STARS HEALTHCARE PIONEERS REPORT - SHOWCASING BEST PRACTICE IN SYNCOPE 2021 In memory of Dr Adam Fitzpatrick - Arrhythmia Alliance
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

STARS HEALTHCARE PIONEERS REPORT SHOWCASING BEST PRACTICE IN SYNCOPE 2021 In memory of Dr Adam Fitzpatrick www.syncopepioneers.org UK Registered Charity No. 1084898

FOREWORD
Syncope is a transient loss of That syncope is commonly confused was launched in memory of Dr Adam
consciousness (TLoC) that occurs with epilepsy is concerning. If Fitzpatrick, who sadly passed away in
because of a fall in oxygenated diagnosed with epilepsy, a person January 2020. Dr Fitzpatrick, as Chair
blood flow to the brain. It is a may be given unnecessary treatments of STARS Medical Advisory Committee,
relatively common event, with (such as anticonvulsants) and/ founded the “Rapid Access Blackout
incidence rates varying from 6.2 to or told to make unnecessary Clinic” in Manchester — the first
39.7 per 1,000 person-years and lifestyle changes (for example, stop in the world. People were referred
accounting for about 1% of all visits driving). However, what is much and seen in less than two weeks,
to emergency departments.1,2 Studies more concerning is that an epilepsy thereby reducing long waiting times,
suggest that, of those with syncope, misdiagnosis can mask cardiac syncope misdiagnoses, and even sudden
37% and 56% seek medical attention and a potentially life-threatening cardiac death from undiagnosed
from, respectively, a doctor or a arrhythmia — meaning that there cardiac arrhythmia. This concept has
hospital. Furthermore, of those who is failure to receive the needed treatment now been widely adopted and has
visit the emergency department and the patient is not protected against improved outcomes for these patients.
because of syncope, ≥40% are sudden cardiac arrest and sudden
admitted for further investigations. cardiac death.5 We hope that this report will be one
of his legacies — not only providing
A major challenge with syncope, However, overall, the risk of death in examples of best practice but also
given it is a symptom rather than people with syncope is low because, as inspiring healthcare professionals
a diagnosis, is making the correct Koene et al report, “in most cases the to consider new approaches
diagnosis and to allow optimal cause itself is relatively benign”.5 While and to “think outside the box” in
treatment. In fact, syncope can be syncope may not always be life- the management of syncope. The
frequently misdiagnosed as epilepsy threatening, it can frequently be life case studies selected for their
— with Ziadi and colleagues, led by changing. The uncertainty while waiting impact on patient care, examine new
Dr Adam Fitzpatrick, first recognising for a diagnosis (which can be prolonged) technologies, multidisciplinary
this in 2000. Writing in the Journal of and the fear of not knowing of when an team working, managing
the American College of Cardiology attack will occur and/or how to prevent postural orthostatic tachycardia
(JACC), they reported that of 74 men an attack occurring can have a serious syndrome (PoTS) related to
previously diagnosed with epilepsy, impact on quality of life — affecting both deconditioning, and the importance of
31 (41.9%) had an alternative professional and social life. patient education.
diagnosis.3 They add that 19 (25.7%)
had vasovagal syncope and seven To address these challenges of Furthermore, we hope that these case
(9.5%) “had significant ECG pauses misdiagnosis and poor quality of life, studies will inspire you to become
during carotid sinus massage”. last year, STARS launched the Syncope a “Syncope Pioneer” and perhaps
Additionally, Oto, more recently, Healthcare Pioneers Report to “showcase” even submit a case study for next
noted similar findings and that a best practice in syncope. The aim is to year’s report. Submissions for next
Danish study found 30% of children encourage healthcare professionals to year’s report will open in December
with a definite diagnosis of epilepsy explore new and innovative approaches 2021 but, in the meantime, you
did not have the condition.4 to improving the care and quality of can still register as a syncope Centre
life for people with syncope. The report of Excellence here: https://bit.ly/
SyncopeCoEApply
Trudie Lobban MBE Prof. Richard Sutton
Founder and CEO, STARS Medical
STARS Advisory
Committee Member
References
1. Vanbrabant P, Gillet JB, Buntinx F, et al. Incidence and outcome of first syncope in primary care: A retrospective cohort study. BMC Family Practice 2011, 12: 102
2. Saklani P, Krahn A, Klein g, et al. Syncope. Circulation 2013; 127: 1330–39
3. Ziadi A, Clough P, Cooper P, Scheepers B, Fitzpatrick AP. Misdiagnosis of epilepsy: many seizure-like attacks have a cardiovascular cause. J Am Coll Cardiol 2000; 36: 181-184.
4. Oto MM. The misdiagnosis of epilepsy: Appraising risks and managing uncertainty. Seizure 2017;44: 143–46.
5. Koene RJ, Adkisson WO, Benditt DG, et al. Syncope and the risk of sudden cardiac death: Evaluation, management, and prevention. Journal of Arrhythmia 2017; 33: 533–44.
2 www.syncopepioneers.org
CONTENTS
ESTABLISHING A SMARTPHONE AMBULATORY ECG SERVICE FOR
4 PATIENTS PRESENTING TO THE EMERGENCY DEPARTMENT WITH
PRE-SYNCOPE AND PALPITATIONS
JERSEY HEART TEAM DELIVERS ENHANCED INTEGRATED
5 MULTIDISCIPLINARY CARE FOR ISLANDERS WITH BLACKOUTS
NOVEL USE OF A HEART-RATE MONITOR AND ALARM SYSTEM IN
6 THE MANAGEMENT OF SYMPTOMATIC BRADYCARDIA EPISODES
7 CAN AN EARLIER DIAGNOSIS OF PoTS IMPROVE OUTCOMES?
A CASE SERIES ON SWALLOW SYNCOPE – PATIENT EDUCATION AND
8 EMPOWERMENT AS THE MAINSTAY OF MANAGEMENT
COLLABORATIVE WORKING BETWEEN CARDIOLOGISTS AND
9 NEUROLOGISTS SHOULD BE ENCOURAGED FOR THE BENEFIT OF
PATIENTS WITH TRANSIENT LOSS OF CONSCIOUSNESS
10 CENTRES OF EXCELLENCE
11 STARS BLACKOUTS CHECKLIST
16 STARS PUBLICATIONS
17 GLOSSARY
18 NOTES
www.syncopepioneers.org 3
ESTABLISHING A SMARTPHONE AMBULATORY ECG SERVICE FOR
PATIENTS PRESENTING TO THE EMERGENCY DEPARTMENT WITH
PRE-SYNCOPE AND PALPITATIONS
DR MATTHEW J. REED, DR JULIA CULLEN, DR ALEXANDRA MUIR, DR ROSS MURPHY,
DR VALERY POLLARD, DR GORAN ZANGANA, DR SEAN KRUPEJ, SYLVIA ASKHAM,
PATRICIA HOLDSWORTH, DR LAUREN DAVIES
Royal Infirmary of Edinburgh Smartphone Palpitation and Pre-Syncope Ambulatory Care Clinic (SPACC)
service, Edinburgh, UK
INTRODUCTION RESULTS
The Investigation of Palpitations Between 24th July 2019 and
in the ED (IPED) study showed 23rd July 2020, 290 patients
that use of a smartphone-based (aged between 16 and 80
event recorder (AliveCor/Kardia) years; mean age 43.3, SD
led to a five-fold increase in the 15.0) were referred; 120
number of patients in whom an (41.4%) were male. Of the
electrocardiogram (ECG) was 237 (81.7%) who were fitted
captured during symptoms — with the device, 17 (7.2%)
to more than 55% at 90 days had a cardiac diagnosis
compared to 9.5% with standard (12 atrial fibrillation/
care. Therefore, use of an event flutter, five supraventricular
recorder was concluded to be lead devices in the first instance. The tachycardias, and one
a safe, non-invasive, and easy- devices can be cleaned and reused atrial tachycardia). There
to-use device that should be multiple times. were also 200 non-cardiac
considered part of ongoing care diagnoses (84.3%) and 20
From 24 July 2019, when the clinic was
to all patients presenting acutely undiagnosed patients (8.4%).
launched, all patients aged 16 years
with unexplained palpitations or Cost per symptomatic
or older presenting to the ED or AMU
pre-syncope. In this case study, we rhythm diagnosis was £358
of the Royal Infirmary of Edinburgh
report the process of establishing and per cardiac dysrhythmia
(RIE), UK, with palpitations or pre-
a novel Smartphone Palpitation diagnosis was £4,570.
syncope, whose ECG was normal,
and Pre-Syncope Ambulatory
who had a compatible Apple/Android CONCLUSION
Care Clinic (SPACC) service,
phone, tablet or watch, and in whom
enabling Emergency Department This is the first clinical
an underlying cardiac dysrhythmia
(ED) or Acute Medicine Unit implementation of the
was possible, were discharged
(AMU) patients to be referred for AliveCor/Kardia in an
with a patient advice leaflet and an
assessment and education on use ED setting for patients
appointment at the SPACC service
of the device with subsequent presenting with palpitation
(based in Ambulatory Care adjacent
review of device recordings in an or pre-syncope and
to the ED) on the next available day.
ambulatory setting. demonstrates similar
History of the event was revisited in
detection rates to the IPED
METHODS the clinic and eligible patients were
study. A smartphone-based
A clinical Standard Operating fitted with the smartphone-based
event recorder clinic like
Procedure (SOP) was devised, and event recorder. Electronic Patient
ours should be considered
funding was secured through a Record (EPR) data of sequential clinic
for acute palpitation.
business case for the purchase attendees over a 12-month period was
of 40 AliveCor/Kardia single- collected and analysed.
4 www.syncopepioneers.org
JERSEY HEART TEAM DELIVERS ENHANCED INTEGRATED
MULTIDISCIPLINARY CARE FOR ISLANDERS WITH BLACKOUTS
MRS KELLY ANNE KINSELLA, MRS KARI PITCHER, MISS CHARLOTTE HERDMAN,
MRS CATHERINE FRYER, MRS ANGELA HALL, DR ANDREW MITCHELL, DR PIERRE LE PAGE
Jersey Heart Team, Jersey, Channel Islands
INTRODUCTION was monitored
remotely by the
Physiologist-led clinical physiologists.
implantable loop
recorder (ILR) insertion • Day 21: Automated
commenced locally in event, via remote
2019. Initial motivation monitor, records
for its introduction was six seconds of
to free-up the consultant asystole with patient
cardiologist’s time symptom activation
and theatre slots for due to presyncope.
complex cases. However, Cardiologist
important unanticipated recommends device
benefits have been recognised. CASE STUDY upgrade.
The most important being An 81-year-old gentleman, with
an improved patient journey a history of hypertension and • Day 42: Pacemaker
and patient-centred care. spinal stenosis, presented to the is implanted by a
When an ILR is indicated, the Emergency Department following an consultant cardiologist
care of the patients is taken episode of blackout whilst walking and programmed
over by a clinical physiologist, his dog. by the senior clinical
who implants the device and physiologist who
remotely monitors the patient. • Day 11: Patient was assessed in implanted the
the nurse-led TLoC clinic. Patient patient’s ILR.
Clinical physiologists provide reported similar episodes of
device technical support, syncope with head injuries and CONCLUSION
consultation after symptom episodes of presyncope whilst
activation and general follow-up The introduction of
sitting but with no prodrome. dedicated TLoC and a
for these patients. This approach Episodes were happening every
is enabled by the development clinical physiologist-led
six weeks. The examination ILR implantation service
of a greater connection with was normal, with the 12-lead
the arrhythmia specialist nurses has resulted in a more
ECG showing no evidence of efficient use of resource
(who run the transient loss of atrioventricular (AV) block. No
consciousness [TLoC] clinic). This and an improved patient
significant postural drop in journey. The Jersey
has reduced the amount of ILR blood pressure. Transthoracic
data the consultant cardiologist Heart Team continues
echocardiogram showed to consider new ways of
reviews. If a patient requires satisfactory left ventricular
device upgrade, a clinical working to best utilise
function and no valve resources and improve
physiologist will be present abnormalities were noted. The
in theatre and will carry out our patient care. Our
cardiologist agrees periodic multidisciplinary team
patient follow-up care. Thus, the recurrent symptoms warrant
same specialist cares for them approach ensures the best
ILR. Senior clinical physiologist person to provide care for
throughout their patient journey. implanted the ILR. The patient the patient does so.
www.syncopepioneers.org 5
NOVEL USE OF A HEART-RATE MONITOR AND ALARM SYSTEM IN
THE MANAGEMENT OF SYMPTOMATIC BRADYCARDIA EPISODES
DR BETH TAYLOR AND DR BRIAN GORDON Peterborough City Hospital, Peterborough, UK
INTRODUCTION
Episodic symptomatic
bradycardia can occur
because of neck masses
compressing local
structures regulating
autonomic function. Here
we describe a case in which
novel use of a heart rate
monitoring system prior to
decompressive surgery was
utilised to avoid permanent
pacemaker insertion.
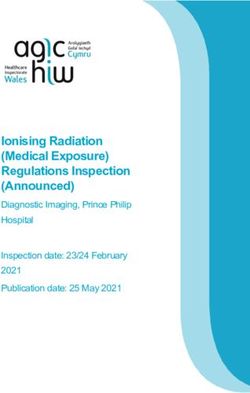
CASE STUDY
A 54-year-old male with
no previous cardiac history from a primary squamous cell provided symptomatic relief for the
presented upon multiple carcinoma in the left tonsil. patient whilst awaiting definitive
occasions with increasingly management of the neck mass with
frequent nocturnal syncope Given the underlying cause tonsillectomy and adjuvant therapy.
episodes characterised by of the bradycardic episodes,
bradycardia and hypotension. permanent pacemaker insertion CONCLUSION
He was admitted to our was contraindicated by the low Autonomic disturbance from
cardiology department and likelihood of success in resolving compressive neck masses has
a 24-hour electrocardiogram the bradycardia and potential previously been described, with
(ECG) was conducted, reversibility following treatment to signs including bradycardia
identifying 125 episodes of reduce mass effect. and hypotension resulting from
nocturnal bradycardia, with mass effect upon local structures
Instead, novel use of a
the longest episode lasting including the carotid sinus and
“PulseGuard” heart-rate
for 28 beats and a slowest vagus nerve. They are potentially
monitoring system was trialled with
recorded heart rate of 39 modifiable causes of episodic sinus
success; the system was originally
beats per minute (Figure 1A bradycardia that may be reversible
designed for use in epilepsy
and 1B). These episodes were following surgical decompression.
management. The two-component
accompanied by a history of Identification of therapeutic methods
system consists of a lightweight
progressive voice weakening to manage symptomatic bradycardia
infrared sensor and tablet that
and swallowing difficulty, with obviates the need for permanent
communicate via Bluetooth within
examination demonstrating pacemaker implantation in patients
a 2m range (Figure 1C). A target
multiple left lower cranial awaiting decompressive surgery.
heart rate can be programmed,
nerve palsies and a left-sided This case study illustrates the novel
outside of which an alarm will
neck mass. MRI imaging use of heart-rate monitoring alarm
sound. By instigating awakening
revealed the mass to be an device as a low-cost temporary
upon detection of bradycardia,
enlarged lymph node with alternative to permanent pacing in
prior to onset of syncopal
histology and PET-CT imaging the management of these patients.
symptoms, use of the system
confirming metastatic spread
6 www.syncopepioneers.org
CAN AN EARLIER DIAGNOSIS OF PoTS IMPROVE OUTCOMES?
DR SHAMIL YUSUF, MS HELEN EFTEKHARI, MS GEETA PAUL, MS SARAH ABBOTT, MS ALBIONA ZHUPAJ
University Hospitals Coventry & Warwickshire, Coventry, UK | University of Warwick (HE)
INTRODUCTION
In UK, on average, it takes seven years to
achieve a diagnosis of postural tachycardia
syndrome (PoTS), which can have a significant
impact on quality of life, including having to
stop studying and working.
The 2018 European Society of Cardiology
(ESC) syncope guidelines identify more
evidence of the role of nurses in syncope
clinics. Arrhythmia nurses and one lead
syncope electrophysiology consultant run ECG-Sinus-Tachycardia 19 PoTS
our syncope clinic. The nurses are trained in
health assessment and prescribing, seeing DIAGNOSIS & MANAGEMENT
75% of patients. Deconditioning PoTS
PATIENT HISTORY AND TESTS • Education & counselling on PoTS, symptoms &
prognosis.
A previously fit, active 19-year-old (Ms
C) was referred to the multidisciplinary • Fluids front loading, aiming for 2.5 litre and good
Syncope & PoTS clinic following a recent quality fluids.
A&E attendance, reviewed by our nurse. • Salt intake to aim for 10g per day.
She has attended A&E eight times in the • Dietary changes: small frequent meals, with minimal
past two months with a six-month history of refined carbohydrates.
palpitation and near syncope. The symptoms
were scaring her. • Home exercise programme given to start with
recumbent exercises.
Throughout the COVID-19 lockdown, she was • Aim to return to studies.
studying in bed and staying in her room all
day. After three months, her symptoms began At a virtual review at five months, there had been no further
and she stopped her studies. Fluid intake A&E attendances & she returned to college. Delta heartA CASE SERIES ON SWALLOW SYNCOPE – PATIENT EDUCATION
AND EMPOWERMENT AS THE MAINSTAY OF MANAGEMENT
DR MELANIE DANI, DR PATRICIA TARABORRELLI, MR ANDREAS DIRKSEN, DIMITRIOS
PANAGOPOULOS, MIRIAM TOROCASTRO, PROFESSOR RICHARD SUTTON, DR BOON LIM
Imperial Syncope Unit, Imperial College Healthcare NHS Trust, Hammersmith Hospital, London, UK
INTRODUCTION
Our syncope unit places high
value on patient education
and empowerment, and we
strive to reflect this in all our
consultations, investigations,
and treatments. We describe
three patients in our service Stop Fainting! This is the logo of the authors’ free educational
website, www.stopfainting.com
with swallow syncope — a
form of reflex neural syncope
that she could control her modified her diet by time she
occurring on swallowing. By
symptoms by diet and bite size had her cardiac investigations,
understanding the underlying
modification. She remains well which were normal, and she
pathophysiology and the
to date. remains asymptomatic to date.
triggers and modifiers for their
syncope, all three patients were PATIENT TWO RESULTS
able to ameliorate or abolish
A 46-year-old woman described All three of these patients had
their symptoms; thus, avoiding
light-headedness upon eating a rare form of reflex neural
invasive medical interventions
for 18 months. Investigations syncope occurring during
and retaining a sense of control.
revealed bradycardia and a vital action — eating. The
We have recently described
a three-second pause consequences of this condition
this management strategy in a
occurring during eating. She can be significant and can require
journal publication, as we wish
also considered ganglionic potentially invasive therapies
to share the importance of
plexus ablation but following such as pacemaker implantation
patient education with our wider
comprehensive education about and cardioneuroablation.
community of colleagues.
conservative measures between
her appointments, she modified CONCLUSION
PATIENT ONE
her diet to the extent that her We place a strong emphasis on
A 25-year-old woman reported
symptoms almost completely patient education, information,
light-headedness when eating
resolved. and empowerment. This short
sandwiches and sausage rolls.
case series emphasises this
Continuous cardiac monitoring PATIENT THREE and highlights the fact that
while eating these trigger
A 54-year-old woman reported these individuals improved
foods revealed pauses lasting
a sensation of food getting with effective conservative
four seconds, and crucially
stuck in her throat followed by care, avoiding invasive medical
showed her the direct effects
sudden unheralded collapse. procedures — resulting in high
of eating these foods on her
Conservative strategies were satisfaction. We strive to make
cardiac conduction system,
emphasised, and she modified patients’ wellbeing at the centre
prompting diet modification.
her diet to choose soft foods, of our service, and we believe that
Cardioneuroablation was
and adopted “slow cooking” this short case series reflects this.
discussed, but she was satisfied
methods. She had successfully
8 www.syncopepioneers.orgCOLLABORATIVE WORKING BETWEEN CARDIOLOGISTS AND NEUROLOGISTS
SHOULD BE ENCOURAGED FOR THE BENEFIT OF PATIENTS WITH TRANSIENT LOSS
OF CONSCIOUSNESS
DR NASRIN KHAN, DR SAQIB AHMAD, DR JANAKA PATHIRAJA, DR FRANCESCO MANFREDONIA,
DR SANJIV PETKAR
New Cross Hospital, Wolverhampton, UK
INTRODUCTION Reflex syncope group (12)
Syncope, epilepsy, and Test Performed in Result
psychogenic disorders are the (%)
Baseline 12-lead ECG 12 (100) No abnormalities detected
three most common causes of ECHO 12 (100) One abnormal
transient loss of consciousness Holter (mean duration 65±33 hours) 7 (58.3) No significant arrhythmias
(TLoC), of which syncope is Implantable loop recorder 3 (25.0) One patient with significant symptomatic sinus
the most prevalent. Clinical bradycardia
presentation of all three are Tilt table test 2 (16.7) One patient with vasodepressor syncope
similar. In the majority, a Carotid sinus massage 1 (8.3) Negative
Exercise tolerance test 2 (16.7) No abnormalities — cardiac ischaemia/arrhythmias
complete history, physical Follow-up: Seven patients (58.3%) were discharged — five (41.7%) after the first consultation. In nine (75%),
examination, lying and standing initial diagnosis confirmed at follow-up. One patient (8.3%) had epilepsy.
blood pressure, and 12-lead Arrhythmic syncope group (8)
electrocardiogram (ECG) help Test Performed in Result
in arriving at a diagnosis. The (%)
Baseline 12-lead ECG 8 (100) Two abnormal (1 = q waves V1–V3; 1 = T inversion)
National Institute for Health ECHO 8 (100) One abnormal
and Clinical Excellence (NICE) Holter (mean duration 88±36 hours) 6 (75) No significant arrhythmias detected
TLoC guidelines recommend Implantable loop recorder 4 (50) One patient had paroxysmal atrial fibrillation
first-stage assessment for (consequently, anticoagulated)
all patients with TLoC, with Exercise tolerance test 2 (25) No abnormalities – cardiac ischaemia/arrhythmias
selected patients undergoing Follow-up (so far): diagnosis confirmed in three (37.5%).
Uncertain cause group (10)
second-stage assessment. Test Performed in Result
(%)
METHODS Baseline 12-lead ECG 10 (100) Two abnormal (one T inversion; one right bundle
branch block)
Our aim was to assess the
ECHO 10 (100) One abnormal
prevalence of syncope in Holter (mean duration 87±53 hours) 8 (80) One showed non-significant sinus pauses
patients referred to a First Implantable loop recorder 3 (30) One showed significant sinus pauses, requiring
Seizure Clinic and the type of pacemaker insertion and one showed sinus
syncope and management of tachycardia secondary to epilepsy.
such patients. Tilt table test 1 (10) Negative
Carotid sinus massage 1 (10) Negative
We examined medical records Exercise tolerance test 1 (10) No abnormalities – cardiac ischaemia/arrhythmias
Stress MRI 1 (10) Normal
for all patients (n=36) referred Follow-up: one patient (10%) each had arrhythmogenic syncope, reflex syncope, and postural hypotension,
to TLoC clinic at a tertiary Three patients (30%) had epilepsy
cardiology centre from a First
Seizure Clinic (n=83) between 13 (36%) had variable frequency, and the remainder had about three episodes per
April 2016 and March 2017 who month. After cardiology second-stage assessment, the provisional diagnosis of TLoC
had completed a minimum of was as follows: reflex syncope (12); arrhythmogenic syncope (8); uncertain cause (10);
one-year follow-up and who epilepsy (5); migraine (1).
were assessed as per NICE
TLOC Guidelines. CONCLUSION: A high proportion (at least 25%) of patients with syncope were
initially referred to a neurologist led First Seizure Clinic, following which they were
RESULTS appropriately redirected to cardiology. This referral pattern causes unnecessary
The mean age of patients delay in assessment, diagnosis and treatment and only increases patient anxiety
(36 overall) was 41±16.5 years and distress, while wasting scarce NHS resources. Education of referrers will help.
(median: 38; range: 28-54) and This study also highlights the close collaborative working between cardiologists
58% (21) were male. Nine (25%) and neurologists at our centre and the appropriate application of second stage
had a single episode of TLoC; assessment of NICE TLoC guidelines for the benefit of patients.
www.syncopepioneers.org 9THE 2021 SYNCOPE PIONEERS CENTRES OF EXCELLENCE
The following centres (listed alphabetically by location) are acknowledged as a Syncope Centre of
Excellence. As evidenced by the case studies that have been submitted, and that have been published in
this report, each centre takes an innovative approach to managing syncope. Their work can be used to
inspire other centres to improve care and quality of life for people with syncope.
COVENTRY, UK
Can an earlier diagnosis of PoTS improve outcomes? (page 7)
University Hospitals Coventry & Warwickshire, Coventry, UK
University of Warwick (HE)
Dr Shamil Yusuf, Ms Helen Eftekhari, Ms Geeta Paul, Ms Sarah Abbott, Ms Albiona Zhupaj
www.uhcw.nhs.uk
EDINBURGH, UK
Establishing a smartphone ambulatory ECG service for patients presenting to
the emergency department with pre-syncope and palpitations (page 4)
Royal Infirmary of Edinburgh Smartphone Palpitation and pre-syncope Ambulatory Care Clinic
(SPACC) service, Edinburgh, UK
Dr Matthew J. Reed, Dr Julia Cullen, Dr Alexandra Muir, Dr Ross Murphy, Dr Valery Pollard,
Dr Goran Zangana, Dr Sean Krupej, Sylvia Askham, Patricia Holdsworth, Dr Lauren Davies
www.emergeresearch.org/trial/iped-implementation-study
JERSEY, CHANNEL ISLANDS
Jersey Heart Team delivers enhanced integrated multidisciplinary care
for Islanders with blackouts (page 5)
Jersey Heart Team, Jersey, Channel Islands
Mrs Kelly Anne Kinsella, Mrs Kari Pitcher, Miss Charlotte Herdman, Mrs Catherine Fryer, Mrs Angela Hall, Dr
Andrew Mitchell, Dr Pierre Le Page.
www.gov.je/Health/IllnessVaccine/Pages/HeartCardiac.aspx
LONDON, UK
A case series on swallow syncope – patient education and empowerment
as the mainstay of management (page 8)
Imperial Syncope Unit, Imperial College Healthcare NHS Trust, Hammersmith Hospital, London, UK
Dr Melanie Dani, Dr Patricia Taraborrelli, Mr Andreas Dirksen, Dimitrios Panagopoulos,
Miriam Torocastro, Professor Richard Sutton, Dr Boon Lim
www.stopfainting.com
PETERBOROUGH, UK
Novel use of a heart-rate monitor and alarm system in the management
of symptomatic bradycardia episodes (page 6)
Peterborough City Hospital, Peterborough, UK
Dr Beth Taylor and Dr Brian Gordon
www.nwangliaft.nhs.uk/a-z-of-services/c/cardiology
WOLVERHAMPTON, UK
Collaborative working between cardiologists and neurologists should be encouraged for
the benefit of patients with transient loss of consciousness (page 9)
New Cross Hospital, Wolverhampton, UK
Dr Nasrin Khan, Dr Saqib Ahmad, Dr Janaka Pathiraja, Dr Francesco Manfredonia, Dr Sanjiv Petkar
www.royalwolverhampton.nhs.uk
10 www.syncopepioneers.orgwww.stars-international.org
The Blackouts Checklist was prepared under the guidance of STARS’ expert Medical Advisory
Committee. Its principal aim is to help you and your doctor reach the correct diagnosis for any
unexplained loss of consciousness (blackout).
The Checklist gives you information and advice on the major reasons for experiencing a blackout, helps you prepare for a doctor’s
appointment, and provides information on what to expect if you have to attend a hospital appointment.
CHECKLIST: What do you need to know?
� A blackout is a temporary loss of consciousness � Many syncopal attacks only require reassurance from
If someone loses consciousness for a few seconds or your GP
minutes, they are often said to have had a blackout. Many syncopal attacks require only explanation and
reassurance from a GP or trained nurse regarding the
� There are three major reasons for why people may likely absence of anything being seriously wrong.
experience a blackout(s): Consultation with a specialist will be necessary, though,
● Syncope: a sudden lack of blood supply to the if the cause of the syncope remains uncertain or if there
brain. Syncope is caused by a problem in the regulation are particularly concerning symptoms or there is a family
of blood pressure or by a problem with the heart. history of a heart condition. Also, if the blackouts happen
● Epilepsy: an electrical ‘short-circuiting’ on several occasions, you may be referred to a specialist.
in the brain. Epileptic attacks are usually called seizures. � Misdiagnosis is common but avoidable:
Diagnosis of epilepsy is made by a neurologist.
● Many syncopal attacks are mistaken for epilepsy.
● Psychogenic blackouts: resulting from stress
or anxiety. Psychogenic blackouts occur most often ● However, epilepsy only affects slightly less than
in young adults. They may be very difficult to diagnose. 1% of the population.
‘Psychogenic’ does not mean that people are ‘putting ● UK research has shown that approximately 30%
it on’. However there is often underlying stress due to of adults and up to 40% of children diagnosed
extreme pressure at school or work. In exceptional cases it with epilepsy in the UK do not have the condition.
may be that some people have experienced ill treatment ● Many elements of a syncopal attack, such as
or abuse in childhood. random jerking of limbs, are similar to those
� Every patient presenting with an unexplained experienced during an epileptic seizure.
blackout should be given a 12-lead ECG (heart ● It can be difficult to tell the causes of the
rhythm check) blackout apart.
It is important that the ECG is passed as normal. � Syncope causes falls:
� Witness information is vital for the evaluation ● Syncope causes a signicant number of falls in older
of blackouts adults, particularly where the falls are sudden and not
obviously the result of a trip or slip.
Make sure a witness (family or friend) who has been
with you during a blackout or fall is present during any ● Many older adults will only recall a fall and will not
meeting with a doctor. realise they have blacked out.
● Greater awareness of syncope as a cause of falls
� Most unexplained blackouts are caused by syncope
is key to effective treatment and prevention of
But much more commonly they are due to syncope recurring falls.
(pronounced sin-co-pee) – a type of blackout which is
caused by a problem in the regulation of blood pressure or
sometimes with the heart. Up to 50% of the population will
lose consciousness at some point in their life due to syncope.
Syncope can affect all age groups but the causes vary with
age, and in older adults multiple causes often exist.
If you would like further information or would like to provide feedback please contact:
www.syncopepioneers.org
STARS, Unit 6B, Essex House, Cromwell Business
Registered Charity Park, Chipping Norton, Oxfordshire OX7 5SR
No. 1084898 11
� +44(0)1789 867 503 � www.stars.org.uk @ info@stars.org.ukThe Blackouts Checklist
www.stars-international.org
Helping you and your doctor reach the
correct diagnosis following unexplained
loss of consciousness or falls
CHECKLIST: Preparing for an appointment with your GP
Before visiting your doctor, it is important to write down If there are any questions you want to ask your doctor or
what happens before, during and after a blackout or fall, specialist, make a note of them on the Checklist as it can
including any symptoms you may experience. be easy to forget to ask them during the consultation.
Try to take along a family member or friend, who has seen Check that both syncope and epilepsy have been
your blackout(s) or fall(s), to your appointment. If they considered. Ask for a referral to a paediatrician
cannot accompany you, ask them to write down exactly (for a child) or a cardiologist/electrophysiologist
what they saw in the Checklist booklet or ask them how the (heart rhythm expert) if possible or, if you are unsure
doctor could contact them if necessary. If it is safe to video that the diagnosis is accurate, to both a cardiologist
an attack, this is often very helpful in making a diagnosis. and neurologist. You could also ask about possible
referral to local rapid-access clinics for blackouts,
Family history; check with relatives whether there is any falls or arrhythmias.
family history of blackouts, faints, epilepsy, or sudden/
unexplained deaths. This is important as it can often Make detailed notes – use the space later in the Checklist.
provide a clue to the possible cause of your blackout.
Take the Checklist and your notes with you to your
appointment.
CHECKLIST: Questions to ask your GP
During your GP appointment it can be hard to remember everything. Here are some suggestions of questions which you may nd
useful to ask during your appointment. There is a section on the Checklist for you to make a note of any questions for your GP.
Can I still go to school, college or work whilst I am waiting to What is the likelihood that a diagnostic test will deliver a
see the specialist? denitive result?
Can I go to the gym/play sport whilst I am waiting to see What will the treatment involve? Do you think I will have
the specialist? to visit the hospital frequently or stay overnight?
Can I still drive whilst I am waiting to see the specialist?
12 www.syncopepioneers.org
Authors: STARS Medical Advisory Committee Reviewed by Dr Charlotte D’Souza
Registered Charity No. 1084898 © STARS Published October 2009, Reviewed May 2018www.stars-international.org
CHECKLIST: Preparing for specialist tests at the hospital
� Following your appointment with the doctor you may be ● Heart monitor – This is used to record heart rhythms
referred for some tests with a specialist to determine the whilst away from the hospital or to activate during an
cause of your blackouts. Being prepared for these can episode. A 24-hour/seven day heart rate monitor is
signicantly reduce the anxiety of a hospital visit. Try to very unlikely to identify any problems if you experience
learn about these in advance at www.stars.org.uk and go blackouts once a week or less, so do not be afraid to
to ‘For Patients’ section of the website. ask about other options.
� The latest guidelines on the diagnosis of syncope state that ● Insertable cardiac monitor (ICM) – This device
patients suspected of having syncope should receive one of should be used to monitor heart rhythms for months
the following tests. Make sure that you receive the right test at a time if the episodes are less frequent than every
based on the nature of your symptoms. two weeks. The device can remain in place for up to
three years.
� There are information sheets on the following diagnostic
tests available from www.stars.org.uk ● Tilt table testing – This procedure can be used to
induce a syncopal/fainting attack whilst connected
Every patient presenting with an unexplained to heart and blood pressure monitors.
blackout should be given a 12-lead ECG
● 12-lead electrocardiogram (ECG) for heart Tests aimed at epileptic seizures:
rhythm analysis – Every patient presenting with an ● Electroencephalogram (EEG) – For brain activity
unexplained blackout should be given a 12-lead analysis to check for epilepsy. The EEG cannot be used
electrocardiogram (ECG). If there is uncertainty about to diagnose epilepsy, but it is helpful to neurologists
diagnosis the ECG should be reviewed by a heart to decide which type of epilepsy is happening. The EEG
rhythm specialist (electrophysiologist). is much less useful over the age of 35 years.
Tests aimed at syncope: ● MRI or CT-scan – These are not aimed at showing
● Lying and standing blood pressure recording that someone has epilepsy, but are used to seek the
Drops in blood pressure with changes in posture can cause when epilepsy is likely, and look for more sinister
cause dizziness, falls and blackouts, particularly in older causes of blackouts and/or seizures.
patients and those on blood pressure medicines and
diuretics (water tablets).
CHECKLIST: Questions to ask your GP and specialist
During your GP or Specialist appointment it can be hard to remember everything. Here are some suggestions of questions which
you may nd useful to ask during your appointment. There is a section on the Checklist for you to make a note of any questions for
your GP/Specialist.
� Can I continue to drive? � If treatment is offered you may wish to ask whether it
will completely stop you having blackouts or falls. If no
� What is the likelihood that a diagnostic test will deliver a treatment is offered be sure to ask the best way to
denitive result? manage your condition.
Further Information: STARS, Unit 6B, Essex House, Cromwell Business Park, Chipping Norton, Oxfordshire OX7 5SR
� +44(0)1789www.syncopepioneers.org
867 503 � www.stars.org.uk @ info@stars.org.uk 13The Blackouts
Blackouts Checklist
Checklist
www.stars-international.org
www.stars-international.org
Sometimes during
Sometimes during aa consultation
consultation it it can
can be
be hard
hard to
to remember
remember everything.
everything.TheThechecklist
checklistisisdesigned
designed
for you to complete. If you have a friend or family member (witness) who has been with youduring
for you to complete. If you have a friend or family member (witness) who has been with you during
a blackout or fall, it is VITAL to ask for their help in lling out parts of the form.
a blackout or fall, it is VITAL to ask for their help in lling out parts of the form. Please ensure Please ensure
your witness
your witness completes
completes their their sections
sections of of the
the Checklist.
Checklist. This
This will
will help
help your
your GP
GP toto refer
referyou
youto
tothe
the
appropriate specialist to make the right diagnosis.
appropriate specialist to make the right diagnosis.
Preparing your own CHECKLIST
Preparing your own CHECKLIST
To give the doctors the best chance of making the right referral or diagnosis you should provide as many details as possible about
To give
your the doctors
blackout(s) or the best chance of making the right referral or diagnosis you should provide as many details as possible about
fall(s).
your blackout(s) or fall(s).
Name:
Name:
1. List any medication(s) you are currently taking:
1. List any medication(s) you are currently taking:
2. Do you experience blackouts, falls or both? (Tick as appropriate)
2. Do you experience blackouts, falls or both? (Tick as appropriate)
Blackouts Falls Blackouts and Falls
Blackouts Falls Blackouts and Falls
If you experience falls, are they unexplained or due to a slip or trip?
If youUnexplained
experience falls, are they unexplained or Slip
dueortotrip
a slip or trip?
Unexplained Slip or trip
3. Do you always lose consciousness? Please ask a witness (Tick as appropriate)
3. Do you
Yes always lose consciousness? PleaseNo
ask a witness (Tick as appropriate)
Yes No
How long are you unconscious for?
How long are you unconscious for?
4. How frequent are your blackouts or falls? (Tick as appropriate)
4. HowDaily
frequent are your blackouts or falls?Weekly
(Tick as appropriate) Every one to two weeks
Daily
Less frequent than every two weeks Weekly Every one to two weeks
Less frequent than every two weeks
5. Before a blackout or fall did you have any warning signs? (Tick as appropriate)
5. Before a blackout or fall did you have anySweating
Light-headedness warning signs? (Tick as appropriate) Nausea
Light-headedness
Looking pale Sweating
Palpitations Nauseaout or dots in vision
Greying
Looking
Change pale
in hearing Palpitations
Other (give details below) Greying out or dots in vision
Change in hearing Other (give details below)
6. Is there anything that triggers your blackout or fall?
6. Is(Tick
there anything that
as appropriate; if onetriggers your blackout
trigger occurred at one timeorand
fall?
another at another time, tick both)
(Tick Pain
as appropriate;
or a fright if one trigger occurred at one time
Not and another at another time, tick both) Alcohol
eating
Pain
Lackor
ofasleep
fright Not eating
Stressful situation Alcohol lights
Flashing
Anxiety
Lack of sleep Going from
Stressful sitting or lying to standing
situation Standing
Flashingfor a long time
lights
Being very hot
Anxiety Exercise
Going from sitting or lying to standing Other (givefor
Standing details
a longbelow)
time
Being very hot Exercise Other (give details below)
14 www.syncopepioneers.org7. Describe what happens during your blackout or fall. Please include whether your episodes are identical on
each occasion or if there are differences.
If you are not conscious or cannot remember to ask someone who was with you at the time to describe what happened.
Your description
Friend or family description
WITNESS: Do the individual’s limbs move whilst they are unconscious? Do they jerk about randomly or rhythmically?
Randomly Rhythmically
WITNESS: Do the individual’s arms move around their head?
Yes No
WITNESS: Are the individual’s eyes opened or closed?
Don’t know Open Closed
If open, how do their eyes move?
8. After your blackout
WITNESS: Following the individual’s blackout or fall, how long before they regain consciousness?
After the blackout or fall are you confused on coming around? How long does the feeling last?
How do you feel after a blackout or fall?
Are your blackouts or falls affecting your daily activities or quality of life?
Yes No
9. Family history If there is, who/what relation?
Is there a history of loss of consciousness in your family? Yes No
Is there a history of deafness in your family? Yes No
Has anyone suffered a sudden cardiac death in your family? Yes No
Have there been any sudden deaths in the family under 55 years? Yes No
Is the cause known?
Any other questions you would like to ask the doctor or specialist:
www.syncopepioneers.org 15STARS PUBLICATIONS
STARS patient resources available to download from the STARS website:
http://bit.ly/STARSPatientResources
If you are a healthcare professional, you can bulk order these resources by emailing
jenni@stars.org.uk or calling 01789 867 503
CHECKLIST
• The Blackouts Checklist
BOOKLETS
• Arrhythmias: Understanding your condition
• Bereavement: Life following the loss of a loved one
• Cognitive behavioural therapy for chronic health conditions
• Diagnostic tests for syncope – Patient information
• Insertable Cardiac Monitor (ICM)
• Living with low blood pressure
• Mindfulness and Healthy Living with Syncope
• Pacemaker patient information
• Postural tachycardia syndrome (PoTS)
• PoTS FAQs
• Psychogenic blackouts
• Reflex anoxic seizures (RAS)
• RAS Frequently asked questions
• Reflex syncope (Vasovagal Syncope)
• Syncope and Falls in the Elderly (SaFE)
• Syncope in care home residents
• Tilt table test
• Understanding your blood pressure
• What can I do about sudden cardiac arrest?
• Which ECG is right for you?
PAEDIATRIC RESOURCES
Specifically written for children
• Bertie’s pacemaker
• Jack has RAS
• Jane’s ILR
• RAS Children’s factsheet
16 www.syncopepioneers.orgGLOSSARY
ARRHYTHMIA = An abnormal heart rhythm.
ATRIAL FIBRILLATION = An irregular heart rhythm that originates in the upper chambers (atria) of the
heart and is a major cause of stroke.
ATRIOVENTRICULAR (AV) BLOCK = The electrical signal travelling from the upper chambers (atria) of
the heart to the lower chambers (ventricles) of the heart is impaired.
BLACKOUT = A temporary loss of consciousness (TLoC) of unknown cause.
BRADYCARDIA = A slower than normal heart rate (less than 60 beats per minute).
CARDIONEUROABLATION = Radiofrequency (RF) catheter ablation of the cardiac vagal nervous
system aiming for permanent attenuation or elimination of the cardioinhibitory reflex.
ELECTROCARDIOGRAM (ECG) = A non-invasive test that records the heart’s rhythm and rate.
HYPOTENSION = Low blood pressure.
INSERTABLE CARDIAC MONITOR (ICM) = A miniature device that is implanted, via a minimally
invasive procedure, under the skin to continually record your heart rhythm. Typically used when other
tests, such as an ECG, have not identified an arrhythmia in the presence of continued symptoms.
MULTIDISCIPLINARY TEAM (MDT) = A team of healthcare professionals that includes different
disciplines (e.g., doctors and nurses) and specialisms (e.g. cardiologist and neurologist).
PACEMAKER = A small device implanted under the skin that produces electrical impulses to treat an
abnormal heart rhythm.
PALPITATION = A rapid noticeable heartbeat, which can be a sign of an arrhythmia.
POSTURAL TACHYCARDIA SYNDROME (PoTS) = An abnormal response by the autonomic
(involuntary) nervous system when changing to an upright position. It is defined as a persistent increase
in heart rate of over 30 beats per minute (or higher than 120 bpm) when standing upright.
REFLEX (VASOVAGAL) SYNCOPE = A transient condition resulting from an abrupt dysfunction of the
autonomic nervous system, which regulates blood pressure and heart rate.
SMARTPHONE-BASED [ECG] EVENT RECORDER = a device (for example, AliveCor/Kardia) that uses
a smartphone (or tablet) app to perform an ECG, which can either be recorded via the smartphone’s
camera or via a small hand-held machine.
SYNCOPE = A sudden temporary loss of consciousness (more commonly known as a faint) that is the
result of reduced blood flow to the brain.
SUPRAVENTRICULAR TACHYCARDIA = An abnormally fast heart rate (resting heart rate above 100
beats per minute) that arises from the upper chambers of the heart (the atria).
TACHYCARDIA = An abnormally fast heart rate over 100 beats per minute.
TILT TABLE TEST = An autonomic test used to induce an episode whilst connected to heart and blood
pressure monitors.
www.syncopepioneers.org 17NOTES 18 www.syncopepioneers.org
NOTES
www.syncopepioneers.org 19WORKING TOGETHER WITH INDIVIDUALS,
FAMILIES AND MEDICAL PROFESSIONALS
TO OFFER SUPPORT AND INFORMATION ON
SYNCOPE CONDITIONS.
To view case studies, centres of excellence, syncope healthcare
pioneer reports or to submit a case study visit:
www.syncopepioneers.org
Founder & CEO
Trudie Lobban MBE FRCP (Edin)
UK Registered Charity No:
1084898
E: info@stars-international.org
T: +44 (0) 1789 867 502
W: www.stars-international.org
Copyright
Published June 2021
www.syncopepioneers.orgYou can also read