The Implementation of External Reference Pricing within and across Country Borders - Panos Kanavos Anna-Maria Fontrier Jennifer Gill Dionysis ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Implementation of External Reference Pricing within and across Country Borders Panos Kanavos Anna-Maria Fontrier Jennifer Gill Dionysis Kyriopoulos
The Implementation of External Reference Pricing within and across Country Borders 2
London School of Economics
Houghton Street
London
England
WC2A 2AE
web: www.lse.ac.uk
First published 2017
Copyright© Panos Kanavos, Anna-Maria Fontrier, Jennifer Gill, Dionysis Kyriopoulos 2017
DOI: https://doi.org/10.21953/lse.y1tbizsxrl3n
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 3
CONTENTS
List of Figures 4
List of Tables 4
List of Acronyms 5
Acknowledgements 6
Abstract 7
Background 7
Method 7
Results 7
Conclusion 7
Executive summary 8
1. Introduction 9
2. Methods 10
2.1 Study endpoints 10
2.2 Systematic Literature Review: Data sources, search strategy and keywords 11
2.3 Study selection, data extraction, evaluation and synthesis 11
2.4 Primary Data Collection 11
3. Results 13
3.1 Results of the literature review 13
3.2 Objective of ERP and alignment with health system objectives 13
3.3 Characteristics of products subject to ERP price regulation 14
3.4 Is ERP the main pricing policy or a supportive tool? 15
3.5 Transparency of ERP pricing policy 16
3.6 Competent authorities responsible for ERP implementation 16
3.7 Appeals by stakeholders to regulator decisions 18
3.8 Number of basket countries 18
3.8 Frequency of price revisions 18
3.9 Criteria for basket country selection 19
3.10 Type of comparator price used in ERP 22
3.11 Methods for calculation of the reference price 22
3.12 Sources of information for pricing decisions 22
3.13 Inclusion of wealth adjustments in ERP calculations 23
3.14 Accounting for exchange rate fluctuations 23
3.15 Link between price and reimbursement 24
3.16 Interaction of ERP with HTA and VBP 25
3.17 ERP alignment with other negotiation tools of reimbursement 25
3.18 Link between ERP regulation and patent status 25
4. Discussion & Policy Implications 28
4.1 Policy implications 30
4.1.1 Objectives and scope of external price referencing system 31
4.1.2 Administration and operations 31
4.1.3 Methods for the conduct of external price referencing 32
4.1.4 Implementation of external price referencing 33
4.2 Country Adherence to 14 Best Practice Principles 33
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 4
5. Conclusion 35
6. References 36
Appendix 1 42
List of Figures
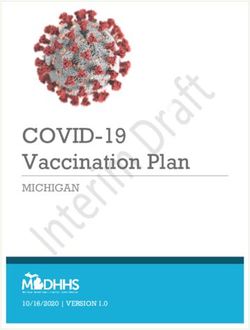
Figure 1: PRISMA flow diagram with search results from the systematic literature review 13
List of Tables
Table 1: Definition of endpoints in ERP implementation 10
Table 2: Results of systematic literature search by source 14
Table 3: Type of pharmaceuticals subject to ERP across countries 15
Table 4: Main role of ERP 16
Table 5: Transparency in ERP across countries 17
Table 6: Competent authorities in ERP implementation across countries 17
Table 7: Presence of appeals process for stakeholders 18
Table 8: Overview of basket across countries 19
Table 9: Number of reference countries of basket across other non-EU countries 20
Table 10: Frequency of price revisions across the studied countries 20
Table 11: Criteria for basket selection across studied countries 21
Table 12: Price selection across countries 21
Table 13: Method for calculation of reference price across countries 22
Table 14: Sources of information across countries 23
Table 15: Inclusion of wealth adjustments in ERP calculation 24
Table 16: Methods for dealing with exchange rate fluctuations 24
Table 17: ERP relationship with other pricing and reimbursement policies 26
Table 18: Adherence to the 14 best practice principles 34
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 5
List of Acronyms
AUT Austria LTU Lithuania
BEL Belgium LUX Luxemburg
BGR Bulgaria LVA Latvia
BMI Business Monitoring International MDA Moldova
CHE Switzerland MLT Malta
CRD Centre for Reviews and Dissemination NLD The Netherlands
CYP Cyprus NOR Norway
CZE Czech Republic OECD Organisation for Economic Cooperation and
DEU Germany Development
DNK Denmark POL Poland
EFPIA European Federation of Pharmaceutical PPP Purchasing Power Parity
Industries and Associations PRT Portugal
ERP External Reference Pricing R&D Research and Development
ESP Spain ROU Romania
EST Estonia RUS Russia
EU European Union SRB Serbia
FIN Finland SVK Slovakia
FRA France SVN Slovenia
GRC Greece SWE Sweden
HiT Health in Transition TUR Turkey
HRV Croatia VBP Value Based Pricing
HTA Health Technology Assessment VED Vital & Essential Drugs
HUN Hungary WHO World Health Organization
IRL Ireland WHO-CC World Health Organisation Collaborating
ISL Iceland Centres
ISR Israel WoS Web of Science
ITA Italy
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 6
ACKNOWLEDGEMENTS
We would like to thank Mackenzie Mills, Erica Visintin,
Olina Efythimiadou and David Taylor for their insight
and support throughout the development of the
paper. Finally, we thank Pfizer Ltd. for providing
the sponsorship that allowed us to carry out this
research.
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 7
ABSTRACT
BACKGROUND RESULTS
External reference pricing (ERP), a frequently The systematic literature review confirmed that
implemented pricing policy, seeks to rationalize there is heterogeneity in the way that ERP is
prices and contain costs by using foreign prices implemented across countries. There tends to be
as reference for the determination of domestic variation in the size of the country baskets, with
prices and facilitation of negotiation. Its use across larger baskets becoming more common and in the
countries varies significantly in terms of objectives, way that countries chose their basket countries
methods, administration and implementation. – some choose those with similar socioeconomic
characteristics whilst others do not. Furthermore
METHOD there is variation in the calculation used with most
countries vying away from the average-based
A systematic literature review was conducted
calculations towards the lowest basket price or the
according to CRD guidelines. 17 Study endpoints
average of the lowest ‘n’ prices. The frequency of
were used to identify characteristics of ERP
price revisions differs according to authorities and
implementation across 29 countries, of which 17
government negotiations, as does the rate at which
were EU member states. Multiple databases were
exchange rate fluctuations are taken into account in
examined to provide a wide range of ERP sources.
pricing decisions. In terms of the 14 best practice
After filtering for mention of ERP implementation
principles Belgium, France, and South Africa adhered
related to at least one of the 17 study endpoints 176
to the most principles whilst Bulgaria, Hungary and
studies remained. Primary data collection, in the
Romania had the most instances of non-adherence.
form of questionnaires directed at key stakeholders,
were also used to supplement data in instances
where information received from the systematic CONCLUSION
literature review was outdated or minimal. Findings Heterogeneity and recent trends in ERP design have
from the systematic literature review and primary policy implications for governments, which include
evidence from key stakeholders were benchmarked globally declining pharmaceutical prices and other,
against 14 best practice principles inherent to an potentially more undesirable consequences such as
optimal ERP system to determine the quality of ERP launch delays in low-income countries, parallel trade
systems implemented by the countries of interest. reducing drug stock levels, inflated prices in low-
income countries, reduced incentive for continued
R&D and reduced access to medicines in some
regions. Overcoming this issue to ensure that ERP
is beneficial to all stakeholders will require a focus
on developing sustainable, transparent, simple and
stable systems using a set of key guidelines that
should maximise the benefits of the pricing policy.
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 8
EXECUTIVE SUMMARY
This paper aimed to highlight differences in the Rapidly evolving healthcare costs and increases in
way that 29 countries implement ERP, which aims life expectancy and chronic disease prevalence mean
to contain medicine costs, using a systematic that reduced drug prices are the ultimate aim for most
literature review-based process combined with country governments. However, badly designed ERP
primary evidence from key stakeholders. Of the systems can be detrimental to all stakeholders and
29 countries analyzed 17 were European Member should be avoided at all costs. ERP systems should
States, with the remainder representative of Latin be designed with both health and industrial policy
America, South East Asia, the Middle East and North aims in mind to ensure that the requirements of all
Africa. Secondary data was collected from literature stakeholders including patients, manufacturers and
published between 2000 and 2015 on a set of 17 governments are represented in order to ensure that
criteria (endpoints) based on the ERP system design. patients get access to well-priced medicines as and
Databases examined included Web of Science (WoS), when required, governments can spend within their
CINAHL, EconLit, Medline, ProQuest, Cochrane means and manufacturers have enough incentive to
Library and Scopus. Special keywords and a defined continue investing in future R&D in order to benefit
search strategy were used to arrive at an initial future patient populations.
list of studies. After filtering for mention of ERP
implementation related to at least one of the 17 study There are a number of key criteria that can be adhered
endpoints 176 studies remained. Primary evidence to that may ensure an ERP system is designed to
was collected via questionnaires distributed among benefit all stakeholders and remains transparent,
key stakeholders. Results of the systematic literature simple, stable and sustainable. These criteria are
review and of the primary evidence collection were based on the selection of reference countries and
contrasted with analysis of the goals and observed prices; the use of exchange rates; the types of products
impacts of the different ERP systems to identify for which ERP should be used; price revisions; and
optimal design features of ERP systems. the derivation of target prices. Furthermore, as no
two countries are identical any EPR system should
Findings confirmed high levels of heterogeneity outline the objective and scope of the ERP system
between the ERP systems of different countries. and ensure it reflects the overall healthcare system’s
Variation was present in many of the 17 endpoints values and objectives. It is also recommended that
analyzed. For example, some countries use ERP target prices should align with the expected value of
for all medicines, regardless of their patent status, the product, determined by using HTA or a similar
whilst others use it only for in-patent medicines. ERP mechanism. Encouraging countries to follow such
processes range from formal to informal and from guidelines could ensure that ERP systems do not
the main to the supportive pricing policy in place in a alienate the innovative pharmaceutical company
country. In cases where the process is informal there and ensure that they are incentivized to continue
is limited definition of policy objective and scope investing in global R&D which in the long run will
which can affect transparency. Country baskets range maximize global population health. In this paper, 14
in size from three to 36 (not including those countries basic principles that an optimal ERP system should
that use prices in the medicine country of origin) follow were benchmarked against the findings
whilst very few countries use any kind of wealth from the systematic literature review and primary
adjustment, even if countries are not selected based evidence from key stakeholders to determine the
on financial characteristics. Reference calculations quality of ERP systems implemented by the countries
tend to be based on a lowest price in the basket style of interest. Belgium, France, and South Africa adhered
calculation, rather than an average based calculation. to the most principles whilst Bulgaria, Hungary and
Some countries use ex-factory prices, which do not Romania had the most instances of non-adherence.
reflect confidential discounts or rebates, to form the
basis of their calculations meaning referenced prices
do not reflect reality.
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 9
1. INTRODUCTION
ERP, also known as external price referencing or trigger a manufacturer to set either a single price or
international price comparison/ benchmarking, is a narrow band of prices before launch is allowed. Such
widely used pricing policy with high global research linking of low and high income markets can lead to
interest. It is introduced when governments decide prices converging at a higher level than would have
to use foreign drug prices to regulate domestic prices been the case if markets had been separate. In low-
(EFPIA, 2014; Danzon and Towse, 2003) and to income countries, this can lead to inappropriately
impose price caps based on prices of similar drugs in high prices and reduced access for patients. In high-
other reference countries (Houy and Jelovac, 2014) income countries, whilst in the short run imported
with the official definition being: “the practice of lower prices may be beneficial, in the long run,
using drug prices in several countries to derive a lower revenues can lead to reduced return on R&D
benchmark or reference price for the purposes of investment and consequently fewer new medicines
setting or negotiating prices in countries” (WHO, (Danzon and Towse, 2003). Furthermore, marketing
2013; EFPIA, 2014). The primary aim of the pricing authorization holders may prefer initially to promote
mechanism is to control in-patent drug prices their products to high-price countries rather than
(Ruggeri and Nolte, 2013) via the containment of low-price countries so that these high prices are
pharmaceutical prices and expenditure (Espin et used as references in countries performing ERP
al., 2010). The widespread use of ERP generally (Vogler et al., 2015). At the same time, the accuracy
arises due to government cost control requirements. of international comparisons may be distorted due
Authorities can use international comparisons to to methodological issues and differences across
evaluate the fairness or appropriateness of the actual countries in strength, formulation and pack sizes
price related to comparative cases (OECD, 2008). available (Timur and Picone, 2010). ERP assessment
Specifically, drug prices in other countries are used is considered complex compared to other pricing
as a reference to determine a limit for the entry price methods. The promotion of transparency around
of a drug or reimbursement price (Nguyen et al., the use of ERP may improve the accountability of
2015). decision-making, which could reduce uncertainty
for manufacturers and eliminate discrimination and
The implementation of ERP varies significantly corruption (Espin et al., 2014).
between countries in terms of the various rules
followed by individual countries to calculate the There is a need to study the implementation of
final product price (Espin et al., 2014). For example, ERP with a focus on differences in implementation
an increase in the number of reference countries across countries. The present study will attempt, via
in a basket generally leads to further reductions in a combination of primary and secondary evidence,
drug prices (BMI Research, 2010). Furthermore, to contribute to the review, analysis and body of
the countries used in the basket can affect price information about ERP structure and its alignment
variation. Financial performance of the country, with other policies across countries where the
pharmaceutical pricing systems, publication of following countries are of interest: Austria, Belgium,
actual versus negotiated or concealed prices, exact Bulgaria, Czech Republic, Estonia, France, Germany,
comparator products and disease burden of the Greece, Hungary, Italy, Latvia, Poland, Portugal,
potential reference country all need to be taken into Romania, Russia, Slovakia, Slovenia, Spain, Turkey,
account when choosing reference countries (WHO, Brazil, Egypt, Jordan, Kuwait, Lebanon, Qatar, Saudi
2015). Arabia, South Africa, South Korea and United Arab
Emirates. To determine the quality of ERP systems
Although ERP may have the potential to contribute implemented by the countries of interest we
to improved access and counteract affordability benchmark findings from the systematic literature
problems sometimes seen in lower-income review and primary evidence from key stakeholders
countries, there are potential consequences. The against 14 basic principles that an optimal ERP
most significant concern is related to the fact that system should follow (Sullivan et al., 2017).
ERP could lead high-income countries to demand
low prices creating resulting difficulties for low-
income countries. ERP-related price leakages can
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 10
2. METHODS
Both primary and secondary evidence have been used The number of basket countries and the criteria
to identify characteristics of ERP implementation used for their selection was also analysed alongside
across 29 countries and to inform the discussion the methods used for price calculation. The role
and analysis in the sections that follow. Secondary of the patent status and innovation was taken into
evidence was collected via a systematic literature account. Furthermore, investigation around the
review, which was carried out based on the CRD inclusion of wealth adjustments, price revisions
guidelines for systematic reviews. and exchange rate fluctuations was necessary given
their impact on price determination (Toumi et al.,
2.1 STUDY ENDPOINTS 2014). The sources, dissemination and accessibility
A number of defined endpoints relating to the of price data were also assessed as key issues in
structural elements of ERP were analysed in this price setting. As far as interaction with other policies
systematic literature review (see Table 1). The main is concerned, the alignment of the pricing process
role of ERP in each country of interest was analysed with the reimbursement process was examined and
in order to determine differences in application the combination of ERP with different negotiation
across countries. Transparency was evaluated to tools for reimbursement was used as an endpoint.
examine fairness in pricing. We also investigated the The interaction of other pricing processes such as
role of stakeholders in the design of ERP systems value based pricing (VBP) and health technology
and their involvement in any appeals processes. assessment (HTA) with ERP was also examined.
Table 1: Definition of endpoints in ERP implementation
Endpoints Definition
Structural Elements
Objective and alignment with health system Assesses the aim of international comparisons and the relationship with health
objectives systems’ objectives
Characteristics of pharmaceuticals subject to Takes into account the categories of drugs included in the ERP system
ERP
Main role Determine whether ERP provides the major or supportive role in negotiations and
determination of drug prices
Transparency Includes the legislative criteria used by countries to promote a fair pricing process
Competent authorities in ERP implementation Presents the authorities in control of ERP policy implementation
Appeals by stakeholders to regulator decisions Assesses the possible appeals of stakeholders in pricing process
Number of basket countries and countries in Presents the countries and the number of members included in each basket
the basket
Criteria for basket country selection Assesses the appropriate criteria to select reference countries
Type of comparator price Presents the selection of price category across countries
Method for calculation of the reference price Examines the different methods of countries to determine reference price
Sources of information for pricing decisions Presents the sources and stakeholders that contribute to public access of price data
Inclusion of wealth adjustments Assesses whether wealth adjustments made to the reference price when countries
of higher or lower GDP are included in the basket
Accounting for exchange rate fluctuations Assesses whether calculations used to account for exchange rate fluctuations
across countries
Interaction with other policies
Link between price and reimbursement Refers to the countries that take into account price determination and
reimbursement process at the same time
Interaction with HTA or VBP Assesses the parallel use of international comparisons with other methods to set
drug prices
Alignment with other negotiation tools of Refers to the combination of international comparisons with reimbursement
reimbursement purposes
Link between ERP regulation and patent status Takes into consideration the role of patent status in ERP price calculation
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 11
2.2 SYSTEMATIC LITERATURE 2.3 STUDY SELECTION, DATA
REVIEW: DATA SOURCES, SEARCH EXTRACTION, EVALUATION AND
STRATEGY AND KEYWORDS SYNTHESIS
Both peer-reviewed and grey literature were The results were filtered according to title and
examined to minimize bias and identify all relevant abstract relevance to the topic. Papers with relevant
information. Multiple databases were utilised, these titles were downloaded for further examination. In
were the Web of Science (WoS), CINAHL, EconLit, order to arrive at a final set of studies, the main body
Medline, ProQuest, Cochrane Library and Scopus. A of these texts was assessed according to the following
combination of broad and policy key words were used criterion: mention of ERP implementation relating to
to ensure that all relevant literature was captured. All at least one of the selected endpoints. The number
synonyms and different phrasings of ERP or External of studies based on evidence at each endpoint was
Price Referencing were included in the search. The noted with cases where some papers related to
search run was (“Pharmaceutical Price Regulation” OR multiple endpoints, and were therefore referenced
“Pharmaceutical Regulation” OR “Cost Containment” multiple times, being taken into account.
OR “Pharmaceutical Pricing” OR “External Price
Referencing” OR “External Price Referencing” OR An excel spreadsheet was used to extract the
“International Price Comparisons” OR “International relevant information on each endpoint for the
Reference Pricing” OR “International Price selected studies. It includes paper titles in the
Referencing”) AND (drug OR drugs OR medicine OR rows, endpoints in the columns and significant
medicines OR pharmaceutical OR pharmaceuticals). information from the texts being extracted and
The search was restricted to keywords present within entered into the respective cells. A comprehensive
abstracts only, to limit the number of irrelevant synthesis of the literature was carried out to identify
papers being returned. When searching the WoS, key trends related to ERP implementation across
the search terms were restricted to title only, as the countries. Results from other systematic literature
option to restrict to abstract was not available. This reviews were included if the selected endpoints
study includes only papers in English. There were no in the review were different to the respective
restrictions in terms of country in the initial search endpoints in this study. This process is significant
to ensure that evidence is representative of a wide in order to minimize bias of results.
geographical range. However, once the search was
concluded, the study was limited to the following 2.4 PRIMARY DATA COLLECTION
countries: Austria, Belgium, Bulgaria, Czech Republic,
As evidence drawn from the systematic literature
Estonia, France, Germany, Greece, Hungary, Italy,
review was not conclusive, primary evidence was
Latvia, Poland, Portugal, Romania, Russia, Slovakia,
Slovenia, Spain, Turkey, Brazil, Egypt, Jordan, Kuwait, collected to complement the secondary evidence
Lebanon, Qatar, Saudi Arabia, South Africa, South findings. Primary evidence was gathered via
Korea and United Arab Emirates. Our study included questionnaires distributed to key stakeholders in
literature published from 2000 to 2016. all study countries, from which there were returns
from 21 countries i.e.: Belgium, Bulgaria, Jordan,
We also completed a targeted and comprehensive Qatar, Italy, Brazil, South Africa, Romania, Slovenia,
search of the WHO, the WHO collaborating Centre for Spain, Germany, Egypt, Latvia, Poland, Portugal,
Pharmaceutical Pricing and Reimbursement policies Russia, Hungary, Greece, France, Estonia and
and the OECD online databases to ensure that no Slovakia. Respondents included representatives
valuable reports were excluded. The key words used from government agencies, industry representatives
to search these were “External Price Referencing” and academics, all of whom expressed personal
OR “External Price Referencing” OR “International views on how ERP is implemented in their respective
Reference Pricing” OR “International Price countries. Beyond understanding the characteristics
Referencing”. Relevant information was recorded and of ERP in different settings, other important
combined with the results of the systematic literature endpoints, such as the national and international
review. Finally, additional literature gathered from effects of implementing ERP, were addressed in the
contacts was also included. questionnaires to increase understanding of how
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 12
different ERP systems perform against 14 basic A combination of both primary and secondary
principles that each country should follow to achieve evidence is presented in the results section. When
an optimal ERP system (see Appendix 1) (Sullivan et evidence from the systematic literature review was
al. 2017). The questionnaire was divided into four used, primary data were used to validate the findings.
sections in order to address specific thematic areas In cases where minimal or outdated evidence was
around ERP and its use within specific jurisdictions. drawn from the systematic literature review, primary
These areas were (i) Objectives and Scope of External data was used.
Price Referencing Systems, (ii) Administration and
Operations, (iii) Methods for the Conduct of External Findings from both primary and secondary evidence
Price Referencing, and (iv) Implementation of were then benchmarked against a framework of
External Price Referencing. 14 basic principles (Sullivan et al. 2017), which
countries should follow in order to achieve an
optimal ERP system (Appendix 1).
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 13
3. RESULTS
3.1 RESULTS OF THE LITERATURE Figure 1: PRISMA flow diagram with search
REVIEW results from the systematic literature review
The database search yielded 6,877 studies and the
results of the systematic literature search were Records identified Additional records
combined with the results from the search of the WHO, through database identified through
the WHO Collaborating Centre for Pharmaceutical searching (n=6,877) other sources (n=143)
Pricing and Reimbursement policies and the OECD
online databases. Additional literature was provided Records after duplicates removed (n=3,979)
by our network. 3,979 studies remained and were
screened based on relevant titles and abstracts by
removing the duplicates using EndNote software Records excluded of
Records screened
(see Figure 1). From the 3,979 studies, 3,526 were irrelevance of title or
(n=3,979)
peer-reviewed papers and 453 were grey literature. abstract (n=3,430)
549 papers were then downloaded and assessed for
eligibility. Many studies were excluded because they
did not relate to ERP, others because they referred Full text articles Full text articles
to internal reference pricing or because only the assessed for eligibility excluded
abstract was available, rather than the full text. (n=549) (n=266)
The main body of 283 texts was then assessed. The
detailed analysis of the studies providing evidence on
Number of articles
each of the endpoints included can be seen in Table Articles excluded
assessed relative to
2. 176 papers were included as final studies in this due to poor evidence
the inclusion criteria
systematic literature review, a significant proportion (n=107)
(n=283)
of which were grey literature (138 studies) with only
38 peer-reviewed papers (Table 2). Throughout the
text, the evidence shown in the tables refers to the Final studies included
latest available source. (n=176)
3.2 OBJECTIVE OF ERP AND ERP to limit pharmaceutical and budget spending
ALIGNMENT WITH HEALTH SYSTEM (Economou, 2010), Turkey introduced ERP in order
OBJECTIVES to control drug expenditure (BMI Research, 2016),
ERP is a commonly implemented pricing policy, Slovenia uses ERP as a tool to regulate the growth of
related to the use of prices of similar drugs to set and public and private drug expenditure (Albrecht et al.,
benchmark domestic prices (BMI Research, 2012). 2009), and in 2010, Russia promoted ERP to regulate
Generally, ERP has three main aims (Kanavos et al., prices (Popovich et al., 2012). In Spain, ERP was
2010): (a) negotiate or set prices within a country, implemented to control drug prices for which there
(b) negotiate coverage and reimbursement and (c) are no alternatives available on the market (Rémuzat
authorize product marketing. The use of ERP has et., 2015); Latvia implements ERP to reimburse
increased significantly as a price control method drugs at manufacturer prices (Behmane, 2007); and
(Kanavos and Vandoros, 2011) in in-patent medicines in Bulgaria, ERP aims to estimate a ceiling price for
and as a cost containment measure due to issues like innovative and generic prescription drugs (Kazakov,
the global financial crash in 2008, the increase in life 2007). In 2004, the Turkish government introduced
expectancy and the increase in prevalence of chronic ERP to contain pharmaceutical expenditure.
conditions (Rémuzat et al., 2015).
However, complicated interrelations between
The general aim of ERP is the attainment of low countries can lead to issues around the achievement
domestic prices to limit pharmaceutical spend. For of these low prices (Barros et al. 2010) due to
instance, Greece implemented price controls through variations in the basket of reference countries,
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 14
Table 2: Results of systematic literature search by source
CINAHL Cochrane Econ- Pro- Pub- Scopus WoS OECD WHO WHO- WHO Net-
Library Lit Quest Med HiT CC- work
PPRI
No. of original
30 11 26 2,169 58 684 796 10 18 60 68 49
studies
Peer-Reviewed
30 11 17 1,899 58 678 796 - - - - 37
studies
Grey Literature - - 9 270 - 6 - 10 18 60 68 12
No. of studies
with relevant
6 1 6 299 12 39 40 10 18 32 37 49
titles &
abstracts
Peer-Reviewed
6 1 6 29 12 39 40 - - - - 37
studies
Grey Literature - - - 270 - - - 10 18 32 37 12
No. of studies
that match 2 0 1 104 5 15 10 10 18 32 37 49
endpoints
Peer-Reviewed
2 - - 11 4 15 10 - - - - 37
studies
Grey Literature - - 1 93 1 - - 10 18 32 37 12
No. of studies
that match
2 0 0 87 2 6 7 8 2 15 27 19
ERP Impact
endpoints
Peer-Reviewed
2 - - 7 2 6 7 - - - - 14
studies
Grey Literature - - 1 80 - - - 8 2 15 27 5
the type of price compared, calculation methods all marketed medicines, or particular categories
employed, exchange rate fluctuations and data of medicines such as reimbursable medicines,
availability (European Commission, 2015). Another prescription-only medicines or innovative medicines
paper in this series examines the impact of variations (European Commission, 2015 and WHO 2015) (Table
in ERP system design within- and across-countries 3). According to the recommendations of EFPIA
on a number of different endpoints including (2014), ERP should be limited to in-patent medicines
pharmaceutical price levels, launch delays and price because: (a) More dynamic and effective methods
convergence (Kanavos et al., 2017) can enhance competitive prices in the off-patent
market (b) Price comparison between in-patent and
3.3 CHARACTERISTICS OF PRODUCTS off-patent drugs undermines patent protection and
intellectual property characteristics.
SUBJECT TO ERP PRICE REGULATION
There are a number of variations in terms of the type Whilst there is some evidence describing the type
of medicines subject to ERP systems. For example, of medicines covered by ERP policies in individual
the system can focus only on in-patent, originator countries (see Table 3), ERP implementation mainly
drugs that are reimbursable (included in the national relates to reimbursable medicines (Vogler et al.,
positive list), or, less commonly, on off-patent, generic 2008); Bulgaria, Romania, Slovenia and Poland
drugs that are paid out of pocket. Generally the use set prices for generic prescribed drugs based on
of ERP is limited to originator products (Leopold international reference pricing policy (Kazakov,
et al. 2012, WHO 2015) but it can be applied to 2007). Russia refers to retail prices of publicly
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 15
Table 3: Type of pharmaceuticals subject to ERP across countries
Pharmaceuticals subject to ERP
All medicines (regardless Only medicines In-patent All drugs
of inclusion in the included in the drugs only regardless of
national positive list) national positive list patent status
Austria ü ü
Belgium ü ü
Bulgaria ü ü
Czech Republic ü ü
Estonia ü ü
France ü ü
Germany ü ü
Greece ü ü
Hungary ü ü
Italy ü ü
Latvia ü ü
Poland ü ü
Portugal ü ü
Romania ü ü
Slovakia ü ü
Slovenia ü ü
Spain ü ü
Egypt ü ü
Jordan ü ü
Kuwait
Lebanon ü
United Arab Emirates ü ü
Brazil ü
Russia ü ü
South Korea ü
Turkey ü ü
South Africa ü
Sources: The authors, adapted from secondary and primary evidence
reimbursed medicines (Rudisill et al., 2014); Latvia, 3.4 IS ERP THE MAIN PRICING POLICY
Poland and Austria use reimbursed drugs (Espin et OR A SUPPORTIVE TOOL?
al., 2014); and Portugal excluded hospital drugs from
Our analysis showed that 29 EU countries
ERP, and Austria includes outpatient drugs in the
implemented ERP as a major or supportive criterion
ERP system (Rémuzat et al. 2014). Many countries
in price determination (European Commission, 2015;
do not specify officially whether ERP is used for the
Paris and Belloni, 2013; Mossialos et al., 2006), either
in-patent or off-patent market.
formally or informally (OECD, 2008), 16 of them use
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 16
international comparisons as a core concept, while to facilitate negotiations between industry and the
some countries focus on specific sectors or specific Medicine Agency (Martini et al., 2012, Ferre et al.,
medicines. The countries of interest are presented in 2014). In Poland ERP serves only a complementary
Table 4 below. role to control the expenditure of the National Health
Fund (Janiszewski and Bondaryk, 2007). In Slovenia
Russia seeks to inform pricing rules through ERP ERP is the main policy used to determine maximum
unofficially (Rudisill et al., 2014). In Belgium ERP is allowed prices, but it is also used in a supplementary
used as a supplementary tool, although comparisons role when prices are set at a particularly high or low
have resulted in price reductions in reimbursed level (European Commission, 2015).
patented drugs over the last five years (Toumi et
al., 2014). Germany introduced ERP to control
reimbursement prices, while Italy changed the role 3.5 TRANSPARENCY OF ERP PRICING
of ERP from the major to a supplementary method POLICY
An ideal ERP system would be a transparent,
Table 4: Main Role of ERP administratively simple process requiring minimal
information input (Kanavos et al., 2010) based on
ERP as main (M) or supportive (S) method statutory pricing rules and regulations (Leopold et
Austria M al., 2012). In reality ERP implementation contains a
Belgium S number of composite points which can be resource
Bulgaria S intensive and administratively complex, resulting in
Czech Republic M poor transparency. The level of transparency can be
Estonia S enhanced by specifying the basket of countries and
France S improving the accessibility of pricing data sources
Germany S used by countries for the referencing process. The
Greece M estimation of medicine prices based on price caps or on
Hungary S
the reference country average promotes predictability
for industry, while flexible negotiations between
Italy S
authorities and industry may lead to a less transparent
Latvia S
procedure (OECD, 2008). Many low-income countries
Poland S
face difficulties in achieving transparency as they
Portugal M
lack a reliable historic and systematic data source on
Romania M medicine prices (Nguyen et al., 2015). This can lead
Slovakia M to ERP system distortion, as decisions will be based
Slovenia M on virtual prices. It is difficult to find information
Spain S on the level of ERP system transparency in different
Egypt M countries but the systematic literature review
Jordan M completed here showed that countries like Austria,
Kuwait M Portugal have highly transparent, well-established
Lebanon M processes (Toumi et al., 2014) whilst countries like
Qatar M Estonia have reduced transparency (Table 5).
Saudi Arabia M
United Arab Emirates M 3.6 COMPETENT AUTHORITIES
Brazil S RESPONSIBLE FOR ERP
Russia S IMPLEMENTATION
South Korea S ERP systems are implemented by different authorities
Turkey M across different countries. In some countries, ERP
South Africa M lies in the jurisdiction of the Ministry of Health and in
Sources: The authors, adapted from secondary and primary others pricing committees or medicines associations
evidence are responsible for the process (see Table 6).
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 17
Table 5: Transparency in ERP across countries
Transparency in price setting
Austria Well-established process
Bulgaria Lack of transparency
Estonia Insufficient granularity on the ERP rules
France See note below1
Germany Insufficient granularity on the ERP rules
Italy Pricing and reimbursement not straightforward. Conflict between government and industry
Portugal Introduction of well-established pricing rules2
Saudi Arabia Concern related to the weight of different factors in estimating prices
Russia Ministry of Health and Social Development of Russia provide official prices for drugs to consumers, which are
included on the essential medicines list.
Notes: 1In France, ERP is a part of an agreement between the Healthcare Products pricing committee and the pharmaceutical companies
(Toumi et al., 2014). The use of France as a reference country led authorities and industry to find many incentives in order to induce
hidden price payback rules. As a result, authorities can buy medicines at a reasonable price and industry can benefit from participation
in a large market. Nevertheless, applied discounts can create a gap between the actual and nominal price, while the actual price is not
public in France. 2Portugal have promoted defined rules about price comparisons in case of non-availability of similar drugs in the
reference countries. (Leopold et al., 2012).
Sources: The authors, adapted from secondary and primary evidence
Table 6: Competent authorities in ERP implementation across countries
Authorities
Austria The Pricing Committee of the Federal Ministry of Health and Women’s Issues
Belgium Ministry of Economic Affairs
Bulgaria National Council for Pricing and Reimbursement of Medicinal Products (NCPR)
Czech Republic State Institute for Drug Control (SUKL)
Estonia Ministry of Health
France Comité Economique des Produits de Sante (CEPS)
Germany National Association of Statutory Health Insurance Funds
Greece EOF and Pricing committee of MOH
Hungary National Health Insurance Fund Administration (OEP)
Italy AIFA
Latvia State Medicines Pricing and Reimbursement Agency (SMPRA) under the Ministry of Health
Poland Ministry of Health
Portugal Infarmed
Romania Ministry of Health
Slovakia Ministry of Health
Slovenia Medicines Agency – Public Agency of the Republic of Slovenia for Medicinal
Spain Interministerial Committee for Pricing and Reimbursement (CIPM)
Egypt Ministry of Health
Jordan Jordan Food and Drug Administration (JFDA)
Kuwait Ministry of Health
Lebanon Ministry of Health
Qatar Ministry of Health
Saudi Arabia Saudi Food and Drug Authority (SFDA)
United Arab Emirates Ministry of Health
Brazil National Health Surveillance Agency (ANVISA)
Russia Ministry of Health and Federal Antimonopoly Service
South Korea The Health Insurance Review & Assessment Service (HIRA) and the National Health Insurance Service (NHIS)
Turkey General Directorate of Pharmaceuticals and Pharmacies
South Africa Pharmaceutical Economic Evaluations (PEE) Directorate
Sources: The authors, adapted from secondary and primary evidence
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 18
3.7 APPEALS BY STAKEHOLDERS TO EU members generally elect to use a reference basket
REGULATOR DECISIONS that contains 5 to 20 countries (Ruggeri and Nolte,
2013). Table 8 (adapted from Kanavos et al. (2010)
There is limited evidence on the presence of an
and Toumi et al. (2014)) highlights the size of country
appeals process for stakeholders. Information was
baskets in European countries and the number
only isolated in one country – the Czech Republic,
of times each country is used as a reference in the
where in June 2008 a newly implemented ERP
basket of another country. Italy currently selects
system set maximum prices for 3,944 products. As a
drug prices by referencing the largest number of
result, at the end of 2008, price cuts led to a number
EU countries, while it is referenced by only a limited
of appeals by industry due to distortion in price
number of reference countries (Austria, Belgium,
regulation (BMI Research, 2010).
France, Germany, Greece, Portugal and Spain). In
Table 7: Presence of appeals process for recent years there has been a trend to increase the
stakeholders basket size (Houy and Jelovac, 2014), potentially as a
means to reduce medicine prices further.
Presence of appeals process for stakeholders
Austria ü Austria expanded its basket of countries from 14 to
Belgium ü 24 countries, while the Czech Republic used only 8
Bulgaria ü countries until 2009 (Leopold et al., 2012). In 2010,
Czech Republic ü
Greece increased its basket to 22 EU countries in
order to reduce pharmaceutical prices and cut
Estonia
pharmaceutical expenditure due to the financial
France
crisis. Other countries have also increased or have
Germany ü
expressed interest in increasing the number of
Greece ü
reference countries they use: Slovakia (from 8
Hungary countries in 2009 to all EU members) and Latvia
Italy (which is carrying out negotiations for the expansion
Latvia ü of the number of reference countries used).
Poland
Germany, UK and France are the most referenced
Portugal ü
countries, because they launch drugs early and two
Romania of them (Germany, UK) employ free pricing methods
Slovakia ü for in-patent drugs (OECD, 2008).
Slovenia ü
Spain ü
3.8 FREQUENCY OF PRICE REVISIONS
Egypt ü
Alongside the number, and choice, of countries, in the
Brazil ü
basket the frequency of price revisions can affect the
Russia
prices derived using ERP. Many EU countries have
Turkey ü
a legal framework that calls for price renewals on a
South Africa ü regular basis with regular intervals lasting from three
Sources: The authors, adapted from secondary and primary months to five years (Rémuzat et al., 2015). Frequent
evidence price revisions may distort the role of the market, as
they may reduce predictability and produce errors,
3.8 NUMBER OF BASKET COUNTRIES
especially when large baskets of countries are used
The number of countries in a basket, and the specific (EFPIA, 2014). Nevertheless, the appropriate interval
countries chosen, can have a significant impact on of price revisions depends on the respective national
resulting drug prices (Houy and Jelovac, 2013) – policy (European Commission, 2015) (See Table 10).
a small number of reference countries could give
significant weight to few countries whilst a large
basket size can increase administrative difficulty
without adding any value.
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 19
Table 8: Overview of baskets across countries
Countries acting as references Basket size
(countries)
AUT BEL BGR HRV CYP CZE DNK EST FIN FRA DEU GRC HUN ISR ISL IRL ITA LVA LTU LUX MLT MDA NLD NOR POL PRT ROU RUS SRB SVK SVN ESP CHE TUR SWE GBR
AUT 24
BEL 26
BGR 10
HRV 3
CYP 10
CZE 17
DNK 9
EST 3
FIN 28
FRA 4
Countries with reference baskets
DEU 0
GRC 22
HUN 29
ISR 8
ISL 4
IRL 9
ITA 27
LVA 7
LTU 8
LUX 0
MLT 11
MDA 9
NLD 4
NOR 9
POL 30
PRT 3
ROU 12
RUS 4
SRB 3
SVK 27
SVN 3
ESP 16
CHE 6
TUR 5
SWE 0
GBR 0
Times
country is 15 16 11 7 10 14 14 11 13 20 20 13 14 0 2 12 17 12 15 9 8 0 15 5 10 15 10 0 1 15 15 19 3 0 12 17
in a basket
Notes: 1Belgium, the Czech Republic, Poland, Hungary, Denmark, Finland and Estonia are included as additional reference countries in
case of non-availability of drug pricing data in other basket countries. 2The Czech Republic and Spain contribute as alternatives in case
of non-availability of drug pricing data in other basket countries. 3Whilst Cyprus has an overall basket of 10 countries the actual price
is based on a selection of countries from each of three sub baskets – high income (Denmark, Germany and Sweden); medium income
(Austria, Belgium, France and Italy); and low income (Greece, Portugal and Spain).
Sources: The authors, adapted from secondary and primary evidence
3.9 CRITERIA FOR BASKET COUNTRY There is limited information on the criteria that
SELECTION most countries use to choose their basket. Most
EU countries use other EU members as references
In terms of basket content, countries mainly take
(OECD, 2008). For instance, the three Baltic countries
into account the following components to create a
(Estonia, Latvia and Lithuania) use each other
basket: (a) geographical characteristics, (b) financial
in their reference baskets as they have common
similarity (Vogler et al., 2011), (c) availability of
socioeconomics factors (Pudersell et al., 2007;
price data, (d) public health status and health
Behmane et al., 2008), while northern and southern
insurance and (e) investment and contribution of
EU countries follow a similar trend (European
pharmaceutical industry in financial performance
Commission, 2015).
(Critchley 2006).
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 20
Table 9: Number of reference countries in basket Table 10: Frequency of price revisions across the
across other non-EU countries studied countries
Countries Number of reference Frequency of price revisions
countries of basket Austria Two additional evaluations at six-month
Brazil1 9 intervals, if reference prices were available
in fewer than 12 EU Member States at
Egypt 36 (and other optional)
the time of the initial evaluation; ad hoc
Jordan 16 revisions
Kuwait Country of origin Belgium At launch only
Lebanon 14 Bulgaria For reimbursed pharmaceuticals- every
6 months, For non-reimbursed- at launch
Qatar Country of origin (and 2 optional) only
Saudi Arabia 30 Czech Republic Annually
South Africa2 5 Estonia For outpatient: on the basis of price
South Korea 7 agreement duration; For inpatient: once,
annually
United Arab Emirates3 31
France Every 4 to 5 years at product re-
Notes: 1Brazil includes the following countries in the basket: assessment
USA, Canada, Portugal, Spain, France, Italy, Greece, New Zealand
and Australia. 2South Africa includes the following countries Germany At launch only, at manufacturer’s request
in the basket: Australia, New Zealand, Canada, Spain. 7Prices and if new evidence becomes available
are set to innovative drugs based on the ex-factory prices in Greece Biannual revision within four years of
seven industrialized countries (BMI Research, 2012). 3Pricing market entry
is set at the median from referenced EU countries, the lowest Hungary At launch only
price paid either in Saudi Arabia or the lowest price of an
active pharmaceutical ingredient in the country of origin (BMI Italy Ad-hoc and periodically depending on
Research, 2015). specific agreements
Sources: The authors, adapted from secondary and primary Latvia Every two years
evidence Poland Ad-hoc and periodically in tiered intervals
(every two, three, or five years)
Portugal Annually
Romania Annually
Slovakia Twice per year
Slovenia Twice per year
Spain Every two years and ad hoc
Egypt At launch, at manufacturer’s request and
on a random basis
Jordan Every 2 years (plus four months after th
reduction of prices in a reference country)
Kuwait At launch only
Lebanon Every 5 years
Qatar At launch only
Brazil At launch only
Russia At manufacturers’ request
South Africa At manufacturers’ request
Sources: The authors, adapted from secondary and primary
evidence
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 21
Table 11: Criteria for basket selection across Table 12: Price selection across countries
studied countries
Type of comparator price used
Criteria for basket selection Austria Ex-factory price
Austria All EU countries Belgium Ex-factory price
Belgium Geographical proximity and comparable Bulgaria Ex-factory price
GDP levels
Czech Republic Ex-factory price
Bulgaria Not well defined criteria; usually countries
Estonia Ex-factory price
with similar GDP
France The starting point is the price claimed
Czech Republic All EU countries
by the manufacturer; negotiation can
Estonia Geographical proximity and comparable use the ex-factory price
GDP levels
Germany Retail price (NB: ERP as guidance)
France Geographical proximity and comparable
Greece Ex-factory price
GDP levels
Hungary Ex-factory price
Germany Geographical proximity and comparable
GDP levels Italy Ex-factory price
Greece All EU countries Latvia Ex-factory price
Hungary Geographical proximity Poland Ex-factory price
Italy ERP system is increasingly redundant Portugal Ex-factory price
Latvia Socioeconomic criteria Romania Ex-factory price
Poland All EU countries Slovakia Ex-factory price
Portugal The countries selected for the basket must Slovenia Ex-factory price
have a similar per capita GDP to Portugal Spain Ex-factory price
Romania No clear criteria are used to select basket Egypt Retail price
countries
Jordan Ex-factory price
Slovakia Geographical proximity
Lebanon Wholesale price
Slovenia Geographical proximity
Saudi Arabia Ex-factory price
Spain Countries where the medicines are
United Arab Emirates Wholesale price
available
Brazil Ex-factory price
Egypt Geographical proximity, comparable GDP
levels and the country of origin of the Russia Wholesale and retail price
product South Korea Ex-factory price
Lebanon The price of an imported drug is based on Turkey Ex-factory price
the cost in the country of origin
South Africa Ex-factory price
Brazil Countries with profile similar to Brazil
Sources: The authors, adapted from secondary and primary
Russia Countries with similar GPD per capita level
evidence
and consideration of the country of origin
South Korea South Korea does not specify the countries
in the basket and decide on an ad-hoc basis
Turkey Lowest in EU + geographical criteria
South Africa Countries where prices are accessible
and are regulated. Quality standards of
countries also need to be similar.
Sources: The authors, adapted from secondary and primary
evidence
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEThe Implementation of External Reference Pricing within and across Country Borders 22
Table 13: Method for calculation of reference 3.10 TYPE OF COMPARATOR PRICE
price across countries USED IN ERP
Method of calculation of reference price Most European countries have used ex-factory
prices in their international comparisons (Kalo et
Austria Average across basket
al., 2015), because this method helps to minimize
Belgium Average across basket
price deviations that may arise due to differences
Bulgaria Lowest price in basket
in distribution mark-ups (Nguyen et al, 2015). The
Czech Average of the three lowest prices in basket
implementation of ERP using the ex-factory price is
Republic
considered to be more suitable than other methods,
Estonia Price cannot exceed the highest price in the
basket for example, using the wholesale price, as distribution
France “Prices similar to reference countries and not
margins and tax rates are different across countries
lower than the lowest price” leading to difficulties in international comparisons
Germany Weighted based on market size and (EFPIA, 2014). However, there are some countries
purchasing power parity that use the wholesale price and some that use the
Greece Average of the three lowest prices in basket pharmacy retail price (Espin et al., 2014) (see Table
12). ERP is generally based on officially published
Hungary Lowest price in basket
prices. Since price negotiations and discounts are
Italy Average across basket
kept confidential within a country most countries
Latvia Third lowest price among Denmark, Czech
will be using reference prices that may be higher
Republic, Romania, Slovakia and Hungary
than the negotiated price enjoyed in the reference
Poland Lowest price in basket country.
Portugal Follows different calculation methods
depending on the sector. Outpatient: country
average, Inpatient: lowest price 3.11 METHODS FOR CALCULATION OF
Romania Lowest price in basket THE REFERENCE PRICE
Slovakia Average of the three lowest prices in basket Generally, the most preferred method of reference
price calculation is the use of an average formula
Slovenia Lowest price in basket
(Gandjour, 2013) although there are other
Spain Lowest price in basket
mechanisms in use, such as using the average
Egypt Lowest price in basket of the n lowest or the lowest price in the basket.
Jordan Average across basket (European Commission, 2015). In the countries
Lebanon The price of an imported drug is based on the studied in this paper using a lowest price based
cost in the country of origin. Final price needs
calculation is the most common (Table 13), against
to be lower than one of the following: (i) The
ex-factory price in the country of origin. (ii) the recommendation of EFPIA (2014) which states
Import prices charged for the same brand that an average price be used to enhance fairness.
in seven countries in the Middle East.(iii) According to our results, some countries may include
The median manufacturers’ price in seven
European countries, or (iv) The import price
more than one criterion to set the reference price of
of similar drugs that are already marketed in a product, while other members may not refer to the
Lebanon. selected method officially.
Saudi Arabia Lowest price in basket
United Arab Lowest price in basket 3.12 SOURCES OF INFORMATION FOR
Emirates
Brazil Lowest price in basket
PRICING DECISIONS
Russia Lowest price in basket The implementation of ERP requires access to price
South Korea Average across basket
information and according to EFPIA (2014), this
data should be publicly available and reliable. Non-
Turkey Lowest price in basket
availability, price heterogeneity, non-reliability and a
South Africa Lowest price in basket
lack of transparency can reduce the effectiveness of
Sources: The authors, adapted from secondary and primary ERP (Rémuzat et al., 2015). Many countries support
evidence
free access to price data, although the extent that
LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCEYou can also read