The Effects of Immersive Virtual Reality in Reducing Public Stigma of Mental Illness in the University Population of Hong Kong: Randomized ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

JOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Original Paper
The Effects of Immersive Virtual Reality in Reducing Public Stigma
of Mental Illness in the University Population of Hong Kong:
Randomized Controlled Trial
Anna S Y Yuen, BSocSci; Winnie W S Mak, PhD
Department of Psychology, The Chinese University of Hong Kong, Hong Kong, Hong Kong
Corresponding Author:
Winnie W S Mak, PhD
Department of Psychology
The Chinese University of Hong Kong
Room 354, Sino Building
Hong Kong
Hong Kong
Phone: 852 3943 6577
Email: wwsmak@cuhk.edu.hk
Abstract
Background: Public stigma in mental health often brings various adverse effects on people with mental illness. Researchers
have been developing different interventions in combating public stigma.
Objective: This study investigates the effects of immersive virtual reality (IVR) in reducing the public stigma of mental illness
using a single-blinded randomized control trial.
Methods: A pre-post experimental design with a 1-week follow-up was conducted. Participants (N=206) were recruited through
the mass mail system of The Chinese University of Hong Kong and randomized into 3 conditions: immersive animation, text,
and control. In the immersive animation condition (n=72), participants experienced the simulation of daily life and the stigma
experienced as an animated story protagonist with mixed anxiety and depressive disorder with IVR. In the text condition (n=65),
participants experienced an identical story to the immersive animation condition with first-person audio narration using the same
virtual reality headset. In the control condition (n=69), participants watched a video about planets with IVR. All participants
received interventions with a researcher-assisted Oculus Go virtual reality headset. Participants’ public stigma was measured
through self-administered online questionnaires and compared across conditions and at different time points using repeated
measures analysis of variance. Simple and sequential mediation analyses on the relationship of condition (immersive animation
vs text) and follow-up public stigma with possible mediators, including sense of embodiment and story transportation, were
conducted using PROCESS.
Results: Public stigma did not differ significantly across conditions at pre-experiment (P>.99). In the immersive animation and
text conditions, public stigma was significantly reduced at postexperiment and at the 1-week follow-up compared to pre-experiment
(all with P.99). In simple mediation models, both sense of embodiment (95% CI –0.22 to 0.46) and story transportation (95% CI –0.18
to 0.00) were not significant mediators. In the sequential mediation model, both sense of embodiment and story transportation
were significant sequential mediators. Sense of embodiment was positively associated with story transportation (P
JOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
(J Med Internet Res 2021;23(7):e23683) doi: 10.2196/23683
KEYWORDS
immersive virtual reality; narrative persuasion; public stigma; mental health stigma; sense of embodiment; story transportation;
stigma intervention
However, as in vivo contact required presenters to travel to
Introduction venues and be well trained, it could be tedious and hard to
Background implement widely and frequently [4]. Researchers have therefore
investigated the possibilities of using other types of contact
One of the biggest challenges that people with mental illness [4,20,21]. Filmed contact has been used, and it yielded similar
face is psychiatric stigma [1,2]. Stigma refers to a phenomenon or weaker effects than in vivo contact [4,19-21]. Recently,
in which people are socially discredited as a result of their social researchers have begun to investigate the effect of immersive
identity, health condition, or other characteristics deemed virtual reality (IVR) in reducing public stigma, although this
“undesirable” by the dominant group [3]. The public’s effort is limited [22].
stereotypical and negative beliefs, prejudicial emotional
reactions, and discriminatory responses toward minority or Reducing Public Stigma With Immersive Virtual
disadvantaged groups in the society are referred to as public Reality
stigma [2,4,5]. People endorsing public stigma toward people With technological advancement, IVR becomes a possible
with mental illness often make negative but inaccurate option to reduce negative stereotypes and prejudice. IVR allows
assumptions about them, including that people with mental people to be put into another character by changing their body
illness are violent, dangerous, weak, and childlike [2,6-10]. representation [23-25]. It is done by a process referred to as
People with public stigma also tend to negatively label people virtual embodiment, in which individuals can see a virtual body
with mental illness as “them” and regard them as fundamentally substituting their bodies through a head-tracked head-mounted
different and undesirable to be part of “us” [2,11]. display [23,24]. Some can even wear body-tracking suits to
Public stigma often hampers the recovery and reintegration of induce synchronous virtual body movements [24]. Previous
people with mental illness into society [9,12]. For example, the research revealed that IVR could successfully induce ownership
public who hold prejudice toward people with mental illness as over bodies and identities of outgroups and significantly reduce
childlike and having mental illness due to weak character may negative stereotypes, including reducing implicit racial bias
discriminate against them through supporting coercive treatment [24] and stigma toward older adults [26]. The public generally
[13]. The public who find people with mental illness fearful regard people with mental illness as different and outgroup
may call for institutional segregation and avoidance [13]. People members [2,11]. With IVR, participants could have first-person
with mental illness are often deprived of employment experiences as people with mental illness. They might regard
opportunities [5,10,14] or are falsely alleged to be involved in people with mental illness as ingroup members and have lower
violent crimes [2]. Recognizing the existence of public stigma, stigma. With the aids of immersive experience, participants’
some people with mental illness may concur and internalize identities and perspectives might also be changed more easily
these public views, leading to self-stigma [2,10,15,16]. The and substantially than nonimmersive means. Therefore, this
“why try” model has illustrated the complex process of how study applies IVR and compares it to a nonimmersive medium
people with mental illness may be aware of, agree with, and to investigate its effects in reducing public stigma toward mental
apply the stereotypes of mental illness [17]. As a result, illness.
self-esteem and self-efficacy are undermined, which yields “why In previous IVR research related to mental health public stigma,
try” responses in pursuit of life goals [17]. People with mental they mainly focused on the simulation of schizophrenic
illness may think they are not worthy of attaining life symptoms [22,27]. Instead of reducing stigma, simulation of
achievements [17] and have reduced help-seeking behavior symptoms through IVR further increased social distance with
[1,5,14,16,17]. Regarding these alarming consequences brought people with schizophrenia [22]. Simulation of auditory
by stigma, varied efforts have been advocated to reduce public hallucination without using IVR also yielded similar results
stigma and empower people with mental illness. [27-29]. In these studies, some comparison groups even reduced
Prior Work of Combating Public Stigma greater stigma than the simulation conditions [22,29]. Often,
the comparison groups highlighted other components than just
Past efforts in combating public stigma found education and
symptoms, such as feelings, treatments, difficulties, and
contact between the public and people with mental illness to be
accomplishments of a person with mental illness [22,29].
the most effective strategies [5,7,18]. Education mainly aims
Similarly, in the few virtual reality studies, both immersive and
at replacing stigmatizing myths with accurate information and
nonimmersive, that had successfully reduced public stigma, the
knowledge, and contact attempts to replace negative stereotypes
simulation condition was either paired with written empathetic
with a positive experience through interpersonal contact on an
tasks [22] or participants could get information more than
equal footing [7]. Education and contact significantly led to
symptoms [30]. For example, participants could understand
positive attitudinal change. Among all, contact seemed to yield
symptoms, biographies of people with mental illness, and false
the most efficacious effect in reducing public stigma, especially
negative beliefs in the virtual reality [30]. They were found to
for adults [2,5,19].
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 2
(page number not for citation purposes)
XSL• FO
RenderX
JOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
have decreased stereotypes and perceived dangerousness of the possible sequential effects of sense of embodiment and story
people with schizophrenia [30]. transportation in the same mediation model. In this study,
participants would be experiencing the story as the protagonist.
Therefore, rather than emphasizing symptom simulation, this
Therefore, embodying the avatar could readily enable the
study took a person-centered approach by simulating the daily
participants to become the story protagonist themselves and be
life interactions and stigmatized experience of a person with
part of the virtual settings. Thus, it was hypothesized that sense
mental illness. We hypothesized that IVR that immersed
of embodiment might increase story transportation, leading to
participants into the everyday living of someone with mental
reduced public stigma.
illness could significantly reduce public stigma toward mental
illness.
Methods
Hypothesized Mediation Models of Immersive Virtual
Reality and Public Stigma Trial Registration
This study was approved by the Survey and Behavioral Research
Sense of Embodiment as Mediator Ethics Committee at The Chinese University of Hong Kong
To examine how the IVR might affect public stigma, mediation (approval reference number: SBRE-18-078). It is registered at
analyses were also conducted. To expand the proposed idea of The Centre for Clinical Research and Biostatistics Clinical Trial
IVR changing stigma through virtual embodiment, one proposed Registry (trial registration number: CUHK_CCRB00638).
mediator was sense of embodiment. It refers to the sensations
of being inside, controlling, and having ownership over an Recruitment
artificial body [23]. It is possible because our body schema and The study was conducted from January to March 2019. A
the concept of the self are labile [31]. Through mapping the single-blinded randomized controlled trial was used for this
physical body to the virtual body, our body schema can be study. According to previous studies that aimed at changing
radically altered to the virtual one [32]. As an avatar’s body can attitudes to outgroup members using IVR, a medium effect size
embed different social roles or meanings, our social identities was observed [24]. Meta-analysis showed that video contact
may also be altered accordingly [33]. Previous IVR literature and in vivo contact had medium to large effect sizes respectively
on racial bias had suggested that with sense of embodiment, on changing stigmatizing attitude [19]. With IVR having
participants embedded new physical and conceptual identities stronger perceptive stimulation than video contact, but less
[33]. Other racial groups might become in-group to the intense and interactive than in vivo contact, a medium effect
participants, leading to generalization of affective processing size was hypothesized. Assuming a medium effect size
and positive evaluation of the race and a reduction in racial bias (ηρ2=0.06) with 80% power and a probability of a type I error
[33]. Thus, this study hypothesized that sense of embodiment of 0.05, a total sample size of 141 was needed. Participants were
could mediate IVR’s relationship with stigma reduction though recruited through the mass mail system of The Chinese
changing body schema and social identity. University of Hong Kong. The purpose of this study and
Story Transportation as Mediator assignment of conditions were concealed until the debriefing
session at the end of the entire study. The email and informed
Another proposed mediator was story transportation. It describes
consent form only stated that the experiment would be related
how much an individual can be immersed in a story [34,35].
to IVR. Since the content of the interventions were in Chinese,
With strong story transportation, readers can have their
participants who were 18 years or older and fluent in Chinese
cognition, affection, and attention dominated by the story
were eligible for this study. After completing the pre-experiment
[34-37]. Story transportation was suggested to have various
questionnaire online, participants who failed to answer attention
effects on belief and stigma change [38-43]. It might reduce
check questions correctly (eg, “Please choose extremely
cognitive and elaborative activities that resist persuasion [42,43].
disagree.”) were excluded to ensure that participants were
It could also elicit broad affective responses that allow
answering the questions diligently. Participants who failed to
participants to be more receptive to belief change [42]. People
provide correct contact information or any available experiment
might also have more vivid mental images that make contents
time slots were also excluded. Afterward, each participant was
and messages more memorable, leading to a greater intention
randomly assigned into one of the three conditions: IVR
of belief change [42,43]. A previous empirical study had shown
animation (immersive animation), the first-person audio
that with story transportation, participants felt related to the
narration of the same story (text), and IVR space control
story protagonist through reading a written vignette and had
(control). Simple randomization was used with computerized
reduced social distance with people with depression [37]. With
random numbers. Upon signing the consent form online with
various special features of IVR, such as the first-person field
checkboxes, participants were administered their assigned
of view and tracking of head movements, IVR might result in
condition and completed an online postexperiment questionnaire
stronger engagement with the story [44], thus stronger stigma
immediately in the experiment room and 1 week after the
change than a nonimmersive medium.
experiment at home. A total of HK $50 (US $6.44) were given
Sense of Embodiment and Story Transportation as to each participant as a remuneration of time after the
Sequential Mediators accomplishment of the experiment. Responses from participants
who completed the postexperiment and follow-up questionnaires
Besides testing a sense of embodiment and story transportation
were analyzed.
as stand-alone mediators, this study also attempted to explore
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 3
(page number not for citation purposes)
XSL• FO
RenderX
JOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
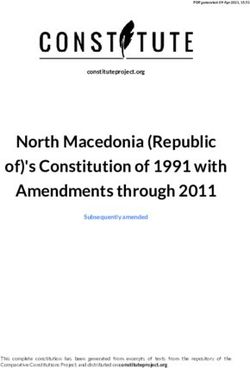
Experimental Conditions who had mixed anxiety and depressive disorder. In the IVR,
All experimental conditions were around 10 minutes long. To Yan’s body would be in the position of the participants’ bodies.
avoid any placebo effect and to keep other factors constant, all Participants would be seeing things from Yan’s perspective
three conditions were conducted with a researcher-assisted (Figure 1). The story started with Yan working at the office.
virtual reality headset, Oculus Go (Facebook), which could The scene then changed to Yan sitting on a sofa alone at home,
provide 360° head-tracking IVR with corresponding audio and where stigma from colleagues and pressure from work and
sound effects. With the exception of the researcher assisting family were illustrated. Afterward, Yan talked to her uncle who
with the operation of the IVR headset at the commencement of was visiting. The uncle was an antagonist who stigmatized and
the experiment, all presentation of experimental content was imposed more pressure onto Yan. Yan’s field of view would
automatic with minimal technical support from the researcher sink while the uncle talked, and everything else would seem
to minimize researcher bias. All participants received their larger and higher to create a sense of inferiority. There were
assigned condition in a dark room while seated on a swivel also pop-up messages on the side to illustrate the problematic
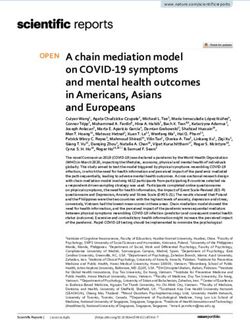
chair. issues in the uncle’s speech during the conversation (Figure 2).
Examples included trivializing experience, attributing all
In the immersive animation condition, participants were responsibilities to the person, and advice-giving without
immersed in an animated story as the female protagonist, Yan, consideration of appropriateness.
Figure 1. Screenshot of participants seeing the female protagonist’s, Yan’s, body in the immersive animation condition.
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 4
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Figure 2. Screenshot of Yan talking to her uncle, and showing how messages pop up to illustrate problematic issues in the uncle’s speech in the
immersive animation condition.
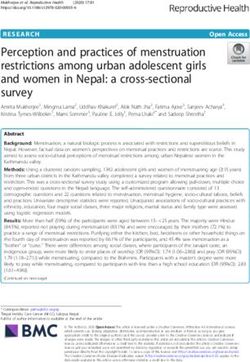
In the text condition, participants read the text and listened with was a conventional medium that provided a rigorous comparison
audio narration to the same story as the immersive animation to the immersive animation condition. It kept the story
condition. Participants still wore the virtual reality headset to components identical except for the visual inputs and immersive
avoid any placebo effect. However, they read the story in a experience in the IVR. This condition was compared with the
textual and 2D format on a white background with black text immersive animation condition in both the main effects of
(Figure 3). To investigate the separate effects of visual inputs stigma reduction and mediation analyses. It allowed examination
in the IVR condition, the first-person voice-over and sound of possible mechanisms of how IVR might affect public stigma
effects in the IVR remained unchanged here and accompanied differently than nonimmersive means through proposed
the text in accordance to the story development. This condition mediators.
Figure 3. Screenshot of the text condition.
In the control condition, participants watched a 360° exoplanet created by the University of Exeter Astrophysics group in
virtual reality video with corresponding audio and sound effects. partnership with We the Curious and Engine House VFX. This
The exoplanet video was titled “Take a Virtual Reality tour of video was used in the study by permission of the University of
six REAL exoplanets” on YouTube with its copyright owned Exeter.
by the University of Exeter, 2018 (Figure 4). The video was
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 5
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Figure 4. Screenshot of the space control condition.
Mediators
Measures
Sense of Embodiment
The Main Effect on Public Stigma
To account for possible mediation effects, sense of embodiment
To measure changes in public stigma, the 21-item Public Stigma and story transportation were measured post experiment in the
and Acceptance Scale [45] was used at pre-experiment, immersive animation and text conditions. Since the topic of
postexperiment, and 1-week follow-up. It measures public interest was on what might influence change in public stigma
stigma and acceptance toward mental illness on a 6-point Likert and how IVR’s effect differed from the conventional audio
scale from 1 (strongly disagree) to 6 (strongly agree). It consists narration, scales on mediation were not administered in the
of two subscales, 12 items measuring public stigma (eg, “People control condition.
with mental illness are a burden to the society.”) and 9 items
measuring personal advocacy toward accepting people with Although previous studies have measured sense of embodiment
mental illness (eg, “I take the initiative to reach out to people [24,46,47], the items were mostly context-specific to the virtual
with mental illness.”). The higher the mean scores of the public environments and avatars in those studies. Therefore, with no
stigma subscale and the lower the mean scores of the personal standardized scale available, a 7-item Sense of Embodiment
advocacy subscale, the greater the stigma and the lower the Scale was developed to fit this experiment context based on
acceptance toward mental illness. For the total mean scores, previous virtual reality studies [24,46,47] and rubber hand
items in the personal advocacy subscale were reverse coded so illusion literature [48]. Seven items were developed based on
that higher total mean scores indicated greater stigmatizing components that were commonly shared among the previous
attitudes. In this study, total mean scores of all items were used literature, such as ownership (eg, “I felt like I was looking at
to measure public stigma. Possible total mean scores ranged my own body when I looked at Yan’s.”) and agency (eg, “If I
from 1 to 6. The Cronbach α of the public stigma and personal had wanted, I felt like I could have controlled Yan’s body.”).
advocacy subscales were .92 and .87, respectively. The overall Items were rated on a 7-point Likert scale from 1 (strongly
Cronbach α was .93 for the entire scale in this study. disagree) to 7 (strongly agree; see Textbox 1 for complete scale
items). The higher mean score indicated a greater sense of
embodiment. The Sense of Embodiment Scale had a Cronbach
α of .85 in this study.
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 6
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Textbox 1. Items in the Sense of Embodiment Scale, with items 6 and 7 as reversed items.
1. I felt as if I was looking at my own body when I looked at Yan’s.
2. When Yan was sitting on the sofa, I felt as if I was sitting on the sofa.
3. I felt as if Yan’s body was my body.
4. When the uncle was talking to Yan, I felt as if he was talking to me.
5. If I had wanted, I felt like I could have controlled Yan’s body.
6. I found it difficult to get into the role of Yan.
7. I felt as if I was an outsider to the story.
models, Pearson correlations of condition (immersive animation
Story Transportation
vs text), sense of embodiment, story transportation, and
The Transportation Scale [36] measures how well an individual follow-up public stigma were obtained. A simple mediation
is absorbed into a story. Some wordings of the 15-item scale analysis was conducted with the condition (immersive animation
were modified to fit the current context (eg, changing “While vs text), sense of embodiment, and follow-up public stigma. A
reading the narrative I had a vivid image of Katie” to “While similar simple mediation analysis was also conducted using
experiencing the story I had a vivid image of Yan.”). The scale story transportation as the mediator. To further investigate the
was rated on a 7-point Likert scale from 1 (strongly disagree) relationship of sense of embodiment and story transportation,
to 7 (strongly agree). The higher mean score indicated greater sequential mediation analysis was also conducted. The condition
devotion in the story. The Transportation Scale had a Cronbach (immersive animation vs text) and follow-up public stigma were
α of .79 in this study. put into the model, having sense of embodiment and story
The Public Stigma and Acceptance Scale and the Sense of transportation as sequential mediators. The level of statistical
Embodiment Scale were originally developed in Chinese. The significance was set at P≤.05 threshold (two-tailed) and
Transportation Scale was translated into Chinese and determined by 95% CIs. PROCESS on SPSS was used to
back-translated into English to check on conceptual equivalence. generate all the mediation analyses. Model 4 was used to
generate simple mediation analyses, and model 6 was used to
Data Analysis generate sequential mediation analysis according to the
Analyses were conducted using SPSS 24.0 for Mac (IBM Corp). suggestion of Hayes [49].
First, descriptive statistics were obtained. Information related
to age, gender, education, occupation, sexual orientation, Results
religious belief, marital status, mental illness history, and
previous social contact with people with mixed anxiety and Participants
depressive disorder was obtained. Chi-square tests on nominal Data from 206 participants were analyzed. Out of the 298
demographic variables and one-way analysis of variance participants who provided informed consent and completed the
(ANOVA) on continuous variables were conducted to examine pre-experiment questionnaire, 18 participants who failed to
any systematic differences on demographics among the 3 groups. answer the attention check questions correctly, 1 participant
If there were any systematic differences among the groups, who failed to provide adequate contact information, and 35
results would be adjusted, controlling for possible confounders. participants who failed to provide available experiment time
Second, to compare the change in public stigma, repeated slots were excluded (Figure 5). A total of 244 participants were
measures ANOVA was used. The main effect of groups randomized into the three conditions. A total of 35 participants
(immersive animation vs text vs control), time (pre-experiment, who did not show up and 3 participants who applied to the same
postexperiment, follow-up), and their interaction effect (time experiment twice were excluded. A total of 206 participants
× group) were examined. The level of statistical significance went through the experiment and completed questionnaires post
was set at a P≤.05 threshold (two-tailed). If a significant effect experiment and at a 1-week follow-up. The final sample size
was found, post hoc analysis was conducted. was 72 for the immersive animation condition, 65 for the text
Bonferroni-adjusted pairwise comparisons were used to avoid condition, and 69 for the control condition, with a total sample
inflated type I error. Third, to test the proposed mediation size of 206.
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 7
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Figure 5. CONSORT (Consolidated Standards of Reporting Trials) diagram of participant recruitment.
For demographic information, see Table 1. The mean age of (n=153, 74.3%). Among the 206 participants, 92 (44.7%) had
participants was 21.76 (SD 5.04, range 18-64) years. Out of the social contact with people with mixed anxiety and depressive
206 participants, 114 (55.3%) were females and 91 (44.2%) disorder before. Chi-square tests on demographic variables and
were males. Most participants had a Bachelor’s degree (n=166, one-way ANOVA on continuous variables were conducted. No
80.6%) and were single (n=198, 96.1%), students (n=173, systematic differences in any demographic variables among the
84.0%), and heterosexual (n=183, 88.8%). Most of them had three conditions were found. Demographics variables were not
no mental illness history (n=198, 96.1%) and no religious belief expected to impact the results in this study.
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 8
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Table 1. Participant demographic data.a
Characteristic Total (N=206) Immersive animation Text (n=65) Control (n=69) P value differ-
(n=72) ence across
conditions
Age (years), mean (SD) 21.76 (5.04) 21.57 (4.18) 21.95 (6.31) 21.77 (4.55) .91
Gender, n (%) .68
Female 114 (55.3) 38 (52.8) 35 (53.8) 41 (59.4)
Male 91 (44.2) 33 (45.8) 30 (46.2) 28 (40.6)
Others 1 (0.5) 1 (1.4) 0 (0.0) 0 (0.0)
Education, n (%) .37
High school 6 (2.9) 1 (1.4) 1 (1.5) 4 (5.8)
Bachelor’s degree 166 (80.6) 60 (83.3) 54 (83.1) 52 (75.4)
Master’s degree 27 (13.1) 10 (13.9) 7 (10.8) 10 (14.5)
PhD 2 (1.0) 1 (1.4) 0 (0.0) 1 (1.4)
Others 5 (2.4) 0 (0.0) 3 (4.6) 2 (2.9)
Faculty, n (%) .93
Arts 25 (12.1) 9 (12.5) 8 (12.3) 8 (11.6)
Business 51 (24.8) 17 (23.6) 17 (26.2) 17 (24.6)
Education 14 (6.8) 7 (9.7) 4 (6.2) 3 (4.3)
Engineering 16 (7.8) 5 (6.9) 5 (7.7) 6 (8.7)
Law 2 (1.0) 0 (0.0) 1 (1.5) 1 (1.4)
Medicine 25 (12.1) 5 (6.9) 11 (16.9) 9 (13.0)
Science 27 (13.1) 12 (16.7) 6 (9.2) 9 (13.0)
Social science 44 (21.4) 16 (22.2) 12 (18.5) 16 (23.2)
Others 2 (1.0) 1 (1.4) 1 (1.5) 0 (0.0)
Occupation, n (%) .29
Student 173 (84.0) 63 (87.5) 57 (87.7) 53 (76.8)
Full-time employment 29 (14.1) 8 (11.1) 7 (10.8) 14 (20.3)
Others 4 (1.9) 1 (1.4) 1 (1.5) 2 (2.9)
Sexual orientation, n (%) .68
Heterosexual 183 (88.8) 66 (91.7) 58 (89.2) 59 (85.5)
Homosexual 11 (5.3) 3 (4.2) 4 (6.2) 4 (5.8)
Bisexual 7 (3.4) 2 (2.8) 2 (3.1) 3 (4.3)
Others 5 (2.4) 1 (1.4) 1 (1.5) 3 (4.3)
Religious belief, n (%) .15
No religious belief 153 (74.3) 47 (65.3) 53 (81.5) 53 (76.8)
Christian 43 (20.9) 22 (30.6) 9 (13.8) 12 (17.4)
Others 10 (4.9) 3 (4.2) 3 (4.6) 4 (5.8)
Marital status, n (%) .42
Single 198 (96.1) 68 (94.4) 62 (95.4) 68 (98.6)
Married 8 (3.9) 4 (5.6) 3 (4.6) 1 (1.4)
Mental illness history, n (%) .46
Yes 8 (3.9) 4 (5.6) 1 (1.5) 3 (4.3)
No 198 (96.1) 68 (94.4) 64 (98.5) 66 (95.7)
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 9
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Characteristic Total (N=206) Immersive animation Text (n=65) Control (n=69) P value differ-
(n=72) ence across
conditions
Social contact with people with MADDb, n (%) .64
Yes 92 (44.7) 29 (40.3) 31 (47.7) 32 (46.4)
No 114 (55.3) 43 (59.7) 34 (52.3) 37 (53.6)
a
All percentages may not total to 100% due to rounding.
b
MADD: mixed anxiety and depressive disorder.
P=.003). The text group (mean 2.47, SD 0.62) yielded similar
Changes in Public Stigma results by having significantly lower public stigma than the
Repeated measures ANOVA on public stigma yielded a control group (P=.007). A similar pattern of results was also
significant interaction (time × group) effect (F4,404=5.2; P.99). Post experiment, the immersive However, the immersive animation and text groups did not
animation group (mean 2.45, SD 0.63) had significantly lower differ from each other significantly at postexperiment and at
public stigma than the control group (mean 2.80, SD 0.63; the 1-week follow-up (P>.99; see Table 2 for descriptive
statistics and Table 3 for detailed pairwise comparison).
Table 2. Public stigma scores across conditions at different time points.
Time points Immersive animation (n=72), mean (SD) Text (n=65), mean (SD) Control (n=69), mean (SD)
Pre-experiment 2.73 (0.64) 2.78 (0.68) 2.84 (0.64)
Postexperiment 2.45 (0.63) 2.47 (0.62) 2.80 (0.63)
Follow-up 2.52 (0.66) 2.53 (0.68) 2.82 (0.61)
Table 3. Detailed Bonferroni-adjusted pairwise comparison of public stigma between conditions at different time points.
Time points Condition Condition for comparison Mean difference (SE) P value
Pre-experiment Immersive animation Text –0.05 (0.11) >.99
Pre-experiment Immersive animation Control –0.11 (0.11) .99
Pre-experiment Text Control –0.06 (0.11) >.99
Postexperiment Immersive animation Text –0.02 (0.11) >.99
Postexperiment Immersive animation Control –0.36 (0.11) .003
Postexperiment Text Control –0.33 (0.11) .007
Follow-up Immersive animation Text –0.01 (0.11) >.99
Follow-up Immersive animation Control –0.30 (0.11) .02
Follow-up Text Control –0.29 (0.11) .03
In the immersive animation group, a significant time effect was followed a similar pattern of time effect as the immersive
found (F2,202=20.0; PJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Mediation Analyses correlations of variables included in the mediation analyses,
The mean scores of sense of embodiment, story transportation, including condition (immersive animation vs text), sense of
and follow-up public stigma are reported in Table 4. Pearson embodiment, story transportation, and follow-up public stigma
are also reported in Table 4.
Table 4. Correlations and descriptive statistics of variables included in the mediation analyses.
Variables Correlations of variables included in the mediation analyses
Condition (immersive Sense of embodiment Story transportation Follow-up public stigma
animation vs text)
Condition (immersive animation vs text)a
r 1 0.49 0.17 –0.004
P value — b .99
Sense of embodiment
r 0.49 1 0.512 –0.091
P valueJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Figure 6. Simple mediation model of the condition, sense of embodiment, and public stigma.
Figure 7. Simple mediation model of the condition, story transportation, and public stigma.
Sense of embodiment and story transportation were then put t134=6.68; PJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Figure 8. Sequential mediation model of the condition, sense of embodiment, story transportation, and public stigma.
emphasized the existence of positive symptoms, instead of
Discussion allowing participants to understand and feel other aspects of
Overall Effect of Immersive Animation on Public the living experience. Positive symptoms that could be perceived
as uncontrollable and dangerous by the public might deter
Stigma
participants from engaging with people with schizophrenia [50].
This study compared the effect of IVR and text with audio Therefore, simulating positive symptoms might increase social
narration in reducing public stigma. Both IVR and text with distance and discrimination instead.
audio narration successfully reduced public stigma, and the
effect was sustained at the 1-week follow-up. In contrast, the On the other hand, different from the hypothesis, IVR did not
control space video did not elicit any change in public stigma outperform text with audio narration in reducing public stigma
as expected. It could be inferred that the simulation of daily significantly. In the few stigma studies that compared virtual
interactions and stigma experienced by a person with mental reality with a rigorous comparison group, it was shown that
illness could effectively reduce public stigma. The result also only virtual reality with interactive components such as allowing
supported the hypothesis that IVR could successfully reduce participants to move closer to other virtual characters had
public stigma. significantly reduced greater stigma than the written vignettes
of people with mental illness [51]. Immersive experience without
The results were consistent with previous studies that used IVR active interaction did not outperform the written vignettes in
to reduce negative stereotypes toward outgroup members, stigma reduction [22]. Therefore, the visual immersive
including other racial groups [24] and older adults [26]. In the experience of IVR might not be strong enough to induce a
mental health setting, it was also consistent with virtual reality significant difference than text with audio narration in stigma
literature that focused on interacting with people with mental reduction. Interactive features in IVR, such as making choices
illness and dismissing negative beliefs [30]. However, the results or controlling objects in the virtual environment [52], or even
in this study were not consistent with previous IVR and studies having body or arm tracking for synchronized movements with
that simulated symptoms of people with schizophrenia. The avatars, might induce a stronger effect in stigma reduction than
simulations of hallucinations had led to increases in social text. These features of IVR should be tested in the future.
distance and negative attitudes toward people with schizophrenia
[22,29]. The different results from this study might be due to Another possible explanation of the similar performance of the
the different emphasis of immersive content. IVR and text conditions might be due to the type of graphics
used. This IVR used animated cartoons. In the text condition,
This study had purposely included little simulations of although without pictorial inputs, voice-over and detailed
symptoms in the IVR. It aimed to construct the everyday living descriptions of the story, including the virtual environment,
experience of the story protagonist as a person, instead of just characters, and actions, were included. It might help with
a combination of symptoms. Although, unlike IVR studies on imagining the story in participants’ minds. Those imaginations
racial groups or older adults, there was not a change in might perform similarly with animated cartoons in engaging
appearance according to an outgroup member in this study, the the participants. Thus, having similar effects on stigma
first-person field of view and immersion as the story protagonist reduction. With more realistic animation, IVR might allow
with mixed anxiety and depressive disorder might already have participants to resonate better and be more involved in the story
allowed participants to take on the outgroup identity and [52]. Therefore, IVR with more realistic graphics should be
perspective as a person with mental illness [24]. On the contrary, investigated in the future.
in previous literature on stigma change toward people with
schizophrenia, the simulation of a hallucination might have
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 13
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Sense of Embodiment, Story Transportation, and developed scales is needed. Second, the participants in this study
Public Stigma were mainly college students. It might pose a challenge to the
generalization of results to the general population. Therefore,
Moving on to the mediation analyses, although the condition
replication of the study on a more diverse sample is needed to
was not directly associated with story transportation, story
understand the effects of IVR on the public. Third, moderate to
transportation was found to be a preceding variable directly
long-term effects of stigma change were unknown. Although
associated with a reduction in public stigma. As mentioned
there was a 1-week follow-up in this study, the follow-up would
previously, story transportation emphasized the cognitive and
still be considered as measuring a rather short-term effect of
affective immersion in a story [34,36], which might elicit various
the interventions [5]. Longer follow-up, such as 1 month, is
cognitive and affective effects on belief change [40-43]. It might
needed to examine how stigma change may be sustained over
also reduce elaborative activities that resist stigma change
time.
[42,43] and elicit broad affective responses that allow
participants to be more conducive to reduce their public stigma Fourth, actual behavioral consequences were not measured.
[42]. Therefore, stigma change might benefit from the broad Research showed that there could be a difference between
cognitive and affective influences by story transportation. intention and actual behavior [53-55]. Future IVR studies could
consider measuring participants’ gaze orientation and
On the other hand, although the condition was associated with
interpersonal distance toward a person with mental illness in
sense of embodiment, sense of embodiment was not directly
the virtual environment [56]. This would require participants
associated with stigma change. However, with the sequential
to walk around the experiment room with full-body tracking
mediation model, sense of embodiment was significantly and
[56]. Fifth, compared to text, IVR could be quite novel to most
positively associated with story transportation, which was then
people. Interventions in this study all lasted 10 minutes.
linked to the reduction of public stigma. This showed that the
Participants might struggle to get accustomed to IVR within a
physical sensation of being inside an avatar’s body might not
short period. Future studies can give participants an embodiment
be sufficient for reducing public stigma. However, sense of
phase or a practice session to freely familiarize with and explore
embodiment might allow participants to feel as if they were the
their virtual bodies and the virtual environment [24,26]. Sixth,
story protagonist and be transported in the story. Afterward,
in the text condition, there were no pictorial or animated inputs.
participants might have different cognitive and affective
Filmed contact or videos are of greater visual similarity with
reactions from story transportation, which facilitated reduced
IVR than text. In vivo contact even allows participants to have
public stigma.
real life perception and interaction with people. They may allow
The results from mediation analyses also gave more clues as to more rigorous comparison with IVR. However, due to the lack
why IVR and text conditions performed similarly. The only of available presenters and funding, in vivo contact, filmed
difference between the two conditions was the absence of IVR’s contact, and video were not available in this study. Future
visual inputs and 3D immersive experience in the text condition. studies can consider including them as comparison groups.
However, from the mediation analyses, the intense absorption
Notwithstanding these limitations, this study was one of the
of thoughts and emotions to the story was more important and
few attempts to investigate the effects of IVR on public stigma
closely linked with reducing public stigma than merely the
by comparing it with two rigorously designed comparison
physical sensation in another body. The complexity of stigma
groups that attempted to rule out the separate effects of IVR
change called for more holistic simulation of experiences that
and text with audio narration.
allow participants to be more absorbed in the stories, lives, and
feelings of a person with mental illness. Thus, the differences Conclusion
in visual inputs or physical experience in this IVR setting might This study provided novel findings and a rigorous comparison
not be sufficient to induce stronger story transportation and in understanding the effects of IVR as a medium of public
stigma reduction than the text condition. stigma reduction. The findings showed that IVR and text with
Limitations and Future Directions audio narration both performed similarly well in reducing public
stigma. Sense of embodiment and story transportation were
Although this study investigated a novel medium, IVR and its
found to be sequentially associated with public stigma reduction.
effects on public stigma, several limitations were acknowledged.
This study gave a more nuanced understanding to the complexity
First, some scales in this study, such as the Sense of
of reducing public stigma and components in building an
Embodiment Scale, were originally developed in this study due
effective medium of stigma reduction in the future.
to the lack of available scales. Further validation of the newly
Acknowledgments
The IVR was developed for the Jockey Club TourHeart Project, which is sponsored by the Jockey Club Charities Trust.
Conflicts of Interest
None declared.
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 14
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
Multimedia Appendix 1
CONSORT-eHEALTH checklist (V 1.6.1).
[PDF File (Adobe PDF File), 393 KB-Multimedia Appendix 1]
References
1. Kosyluk KA, Al-Khouja M, Bink A, Buchholz B, Ellefson S, Fokuo K, et al. Challenging the stigma of mental illness
among college students. J Adolesc Health 2016 Sep;59(3):325-331. [doi: 10.1016/j.jadohealth.2016.05.005] [Medline:
27324577]
2. Rüsch N, Angermeyer MC, Corrigan PW. Mental illness stigma: concepts, consequences, and initiatives to reduce stigma.
Eur Psychiatry 2005 Dec;20(8):529-539. [doi: 10.1016/j.eurpsy.2005.04.004] [Medline: 16171984]
3. Goffman E. Stigma: Notes on the Management of Spoiled Identity. New York: Touchstone; 1986.
4. Chan JYN, Mak WWS, Law LSC. Combining education and video-based contact to reduce stigma of mental illness: "The
Same or Not the Same" anti-stigma program for secondary schools in Hong Kong. Soc Sci Med 2009 Apr;68(8):1521-1526.
[doi: 10.1016/j.socscimed.2009.02.016] [Medline: 19282079]
5. Thornicroft G, Mehta N, Clement S, Evans-Lacko S, Doherty M, Rose D, et al. Evidence for effective interventions to
reduce mental-health-related stigma and discrimination. Lancet 2016 Mar 12;387(10023):1123-1132. [doi:
10.1016/S0140-6736(15)00298-6] [Medline: 26410341]
6. Crisp AH, Gelder MG, Rix S, Meltzer HI, Rowlands OJ. Stigmatisation of people with mental illnesses. Br J Psychiatry
2000 Jul;177:4-7. [doi: 10.1192/bjp.177.1.4] [Medline: 10945080]
7. Corrigan PW, Green A, Lundin R, Kubiak MA, Penn DL. Familiarity with and social distance from people who have serious
mental illness. Psychiatr Serv 2001 Jul;52(7):953-958. [doi: 10.1176/appi.ps.52.7.953] [Medline: 11433114]
8. Link BG, Phelan JC, Bresnahan M, Stueve A, Pescosolido BA. Public conceptions of mental illness: labels, causes,
dangerousness, and social distance. Am J Public Health 1999 Sep;89(9):1328-1333. [doi: 10.2105/ajph.89.9.1328] [Medline:
10474548]
9. Pinfold V, Toulmin H, Thornicroft G, Huxley P, Farmer P, Graham T. Reducing psychiatric stigma and discrimination:
evaluation of educational interventions in UK secondary schools. Br J Psychiatry 2003 Apr;182:342-346. [doi:
10.1192/bjp.182.4.342] [Medline: 12668411]
10. Seeman N, Tang S, Brown AD, Ing A. World survey of mental illness stigma. J Affect Disord 2016 Jan 15;190:115-121.
[doi: 10.1016/j.jad.2015.10.011] [Medline: 26496017]
11. Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol 2001 Aug;27(1):363-385. [doi: 10.1146/annurev.soc.27.1.363]
12. Wahl OF. Stigma as a barrier to recovery from mental illness. Trends Cogn Sci 2012 Jan;16(1):9-10. [doi:
10.1016/j.tics.2011.11.002] [Medline: 22153582]
13. Corrigan PW, Watson AC. Understanding the impact of stigma on people with mental illness. World Psychiatry 2002
Feb;1(1):16-20 [FREE Full text] [Medline: 16946807]
14. Wahl OF. Mental health consumers' experience of stigma. Schizophr Bull 1999;25(3):467-478. [doi:
10.1093/oxfordjournals.schbul.a033394] [Medline: 10478782]
15. Livingston JD, Boyd JE. Correlates and consequences of internalized stigma for people living with mental illness: a
systematic review and meta-analysis. Soc Sci Med 2010 Dec;71(12):2150-2161. [doi: 10.1016/j.socscimed.2010.09.030]
[Medline: 21051128]
16. Mak WWS, Cheung RYM. Self-stigma among concealable minorities in Hong Kong: conceptualization and unified
measurement. Am J Orthopsychiatry 2010 Apr;80(2):267-281. [doi: 10.1111/j.1939-0025.2010.01030.x] [Medline: 20553520]
17. Corrigan PW, Larson JE, Rüsch N. Self-stigma and the "why try" effect: impact on life goals and evidence-based practices.
World Psychiatry 2009 Jun;8(2):75-81 [FREE Full text] [doi: 10.1002/j.2051-5545.2009.tb00218.x] [Medline: 19516923]
18. Pinfold V, Thornicroft G, Huxley P, Farmer P. Active ingredients in anti-stigma programmes in mental health. Int Rev
Psychiatry 2005 Apr;17(2):123-131. [doi: 10.1080/09540260500073638] [Medline: 16194782]
19. Corrigan PW, Morris SB, Michaels PJ, Rafacz JD, Rüsch N. Challenging the public stigma of mental illness: a meta-analysis
of outcome studies. Psychiatr Serv 2012 Oct;63(10):963-973. [doi: 10.1176/appi.ps.201100529] [Medline: 23032675]
20. Clement S, van Nieuwenhuizen A, Kassam A, Flach C, Lazarus A, de Castro M, et al. Filmed v. live social contact
interventions to reduce stigma: randomised controlled trial. Br J Psychiatry 2012 Jul;201(1):57-64. [doi:
10.1192/bjp.bp.111.093120] [Medline: 22157800]
21. Corrigan PW, Larson J, Sells M, Niessen N, Watson AC. Will filmed presentations of education and contact diminish
mental illness stigma? Community Ment Health J 2007 Apr;43(2):171-181. [doi: 10.1007/s10597-006-9061-8] [Medline:
16988883]
22. Kalyanaraman SS, Penn DL, Ivory JD, Judge A. The virtual doppelganger: effects of a virtual reality simulator on perceptions
of schizophrenia. J Nerv Ment Dis 2010 Jun;198(6):437-443. [doi: 10.1097/NMD.0b013e3181e07d66] [Medline: 20531123]
23. Kilteni K, Groten R, Slater M. The sense of embodiment in virtual reality. Presence Teleoperators Virtual Environments
2012 Nov;21(4):373-387. [doi: 10.1162/pres_a_00124]
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 15
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
24. Peck TC, Seinfeld S, Aglioti SM, Slater M. Putting yourself in the skin of a black avatar reduces implicit racial bias.
Conscious Cogn 2013 Sep;22(3):779-787. [doi: 10.1016/j.concog.2013.04.016] [Medline: 23727712]
25. Petkova VI, Khoshnevis M, Ehrsson HH. The perspective matters! Multisensory integration in ego-centric reference frames
determines full-body ownership. Front Psychol 2011;2:35. [doi: 10.3389/fpsyg.2011.00035] [Medline: 21687436]
26. Yee N, Bailenson JN. Walk a mile in digital shoes: the impact of embodied perspective-taking on the reduction of negative
stereotyping in immersive virtual environments. 2006 Presented at: Presence 2006: The 9th Annual International Workshop
on Presence; August 24-26, 2006; Cleveland, OH.
27. Ando S, Clement S, Barley EA, Thornicroft G. The simulation of hallucinations to reduce the stigma of schizophrenia: a
systematic review. Schizophr Res 2011 Dec;133(1-3):8-16. [doi: 10.1016/j.schres.2011.09.011] [Medline: 22005017]
28. Brown SA. Implementing a brief hallucination simulation as a mental illness stigma reduction strategy. Community Ment
Health J 2010 Oct;46(5):500-504. [doi: 10.1007/s10597-009-9229-0] [Medline: 19669675]
29. Brown SA, Evans Y, Espenschade K, O'Connor M. An examination of two brief stigma reduction strategies: filmed personal
contact and hallucination simulations. Community Ment Health J 2010 Oct;46(5):494-499. [doi: 10.1007/s10597-010-9309-1]
[Medline: 20414723]
30. Cangas AJ, Navarro N, Parra JMA, Ojeda JJ, Cangas D, Piedra JA, et al. Stigma-Stop: a serious game against the stigma
toward mental health in educational settings. Front Psychol 2017;8:1385. [doi: 10.3389/fpsyg.2017.01385] [Medline:
28878702]
31. Fisher S, Cleveland SE. Body Image and Personality. 2nd edition. Michigan: Dover Publications; 1968.
32. Biocca F. The cyborg's dilemma: progressive embodiment in virtual environments. J Computer-Mediated Commun 1997
Sep 01;3(2):1. [doi: 10.1111/j.1083-6101.1997.tb00070.x]
33. Maister L, Slater M, Sanchez-Vives MV, Tsakiris M. Changing bodies changes minds: owning another body affects social
cognition. Trends Cogn Sci 2015 Jan;19(1):6-12. [doi: 10.1016/j.tics.2014.11.001] [Medline: 25524273]
34. Green MC, Kass S, Carrey J, Herzig B, Feeney R, Sabini J. Transportation across media: repeated exposure to print and
film. Media Psychol 2008 Dec 23;11(4):512-539. [doi: 10.1080/15213260802492000]
35. Tal-Or N, Cohen J. Understanding audience involvement: conceptualizing and manipulating identification and transportation.
Poetics 2010 Aug;38(4):402-418. [doi: 10.1016/j.poetic.2010.05.004]
36. Green MC, Brock TC. The role of transportation in the persuasiveness of public narratives. J Pers Soc Psychol 2000
Nov;79(5):701-721. [doi: 10.1037//0022-3514.79.5.701] [Medline: 11079236]
37. Caputo NM, Rouner D. Narrative processing of entertainment media and mental illness stigma. Health Commun 2011
Oct;26(7):595-604. [doi: 10.1080/10410236.2011.560787] [Medline: 21516556]
38. Mann CE, Himelein MJ. Putting the person back into psychopathology: an intervention to reduce mental illness stigma in
the classroom. Soc Psychiatry Psychiatr Epidemiol 2008 Jul;43(7):545-551. [doi: 10.1007/s00127-008-0324-2] [Medline:
18286216]
39. Oliver MB, Dillard JP, Bae K, Tamul DJ. The effect of narrative news format on empathy for stigmatized groups. Journalism
Mass Commun Q 2012 Mar 14;89(2):205-224. [doi: 10.1177/1077699012439020]
40. Winterbottom A, Bekker HL, Conner M, Mooney A. Does narrative information bias individual's decision making? A
systematic review. Soc Sci Med 2008 Dec;67(12):2079-2088. [doi: 10.1016/j.socscimed.2008.09.037] [Medline: 18951673]
41. Kaufman GF, Libby LK. Changing beliefs and behavior through experience-taking. J Pers Soc Psychol 2012 Jul;103(1):1-19.
[doi: 10.1037/a0027525] [Medline: 22448888]
42. Appel M, Richter T. Transportation and need for affect in narrative persuasion: a mediated moderation model. Media
Psychol 2010 May 28;13(2):101-135. [doi: 10.1080/15213261003799847]
43. Green MC, Brock TC, Kaufman GF. Understanding media enjoyment: the role of transportation into narrative worlds.
Commun Theory 2004 Nov;14(4):311-327. [doi: 10.1111/j.1468-2885.2004.tb00317.x]
44. Schutte NS, Stilinović EJ. Facilitating empathy through virtual reality. Motivation Emotion 2017 Oct 16;41(6):708-712.
[doi: 10.1007/s11031-017-9641-7]
45. Mak WWS, Chong ESK, Wong CCY. Beyond attributions: understanding public stigma of mental illness with the common
sense model. Am J Orthopsychiatry 2014 Mar;84(2):173-181. [doi: 10.1037/h0099373] [Medline: 24826933]
46. Ehrsson HH. The experimental induction of out-of-body experiences. Science 2007 Aug 24;317(5841):1048 [FREE Full
text] [doi: 10.1126/science.1142175] [Medline: 17717177]
47. Slater M, Spanlang B, Sanchez-Vives MV, Blanke O. First person experience of body transfer in virtual reality. PLoS One
2010 May 12;5(5):e10564 [FREE Full text] [doi: 10.1371/journal.pone.0010564] [Medline: 20485681]
48. Longo MR, Schüür F, Kammers MPM, Tsakiris M, Haggard P. What is embodiment? A psychometric approach. Cognition
2008 Jun;107(3):978-998. [doi: 10.1016/j.cognition.2007.12.004] [Medline: 18262508]
49. Hayes A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New
York: The Guilford Press; 2013.
50. Lysaker PH, Davis LW, Warman DM, Strasburger A, Beattie N. Stigma, social function and symptoms in schizophrenia
and schizoaffective disorder: associations across 6 months. Psychiatry Res 2007 Jan 15;149(1-3):89-95. [doi:
10.1016/j.psychres.2006.03.007] [Medline: 17156853]
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 16
(page number not for citation purposes)
XSL• FO
RenderXJOURNAL OF MEDICAL INTERNET RESEARCH Yuen & Mak
51. Sarge MA, Kim H, Velez JA. An intervention: the role of perspective taking in combating public stigma with virtual
simulations. Cyberpsychol Behav Soc Netw 2020 Jan;23(1):41-51. [doi: 10.1089/cyber.2019.0678] [Medline: 31976769]
52. Rohrer MW. Seeing is believing: the importance of visualization in manufacturing simulation. 2000 Presented at: The 32nd
Conference on Winter Simulation; December 2000; Orlando, FL. [doi: 10.1109/wsc.2000.899087]
53. Corrigan PW, Bink AB, Fokuo JK, Schmidt A. The public stigma of mental illness means a difference between you and
me. Psychiatry Res 2015 Mar 30;226(1):186-191. [doi: 10.1016/j.psychres.2014.12.047] [Medline: 25660735]
54. Reinke RR, Corrigan PW, Leonhard C, Lundin RK, Kubiak MA. Examining two aspects of contact on the stigma of mental
illness. J Soc Clin Psychol 2004 Jun;23(3):377-389. [doi: 10.1521/jscp.23.3.377.35457]
55. Thornicroft G, Rose D, Kassam A, Sartorius N. Stigma: ignorance, prejudice or discrimination? Br J Psychiatry 2007
Mar;190:192-193. [doi: 10.1192/bjp.bp.106.025791] [Medline: 17329736]
56. Gillath O, McCall C, Shaver PR, Blascovich J. What can virtual reality teach us about prosocial tendencies in real and
virtual environments? Media Psychol 2008 Jun 25;11(2):259-282. [doi: 10.1080/15213260801906489]
Abbreviations
ANOVA: analysis of variance
IVR: immersive virtual reality
Edited by R Kukafka; submitted 26.08.20; peer-reviewed by C Stunden, A Algarin, S van Beugen; comments to author 06.10.20;
revised version received 29.12.20; accepted 24.05.21; published 14.07.21
Please cite as:
Yuen ASY, Mak WWS
The Effects of Immersive Virtual Reality in Reducing Public Stigma of Mental Illness in the University Population of Hong Kong:
Randomized Controlled Trial
J Med Internet Res 2021;23(7):e23683
URL: https://www.jmir.org/2021/7/e23683
doi: 10.2196/23683
PMID: 34259636
©Anna S Y Yuen, Winnie W S Mak. Originally published in the Journal of Medical Internet Research (https://www.jmir.org),
14.07.2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium,
provided the original work, first published in the Journal of Medical Internet Research, is properly cited. The complete bibliographic
information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must
be included.
https://www.jmir.org/2021/7/e23683 J Med Internet Res 2021 | vol. 23 | iss. 7 | e23683 | p. 17
(page number not for citation purposes)
XSL• FO
RenderXYou can also read