Surrey and Sussex Healthcare NHS Trust East Surrey Hospital Regional weekly PA Teaching Program Rheumatoid Arthritis(RA) - MBBS MRCSEd Lead T&O SHO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Surrey and Sussex Healthcare NHS Trust
East Surrey Hospital
Regional weekly PA Teaching Program
Rheumatoid Arthritis(RA)
Presented by :
Dr.Eltayeb Shammeseldin
MBBS MRCSEd
Lead T&O SHO
10.3.2021
Introduction Commonest Chronic inflammatory joint disease 1-3%prevelance 40s-50s of age F:M 3-4:1 Commoner in Caucasian in N. America and Europe, but it is everywhere
Etiopathogenesis theories
1. Genetic susceptibility:
1st degree relative of RA pt
HLADR4 +ve in 70% of RA pt
2. Autoimmune response:
Antigen attracted to synovium?
Presented to APC(B-cell with HLADR4)
Type 4 reaction=chronic IFN(T-cell)
Type 3 reaction=(anti-CCP Ab
+R.F(anti-IgG Ab))Etiopathogenesis theories
3. Chronic synovitis(joints&tendon
sheaths)=(cytokines(TNF,IL-1&IL-
6)+Ab/Ag complexes,PGs)=destruction,
granulation tissue,fibrosis
4. Systemic involvement with Chronic IFN
process
Every organ involvement in different
pace,not a one type processRA pathological stages 1. Pre-clinical(years earlier)=no S&S,high CRP&ESR and RF present 2. Synovitis=acute IFN,joint mobile,not stiff (potentially reversible) 3. Destruction=chronic IFN destroy by : WCC +osteoclasts enzs Vascular and pannus invasion(granulation) Joint destruction+tendon rupture 4. Deformity =due to joint destruction +tendon rupture+ capsule laxity+
Extra-articular lesions pathology 1. Rheumatoid nodules=non-caseating necrotic subcutaneous granuloma over bony prominences, tendon(trigger), synovium,sclera,viscera(lung,kidey,GI ,heart) 2. LNs+splenomegaly(cells hyperactivity) 3. Vasculitis=nail infarction,MI 4. Myopathy or C1/C2 sublux,spine # or Cord compression 5. Peripheral neuropathy or nerve compression(CTS)
Clinical features
Mostly insidious over months, but
sometimes acute
Early:
1. Symmetrical bilateral PIP
arthritis/stiffness
2. Tiredess,muscleache,wt
loss,unwellness
3. Early morning stiffness>30min
4. Spread to
wrist>feet>knee>shoulder
5. Tender swollen joints, thick
tendons (EPL,FDP,FDS),but no
deformity, no restricted ROMClinical features
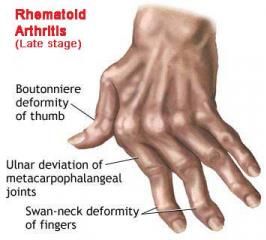
Late:
1. Deformity, stiffness,
dull ache pain,
decrease ROM
2. Valgus knees&feet
&finger
3. Claw toes
4. Volar radial wrist
displacement
5. 30%painfull/stiff
neckClinical features Advanced: Late stage+extra- articular features In 25% of cases but pathonomoic
Investigations
Bloods:
1. FBC(normo
normo,why?)
2. ESR,CRP
3. ANA +Ve in 30%,R.F
80%=not specific or
senstive
4. Anti-CCP specific
XRs:
Early=swelling+peri-
articular OP
Late=decrease joint
space+bone erosionsInvestigations+Diagnosis US/MRI=for early ∆ of synovitis Synovial biopsy=not specific histo to RA ∆=clinical features>6/52 + blood results If u find RA, search for other autoimmune IDDM,Hashimoto’s, pernicious anemia anemia, Addison’s ,ITP,MG,SLE,PBC..etc
Differential diagnosis 1. Psoriasis=skin lesions+DIP 2. SLE=slap cheeks+lungs,ANCA 3. AS=SIJ+bamboo spine,seronegative 4. Reiter’s=urethritis,colitis,conjunctivitis 5. Polyarticular gout=crystals,tophi Histo. 6. Peudogout=chondrocalcinosis+crystals 7. Sarcoidosis=hilar LNs,high ACE,erthyma nodosum 8. Lyme disease=endemic areas,tics,serology
Differential diagnosis
9. PMR=pelic/pectrol girdle,respond to low
steriods,risks of GCA
10. Polyarticular OA=DIP&WB joints,there
is osteophytes
RA can do 2nd OA features,but no
osteophytesRx(no CURE!!)
1. Immediate IFN control by high dose
prednislone and taper it
2. Immediate DMARDs start to maintain
control(single or combined)
MTX or leflunomide +sulfasalazine or
hydroxycholorquine
If fail=biological TNF inhibitors(TFNI)=
infliximab,etanercept,adalimumabRx(no CURE!!)
3. Orthotics+physio
4. Surgery=for pain,deformity,dysfunction
Synvectmy,osteotomy,stabilization
Tendon repair or transfer
Arthroplasty,arthrodesis
Need plan to stop/resume MTX and
TFNI peri-operatively to help wound
healing, in liaise with rheumatologistPrognosis Worse with: 1. Female, younger age 2. High ESR,CRP, positive RF&anti-CCP 3. Bone erosions on first presentation 4. Extra-articular features presence Outcome: 60% wax/wane,10%improves, 10% deteriorates in 5 yrs 10% becomes disabled
Complications 1. Deformity 2. Joint rupture 3. Muscle weakness 4. Septic arthritis 5. Spinal cord compression 6. Vasculitis and MI 7. Amyloidosis and nephrotic syndrome 8. Death,mostly by IHD
THANK YOU QUESTIONS ARE WELCOMED, BEFORE BEEN QUESTIONED
Question1 What is the commonest gene related to RA? 1. HLA DR1 2. HLA B27 3. HLA DR4 4. HLA DQ2
Question 2 What is the least joint to be affected by RA? 1. PIPJ 2. Carporadial joint 3. Thumb IPJ 4. Hip
Question 4 What is the best blood test to diagnose RA? 1. RF 2. Anti-CCP 3. SMA 4. c-ANCA
Question 5 What is rheumatoid factor? 1. Anti-IgM antibodies 2. Anti-IgG antibodies 3. Anti-smooth muscle antibodies 4. Anti-T cell antibodies
You can also read