STAFF - 2021 BENEFITS GUIDE - My Gardner White Benefits
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2 0 21 B E N E F I T S G U I D E
- S T A F F -
TABLE OF CONTENTS
Welcome........................................................................................................................... 3
Elections........................................................................................................................... 4
Benefits At-A-Glance........................................................................................................ 5
Medical Plan Options....................................................................................................... 6
Wellness Program............................................................................................................ 7
Non-Smoking Incentive.................................................................................................... 7
Medical..........................................................................................................................8-9
Health Equity HSA Account............................................................................................ 10
Blue Member Secured Services..................................................................................... 11
Online Telemedicine Visits............................................................................................. 12
Dental.........................................................................................................................13-15
Vision............................................................................................................................... 16
Basic Life and AD&D....................................................................................................... 17
Voluntary Life and AD&D................................................................................................ 18
Short Term Disability....................................................................................................... 19
Voluntary Long Term Disability....................................................................................... 20
FSA.............................................................................................................................21-22
Employee Assistance Program...................................................................................... 23
Will Preparation Services............................................................................................... 24
Identity Theft................................................................................................................... 24
Travel Assist.................................................................................................................... 25
Pet Insurance.................................................................................................................. 26
Accident.....................................................................................................................27-28
Whole Life....................................................................................................................... 29
Hospital Indemnity.......................................................................................................... 30
Mandatory Notices......................................................................................................... 31
Medicare Part D Notice.............................................................................................32-33
CHIP Notice................................................................................................................34-37
Resources....................................................................................................................... 37
2
WELCOME
Gardner-White Furniture is pleased to offer an
excellent benefit program. These health and welfare Medicare Part D Prescription
benefits are designed to protect you and your Drug Information
family while you are an active employee. We If you are enrolled in or will be eligible
encourage you to carefully review this information
for Medicare in the next 12 months,
and share it with your covered dependents.
Federal law gives you more choices for
Eligibility prescription drug coverage. See pages
Health and welfare benefits are available to all 32-33 for more information.
full-time regular employees who work more than 30
hours per week.
New Hire Waiting Period
Dependent Eligibility As a condition of eligibility for benefits, employees must
Your dependents may also be covered under the complete a one-month bona fide employment-based
medical, dental, vision and optional life benefits. orientation period.
Eligible dependents include:
Eligible employees may enroll for benefits on the first
• Your legal spouse. of the month following 60 days after they complete
• Medical, Dental and Vision: the orientation period. If elected, coverage will be
Your children to the end of the calendar year effective on that date if you completed the necessary
they attain the age 26 regardless of their online enrollment. As a new employee you have up to
marital, student, or financial status. 30 days after your eligibility date to make your benefit
• Optional Life: selections. If you do not enroll within the first 30 days
Your children to the end of the calendar year of your eligibility date, you will not be eligible for
they attain the age 26 regardless of their coverage until the next open enrollment period.
marital, student, or financial status.
Terminating Coverage
If you leave Gardner White for any reason all benefit
coverages will end on your last date of employment.
This guide highlights the main benefits available. For a more complete description, please see the Plan Documents. If any
conflict should arise between this guide and the Plan Documents, the Plan Documents will govern.
3
ELECTIONS
Knowing that every employee has different needs, Gardner-White Furniture’s Employee Benefit Program is
specifically designed to provide basic benefits and allow you the flexibility to elect those levels of coverage you
choose for you and your family.
Elections
It is important that you make your choices carefully. Changes to those elections can generally only be made
during the annual open enrollment period. Exceptions will be made for certain changes in status during the year,
allowing you to make a mid-year benefit change consistent with the change in status. If you have a change in
status, you must change your benefit elections within 30 days of the qualifying event, or you will need to wait
until the next annual open enrollment period. A change in status includes:
• Change in legal marital status (marriage, death of spouse, divorce or legal separation)
• Change in the number of dependents (birth, death, adoption or placement for adoption)
• Change in the employment status of the employee or the employee’s spouse including begin or terminate
employment, change in eligibility (full time to part time), a strike or lockout, commencement or return from
an unpaid leave of absence and a change in worksite
• Dependent satisfies or ceases to satisfy eligibility requirements (attains a particular age)
• Alternate open enrollment time frame for spouse or loss of other coverage
What happens if I do not enroll?
If you do not enroll within the required time period, you will not be eligible for benefits until the next annual open
enrollment period or you experience a change in status. You may
be subject to waiting periods or reduced benefits if you decide to
enroll at a later date.
Will my election choices continue if I do not make changes
during Open Enrollment?
No, you must actively call the enrollment center to make your 2021
elections.
COBRA Continuation Coverage
When you or any of your dependents no longer meet the
eligibility requirements for your employer’s health and welfare
plans, you may be eligible for continued coverage as required by
the Consolidated Omnibus Budget Reconciliation Act of 1986
(COBRA). In the event of divorce, legal separation or change in
dependent status, it is your responsibility to notify human
resources within 60 days for complete COBRA detail requirements.
Your Tax Advantage
Your contributions for medical, dental, vision and FSA benefits are
made on a pre-tax basis. Your taxable income will be reduced
by the amount you contribute for each benefit. You will not pay
income tax on the amount you contribute, thus saving you tax
dollars. The fact that your taxable income will be lowered does
not affect your salary-related benefits, which will continue to be
calculated upon your base earnings before contributions. You may,
however, realize slightly lower Social Security benefits in the future
because of this pre-tax feature.
4
BENEFITS AT-A-GLANCE
We take pride in offering a benefits program which provides flexibility for the diverse and changing needs of our
employees. The following is an overview of the benefits provided to eligible employees and their dependents.
Benefit Plan Options
4 Plans Options (New HSA Plan)
Medical/Rx Insurance • BCN HMO HRA 1,500
Blue Cross Blue Shield of Michigan • BCN HMO 4,000
(BCBSM) • BCBS Simply Blue PPO 500
Blue Care Network (BCN) • BCBS Simply Blue QHDP PPO 2,000
• Health Savings Account (HSA) via Health Equity
2 Plans Options
Dental Insurance
• Delta DHMO
Delta Dental (New Carrier)
• Delta Dental PPO
Voluntary Vision Insurance Enhanced Benefits
NVA (New Carrier) • $150 frame and contact allowance
Basic Life / AD&D Insurance Employer Paid
Mutual of Omaha (New Carrier) • $10,000 Benefit
Voluntary Benefit - 100% Employee Paid
Voluntary Term Life Insurance • Coverage up to $500,000
Mutual of Omaha (New Carrier) • Guaranteed Issue (GI) increased to $250,000
• TRUE Open Enrollment for all employees with GI
Voluntary Benefit - 100% Employee Paid
• Spouse: Coverage up to $250,000 or 100% of employee amount
Voluntary Dependent Term Life Insurance
• Guaranteed Issue (GI) increased to $50,000
Mutual of Omaha (New Carrier)
• TRUE Open Enrollment for all employees with GI
• Child(ren): Coverage $5,000 or $10,000
Voluntary Benefit - 100% Employee Paid
Voluntary Short Term Disability • 60% of weekly earnings
Mutual of Omaha (New Carrier) • Maximum weekly benefit of $1,000
• TRUE Open Enrollment for all employees
Voluntary Benefit - 100% Employee Paid
Voluntary Long Term Disability • 60% of monthly earnings
Mutual of Omaha (New Carrier) • Maximum monthly benefit of $5,000
• TRUE Open Enrollment for all employees
Health Care:
Flexible Spending Account • Annual Max of $2,000 tax-free for eligible health care expenses
iSolved (New Vendor) Dependent Care:
• Annual Max of $5,000 tax-free for eligible day care expenses
100% CONFIDENTIAL SUPPORT
Employee Assistance Program (EAP)
• 24/7 services to support you and your family
Mutual of Omaha (New Carrier)
• Legal/Financial, Substance abuse, grief and loss, stress manage
Voluntary Benefit - 100% Employee Paid
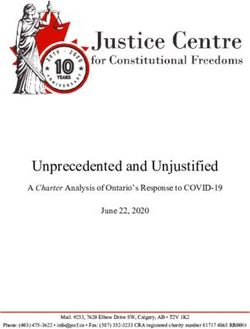
Voluntary Accident Insurance
• Pays a set benefit amount based on the type of injury
UNUM
• Wellness Benefit
Voluntary Whole Life Insurance Voluntary Benefit - 100% Employee Paid
UNUM • Earns cash value
Voluntary Benefit - 100% Employee Paid
Voluntary Hospital Indemnity Insurance
• Pays a set benefit amount
UNUM
• Wellness Benefit
Voluntary Benefit - 100% Employee Paid
Pet Insurance New Offering • 2 levels of benefit offerings
Nationwide • My Pet Protection
• My Pet Protection with Wellness
5
MEDICAL PLAN OPTIONS
Gardner-White Furniture offers four medical options with different benefit levels so that you may select the
option that best meets the needs of you and your family.
• BCN HMO HRA 1,500
• BCN HMO 4,000
• BCBS Simply Blue PPO 500
• BCBS Simply Blue QHDP PPO 2,000
• Health Savings Account (HSA) via Health Equity
HMO Specifics (Only available to Michigan residents)
• An HMO utilizes a network of participating doctors and hospitals.
• Coverage is limited to use of in-network providers except in the case of an emergency.
• You must pick a primary care physician (PCP) and this doctor coordinates all of your health care services.
• Females using this option may select a PCP as well as an OB/GYN and are not required to obtain referrals for
routine OB/GYN services.
• If you need to see a specialist, your PCP must give you a referral to a specialist within the network. If you
see a specialist without obtaining a referral, you will either have no benefits for that service or have a
reduced benefit.
• To find an HMO provider, go to www.bcbsm.com or call the phone number on the back of your ID card.
PPO Specifics
• Benefits are provided through a Preferred Provider Organization (PPO), where a network of hospitals and
doctors are available for your use.
• If you use the network, you will receive the highest level of benefits offered by the PPO.
• Although the network is available, you are not required to use it. You always have the complete freedom to
select any provider whenever you need care. However, the out-of-network benefits are lower and your
out-of-pocket costs will be higher.
• This option does not require any referrals to see a specialist.
• To find a PPO provider, go to www.bcbsm.com or call the phone number on the back of your ID card.
Elections
You may elect medical coverage for yourself; you and your
spouse; you and child(ren); or for your entire family.
Contributions
You and Gardner-White Furniture share in the cost of
coverage. Please see the ADP benefit portal for
information on your contributions.
6
WELLNESS PROGRAM
Gardner-White Furniture is continuing their wellness program incentive for the 2021 plan year.
The below will explain the requirements for both the member and any applicable spouse. In order to qualify for
the incentive, both items must be completed. You and your spouse are eligible for two separate rewards.
Wellness Requirements
• Schedule and obtain your annual physical with your Primary Care Physician. Ask him or her to complete the
2021 Annual Wellness Incentive Form. The 2021 Annual Wellness Incentive Form can be found on the ADP
benefits portal.
• Go to www.bcbsm.com and log in as a member and complete your Health Risk Assessment. You and your
spouse will each need separate logins due to HIPAA. Your results are completely confidential.
In order to qualify for the incentive, both the 2021 Annual Wellness Incentive Form and the BCBSM/BCN Health
Risk Assessment must be completed within 90 days of your new hire benefits eligibility (or by July 1, 2021 for
open enrollment).
Incentive
Each employee and their applicable spouse has the opportunity to earn a $100 gift card. The potential combined
gift card for both employee and spouse is $200. Please keep in mind in order to qualify for the gift card, you must
complete both the Health Assessment as well as have your Primary Care Physician complete the 2021 Annual
Wellness Incentive Form within the specified time frame.
Please note: The gift card is a taxable benefit and must be reported as income at the end of the year under your
W2 earnings.
NON-SMOKING INCENTIVE
Gardner-White Furniture will continue to provide the non-tobacco incentive contribution rates for 2021.
Gardner-White offers a wellness incentive in the form of reduced weekly employee contributions if you and your
spouse are both non-tobacco users.
Blue Cross Blue Shield and Blue Care Network offer resources to assist you on your tobacco free journey.
To qualify as a non-tobacco user, you must be tobacco free for the last 12 months.
All non-tobacco members will receive the reduced contributions as of 4/1/2021 (or your initial effective date for
new hires), however, you must confirm and verify that you are a non-tobacco user at the time of your enrollment.
If the required documentation is not received within 30 days of your effective date, your payroll deductions will
change to the standard contribution. In addition, if a member ceases to actively participate in a tobacco
cessation program throughout the year they will move back to the standard contribution rate.
Please be advised that any reporting and information obtained in regards to a member’s participation status will
be used only for the purposes of certifying willingness to comply and will be kept completely confidential.
7
MEDICAL HMO OPTIONS – BLUE CARE NETWORK (BCN)
Both Blue Care Network HMO Plans will renew and accumulate the deductible and annual out-of-pocket
maximum on a plan year basis. This means that all deductibles and out-of-pocket maximums will restart as of
April 1 each year.
BLUE CARE NETWORK BCN HMO HRA $1,500 BCN HMO $4,000
Deductible $4,000 per member $4,000 per member
(Plan Year 4.1.2021 - 3.31.2022) $8,000 per family $8,000 per family
$1,500 per member $4,000 per member
Member Deductible Responsibility
$3,000 per family $8,000 per family
$6,350 per member $6,350 per member
Annual Out-of-Pocket Maximum
$12,700 per family $12,700 per family
Lifetime Dollar Maximum None None
Primary Care Visit $20 copay $20 copay
Specialist Visit $40 copy after deductible $40 copy after deductible
Preventive Care/Screening/ 100% covered; 100% covered;
Immunization deductible does not apply deductible does not apply
Diagnostic Test (x-ray, blood work) 80% after deductible 80% after deductible
Imaging (CT/PET Scans, MRIs) $150 copay after deductible $150 copay after deductible
Emergency Room Care $150 copay after deductible $150 copay after deductible
Urgent Care $50 copay $50 copay
Online Visit $20 copay $20 copay
Prescription Drugs
Tier 1A - Value Generics $6 copay $6 copay
Tier 1B - Generics $40 copay $40 copay
Tier 2 - Preferred Brand $60 copay $60 copay
Tier 3 - Non-Preferred Brand $80 copay $80 copay
Tier 4 - Preferred Specialty 20% coinsurance (max $200) 20% coinsurance (max $200)
Tier 5 - Non-Preferred Specialty 20% coinsurance (max $300) 20% coinsurance (max $300)
What is an HRA?
HRA’s are health care accounts funded by your employer to help cover employees’ out-of-pocket costs when they
receive health care services.
• Member carry a single medical ID card with a BCN HMO - HRA Designation
• A continuous care process that is seamless for HRA and medical services
• Hassle-free coverage with no reimbursement paperwork
• You receive a single Explanation of Benefits statement that tracks your deductible and coinsurance
obligations and your HRA balances
• You can view your balances online at www.bcbsm.com through Member Secured Services
• The plan utilizes the same extensive BCN provider network.
BCN HMO Plan Deductible Your Deductible Deductible
Requirement Responsibility BCN HRA Reimburses
(Employer Funded Account)
$4,000 Single/$8,000 Family $1,500 Single/$3,000 Family Up to $2,500 Single/$5,000 Family
As a reminder, the BCN Buy-Down HMO does not include the HRA aspect and truly does have a $4,000 Single/
$8,000 Family Deductible.
8
MEDICAL PPO OPTIONS
BLUE CROSS BLUE SHIELD OF MICHIGAN (BCBSM)
Blue Cross Blue Shield Simply Blue PPO plan elections are effective April 1, 2021, however the deductibles and
annual out-of-pocket maximums will accumulate on a calendar year basis (January 1 - December 31).
Simply Blue QHDHP
BCBSM Simply Blue PPO $500
PPO $2,000 with HSA
Deductible $500 per member $2,000 per member
(1.1.2021 - 12.31.2021) $1,000 per family $4,000 per family
$1,500 per member
Annual Coinsurance Maximum None
$3,000 per family
Annual Out-of-Pocket Maximum $8,150 per member $4,000 per member
(includes deductibles, coinsurance and copays) $16,300 per family $8,000 per family
Lifetime Dollar Maximum None
Primary Care Visit $20 copay 80% after in-network deductible
Specialist Visit $20 copay 80% after in-network deductible
100% covered;
Online Visit $20 copay
deductible does not apply
Preventive Care/Screening/ 100% covered;
80% after in-network deductible
Immunization deductible does not apply
Diagnostic Test (x-ray, 80% coinsurance after in-network
80% after in-network deductible
blood work) deductible
80% coinsurance after in-network
Imaging (CT/PET scans, MRIs) 80% after in-network deductible
deductible
Emergency Room Care $150 copay 80% after in-network deductible
Urgent Care $20 copay 80% after in-network deductible
Prescription Drugs
$15 copay after deductible
$15 copay for 30-day supply; for 30-day supply;
Generic
$30 copay for 90-day supply $30 copay after deductible
for 90-day supply
$30 copay after deductible
$30 copay for 30-day supply; for 30-day supply;
Preferred Brand-Name Drugs
$60 copay for 90-day supply; $60 copay after deductible
for 90-day supply;
$60 copay after deductible
Non Preferred Brand-Name $60 copay for 30-day supply; for 30-day supply;
Drugs $120 copay for 90-day supply $120 copay after deductible
for 90-day supply
*Out-of-Network deductibles and coinsurance are higher when utilizing out-of-network services. Refer to the
Summary Benefits of Coverage for details.
Embedded Deductible: Under family coverage, the deductible is the individual deductible for each covered
person. The Simply Blue PPO 500 plan has an embedded deductible.
Aggregate Deductible: The total family deductible must be paid out-of-pocket before the insurance begins
paying for services. The Simply Blue QHDHP PPO $2000 with HSA plan has an aggregate deductible.
9
HEALTH SAVINGS ACCOUNT (HSA)
A Health Savings Account (HSA) is a tax advantaged medical savings account designed to help individuals pay for
their health care. Gardner White partners with Health Equity.
Who is Eligible for an HSA?
To qualify for an HSA, eligible individuals must meet the following requirements:
• You must be covered under a Qualified High Deductible Health Plan on the first day of the month
• You have no other health coverage (that is not an QHDHP)
• You are not enrolled in Medicare
• You cannot be claimed as a dependent on another person’s income tax return
The Benefits of an HSA
• You can claim a tax deduction for contributions that you make to
your HSA
• HSA distributions may be tax-free if you use them to pay for
qualified medical expenses
• The interest in your account are tax-free
• An HSA is “Portable” so it stays with you even if you change jobs,
become unemployed or retire
How Much Can You Contribute to Your HSA for 2021?
2021 Contributions
Individual $3,600
Family $7,200
55 Years or Older Additional $1,000
10BLUE MEMBER SECURED SERVICES
You and your family members can manage your health and health plan online at bcbsm.com.
Register for Member Secured Services to access all of our online services.
Registering is easy. Here’s how:
• Visit bcbsm.com
• Click on the I am a Member tab
• Click on Register
• Follow the registration steps that appear on the screen
If you are registering for the first time, you will be asked a few brief questions to verify your identity. This security
step is required because Member Secured Services offers you personalized online services that contain
protected health information. We are committed to protecting your privacy.
If you are the Blues subscriber on the account, you will also be given the opportunity to “go green” and receive
your Explanation of Benefit Payments statements electronically.
Once you register you will be able to:
• Review you Explanation of Benefit Payments
statements online. We’ll send you an email when
each statement becomes available. In addition to
viewing the statements online, you can also save
them as a PDF.
• View detailed claim and benefit information.
• Access your pharmacy information.
• Take an interactive health assessment and receive a
lifestyle score and tailored action plan.
• Participate in online health coaching programs so
you can achieve health goals identified by your
health assessment.
• Access extensive, up-to-date health content,
including multimedia components like podcasts and
videos.
• Find and compare doctors and hospitals based on
factors most important to you, like cost and quality.
• Save money on the healthy products and services
you use everyday through our member savings
programs, Health Blue XtrasSM and Blue365®.
All features may not be available, depending on your plan.
Questions?
For Web registration or access help, call 888-417-3479.
For benefit, eligibility or claims information, call the
Customer Service number on the back of your BluesID
card.
11ONLINE TELEMEDICINE VISITS
When you use Blue Cross Online VisitsSM (previously called 24/7 online health care), you will have access to
online medical and behavioral health services anywhere in the US.
You can rest assured knowing you and your covered family members can see and talk to:
• A doctor for minor illnesses such as a cold, flu or sore throat when your primary care doctor is not
available.
• A behavioral health clinician or psychiatrist to help work through different challenges such as anxiety,
depression and grief. (Behavioral health visits are available by appointment only.)
While online health care should not replace your relationship with your primary care physician, it can be
invaluable when:
• Your doctor is not available
• You can not leave home or your workplace.
• You are on vacation or traveling for work.
• You are looking for affordable after-hours care.
How do I get started?
Start by doing one of the following:
• Mobile - Download the BCBSM Online Visits app
• Web - Visit bcbsmonlinevisits.com
• Phone - Call 844-606-1608
If you are new to online visits, you will need to register with your Blue Cross or Blue Care Network health
plan information.
Share information with your primary care physician
To ensure that your primary care physician knows about all of your
medical care, let them know when you use online health care. At the
end of your visit, check the box to share your visit summary report with
your family doctor or other health care providers.
How much does it cost?
For medical services, an online visit is based on your office visit
cost share. Costs for behavioral health services vary depending
on the type of provider and service received. You will be charged
using your existing outpatient behavioral health benefits.
Questions?
For questions regarding online health care, contact:
844-606-1608
bcbsmonlinevisits.com
12DENTAL
Gardner-White Furniture provides you with a choice of two different dental options through Delta Dental.
• Delta Dental PPO
• Delta Dental DHMO
To find providers near you, refer to the network directory online at www.deltadentalmi.com or call 800-524-0149.
DHMO
With a Delta Dental DHMO plan, you enjoy negotiated discounts from network dentists. You pay a fixed copay
for each covered service. Out of network dentists are not covered. This plan also features no annual
maximum.
PPO
Through the PPO, you are not required to use a network provider – you have freedom to select any dentist.
However, benefits are highest if you receive care from a PPO network provider in the Delta Dental PPO network.
Using a PPO dentist is the best way to maximize your dental benefits as these dentists agree to accept the PPO
network pre-negotiated fee and are prohibited from billing you for amounts in excess of this fee. You are still
responsible for any applicable employee copayment based on the type of service performed.
Delta Premier
Delta Premier dentists are not part of the PPO network, however Premier dentists agree to adhere to Delta Dental
processing policies and are prohibited from billing a patient above the pre-negotiated fee for the Premier
network. The pre-negotiated fee under the Premier network may be higher than the PPO network, potentially
increasing your out-of-pocket expense.
Out-of-Network (Nonparticipating dentists)
If you use a non-participating provider you may be balance billed for up to the actual billed amount, even when
it exceeds the amount Delta Dental approves. Using an out-of-network dentist can significantly increase your
out-of-pocket expense.
DELTA DENTAL DHMO DELTA DENTAL PPO
You are only covered if you
What’s the most You may go to any dentist, however those who
go to a dentist who belongs
cost-effective way to use belong to the Delta Dental - Michigan network will
to the Delta Dental - HMO
dental insurance? be most cost effective.
(MI) network.
PPO™ Premier® Non-Participating
Dentist Dentist* Dentist*
$25 single $25 single
Calendar year deductible None None
$75 family $75 family
Calendar Year Maximum
Unlimited $1,500
Benefit
Lifetime Orthodontia
Not Applicable $1,500
Maximum
Office Visit Co-pay (one
office visit may cover $0 N/A N/A N/A
multiple services)
Preventive Care Refer to the fee schedule 100% 100% 100%
Basic Care Refer to the fee schedule 80% 80% 80%
Major Care Refer to the fee schedule 50% 50% 50%
Orthodontia up to age 19 Refer to the fee schedule 50% 50% 50%
13DENTAL Delta Dental Plan EPO 32
MEMBER COPAYMENT SCHEDULE
Delta Dental DHMO Fee Schedule CDT-202 1
DIAGNOSTIC SERVICES D2980 Crown repair, by report $70
C L I N I C A L O RA L EV A L U A TI O N S R E S I N RE S TO R A T IO N S D2981 Inlay repair $70
D0120 Oral examination, periodic $0 D2330 1 surface, anterior $39 D2982 Onlay repair $70
D0140 Oral examination, limited, problem $0 D2331 2 surfaces, anterior $48
focused (emergency) D2332 3 surfaces, anterior $57 ENDODONTICS
D0145 Oral evaluation for patients under $0 D2335 Involving incisal angle or 4 or more $72 P U LPO T OM Y
age 3 and counseling with primary surfaces, anterior D3220 Therapeutic pulpotomy $48
caregiver D2390 Crown, anterior $60 D3221 Pulpal debridement, primary and $46
D0150 Oral examination, comprehensive $0 D2391 1 surface, posterior $45 permanent teeth
evaluation D2392 2 surfaces, posterior $59
D0160 Oral examination, detailed and $0 D2393 3 surfaces, posterior $72 R O O T CA N A L TH ER A P Y
extensive evaluation, problem D2394 4 or more surfaces, posterior $88 D3310 Anterior (excludes final restoration) $201
focused, by report D3320 Premolar (excludes final restoration) $239
D0180 Oral examination, comprehensive $0 R E ST O R A T IO N S 1
I N L A Y / O N LA Y D3330 Molar tooth (excludes final $295
periodontal evaluation restoration)
D2510 Inlay, metallic, 1 surface $252
D0190 Screening of a patient $0 D3346 Retreatment, anterior $220
D2520 Inlay, metallic, 2 surfaces $265
D2530 Inlay, metallic, 3 or more surfaces $279
W h e n a n y e x a m is p e r f o r m e d b y a s pe c i a l i s t , t h e r e is D3347 Retreatment, premolar $268
D2542 Onlay, metallic, 2 surfaces $292
a $1 2 c op a ym e nt .
D2543 Onlay, metallic, 3 surfaces $302 D3348 Retreatment, molar $326
D2544 Onlay, metallic, 4 or more surfaces $313
R A D I O G R AP H S
D2610 Inlay, porcelain/ceramic, 1 surface $256 P E R I AP I C A L S E R VIC E S
D0210 Intraoral, complete series (includes $0
D2620 Inlay, porcelain/ceramic, 2 surfaces $268 D3410 Apicoectomy/periradicular surgery - $173
bitewings)
D2630 Inlay, porcelain/ceramic, 3 or more $281 anterior
D0220 Intraoral, periapical first film $0
surfaces D3421 Apicoectomy/periradicular surgery - $186
D0230 Intraoral, periapical each addt'l film $0 premolar, first root
D2642 Onlay, porcelain/ceramic, 2 surfaces $311
D0240 Intraoral, occlusal $0 D3425 Apicoectomy/periradicular surgery - $207
D2643 Onlay, porcelain/ceramic, 3 surfaces $321
D0270 Bitewing, 1 film $0 molar, first root
D2644 Onlay, porcelain/ceramic, 4 or more $332
D0272 Bitewing, 2 films $0 D3426 Apicoectomy/periradicular surgery - $74
surfaces
D0273 Bitewing, 3 films $0 each additional root
D2650 Inlay, resin-based, 1 surface $220
D0274 Bitewing, 4 films $0 D3430 Retrograde filling - per root $49
D2651 Inlay, resin-based, 2 surfaces $232
D0277 Bitewing, vertical, 7 to 8 films $0
D2652 Inlay, resin-based, 3 or more surfaces $245
D0330 Panoramic film $0 PERIODONTIC SERVICES
D2662 Onlay, resin-based, 2 surfaces $257
S U R G I C A L S E R V ICE S
D2663 Onlay, resin-based, 3 surfaces $267 D4210 Gingivectomy or gingivoplasty – 4 or $117
T E S T S & L A B O R ATO R Y
D2664 Onlay, resin-based, 4 or more $277 more teeth per quadrant
D0460 Pulp vitality $0
surfaces D4211 Gingivectomy or gingivoplasty – 1 to $82
D0486 Accession of brush biopsy sample, $0
microscopic exam, prep and written 3 teeth per quadrant
C R O W N S - S IN G L E R E S T O RA T I ON ON L Y 1
report D4240 Gingival flap procedure, includes root $159
D2710 Resin (indirect) $229 planing – 4 or more teeth per quadrant
D0999 Diagnostic procedure - unspecified, $0
by report D2720 Resin with high noble metal $317 D4241 Gingival flap procedure, includes root $111
D2721 Resin with predominantly base metal $279 planing, 1 to 3 teeth per quadrant
PREVENTIVE D2722 Resin with noble metal $298 D4245 Apically positioned flap $185
D E N T A L P R OP H Y L A X I S ( c l ea n i n g ) D2740 Porcelain/ceramic $345 D4249 Clinical crown lengthening $141
D1110 Prophylaxis – adult $0 D2750 Porcelain fused to high noble metal $327 D4260 Osseous surgery – 4 or more teeth $233
D1120 Prophylaxis – child $0 D2751 Porcelain fused to predominantly $289 per quadrant
base metal D4261 Osseous surgery – 1 to 3 teeth per $148
F L U O R I D E T RE A TM E N T D2752 Porcelain fused to noble metal $308 quadrant
D1206 Topical fluoride varnish - child $0 D2753 Porcelain fused to titanium and $327
D1208 Topical application of fluoride $0 titanium alloys N O N -S U R G I CA L S ER V I C E S
D2780 3/4 cast high noble metal $303 D4341 Periodontal scaling and root planing – $72
O T H E R P R EV E N TIV E SE R V I C ES D2781 3/4 cast predominantly base metal $268 4 or more teeth per quadrant
D1351 Sealant (per tooth) $0 D2782 3/4 cast noble metal $284 D4342 Periodontal scaling and root planing – $45
D1353 Sealant repair (per tooth) $0 D2783 3/4 porcelain/ceramic $337 1 to 3 teeth per quadrant
D2790 Full cast high noble metal $322 D4346 Scaling in the presence of $0
S P A CE MA I N TA I N ER S D2791 Full cast predominantly base metal $284 inflammation
D1510 Fixed, unilateral – per quadrant $0 D2792 Full cast noble metal $303 D4355 Full mouth debridement to enable $51
D1516 Fixed, bilateral, maxillary $0 D2794 Titanium $322 comprehensive evaluation and
D1517 Fixed, bilateral, mandibular $0 diagnosis
D1520 Removable, unilateral – per quadrant $0 O T H E R RE S TO R A TI V E SE R V I CE S D4910 Periodontal maintenance $46
D1526 Removable, bilateral, maxillary $0 D2910 Recement onlay or partial coverage $30
D1527 Removable, bilateral, mandibular $0 restoration PROSTHODONTICS (Removable)2
D1551 Recement or rebond bilateral – $0 C O M P LE T E DE N TU R E S
D2915 Recement cast or prefabricated post $30
maxillary and core D5110 Denture - complete, maxillary $120
D1552 Recement or rebond bilateral – $0 D2920 Recement crown $30 D5120 Denture - complete, mandibular $120
mandibular D2930 Crown - prefabricated stainless steel, $83 D5130 Denture - immediate, maxillary $432
D1553 Recement or rebond – unilateral – per $0 primary D5140 Denture - immediate, mandibular $432
quadrant D2931 Crown - prefabricated stainless steel, $83
D1556 Removal, fixed unilateral – per $0 permanent P A R T IA L D E NT U RE S
quadrant D2932 Crown - prefabricated resin $95 D5211 Maxillary, resin base $332
D1557 Removal, fixed bilateral – maxillary $0 D2933 Crown - prefabricated stainless $111 D5212 Mandibular, resin base $332
D1558 Removal, fixed bilateral - mandibular $0 steel with resin window D5213 Maxillary, cast metal framework with $445
D1575 Distal shoe – fixed, unilateral – per $0 D2940 Sedative filling $33 resin denture base
quadrant D2950 Crown buildup (substructure) $83 D5214 Mandibular, cast metal framework $445
including any pins with resin denture base
RESTORATIVE PROCEDURES D2951 Pin retention - per tooth, in addition $15 D5221 Maxillary, immediate, resin base $365
A M A LG AM R ES T OR A T I O NS to restoration D5222 Mandibular, immediate, resin base $365
D2140 1 surface $31 D2952 Post and core in addition to crown, $111 D5223 Maxillary, immediate, cast metal $490
D2150 2 surfaces $38 indirectly fabricated framework with resin denture base
D2160 3 surfaces $46 D2954 Prefabricated post and core in $99 D5224 Mandibular, immediate, cast metal $490
D2161 4 or more surfaces $56 addition to crown framework with resin denture base
D2971 Addt’l procedures to construct new $65 D5225 Maxillary partial denture – flexible $452
crown under existing partial denture base (including retentive/clasping
14DENTAL
Delta
DeltaDental
DentaDHMO
l EPO Fee
PlanSchedule
32 continued
materials, rests, and teeth) D5863 Overdenture, complete maxillary $159 D7140 Extraction, erupted tooth or exposed $38
D5226 Mandibular partial denture – flexible $452 D5864 Overdenture, partial maxillary $159 root
base (including retentive/clasping D5865 Overdenture, complete mandibular $159
materials, rests, and teeth) D5866 Overdenture, partial mandibular $159 S U R GI C A L E XT R AC T I O N S
D5282 Removable unilateral partial denture – $223 D7210 Surgical removal of erupted tooth $76
one piece cast metal (including PROSTHODONTICS (Fixed)1 D7220 Removal of impacted tooth – soft $92
retentive/clasping materials, rests, BRIDGE P O N T IC S (P e r U n i t ) tissue
and teeth), maxillary D6210 Cast high noble metal $300 D7230 Removal of impacted tooth – partially $125
D5283 Removable unilateral partial denture – $223 D6211 Cast base metal $286 bony
one piece cast metal (including D6212 Cast noble metal $292 D7240 Removal of impacted tooth – $146
retentive/clasping materials, rests, completely bony
D6240 Porcelain fused to high noble metal $313
and teeth), mandibular D7241 Removal of impacted tooth – $184
D6241 Porcelain fused to base metal $292
D5284 Removable unilateral partial denture – $223 completely bony with complications
D6242 Porcelain fused to noble metal $302
one piece flexible base (including D7250 Surgical removal of residual roots $80
D6243 Porcelain fused to titanium and $313
retentive/clasping materials, rests,
titanium alloys
and teeth) – per quadrant
D6250 Resin with high noble metal $288 O T H E R S U R G I CA L P R O C E DU R E S
D5286 Removable unilateral, one piece resin $223
D6251 Resin with base metal $274 D7286 Biopsy of oral tissue – soft $46
(including retentive/clasping
D6252 Resin with noble metal $280 D7288 Brush biopsy $35
materials, rests, and teeth) – per
quadrant
F I X E D B R I D G E RE TA I N E R S – I N L A Y S/O N L A Y S A L V E O L OP L A S T Y ( S u r g i c a l P r e p a r a t io n o f R i d g e f o r
A D J U S TM E NT T O D E N T U RE S D6545 Retainer - cast metal for resin bonded $87 Dentures )
D5410 Complete, maxillary $25 fixed prosthesis D7310 In conjunction with extractions, 4 or $73
D6548 Retainer - porcelain/ceramic for resin $87 more teeth or spaces per quadrant
D5411 Complete, mandibular $25
bonded fixed prosthesis D7311 In conjunction with extractions, 1 to 3 $45
D5421 Partial, maxillary $25
D6549 Retainer – resin for resin bonded fixed $87 teeth or spaces per quadrant
D5422 Partial, mandibular $25
prosthesis D7320 Not in conjunction with extractions, 4 $80
D6600 Inlay, porcelain/ceramic, 2 surfaces $287 or more teeth or spaces per quadrant
R E P A I RS T O C OM PL E T E D EN T U RE S
D6601 Inlay, porcelain/ceramic, 3 or more $296 D7321 Not in conjunction with extractions, 1 $48
D5511 Repair broken complete denture base, $58 surfaces to 3 teeth or spaces per quadrant
mandibular D6602 Inlay, cast high noble metal, 2 $279
D5512 Repair broken complete denture base, $58 surfaces
E X C I S I ON O F BO NE T I SS U E
maxillary D6603 Inlay, cast high noble metal, 3 or more $292
D7471 Removal of lateral exostosis $143
D5520 Replace missing or broken teeth $48 surfaces
D7472 Removal of torus palatinus $143
(each tooth) D6604 Inlay, cast predominantly base metal, $252
2 surfaces D7473 Removal of torus mandibularis $143
R E P A I RS T O PA R T IA L D E N TU R E S D6605 Inlay, cast predominantly base metal, $265
3 or more surfaces S U R G I C A L I N C I SI ON
D5611 Repair resin partial denture base, $58
D6606 Inlay, cast noble metal, 2 surfaces $265 D7510 Incision and drainage of abscess – $49
mandibular
D6607 Inlay, cast noble metal, 3 or more $279 intraoral soft tissue
D5612 Repair resin partial denture base, $58 surfaces
maxillary D7922 Placement of intra-socket biological $0
D6608 Onlay, porcelain/ceramic, 2 surfaces $231 dressing to aid in homeostasis or clot
D5621 Repair cast partial framework, $83 D6609 Onlay, porcelain/ceramic, 3 or more $301 stabilization – per site
mandibular surfaces
D5622 Repair cast partial framework, $83 D6610 Onlay, cast high noble metal, 2 $224
O T H E R RE PA I R P RO C E D U RE S
maxillary surfaces
D7961 Buccal/labial frenectomy $89
D5630 Repair or replace broken clasp (per $83 D6611 Onlay, cast high noble metal, 3 or $292
(frenulectomy)
tooth) more surfaces
D7962 Lingual frenectomy (frenulectomy) $89
D5640 Replace broken tooth (each) $48 D6612 Onlay, cast predominantly base metal, $252
D7963 Frenuloplasty $89
D5650 Add tooth to existing partial denture $61 2 surfaces
D5660 Add clasp to existing partial denture $83 D6613 Onlay, cast predominantly base metal, $265
ADJUNCTIVE GENERAL SERVICES
(per tooth) 3 or more surfaces
U N C L A SS I F I E D T RE A T ME N T
D5670 Replace all teeth and acrylic on cast $249 D6614 Onlay, cast noble metal, 2 surfaces $292
metal framework (maxillary) D9110 Palliative (emergency) treatment of $30
D6615 Onlay, cast noble metal, 3 or more $302
dental pain – minor procedure
D5671 Replace all teeth and acrylic on cast $249 surfaces
metal framework (mandibular)
P R O F E S SI O NA L CO N S U L TA T I ON
BRIDGE R E TA I NE RS – C R O W N S
D E N T U RE R E BA S E P R O CE D U R ES D9310 Consultation by dentist other than $20
D6720 Resin with high noble metal $317
D5710 Complete maxillary denture $159 requesting dentist
D6721 Resin with base metal $279
D5711 Complete mandibular denture $159
D6722 Resin with noble metal $298 P R O FE S SI O NA L V IS I T S
D5720 Maxillary partial denture $162
D6750 Porcelain fused to high noble metal $327 D9440 Office visit after regularly scheduled $0
D5721 Mandibular partial denture $162
D6751 Porcelain fused to base metal $289 hours
D E N T U RE R E L IN E P R O C E DU R E S D6752 Porcelain fused to noble metal $308
D5730 Complete maxillary, direct $99 D6753 Porcelain fused to titanium and $327 M I S C E L L AN E OU S S E R V I CE S
titanium alloys D9997 Dental case management – patients $0
D5731 Complete mandibular, direct $99
D6780 3/4 cast high noble metal $317 with special health care needs
D5740 Maxillary partial, direct $93
D6781 3/4 cast base metal $279 D9999 Unspecified, by report $50
D5741 Mandibular partial, direct $93
D6782 3/4 cast noble metal $298
D5750 Complete maxillary, indirect $130
D5751 Complete mandibular, indirect $130
D6784 3/4 titanium and titanium alloys $317 ORTHODONTICS3
D6790 Full cast high noble metal $322 R E C O R D S (s o l e l y fo r o r t h o d o n t i c p u r p o s e s )
D5760 Maxillary partial, indirect $130
D6791 Full cast base metal $284 D0340 Cephalometric film $0
D5761 Mandibular partial, indirect $130
D6792 Full cast noble metal $303 D0350 Oral/facial photographic images $0
O T H E R RE MO V A BL E P R OS T H ET I C SE R V I C ES D0470 Diagnostic casts $0
O T H E R F I X ED P ROS T H E TI C SE R V I C ES
D5820 Interim partial denture (including $148
retentive/clasping materials, rests, D6930 Recement fixed partial denture $42 C O M P RE H EN S I VE O R T H O DO N T I C T RE A T ME N T
and teeth), maxillary D6940 Stress breaker $68 D8070 Transitional dentition $2,100
D5821 Interim partial denture (including $148 D8080 Adolescent dentition $2,100
retentive/clasping materials, rests, ORAL SURGERY D8090 Adult dentition (to age 19) $2,100
and teeth), mandibular E X T R A C T I ON S (S im p l e )
D5850 Tissue conditioning, maxillary $64 D7111 Extraction, coronal remnants – $29
D5851 Tissue conditioning, mandibular $64 primary tooth
11/2020 15VISION
Gardner-White Furniture offers you vision benefits administered by NVA. You may choose to visit a provider
within the NVA network and take advantage of higher benefits coverage, or visit an out-of-network provider of
your choice for a reduced benefit if desired. Keep in mind, when you stay within the network, you will pay less.
To find a provider go to www.e-nva.com.
In- Network Out-of-Network
Exams: Every 12 months
How often can I obtain service? Lenses: Every 12 months
Frames: Every 12 months
Eye exams $0 Up to: $46
Lenses $10 Copay
Single vision lenses Covered 100% Up to: $47
Lined bifocal lenses Covered 100% Up to: $66
Lined trifocal lenses Covered 100% Up to: $85
Lenticular lenses Covered 100% Up to: $125
Lens Options
Polycarbonate - Under age 19 Covered 100% N/A
Solid Tints Covered 100% N/A
Fashion Gradient Tint Covered 100% N/A
Oversized Covered 100% N/A
Frames
Retail Frame Allowance2 Covered up to $150 Up to $47
20% Discount of Frame Balance3 Yes N/A
Contact Lenses Fit/Follow-up1
Standard Daily Wear Covered 100% Up to: $20
Standard Extended Wear Covered 100% Up to: $30
Specialty Wear Covered 100% Up to: $50
Elective4 Covered up to $150 Up to: $105
15% discount on Conventional/ Yes N/A
10% discount on Disposable on
remaining balance5
Medically Necessary6 Covered 100% Up to: $210
1
Only covered if member chooses contact lenses.
2
Includes frames up to $61 every day low price-price point at Walmart/
Sam’s Club locations (if included in the network).
3
Discount does not apply at Walmart/Sam’s Club locations, LensCrafters
or for certain proprietary frame brands or where prohibited by law.
4
$105 every day low price-price point for contact lenses at Walmart/
Sam’s Club locations (if included in the network).
5
Discount does not apply at Walmart/Sam’s Club locations, Cole
corporate locations (if applicable), LensCrafters or Contact Fill or where
prohibited by law. Prohibited by some manufacturers.
6
Prior authorization required from NVA included fitting & follow-up.
Note: if covered participants choose extra options, they are responsible
for the additional cost of the options paid directly to the provider.
16BASIC LIFE AND AD&D
Gardner-White Furniture provides Basic Life and Accidental Death & Dismemberment (AD&D) insurance benefits
to all eligible employees through Mutual of Omaha Life Insurance.
Basic Life
As an active employee of Gardner-White Furniture, you have access to a life insurance policy from Mutual of
Omaha Life Insurance Company.
How much insurance is enough?
When determining how much life insurance you need, think about the expenses you may encounter now and
through every stage of your life. Coverage guidelines and benefits are outlined in the chart below.
BASIC LIFE AND AD&D INSURANCE
You must be actively working a minimum of 30 hours per week to be
Eligibility Requirement
eligible for coverage.
The premiums for this insurance are paid in full by Gardner-White
Premium Payment
Furniture. There is no cost to you for this insurance.
Life Insurance Benefit Amount For You: $10,000
In the event of death, the benefit paid will be equal to the benefit
amount after any age reductions less any living care/accelerated death
benefits previously paid under this plan.
Accidental Death & For You: The Principal Sum amount is equal to the amount of your life
Dismemberment (AD&D) Benefit insurance benefit.
Amount
Living Care/Accelerated 50% of the amount of the life insurance benefit is available to you if ter-
Death Benefit minally ill, not to exceed $5,000.
In addition to basic AD&D benefits, you are protected by the following
benefits:
Additional AD&D Benefits
- Childcare - Child Education - Seat Belt
- Airbag - Spouse Education - Common Carrier
Insurance benefits and guarantee issue amounts are subject to age
reductions:
Age Reductions and Exclusions - At age 70, amounts reduce to 50%
Information about the AD&D exclusions for this plan will be included in
the summary of coverage, which you will receive after enrolling.
17VOLUNTARY LIFE AND AD&D
As an active employee of Gardner-White Furniture, you have access to a life insurance policy from Mutual of
Omaha Life Insurance Company.
How much insurance is enough?
When determining how much life insurance you need, think about the expenses you may encounter now and
through every stage of your life.
Coverage guidelines and benefits are outlined in the chart below.
VOLUNTARY LIFE AND AD&D INSURANCE
You must be actively working a minimum of 30 hours per week to be
Eligibility Requirement
eligible for coverage.
To be eligible for coverage, your dependents must be able to perform
normal activities, and not be confined (at home, in a hospital, or in any
Dependent Eligibility
other care facility), and any child(ren) must be under age 26. In order for
Requirement
your spouse and/or children to be eligible for coverage, you must elect
coverage for yourself.
Premium Payment The premiums for this insurance are paid in full by you.
COVERAGE GUIDELINES
Minimum Guaranteed Issue Maximum
$500,000, in increments of
5 times annual salary, up to
For You $10,000 $10,000, but no more than 5
$250,000
times annual salary
Spouse 100% of employee’s 100% of employee’s
$10,000
benefit, up to $50,000 benefit, up to $250,000
Children 100% of employee’s benefit, up
$5,000 100% of employee’s benefit
to $10,000
BENEFITS
Within the coverage guidelines defined above, you select the amount of
life insurance coverage you want.
This plan includes the option to select coverage for your spouse and
dependent children.
Life Insurance Benefit Amount
Children include those, up to age 26.
In the event of death, the benefit paid will be equal to the benefit
amount after any age reductions less any living care/accelerated death
benefits previously paid under this plan.
For you, your spouse and your dependent child(ren): The Principal Sum
amount is equal to the amount of the life insurance benefit.
Accidental Death &
AD&D coverage is available if you or your dependents are injured or die
Dismemberment (AD&D)
as a result of an accident, and the injury or death is independent of
Benefit Amount
sickness and all other causes. The benefit amount depends on the type
of loss incurred, and is either all or a portion of the Principal Sum.
Age Reductions and Exclusions Insurance benefits and guarantee issue amounts are subject to age
reductions:
- At age 70, amounts reduce to 50%
Spouse coverage terminates when you reach age 70.
18VOLUNTARY SHORT-TERM DISABILITY INSURANCE
As an active employee of Gardner-White Furniture, you have access to a disability income insurance policy from
Mutual of Omaha Life Insurance Company. A disability income insurance policy can help provide security when
you need it, plus give you peace of mind so you can recover faster and get back on the job sooner.
Coverage guidelines and benefits are outlined below.
VOLUNTARY SHORT-TERM DISABILITY
You must be actively working a minimum of 30 hours per week to be
Eligibility Requirement
eligible for coverage.
Premium Payment The premiums for this insurance are paid in full by you.
Elimination Period If you become disabled, there is an elimination period before benefits
are payable. Your benefits begin:
• On the 15th day of your disabling injury.
• On the 15th day of your disabling illness.
Weekly Benefit Your benefit is equivalent to 60% of your before-tax weekly earnings,
not to exceed the plan’s maximum weekly benefit amount less other
income sources.
The premium for your short-term disability coverage is waived while you
are receiving benefits.
Maximum Benefit Period Up to 24 weeks
Maximum Weekly Benefit $1,000
Minimum Weekly Benefit $25
19VOLUNTARY LONG-TERM DISABILITY INSURANCE
As an active employee of Gardner-White Furniture, you have access to a disability income insurance policy from
Mutual of Omaha Life Insurance Company. A lengthy disability can be devastating, and is more common than you
might think. It may lead to a loss of income, independence and financial security. A disability income insurance
policy can help provide security when you need it most. It pays you cash benefits when you’re sick or hurt and
can’t work.
Coverage guidelines and benefits are outlined in the chart below.
VOLUNTARY LONG-TERM DISABILITY
You must be actively working a minimum of 30 hours per week to be
Eligibility Requirement
eligible for coverage.
Premium Payment The premiums for this insurance are paid in full by you.
Elimination Period Your benefits begin on the later of 180 calendar days after the onset of
your disabling injury or illness or the date your short term disability ends.
Monthly Benefit Your benefit is equivalent to 60% of your before-tax monthly earnings,
not to exceed the plan’s maximum monthly benefit amount less other
income sources.
The premium for your long-term disability coverage is waived while you
are receiving benefits.
Maximum Monthly Benefit $5,000
Minimum Monthly Benefit $100
If you become disabled prior to age 62, benefits are payable to age 65,
your Social Security Normal Retirement Age or 3.5 years, whichever
Maximum Benefit Period
is longest. At age 62 (and older), the benefit period will be based on a
reduced duration schedule.
20FLEXIBLE SPENDING ACCOUNT
With an FSA, participants elect an annual contribution amount, up to the IRS maximum, to be deducted from their
paychecks each pay period in equal installments throughout the year. The amount of pay that goes into an FSA
will not count as taxable income, so participants will have immediate tax savings. FSA dollars can be used during
the plan year to pay for qualified expenses and services. Isolved Benefit Services is the plan administrator for the
FSA plan.
• A Health FSA allows reimbursement of qualifying out-of-pocket medical expenses NOT enrolled in the
Simply Blue QHDHP PPO $2,000
• A Dependent Care FSA allows reimbursement of dependent care expenses, such as day care, incurred by
eligible dependents.
With all FSA account types, participants receive access to a secure, easy-to-use web portal and smartphone app
where they can track their account balances and submit requests for reimbursements.
In addition, you will receive a convenient debit card to make it easy to pay for eligible services and products.
When participants use the card, payments are automatically withdrawn from the FSA account, so there are no
out-of-pocket costs and many times they won’t have to submit receipts to verify the purchase.
Health Care FSA
Allows you to pay for medical, dental, vision and other health care expenses that are not covered under any other
plan with pre-tax dollars. The maximum amount you may contribute to your health care FSA is $2,000. Funds are
available on first day of plan year. Plan carefully—Claims must be incurred in the plan year in order to be eligible
for reimbursement.
Dependent Care FSA
A Dependent Care FSA provides pre-tax reimbursement of out-of-pocket expenses related to dependent care. It’s
a great option for employees who have dependent children under the age of 13 who attend day care, afterschool
care or summer day camp, and/or provide care for a person of any age who is claimed as a dependent on the
federal income tax return and who is mentally or physically incapable of caring for himself or herself.
Who is a qualified dependent under the Dependent Care FSA?
• Dependent under the age of 13
• Dependent or spouse of employee who is mentally or physically disabled and whom the employee claims
as a dependent on their federal income tax return
Rollover of Unused Funds
This plan does contains a provision which allows you to rollover unused funds to the next plan year as long as
the balance does not exceed the maximum rollover amount of $550. If you rollover funds it will not decrease
your ability to elect the full plan maximum of $2,000.
Use it or Lose It
IRS regulations specify that the money you contribute to your spending accounts for any plan year may only be
used to reimburse eligible expenses incurred during that year. Any money over the $550 rollover limit remaining
in your account, at the end of the plan year, will be forfeited. iSolved Benefit Services gives a 90-day run out
period which allows you to submit claims from the prior plan year, participants have until June 29, 2022.
21FLEXIBLE SPENDING ACCOUNT
Prepaid Benefits Card
The Prepaid Benefits Card is a special-purpose MasterCard® card that gives participants an easy, automatic
way to pay for eligible health care/benefit expenses. The card lets participants electronically access the pre-tax
amounts set aside in their Flexible Spending Accounts (FSAs).
How does the Benefits Card work?
It works like a MasterCard® card, with the value of your account(s) contribution stored on it. When you have
eligible expenses at a business that accepts MasterCard® debit cards, you simply use the card. The amount of
the eligible purchase will be automatically deducted from your account and the pre-tax dollars will be
electronically transferred to the provider/merchant for immediate payment.
Where can you use the Benefits Card?
You to use the Benefits Cards in participating pharmacies, mail-order pharmacies, discount stores, department
stores and supermarkets that can identify FSA/HRA eligible items at checkout and accept MasterCard® prepaid
cards. You can find out which merchants are participating by visiting the website on the back of the card.
You may also use the card to pay a hospital, doctor, dentist or vision provider that accepts MasterCard®. In this
case, auto-substantiation technology is used to electronically verify the transaction’s eligibility according to IRS
rules. If the transaction cannot be auto substantiated, follow-up will be required.
The iFlex App
You have your phone with you all the time. Why not use the iFlex App to review your account information, take a
photo of the receipt and submit the claim right away?
The iFlex App connects you with the details
• Quickly check available balances 24/7
• Access account details
• View charts summarizing account(s)
• Click to call or email Customer Service
Provides additional time-saving options
• View claims requiring receipts
• Submit medical FSA and HRA claims
• Take a picture of a receipt to submit for a claim
• View HSA transaction details
• Using Expense Tracker, enter medical expense information and support documentation to store for later use
in paying claims via your health benefits website
• Report a lost or stolen debit card
The iFlex App is easy, convenient and secure. Simply login to the app using your same health benefits website
username and password (or follow alternative instructions if provided to you).
Follow these steps to download the iFlex App
1. Visit the iTunes App Store or the Android Market to download the isolved app on your iPhone, iPad or
Android.
2. Once installed, enter the Username and Password to log into your account at
www.isolvedbenefitservices.com
22You can also read