The analgesic tramadol has minimal effect on gastrointestinal motor function
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
B r j Clin Phormocol 1997; 43: 7 1-75
The analgesic tramadol has minimal effect on gastrointestinal motor
function
Clive H.Wilder4mith & Andrea Bettiga
Gastruintestiml Utiit and Nociceptiue Research Grurrp, Beau-Site Hospital, Berne, Suitzerland
Aims The analgesic tramadol, an opioid agonist and monoaminergic reuptake
blocker, has been assumed to interfere less with gastrointestinal motor function than
other opioid analgesics, but this has not been specifically investigated. In this study
we examined the effect of tramadol on variables of gastrointestinal motor fimction.
Methods Ten healthy volunteers participated in a two-arm, placebo-controlled,
double-blind, randomized, cross-over study comparing tramadol 50 mg and placebo
solutions given four times a day for 10 days. Oro-caecal (lactulose H,-breath test)
and colonic (solid markers) transit times and anal sphincter pressures were measured
after 10 days dosing.
Results Mehan oro-caecal transit time was 90 min (interquartile range: 75-105)
with placebo and 90 min (60-105) with tramadol (not signlficant). The mehan total
colonic transit time increased from 45.6 h (25.2-64.8) with placebo to 58.8 h
(50.4-78.0) with tramadol (not significant), which is still withm the normal range
( < 60 h). Anal sphincter resting pressures were not significantly changed by tramadol
compared with placebo.
Concfrrsions Tramadol has a minor delaying effect on colonic transit, but no effect
on upper gastrointestinal transit or gut smooth muscle tone. Tramadol may be a
useful analgesic where interference with gut motor function is undesirable.
Keywords: gastrointestinal transit, tramadol, opioids, smooth muscle tone, constipation
A low incidence of constipation during treatment with
Introduction
tramadol has been postulated and observed, but not invest-
Opioids are commonly used analgesics in both the acute igated systematically [lo-141. In a previous 4-day cross-over
and chronic setting. These drugs, especially y-opioid trial in cancer patients hospitalised for treatment of severe
agonists, have undesirable effects on gastrointestinal pain, less constipation, nausea and emesis developed with
function, resulting in nausea, emesis, crampy abdominal oral tramadol compared with morphine (10). Tramadol also
pain and constipation [ l , 21. Unwanted drug effects may hffers from typical opioids in having a very low addiction
lead to postoperative problems, such as prolonged ileus or potential, little respiratory depression and a minor effect on
aspiration. When given chronically, initial nausea and the sphincter of Oddi [15-201. To examine specifically the
vomiting or persistent constipation can cause the physician effects of tramadol on gastrointestinal motor function, we
or patient to discontinue an otherwise effective therapy. designed a placebo-controlled, cross-over trial with differen-
To prevent these side-effects of y-opioids, antiemetics and tiated measures of gut transit and anal sphincter pressures.
laxatives are often prescribed preemptively [3]. The The dose of tramadol chosen is an average dose used for
analgesic tramadol has recently become available in the chronic pain treatment.
United States, Great Britain and other countries. Its Thls work was presented as an abstract at the South
analgesic potency compared with morphine is approxi- African Gastroenterology Symposium (SAGES) 1995 in
mately one quarter when given orally and a sixth to a Sun City, RSA and at the American Gastroenterological
tenth parenterally. After initial classification as a weak, Association (AGA) in San Francisco, 1996.
predominantly y-opioid agonist, a second complementary
analgesic mechanism of approximately equal importance
has become evident [4-91. This second mode of action of Methods
tramadol is effected via blockade of noradrenaline and
serotonin reuptake, with some differences in selectivity Ten healthy male volunteers between 22 and 28 years of
age were recruited for this study. None of them had a
between the two stereoisomers of tramadol [4-91. The
principal metabolite of tramadol (Ml) also has analgesic history of upper or lower gastrointestinal symptoms ( > 1
effect, with a greater affinity to the y-receptor than the episode/week) or intestinal surgery. Volunteers with less
parent compound. than two defaecations per week or more than three per day
or strong straining during evacuation, any ongoing medi-
Correspondence: D r med. Clive H. Wilder-Smith, Gastrointestinal Unit and Nociceptive
cation, metabolic disorders (especially thyroid dysfunction,
Research Group, Bubenbergplau I I. CH-30 I I Berne, Switzerland diabetes mellitus), alcohol or drug abuse, renal insufficiency
0 1997 Blackwell Science Ltd 71C.H. Wilder-Smith & A. Bettiga
or chronic pain were excluded from the study. Use of the day after 10 days of dosing a supine abdominal X-ray
antibiotics in the previous 30 days was an additional was taken between 9.30 and 10.30 h. This is a standardized
exclusion criterion. All volunteers gave written infomied procedure to measure colonic transit, by counting the
consent and University of Berne Ethics Committee approval number of particles seen on a plain abdominal X-ray after
was gained for the study. The two-arni cross-over study was 6 days of marker ingestion [24, 251. Colonic transit times
single-centre, double-blind and randomized. Before the were not performed in the pre-trial control arm to ininimise
study began, a n additional control arm was performed the radiation exposure of the volunteers.
without any medication to familiarise subjects with the test A retrospective evaluation of bowel function including
procedures. There was a washout period of at least 1 week defaecatory frequency, stool consistency and defaecatory
between the subsequent t\vo study amis. Volunteers \vere straining was elicited using standardised questionnaires.
randomized to receive either traniadol 50 mg or placebo Throughout the study volunteers were asked not to change
(0.9% saline) solution for 1 0 successive days at 8.30, 13.00, their normal dietary habits and not to participate in parties
18.00 and 23.00 h. The solutions were adapted for taste and or drink more than two glasses of wine or beer. Docu-
colour and were dispensed from a coded bottle using a mentation of study data was on special data sheets.
calibrated pipette. Volunteers took the study drug at home,
but telephoned the study monitor at each time of dosing to
corifirni compliance and report side-effects. Volunteers L4i~alysis
attended the research ward for nieasurenients on three
occasions: for the preliniinq control arni without niedi- Data are reported as medians and interquartile ranges
cation and on the day after 10 days of dosing with placebo throughout. Anal resting pressures are reported in mmHg.
and traniadol. The time schedule on each study day was The colonic transit times are analysed according to the
standardized. All measurements were staggered at 3 min reference literature [24, 251. In brief, the numbers of markers
intervals benveen volunteers, to maintain constant timing in the total colon as well as in each colonic segment (defined
for each individual. In the following the time of measurement as in reference [24]: right colon: markers to the right of the
for the first volunteer is ahl-ays stated. vertebral spinous processes and above a line from L5 to the
Volunteers arrived at the research ward at 8.00 h. They pelvic outlet; left colon: markers to the left of the vertebral
had fasted and had not smoked. drunk sweet drinks, eaten spinous processes and above a line from L5 to the anterior
sweets or chewed chewing gum since midnight. At 8.30 h superior iliac crest; rectosignioid or pelvic colon: markers
the m a / rrstirg prcwirc was determined with a standardized inferior to a line from the pelvic brini on the right and the
rnanonietric apparatus. This consists of a water-filled anterior superior iliac crest on the left) are counted and
embolectoniy balloon catheter (diameter 4 nim) linked niultipled by 2.4 to give the transit time in hours. This
to a presture transducer, which is connected to a six-channel
analysis is based on 10 particles swallowed at a standardized
solid-state datalogger (Gastroscanf 6020, Mehcal Instru- time per 24 h period, hence the multiplication by the factor
ments Corp., Solothurn, Switzerland). Calibration at 0 and 2.4. Oro-caecal transit times by breath test are shown as the
350 inn1 Hg \vLii performed before the investigation. The time taken for the hydrogen content of the expired air to
catheter was inserted 5 cni rectally and a slow-pullthrough reach a threshold of 20 ppm. Confirmative comparisons
performed with the subject in the left lateral position to between the study arms of the total colonic and oro-caecal
localise the point of maximum resting pressure in the anal transit times and the maximum anal resting pressure were
canal. This was confimied in a second station- performed with the Wilcoxon signed-rank test. All other
ary nieasurenient at the previously noted position of analyses are exploratory. A significance level of PJramadol and g.i. function
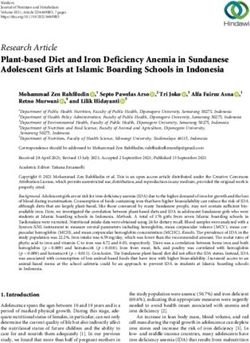
'100
*OF
Placebo Tram ado I
T
Figure 1. Total and segmental (right,
left and pelvic) colonic transit times
in nine healthy volunteers after 10
days dosing with tramadol solution
50 mg or placebo four times daily.
The box-whisker plots show the
median (line), interquartile range
(box) and total range (whiskers). The
upper range of normal in men is
delineated at 60 h.
Coloriic trarisit times Discussion
Total and segmental transit times are shown in Figure. 1. This 10-day, double-blind, randomized, cross-over study in
The median total colonic transit time was 58.8 h (IQR: healthy volunteers investigated the effect of oral tramadol in
50.4-78.0) with tramadol and 45.6 h (25.2-64.8) with clinically used doses on intestinal motor function. Compared
placebo (P=0.053) and there was also a trend to longer with placebo, tramadol did not significantly interfere with
transit times in the pelvic colon segment (18 h (10.8-27.6) oro-caecal or colonic transport and did not raise the anal
DS 9.6 h (2.4-16.8) respectively, P=0.07). sphincter resting pressure.
The colonic transit time did increase slightly after 10 days
dosing with tramadol, however the median transit times
Oro-caecal transit times
were still within the normal range of 60 h [25]. The sample
The median (IQR) oro-caecal transit times were 90 min size chosen was adequate to detect clinically relevant changes
(75-105) with placebo and 90 min (60-105) with tramadol of 10% in the colonic transit times, but it is possible that
(not significant). the increase in colonic transit times would become significant
with a larger sample size. The absence of a delaying effect
on upper g.i. transit implies that the nausea and vomiting
Side-effects associated with tramadol is likely to be a central effect
The individual number of side-effects was increased from 0 mediated via the vomiting centre, rather than gross
(0-1) with placebo to 2.0 (0-3) with tramadol (P=O.05). dysmotility [13, 261. This is in contrast to morphine, which
All side-effects occurred in the first 2 days of dosing and has several antipropulsive effects in the upper and lower g.i.
subsequently faded. The side-effects are listed in Table 1. tract. In the present study comparison of tramadol with a
standard opioid agent, such as morphine, given for several
days was considered unethical, because of the established
Retrospective evaltiatiori
risk of dependence. It is clear, however, from animal and
Defaecatory frequency, stool consistency and defaecatory human studies that morphine increases pyloric and ileocaecal
straining by the volunteers indicated the following changes sphincter pressures, and induces increased simultaneous,
during tramadol compared with placebo dosing: decreased colonic high pressure contractions and decreased right
defaecation frequency in seven subjects, more compact stool colonic tone, resulting in prolonged gastrointestinal transit
consistency in three, and five had increased straining, three [l, 2, 27-31]. Prolonged oro-caecal transit times following
had less straining. morphine have been shown by hydrogen breath test in
healthy volunteers [32]. During epidural anaesthesia with
Table 1 Numbers of healthy volunteers with side-effects during morphine gastric emptying and ororcaecal transit were
10 days dosing with placebo and tramadol. delayed and the number of duodenal contractions was
increased compared with epidural bupivacaine [33]. Post-
Tramadd Placebo operative analgesia with intramuscular morphine significantly
slowed gastric emptying and delayed resolution of postopera-
Nausea/Emesis 6*/4 1/1 tive ileus by impairing colonic motility compared with
Dizziness 5* 0
ketorolac in two separate studies [34, 351. These recent
Drowsiness 3 1
studies collectively demonstrate the interfering effect of
Bloating 0 1
morphine on gastric, small intestinal and colonic motor
Epigastric cramps 0 1
Sweating 1 0
function. Several of the studies employed the same transit
measurement techniques used in the current study, thus
*PC.H. Wilder-Smith & A. Betriga
Tramadol does not increase smooth muscle sphincter ‘atypical’opioid analgesic. J P l ~ ~ ~ r t t ~Exp
a i o I Ther 1992; 260:
pressures, as demonstrated with anal sphincter pressures i n 275-285.
the present study and sphincter of O d d i measurements i n 3 Sevcik J, Nieber K, Driessen B, Illes B. Effects of the central
previous investigations [I‘), 201. T h e anal resting pressure is analgesic tramadol and its niain metabolite, 0-desmethyl
largely representative of smooth. involuntary muscle tone. tramadol. on rat locus coeruleus neurones. B r J Phnrrriad
1993; 110: 169-176.
T h e retrospective statements niade by the subjects indicated
6 Hennies HH, Friedrichs E, Schneider J. Receptor binding,
a tendancy t o reduced defaecatory frequency and more
analgesic and antitussive potency of traniadol and other
conipact stools with tramadol, but all subjects had bowel
selected opioids. Arztzeimitte~~rsrhung 1988; 38: 877-880.
motions at least every third day. Retrospective evaluation
7 Kayser V, Besson JM, Guilbaud G. Evidence for a
of bowel habits is notoriously unreliable, but this supports noradrenergc component in the antiiiociceptive eKect of the
the minor changes in colonic transit 1361. analgesic agent tramadol in the animal model of clinical pain,
T h e nature of the interference of tramadol with colonic the arthritic rat. Errrj Pharniacol 1992; 224: 83-88.
motility was not investigated, but may involve a direct 8 Driessen B, Reiniann W. Interaction of the central analgesic,
influence on the niyentenc plexus or central modulation via tramadol, with the uptake and release of 5-HT in the rat
opioid and riinnoaniinergic mechanisms. 2,-adrenoceptor brain in vitro. B r ] Pliannarol 1992; 105: 147-151.
agonists, such as clonidine, have similar spinal actions t o the 9 Friedrichs E, Reiinann W, Selve N. Contribution of both
non-opioid component of tramadol, modulating monoami- enantiomers to antinociception of the centrally acting
nergic inechanistiis [37J. They have potent analgesic effects analgesic tramadol. Ivarrriyn-Sdit~tiedeb~rg’s Arch of Pharmacol
-
and can induce constipation. I,-adrenoceptor agonists, 5-HT 1992; 346 (SUPPI 1): R36.
receptor subtype\ I , Z and 3 as w d as morphine spinally 10 Wilder-Smith CH, Schlmke J, Ostenvalder B, Senii HJ. Oral
tramadol, a p-opioid agonist and tnonoamine reuptake-
mediate antinociception in responce t o colorectal distension
blocker, and morphine for strong cancer-related pain. Anfi
in conscious rats [38-40]. T h e variables used in this study
Clitl 0 t 1 d 1994; 5: 111-116.
are well-validated in the clinical setting and the limitations
11 Raffa RB, Friedrichs E, Reirnann W, Shank RP, Codd Eem
of the transit methods as estimates of motility should be Vaught JL, Jacob HL. Belvtt N. Complementary and
recognised. T h e lactulow breath test determines the time of synergstic antinociceptive interaction between the
amval of the head of the lactulose bolus i n the caecum, enantiomen of tramadol. J PIiarttiad Exp 77ier 1993; 267:
rather than the main mass [41, 421. With the prestudy meal 331 -340.
used and the volunteer preparation the intraindividual 12 Twycross RG. Opioids. In Textbook of’Pairt. 3rd edition, eds
variability of the method is relatively low [13,441. O u r Wall PD, Melzack R. New York: Churchill Livingstone;
transit values were within the established normal range [23, 1994: 956.
43, 451. T h e c o l d marker colonic transit estimation is based 13 Budd K. Chronic pain-challenge and response. Drugs 1994;
on the conirno~ilyused method developed by Metcalf et d., SUPPI PI 1): 33-38.
\yhich is influenced by upper g.i. transit [24]. This method 14 Rauck RL. Ruoff GE, McMillan JI. Comparison of tramadol
has been validated against radioisotope labelled meal transit and acetaminophen with codeine for long-term pain
and median intraindividual variabilty was 17% [45, 461. management in elderly patients, Ccrrr n e r Res 1994; 55:
1417-1 43 1.
I n conclusion. this study demonstrates a minor interference
15 Preston KL.. Jasinslu D R , Testa M. Abuse potential and
of trainadol \vith gastrointestinal motor function compared
phamiacological coniparison of tramadol and morphine. Drug
with placebo. This is compatible with the clinical obser-
Alcohol Deyettd 1991; 27: 7-17.
vationt of ‘I lesser constipatory effect of tramadol compared
16 Vicken MD, O’Flaherty D, Szekely SM, Kead M, Yoshizumi
with other opioids. A comparative study of adequate J. Tramadol: pain relief by an opioid without depression of
duration with potent opioids would be unethical in healthy respiration. rlriaesthcsia 1992; 47: 29 1-296.
subjects, but ha\ just been completed in patients with 17 Hounies R-JM, Voets MA. Verkaaik A, Erdmann W,
pain 1471. Lachniann B. Eficacy and safety of tramadol versus morphine
for moderate and severe postoperative pain with special regard
to respiratory depression. Arresdz Atralg 1992; 74: 510-514.
This midy \vas supported by a research grant from
18 Paravicini D, Zander J, Hansen J. Effects of tramadol on
Protochenue AG. Switzerland
haemodynamics and blood gases in the early postoperative
period. Atiiishesist 1982; 31: 61 1-614.
19 Staritz M, Poralla T, Manns M, Meyer zum Buschenfelde
References KH. Effect of modem analgesic drugs (tramadol, pentazocine
1 Jaffe JH. Martin WR. Opioid analgesics and antagonists. In and buprenorphine) on the bile duct sphincter in man. Girt
Tlrc p,lroritiacolqsii‘~/basis q / tlierapeirfiij,7th edition, ed Gilinan 1986; 27: 567-569.
AG, Goodniai LS. Kall T W . Murid F. Basingstoke: 20 Coelho JCU, Runkel N, Herfarth C , Senninger N, Messmer
M~~cniillari tW2. K. E f k t of analgesic drugs o n the electromyographic activity
2 Burkr TF, Hirntns LD, Gdigan JJ. Davis TP. Motility efi-ects of the gastrointestinal tract and sphincter of Oddi and on
of opioid peptides i n dog tntestlne. Ltti Sit 1982; 31: blliary pressure. Atrrr Surg 1986; 204: 53-58.
22.3-2?4( I. 71 Thompson DG, Binfield P, DeBelder A, O’Brien J, Warren
.? T\xTcross R G . Lack SA. Syfqmwi c o r m 1 i t i $ir a d i m i c d iaitccr: S. Extra intestinal influences o n exhaled breath hydrogen
, I W I ~ I rtdit;t: London: Pttman Publishing Ltd; 1984. measurements dunng the investigation of gastrointstinal
4 Ratf:~RB. Fncdrichs E. Reimann W, Shank RP, Codd EE, disease. Girt 1985; 26: 1349-1352.
Vaught JL. Optoid and non-opioid components independently 72 La Brooy SJ, Male PJ, Beavis AK, Misiewicz JJ. Assessment of
contnhute to the mrchammi of action of tramadol, an the reproducibility of the lactulose H,-breath test as a
74 0 1997 Blackwell Science Lrd B r J Clin Phormocol, 43, 71-75Tromodol and g.i. function
measure of mouthy to caecum transit time. Girt 1983; 24: 36 Ashraf W, Park F, Lof J. Quigley EM. An examination of the
893-896. reliability of reported stool frequency in the diagnosis of
23 Read NW, Miles CA, Fisher D, er al. Transit of a meal idiopathic constipation. Am J Gasrroeiitercil 1996; 91: 26-32.
through the stomach, small intestine and the colon in normal 37 Yaksh TL. Pharmacology of spinal adrenergc systenis which
subjects and its role in the pathogenesis of harrhea. modulate spinal nociceptive processing. Pharriiarol Biochern
Gasfroetiterology 1980; 79: 1276-1 282. Behav 1985; 22: 845-858.
24 Metcalf AM, Phdlips SM, Zinsmeister AR, MacCarty RL, 38 Danzebrink RM, Gebhart GF. Antinociceptive effects of
Beart R W , Wolff BG. Simplified assessment of segmental intrathecal adrenorecteptor agonists in a rat model of visceral
colonic transit. Gasfroenterology 1987; 92: 40-47. nociception. J Pharmacol Exp T h e r 1990; 253: 698-705.
25 Meier R, Beglinger C, Dederding JP, et al. Alters- und 39 Danzebrink RM, Gebhart GF. Evidence that spinal 5HT1,
geschlechtsspezifische Normwerte der Dickdanntransitzeit bei 5HT2 and 5HT3 receptor subtypes modulate responses to
Gesunden. Schweiz Med Wschr 1992; 122: 940-943. noxious colorectal distension in the rat. Brairi Rex 1991; 538:
26 Sunshine A. New clinical experience with tramadol. Drugs 64-75.
1994; ~ ~ ( S U P1):
P ~8-18. 40 Maves TJ, Gebhart G. Antinociceptive synergy between
27 Stewart JJ, Weisbrodt NW, Burks TF. Central and peripheral intrathecal morphine and lidocaine during visceral and somatic
actions of morphine on intestinal transit. J Phannacol E x p Ther nociception in the rat. Anesthesiology 1992; 76: 91-99.
1978; 205: 547-555. 41 Bond JH, Levitt MD. Investigation of small bowel transit rime
28 Ogdvy AJ, Smith G. The gastrointestinal tract after in man utilising pulmonary hydrogen measurements. J La6
Chi Med 1975; 85: 546-552.
anaesthesia. EurJ Atiaestheriol 1995; lO(supp1): 35-42.
29 Schiller LR. Review article: anti-diarrhoeal pharmacology and 42 Spiller R C . Chemical detection of transit. In Illirstrated guide to
gastroiritestinal motility. 2nd edition, eds Kumar D, Wingate D.
therapeutics. Aliment Phamiacol Ther 1995; 9: 87-106.
Edinburgh: Churchill Livingstone; 1993: 308-3 18.
30 Coupar IM. The peristaltic reflex in the rat ileum: evidence
43 Welsh JD, Payne DL, Manion C , Morrison R D . Nichols
for functional mu and delta opiate receptors. J Pharm
MA. Interval sampling of breath hydrogen as an index of
Phamiacol 1995; 47: 643-646.
lactose malabsoprtion in lactase deficient subjects. D(q Dis Sci
31 Culpepper-Morgan JA, Holt P R , LaRoche D , Kreek
1981; 26: 681-687.
MJ. Orally administered opioid antagonists reverse both mu
44 Scarpello J. Hydrogen breath testing for lactose malabsorption.
and kappa opioid delay of gastrointestinal transit in the guinea
Gift 1976; 17: 245-251.
pig. Lfe Sci 1995; 56: 1187-1192.
45 Caride VJ, Prokop EK, Troncale FJ, Buddoura W.
32 Yuan CS, Foss JF, O’Connor M, Toledano A, Roizen MF, Winchenbach K, McCalluni RW. Scintigraphic
Moss J. Methylnaltrexone prevents morphine-induced delay in detenriination of small intestinal transit time: a comparison
oral-cecal transit time without affecting analgesia: a double- with the hydrogen breath test. Gastroenterology 1984; 86:
blind randomized placebo-controlled trial. Clin Pharmaol Ther 714-720.
1996; 59: 469-475. 46 Van der S i p JRM, Kamm MA, Nightingale JMD, et a / .
33 Thorn SE, Wattwil M, Kallander A. Effects of epidural Radioisotope determination of regonal colonic transit in
morphine and epidural bupivacaine on gastroduodenal severe constipation: comparison with raho opaque markers.
monlity during the fasted state and after food intake. Acta Glif 1993; 34: 402-408.
Aiiaestheriol Scand 1994; 38: 57-62. 47 Wilder-Smith CH, Cariem AK, Osler W, Radebold K,
34 Petring OU, Dawson PJ, Blake DW, et al. Normal Bomman P, O’Keefe SJD. The effects of tramadol and
postoperative gastric emptying after orthopaedic surgery with morphine on gastrointestinal transit and smooth muscle tone.
spinal anaesthesia and i.m. ketorolac as the first postoperative Part 2: chronic pancreatitis patitients with severe pain-an
analgesic. B r J Atiaesth 1995; 74: 257-260. interim analysis. Gustroetiterology 1996; 110: A780.
35 Ferraz AA, Cowles VE, Condon RE, et al. Nonopioid
analgesics shorten the duration of postoperative ileus. A m Suvg (Received 29 April 1996,
1995; 61: 1079-1083. accepted 17 Septettiber 1996)
0 1997 Blackwell Science Ltd BrJ Clin Pharmacol. 43, 71-75 75You can also read