Selecting a fixed combination to improve morbidity/ mortality: the weight of evidence with ASCOT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

European Heart Journal Supplements (2008) 10 (Supplement G), G21–G28
doi:10.1093/eurheartj/sun024
Selecting a fixed combination to improve morbidity/
mortality: the weight of evidence with ASCOT
Downloaded from https://academic.oup.com/eurheartjsupp/article/10/suppl_G/G21/476006 by guest on 23 June 2022
Neil R. Poulter*
International Centre for Circulatory Health, NHLI, Imperial College, London, UK
KEYWORDS The Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure-Lowering Arm was
Hypertension; designed to compare the effects of a standard combination starting with atenolol and
Randomized trial; adding a thiazide as needed and a newer combination starting with amlodipine and
Amlodipine; adding perindopril as needed. Because the newer regimen was associated with a signifi-
Perindopril;
cant reduction in all-cause mortality, the trial was stopped early. Nevertheless, the
Atenolol;
newer regimen was associated with a significantly superior effect on the primary end-
Bendroflumethiazide;
Cardiovascular benefits
point excluding silent myocardial infarction, or including revascularization procedures,
on total coronary events, cardiovascular (CV) mortality, fatal and non-fatal strokes,
unstable angina, total CV events and procedures, new-onset diabetes, and development
of renal impairment. The newer regimen was associated with an average blood pressure
(BP) which was 2.7/1.9 mmHg lower than that of the standard regimen. Although it
seems likely that this BP difference contributed to the superior prevention by the
newer regimen, extensive analyses suggested that other advantages of the newer
regimen contributed to this superiority. This is in keeping with other findings which
suggest that angiotensin-converting enzyme inhibitors may have benefits beyond BP
lowering in relation to coronary heart disease events and that calcium channel blockers
may have benefits beyond BP lowering in relation to stroke protection.
Evidence from randomized trials1,2 are consistent in In this latest European version, calcium channel
showing that the majority of patients with hypertension blockers (CCBs) and diuretics are considered a logical
require at least two blood pressure (BP)-lowering agents combination despite sharing, at least in part, a common
if currently recommended targets are to be reached. mechanism of action. Furthermore, these two agents
Although the vast majority of trials of BP management have, in earlier studies, been shown not to produce
have involved the use of BP-lowering regimens including optimal BP lowering when used in combination.3 Interest-
two or more agents, the choice of the second or third ingly, this combination—logical or not—was recently
agent has usually been unstructured. Hence, the results shown to be in common use, at least in the UK.4
of these trials cannot inform recommendations for In June 2006, the British Hypertension Society (BHS) and
optimal combinations of antihypertensive agents. Advice NICE published the A/CD algorithm—for how best to
is, therefore, based on the theoretical benefits of select- combine drugs to achieve optimal BP control5 (Figure 2).
ing agents, which have complementary rather than over- Each letter refers to a BP-lowering drug class (A, ACE
lapping mechanisms of action. This has given rise to inhibitor or ARB; C, dihydropyridine CCB; D, diuretic),
several similar sets of recommendations for drug combi- and the theory underpinning this approach is that
nations, and recently, the ESH-ESC guidelines have pro- hypertension can be broadly classified as ‘high renin’ or
duced a further version of these earlier models (Figure 1). ‘low renin’. The former is, therefore, best treated by
those drug classes that inhibit the renin–angiotensin
* Corresponding author. Tel: þ44 20 7594 3445; fax: þ44 20 7594 1145. system (A), and the latter by those classes that do not
E-mail address: n.poulter@imperial.ac.uk (C or D).6,7
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008.
For permissions please email: journals.permissions@oxfordjournals.org
G22 N.R. Poulter
In general, younger Caucasian people (,55 years) tend people below age 55 years and so the critical age effects
to have higher renin status than older people (55 years) could not be evaluated and trials, such as VALUE9 and
or black people; hence, the recommended allocation of ASCOT,10 which showed clear differences in BP lowering
drugs for step 1 based on age and race is shown in between A and C drugs and B and C drugs, respectively,
Figure 2. The idea of prescribing initial therapy based on were not included in the analyses. In contrast, more
age has recently been challenged by analyses carried careful evaluation of drug classes used as monotherapy
out by the Blood-Pressure Lowering Treatment Trialists’ across the whole age range is consistent in showing that
Collaboration.8 These analyses suggest that age is not a A and B drugs are less effective with increasing age and
major determinant of BP response to the major antihyper- C and D drugs are less effective with decreasing age.6,7
tensive drug classes. However, the collaboration includes The rationale for steps 2, 3, and 4 in the A/CD algor-
virtually no data to allow true comparisons of monother- ithm are less soundly based and are recommended on
apy by age because, as mentioned earlier, almost all the logical grounds of selecting combinations of agents,
Downloaded from https://academic.oup.com/eurheartjsupp/article/10/suppl_G/G21/476006 by guest on 23 June 2022
trials hitherto have involved extensive mixtures (often which do not have overlapping mechanisms. At first
unstructured) of multiple agents. Once the classes of sight, it seems obvious that two drugs will be more
agents are mixed, age effects would not be expected effective than one drug in lowering BP. However, the
to be apparent. Furthermore, several trials excluded fact that two lower doses of drugs in combination may
be more effective than a full dose of one drug is
perhaps less well established and intuitive. Nevertheless,
best data suggest that adding a second drug (of whatever
class) is more effective than uptitrating monotherapy.11
A striking example supporting this approach was a
recently published comparison of the BP-lowering effects
of each of four drugs at full dose vs. a quarter dose of
the same four drugs in combination in one tablet.12 The
combination of four drugs at quarter dose was far superior
to any of the monotherapy agents at full dose.
Whether the choice of second drug matters in terms
of BP-lowering efficacy is less clear, but a recent
meta-analysis suggests that some combinations produce
more than additive BP-lowering effects whereas others
produce less than additive effects.13 Among those produ-
cing better additive effects are A and C, and A and D drug
classes. These are the two pairs of drug classes rec-
ommended as the second-line approaches in the British
A/CD algorithm (Figure 2).5 Until very recently, A plus C
has been less commonly used than A plus D. However,
two recent studies are likely to impact on current clinical
practice.14,15 Firstly, the STAR study14 showed that in
patients with impaired glucose tolerance, the use of tran-
Figure 1 The ESH-ESC approach to combining antihypertensive drug dolapril and verapamil produced significantly less type 2
Classes.
Figure 2 The NICE/BHS approach to sequencing antihypertensive drug classes.
Fixed combination to improve morbidity/mortality G23
diabetes than losartan and thiazide, during up to 52 and currently under investigation. Note that b-blockers
weeks of follow-up. Perhaps more importantly, the have been relegated to fourth-line agents based on the
ACCOMPLISH trial established that benazapril plus amlo- results of a series of meta-analyses that were consistent
dipine was clearly superior to benazapril plus thiazide in showing this drug class to be inferior to A, C, and D
in terms of preventing all major cardiovascular (CV) drugs in terms of preventing CV events.17,18
events, despite achieving very similar levels of clinical British,19 American,20 and European21 guidelines have
BP reduction.15 It seems likely therefore that an A plus all moved towards recommending the use of fixed
C combination should be preferred to A plus D, except low-dose combinations of drugs. Historically, the use of
where compelling indications and/or side-effects pre- such agents has been considered infra dig, but in light
clude this preference. of the real need for more than one agent for most
The A/CD algorithm has the unique advantage of provid- patients and for several other reasons, it seems a
ing advice on how best to control more severe levels of logical approach that should improve BP lowering. With
this in mind, the American (JNC7)20 and the latest
Downloaded from https://academic.oup.com/eurheartjsupp/article/10/suppl_G/G21/476006 by guest on 23 June 2022
raised BP. For those patients with apparently resistant
hypertension (uncontrolled despite the use of three European guidelines21 formally recommend combination
agents—one of which should be a diuretic), the use of therapy as first-line treatment (Figures 3 and 4).
aldosterone antagonists (e.g. spironolactone 25 mg o.d.) Despite the need to use two or more drugs for BP
appears to provide (albeit based on observational data) control in most patients, trials specifically designed to
dramatic BP-lowering effects.16 Whether other diuretics compare the effects of different combinations of antihy-
would be equally successful in this context is controversial pertensive treatment are relatively rare.
Figure 3 JNC 7: algorithm for the treatment of hypertension.
Figure 4 ESH–ESC: algorithm for the treatment of hypertension.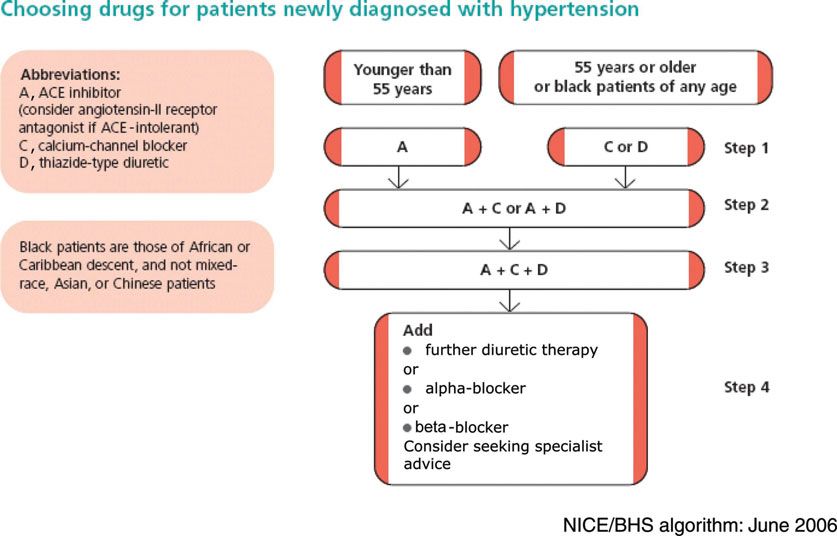
G24 N.R. Poulter
The LIFE trial22 compared an ARB and diuretic with a
b-blocker and diuretic, whereas the VALUE trial10 com-
pared an ARB and diuretic with a CCB and diuretic. More
recently, as described earlier, the ACCOMPLISH trial15 has
reported a comparison of an ACE inhibitor plus thiazide
vs. an ACE inhibitor plus CCB, but the ASCOT trial10 is
almost unique in comparing two different pairs of drug
classes—b-blocker and diuretic vs. CCB and ACE inhibitor.
The results of this trial are discussed in more detail below.
Before the results of the ACCOMPLISH trial, the
preferential choice of ACE inhibition with a CCB has
been proposed for renal protection, for the potential
Downloaded from https://academic.oup.com/eurheartjsupp/article/10/suppl_G/G21/476006 by guest on 23 June 2022
complementary effects of co-administering both drug
classes on the microcirculation and the mesangium.
Once any given drug combination has been identified
as ‘optimal’, the issue of whether the drugs should be Figure 5 The ASCOT-BPLA trial: treatment steps in the two randomized
produced as a fixed-dose combination (FDC) (albeit groups.
potentially with various dose combinations) arises.
There seems to be no reason for FDCs to be considered event within the previous 3 months, fasting triglycerides
poor quality medicine when used for hypertension, .4.5 mmol/L, heart failure, uncontrolled arrhythmias,
anymore than in the fields of respiratory medicine, or any clinically important haematological or biochemical
diabetes, or oncology where the use of such products is abnormality on routine screening.
the norm. Patients were randomized to a regimen based on
Concerns that FDCs are expensive are frequently ill- amlodipine+perindopril or atenolol+bendroflumethiazide
founded in that, for example in the UK, when diuretics and treated according to a pre-specified algorithm outlined
are combined with ARBs or ACE inhibitors, the products in Figure 5. At each follow-up visit, antihypertensive drug
are flat-priced against the RAS-blocker. Furthermore, therapy was titrated to achieve target BPs (,130/
up-titration costs and prescription costs and hence 80 mmHg for diabetic patients and ,140/90 mmHg for all
overall direct costs may be reduced when FDCs are used. other patients).
Although data are limited, evidence suggests that com- Patients with a non-fasting total cholesterol of
pliance with two drugs delivered as an FDC is greater 6.5 mmol/L or less currently untreated with a statin or
than with the two agents provided separately.23,24 fibrate were randomized to atorvastatin 10 mg daily
Hence, it is a reasonable assumption, supported by or matching placebo in the Lipid-Lowering Arm of the
some data, that BP lowering is superior with the use of study (ASCOT-LLA).26 The primary endpoint was fatal
FDCs and hence CV events and thereby indirect health- CHD and non-fatal (including silent) MI.
care costs are reduced.
Currently, these potential benefits of FDCs are under-
utilized in the UK and provide a relatively simple way Results
of improving BP control.
In October 2004, the Data Safety Monitory Board rec-
ommended that the BP-lowering arm (BPLA) of the trial
The ASCOT trial methods should be stopped on the grounds that, compared with
those allocated amlodipine+perindopril therapy, those
The study design, organization, and main results of the allocated the atenolol+thiazide therapy had significantly
study have been published previously.10,25 Patients eli- higher all-cause mortality as well as worse outcomes on
gible for inclusion in ASCOT were men and women aged several secondary endpoints including stroke.
between 40 and 79 years, with either untreated hyper- After a median follow-up of 5.5 years, the CV benefits
tension, defined as systolic BP of 160 mmHg or more associated with allocation to the amlodipine+perindopril
and/or diastolic BP of 100 mmHg or more, or treated regimen are apparent in Figure 5. Having stopped this limb
hypertension with systolic BP of 140 mmHg or more of the study earlier than planned due to benefits in all-
and/or diastolic BP 90 mmHg or more. In addition, the cause mortality, the study had become underpowered to
study population was required to have at least three of evaluate the primary endpoint that was non-significantly
the following additional risk factors for CV disease reduced by 10% (P ¼ 0.105). However, all coronary
(CVD): male sex, age 55 years or older, smoking, type 2 events and the primary endpoint minus silent MI and the
diabetes, peripheral arterial disease, previous stroke or primary endpoint plus coronary revascularizations were
transient ischaemic attack, microalbuminuria or protei- significantly reduced (Figure 6).
nuria, ratio of plasma total cholesterol to HDL cholesterol Despite strenuous efforts to lower BP equally in both
of 6 or higher, or family history of premature coronary limbs of BPLA (and BP was lowered very effectively in
heart disease (CHD). both groups), those allocated the amlodipine+perindopril
Exclusion criteria included previous myocardial infarc- regimen had lower average BP reductions of 2.7/1.9 mmHg
tion (MI), currently treated angina, a cerebrovascular throughout the trial. Analyses were carried out to evaluate
Fixed combination to improve morbidity/mortality G25
Downloaded from https://academic.oup.com/eurheartjsupp/article/10/suppl_G/G21/476006 by guest on 23 June 2022
Figure 6 The ASCOT-BPLA trial: summary of effects of all endpoints.
the vexed question of how far these BP differences explain
the superior CV protection afforded by the amlodipine+
perindopril therapy.27
Differences in CV events between BP-lowering regimens
were adjusted for the combined effect of differences in
BP, weight, heart rate, and biochemical variables, which
appeared during the trial associated with the two
BP-lowering regimens. Adjustment, however, accounted
for only 50% and 40% of the differences in coronary and
stroke events, respectively. BP differences were the
biggest contributor to stroke event differences, but
HDL-cholesterol differences were the biggest contributor
to coronary event differences.
We concluded, therefore, that BP was an unlikely
Figure 7 New-onset diabetes by treatment group in the ASCOT-BPLA trial.
explanation for all the CV advantages of the amlodipine+
perindopril regimen. Subsequently, the CAFE substudy of
in both the UK and Sweden. Compared with the thresholds
ASCOT28 provided interesting data which suggested that
applied by NICE and the relevant Swedish Board, the
the bigger effects of the amlodipine+perindopril
amlodipine+perindopril regimen was found to be cost-
regimen on central BP may have also contributed to the
effective compared with the atenolol+thiazide regimen.
different CV outcomes.
Clearly, the CV effects associated with the
One of the tertiary outcomes of the ASCOT-BPLA trial
amlodipine+perindopril regimen were compared with
was the evaluation of the impact of two regimens on
another active regimen in the ASCOT trial. Hence, the
new-onset diabetes (NOD). The initially reported 31%*
differential beneficial effects of amlodipine+perindopril
reduction in NOD associated with the amlodipine+
are over and above those which can reasonably be
perindopril regimen (Figure 7) was more rigorously
expected to have accrued in the atenolol+thiazide
scrutinized.29 These analyses revealed a 34% reduction
limb by virtue of large BP reductions achieved (27/
in NOD associated with an amlodipine+perindopril
17 mmHg). Therefore, it seems a reasonable assumption
regimen, compared with the atenolol+thiazide
that had the amlodipine/perindopril combination been
regimen. This variable in multiple regression analyses
compared with placebo, even larger and more significant
was the most-powerful protective factor against the
and important impacts on CV events would have accrued
development of NOD in this population.
from the use of this antihypertensive regimen.
Having confirmed the superiority of the newer
BP-lowering regimen, it was critical to evaluate the cost-
efficacy of this regimen. This was addressed in a health- Summary/conclusions/discussion
economic analysis30 of the cost per CV event or procedure
avoided and the cost per quality-adjusted life year gained Despite having the results of more than 30 major morbidity
and mortality trials,31 many outstanding questions relating
*In earlier publication, by error, 30% reduction was mentioned. to hypertension management remain unanswered.
G26 N.R. Poulter
Confusion remains as to optimal first-line therapy and (despite the inevitable tradeoff of a degree of inaccur-
although it may seem reasonable to recommend diuretics acy) are required.
as a starting point for many patients, the trial evidence to There is a continuing need for more effective agents
support using low-dose thiazides in this context is non- from among currently available drug classes, ideally
existent and can only be condoned for cost reasons. Fur- with fewer side effects. Perhaps, more importantly,
thermore, it is inherently unlikely, given the heterogeneity newer classes of agents are required and several new
of the hypertensive population, that any one drug is the classes of agents are being developed. To provide real
best for all subgroups and types of patient. However, advances over currently available agents, such products
given the need in most patients for at least two agents will be required to have long duration of action and low
to control BP effectively, more trials of pairs of antihyper- side effect rates, with BP-lowering efficacy associated
tensive agents are required, and ideally they are required with commensurate reduction in CV events. The benefits
in the setting of different patient subgroups (e.g. those of pharmacogenetics whereby drugs may be targeted on
Downloaded from https://academic.oup.com/eurheartjsupp/article/10/suppl_G/G21/476006 by guest on 23 June 2022
with LVH, diabetes, and so on). the basis of genetic profiling are considered by some to
It seems unlikely that validation of treating low-risk be on the horizon, whereas others believe that it is a
patients with a systolic BP in the range of 140–159 mmHg rather distant horizon. Meanwhile with the increasing
in a placebo-controlled trial will be carried out. However, need and use of polypharmacy in an ageing population,
the randomized trial evidence for doing so is not available, the trends are likely to move further towards the use
and the cost implications of this policy (already effectively of combination therapies. This is likely to involve not
a worldwide recommendation) are massive. The tradeoff of just the combination of two (or more) antihypertensive
risk and benefit in this group should be evaluated in a trial. agents but also the combination of various products
The shortcomings of the Hypertension Optimal Treat- that act on different CV risk factors.
ment (HOT) trial1 highlight the need for a more definite Meanwhile, pending further evidence from randomized
trial focused on systolic targets given the greater predic- trials to further guide drug selection and sequencing, the
tive value of systolic BP for most patients with hyperten- combination of A and C drug classes appears to be logical
sion. The need for such a trial was highlighted in the from a mechanistic viewpoint,34 metabolically beneficial
WHO-ISH guidelines produced in 1999,32 as one of eight (or at worst neutral),35 cost effective,30 well tolerated,10
areas of further research still required. Another glaring supported by extensive trial evidence of the individual
omission is work in the developing world. This is the criti- components,31 and in combination in the ASCOT trial,10
cal target for preventing the anticipated increase in the and may produce greater benefits in terms of coronary
burden of hypertension and CVD in the next two and stroke protection than the BP reduction so-produced
decades. The potential for primordial prevention and would predict.36
improved BP management remains, but only if suitable Based on trials in which any of the currently rec-
research is designed, resourced, and carried out urgently. ommended pairs of agents5,19,26 have been compared,
In the most recent hypertension guidelines (except JNC ACE inhibitors plus CCBs probably have the best evidence
7), thresholds for treating hypertension are increasingly to support their use for the management of hypertension.
based on estimated CV risk. It should be acknowledged,
however, that no trials have been designed to include Conflict of interest: I confirm that the above manuscript is the
patients on the basis of a specific level of risk. Hence, work of the authors as stated, and declare that I participated
it is difficult and perhaps inappropriate, pending such in the design, execution, and analysis of the paper. I also
information, to replace BP levels by risk levels when declare that I have the following potential conflicts of interest
in connection with this paper. (a) Speaker honoraria: I have
making treatment recommendations.
and continue to receive honoraria for speaking at industry-
At a population level, the advice given to the general sponsored meetings including those organised by Servier. (b) I
public and those responsible for healthcare delivery am currently co-ordinating a randomized trial of up to 3000
needs to improve dramatically if we are to lower the patients with hypertension. This trial is funded by Servier Lab-
healthcare burden due to raised BP. Public education oratories and employs approximately 20 people in my research
on health is achievable. Despite some cynical views unit. (c) I intermittently receive payment for appearing on ad
regarding large population-based interventions, startling hoc advisory boards for drug and food companies. I own no
beneficial effects on CVD and mortality have been demon- stock of any kind and have no academic or intellectual commit-
strated at the population level. For example, in Finland, ments that would bias the work submitted for publication.
the reduction in CV deaths over a 20-year period, follow-
ing a broad-based national campaign to improve diet and Funding
lifestyles, appears to have been almost completely
attributable to the healthy life changes that were made.33 N.R.P. has received funding from Servier to present data
The improved implementation of guidelines necessi- at several international symposia and as in this case for
tates more effective communication between those pro- producing an associated brief article.
ducing the guidelines and the healthcare professionals
charged with managing patients. It may also be useful
to produce documents—written, visual, or electronic— References
designed to inform the general public. In the interests 1. Hansson L, Zanchetti A, Carruthers SG, Dahlöf B, Elmfeldt D,
of optimal broad-based uptake of guidelines, a pivotal Julius S, Ménard J, Rahn KH, Wedel H, Westerling S; HOT Study
component required is simplicity. Brief, simple messages Group. Effects on intensive blood pressure lowering and low-doseFixed combination to improve morbidity/mortality G27
aspirin in patients with hypertension: principal results of the Hyper- report of the fourth working party of the British Hypertension
tension Optimal Treatment (HOT) randomised trial. Lancet 1998; Society 2004-BHS IV. J Human Hypertens 2004;18:139–185.
351:1755–1762. 20. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo L Jr,
2. Tight blood pressure control and risk of macrovascular and micro- Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ. The
vascular complications in type 2 diabetes: UKPDS38. Br Med J 1998; Seventh Report of the Joint National Committee on Prevention,
317:703–713. Detection, Evaluation, and Treatment of High Blood Pressure: The
3. Cappuccio FP, Markandu ND, Tucker FA, Shore AC, McGregor GA. JNC 7 Report. J Am Med Assoc 2003;289:2560–2571.
A double blind study of the blood-pressure lowering effect of a 21. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R,
thiazide diuretic in hypertensive patients already on nifedipine and Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S,
a beta-blocker. J Hypertens 1987;5:733–738. Narkiewicz K, Ruilope L, Rynkiewicz A, Schmieder RE, Boudier HA,
4. Primatesta P, Brookes M, Poulter NR. Improved hypertension manage- Zanchetti A, Vahanian A, Camm J, De Caterina R, Dean V,
ment and control. Results from the Health Survey for England 1998. Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I,
Hypertension 2001;38:827–832. Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M,
5. National Collaborating Centre for Chronic Conditions. Hypertension: Widimsky P, Zamorano JL, Erdine S, Kiowski W, Agabiti-Rosei E,
management of hypertension in adults in primary care: partial Ambrosioni E, Lindholm LH, Viigimaa M, Adamopoulos S, Agabiti-
Downloaded from https://academic.oup.com/eurheartjsupp/article/10/suppl_G/G21/476006 by guest on 23 June 2022
update. NICE Clinical Guideline. London: Royal College of Physicians; Rosei E, Ambrosioni E, Bertomeu V, Clement D, Erdine S, Farsang C,
2006. Gaita D, Lip G, Mallion JM, Manolis AJ, Nilsson PM, O’Brien E,
6. Dickerson JE, Hingorani AD, Ashby MJ, Palmer CR, Brown MJ. Ponikowski P, Redon J, Ruschitzka F, Tamargo J, van Zwieten P,
Optimisation of antihypertensive treatment by crossover rotation of Waeber B, Williams B; Management of Arterial Hypertension of the
four major classes. Lancet 1999;353:2008–2013. European Society of Hypertension (ESH) and of the European
7. Materson BJ, Reda DJ, Cushman WC, Massie BM, Freis ED, Kochar MS, Society of Cardiology (ESC). J Hypertens 2007;25:1105–1187.
Hamburger RJ, Fye C, Lakshman R, Gottdiener J; Department of 22. Dahlöf B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, Faire U,
Veterans Affairs Cooperative Study Group on Antihypertensive Fyhrquist F, Ibsen H, Kristiansson K, Lederballe-Pedersen O,
Agents. Single-drug therapy for hypertension in men. A comparison Lindholm LH, Nieminen MS, Omvik P, Oparil S, Wedel H, for the
of six antihypertensive agents with placebo. N Engl J Med 1993; LIFE study group. Cardiovascular morbidity and mortality in the
328:914–921. Losartan Intervention For Endpoint reduction in hypertension study
8. Neal B, Turnbull F. The effects of different blood pressure lowering (LIFE): a randomised trial against atenolol. Lancet 2002;359:
995–1003.
regimens on major cardiovascular events. Lancet 2004;363:331–332.
23. Wanovich R, Kerrish P, Gerbino PP, Shoheiber O. P-518: compliance
9. Dahlöf B, Sever PS, Poulter NR, Wedel H, Beevers G, Caulfield M,
patterns of patients treated with 2 separate antihypertensive
Collins R, Kjeldsen S, Kristinsson A, McInnes GT, Mehlsen J,
agents versus fixed-dose combination therapy. Am J Hypertens
Nieminen M, O’Brien E, Ostergren, for the ASCOT investigators.
2004;17:223A–223A; doi:10.1016/j.amjhyper.2004.03.592
Prevention of cardiovascular events with an antihypertensive
24. Jackson K et al. Persistence of fixed versus free combination with
regimen of amlodipine adding perindopril as required versus atenolol
valsartan and HCTZ for patients with hypertension. Value Health
adding bendroflumethiazide as required, in the Anglo-Scandinavian
Suppl 2006;9:A363.
Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA):
25. Sever PS, Dahlöf B, Poulter NR, Wedel H, Beevers G, Caulfield M,
a multicentre randomised controlled trial. Lancet 2005;366:895–906.
Collins R, Kjeldsen SE, McInnes GT, Mehlsen J, Nieminen M,
10. Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L,
O’Brien E, Ostergren J. Rationale, design, methods and baseline
Hua T, Laragh J, McInnes GT, Mitchell L, Plat F, Schork A, Smith B,
demography of participants of the Anglo-Scandinavian Cardiac Out-
Zanchetti A, for the VALUE trial group. Outcomes in hypertensive
comes Trial. J Hypertens 2001;19:1139–1147.
patients at high cardiovascular risk treated with regimens based on
26. Sever PS, Dahlöf B, Poulter NR, Wedel H, Beevers G, Caulfield M,
valsartan or amlodipine: the VALUE randomised trial. Lancet 2004;
Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J,
363:2022–2031.
Nieminen M, O’Brien E, Ostergren J; ASCOT Investigators. Prevention
11. Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combi-
of coronary and stroke events with atorvastatin in hypertensive
nation treatment with blood pressure lowering drugs: analysis of
patients who have average or lower-than-average cholesterol con-
354 randomised trials. Br Med J 2003;326:1427.
centrations, in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid
12. Mahmud A, Feely J. Low-dose quadruple antihypertensive combi- Lowering Arm (ASCOT-LLA): a multicentre randomised controlled
nation. Hypertension 2007;49:272. trial. Lancet 2003;361:1149–1158.
13. Wald D et al. Impact of second line agents for hypertension. Further 27. Poulter NR, Wedel H, Dahlöf B, Sever PS, Beevers G, Caulfield M,
analyses of ref 11. (submitted/personal communication). Collins R, Kjeldsen S, Kristinsson A, McInnes GT, Mehlsen J,
14. Bakris G, Molitch M, Hewkin A, Kipnes M, Sarafidis P, Fakouhi K, Nieminen M, O’Brien E, Ostergren, for the ASCOT investigators.
Bacher P, Sowers J, on behalf of the STAR Investigators. Differences Role of blood pressure and other variables in the differential
in glucose tolerance between fixed-dose antihypertensive drug cardiovascular event rates noted in the Anglo-Scandinavian Cardiac
combinations in people with metabolic syndrome. Diabetes Care Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA). Lancet
29:2592–2597. 2005;366:907–913.
15. Weber MA, Bakris GL, Dahlöf B, Pitt B, Velazquez E, Gupte J, 28. The CAFE Investigators, for the Anglo-Scandinavian Cardiac Outcomes
Lefkowitz M, Hester A, Shi V, Weir M, Kjeldsen S, Massie B, Trial (ASCOT) Investigators, CAFE Steering Committee and Writing
Nesbitt S, Ofili E, Jamerson K, for the Accomplish Investigators. Base- Committee, Williams B, Lacy PS, Thom SM, Cruickshank K,
line characteristics in the Avoiding Cardiovascular events through Stanton A, Collier D, Hughes AD, Thurston H, O’Rourke M. Differential
Combination therapy in Patients Living with Systolic Hypertension impact of blood pressure-lowering drugs on central aortic pressure
(ACCOMPLISH) trial: a hypertensive population at high cardiovascular and clinical outcomes: principal results of the Conduit Artery
risk. Blood Press 2007;16:13–19. Function Evaluation (CAFE) Study. Circulation 2006;113:1213–1225.
16. Chapman N, Dobson J, Wilson S, Dahlöf B, Sever PS, Wedel H, 29. Gupta AK, Dahlöf B, Dobson J, Sever PS, Wedel H, Poulter NR,
Poulter NR, on behalf of the Anglo-Scandinavian Outcomes Trial on behalf of the ASCOT Investigators. Determinants of new-onset
Investigators. Effect of spironolactone on blood pressure in subjects diabetes among 19,257 hypertensive patients randomised in the
with resistant hypertension. Hypertension 2007;49:839–845. ASCOT-BPLA trial and the relative influence of antihypertensive
17. Lindholm LH, Carlberg B, Samuelsson O. Should b blockers remain first medication. Diabetes Care 2008; published online ahead of print.
choice in the treatment of primary hypertension? A meta-analysis. 30. Lindgren P, Buxton M, Kahan T, Poulter NR, Dahlöf B, Sever PS,
Lancet 2005;366:1545–1553. Wedel H, Jönsson B, on behalf of the ASCOT Trial Investigators.
18. Wiysonge CS, Bradley H, Mayosi BM, Maroney R, MBewu A, Opie LH, Economic evaluation of ASCOT-BPLA: antihypertensive treatment
Volmink J. Beta-blockers for Hypertension (Review). John Wiley & with an amlodipine-based regimen is cost-effective compared with
Sons, Ltd; 2007. an atenolol-based regimen. Heart 2008;94:4.
19. Williams B, Poulter NR, Brown M, Davies M, McInnes G, Potter J, 31. Turnbull F; Blood Pressure Lowering Treatment Trialists’
Sever PS, Thom S. Guidelines for management of hypertension: Collaboration. Effects of different blood-pressure-loweringG28 N.R. Poulter
regimens on major cardiovascular events: results of prospectively- 34. Epstein M. The benefits of ACE inhibitors and calcium antagonists in
designed overviews of randomised trials. Lancet 2003;362: slowing progressive renal failure: focus on fixed-dose combination
1527–1535. antihypertension therapy. Ren Fail 1996;18:813–832.
32. Guideline Subcommittee 11999 World Health Organization-International 35. Elliott WJ, Meyer PM. Incident diabetes in clinical trials of antihyper-
Society of Hypertension Guidelines for the Management of Hyperten- tensive drugs: a network meta-analysis. Lancet 2007;369:201–207.
sion. J Hypertens 1999;17:151–183. 36. Verdecchia P, Reboldi G, Angeli F, Gattobigio R, Bentivoglio M, Thijs L,
33. Vartiainen E, Puska P, Pekkanen J, Tuomilehto J, Jousilahti P. Changes Staessen JA, Porcellati C. Angiotensin-converting enzyme inhibitors
in risk factors explain changes in mortality from ischaemic heart and calcium channel blockers for coronary heart disease and stroke
disease in Finland. Br Med J 1994;309:23–27. prevention. Hypertension 2005;46:386–392.
Downloaded from https://academic.oup.com/eurheartjsupp/article/10/suppl_G/G21/476006 by guest on 23 June 2022You can also read