THE SILENT PANDEMIC The Impact of the COVID-19 Pandemic on the Mental Health and Psychosocial Wellbeing of Children in Conflict-Affected ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

THE SILENT PANDEMIC The Impact of the COVID-19 Pandemic on the Mental Health and Psychosocial Wellbeing of Children in Conflict- Affected Countries

ACKNOWLEDGEMENTS This report was prepared by World Vision and War Child Holland. Lead authors: Nadine Haddad, Eamonn Hanson and Phiona Naserian Koyiet. We would also like to acknowledge and thank all the children, adolescents and young people, parents and carers and child protection experts and community leaders who participated in this study in six conflict-affected countries: Colombia, the Democratic Republic of the Congo, Jordan, Lebanon, the occupied Palestinian territory and South Sudan. Special thanks to Mirette Bahgat, Erica Hall, Mallissa Watts, Dr Unni Krishnan, Kate Shaw, Ridiona Stana, Ruba Abumraighi, Iman Bahri, Micah Branaman-Sharma, Juan Jose Castellanos, Gloria Camilo, Henriette Diaka, Heba Ghalayini, Linda Abu Al Halaweh, Patient Harakandi, Lyndsay Hockin, Jasem Humeid, Ahmed Jaber, Florence Kiff, Chimere Kiombwe, Larissa Koekoek, Jeroen Kostense, Johnson Lafortune, Marianna Narhi, Kenneth Miller, Dane Moores, Carsten Bockemueuhl, Eric Numubona, Martin Omoro, Abedi Ramazani, Franck Tsaf, Faith Mathenge, Vanessa Saraiva, Eva Smallegange, Sahar Smoon, Sara Valerio, Anne Marie Connor, Mesfin Loha, Maha El Sheikh, Laura Miller, AnneMarike Smiers, Flutra Gorana and Don McPhee. The names of all children and adults quoted in this report have been changed to protect their identities. Design: Diana De León Editor: Karen Homer Cover photograph: ©2020 Katherine Maldonado/ World Vision – a young girl in Colombia World Vision and War Child would appreciate receiving details of any use made of this material in training, research, program design, implementation or evaluation.

THE SILENT The Impact of the COVID-19 Pandemic on the Mental Health and
PANDEMIC Psychosocial Wellbeing of Children in Conflict-Affected Countries
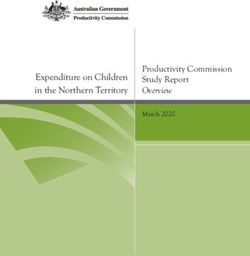
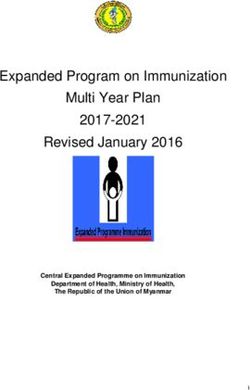
We spoke to: In six conflict-affected countries, to see how they had been affected by COVID-19.
220
children
287 OCCUPIED LEBANON
parents and PALESTINIAN
carers TERRITORY JORDAN
SOUTH
COLOMBIA SUDAN
245 44
adolescents and
young people child protection DEMOCRATIC
experts and REPUBLIC OF
community leaders THE CONGO
of children living in conflict-affected regions said they were Overall:
12%
continuously feeling extremely sad and fearful, and could
be at risk of developing moderate to severe mental health 38% 25%
disorders such as depression and anxiety. of children and did not
young people express their
This is a 33% Prior to the pandemic, World Health Organisation
estimated 9% of children and adults in conflict
increase
feel sad and
fearful.
emotions at
all.
settings1.
38%
Most children and parents feared contracting COVID-19
themselves or that relatives may die from the virus. 40%
of children and 48% of parents indicated that COVID-19 children also identified family poverty and
is the main risk affecting their emotions. food security as a chief concern.
Children and young people were affected as parents noticed changes in their relationships with their
services became less available due to the
pandemic: 44% children, including children’s aggressive behaviour, and stress
and pressure on both children and parents.
What children said they needed:
1.2% 0.3%
Almost
72% 65% health services
90% struggled to access to
family support
57%
could not go access services playgrounds
to schools and activities 17.5% psychosocial support. This rose to 70% for
displaced children, three times the pre-COVID-19
education estimate of 22%1. This means 456 MILLION
CHILDREN WORLDWIDE ARE CURRENTLY
24% LIKELY TO BE IN NEED OF MENTAL HEALTH
AND PSYCHOSOCIAL SUPPORT.
basic services
42% 38%
health centres
access
11%
water
Children especially wished for sports, play,
family (especially parents), peace (addressing
closed to food armed conflict), and the opening of schools.
USD 1.4 billion is needed to provide mental Currently, funding for mental health and
health and psychosocial support to the 456 psychosocial support makes up JUST 1% of
million children living in fragile and all humanitarian health funding.
conflict-affected regions.
1
Charlson, F., van Ommeren, M., Flaxman, A., Cornett, J., Whiteford, H., & Saxena, S. (2019). New WHO prevalence estimates of mental disorders in conflict settings: a systematic review
and meta-analysis. The Lancet, 394(10194), 240-248.
EXECUTIVE SUMMARY
The mental health and wellbeing of psychosocial support as a direct
children living in conflict-affected result of the COVID-19 pandemic
countries is dangerously deteriorating and lockdowns. This rises to 70%
as they struggle to cope with the for refugee and displaced children
socio-economic fallout of the as opposed to 43% for children in
COVID-19 pandemic. Having survived host communities.
life-threatening, life-altering conflicts,
their ongoing fear, trauma and chronic
stress is compounded by the daily
anxiety, uncertainty and hardship
This finding could
produced by the pandemic.
indicate that 456 million
These children are best placed to children worldwide
articulate their worries and concerns are currently likely to
about the devastating toll that
COVID-19 is taking on their mental need mental health and
health and their future, as well as its psychosocial support.2
insidious impact on their families and
communities.
• Children and young people (38%)
To better comprehend this alarming, say they are feeling sad and fearful,
underreported global situation, with 12% on the extreme end of
World Vision and War Child Holland continuously feeling sad and fearful
spoke to 220 children, 245 adolescents who may be at risk of developing
and young people, 287 parents mental health disorders, such
and carers and 44 child protection as depression and anxiety. This
experts and community leaders in six is higher than the World Health
conflict-affected countries: Colombia, Organization’s estimate of 9%i of
the Democratic Republic of the young people and adults combined
Congo (DRC), Jordan, Lebanon, the experiencing extreme distress in
occupied Palestinian territory and conflict settings.
South Sudan. The interviews took
place between August and December • The children’s feelings stem from
2020 across refugee camps, shelters complex daily worries. Most
for the displaced people and host children and parents feared
communities. contracting COVID-19 themselves
or that relatives might die from the
The findings of this consultation, as virus. 40% of children and 48% of
summarised below, are startling and parents indicate that COVID-19
deeply concerning and need urgent is the main risk affecting their
action. emotions. Children are anxious
about school closures, interrupted
• More than half (57%) of children access to basic services and their
living in fragile and conflict- families’ economic hardships
affected countries expressed due to COVID-19 containment
a need for mental health and measures. Some shared that they
1
n=480 children and young people were interviewed, 15 did not provide an exact age and considered
missing for the age analysis. Age categories: 7-14; &15-18 (for children), and 19-24(for adolescents)
2
Based on data collected for this report, if 57% children and young people who need psychosocial
support is applied to all 800 million children in fragile and conflict-affected areas globally, it could
indicate that 456 million children are in need of psychosocial support worldwide.
4 THE SILENT PANDEMIC
have gone hungry after parents services. They mentioned schools
lost their jobs. most frequently as being less
available (89.2%), followed by
• Children (aged 7-14) confided
services and activities (70.9%),
that they turn to trusted friends
playgrounds (65.0%), health
and family members for emotional
centres (41.9%), food (38.1%)
support (86%), but youth (aged
and water (10.6%). COVID-19
19-24) are struggling to cope with
containment measures have also
the distress on their own. Less
hampered community-based
than half (41.8%) say they have
child protection, prevention and
someone they can look to for help.
monitoring activities, putting
• More than half of the parents children even more at risk.
(51.2%) reported changes in how
• Children identified family poverty
their children spend their days in
and food insecurity (38.1%) as
the community since the start of
a chief concern. For displaced
the COVID-19 pandemic. Of the
children or those living in
parents, 44.3% noticed changes
conflict zones, their parents’ and
in their relationships with their
caregivers’ job loss puts them
children, including children’s
at grave risk of food insecurity,
aggressive behaviour, and stress
forcing them to resort to negative
and pressure on both children and
coping mechanisms and potentially
parents.
resulting in violations of their
• Children and young people rights and protections. This in turn
emphasized the negative effect on contributes to their increased
their mental health and wellbeing sense of helplessness and stress.
of disrupted access to critical
©2020 Scovia Faida Charles / World Vision - Gloria, 13, is thrilled to be back in school again. During the closures at
the height of the pandemic, three of her friends were married.
THE SILENT PANDEMIC 5
RECOMMENDATIONS
Data from this study reveals that is estimated to go toward meeting
children’s mental health and well-being these needsiii and to addressing the
is deteriorating significantly across factors and root causes that fuel these
all six countries surveyed. The global vulnerabilities.
implications are clear: Unless this
hidden crisis is urgently addressed, World Vision and War Child are
a generation of the world’s most calling on governments, inter-
vulnerable children will likely suffer governmental agencies, donors,
devastating lifelong and potentially foundations, INGOs, media, businesses
life-threatening consequences. and individuals to prioritise mental
health and psychosocial wellbeing in
In 2021, an estimated USD 1.4 billion all COVID-19 recovery initiatives and
is required to provide urgent mental humanitarian response plans. (For the
health and psychosocial support for full recommendations, see page 27.)
456 millionii children living in fragile Parties to Conflict must take immediate
and conflict-affected regions3. Funds measures to end conflicts through
allocated to integrating mental health peaceful, diplomatic and political
and psychosocial support in emergency solutions. This is the most important,
responses are still woefully inadequate. critical step in addressing the rising
Although 20% of emergency health mental health crisis faced by children
care needs in crisis contexts involves in contexts affected by conflict and
mental or psychosocial health, less COVID-19.
than 1% of all humanitarian funding
©2020 Salam Qumsiyeh / World Vision – children return back to school after the long lockdown in central West Bank.
3
Based on the Lancet figures corrected for inflation. Lancet Global Mental Health Group, the required
$2 per child for scale up in 2007 would equal $3.07 in 2021. Multiplied by 456 million children, the
figure is approximately 1.4 billion USD.
6 THE SILENT PANDEMIC
© 2020 Marc Aj / World Vision – His mum says that Chaib, 5, has been struggling with the lockdown restrictions in
Lebanon, but looks forward to his psychosocial support sessions.
• The United Nations must peacebuilding initiatives.
ensure a dedicated sub-section
• Humanitarian actors must ensure
on MHPSS in all humanitarian
that MHPSS is integrated across
appeals (Humanitarian Response
all sectors, including protection,
Plans, Refugee Response Plans)
education, livelihoods and
with set targets for children and
nutrition, and that children,
other affected people, funding
youth, caregivers, families
and reporting. This allows the
and communities play a role in
international community to
determining and designing the
highlight and prioritise the
services needed to support their
MHPSS needs of conflict-affected
individual and collective wellbeing.
populations and track allocated
funding and gaps. • Governments must draft national
mental health strategies that
• Donors must adopt MHPSS
centralise children’s mental health
as a priority in aid strategies,
and psychosocial wellbeing.
recognising it as a right for children
This includes specific lines in
and their families, as a life-saving
health, education and child
intervention in emergency
protection budgets to support
responses and in long-term
the implementation of locally led
recovery and development work,
MHPSS services.
as well as a critical component in
THE SILENT PANDEMIC 7
©2020 Scovia Faida Charles / World Vision - ‘Aunty’ Sarah listens to John, 7. A social worker in South Sudan,
Sarah provides psychosocial support and advice to parents and children.
8 THE SILENT PANDEMIC
01
INTRODUCTION
Conflict, displacement and COVID-19: life for
the world’s most vulnerable children
As the world enters the second year of the COVID-19 pandemic, millions of
conflict-affected children and their families are marking some additional grim
milestones:
8 of conflict in
South Sudan
10 of war in Syria and refugee
crisis in neighbouring
of instability
NEARLY and conflict
54
YEARS YEARS countries in the
Democratic
20
YEARS
of military occupation and
conflict in the occupied
Palestinian territory
52
YEARS
of conflict in
Colombia
YEARS Republic of
the Congo
(DRC)
Children are disproportionately Particularly in the country’s eastern
affected by conflict. Globally, an zone, community health centres and
estimated 800 million children live in schools have been looted, homes
fragile and conflict-affected areasiv, burned and whole villages destroyed,
one in six children live in conflict- forcing children and families to flee to
affected areasv and more than 30 survive. During the fighting, children
million have been forcibly displacedvi,vii. have witnessed friends and family
Many have been separated from members being hacked to death.
their caregivers, endured or
witnessed unspeakable violence, The DRC is known to have the world’s
sustained injuries and faced the risk poorest health system, a situation
of recruitment into armed groups. that has been exacerbated by the
Many more are denied access to basic country’s battle with Ebola, cholera
services, including clean water, food, and now COVID-19. Today, more than
education and healthcare. 27.3 million people, including nearly 4
million children under age 5ix, across
Conflict and displacement can have the country are facing high levels of
devastating and lifelong effects on food insecurity.
children’s mental, emotional and
physical health. Bombardments, Similarly in South Sudan, during the
attacks, occupation and being forced COVID-19 pandemic children and their
to flee erode their sense of safety. The families are facing increased protection
risk of being injured or maimed due to risks from rising inter-communal
conflict results in acute fear. conflict, as well as grave food insecurity
and malnutrition.
In the DRC, more than 3 million
children have been displaced, half The country’s chronically
of them in the last 12 monthsviii. underdeveloped health system is often
THE SILENT PANDEMIC 9
unable to meet the most basic primary disease outbreaks have demonstrated
health needs for child survival. Mental that the rates of distress and mental
health conditions are widespread and health conditions increase dramatically
go largely untreated. A recent Food during public health emergencies.
Security Nutrition Monitoring System The Ebola outbreak in West Africa
(FSNMS)x assessment found that 30% in 2013-2016 affected the physical
of children exhibited behavioural health of more than 28,000 people
change, showing signs of distress due and the mental health of countless
to repeated exposure to conflict and more. The World Health Organization
shocksxi. (WHO) concluded the outbreak had
psychological consequences at the
Children, such as those in the DRC individual, community, national and
and South Sudan, who experience regional levels, both acutely and in the
extraordinary levels of distress are long termxvii.
at greater risk of developing chronic
mental health disorders or psychosocial Like the Ebola outbreak, the COVID-19
issues. Exposure to traumatic events pandemic and its related socio-
and toxic stress at a young age can economic implications are placing
alter a child’s brain developmentxii. additional stressors on children and
Exacerbated by previous traumatic their caregivers who live in fragile and
experiences, children affected by conflict-affected areas. In a recent
conflict are at heightened vulnerability update by the Global Protection
to experience high levels of stress when Cluster, 100% of the protection
encountering a new crisis. clusters reported psychological
distress of affected populations as
Inadequate Services being severe or extreme at the end of
2020.
Despite the enormous needs
worldwide, most children who require The underprioritising and underfunding
mental health and psychosocial support of mental health in humanitarian
do not receive it. National governments responses is a key barrier to supporting
spend only 2-4% of their national children affected by conflict. It is
health budgets on mental healthxiii. impossible to precisely calculate the
Services are limited and sometimes extent of MHPSS underfunding, as data
non-existent for children living in on funding allocated specifically to
fragile and conflict-affected regions. MHPSS are not earmarked or captured
There is less than one mental health systematicallyxviii.
worker for every 100,000 people in
low-income countriesxiv. Despite some Policymakers, governments and donors
increases in recent years, development do not prioritise mental health and
assistance specifically dedicated to psychosocial needs in humanitarian
mental health accounts for just 0.3% of settings. Funding for mental health
all health aidxv. continues to be inadequate in the great
majority of humanitarian and conflict-
For example, South Sudan, with a affected settings. Before the pandemic,
population of more than 10 million, has mental health programmes received
one eight-bed mental health hospital less than 1% of the funding earmarked
ward served by one psychologist. The for healthxix from global donors. In some
burden of providing the remaining countries, there are swift and diverse
mental health and psychosocial support responses to address mental health,
care falls to humanitarian actorsxvi. particularly through the development
While the NGO-run mental health and of national COVID-19 response
psychosocial support (MHPSS) services plans for mental health services,
employ qualified professionals and implementation of WHO guidance
experts, services only exist in certain and the use of digital platforms. This
areas and capacity is insufficient given signifies a welcome recognition of
the scale of need. the salience of mental health, but
this is not enough. Strong political
Addressing mental health issues is a commitment, clear policy directions
perennial challenge. However, previous and improved investments are urgently
needed to address the pandemic’s
10 THE SILENT PANDEMICimpact on mental health and to build by COVID-19 in conflict settings is
robust mental health and psychosocial particularly acute. Scaling services
services. If left unattended, the impacts to respond to the mental health and
will linger, derailing other efforts to psychosocial needs of children and
rebuild societies. youth is urgently required, but the
best way to protect them is to prevent
Resilient Children such distress in the first place. This
requires, first and foremost, ending
Children are remarkably resilient, wars through peaceful political
and with adequate support, they can and diplomatic solutions. It also
recover from the many compounded requires a commitment to strengthen
stressors that they encounter. children’s protective environments,
including schools and safe play spaces,
As the world seeks to rebuild community-based networks and
economies and health systems after access to basic services. Parents and
the COVID-19 pandemic, we must caregivers need to be equipped with
also invest in people’s mental health the skills to help their children through
so they and their communities can these difficult times. They also need the
recover and rebuild. While this is means to minimise household stressors
important in all contexts, the complex such as unemployment, food insecurity
stress faced by children affected and shelter.
Lebanon
In 2020, Lebanon endured multiple crises, including a massive explosion in Beirut’s port,
an economic collapse, rising political instability and the COVID-19 global pandemic. Of the
1.5 million Syrian refugees in Lebanon, about 78% lack legal statusxx, an increase from the
previous year. In the midst of this socioeconomic situation, COVID-19 awareness and access
to information and care is being pushed to the background. In addition, the number of street
children is increasing due to the socioeconomic crisis. They are exposed to child labour, child
marriage, and other forms of violence, as well as education gapsxxi. For children following online
education, success rates are low due to a lack of internet access and frequent power cuts.
South Sudan
After six years of civil conflict in South Sudan, more than 80% of the population lives below the
poverty line. Some 3.8 million people are forcibly displaced, and more than half of the population
requires urgent food assistance. Within the country, 1.6 million internally displaced people (IDP)
live in precarious conditions where physical distancing is impossible and access to basic services
extremely limited. Floods and locusts have ravaged the country, further worsening food security
and living conditions. The COVID-19 pandemic has resulted in a drastic decline in domestic
production and a sharp increase in living costs. School closures since the start of the pandemic
have left tens of thousands of children and youth without access to education. Remote and home
schooling are simply unavailable. Curfews, travel restrictions, market closures and lockdowns
are frequently imposed as the country tries to respond to the growing caseload. The restrictions
have led to increased idleness among youth and children, and the restricted movement of girls
and women who are at an even greater risk of gender-based violence. Girls and boys also face
increased risk of being recruited into armed groupsxxii.
THE SILENT PANDEMIC 11© 2020 Marc Aj / World Vision – Jude, 13, is excited to receive her psychosocial support kit. 12 THE SILENT PANDEMIC
02
METHODOLOGY
The report presents the experiences of effect of these compounded stressors
children in conflict-affected areas who on their mental health and their
are also dealing with COVID-19 and its resulting MHPSS needs. The project
aftershocks. The assessment adopted a gathered the perceptions of various
mixed-method approach to obtain both stakeholders, including children, child
quantitative and qualitative data. protection actors, faith leaders and
caregivers following Do No Harm
The project reviewed the impact of and safeguarding principles. Trained
the pandemic and related lockdowns staff used constructive questions to
on children, taking into account the interview consenting respondents
pre-existing conflict situations in who are part of continuous support
which they live, to determine the programmes.
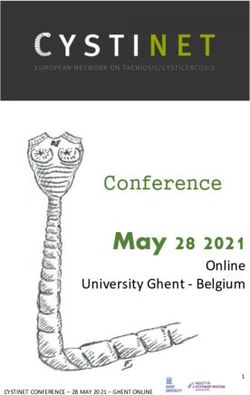
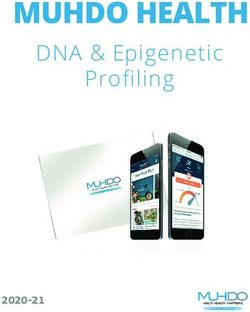
PARTICIPANTS IN THE STUDY
Demographic Frequency Percent
information (n) (%)
Region
Middle East 231 48.1%
220
children
170
adolescents
75
young people
Africa
South America
160 33.3%
89 18.5%
Country
(aged 7-14) (aged 15-18) (aged 19-24)
Jordan 80 16.7%
44
oPt 69 14.4%
287
child protection
experts and Lebanon 81 16.9%
parents community DRC 80 16.7%
leaders South Sudan 81 16.9%
Colombia 89 18.5%
The data collection took place between July and
Age group
December 2020 in six countries.
7-14 years 220 45.8%
15-18 years 170 35.4%
19-24 years 75 15.6%
Missing 15 3.1%
Gender
OCCUPIED LEBANON Male 236 49.2%
PALESTINIAN
TERRITORY JORDAN Female 244 50.8%
Location status
SOUTH
SUDAN
Refugees, IDPs,
COLOMBIA
Returnees and 252 52.5
others
Members
DEMOCRATIC
REPUBLIC OF
of host 228 47.5
THE CONGO community
4
n=480 children and young people were interviewed, 15 did not provide an exact age and considered
missing for the age analysis.
5
There is no conflict in Jordan, however, the country is impacted by regional conflicts, mainly Syria and
is hosting thousands of refugees.
THE SILENT PANDEMIC 13©2021 Elias Abu Ata / World Vision – Ayman, 20, struggled with his education since fleeing Syria in 2014. 14 THE SILENT PANDEMIC
03
FINDINGS
Children who have previously experienced traumatic events are more
vulnerable to new stressorsxxiii. The stress of the COVID-19 pandemic
may resemble past traumatic experiences, such as bombings, escapes or
conflict events. Fear of death, destruction, injury and loss of loved ones
may resurface. Some children may not be stressed by COVID-19 itself,
but by the memories and emotions that the situation evokes.
The children participating in this study More than one third (38%) of
reported significant levels of distress children surveyed expressed
and support needs. They identified key sadness and fear; 12% feel
areas of concern, as outlined below. this continuously, putting them at
risk of developing long-term anxiety
1. Fear, sadness and risks and depression. Of the children
interviewed, 25% did not express being
of children and young happy or unhappy, their silence may be
people a silent siren.
“Being safe is a “We are still in the midst
challenge. I am of the COVID-19 crisis
constantly scared. and infection remains
Scared of people and a great risk for the
what happens in my community.”
country. Now poverty
Kiyombele,
also scares me.” 15-year-old boy
Amina,
16-year-old girl Children are constantly fearful having
survived or witnessed war and conflict,
including abuse in the community,
Living through conflict and forced and/or early marriages, and
displacement, compounded by rape and domestic violence. Children
the pandemic’s consequences and identified COVID-19 (fear of the virus),
restrictions, was found to have abuse, armed conflict, violence6 and
significantly affected children’s mental poverty as the main risks during the
and emotional wellbeing. pandemic. (See Figure 1).
6
In oPt violence was mainly related to occupation
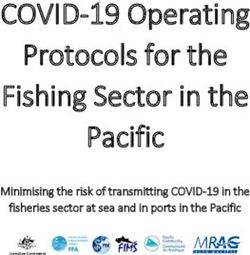
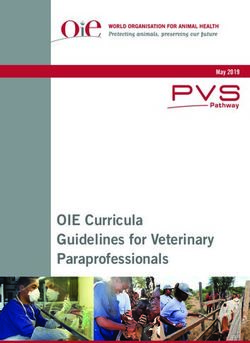
THE SILENT PANDEMIC 15FIGURE 1: Risks reported by children and parents
Poverty
Gang/Criminal violence
Domestic abuse
Confict/war
COVID-19
0.0% 10.0% 20.0% 30.0% 40.0% 50.0% 60.0%
Parents Children
Most children and parents feared on the extreme end according to this
contracting COVID-19 themselves or report data, is an indication that 12% of
that relatives may die from the virus. children in all conflict-contexts across
the board could be at risk of developing
40% of children and 48% of mental health disorders, such as
parents indicate that COVID-19 depression and anxiety. This is higher
is the main risk affecting than the World Health Organization’s
their emotions. The lack of access estimate of 9% of young people and
to education due to school closures adults combined experiencing extreme
was linked with increased teenage distress in conflict settingsxxiv.
pregnancies, domestic abuse, diseases
and accidents, isolation, as well as This finding highlights the severity of
idleness, homelessness, and forced and the compounded impacts of the conflict
early marriages. and COVID-19 on children, and the
urgent need for age -and context-
Research has shown prolonged fear appropriate mental health services.
and anxiety, with limited opportunities
to act, may result in learned
helplessness and depression. The study
found that 37.7 % of children feel sad
and fearful, with 12 % on the extreme
end. The 12% of children who are
“Before the pandemic,
children were at risk
of exploitative labour,
exploitation, sexual
“Domestic violence, violence and forced
and forced and early marriage. These days, all
marriage are the biggest these risks still exist, but
risks children are facing are magnified leading
in the country.” to increased trends in
emotional aggressions.”
16-year-old boy in South
Sudan Catholic priest, DRC
16 THE SILENT PANDEMIC2. Support needs
(disaggregated by age
and vulnerability) “We need to be
psychologically and
Children participating in the study
ranked the five areas of support they materially assisted, and
need most. More than half of those for the security situation
aged 7-17 (57%)7 said they needed
psychosocial support8; 22.5% said they
to be improved.”
needed basic services9; 19.2% identified
educational support, while 1.5% asked Sara, 14-year old girl
for family support and 0.4% for health
services. Children reported that they When children live in protracted
especially appreciated sports, play, conflict situations, having someone
family (especially parents), peace in the they trust at home or in their
community and the opening of schools. community is essential for their
wellbeing. Children and youth
The data show that a significantly participating in the study were asked
higher proportion of refugees, IDPs about the availability of support, and
and returnee children (70.2%) ask for if they had someone they could go
psychosocial support compared to to for support. A majority (80.6%) of
children from the host communities the children reported that they have
(42.5%). (See Figure 2). someone they trust for emotional
If the identified figure of 57% children and young people who said
they need psychosocial support is applied to all children in fragile
and conflict-affected areas globally, it could indicate that 456 million
children are in need of psychosocial support worldwide.
FIGURE 2: Need for psychosocial support based on location states
70.2% 42.5%
Refugees, IDPs Host community
and returnees member
“When there is peace in the family and in the community,
I feel happy and safe.”
Okech, 15-year-old boy
7
The analysis for the older age group (18-24) was also run, and the result was almost similar; 56.8%
asked for psychosocial support.
8
The interviewers were trained by a technical expert in psychosocial support. The respondents replied
providing needs, which were categorised into the main categories provided here.
9
This includes food, water, and money for clothes and school fees.
THE SILENT PANDEMIC 17Availability of support
FIGURE 3: Children, youth with someone they can trust for emotional support
86.0% 81.2% 41.8%
Age 7-14 Age 15-18 Age 19-24
support. This was particularly the case show that parents are stressed with
for the youngest group of children their own issues and are struggling
(aged 7-14) (86.0%) and adolescents to cope in an increasingly difficult
(aged 15-17) (81.2%), compared to situation. Given that children reported
the youth (aged 19-24) (41.8% ). (See relying on their parents for emotional
Figure 5). Most young people (67.7%) support, it is critical that parents are
said they went to parents; 11.4% said also adequately supported.
friends or partners; 11.1% said siblings;
6.8% said other relatives, while 3.1% 3. Impact of COVID-19 on
said others, including teachers, church
leaders, psychologists and neighbours. the services available for
children, young people
Older youth were less likely to have
someone trusted to turn to for and their families
emotional support. Their loss of peer
support during the pandemic may Children reported that services
be why fewer youth report having and activities (70.9%), playgrounds
someone trusted for emotional (65.0%), food (38.1%) and water
support. A recent survey conducted (10.6%) had become less available.
in the U.K. showed that young (See Figure 4). There were no
adults aged 18-24 had high levels significant differences between
of loneliness during the COVID-19 the children of refugees, IDP
pandemicxxv. This is attributed to the and returnees and those of host-
loss of peer support, which is key for community members regarding
this group’s development and mental service availability, except regarding
health wellbeingxxvi. water. A higher proportion of refugee,
IDP and returnee children (14.7%)
In addition to questions regarding compared to host-community
trusted emotional support, participants children (6.1%) reported that water
were also asked about the availability had become less available. Similarly,
of health facilities and services should according to most parents, 83.3%
a child be infected with COVID-19. In reported services had become
most cases, there was a hospital nearby less available since the COVID-19
(58.9%) or a community health post pandemic began, 63.8% playground,
(33.3%); 24.0% mentioned they had to go 60.6% food, and 19.2% water.
to the city for services. Almost a quarter
of the respondents reported that no Of those who reported that services
services are available or accessible. had become less available, 52.5%
of children and 55.6% of parents
While it is important children feel reported that access to health centres
supported by their parents or someone had become less available, while
in their community, the study’s findings 91.2% of the children and 85,8% of
18 THE SILENT PANDEMIC“COVID-19 has affected the mobility of children in
urban areas. In rural areas, they are not in quarantine.
With school closures, they are at increased risk of being
“seduced” or forcibly recruited into armed forces or
gangs, as they can no longer attend schools. Remote
learning does not include rural areas. To say the least,
the internet is bad and children are not meaningfully
included. In addition, I have seen an increase in domestic
violence. Many families are hungry.”
NGO project coordinator for protection and education, Colombia
FIGURE 4: Services and needs less available with COVID-19
83.5%
70.6%
65.0% 63.4% 60.3%
38.1%
19.2%
10.6%
Services Playgrounds Food Water
Children Parents
the parents reported that access to
schools had become less available.
(See Figure 5). “Online education is
not working here inside
Vulnerable students have been
disproportionately affected by the the camp. The internet
COVID-19 pandemic because of connection is bad, the
school closures, given the barriers
they face in accessing distance
teachers do not care
learning. In Jordan, the government about us and we do not
used television and the internet have electronic devices.”
to provide distance learning for
students during COVID-19-related Aman, 16-year-old boy
school closures. According to
UNICEF, around 70% of Jordanian
children have internet access, but
THE SILENT PANDEMIC 19FIGURE 5: Specific services less available with COVID-19
91.2%
85.8%
55.6%
52.5%
Health centres Schools
Children Parents
that figure drops sharply for refugees, wherever possible. Furthermore,
and poorer and marginalised barriers to education should be
Jordanians. reduced and new, innovative tailored
education programmes should be
Given the well-established connection inclusive of all children. Policies that
between learning and wellbeing, prevent or create barriers for refugee
access to educational opportunities children to fully participate in learning
is critical, integrating MHPSS must be addressed.
components into the classroom
“Many vulnerable parents do not have the ability to
teach their children. [Many] parents are illiterate, which
affects the educational level of the students.”
Mental health advisor, Jordan
“In rural as well as urban areas, they [children] are
staying at home. They are the victims of domestic
violence by their parents, who are already under
pressure from losing their jobs and the economic crisis.
The children who stay at home have little entertainment
and they spend too long on their electronic devices,
which affects their mental and physical development.”
Psychologist, Lebanon
20 THE SILENT PANDEMICOccupied Palestinian territory (oPt)
The COVID-19 pandemic has exacerbated the already dire health, socio-economic and protection
situation in the oPt. Approximately 2.45 million Palestinians will be in need of humanitarian
assistance in 2021, with an increased number of people in severe need for assistancexxvii. Amongst
the most vulnerable are children in detention, who are not allowed to see their parents or lawyers.
Reports of domestic abuse and sexual and gender-based violence against women and children
have increased, exacerbated by COVID-19-related restrictions and the resulting economic
deterioration. Under lockdown, increased violence and physical abuse of children by parents and
caregivers has also been reported. Many parents lost their income during the pandemic, highly
affecting their ability to provide for their families’ basic needs. The World Bank projected a decline
of about 8% in the oPt’s gross domestic product in 2020xxviii. Mental health service providers also
reported a spike in hotline calls and requests for telephone counselling from people experiencing
general psychosocial distress and those threatening self-harm.
A caregiver from oPt said, “Internet connection issues make things difficult for us. Having only
one available smartphone, which is also being used for online education, for all the children is
causing a lot of stress”.
Many children who participated in the associated control measures have
study are excluded from remote and affected their financial situation, with
online education because they lack most losing their source of income.
smart devices and tablets or adequate Most say they have experienced
internet connections in their homes. financial distress and cannot find jobs.
Many also lack study space and/or
learning support at home.
“I feel that my son has lost
4. Impact of COVID-19 on
a lot of affection for me. He
the family and parent-
feels that I scold him a lot.”
child relationships
More than half of the parents (51.2%) Mariana, a mother
reported changes in how their children
spend their days in the community
since the start of the pandemic. Almost 28% of parents observed
Of the parents, 44.3% noticed a change in the behaviour of other
changes in their relationships with parents: their inability to take
their children, including children’s care of their children’s needs, which the
aggressive behaviour, and stress and children usually could not understand.
pressure on both children and parents. The already high rates of poverty and
Others felt that they were losing touch unemployment have been exacerbated
with their children, which they noted by governments’ imposed lockdowns and
affected their children. home quarantines, such as in occupied
The majority of parents (85.0%) Palestinian territory and Jordan. This
reported that COVID-19 and its
“We cannot find jobs, and
“Isolation, fear and sometimes we do not have
anxiety, an increase in enough bread. One time
emotional stress. That is during the lockdown, my
what I have witnessed.” son got sick. I could not find
MHPSS programme
medicine to treat him.” ”
manager, Lebanon Abdel, a displaced father
THE SILENT PANDEMIC 21has led to increased emotional distress spend more time with their children.
and psychosocial disorders among Support workers should build on such
parents, including increased stress and positive aspects to address the negative
anxiety, with some exhibiting aggressive impact of the pandemic on family life and
behaviour towards their children. parent-child relations.
Positively, it enabled some parents to
Colombia
As of April 2020, Colombia had registered more than 2.5 million COVID-19 cases and 65,000
related deaths. Levels of domestic abuse and gender-based violence have increased during
the pandemicxxvix,xxx. Conflict-related violence and serious human rights abuses still continue
following the landmark peace agreement signed in 2016 by some of the involved parties. In line
with the findings of this study, UNICEF also reports an increase in anxiety symptoms as a result
of the pandemicxxxi. The challenges posed by COVID-19 have been compounded due to lack of
basic resources, disruption of care services, weakening of the social fabric, and the impact of
ongoing conflict, which affects humanitarian assistance delivery in some areas of the countryxxxii.
“... Institutions do not have the human capital to respond to
the demand they have. I believe that there is a weakness in
operational capacity, technical capacity and awareness of
the problems. In addition, access to the territory is difficult,
due to prices and armed conflict. There are limitations in
relation to the ethnic approach, institutions do not respond
to the specific needs of indigenous communities.”
Training Coordinator, NGO, Colombia
How do World Vision and
War Child Holland provide
MHPSS support?
War Child Holland (WCH) An example of a core intervention that is
being developed is the Early Adolescent
WCH is developing nine core Skills for Emotions (EASE) intervention.
interventions in its integrated EASE is developed in collaboration
(education, child protection and with World Health Organization
psychosocial support) care and support and other expert organisations, and
system. Every intervention in the care aims to address the urgent mental
system is scientifically tested, developed health treatment gap among youth.
and adapted to guarantee the highest The intervention sees non-specialist
quality standards and to develop good providers deliver psychosocial support
practices. These mutually reinforcing in low-resource settings. Its design
interventions ensure maximum impact, allows for rapid scale-up, and has
and are supplemented by a range of the potential to make quality mental
tools and measures to increase access healthcare more widely available to
to care and reduce stigmatisation. They vulnerable young people worldwide.
vary in intensity according to the needs
of children and their communities in War Child provides support across
order to ensure all mental healthcare the four layers of the MHPSS pyramid
needs are met. through child protection case
22 THE SILENT PANDEMICmanagement. Child protection case 2. Community and family support:
management provides individualised, World Vision assists children,
coordinated, holistic, multi-sectoral families and communities to
support for individual children with reconnect with each other. For
protection concerns, through direct example, we equip community
support or referrals. This can mean faith agents to provide faith-based
for example connecting caregivers of psychosocial support to children
children at risk of child labour and families through the “Walking
to livelihoods programmes with Children in Hardship”
(level 1), providing parenting support programme. During humanitarian
to distressed caregivers (level 2-3) or emergencies, children in our child-
identifying children with severe mental friendly spaces benefit from an
health conditions and referring them enhanced package of psychosocial
to specialised services (level 4). Other activities that help foster normalcy,
examples of psychosocial interventions and prevent distress and suffering
include the creative life skills from developing into more severe
intervention DEALS, Caregiver Support conditions. Our “Go Baby Go”
Intervention and structural recreative parenting programme focuses on
activities for children (Team Up). For a child’s first 1,000+ days, building
specialised mental health services War knowledge, skills and resilience-
Child collaborates with partner expert promoting techniques to improve
organisations. parenting practices across each
child development phase.
World Vision 3. Focused, non-specialised
supports: World Vision is
World Vision’s MHPSS work an innovator in developing
commenced following the 1994 psychological first aid for field
genocide in Rwanda, where we workers, group interpersonal
developed tools to measure depression psychotherapyxxxv and community
in order to assist survivorsxxxiii. materials to support of the WHO’s
Programmes such as interpersonal Mental Health GAP (mhGAP)
psychotherapy for groups were also Humanitarian Intervention Guide’s
developed and later implemented in Clinical Management of Mental,
Uganda, particularly among people Neurological and Substance Use
affected by HIV/AIDS, with impressive Conditions.xxxvi programme. World
results for sustained symptom Vision also leads in demonstrating
reductionxxxiv. Today, World Vision the effectiveness of the Problem
provides MHPSS services in almost 70 Management Plus (PM+)xxxvii
countries, with especially established low-intensity psychological
programmes in more than 20 countries, intervention.
including Colombia, DRC, Jordan,
Lebanon, the oPt and South Sudan. 4. Specialised services: World Vision
works to improve the well-being
Grounded in the current Inter-Agency of people affected by mental,
Standing Committee Reference Group neurological and substance
for MHPSS in Emergency Settings use disorders by reducing the
guidelines, World Vision’s interventions treatment gap, in conjunction
are based on four increasing levels of with the WHO’s mhGAP. Where
need, as outlined below. World Vision is not in a position
to implement these guidelines,
1. Basic services and security: World programme staff establish effective
Vision helps facilitate access to systems to refer and support
basic services, advocating that severely affected people to access
they be provided in a safe, socially specialised mental health services.
appropriate and dignified manner,
and that related service information
be made available in a timely,
accessible and accurate manner in
order to reduce people’s distress.
THE SILENT PANDEMIC 23©2020 World Vision - La Guajira, Colombia 24 THE SILENT PANDEMIC
04
A WAY FORWARD
access to food and shelter. To date,
efforts have too often been narrowly
focused on their physical health rather
“Good mental health is than their mental health, despite the
absolutely fundamental two being so interconnected. A more
to overall health and holistic and sytematic approach is
urgently needed.
well-being.”
The Sustainable Development Goals
Dr Tedros Adhanom (SDG) call for a more holistic approach
Ghebreyesus, Director- to achieving physical, mental and
General of the World social wellbeing. As part of SDG 3,
Health Organization world leaders committed to support
the “prevention and treatment
of noncommunicable diseases,
including behavioural, developmental
and neurological disorders, which
We are witnessing a silent pandemic of constitute a major challenge for
mental health disorders and stressors sustainable development”. More
among children and young people in specifically, SDG target 3.4 commits
the wake of conflict and COVID-19 governments to reducing premature
pandemic. However, we have some of mortality from noncommunicable
the solutions ready at hand to address diseases by a third through the
this crisis. There are proven models prevention, treatment and promotion
and initiatives for supporting children’s of mental health and wellbeing. Clearly,
mental health in humanitarian settings, the importance of mental health is
from expressive art, music and play recognised in global frameworks, but
and child-friendly spaces to clinical this must be more than rhetoric. It must
treatments that can be rolled out be translated into concerted action,
at scale. What is needed is global especially when it comes to conflict
leadership to scale up these initiatives settings.
and ensure that mental health
services are made a critical part of all One of the first steps in turning
humanitarian responses. these commitments into action is to
integrate globally accepted standards
Efforts to protect the mental health on psychosocial care and mental health
and psychosocial wellbeing of children into programmes in all emergency
should be prioritised in every response settings. This is easier said than done,
stage, from the early onset of conflict but it is nevertheless achievable.
through to recovery and post-conflict This study reveals deeply concerning
reconstruction efforts. Addressing levels of mental health conditions
mental health should go hand-in-hand in conflict-affected countries. It
with meeting physical health needs makes a compelling case for global
as part of a holistic humanitarian humanitarian, development and health
effort. This is especially the case for actors to develop new (and strengthen
the growing number of displaced existing) mental health services in
children worldwide, who require access conflict and post-conflict settings.
to mental health services alongside Interventions that encompass the
THE SILENT PANDEMIC 25© 2020 George Mghames / World Vision – children play during a psychosocial support session in Lebanon.
wider environment of the child (also It is also important to integrate mental
referred to as an ecological model) health services across different sectors
are crucial and should be considered, (including education, health, food,
including investing in education, nutrition, protection and livelihoods),
because learning is intricately linked ensuring MHPSS integration into
to emotional wellbeing. Adequate local health centres, schools, and
psychosocial support in school is key youth clubs, as well as national social
to supporting children affected by protection and safety net systems.
conflict. This will improve the way in which
other sectoral services are delivered
Given the increasingly protracted in support of children and families
nature of today’s conflicts, it is also who have experienced distressing
critical to break the silos between events. Not least, mental health
humanitarian, development and and psychosocial support should be
peacebuilding interventions to address recognised as a critical component in
both the immediate and longer-term promoting social cohesion and building
mental health needs of conflict- peace. When individuals (especially
affected populations. To promote youth) have the support to process
mental health services across the negative experiences, they are better
‘triple nexus’, it is recommended that equipped to manage stress levels and
donors take a long-term perspective avoid further cycles of violence.
and prioritise sustainable stand-
alone funding for mental health Now is the time to renew commitments
and psychosocial support, as well to support mental health, especially for
as complementary programming children in conflict settings. As billions
approaches. This must include multi- of dollars are invested in rebuilding
year, flexible investment to strengthen health systems around the world, it is
both community-based capacity and essential that COVID-19 response and
national systems simultaneously. recovery efforts consider psychosocial
26 THE SILENT PANDEMICneeds and the mental health impacts of their lives, their short and long-
the pandemic on children affected by term development may be seriously
conflict. endangered.
Why urgent action is needed Thirdly, children forced out of
school in a crisis are at higher risk
Firstly, the social measures of child abuse, neglect and dropping
imposed to stop the spread of out of school permanently.
COVID-19 limit children’s ability This is particularly the case for
to cope with existing girls. Their protective environment and
anxieties in their lives. This lifts the level of care they would usually
their stress levels further, even more receive is lost.
so for those with pre-existing mental
health conditions. This is particularly Finally, given their limited resources
hard for children who have already and policy space, fragile and conflict
experienced high levels of distress as a affected countries are facing a
result of conflict. hard decision between maintaining
macroeconomic stability, responding
Secondly, the social measures imposed to the pandemic and meeting peoples’
limit children’s ability to access basic needs, making investment
the support, resources and in ending conflicts paramount if
livelihoods that the adults in COVID-19 is to be addressed. Fragility
their lives largely provide. When in these contexts would not only slow
children, particularly those from down their own recovery, but will
refugee, internally displaced and slow down global recovery and act as
other marginalised communities, don’t a destabilizing force in many fragile
get the necessary support they contextsxxxviii.
need from the significant adults in
©2021 Julandin Murandya / World Vision – “At this safe space I meet other children, we learn and play together, and
this makes me happy.” Eve, 13, at a World Vision CFS near Butembo, Eastern DRC.
THE SILENT PANDEMIC 27©2020 Scovia Faida Charles / World Vision - “I want to become a lawyer someday and fight for the rights of children but right now my prayer
is for COVID-19 to end, so we can go back to school”, says Joseph, 14. Social workers Wilfred Wol and the protection committee provided
psychosocial support and guidance to Joseph as he went back to school.
28 THE SILENT PANDEMIC05
RECOMMENDATIONS
No child should have to bear the access to affected populations,
psychological scars caused by wars or particularly children, to ensure the
pandemics. timely delivery of life-saving and
sustaining assistance to minimising
When given an opportunity, children the impact of conflict on mental
and young people act and advocate health.
for social change. When empowered, 3. Familiarise and integrate the Safe
they can become powerful catalysts Schools Declaration Guidelines into
who bring about social change in operational rules and commands,
a crisis. They are true heroes who and cease attacks on students,
have the ability to improve their own teachers, schools and universities,
circumstances. and cease the use of educational
spaces for military purposes.
During this study, children compellingly 4. Respect the UN Secretary-
articulated what they want. They want General’s call for a global ceasefire
stability and dignified living spaces. in order to collectively focus on
They want their families to have access the fight against COVID-19, to
to livelihoods and sources of income. create opportunities to deliver
Children want access to reliable life-saving aid, open windows
information and quality education so for diplomacy and bring hope to
they can control their futures. They also people suffering in conflict zones
called for psychosocial support to help who are particularly vulnerable to
them as they rebuild their lives. COVID-19.
World Vision and War Child Holland United Nations
stand with these children in calling for
the following actions: Ensure a dedicated sub-section on
MHPSS in all humanitarian appeals
Parties to Conflict (Humanitarian Response Plans,
Refugee Response Plans) with set
Take immediate measures to end targets for beneficiaries, funding and
conflicts through peaceful, diplomatic reporting. This allows the international
and political solutions. This is the most community to highlight and prioritise
important, critical step in addressing the MHPSS needs of conflict-affected
the rising mental health crisis faced by populations and track allocated
children in contexts affected by conflict funding and gaps.
and COVID-19. 1. Standardise the inclusion of MHPSS
1. Adhere to international needs assessment data and analysis
humanitarian law and end in Humanitarian Needs Overviews,
violence, cease attacks on civilians, and in inter-agency, multi-sector
particularly children, abducting or needs assessment tools.
detaining children, and facilitate 2. Amend the OCHA Financial
the safe provision of principled Tracking Service to include space
humanitarian assistance. for reporting MHPSS donor
2. Act in accordance with commitments and related budget
international humanitarian and spending by implementing partners.
human rights law obligations, Introduce a marker to improve the
facilitating safe humanitarian transparency of MHPSS funding
THE SILENT PANDEMIC 29(regarding actual appeals, funds 2. Manage and mitigate the mental
received and expenditures) in health and psychosocial impacts of
humanitarian settings. conflict and COVID-19 by providing
children and their caregivers
Donors with support that is age, gender
and disability appropriate and is
Adopt MHPSS as a priority in aid accessible for marginalised groups,
strategies, recognising it as a right taking into consideration many
for children and their families, as a vulnerable groups’ lack of equitable
life-saving intervention in emergency access to the internet/technology.
responses and in long-term recovery 3. Invest in nationally and locally led
and development work, as well as a mental health services, including
critical component in peacebuilding training for local health actors in
initiatives. psychological first aid, building on
1. Step up international collaboration what is locally available. Support the
to accelerate vaccine rollout wellbeing of teachers in formal and
in fragile and conflict-affected non-formal settings, and build their
countries. Step up financial capacities to support their students’
support to cover costs for logistics healthy psychosocial development.
in order to ensure accessibility
for all vulnerable groups, Governments
including refugees and displaced
communities, recognising that the Draft national mental health strategies
pandemic is not over anywhere until that centralise children’s mental health
is it over everywhere. and psychosocial wellbeing. This
2. Increase funding for MHPSS as a includes specific budget lines in health,
matter of immediate and urgent education and child protection budgets
priority across all sectors. Step to support the implementation of
up financial commitments for locally led MHPSS services.
Humanitarian Response Plans and 1. Endorse the Safe Schools
COVID-19 responses to alleviate Declaration and its guidelines,
the urgent daily needs of children advancing actions to ensure
living in conflict. implementation of these
3. Firmly root MHPSS within the social commitments to protect students,
ecology of the child and strengthen teachers, schools and universities
the capacity within family and from the worst effects of armed
community systems surrounding conflicts. Governments should
children and adolescents in conflict also act early and create enabling
and displacement contexts. environments for children from
their early years through to
Humanitarian Actors adolescence. This includes support
for the safe reopening of schools
Ensure that MHPSS is integrated or access to relevant alternatives,
across all sectors, including protection, as well as economic and livelihood
education, livelihoods and nutrition, support for vulnerable families.
and that children, youth, caregivers, 2. Ensure fair, affordable and equitable
families and communities play a role in access to COVID-19 vaccines
determining and designing the services (once they are safe and available)
needed to support their individual and regardless of people’s legal status
collective wellbeing. (refugee, internally displaced or
1. Support the basic needs of children stateless).
and caregivers, which will also 3. Work in collaboration with the UN
benefit their mental health and and NGOs to support community-
psychosocial wellbeing. This based, multi-disciplinary team
support includes provision of services and interagency
effective, adequately resourced and coordination across sectors in order
rights-based protective, educational to promote the early detection,
and mental health services, as well response and prevention of MHPSS
as economic and livelihood support, concerns among children and their
including direct cash transfers. caregivers.
30 THE SILENT PANDEMICYou can also read