincrease
increasedofetilide
dofetilide (10/11
(10/11events
eventsininthe
thestudies
studiesofofpatients
patientswith
withsupraventricular
supraventriculararrhythmias;
arrhythmias;19/25
19/25and
and4/7
4/7events
eventsinin
plasma
plasmaconcentration.
concentration.TheTherisk
riskofofTdP
TdPcancanbebereduced
reducedby bycontrolling
controllingthe
theplasma
plasma DIAMOND
DIAMONDCHF CHFand andDIAMOND
DIAMONDMI, MI,respectively;
respectively;2/4
2/4events
eventsininthe
theDIAMOND
DIAMONDAF AF
concentration
concentrationthrough
throughadjustment
adjustmentofofthe
theinitial
initialdofetilide
dofetilidedose
doseaccording
accordingtotocreatinine
creatinine subpopulation).
subpopulation).
clearance
clearanceand
andbybymonitoring
monitoringthe theECG
ECGforforexcessive
excessiveincreases
increasesininthe
theQT
QTinterval.
interval.
Mortality:InIna apooled
Mortality: pooledsurvival
survivalanalysis
analysisofofpatients
patientsininthe
thesupraventricular
supraventriculararrhythmia
arrhythmiapopulation
population
Treatment
Treatmentwith withdofetilide
dofetilidemust
musttherefore
thereforebebestarted
startedonly
onlyininpatients
patientsplaced
placedforforaaminimum
minimum (low
(lowprevalence
prevalenceofofstructural
structuralheart
heartdisease),
disease),deaths
deathsoccurred
occurredinin0.9%
0.9%(12/1346)
(12/1346)ofofpatients
patients
ofofthree
threedays
daysininaafacility
facilitythat
thatcan
canprovide
provideelectrocardiographic
electrocardiographicmonitoring
monitoringand andininthe
the receiving
receivingTIKOSYN
TIKOSYNand and0.4%
0.4%(3/677)
(3/677)ininthe
theplacebo
placebogroup.
group.Adjusted
Adjustedfor forduration
durationofoftherapy,
therapy,
presence
presenceofofpersonnel
personneltrained
trainedininthe
themanagement
managementofofserious
seriousventricular
ventriculararrhythmias.
arrhythmias. primary
primarydiagnosis,
diagnosis,age,age,gender,
gender,and andprevalence
prevalenceofofstructural
structuralheart
heartdisease,
disease,the
thepoint
pointestimate
estimateofof
Calculation
Calculationofofthethecreatinine
creatinineclearance
clearancefor
forall
allpatients
patientsmust
mustprecede
precedeadministration
administrationofofthe
the the
thehazard
hazardratio
ratiofor
forthethepooled
pooledstudies
studies(TIKOSYN/placebo)
(TIKOSYN/placebo)was was1.1 1.1(95%
(95%CI:CI:0.3,
0.3,4.3).
4.3).The
The
first
firstdose
doseofofdofetilide.
dofetilide.For
Fordetailed
detailedinstructions
instructionsregarding
regardingdose
doseselection,
selection,see
seeDOSAGE
DOSAGE DIAMOND
DIAMONDCHF CHFand andMI MItrials
trialsexamined
examinedmortality
mortalityininpatients
patientswith
withstructural
structuralheart
heartdisease
disease
AND
ANDADMINISTRATION.
ADMINISTRATION.
(ejection
(ejectionfraction
fraction35%).
35%).InInthese
theselarge,
large,double-blind
double-blindstudies,
studies,deaths
deathsoccurred
occurredinin36%
36%(541/1511)
(541/1511)
ofofTIKOSYN
TIKOSYNpatients
patientsandand37%
37%(560/1517)
(560/1517)ofofplacebo
placebopatients.
patients.InInanananalysis
analysisofof506
506DIAMOND
DIAMOND
The
Therisk
riskofofdofetilide
dofetilideinduced
inducedventricular
ventriculararrhythmia
arrhythmiawas wasassessed
assessedininthree
threeways
waysininclinical
clinical
patients
patientswith
withatrial
atrialfibrillation/flutter
fibrillation/flutteratatbaseline,
baseline,one
oneyear
yearmortality
mortalityononTIKOSYN
TIKOSYNwas was31%31%vs.
vs.
studies:
studies:1)1)bybydescription
descriptionofofthe
theQTQTinterval
intervaland
anditsitsrelation
relationtotothe
thedose
doseandandplasma
plasmaconcentration
concentration
32%
32%ononplacebo
placebo(see(seeCLINICAL
CLINICALSTUDIES).
STUDIES).
ofofdofetilide;
dofetilide;2)2)bybyobserving
observingthethefrequency
frequencyofofTdP
TdPininTIKOSYN-treated
TIKOSYN-treatedpatientspatientsaccording
accordingtoto
dose;
dose;3)3)bybyobserving
observingthe
theoverall
overallmortality
mortalityrate
rateininpatients
patientswith
withatrial
atrialfibrillation
fibrillationand
andininpatients
patients
Because
Becauseofofthe
thesmall
smallnumber
numberofofevents,
events,ananexcess
excessmortality
mortalitydueduetotoTIKOSYN
TIKOSYNcannot cannotbeberuled
ruledout
out
with
withstructural
structuralheart
heartdisease.
disease.
with
withconfidence
confidenceininthe
thepooled
pooledsurvival
survivalanalysis
analysisofofplacebo-controlled
placebo-controlledtrials
trialsininpatients
patientswith
with
supraventricular
supraventriculararrhythmias.
arrhythmias.However,
However,ititisisreassuring
reassuringthat
thatinintwo
twolarge
largeplacebo-controlled
placebo-controlled
mortality
mortalitystudies
studiesininpatients
patientswith
withsignificant
significantheart
heartdisease
disease(DIAMOND
(DIAMONDCHF/MI), CHF/MI),theretherewere
werenono
12You can also read