The invisibilization of health promotion in Australian public health initiatives
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Health Promotion International, 2018;33:49–59
doi: 10.1093/heapro/daw051
Advance Access Publication Date: 18 July 2016
Article
The invisibilization of health promotion in
Australian public health initiatives
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
Lily O’Hara1,*, Jane Taylor2 and Margaret Barnes2
1
Emirates College for Advanced Education, Abu Dhabi, United Arab Emirates and 2University of
the Sunshine Coast, Sippy Downs, QLD 4556, Australia
*Corresponding author. E-mail: lilyohara@ecae.ac.ae
Summary
The field of health promotion has arguably shifted over the past thirty years from being socially proac-
tive to biomedically defensive. In many countries this has been accompanied by a gradual decline, or
in some cases the almost complete removal of health promotion designated positions within
Government health departments. The language or discourse used to describe the practice and disci-
pline of health promotion is reflective of such changes. In this study, critical discourse analysis was
used to determine the representation of health promotion as a practice and a discipline within 10
Australian Government weight-related public health initiatives. The analysis revealed the invisibiliza-
tion of critical health promotion in favour of an agenda described as ‘preventive health’. This was
achieved primarily through the textual practices of overlexicalization and lexical suppression.
Excluding document titles, there were 437 uses of the terms health promotion, illness prevention, dis-
ease prevention, preventive health, preventative health in the documents analysed. The term ‘health
promotion’ was used sparingly (16% of total terms), and in many instances was coupled with the term
‘illness prevention’. Conversely, the terms ‘preventive health’ and ‘preventative health’ were used ex-
tensively, and primarily used alone. The progressive invisibilization of critical health promotion has
implications for the perceptions and practice of those identifying as health promotion professionals
and for people with whom we work to address the social and structural determinants of health and
wellbeing. Language matters, and the language and intent of critical health promotion will struggle to
survive if its speakers are professionally unidentifiable or invisible.
Key words: health promotion discourse, critical perspectives, evaluation methodology, health policy
BACKGROUND move from socially proactive to biomedically defensive
‘The way we name things shapes our feelings, judge- health promotion’ (Porter, 2007) (p. 77). The purpose of
ments, choices and actions’ (Glendon, 1991) (p. 11). the health promotion espoused in the Ottawa Charter
In Porter’s critical analysis of the changing discourse was to enhance the positive concepts of health, well-
in health promotion from the 1986 Ottawa Charter for being and resilience, whereas the purpose of the more
Health Promotion to the 2005 Bangkok Charter for limited form of health promotion presented in the
Health Promotion in a Globalized World, she noted ‘a Bangkok Charter was to prevent the negative state of
C The Author 2016. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com
V50 L. O’Hara et al.
disease (Porter, 2007). The contrasting foci of health promotion, health promotion, wherefore art thou
promotion in these documents are consistent with criti- health promotion?
cal and traditional health promotion respectively (Gregg Discourses on health and health promotion change
and O’Hara, 2007; O’Hara et al., 2015). Critical health over time and reflect the prevailing social, political and
promotion (Ferreira and Castiel, 2009; Simpson and economic contexts and ideologies in which they are pro-
Freeman, 2004; Taylor et al., 2014) is ‘underpinned by duced and maintained (Fisher et al., 2016; Robertson,
values and principles of social justice, equity, holistic 1998). One of the major health topics attracting the at-
and ecological conceptions of health, empowerment, tention of the media, industry and Governments in the
participation, salutogenesis, and evidence-based prac- last decade is that of body weight. Given the consider-
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
tice’ (Tretheway et al., 2015) (p. 1). Traditional health able emphasis on body weight in public health initia-
promotion is underpinned by biomedical and behaviou- tives, this issue will be used to explore the position of
ral models of health and health improvement (Baum, health promotion within such initiatives.
2008; Robison and Carrier, 2004). The shift from criti- The prevalence of people with a body mass index
cal to traditional health promotion that was identified (BMI) (an index of the relationship between height and
by Porter in the Ottawa and Bangkok Charters has been body mass) that are categorized as ‘overweight’ or
echoed by a shift in the language used to describe the ‘obese’ is reported to have increased rapidly throughout
discipline and practice of health promotion within pub- the world on a population wide basis (Anand and
lic health policy and programming in a number of Yusuf, 2011; Campos et al., 2006), and that everyone
countries. everywhere is at risk of becoming ‘overweight’ or ‘obese’
In Canada the term ‘population health’ has gained (Campos, 2004). The use of such terms such as ‘global’,
ascendancy over the term ‘health promotion’ because, ‘epidemic’, ‘pandemic’ and ‘globesity’ have contributed
it is argued, it provides a depoliticized discourse con- to the notion that body weight is increasing exponen-
sistent with the retreat of the welfare state in that tially and that these changes are sweeping through the
country (Raphael, 2008; Robertson, 1998). Since populations of developed and developing countries alike
1997, when ‘New’ Labour was elected to government (Caballero, 2007; Swinburn et al., 2011; World Health
in England, the hegemonic language shifted inexorably Organization, 2003). Despite evidence that the preva-
towards ‘public health’ or ‘health improvement’ lence of children, adolescents and adults in the ‘obese’
(Scott-Samuel and Springett, 2007; Scott-Samuel and category stabilized around the turn of the 21st Century
Wills, 2007). Although the new commitment to public in many parts of the world (Olds et al., 2011; Rokholm
health was regarded as a largely positive development, et al., 2010), the World Health Organization (WHO)
it signalled the start of the decline in health promotion and national governments of Australia and many other
discourse (Scott-Samuel and Springett, 2007). The dis- countries around the world continue to respond to the
appearance of the discourse and professional recogni- perceived ‘obesity epidemic’ with weight-related public
tion of the discipline of health promotion prompted health initiatives (World Health Organization, 2004).
one editorial to ask if health promotion in England The placement of body weight at the focal point of dis-
was a corpse or just a sleeping beauty (Scott-Samuel course about health is referred to as the ‘weight-centred
and Wills, 2007)? In Australia, the biomedical and health paradigm’ (O’Hara et al., 2015). This paradigm
individualized behavioural approach to health promo- has become dominant in public health policy and pro-
tion has been historically dominant in public health grammes in the developed English speaking world.
policy (Fisher et al., 2016). Although this traditional Most weight-related public health policies and pro-
approach to health promotion is regarded as narrow grammes are enacted through the discipline of health
and ineffective, particularly with respect to addressing promotion. However such policies and programmes
the social determinants of health and health inequities have received little critique through a health promotion
(Fisher et al., 2016), it nonetheless signifies some level lens. Further to de Leeuw’s lament that ‘Rhetoric is a
of commitment to health promotion, albeit in a less field of scholarship and study in the health promotion
than ideal form. However events in recent years in field that has received too little attention’ (de Leeuw,
Australia, such as the almost complete obliteration of 2010) (p. 142), in this study we sought to critically ana-
health promotion positions in Queensland and large lyse the rhetoric and discourses in Australian
scale changes in South Australia (though not in New Government weight-related public health initiatives
South Wales and Victoria) suggest that health promo- (WR-PHI) to determine the representation of health pro-
tion may be disappearing from the government public motion as a practice and a discipline within such
health landscape, prompting the question, health initiatives.Invisibilization of health promotion in Australian public health initiatives 51
RESEARCH DESIGN they reported on the progress or evaluation of a weight-
related public health policy or program. Ten documents
Methodology
were retrieved that metal of the inclusion criteria.
Critical discourse analysis (CDA) (Jacobs, 2006) was the
methodology used in the study. CDA focuses on identify-
ing the practices used by text producers to legitimize their
Data analysis
knowledge claims and support their ideology (Sproule,
This study used the eight stage analytical procedure out-
2006). CDA assumes that power and ideology are trans-
lined by Marshall and Rossman (1989): organizing the
mitted through discourse, and therefore aims for a de-
data, immersion in the data, generating categories and
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
tailed critique of text to highlight the connection of text
themes, coding the data, writing analytical memos, offer-
to ideology and the exercise of power. Such connections
ing interpretations, searching for alternative understand-
are often hidden, or appear neutral on the surface, but
ing, and writing the report. All documents were entered
shape the representation of the content for particular
into NVivo data analysis software (QSR International Pty
ends. As a method, CDA has a structured three dimen-
Ltd. Version 10, 2012). Using Machin and Mayr’s frame-
sional approach involving textual practice analysis (for
work (2012), analysis of documents involved examining
lexicon) at the core, within the context of discursive prac-
the vocabulary, grammar, sentence structure, visuals and
tice analysis (for rhetorical and lexical strategies particu-
overall structure of the text for textual practices, discur-
larly with respect to claims-making), which falls within
sive practices and social practices. Documents were ex-
the context of social practice analysis (Jacobs, 2006).
amined for evidence of word connotations,
Social practice analysis explores the role played by power
overlexicalization, lexical suppression and lexical absence
and ideology in supporting or disturbing the discourse.
(Machin and Mayr, 2012) as well as other discourse strat-
Analysis explores how power is maintained in the text,
egies related to health promotion as a discipline and prac-
how hegemonic is the discourse, and whether there is any
tice. Word connotations refer to the choice of words that
evidence of inconsistency in the discourse (Jacobs, 2006;
place the events into a particular framework of reference
Machin and Mayr, 2012). Analytic attention must there-
or discourse. Overlexicalization refers to the use of a sur-
fore be paid to each of these dimensions. Given that texts
feit of repetitious, quasi-synonymous terms, over-
may have meaning in all three dimensions, analysis across
persuasion or excessive description. Lexical suppression
the dimensions was conducted simultaneously rather than
refers to the suppression of important terms, activities, el-
in isolation or in a sequence from textual to discursive to
ements or participants. Lexical absence refers to the ab-
social practice analysis.
sence of important terms, activities, elements or
participants. Where the practices of overlexicalization
Data collection and lexical suppression or absence were identified, the
The texts chosen for analysis were documents describing data were examined to determine if quantitative analysis
weight-related public health initiatives from Australia. A of the usage of terms would yield a meaningful result.
web search was conducted for documents that met the Statistical analysis involved calculating descriptive results
following six inclusion criteria: (i) report, policy, pro- of the number of times specific terms were used, and
gramme, strategy or action plan; (ii) commissioned or where appropriate, the proportion of the total. No statis-
produced by the Australian federal government or par- tical tests were conducted on the data.
liament; (iii) published between 2003 and February The discourse practices and strategies used within
2013; (iv). name, description or rationale of the docu- the documents related to health promotion as a practice
ment is explicitly focused on body weight as the primary and a discipline are identified and discussed. A series of
or major issue; (v) population level focus; and (vi) freely questions is then presented as a heuristic for developing
available on the internet. The start date of 2003 was se- the critical competence of health promotion practi-
lected as this was the date when the Commonwealth, tioners and the general public with respect to the results
State and Territory Health Ministers first declared that presented. The heuristic for developing critical compe-
‘overweight and obesity are significant public health tence uses the 4Rs Model for Critical Reflection: recall,
problems that threaten the health gains made by relive, reinterpret and respond (McKenzie, 2000).
Australians in the last century’ (Australian Government, This study did not involve data collection from hu-
2003) (p. i). References and links in documents that met mans, therefore approval from the Human Research
the inclusion criteria were also searched. Searching con- Ethics Committee was not required. All documents used
tinued until data saturation was reached and no new in the study were available online to the public or
documents were found. Documents were excluded if through the university databases.52 L. O’Hara et al.
Table 1: Weight-related public health initiatives included in analysis
Document Year Document modalities
Healthy Weight 2008—Australia’s Future: the National Action Agenda 2003 26 page written policy
for Children and Young People and their Families (Australian
Government, 2003)
Measure Up Social Marketing Campaign (Australian Government 2006 Brochures, booklet, posters, tape mea-
Department of Health and Ageing, 2011a) sure, 12-week planner, community
guide, print, radio, television, outdoor
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
and online advertisements, websites
Australia: The Healthiest Country by 2020: A discussion paper 2008 80 page written discussion paper
(Australian Government National Preventative Health Taskforce, 2008)
Australia: The Healthiest Country by 2020 Technical Report No. 1 2009 138 page written technical report
Obesity in Australia: a need for urgent action (Australian Government
National Preventative Health Taskforce, 2009c)
Australia: The Healthiest Country by 2020—National Preventative Health 2009 60 page written report
Strategy—Overview (Australian Government National Preventative
Health Taskforce, 2009a)
Australia: The Healthiest Country by 2020—National Preventative Health 2009 316 page written report
Strategy—the roadmap for action (Australian Government National
Preventative Health Taskforce, 2009b)
Weighing it up: Obesity in Australia Report (House of Representatives 2009 223 page written report
Standing Committee on Health and Ageing, 2009)
Taking Preventative Action—A Response to Australia: The Healthiest 2010 125 page written report
Country by 2020—The Report of the National Preventative Health
Taskforce (Australian Government, 2010)
Swap It (Measure Up phase 2) Social Marketing Campaign (Australian 2011 Brochures, posters, cards, fact sheets,
Government Department of Health and Ageing, 2011b) recipe collections, print, radio, televi-
sion, outdoor and online advertise-
ments, website
Australian Government Response to Weighing it up: Obesity in Australia 2013 22 page written report
Report (Australian Government, 2013)
terms relating to ‘prevention’ were used extensively
RESULTS AND DISCUSSION throughout the documents. Excluding the use of
Ten documents were retrieved for analysis (Table 1). All prevention-related terms in the titles of the documents,
of the Australia: The Healthiest Country by 2020 (here- there were 437 uses of the terms health promotion, ill-
after referred to as AHC2020) documents except the ness prevention, disease prevention, preventive
AHC2020 Technical Report No 1 Obesity in Australia: health and preventative health. Where used, each
a need for urgent action (hereafter referred to as the term was most likely to be used alone. Health promo-
AHC2020 Obesity Technical Report) addressed three is- tion was used alone 51 times (12% of the total),
sues: obesity, tobacco use and alcohol use. The sections and coupled with a prevention-oriented term 16 times
of each document specifically related to tobacco and al- (4% of the total). Half of these uses were in the
cohol use were not included in the analysis. All other AHC2020 Discussion paper, where the term health pro-
sections were included. motion/illness prevention was used throughout the doc-
From Healthy Weight 2008 forward, the textual ument. For example:
practices of overlexicalization and lexical suppression
Among its tasks, a national agency would ensure the de-
were evident. Firstly, the term ‘health promotion’ was
livery of a minimum set of evidence-based, illness pre-
used sparingly, and in many instances it was coupled
vention/health promotion programs that are accessible
with the term ‘illness prevention’. Neither term was used to all Australians (AHC2020 Discussion paper p. xiv)
in the social marketing campaigns Measure Up or Swap
It, Don’t Stop It and therefore these documents were Subsequent AHC2020 documents including the AHC2020
therefore excluded from further analysis. Secondly, National Preventative Health Strategy OverviewInvisibilization of health promotion in Australian public health initiatives 53
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
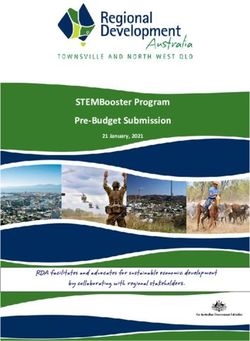
Fig. 1: Relative proportion of use of terms within selected Australian Government weight-related public health initiatives.
Excluding terms in the document titles and references to the National Preventative Health Taskforce. AHC2020, Australia the
Healthiest Country by 2020; NPHS, National Preventative Health Strategy.
(AHC2020 NPHS Overview) and the AHC2020 National A striking finding from this analysis was the domi-
Preventative Health Strategy Roadmap (AHC2020 NPHS nance of use of the term ‘preventive health’ or ‘preventa-
Roadmap) saw a rapid decline in the use of this joint term, tive health’, which draws on the biomedical concept of
and a concomitant rise in the use of prevention-oriented prevention but attempts to remove the disease connotation
terms alone. For example: by coupling it with the term ‘health’. The resulting term is
nonsensical, as the goal of preventive health is not to pre-
Action and leadership on preventative health is urgent
vent health, but to prevent illness, injury, disease and
and long overdue in Australia. (AHC2020 NPHS
death. Thus, despite the attempt to present prevention as a
Roadmap p. 6)
positive concept by coupling it with the word health, it
Health promotion was used alone 40% of the time in cannot escape its root meaning of avoidance of poor
the AHC2020 Obesity Technical Report. This is the health. Notwithstanding the absolute dominance of the
highest rate of use of the term health promotion in any term preventive/preventative health in these Australian
of the policy documents. The AHC2020 Obesity Government policy documents, perhaps the proximity of
Technical Report included a detailed literature review of the term to oxymora has resulted in it gaining little trac-
strategies designed to address the issue of obesity, and tion elsewhere. That is not to say that prevention-related
therefore included many studies that used the term terms are not in use, but they are not the truncated version
health promotion. With the publication of the seen here, and hence make more literal sense.
AHC2020 NPHS Overview and then the AHC2020 Prevention-related terms that are widely used in the
NPHS Roadmap, references to health promotion alone fields of clinical practice, public health and health pro-
decreased to 15 and 11% respectively, demonstrating motion include preventive health behaviours/practices
further lexical suppression. The hegemonic power of the (behaviours or practices that contribute to prevention of
prevention discourse grew further with the health problems) (Chapman and Coups, 2006); preven-
Government’s response Taking Preventative Action, in tative health education (specific process used to prevent
which the term health promotion was used alone only health problems) (Whitehead et al., 2004); preventative
6% of the time and a prevention-focused term was used health model (processes used to prevent health prob-
alone 92% of the time (Figure 1). lems) (Kazak, 2006); preventive medicine (processes54 L. O’Hara et al.
used to prevent health problems) (Rose, 2008); and pre- connotations placed the term health promotion most
ventive health care/services (services provided for the frequently within the specific context of the workplace.
prevention of health problems) (Sabates and Feinstein, Of the 37 uses of the terms related to programs, strate-
2006). But the scaled-back term ‘preventive/preventative gies and activities, 20 of these refer to workplace health
health’ is unused almost anywhere else. The nonsensical promotion. This represented 39% of the total uses of
nature of the term and the cognitive dissonance required the term health promotion, which was by far the most
to use it may account for its notable absence from health common specific use of the term. In Weighing it up,
related policies or programs elsewhere, and confinement there were four mentions of term health promotion, all
to Australian Government initiatives including those ex- of which were within the context of health promotion
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
amined here, and the Preventative Health Research programs, strategies and activities. In the Weighing it up
Flagship of the Commonwealth Scientific and Industrial Government Response, there were also four mentions of
Research Organization (CSIRO), Australia’s national the term health promotion, three of which were work-
science agency (CSIRO, no date). place health promotion, and one related to health pro-
The textual practices of foregrounding the term preven- motion practitioners. In the three phases of action on
tion through overlexicalization, and backgrounding the ‘obesity’ in the AHC2020 NHPS Overview, the term
term health promotion through lexical suppression served health promotion appears twice, and both times as
to invisibilize or remove recognition from health promo- workplace health promotion:
tion as a discipline and practice, replace it with the reduc-
Establish a national action research project to strengthen
tionist biomedical health paradigm concept of disease
evidence of effective workplace health promotion pro-
(health) prevention, and characterize its professionals as
grams in the Australian context (AHC2020 NPHS
the preventative health workforce. For example: Overview p. 13)
There are many very large tertiary institutions across Learn from best practice and promote effective work-
Australia that act as educators of the preventative health place health promotion programs throughout Australia
workforce of the future (AHC2020 NPHS Overview (AHC2020 NPHS Overview p. 15)
p. 33)
The identification of various settings for ‘preventative
The Commonwealth Government has provided
$500,000 for an audit of the preventative health work-
health’ action was common across many of the docu-
force (Taking Preventative Action p. 33) ments. For example Healthy Weight 2008 identified a
range of settings in which health promotion action
Is health promotion on its way to becoming a corpse or would need to take place, including child care, schools,
is it a sleeping beauty? (Scott-Samuel and Wills, 2007). primary care services, family and community care ser-
If health promotion discourse is indeed just sleeping, at vices, neighbourhoods and community organizations,
least in Australian Government weight-related policies workplaces, food supply, and media and marketing. A
and programs, analysis of the textual practice of word similar range of settings was identified in the AHC2020
connotations in the documents provided some ideas documents. However the specific language used to de-
about the source of its life-sustaining breath. Word con- scribe these health promoting settings was inconsistent.
notations placed the term health promotion most fre- In fact workplace health promotion was the only
quently within the context of programs, strategies and settings-based term that was used, and other specific.
activities. Indeed, of the 51 uses of health promotion settings-based terms such as health promoting schools,
alone, 37 of these (73%) occurred within this context. health promoting universities, health promoting health
For example: care services and healthy cities were completely absent.
Through the Healthy Children Initiative, the For example, when referring to the capacity of schools,
Commonwealth Government will make $325.5 million instead of referring to the Health Promoting Schools ap-
available for states and territories to implement health proach, the AHC2020 NPHS Overview stated:
promotion programs and activities in pre-schools,
schools and child care settings. (Taking Preventative We need to create school environments that are support-
Action p. 13) ive of good health, and in particular promote healthy eat-
ing and adequate physical activity, by providing programs
The remaining 27% of uses related to health promotion and services that build skills and knowledge, and reach
practitioners, foundations, associations and investment, people in need. (AHC2020 NPHS Overview p. 32)
the WHO definition of health promotion and mental
health promotion. Within the context of programs, Workplace health promotion has a WHO programme
strategies and activities, the textual practice of word to support it, a model of practice, national andInvisibilization of health promotion in Australian public health initiatives 55
international associations and professional journals dedi- be between private and public sector employers, insurers,
cated to it. But likewise, there are WHO supported initia- health insurers, unions and workplace health promotion
tives for health promoting schools, health promoting providers. (AHC2020 NPHS Overview p. 28)
health care services and healthy cities. For example the
health promoting schools program has an established In a neoliberal capitalist environment where the free
model of practice, robust support structures, and national market is valued, it would be expected that advocacy for
and local support in Australia provided by the Health workplace health promotion programmes from those
Promoting Schools Association. So why was the term with the greatest potential to make profit from such pro-
‘workplace health promotion’ mentioned so frequently in grammes would be stronger than advocacy for health
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
the policy documents, and health promoting schools, or promoting settings programs in schools, hospitals and
any other health promoting setting term was completely cities, where there is less opportunity for profit-making.
absent? One possible explanation may be drawn from the Baum and Fisher (2011, 2014) highlight the need to ex-
examination of the role of economic power as a social prac- amine the ‘increasing efforts of large corporations to in-
tice operating within the documents. fluence health promotion policies of governments’
For-profit companies ‘providing’ workplace health (Baum and Fisher, 2011) (p. 323) and although they are
promotion programs are prevalent in the Australian referring more specifically to tobacco and food compa-
health promotion landscape, with many companies now nies, the dominance of workplace health promotion to
claiming to provide health promotion programs to the exclusion of any other settings-based approaches
workplaces (PricewaterhouseCoopers, 2010). These may also reflect corporate efforts to influence govern-
programs often consist of individual employee health ment policy. From the documents analysed it was appar-
risk assessment and health education, and therefore do ent that a number of for-profit organizations operating
in workplaces took the opportunity to make submissions
not reflect the comprehensive workplace health promo-
and/or appear before the hearings examined in this
tion model of practice (Torp et al., 2011). For-profit
study. For example, Weight Watchers Australia made a
companies selling ‘weight-loss’ programmes are also
written submission to the Parliamentary Inquiry on
tapping into workplaces as a major customer source
Obesity, appeared before the hearings, and was quoted
(Will, 2013) and also focus their strategies on individ-
in Weighing it up. The Weight Management Council, a
uals and their behaviours. For example Weight
peak body representing four of the largest weight loss
Watchers has developed a weight loss programme for
companies in Australia, made a submission to the
implementation in workplaces titled Health Solutions
AHC2020 process.
(Weight Watchers, 2013), and has partnered with nu-
Although it was beyond the scope of this study to ex-
merous health insurance providers in the USA to deliver
amine the content of these submissions, let alone deter-
weight loss programs within workplaces (Will, 2013).
mine the relative contribution that these organizations
There is powerful economic incentive for a range of
made to advocating specifically for workplace health
for-profit organizations to sell their ‘health promotion’
promotion versus other settings based health promotion,
programmes to workplaces, and equally powerful eco-
other studies have identified the power of industry to in-
nomic, moral and social incentives for workplaces to in-
fluence government policy. For example, Jenkin et al.
stitute workplace health promotion programmes
(2011) examined the framing of submissions to the New
(PricewaterhouseCoopers, 2010). Other settings have
Zealand inquiry into obesity and found that those from
the same economic, moral and social incentives to insti-
the marketing and food industries argued more strongly
tute health promoting schools, health promoting health
for health education strategies focused on individual be-
services and health promoting cities programs (World
haviours, compared with submissions from the public
Health Organization, 2013), but there is little opportu-
health sector. Furthermore, Jenkin (2010) found that the
nity for profit-making ‘health promotion providers’
strategies proposed in the industry submissions were dis-
within these largely not-for-profit sectors, compared
proportionately represented in subsequent Government
with the vast opportunity within the workplace sector.
food policy. To our knowledge, no studies have exam-
In the section of the AHC2020 NPHS Overview on de-
ined the role of the ‘weight management’ sector in
veloping strategic partnerships, workplace health pro-
influencing government policy and this is an area that
motion providers were the only settings-based providers
requires further attention.
specifically mentioned:
Through critical discourse analysis we identified the
New partnerships can develop to improve the health backgrounding of any health promotion discourse, be it
of 10 million Australians in the workplace. These can critical or traditional, and the foregrounding of the56 L. O’Hara et al.
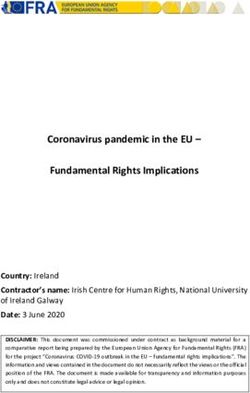
Table 2: Reflection questions to assist in the development of critical competence related to the preventive health
discourse
Reflection Health promotion professionals People in the community
phase
Recall In what ways are you required to reframe your role as a How does the preventive health discourse relate to the
‘preventive health’ practitioner? strategies that you use in everyday life to enhance or
optimize health and wellbeing?
Recall How do you feel about the invisibilization of the health How consistent is the preventive health discourse with
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
promotion discipline and practice in these your lived experiences of health and wellbeing?
documents?
Recall Do you perceive your role to be valued differently What is gained or lost in the preventive health discourse
(more or less) because health promotion discourse that is important to you?
has been overtaken by the preventive health
discourse?
Relive How do these reflections make you feel? How do these reflections make you feel?
Reinterpret Why do you think you feel that way? Why do you think you feel that way?
Respond How might you translate the preventive health dis- How might you convey your views to the health promo-
course into everyday language that resonates with tion practitioners and government representatives re-
people in the community? sponsible for implementing policies and programs
using the preventive health discourse?
Respond What potential risks and benefits are there for you to What potential risks and benefits are there for you to do
undertake such a process? so?
Respond How might you mitigate the potential risks and opti- How might you mitigate the potential risks and opti-
mize the potential benefits? mize the potential benefits?
prevention discourse that excluded any reference to Health promotion strategies would be expected to
health promotion. Prevention discourse was ascribed comprise the majority of the strategies in any major pub-
merit or value and was privileged at the expense of glob- lic health initiative. However, through the analysis we
ally recognized health promotion discourse. This has sig- identified that the discipline of health promotion and
nificant implications for those on the receiving end of the health promotion professionals that practice that
these policies and programs. For health promotion prac- discipline were backgrounded through the preventive
titioners expected to work on preventive health initia- health discourse. Even the broader term ‘public health’
tives, and for members of the public involved in or was minimally represented in the documents. So who is
impacted by such initiatives, the preventive health dis- it that is expected to do the work described in the initia-
course prompts a number of critical questions. tives? Judging from the description of the strategies,
Responding to Baum’s call for all health promotion re- health promotion practitioners are expected to do much
search to have a critical or change oriented focus (Baum, of the work, but are not given the professional courtesy
2008), as an output of this study we developed a set of of being named as such, and instead must be assumed to
reflective questions using the 4Rs Model for Critical exist in the amorphous ‘preventative health workforce’.
Reflection (McKenzie, 2000) to assist in the develop- There was no obvious rationale for the shift away from
ment of critical competence about the preventive health the internationally recognized health promotion terms,
discourse (Table 2). The 4Rs Model includes four cate- and de Leeuw (2010) suggests that the preventive health
gories of questions: (i) Recall: What is your assessment discourse may simply be the ‘political craze of the day’
of the current situation?; (ii) Relive: How do these recol- in a general political environment that is swinging more
lections make you feel?; (iii) Reinterpret: What meaning toward liberal and neo-corporatist perspectives. This is
do you make of the current situation and your feelings consistent with Raphael’s proposal that a similar shift
about it?; and (iv) Respond: What can/will you do now? from health promotion discourse to population health
The purpose of these questions is to provoke conversa- discourse in Canada provided a depoliticized discourse
tion and critical reflection on the utility, desirability, im- consistent with the retreat of the welfare state (Raphael,
plications and consequences of the preventive health 2008), and Fisher and Baum’s analysis of Australian
discourse. health policy as dominated by ‘politically easier’Invisibilization of health promotion in Australian public health initiatives 57
individualized behavioural approaches for neoliberal The study did not include other documents such as pro-
governments (Fisher et al., 2016). gram evaluation reports or submissions to the consulta-
The origin of the term ‘preventative health’ is tive processes, which may have provided additional
unclear—it simply appeared in announcement of the insights. Additionally, the study did not include initia-
National Preventative Health Taskforce commissioned tives undertaken by other levels of Government or the
to develop the AHC2020 National Preventative Health non-Government sector and so the results cannot be
Strategy. No explanation for the use of the term ap- generalized. The study results were constructed by us
peared in any of the documents, and it was presented as and are limited to our interpretation.
a given that this term was the most appropriate term to
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
use. Baum and Fisher (2011) argue that the narrow
terms of reference set for the National Preventative CONCLUSION
Health Taskforce meant that the National Preventative
Health Strategy was inevitably focused on promoting in- Through critical discourse analysis we identified the invis-
dividual behaviour change to address so-called ‘lifestyle’ ibilization of health promotion in favour of the biomedi-
risk factors, but this does not explain the limited use of cally defensive preventive health agenda in Australian
the term ‘health promotion’ in the documents. Government weight-related public health initiatives.
Traditional health promotion is underpinned by the bio- Further research is required on the extent of such changes
medical and behavioural models, but the term ‘health in discourse in other sectors. The implications of such a
promotion’ is still used to describe this approach. shift in discourse on the perceptions and practice of those
Critical health promotion however, is concerned with identifying as health promotion professionals and other
inequity and access to the determinants of health, requir- people in the community need to be explored.
ing strategies that are inherently political, and the back-
grounding of health promotion and even public health REFERENCES
discourse in favour of the more nebulous apolitical pre-
Anand, S. S. and Yusuf, S. (2011). Stemming the global tsunami
ventive health discourse may well have been a deliberate
of cardiovascular disease. The Lancet, 377, 529–532.
attempt to depoliticize the (unavoidably political) disci-
Australian Government. (2003) Healthy Weight 2008:
pline of critical health promotion (Baum, 2008). Australia’s Future - The National Action Agenda for
Whatever the reason, the documents analysed took up Children and Young People and their Families. Retrieved
the preventive health baton with gusto, with barely a from Canberra. http://www.healthyactive.gov.au/docs/
sideways glance at the health promotion and public healthy_weight08.pdf (1 April 2010, date last accessed).
health disciplines and practitioners that were Australian Government. (2010) Taking Preventative Action – A
marginalized in the process. Although the form of health Response to Australia: The Healthiest Country by 2020 –
promotion presented in the Bangkok Charter reflected The Report of the National Preventative Health Taskforce.
this negative biomedical orientation, subsequent Australian Government. (2013) Australian Government re-
sponse to the House of Representatives Standing Committee
Charters such as the Nairobi Call to Action and the
on Health and Ageing report: Weighing it up: Obesity in
Adelaide Statement on Health in All Policies showed
Australia.
that ‘a strong commitment from politicians and practi-
Australian Government Department of Health and Ageing.
tioners to a powerful positive health approach in all sec- (2011a) Measure Up. https://web.archive.org/web/
tors and levels of society is possible and worth pursuing’ 20110817065823/ http://www.measureup.gov.au/internet/
(de Leeuw, 2010) (p. 142). However there was little evi- abhi/publishing.nsf/Content/Aboutþtheþcampaign-lp (7
dence in Australian Government weight-related public August 2011, date last accessed).
health initiatives of a political agenda consistent with Australian Government Department of Health and Ageing.
the positive concept of critical health promotion first es- (2011b) Swap It, Don’t Stop It. https://web.archive.org/web/
poused 30 years ago in the Ottawa Charter for Health 20110830084149/ http://swapit.gov.au (30 August 2011,
Promotion and returned to in the Charters following date last accessed).
Australian Government National Preventative Health
Bangkok.
Taskforce. (2008) Australia: The Healthiest Country by
The study had a number of strengths and limitations.
2020 - A discussion paper.
The study covered a decade from 2003 to 2013 in which Australian Government National Preventative Health Taskforce.
weight-related public health initiatives were initiated by (2009a) Australia: The Healthiest Country by 2020 –
the Australian Government, and produced a set of re- National Preventative Health Strategy – Overview.
flective questions for critical competence for use by Australian Government National Preventative Health
health promotion professionals and the general public. Taskforce. (2009b) Australia: The Healthiest Country by58 L. O’Hara et al.
2020 – National Preventative Health Strategy – the roadmap the New Zealand inquiry into obesity. Obesity Reviews, 12,
for action. 1022–1030.
Australian Government National Preventative Health Taskforce. Kazak, A. E. (2006) Pediatric Psychosocial Preventative Health
(2009c) Australia: the healthiest country by 2020. Technical Model (PPPHM): Research, practice, and collaboration in
Report No 1 Obesity in Australia: a need for urgent action, pediatric family systems medicine. Families, Systems, and
Including addendum for October 2008 to June 2009. Health, 24, 381.
Baum, F. (2008) The New Public Health, 3rd edn. Oxford Machin, D. and Mayr, A. (2012) How to Do Critical Discourse
University Press, Melbourne. Analysis: A Multimodal Introduction. Sage Publications,
Baum, F. and Fisher, M. (2011) Are the national preventive London, UK
health initiatives likely to reduce health inequities? Marshall, C., and Rossman, G. (1989) Designing Qualitative
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
Australian Journal of Primary Health, 17, 320–326. Research. Sage, Newbury Park, CA.
Baum, F. and Fisher, M. (2014) Why behavioural health promo- McKenzie, B. (2000) Phase 1 Workbook: Strategic leadership
tion endures despite its failure to reduce health inequities. development program. Retrieved from Sydney, NSW, AUS.
Sociology of Health and Illness, 36, 213–225. http://www.systemics.com.au/intro.html (19 July 2009,
Caballero, B. (2007) The global epidemic of obesity: an over- date last accessed).
view. Epidemiologic Reviews 29, 1–5. O’Hara, L., Taylor, J. and Barnes, M. (2015) The extent to
Campos, P. (2004) The Obesity Myth. Gotham Books, New York. which the public health ‘war on obesity’ reflects the ethical
Campos, P., Saguy, A., Ernsberger, P., Oliver, E. and Gaesser, values and principles of critical health promotion: a multi-
G. (2006) The epidemiology of overweight and obesity: pub- media critical discourse analysis. Health Promotion Journal
lic health crisis or moral panic? International Journal of of Australia, 26, 246–254.
Epidemiology, 35, 55–60. Olds, T. S., Maher, C., Zumin, S., Péneau, S., Lioret, S.,
Chapman, G. B. and Coups, E. J. (2006) Emotions and preven- Castetbon, K. et al. (2011) Evidence that the prevalence of
tive health behavior: worry, regret, and influenza vaccina- childhood overweight is plateauing: data from nine coun-
tion. Health Psychology, 25, 82. tries. International Journal of Pediatric Obesity, 6,
CSIRO. (no date) Preventative Health. http://www.csiro.au/ 342–360.
Organisation-Structure/Flagships/Preventative-Health- Porter, C. (2007) Ottawa to Bangkok: changing health
Flagship.aspx (2 September 2011, date last accessed) promotion discourse. Health Promotion International, 22,
de Leeuw, E. (2010) Warning! Changing rhetoric ahead! Health 72–79.
Promotion International, 25, 141–142. PricewaterhouseCoopers (2010) Workplace Wellness in
Ferreira, M. S. and Castiel, L. D. (2009) Which empowerment, Australia: Aligning Action with Aims: Optimising the
which Health Promotion? Conceptual convergences and di- Benefits of Workplace Wellness. PricewaterhouseCoopers,
vergences in preventive health practices. Cadernos de Saude Melbourne, VIC, AUS.
Publica, 25, 68–76. Raphael, D. (2008) Grasping at straws: a recent history of health
Fisher, M., Baum, F., MacDougall, C., Newman, L. and promotion in Canada. Critical Public Health, 18, 483–495.
McDermott, D. (2016) To what Extent do Australian Robertson, A. (1998) Shifting discourses on health in Canada:
Health Policy Documents address Social Determinants of from health promotion to population health. Health
Health and Health Equity? Journal of Social Policy, 45, Promotion International, 13, 155–166.
545–564. Robison, J. and Carrier, K. (2004) The Spirit and Science of
Glendon, M. A. (1991) Rights Talk: The Impoverishment of Holistic Health. Authorhouse, Bloomington, IN.
Political Discourse. The Free Press, New York. Rokholm, B., Baker, J. L. and Sørensen, T. I. A. (2010) The
Gregg, J. and O’Hara, L. (2007) Values and principles evident in levelling off of the obesity epidemic since the year 1999 – a
current health promotion practice. Health Promotion review of evidence and perspectives. Obesity Reviews, 11,
Journal of Australia, 18, 7–11. 835–846.
House of Representatives Standing Committee on Health and Rose, G. (2008) Rose’s Strategy of Preventive Medicine. Oxford
Ageing. (2009) Weighing it up: Obesity in Australia. University Press, Oxford, UK.
Jacobs, K. (2006) Discourse analysis. In Walter, M. (ed), Social Sabates, R. and Feinstein, L. (2006) The role of education in the
Research Methods: An Australian perspective. Oxford uptake of preventative health care: the case of cervical
University Press, South Melbourne, VIC, AUS. screening in Britain. Social Science and Medicine, 62,
Jenkin, G. (2010) Individuals, the Environment or Inequalities: 2998–3010.
Industry and Public Health Framing of Obesity and its Scott-Samuel, A. and Springett, J. (2007) Hegemony or health
Presence in New Zealand Government Policy on Food and promotion? Prospects for reviving England’s lost discipline.
Nutrition. (PhD), University of Otago Dunedin, New Zealand. The Journal of the Royal Society for the Promotion of
http://www.otago.ac.nz/wellington/otago042929.pdf (28 Health, 127, 211–214.
December 2012, date last accessed). Scott-Samuel, A. and Wills, J. (2007) Health promotion in
Jenkin, G., Signal, L. and Thomson, G. (2011) Framing obesity: England: sleeping beauty or corpse? Health Education
the framing contest between industry and public health at Journal, 66, 115–119.Invisibilization of health promotion in Australian public health initiatives 59
Simpson, K. and Freeman, R. (2004) Critical health promotion Weight Watchers. (2013) Weight Watchers Health Solutions.
and education—a new research challenge. Health Education http://www.weightwatchers.com/templates/marketing/mar
Research, 19, 340–348. keting_utool_1col.aspx?pageid¼1307891 (17 November
Sproule, W. (2006) Content analysis. In Walter, M (ed), Social 2011, date last accessed)
Research Methods: An Australian Perspective. Oxford Whitehead, D., Keast, J., Montgomery, V. and Hayman, S.
University Press, South Melbourne, VIC, AUS. (2004) A preventative health education programme for oste-
Swinburn, B., Sacks, G., Hall, K. D., McPherson, K., Finegood, oporosis. Journal of Advanced Nursing, 47, 15–24.
D. T., Moodie, M. L. et al. (2011) The global obesity pan- Will, M. (2013) Weight watchers sets its eyes on employers.
demic: shaped by global drivers and local environments. The http://www.huffingtonpost.com/2013/08/09/weight-watch
Lancet, 378, 804–814. ers-employers-_n_3730850.html (27 November 2013, date
Downloaded from https://academic.oup.com/heapro/article-abstract/33/1/49/2555397 by guest on 31 May 2020
Taylor, J., O’Hara, L. and Barnes, M. (2014) Health promotion: last accessed)
a critical salutogenic science. International Journal of Social World Health Organization. (2003) Diet, nutrition and the pre-
Work and Human Services Practice, 2, 283–290. vention of chronic diseases: report of a joint WHO/FAO ex-
Torp, S., Eklund, L. and Thorpenberg, S. (2011) Research on pert consultation, Geneva, 28 January - 1 February 2002.
workplace health promotion in the Nordic countries: a liter- World Health Organization and the Food and Agriculture
ature review, 1986-2008. Global Health Promotion, 18, Organization of the United Nations, Geneva.
15–22. World Health Organization. (2004) Global Strategy on Diet,
Tretheway, R., Taylor, J., O’Hara L. and Percival N. (2015) A Physical Activity and Health. World Health Assembly, Geneva.
missing ethical competency? A review of critical reflection in World Health Organization. (2013) Healthy Settings. http://
health promotion. Health Promotion Journal of Australia, www.who.int/healthy_settings/en/ (16 September 2014,
26, 216–221. date last accessed)You can also read