TRACHOMA 2020 REPORT OF THE 21ST MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION OF - World Health Organization
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

REPORT OF THE 21ST MEETING
OF THE WHO ALLIANCE FOR
THE GLOBAL ELIMINATION OF
TRACHOMA
BY 2020
GENEVA, SWITZERLAND, 20–22 APRIL 2017
Twenty_first_cover.indd 1 4/1/2019 10:04:31 AM
Twenty_first_report_ok.indd 4 4/1/2019 9:58:50 AM
REPORT OF THE 21ST MEETING
OF THE WHO ALLIANCE FOR
THE GLOBAL ELIMINATION OF
TRACHOMA
BY 2020
GENEVA, SWITZERLAND, 20–22 APRIL 2017
Twenty_first_report_ok.indd 1 4/1/2019 9:58:50 AM© World Health Organization 2019
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-
ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes,
provided the work is appropriately cited, as indicated below. In any use of this work, there should be no
suggestion that WHO endorses any specific organization, products or s ervices. The us e of the WHO logo is
not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative
Commons licence. If you create a translation of this work, you should add the following disclaimer along with
the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is
not responsible for the content or accuracy of this translation. The original English edition shall be the binding
and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation
rules of the World Intellectual Property Organization..
Suggested citation. Report of the 21st meeting of the WHO Alliance for the Global Elimination of Trachoma
by 2020, Geneva, Switzerland, 20–22 April 2017. Geneva: World Health Organization; 2019. Licence: CC BY-
NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit
requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as
tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and
to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-
party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not
imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted
and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed
or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and
omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication.
However, the published material is being distributed without warranty of any kind, either expressed or implied.
The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be
liable for damages arising from its use.
This publication does not necessarily represent the decisions or policies of WHO.
Printed in France.
WHO/CDS/NTD/PCT/2019.02
Twenty_first_report_ok.indd 2 4/1/2019 9:58:50 AMContents
Acknowledgements − Country Perspective: Lao People’s Democratic
Republic
VI
− Country Perspective: Nepal
Abbreviations and acronyms
− Country Perspective: Gambia
− Dossier Review Group Perspective
Session 1 – Opening
− High-level Panel
1 −
−
−
Donor Perspective
Report: International Trachoma Initiative
A, F and E for GET2020
− World Health Organization Report − Selecting and Training Community Drug
− Tnternational Coalition for Trachoma Control Distributors
Report − Going to Scale with A, F and E
− Regional reports − Interventions for Facial Cleanliness &
Environmental Improvement
− Thresholds for Environmental Improvement
− Breakout B
Session 2 – Trachoma Scientific
Informal Workshop 12
− Surgery for GET2020 Panel
− Reducing the Trichiasis Backlog
Session 4 – Plans of Action for
2016 and 2017 32
− Getting the Trichiasis Backlog to Zero
− Transitioning Trichiasis Care into Routine − Governments of endemic countries
Services − World Health Organization
− The TT patient tracking app − NGOs and other implementing partners
− The Morbidity Management and Disability − Public and private donors
Prevention Project − Academic and research institutions
− Breakout A − Meeting Close
− Managing PC-NTD Implementation Data
− Forecasting Trachoma Elimination
References
38
23
Session 3 – Panel: Validation of
Trachoma Elimination
− Country perspective: Morocco
Annexes
Annex 1: Agenda
Annex 2: List of participants
45
− Country Perspective: Mexico
Twenty_first_report_ok.indd 3 4/1/2019 9:58:50 AMTwenty_first_report_ok.indd 4 4/1/2019 9:58:50 AM
Acknowledgements
T The 21st meeting of the WHO Alliance for the Global Elimination of Trachoma by 2020 was
supported by the Task Force for Global Health, the United States Agency for International
Development, and Uniting to Combat Neglected Tropical Diseases.
The Alliance thanks Victor V. Florea for his work as meeting rapporteur, and Karen Ciceri-
Reynolds, Anthony W. Solomon and Patrick Tissot for report editing and design
v
Twenty_first_report_ok.indd 5 4/1/2019 9:58:50 AMAbbreviations and
acronyms
DFID Department for International Development
ESPEN Expanded Special Project for Elimination of Neglected Tropical Diseases
ITI International Trachoma Initiative
MDA mass drug administration
NTD neglected tropical disease
SAFE Surgery, Antibiotics, Facial cleanliness, Environmental improvement
TEMF Trachoma Elimination Monitoring Form
TF trachomatous inflammation–follicular
vi USAID United States Agency for International Development
WASH water, sanitation and hygiene
WHO World Health Organization
Twenty_first_report_ok.indd 6 4/1/2019 9:58:50 AMIntroduction
T he 21st meeting of the World Health Organization (WHO) Alliance for the Global
Elimination of Trachoma by 2020 (GET2020) took place at the InterContinental Hotel
Geneva, Switzerland, from 20–22 April 2017, as part of the 2017 Neglected Tropical Disease
(NTD) Summit jointly hosted by the World Health Organization and Uniting to Combat vii
Neglected Tropical Diseases.
Dr Dirk Engels, Director, Department of Control of NTDs, WHO, welcomed participants to
Geneva and congratulated the Alliance on the progress being made towards the GET2020 target
(1). He noted that the stage was set for going to full scale. This was attributable in part to the
work of the Global Trachoma Mapping Project (2), which was a massive effort to understand
the epidemiology of trachoma worldwide, and served as a model for efforts to map other NTDs
(3). Further evidence of hard work by members of the Alliance could be found in the success
of several countries—Oman, Morocco and Mexico by the date of the meeting’s opening—in
being validated as having eliminated trachoma as a public health problem. Other countries were
making progress, he noted, and more countries were expected to undergo validation in 2017
and beyond (1).
Dr Anthony Solomon, Medical Officer, Department of Control of NTDs, WHO, nominated
Chairs and officers for the meeting, who were then confirmed by the Alliance by acclamation. He
thanked the Task Force for Global Health; United States Agency for International Development;
and Uniting to Combat NTDs for their contributions to staging the meeting. Dr Solomon
reminded participants that the purpose of the meeting was to monitor progress towards the
elimination of trachoma at global level, exchange information and experience on implementation
of the SAFE strategy (surgery, antibiotics, facial cleanliness and environmental improvement),
review partnership opportunities at global, regional and national levels, and discuss obstacles
Twenty_first_report_ok.indd 7 4/1/2019 9:58:50 AMand barriers to the achievement of the GET2020 goal. Expected outcomes of the meeting were:
global monitoring of progress towards the elimination of trachoma; exchange of information on
SAFE implementation at global and regional level; refinement of approaches for optimal impact,
where possible; identification of opportunities for increased collaboration with efforts against
other NTDs; and a report of the meeting to share progress towards the WHA51.11 target (4)
with all endemic countries and partners.
The agenda (Annex 1) and list of participants (Annex 2) for the meeting are found at the end of
this report.
viii
Twenty_first_report_ok.indd 8 4/1/2019 9:58:50 AMSESSION 1
Opening
Dr Ren Minghui, Assistant Director-General, NTD Summit showed, he felt, the willingness
HIV/AIDS, Tuberculosis, Malaria and NTDs, of the Alliance to collaborate externally, create
WHO, opened the meeting efficiencies, and share knowledge within the
broader NTD community.
T rachoma causes blindness in the world’s
poorest people. Those affected by trachoma
typically live in the poorest countries; within
Thanks to the efforts of the Alliance, Dr Ren
noted that trachoma was progressively being 1
those countries they live in the poorest eliminated. In 2011, 325 million people
communities; and in those communities, were living in areas that required the SAFE
the people who go blind from trachoma are strategy (8). As of April 2017, that number had
proven to be poorer than their neighbors (5). dropped to 182 million, a 44% decrease (9).
Going blind keeps them poor, and keeps their Dr Ren felt that this was remarkable progress,
children poor, too. and would not have been possible without the
steadfast leadership of endemic country health
Since 1993, WHO has recommended the ministries, most of which were represented in
SAFE strategy to prevent trachoma blindness the meeting room, and the strong collaboration
(6). SAFE is an integrated package of of civil society, academics and donors.
interventions, delivered at community level, Those donors include the United Kingdom’s
that prevents blindness from trachoma at Department for International Development,
multiple stages of its pathogenesis. In 1996, who had doubled their commitment to NTDs
with partners, WHO established the WHO in an announcement made just prior to the
Alliance for GET2020 to help countries use meeting, the Queen Elizabeth Diamond
the SAFE strategy to eliminate trachoma as a Jubilee Trust, and USAID. The donor group
public health problem (7). Dr Ren noted that also included Pfizer, which by the date of
the April 2017 meeting was the 21st Meeting of the meeting had contributed more than 625
the Alliance, and commented that the number million doses of the antibiotic azithromycin
of participants in the room suggested that the (Zithromax®) to trachoma elimination
sense of commitment from its members and programmes around the world (10).
their energy to see trachoma eliminated had
never been stronger. The fact that this Meeting Despite this unprecedented progress, more
was being held as part of the multi-disease work was still required to achieve the shared
Twenty_first_report_ok.indd 1 4/1/2019 9:58:50 AMgoal of a trachoma-free world. Dr Ren specified Trachoma elimination is prioritized in the
new donors, operational research to refine the 2017–2021 roadmap for WHO’s Eastern
way that the SAFE strategy was implemented, Mediterranean Region. Intersectoral
and renewed commitment from governments programmes are being used to improve water
and civil society, as particular priorities (11- supplies and sanitation, and to provide eye care,
13). With these ingredients, a world free of including trichiasis surgery. It is important that
blindness from trachoma would be within our countries meeting their trachoma elimination
reach; without them, he felt that we might lose targets continue to receive support for post-
the incredible gains made over recent years. validation surveillance, and that interventions
Dr Ren welcomed participants to Geneva and are scaled up in countries where trachoma
to the meeting, wished them every success remains a public health problem. Countries
in their discussions, and pledged WHO’s with low burdens of trachoma must be
steadfast, ongoing support to ensuring that prepared to conduct impact and pre-validation
no-one is left behind as a result of trachoma. surveillance surveys.
Dr Mark Jacobs, Director, Division of
High-level Panel Communicable Diseases, Western Pacific
Regional Office, WHO
Mr Bruce Gordon, Coordinator, Water,
Sanitation and Hygiene, WHO, introduced Cambodia, China and Lao People’s Democratic
the panelists and acted as facilitator for the Republic all claim to have eliminated
subsequent discussion. Apologies for being trachoma as a public health problem. Fiji,
unable to participate in the panel discussion Kiribati, Solomon Islands and Vanuatu are
were received from Professor Yifru Berhan making progress toward trachoma elimination
2
Mitke, Minister of Health, Ethiopia; and Dr through implementation of the SAFE strategy.
Marcos Espinal, Director, Communicable Solomon Islands and Vanuatu did their first
Diseases and Health Analysis, Regional Office round of antibiotic mass drug administration
for the Americas, WHO. (MDA) between 2015 and 2016 (1), and intend
to undertake impact surveys in 2017. Kiribati
Dr Mahmoud Fikri, Regional Director, Eastern (15, 16) plans to undertake its first round of
Mediterranean Regional Office, WHO antibiotic MDA in 2017. Solomon Islands
and Vanuatu are known to have populations
In 2016, Morocco submitted its dossier for that are co-endemic for trachoma and yaws
validation of elimination of trachoma as a (17–19), so it is anticipated that the provision
public health problem, and achieved formal of azithromycin will reduce the prevalence of
recognition from WHO for having achieved this both diseases (20); the effect will be closely
milestone (14). In the Eastern Mediterranean measured. Australia and Viet Nam are
Region, trachoma was still known to be implementing targeted MDA in trachoma-
a public health problem in Afghanistan, endemic populations (1). Papua New Guinea
Egypt, Pakistan, Somalia, Sudan and Yemen. implemented baseline surveys for trachoma
Trachoma mapping has been completed in in 2016 (21) and is expected to move forward
Yemen; is ongoing in Egypt, Pakistan and with MDA in endemic districts. Nauru is
Sudan; and is planned for Afghanistan and suspected of having trachoma but has not yet
Somalia. The Islamic Republic of Iran claims started a programme.
to have eliminated trachoma as a public health
problem, but has not yet submitted a dossier
for formal evaluation by WHO.
Twenty_first_report_ok.indd 2 4/1/2019 9:58:50 AMIt is important that there is good Dr Matshidiso Moeti, Regional Director, WHO
communication between WHO and various Regional Office for Africa, WHO.
partners providing direct support to the
countries in the Western Pacific Region. There The African Region is set to make considerable
has been limited support to date for the water, progress towards the elimination of trachoma
sanitation and hygiene (WASH) components in the next few years. Trachoma elimination
of the SAFE strategy. Efforts are being made is now a part of the remit of the Expanded
to encourage multisectoral approaches in a Special Project for Elimination of Neglected
number of countries, in order to strengthen Tropical Diseases (ESPEN), a five-year
WASH delivery (22). It is important that sight project launched in May 2016 to provide
is not lost of what happens after a formerly- national NTD programmes with technical and
endemic country succeeds in eliminating fundraising support to accelerate the control
trachoma as a public health problem. Without and elimination of the five NTDs whose
post-validation surveillance, the disease could management strategy employs mass drug
potentially become re-established, as seen administration or preventive chemotherapy
previously with measles. In addition, trachoma (25). The NTD mapping portal (http://espen.
elimination does not necessarily mean that the afro.who.int/) was launched as part of ESPEN
risk of chronic morbidity has been removed. to enable improved access and use of mapping
Individuals who have received operations for data, including trachoma data. There has been
trichiasis will require follow-up for several excellent collaboration between the AFRO
more years, and efforts need to be made to mapping initiative and the Global Trachoma
detect incident cases, too (23). Mapping Project. Regional updates should
become available on the ESPEN portal as
Dr Ren Minghui approval from countries is obtained to share
data. It is important to note that the African 3
The day is approaching when global Region is the most affected by trachoma, with
elimination of trachoma will become a reality. 27 of a total of 42 endemic countries located
More countries will reach their trachoma in Africa (1). The Region also has the most
elimination targets (23), and national trachoma intensive elimination efforts for trachoma.
programmes will face new challenges related In 2016, about 250,000 people in Africa had
to surveillance (24). In the post-validation operations for trichiasis and nearly 83 million
phase, there is risk that donors may leave and people were treated with antibiotics for
investments from governments may disappear trachoma, both of which represent significant
as trachoma will no longer be an immediate increases from the previous year (1). These
concern. interventions are hugely beneficial, and relieve
people of trachoma-related disability, poverty,
Governments must be prepared to facilitate and chronic morbidity.
integration of public health programmes,
provide leverage for common public health Though trachoma mapping is virtually
interventions and address challenges relating complete for countries suspected of being
to broader public health issues such as endemic for trachoma, thanks to the financial
the development of universal health care support of partners, improved mapping data
coverage. It will be especially challenging for are still needed in some countries to target
governments to coordinate efforts among the interventions to the populations that need
many players involved. them. With additional support from ESPEN,
the WHO Regional Office for Africa hopes
to help to complete trachoma mapping in
Twenty_first_report_ok.indd 3 4/1/2019 9:58:50 AMcurrently unmapped areas, such as in South Ms Emily Wainwright, United States Agency for
Sudan, and to introduce SAFE interventions International Development (USAID)
where required. In 2016, there was a large
expansion of SAFE roll-out in 16 countries USAID supports MDA and/or trachoma
in Africa (1). These interventions reached surveys in 19 countries, most of which are
40 million people in 277 districts, most of in Africa. Partly as a result of this support,
whom were children. Ethiopia has seen a in 2016, the number of people receiving
tremendous scale-up of interventions, funded antibiotics for trachoma worldwide rose from
in part through an increase in commitment 56 million to 85 million (1). There are several
of domestic resources to support application current challenges that USAID foresees. First,
of the SAFE strategy. Ghana and Gambia as success in some areas becomes documented,
have scaled down SAFE implementation and communication within and beyond existing
are awaiting formal validation of elimination stakeholders is important, in order to maximize
of trachoma as a public health problem from the visibility of the programme at global
WHO. level. It is important to show that countries
are meeting their elimination goals, as this
Mr Iain Jones, Department for International provides incentives for continued partner
Development (DFID), United Kingdom support and funding. Second, USAID supports
surgical work in three endemic countries.
The United Kingdom is committed to funding There should be greater emphasis on quality as
antibiotic MDA and some 400,000 surgeries an integral component of surgery interventions
for trichiasis. DFID will also provide specific for trichiasis (26). Third, it is important
support to the Coalition for Operational that trachoma interventions take advantage
Research on Neglected Tropical Diseases of structures that are already in place. For
4 for research and development relevant to instance, monitoring of interventions for facial
trachoma. It is important that partners work cleanliness and environmental improvement
to strengthen healthcare systems in trachoma can be included within existing WASH
endemic countries, in order to sustain public monitoring and evaluation frameworks, in
health interventions and achieve lasting results. order to increase efficiency.
It is equally important to ensure that trichiasis
surgeries being delivered are of high quality. Discussion
Moving forward, DFID will evaluate how
support for and engagement with trachoma Mr Gordon pointed out that many issues had
elimination programmes should change with been raised, and invited the audience to engage
the cessation of MDA, as countries approach with the panelists.
their elimination goals. Evaluation will also
be required to determine how best to use The first question asked about the strategy for
trachoma metrics in models, supported by scaling down in areas where trachoma is no
case studies on health system strengthening, longer a public health problem, and whether
and quality and access to water and sanitation, any lessons for scaling down could be learned
in order to inspire domestic governments and from campaigns to eliminate or eradicate other
other collaborators to continue the fight to diseases, such as polio and malaria.
eliminate trachoma.
Twenty_first_report_ok.indd 4 4/1/2019 9:58:50 AMThe panel agreed that this question was 3. In July 2016, Tropical Data was
important. Mr Jones pointed out that health launched (27, 28). This collaboration
system strengthening and continued disease supports the full trachoma survey
surveillance would be needed post-validation, process from protocol development to
in order to ensure that health systems have data management and analysis.
capacity to sustain the gains made against 4. Also in July 2016, the Alliance published
trachoma. Ms Wainwright reminded Eliminating Trachoma: Accelerating
participants that interventions against NTDs Towards 2020 (12).
benefited low-income communities in many
ways other than specifically addressing 5. In August 2016, WHO’s Strategic and
endemicity of disease. Precipitous scale-down Technical Advisory Group on NTDS
could remove community outreach services to convened a technical consultation to
the most disadvantaged. Dr Moeti said that it review data generated to date by the
was important to continue to engage the people “Trachoma Alternative Indicators
helping with surveillance, data precision and Study”, consider the implications
data quality in the post-elimination phase. Dr for global policy development on
Fikri reiterated that disease monitoring must validation of trachoma elimination,
continue for many years as a component of and plan further work. No changes were
scaling down. Dr Jacobs noted that scaling made to current guidelines. The Group
down occurs in connection with cessation of requested that national programmes
funding. He said that it is important to have continue to help implement the
a planned, measured transition from a single research agenda (29).
disease program to integration within a health 6. Also in August, the 2016 Hilton
system capable of sustaining the impact of Humanitarian Prize was awarded to
previous interventions and able to continue the Task Force for Global Health, the 5
disease monitoring. Dr Ren concluded that parent organization of the International
we should review our messaging for these Trachoma Initiative (ITI).
processes, to help ensure smooth transitions.
7. In September 2016, more than
300 partners came together to
commemorate the 10th anniversary
World Health Organization of the USAID NTD Program, which
Report had by that date delivered more than
1.6 billion treatments against NTDs in
Dr Anthony Solomon, Medical Officer, 31 countries, in the process leveraging
Department of Control of NTDs, WHO US$11.1 billion worth of in-kind
donations from the pharmaceutical
Highlights for the global programme over the industry.
twelve months since the previous (April 2016) 8. In October 2016, at its 10th General
meeting of the Alliance were presented: Assembly in Durban, South Africa, the
International Agency for the Prevention
1. Marked scale-up in interventions of Blindness awarded its Global
against trachoma (1) was noted (see Partnership Award to the Alliance, in
below). recognition of its remarkable work to
2. In June 2016, WHO published its eliminate trachoma.
standard operating procedures for 9. October 2016 also saw the launch of a free
validating national elimination of online course on eliminating trachoma,
trachoma as a public health problem developed by the International Centre
(23).
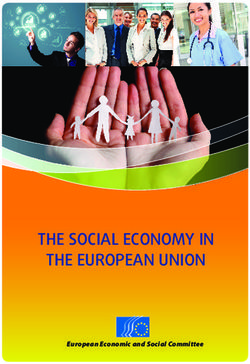
Twenty_first_report_ok.indd 5 4/1/2019 9:58:50 AMfor Eye Health at the London School of 300
Hygiene & Tropical Medicine. 250
10. In November 2016, WHO formally 200
validated elimination of trachoma as a 150
public health problem from Morocco 100
(14). Validation was then undertaken 50
in Mexico in January 2017 (30). 0
2014 2015 2016
11. In April 2017, the United Kingdom
Fig. 1 Number of people operated for trichiasis annually,
announced a doubling of its support worldwide, 2014–2016 (thousands)
to fight NTDs, including trachoma,
over the subsequent five years. The
total support package was anticipated
100
to prevent up to 400,000 cases of
trachomatous blindness. 80
60
40
In 2017, 69 countries were asked by WHO
to submit Trachoma Elimination Monitoring 20
Forms, and 61 countries did so. Of the eight 0
countries that did not, six did not have active 2014 2015 2016
trachoma programmes. Forms were still sent Fig. 2 Number of people given antibiotics for trachoma
to countries that had already been recognized elimination
(millions)
purposes annually, worldwide, 2014–2016
as having eliminated trachoma, in order to help
encourage post-validation surveillance and to
6
maintain visibility for data that continue to 85% of treated districts achieved antibiotic
collect. coverage of ≥ 80% in 2016, an increase from
72% of districts achieving ≥ 80% coverage
Worldwide, 260,759 people with trichiasis in 2015. Recent data (34) support the use of
received corrective surgery in 2016, a 41% 80% as the minimum acceptable coverage in
increase from the 185,000 people managed azithromycin MDA for trachoma.
in 2015 (Figure 1). Available data showed that
54% of those receiving corrective surgery for The number of people living with trichiasis
trichiasis were female. Women are known to be decreased from approximately 3.2 million in
affected by trichiasis up to four times as often 2015 to approximately 2.8 million in 2016.
as men (31, 32), so these data suggest that in The number of people living in districts in
2016, women were still relatively under-served which the most recent estimated prevalence of
by trichiasis surgery programmes (32, 33). trachomatous inflammation—follicular (TF)
was ≥ 5% (and therefore need treatment with
The number of people given antibiotics for the A, F and E components of SAFE) decreased
trachoma increased from 56.1 million in from 192 million in 2015 to 190 million in 2016
2015 to 85.2 million in 2016. In Ethiopia (1); preliminary analyses suggested that by
alone, the number of people given antibiotics April 2017, that number had declined further
for trachoma increased from 32.6 million in to < 182 million.
2015 to 47.2 million in 2016. Global antibiotic
coverage (the number of people treated Dr Solomon noted that in the 12 months
divided by the number living in districts that following the meeting, WHO anticipated
need antibiotic MDA) increased from 30% in receiving completed dossiers claiming
2015 to 45% in 2016 (1). elimination of trachoma as a public health
problem from several more countries. He
Twenty_first_report_ok.indd 6 4/1/2019 9:58:50 AMexpressed a hope that WHO would be able In response to a question asking about what
to validate elimination in these countries and needed to be done to expand trichiasis surgery
continue to focus the efforts of the Alliance output, Dr Solomon said that there was a
on populations where interventions were still continuing need to focus on surgeon training
required. It was also anticipated that regional and supervision (35), quality of operations
elimination plans would be generated for provided, and follow-up with patients to
several regions, detailing the concrete actions ensure that outcomes are good. He added
to be undertaken by various actors to get rid that a protocol for a trichiasis-only prevalence
of trachoma. survey had recently been developed and
validated (36).
Discussion
The first question related to the reasoning for International Coalition for
sending TEMFs to countries which were not
known to be trachoma-endemic. Dr Solomon Trachoma Control Report
said that TEMFS are sent to such countries
in order to raise awareness and encourage Ms Virginia Sarah, Chair, International
engagement with global trachoma elimination Coalition for Trachoma Control, described the
efforts. Coalition as a diverse and highly committed
group of members and observers who come
The second question was a request for an together to amplify support for GET2020.
opinion as to why the return rate for 2017 The Coalition’s 2015–2020 strategic objectives
TEMFs had been so high. Dr Solomon replied are to: increase commitment to trachoma
that the TEMF response rate had been very elimination among donors and decision
high since 2014, but agreed that this was the makers; increase investment in trachoma 7
highest yet. He said that the TEMF format had elimination programmes; strengthen
been progressively revised to reduce the time capacity and human resources needed to
required for its completion and to maximize achieve trachoma elimination; coordinate
the value of the data collected. Redundant the provision of technical assistance and
questions had been removed. In addition, sharing of knowledge by its membership to
integration of the data collection process with support high quality outcomes in trachoma
the process for requesting donated azithromycin elimination programmes; and ensure that the
from ITI and reporting on its use in-country Coalition remained a strong partner within
means that endemic countries now receive one the Alliance. The Coalition’s members include
combined form about trachoma from WHO non-governmental organizations, research
and ITI per year, rather than the five that they and academic institutions, donors and private
received in 2013. Dr Solomon also said that sector organizations.
the ITI team works closely with WHO and
health ministries to ensure that the responsible The Coalition supported the development
individuals within each health ministry are of the Alliance’s current plan of action,
supported to complete the forms. He thanked Eliminating Trachoma: Accelerating Towards
all those involved for their hard work. Dr 2020 (12), which outlines what needs to be
Solomon indicated that the high response rate done to scale up programmes and strengthen
will make the dossier development process health systems to achieve the trachoma
easier, as information shared becomes part of elimination target. The document illustrates
the database that can be used to pre-populate the cost of implementing SAFE, presents a
the spreadsheet component of a draft dossier, strong economic case for investment and
which can then be reviewed and finalized by frames momentum against trachoma within
the health ministry. the broader sustainable development goal and
universal health coverage agendas.
Twenty_first_report_ok.indd 7 4/1/2019 9:58:50 AMPublished in July 2016, the document was backlog of trichiasis surgery to undertake. He
updated in April 2017 to include 2017 global said that Benin was implementing antibiotic
epidemiological data and other relevant MDA, but required external support for its
statistics, to ensure that it remained a useful trichiasis surgery programme in order to reach
tool for assessing progress and advocating GET2020 goals.
for support towards elimination. The updates
were contained in a stand-alone Appendix that Ms Sarah noted that Dr Batcho had raised
could be inserted inside the cover of the parent two very important issues: cross-border
document. transmission and the fact that all components
of the SAFE strategy need to be in place for
Implementation of the SAFE strategy is trachoma to be fully addressed. She said that
being achieved through collaboration and ongoing interventions in Nigeria should reduce
commitment from governments and their the burden of trachoma there, and commented
partners. Eliminating Trachoma: Accelerating that eliminating trachoma in one country
Towards 2020 includes a blueprint for action could have indirect benefits for neighboring
which recognizes the need for this collaboration countries. Ms Sarah also emphasized that
to continue to strengthen, allowing urgent some partners of the Alliance may be more
coordinated action to advance the GET2020 specialized in one component of trachoma
goals. than another, and that creating partnerships
and coordinating interventions was critical to
The updated document was approved by the achieving elimination.
Alliance by acclamation.
With less than four years left until December Regional reports
8 2020, Ms Sarah noted the period in which
the meeting was being held as a critical point
In the absence of a representative from WHO’s
in the campaign to eliminate trachoma as a
South East Asia Regional Office, Dr Promila
public health problem. She commented that
Gupta (representing India), Dr Hla Marlar
the Alliance was making astounding progress
(representing Myanmar), and Mr Sailesh
to reach its goals, and needed to ensure that it
Kumar Mishra (representing Nepal), delivered
engaged new partners to sustain momentum.
brief country-level reports.
Ms Sarah closed by noting that it would be her
India, Myanmar and Nepal each previously
last Alliance meeting as Chair of the Coalition,
had a public health problem from trachoma.
and asked meeting participants to join her in
In India, a series of surveys conducted in ten
welcoming Dr Serge Resnikoff as the incoming
formerly-endemic districts from 2014–2017
Chair.
found the district-level prevalence of TF in
1–9-year-olds to 0.1–2.1%, while the age- and
Discussion
gender-adjusted district-level prevalence of
trichiasis in ≥ 15-year-olds was 0.1–2.4% (42).
Dr Wilfrid Batcho, representing Benin,
Trachoma rapid assessments were conducted
expressed concern that after local elimination
in parallel in 17 other districts; very low
is achieved, trachoma might spread back to
proportions of children examined had active
Benin from Nigeria (37–40), a larger country
trachoma, and very low proportions of ≥
immediately bordering Benin to the East. He
10-year-olds had trichiasis (43). The country
noted that Benin had only two evaluation units
intended to strengthen its trichiasis surgery
(comprising four districts) in which the TF
programme in order to reach elimination
prevalence in 1–9-year-olds was ≥ 10% (41),
targets by 2020. Dr Hla reported that in
though the country still had a considerable
Myanmar, public health-level interventions
Twenty_first_report_ok.indd 8 4/1/2019 9:58:50 AMhad been successful in reducing transmission of from an integrated approach for eliminating
infection. While Myanmar still has individuals trachoma and other NTDs by combining
with trichiasis (44), it no longer required interventions from the health, water and
implementation of the A, F and E components sanitation, education, and other sectors in a
of SAFE to reach the elimination endpoint. coordinated way.
Myanmar hoped to conduct prevalence
surveys in 2017–2018, and to submit a dossier
Many countries nearing elimination targets
for validation of elimination of trachoma have health systems that are not prepared to
as a public health problem soon after thosesustain gains made through implementation
surveys are complete. Mr Mishra reported of the SAFE strategy. It is important that those
a small backlog of trichiasis in Nepal, which
countries receive external guidance on how to
no longer required implementation of the A,establish and maintain effective surveillance
F and E components of the SAFE strategy forsystems in the post-validation phase. The
trachoma elimination purposes. A request toWHO Regional Office is planning to work
WHO to validate elimination of trachoma as with countries to achieve the health-related
a public health problem was expected to occur
Sustainable Development Goals by 2030. If
in 2017 or 2018. a country in the region eliminates trachoma
by 2020, there will be more than a decade in
Dr Rabindra Abeyasinghe, Coordinator, which trachoma may resurface. The Alliance
Malaria, Other Vectorborne and Parasitic should develop a post-validation strategy for
Diseases, Western Pacific Regional Office, countries, which should include methods for
WHO. disease surveillance.
Trachoma was believed to be, or to have recently Dr Simona Minchiotti, Medical Officer, Non
been, a public health problem in ten countries Communicable Diseases, Africa Regional Office, 9
in the Western Pacific Region. Cambodia (45), WHO
China and Lao People’s Democratic Republic
(46) had all already claimed to have eliminated The African Region bears the largest burden
trachoma as a public health problem. of trachoma globally (1). The prevalence of
Implementation of the antibiotic component of TF was ≥30% at most recent survey in areas
the SAFE strategy covers all endemic districts of Democratic Republic of the Congo (53),
in Australia (47, 48), Solomon Islands (15, 19) Guinea, Kenya (54), South Sudan (55), United
and Vanuatu (17). As of April 2017, antibiotic Republic of Tanzania (56) and Zambia,
MDA had not been started in Fiji (15, 49-51), indicating that implementation of the A, F
Kiribati (15, 16), Papua New Guinea (21), or and E components of the SAFE strategy are
Viet Nam (52). Progress towards elimination needed for at least five years before re-survey.
in these countries may be impeded by the The countries with the highest national-level
distribution of the affected populations, which trichiasis backlogs include Chad, Democratic
are scattered, remote and often difficult to Republic of the Congo, Ethiopia and Nigeria
access; political focus on other priorities; and (1). Gambia (57, 58) and Ghana (59, 60) claim
limited donor support for improving access to to have eliminated trachoma as a public health
WASH. problem, and plan to submit dossiers for
formal validation of elimination in 2017.
Many Pacific Island countries have experience
of undertaking successful preventive Since its launch in May 2016, ESPEN has
chemotherapy campaigns for the elimination supported efforts to improve access to NTD
of lymphatic filariasis, which should make local data and enable data sharing. Increased
populations receptive to antibiotic MDA for collaboration between country governments,
trachoma. Countries in the region can benefit donors and partners has helped to coordinate
Twenty_first_report_ok.indd 9 4/1/2019 9:58:50 AMmapping and SAFE interventions. Many trachoma mapping. Mapping in Afghanistan
countries report a lack of communication and Somalia is expected to begin in 2017.
between programmes for other NTDs and The Islamic Republic of Iran is expected
the trachoma programme. Insufficient to soon prepare a dossier in line with the
coordination between these programmes may standard operating procedures for validation
increase costs and make it more difficult to published by WHO (23). The WHO Eastern
secure funding. Several countries in the region Mediterranean Regional Office target for 2019
are experiencing political instability and poor is to have at least four additional countries
security conditions which impede public validated for trachoma elimination, possibly
health programmes. These limitations must including Djibouti, Iraq, the Islamic Republic
be addressed in order to survey unmapped of Iran and Saudi Arabia. The target for 2021 is
regions, introduce interventions, and integrate to have at least six more countries validated for
surveillance into existing health systems. trachoma elimination. These targets have been
endorsed by the Regional Director.
Discussion
Socio-political conflict and unrest, complex
Mr Martin Kabore, representing Burkina emergencies and insecurity are major
Faso, asked what source data were used for challenges in about one-third of countries in the
determining national trichiasis backlogs. Dr region, influencing priority-setting for health
Minchiotti replied that trichiasis backlog care. SAFE interventions have been mostly
estimates were determined from population- undertaken without external donor support.
based prevalence survey data shared with It has been a challenge to facilitate stronger
WHO. networking and developing of partnerships,
participatory planning and comprehensive
10 Dr Ismatullah Chaudhry, Medical Officer, approaches in programme implementation in
Prevention of Blindness, Eastern Mediterranean order to increase productivity and create better
Regional Office, WHO. outcomes. It is important to address weak
health management information systems and
Six countries are believed to be trachoma compromised surveillance systems in most of
endemic in the Eastern Mediterranean Region. the region’s trachoma-endemic countries.
Egypt, Pakistan and Sudan (61, 62) have
undertaken at least some baseline trachoma Dr Martha Saboya, Advisor, Neglected Infectious
mapping. In these countries, surgeons trained Diseases Epidemiology, WHO Regional Office
to undertake trichiasis surgery are beginning for the Americas.
to address trichiasis backlogs in districts
where the prevalence of trichiasis is ≥ 0.2%, Mexico has become the first country in the
and there is engagement with ITI concerning Region of the Americas and the third country
an azithromycin donation, in order to facilitate in the world to be officially validated as
MDA in districts where the prevalence of TF is having eliminated trachoma as a public health
≥ 5%. Yemen has recently completed trachoma problem (30). Mexico has zero new cases of
mapping (63) and urgently requires surgery trichiasis unknown to the health system.
and antibiotics interventions, but insecurity
has delayed implementation. Afghanistan However, trachoma remains endemic in at
and Somalia still need to undertake mapping. least 136 districts across Brazil, Colombia and
Based on trachoma rapid assessment data from Guatemala. Overall, 5 million people live in
eye outreach camps and hospital registries in these endemic districts, and a large proportion
Afghanistan, 25 districts across 19 provinces of them live in 128 known-endemic districts
are prioritized for mapping. In Somalia, 12 in Brazil.
districts from six regions are prioritized for
Twenty_first_report_ok.indd 10 4/1/2019 9:58:51 AMAbout 285 000 people in Brazil, some of The Pan-American Health Organization’s
whom live in indigenous communities, regional trachoma forum takes place
received antibiotic treatment in 2016 (1). biennially, allowing experts from various
Facial cleanliness interventions are being organizations to share recommendations and
delivered as part of an integrated campaign country representatives to share progress on
against leprosy, schistosomiasis, soil- SAFE implementation (64).
transmitted helminthiases and trachoma, and
environmental improvement is being funded There are several challenges that still need to
through local investments in WASH. be addressed in the region. Mapping needs to
be conducted in countries with populations at
Colombia has expanded mapping in districts risk of trachoma but which are not currently
surrounding its known focus in Vaupés, proven to require interventions. In 2017, Peru
delineating four newly-characterized endemic will complete a baseline survey for trachoma
districts. It is now carrying out active case that will also include collection of data on soil-
finding of trichiasis. Colombia is undertaking transmitted helminth infections, but may then
antibiotic MDA interventions across its six require additional support to complete further
known-endemic districts, with interventions mapping. Indigenous populations are at greater
to promote facial cleanliness being delivered risk of trachoma than non-indigenous groups,
concurrently, both in schools and at village- but high costs and limited access to these
level. Interventions to improve WASH are populations makes mapping difficult. The
being financed by various stakeholders. plan is to conduct population-based surveys
Guatemala will carry out impact surveys from in several countries in areas covered by the
April to May 2017. Amazon rainforest. Standardized training of
graders is currently difficult and costly, and
Guatemala is in the pre-validation surveillance endemic countries have trouble affording 11
phase. It had only two trachoma-endemic it. In Mexico, tools and procedures for post-
districts. Village health workers promote validation surveillance have not yet been
facial cleanliness, and water and sanitation defined. There is therefore a risk of undetected
improvements are led by the community. recurrence in populations following validation,
and a system for picking up and notifying
In the Americas, it is currently recommended recurrence needs to be created.
that, to ensure high quality, trichiasis surgeries
be performed by ophthalmologists or The Alliance applauded the success of Mexico,
oculoplastic surgeons. In areas suspected to Morocco and Oman in being validated as
be endemic for trichiasis, active case-finding is having eliminated trachoma.
preferred to passive detection.
Twenty_first_report_ok.indd 11 4/1/2019 9:58:51 AMSESSION 2
Trachoma Scientific
Informal Workshop
The Trachoma Scientific Informal Workshop 5. There is ongoing work to assess the role
had taken place on 18th April 2017, at of serology for use in trachoma surveys
WHO Headquarters. Dr Solomon presented as a tool to understand community
highlights of the Workshop for the information transmission (29). Researchers are
of the Alliance. looking to partner with national
programmes in ongoing work.
12 1. While programmes should aim for 6. New cases of conjunctival scarring may
100% coverage when undertaking continue to appear for at least four years
azithromycin MDA, at least 80% after the prevalence of TF in 1–9-year-
coverage in children has been shown olds has been reduced toQuestions Surgery for GET2020 Panel
One participant asked for clarification on
the role of supervisors in the provision of
Reducing the Trichiasis Backlog
trichiasis surgery. Dr Solomon answered that
Dr Dézoumbé Djoré, Coordonnateur du
supervisors have a number of important roles,
Programme National de Lutte Contre la Cécité,
and in the interests of time, suggested that
Chad
details be sought in the report on the Second
Global Scientific Meeting on Trachomatous
Trichiasis (68). In Chad, trichiasis is a public health problem
in 11 districts with a collective 2.5 million
Another participant asked whether inhabitants. In the district of Mongo, impact
programmes should continue to use two- survey results suggest that the prevalence
dimensional photographs for training graders of trichiasis decreased from 6.2% in 2015 to
to recognize trichiasis. Dr Solomon responded 1.2% in 2017. There are currently an estimated
that training using three-dimensional 63,888 cases of trichiasis nationally that require
photographs was still in development, so corrective surgery. To reduce the prevalence
existing training systems should continue to everywhere to below the elimination
be used until further notice. threshold, the programme needs to manage an
13
© Sightsavers
Twenty_first_report_ok.indd 13 4/1/2019 9:58:51 AMestimated 35,106 individuals with trichiasis, In 2009, surveys were undertaken using a
using a combination of fixed and mobile non-standard integrated mapping approach
surgery teams. In 2014, 2281 individuals with (69). In three districts in which those surveys
trichiasis were managed. In 2015, 9569 cases of suggested an elevated prevalence of trachoma,
trichiasis were managed. In 2016, 17,809 cases cluster-sampled surveys were implemented
of trichiasis were managed, representing 51% in 2011. Very little active trachoma was
of the calculated backlog at that time. Guera, found. District-level prevalence of trichiasis
Salamat, Ouaddai regions are thought to still in women aged ≥15 years was ≥0.2% in two
require surgery interventions in order to reach districts, Binah and Blitta.
elimination prevalence targets.
Subsequently, two strategies have been used
A survey of districts with active surgery to find and address prevalent trichiasis
programmes indicated that 89% of operated cases. The first approach required healthcare
individuals were followed up post-operatively. workers in rural settings to report detection
The incidence of post-operative complications of any new cases of trichiasis. This passive
was 2%. Additional surveys were carried out surveillance system had low sensitivity, and
in other districts to determine the prevalence may have provided limited information. Using
of trichiasis and number of cases requiring this approach, 17 cases of trichiasis were
operation. Results showed 26 new endemic detected, of which 16 had surgery. The second
districts with 9703 new cases of trichiasis to approach, implemented with support from
manage in a population of 5.5 million people. the Bill & Melinda Gates Foundation, was a
Trichiasis endemicity in these districts ranged form of active surveillance involving door-to-
from 0–1.2%. door visits by community health workers or
ophthalmic nurses. This approach was more
14 In order to address the trichiasis backlog in sensitive, and able to detect cases that existed
Chad, graders are being trained to detect in remote areas. However, it was costly, labor
trichiasis, and surgeons are being certified. intensive and difficult to sustain over time.
Trichiasis case-finding is conducted on a door- This approach detected 203 cases of trichiasis,
to-door basis. The Ministry of Health plans to of which 158 had surgery. Some of the detected
continue interventions in the 11 districts that cases did not consent to the operation. Reasons
have completed mapping, and conduct surveys cited for refusing surgery included being too
for trichiasis in the remaining 26 districts. old, being afraid of the procedure, or being
unable to afford the operation. Patients also
Getting the Trichiasis Backlog to refused surgery if their families were resistant
to them doing so.
Zero
A review meeting was held in Lomé, Togo, from
Dr Marcel Awoussi, Togo
1–2 March 2017. The meeting recommended
that all previous and ongoing data from routine
Trichiasis is not a common presentation in trichiasis surgeries at health facilities, surveys
Togo. To help develop a dossier for validation and screening initiatives be collated to inform
of elimination of trachoma as a public health decisions on where to undertake further
problem, prevalence data collection is a very population-based surveys. Those surveys are
important concern. In some areas, people intended to be completed by the end of 2017,
working in the health sector are simply not with the support of Tropical Data and funding
aware of the disease. Data on trichiasis are from USAID, to allow for subsequent planning
not routinely recorded at local health centers. and action.
Twenty_first_report_ok.indd 14 4/1/2019 9:58:51 AMQuestions or 67% of the trichiasis backlog, would need
to be managed by 2020, in order for this to
OA participant asked Dr Djoré for clarification occur. There are currently 14 trainers and 175
on the methodology used to estimate the ophthalmologists trained to deliver trichiasis
prevalence of trichiasis. A question to both surgeries in the country. The Ministério da
speakers asked what was being done to ensure Saúde is now working to build health system
that surgery interventions were effective in capacity by training more surgeons and health
preventing vision loss. personnel. The trichiasis surgical service has
been integrated into local hospital services,
Dr Djoré responded that in 2004, the trachoma and people with trichiasis are being offered
survey performed in Chad was carried out transport to the nearest hospital offering
in a sample of 27 villages in one region (70). surgery free of charge. Local health centers
Surveys were later conducted in three other are continuing to undertake surveillance for
regions. In 2013, the Ministry of Health additional cases of trichiasis.
began surgical activities in all four regions
(11 districts) that had completed trachoma The TT patient tracking app
surveys. In 2014, 41 evaluation units were
surveyed, and 29 had trichiasis prevalence Dr Michael Masika, Ministry of Health, Malawi
estimates which indicated a need for public-
health-level surgery interventions (71). Dr
The Trichiasis Patient Tracking Application
Djoré added that post-operative follow-up
was created in order to address the lack of
was undertaken for all patients. Patterns of
standardized trichiasis monitoring tools.
recurrence and other data were used to inform
Before it was launched, different partners
refresher training for surgeons.
used different tools to monitor output of 15
interventions against trichiasis, and many of
Dr Awoussi said that ophthalmic nurses from
those tools overlapped geographically. Post-
Togo received training to undertake trichiasis
operative patient follow-up was challenging.
surgery in Mali, plus supplementary training
It was difficult for surgeons to provide
in Ghana to correctly assess trichiasis cases.
supervision and support to their patients.
Funding was also being used to provide
Reporting of trichiasis case identification
additional training to surgeons to ensure that
and of surgical delivery did not occur in
they were able to deliver quality surgeries.
timely fashion. These issues created a need
to develop a common system for registering
Transitioning Trichiasis Care into patients with trichiasis, tracking them through
Routine Services to the operation and through their post-
operative follow-up course, and making data
Dr Marilia Messangaie, Mozambique available at all levels of service delivery. As a
solution, WHO held a consultation (72) to
In 2014, the Queen Elizabeth Diamond Jubilee develop a target product profile for a standard
Trust launched an initiative to support the system, which has since been produced and is
Ministério da Saúde to reduce the backlog being piloted in Chikwawa, Malawi. Patient
of trichiasis throughout Mozambique. The registration, surgery and follow-up data are
aim was to achieve 100% coverage across collected on smartphones. The application uses
the 50 districts in which the prevalence of data entry fields modeled on standard forms
trichiasis exceeded the elimination prevalence developed by the International Coalition for
threshold. An estimated 11,709 individuals, Trachoma Control. Patients are tracked using
Twenty_first_report_ok.indd 15 4/1/2019 9:58:51 AMidentification numbers. Data are made available The Morbidity Management and
online for supervisors to plan outreach and Disability Prevention Project
oversee each surgeon’s performance. The
application can be customized as needed to Dr Joe Amon, Helen Keller International.
be interoperable with other databases or other
reporting forms used by national programmes.
The Morbidity Management and Disability
In Malawi, the government will maintain
Prevention Project is a five-year initiative
the system and make data freely available to
funded by USAID to help support efforts in
its partners. This tool will be very useful for
Burkina Faso, Cameroon and Ethiopia to
trichiasis programmes. It is faster and less
eliminate trachoma and lymphatic filariasis
prone to error than paper-based monitoring
as public health problems. The project works
methods. The application can facilitate
to increase availability of quality data for
planning by producing reports of patient
decision-making, increase support for scale-
surgery and follow-up status, organized at
up in implementation, improve quality,
different administrative levels. Downloadable
strengthen capacity within health ministries
summary statistics make it easier to report
and strengthen the evidence base for preferred
programme output to donors and partners. The
practices in morbidity management and
Blantyre Institute for Community Outreach,
disability prevention. For trachoma, tools
Tropical Data, and WHO were acknowledged
and resources developed or augmented by the
for their work in developing this tool.
project include those on infection control and
waste management, supportive supervision,
Questions
epilation, trichiasis surgeon training and a
procurement calculator to determine the cost
The first question addressed to Dr Masika
of surgeries in order to support programme
16 was whether the application uses free, open-
managers.
source software. A follow-up question asked
which other programmes can benefit from this
To date, the project has made good progress
application. A third question asked whether
towards reducing trachoma morbidity in
the data being uploaded from the app were
the three participating countries. More than
secure.
200 trichiasis surgeons have been trained,
300,000 people have been screened, and
Dr Masika asked Dr Khumbo Kalua (Blantyre
25,000 surgeries have been completed. The
Institute for Community Outreach) to help
project supports post-operative follow-up
respond to these questions. Dr Kalua noted
of patients, which is critical both for the
that the application was not open-source. The
patients themselves and to provide feedback to
pilot testing in Malawi had been an excellent
surgeons for continuous quality improvement.
opportunity to refine the system, and the
In Cameroon, the project has supported the
aim was now to undertake a second round of
Ministre de la Santé publique to measure
testing in Ethiopia. The intention is to then
the prevalence of trichiasis more precisely,
make the system available to any country that
and implementation data have been used as
would like to use it. The data are stored and
a tool for sub-district-level trichiasis service
transferred fully encrypted.
Twenty_first_report_ok.indd 16 4/1/2019 9:58:51 AMYou can also read