SA Drug Policy Week tackles effective drug policy - Investigating free resources for SA doctors - SAMA Insider
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

INSIDER
SAMA
October 2017
SA Drug Policy Week
tackles effective
drug policy
Investigating free
resources for SA doctors
PUBLISHED AS A SERVICE TO ALL MEMBERS OF SOUTH AFRICAN
THE SOUTH AFRICAN MEDICAL ASSOCIATION (SAMA) MEDICAL ASSOCIATION
SAMAREC/CPD
WHAT WE ARE ABOUT
SERVICES AVAILABLE:
South Af ric a Medic al Ass oc iation
SAMAREC: CPD:
Res earc h and Ethic s Committee -
SAMAREC Evaluating the ethics of research Assisting health professionals to maintain
protocols developed for clinical trials and acquire new and updated levels of
South Af ric an Medic al Ass oc iation conducted in the private healthcare knowledge, skills and ethical attitudes
Continued Profes s ional
sector. Ensuring the protection and that will be of measurable benefit in
Dev elopment Ac c reditation
respect of rights, safety and well-being of professional practice and to enhance and
participants involved in clinical trials and promote professional integrity. The SA
O ur Mis s ion:
to provide public assurance of the Medical Association is one of the
o Empowering Doctors to bring protection by reviewing, approving and institutions that have been appointed by
health to the nation providing comment on clinical trial the Medical and Dental Professions
o Excellent Service protocols, the suitability of investigators, Board of the Health Professions Council
o Quick Turnaround
facilities, methods and procedures used of SA to review and approve CPD
o Efficiency
to obtain informed consent applications.
.
For further information please contact the SAMAREC/CPD Secretariat on 012 481 2000
CONTENTS
OCTOBER 2017
Source: Shutterstock - bbernard
3 EDITOR’S NOTE 14 SAMA hosts CPD in Burgersfort
Online resources – what do you use? Bokang Motlhaga
Diane de Kock
15 SA Drug Policy Week tackles effective
4 FROM THE PRESIDENT’S DESK drug policy
Genetic link, gamete-donor Dr Lindi Shange
identity, surrogacy – the
controversies of in-vitro fertilisation
Prof. Dan Ncayiyana
16 Discussing climate change
Dr Akhtar Hussain
5 FEATURES
Investigating free resources for SA 17 Medical cannabis discussed at
doctors Mamelodi CPD
SAMA Communications Department Sarah Molefe
7 ABC of fluid and electrolyte therapy 18 SAMA PhD scholarship provides
Jan Pretorius
invaluable support
9 New code to change promotion of
medical devices
Prof. Nicola Wearne
SAMA Knowledge Management and 18
Expansion of NAPPI code to seven
Research Department digits
11
A new age of junior doctors:
Unscripted
SAMA Private Practice Department
19 MEDICINE AND THE LAW
Dr Farah Jawitz Cutting corners
The Medical Protection Society
12 What is the “One Health” approach?
Bernard Mutsago
20
BRANCH NEWS
13 SA Back Week – it’s time to stand up
for yourself
SAMA Communications Department
Alexander Forbes
MEMBER BENEFITS Herman Steyn
012 452 7121 / 083 389 6935| steynher@aforbes.co.za
Offers SAMA members a 20% discount on motor and household insurance
premiums.
Automobile Association of South Africa (AA)
AA Customer Care Centre
0861 000 234 | kdeyzel@aasa.co.za
The AA offers a 12.5% discount to SAMA members on the
AA Advantage and AA Advantage Plus Membership packages.
Barloworld
Lebo Matlala : External Accounts Manager: EVC
011 052 0167 | 084 803 0435 | LeboM@bwmr.co.za
Barloworld Retail Digital Channels offers competitive pricing on New
vehicles; negotiated pricing on demo and pre-owned vehicles; Trade
in’s; Test Drives and Vehicle Finance.
BMW
Melissa van Wyk : Corporate Sales Manager
079 523 9043 | melissa.vanwyk1@bmwdealer.co.za
SAMA members qualify for a minimum of 8% discount on selected
BMW & MINI models. All Members also receive competitive
pricing on Lifestyle items and accessories.
DLT MAGAZINES
Tracey Hack : General Manager
011304 7600 |076 020 5280 | tracey@dltmedia.co.za
DLT Magazines offers medical practices current consumer magazines
for their patients, to keep them relaxed and occupied while that wait
for their service. We work with premium consumer titles from all
major publishers in South Africa. SAMA members qualify for a 10%
discount off any of our current custom and or preselect magazine
packs. We also offer magazine racks at 50% discount for SAMA
Members.
FORD/KIA CENTURION
Burger Genis : New Vehicle Sales Manager – Ford Centurion
012 678 0000 | burger@laz.co.za
Nico Smit : New vehicle Sales Manager – Kia Centurion
012 678 5220 | nico@kiacenturion.co.za
Lazarus Ford/Kia Centurion, as part of the Lazarus Motor Company group,
sells and services the full range of Ford and Kia passenger and commercial
vehicles. SAMA Members qualify for agreed minimum discounts on
selected Ford and Kia vehicles sourced from Lazarus Ford / Kia Centurion.
SAMA members who own a Ford/Kia vehicle also qualify for preferential
servicing arrangements. We will structure a transaction to suit your needs.
Hertz Rent a Car
Lorick Barlow
072 308 8516 | lorick@hertz.co.za
Hertz is proud to offer preferential car rental rates to SAMA members. A
range of value-add product and service options also available. No cost to
register as a Gold Plus Rewards member to enjoy a host of exclusive benefits.
Legacy Lifestyle
Allan Mclellan
0861 925 538 / 011 806 6800 |info@legacylifestyle.co.za
SAMA members qualify for complimentary GOLD Legacy
Lifestyle membership. Gold membership entitles you to
earn rewards at over 250 retail stores as well as
preferred rates and privileges at all Legacy Lifestyle
12/09/2017
partnered hotels and further rewards back on
accommodation and extras.
EDITOR’S NOTE OCTOBER 2017
Online resources –
what do you use?
Welcome to the October edition of SAMA Insider. This month we introduce what
we hope will become a communication platform for readers on the maze of online
resources available to doctors in the form of apps, databases, programs, toll-free
hotlines and online courses. Sharing information about which resources you use on
a regular basis, and why, would be helpful to our readers when faced with so many
choices – personal feedback is always valuable!
In his second-last message (page 4), SAMA president Prof. Dan Ncayiyana looks
at “Genetic link, gamete-donor identity, surrogacy – the controversies of in-vitro
fertilisation”, an article likely to spark some debate, which we hope you will share
Diane de Kock with us by writing a letter to the editor.
Editor: SAMA INSIDER A follow-up article (page 9) by the SAMA Knowledge Management and Research
Department looks at the implications of the recently launched SA Medical Device
Industry Association (SAMED)’s Medical Device Code of Ethical Marketing and
Business Practice, and encourages members to familiarise themselves with the code,
its principles and guidance.
JUDASA Western Cape (page 11) has launched a “Doctors Unscripted” series of
open meetings to brainstorm how junior doctors can make a difference, and Dr Lindi
Shange (page 15) tackles the potentially controversial subject of an effective drug
policy in SA: “We need to have the ‘difficult conversations’ to understand the issues
and identify appropriate solutions.” We look forward to further articles on this subject
from Dr Shange.
On page 16, SEDASA’s Dr Akhtar Hussein discusses climate change, and on page 18
Prof. Nicola Wearne reports on her research project funded by a SAMA PhD scholarship.
We look forward to receiving feedback from all our readers on this edition. Please
email the editor at Dianed@hmpg.co.za.
Editor: Diane de Kock Design: Travis Arendse
Chief Operating Officer: Diane Smith Published by the Health and Medical Publishing Group (Pty) Ltd
Copyeditor: Kirsten Morreira Block F, Castle Walk Corporate Park, Nossob Street
Erasmuskloof Ext. 3, Pretoria
Editorial Enquiries: 083 301 8822
Advertising Enquiries: 012 481 2069 Email: publishing@hmpg.co.za | www.samainsider.org.za | Tel. 012 481 2069
Email: dianes@hmpg.co.za Printed by Tandym Print (Pty) Ltd
DISCLAIMER
Opinions and statements, of whatever nature, are published in SAMA Insider under the authority of the submitting author, and should not be taken to present the official
policy of the South African Medical Association (SAMA) unless an express statement accompanies the item in question.
The publication of advertisements promoting materials or services does not imply an endorsement by SAMA, unless such endorsement has been granted. SAMA does not
guarantee any claims made for products by their manufacturers. SAMA accepts no responsibility for any advertisement or inserts that are published and inserted into SAMA
Insider. All advertisements and inserts are published on behalf of and paid for by advertisers.
LEGAL ADVICE
The information contained in SAMA Insider is for informational purposes and does not constitute legal advice or give rise to any legal relationship between SAMA and the receiver
of the information, and should not be acted upon until confirmed by a legal specialist.
FROM THE PRESIDENT’S DESK
Genetic link, gamete-donor identity, surrogacy
– the controversies of in-vitro fertilisation
husband’s sperm, and then returning In SA, assisted reproduction is regulated by
the embr yo to the womb. However, the National Health Act No. 61 of 2003 and
experimenting in this way with human eggs the Regulations Relating to the Artificial
and sperm outside the body was widely Fertilisation of Persons, 2012, as well as the
considered by many as unethical, if not Children’s Act No. 38 of 2005. According to
immoral, and funding agencies, including the SA Law Reform Commission, “the legal
the UK Medical Research Council, declined position in SA is that gamete donors and
to fund the research. The project was rescued surrogate mothers must be anonymous,
only when the Ford Foundation and some and it is an offence to reveal the identity of
private US financiers agreed to provide the a gamete donor or surrogate mother”. The
funding. The medical fraternity was at best commission has launched a study into the
sceptical (as is usual with pioneering medical appropriateness of this provision, putting
initiatives and ideas), or even downright the question of whether a child has a right to
hostile. James Watson (of the Watson know its biological origins, for reasons of the
and Crick DNA molecule) denounced the child’s sense of identity.
researchers, questioning the wisdom of Anonymity is intended to protect the
tampering with procreation. They were privacy of the egg or sperm donor, or the
denounced by the Catholic Church, which surrogate mother, and rescinding it would
Prof. Dan Ncayiyana, SAMA president remains opposed to IVF to this day for a open a whole new can of worms. Donors do
variety of reasons, including Pope Benedict not donate in order to become parents of a
L
ouise Joy Brown, the world’s first “test- XVI’s view that it “replaces love between multitude of disparate children, and may be
tube baby”, was delivered by caesarean a husband and wife”. Pro-life advocates spooked by the prospect that the resulting
section at 23h47 on 25 July 1978 at the labelled IVF as a “perversion”. progeny might someday seek to establish
Royal Oldham Hospital in the UK. The birth In time, however, IVF went on to gain wide a social or parental bond with their genetic
was a cloak-and-dagger affair. The news of a acceptance. Since the birth of Louise Brown parent. Indeed, countries where donor
human pregnancy artificially contrived in a in 1987, it is estimated that two million babies anonymity has been eliminated have seen
“test tube” (it was actually accomplished in a have been born globally through the use of their donor pool diminish.
petri dish) had caused seismic wonderment, IVF. IVF technology has made huge advances In the realm of surrogate motherhood,
and the press was hounding the pregnant through continuing research that has helped SA law requires that the contemplated child
mother to the point where she had to be improve success rates and widen the pool of be genetically related to one or both of the
delivered in secret under an assumed name. those who qualify. However, it is also hugely commissioning parents. This provision was
The late hour of this historic birth was due to expensive and has become big business, recently challenged, unsuccessfully, in the
Patrick Steptoe, the pioneering obstetrician, with IVF clinics sprouting all over the world, Constitutional Court by a woman who had
having been delayed by his wife’s birthday not least in SA, with its world-class facilities undergone multiple IVF cycles while married,
dinner – presumably indicative of either a and expertise. IVF and plastic surgery have until she ran out of her own eggs. She was
highly devoted husband or a formidable wife. become the predominant engines driving subsequently divorced, and now sought
The two pioneers, Steptoe and his research SA medical tourism. to have a child through surrogacy using a
collaborator, medical physiologist Robert donated ovum and sperm. The Concourt
Edwards, were overjoyed at the birth. Edwards sustained the genetic-link requirement.
(eventually to be awarded a Nobel Prize after IVF conundrums in SA The child is certainly entitled to know
Steptoe’s death) was later to recall: “The new Concerned as it is in the very intimate and at the appropriate age and time about his
citizen continued to cry very loudly, and how emotive subject of human reproduction, or her IVF origins. But it is not clear to me
we all loved that glorious sound.” IVF has aroused social, cultural and religious that disclosure to the child of the identity
Controversy surrounded in-vitro fertilis conundrums around the globe, some of the gamete donor or surrogate mother
ation (IVF) from the very beginning. Steptoe country-specific, some universal, that cut would help to reinforce bonding within
and Edwards started to work together in the across science and sociology, and revolve inter the recipient family, or enhance the child’s
1960s, driven by the desire to help couples alia around IVF opening the door for same- sense of identity. Prioritising the genetic link
with fertility problems due to the woman’s sex couples to have children of their own; and genealogy to define family and identity
damaged fallopian tubes (then accounting upsetting traditional conceptions of family; unduly elevates the biological model above
for about a quarter of all cases of infertility). and raising questions about the psychological all others. Ultimately, what defines family
They pursued the unprecedented idea of impact on the child. For this reason, countries and belonging for a child transcends
extracting eggs directly from a woman’s have sought to make laws to regulate this biology. It is about active caring, nurturing
ovaries, fertilising them in vitro with the medical intervention. and love.
4 OCTOBER 2017 SAMA INSIDER
FEATURES
Investigating free resources for SA doctors
SAMA Communications Department
T
oday we are all constantly attached security measure to keep it exclusively for For more information and other resources,
to our mobile phones and computers, medical professionals. You can also access visit www.inpracticeafrica.com, or email
and depend on them to provide us the app by inserting BlankPage2017 in the customersupport@inpractice.com.
with digital aids of every description. There sign-in box.
are many apps, databases, programs, toll
For more information, contact BlankPage
Foundation for Professional
free hotlines and online courses (complete
Publishing on 087 095 3225 or email on info@
Development (FDP)
with CPD accreditation) available to medical The following courses are offered by FDP
blankpage.co.za.
practitioners, a lot of them for free. free to scholarship holders, and there are
This month we begin a series of articles scholarships available for medical doctors
on these free resources, and appeal to our
inPractice Africa registered with the HPCSA:
The 2017 edition of inPractice Africa is a free,
readers to let us know of any such resources • Short course in financial management:
continuously updated reference and learning
that they use regularly, and which could be of This online course for specialists and
resource for SA clinicians. The program
assistance to fellow practitioners. registrars recognises that private-practice
provides CPD development certificate
specialists need to run well-functioning
programmes, practice guidelines and drug
Med Brief Africa reference information, as well as referral businesses, which requires financial
Med Brief Africa, a unique news-based mobile thinking and smart decision-making.
clinical support. inPractice Africa is designed
phone app available to more than 20 000 of The course assists specialists who are
to be used in two ways:
the country’s healthcare professionals on SAMA members with developing a strong
• To search for and efficiently find the
a daily basis, has been launched by newly foundation in the basics of accounting
information you need to care for individual
established specialist IT publishing entity, and financial literacy. “We would like to
patients
BlankPage Publishing. avoid decisions being made without
• To study complete modules and earn
The app covers 16 specialist medical disci analysing the risk and reward or the profit
credit in the following areas: applying SA
plines, including general practice, and feat and cash flow of the particular practice.
national guidelines on antiretroviral therapy
ures additional posts covering pharmacy, This course will impart the knowledge
(ART); nursing care of HIV-infected patients;
nursing, optometry and psychology.
management of tuberculosis (TB) in HIV-co- necessary for private practitioners to
Content comprises freshly sourced,
infected patients. understand and manage the financial
written and edited clinical, medicopolitical
aspects of their practice,” says FDP.
and practice-management news items
The resource answers many key questions, See https://www.mpconsulting.co.za/
prepared on an ongoing basis by a team of
including: products/online-cme/386/e-learning-
news-media-trained journalists with almost
• Do you know when to start ART in your short-course-in-financial-management.
60 years of medical reporting and editing
patients? • Fraud-risk management for medical doctors:
experience between them.
• What do the latest SA guidelines say about This online course recognises that medical
Provision has also been made for regular
recommended first-line treatment options? doctors have become soft targets for fraud
features such as in-practice management, in both their private and professional
• Do you follow best practices in monitoring
and legal and funding matters. capacities, mainly because doctors rarely
HIV-infected patients receiving therapy for TB?
By arrangement with their professional have the time to investigate the origin
• Are you using the recommended regimens
bodies and with the assistance of a of emails and financial documents, and
leading medical-practice-management to prevent mother-to-child transmission in
your practice? generally do not have the support of IT staff
consultancy, medical specialists, once to reduce fraud risk arising from the use of
registered, can freely access their own technology. The risk of fraud can never be
specific field within the app, with the The resource allows you to earn CPD credits
eliminated, but this CPD/CME course will
appropriate clinical and in-practice news, free of charge for successfully passing the
assist doctors to reduce the risk of financial
while general medical news on matters module post-tests – up to 60 CPD credits are
loss, whether due to online scams, credit-
such as NHI, market enquiry developments available! Good news for clinicians who earned
card fraud, deposits and refunds, identity
and exclusive conference coverage is credit from this programme when it was
theft and many other fraudulent activities.
common to all. initially launched in 2015/16 – as the content Designed by the expert fraud-management
Visiting either the Apple iStore or has been fully updated, you are eligible to earn team at Investec Bank, in association with
Google Play Store and downloading the up to 60 CPD credits once again! FPD and Medical Practice Consulting to
app free of charge allows you to access inPractice Africa also offers SA-specific assist doctors in the management of fraud
Med Brief Africa. There is a brief registration resources, including a drug reference risk, the course is applicable to all doctors,
requirement to ensure that only medical database. You can access information about whether in public or private practice.
professionals have access – doctors are drugs by clicking on the relevant drug, or by See https://www.mpconsulting.co.za/
required to insert their MP number and following your search results where drugs products/online-cme/649/fraud-risk-
complete the registration process, a appear in modules. management-for-medical-doctors.
SAMA INSIDER OCTOBER 2017 5
FEATURES
Primary Health Care Clinical a voucher reward to redeem at KAUAI, Vida highlighting tools which impact clinical
Guide e Caffè, Mugg & Bean or Ster-Kinekor. They practice and serve to impact diagnosis,
Produced by The Open Medicine Project can also choose to donate their rewards to treatment or determining prognosis.
SA, this Department of Health (DoH) app designated charities. Available from https://www.qxmd.com/
gives healthcare workers easy access to the Participating doctors can also access an apps/calculate-by-qxmd.
country’s Primary Care Standard Treatment upfront 50% discount on Apple Watches and • Read by QxMD: The newest studies
Guidelines and the Essential Medicines List. other wearable fitness devices, as well as an become available and you can set your
Aimed at a broad range of healthcare upfront 55% discount on the CardioChek field of interest so that you do not receive
workers, the app includes the following point-of-care device that doctors can use studies from outside your field of interest.
features: to check their patients’ cholesterol and Described as a personalised medical
• A cardiovascular risk-assessment tool, blood sugar levels in their rooms. Doctors journal, this app provides a single place to
which efficiently calculates a patient’s actively engaging in VARD can increase these discover new research, read outstanding
percentage risk of having a cardiovascular discounts to 100%. “We are showing doctors topic reviews and search PubMed. Free on
event such as a stroke or a heart attack in the direct benefit that prioritising their own iPad, iPhone and Android.
the next 10 years wellbeing has on their own lives and their • Eye Chart Pro: To do visual examinations,
• A paediatric drug-dosage calculator, which patients’ lives,” says Dr Goodman. the basic version is free. Eye Chart Pro is
accurately calculates weight- or age-based By placing important patient information a generator for randomised Snellen and
dosage for children at your fingertips, Discovery’s HealthID app Tumbling E charts to offer a rough but useful
• A medicine stock-out tool, which allows provides you with a complete view of your screen of visual acuity. Simply press a button
healthcare professionals to repor t patient’s health history and test results. to randomise the entire eye chart, or touch
medication shortages and stock-outs This improves patient care and reduces an individual line of the chart to randomise
directly to the DoH. the likelihood of serious medical errors and that line. Tap another button to toggle
duplicate or unnecessary pathology tests. between Snellen and Tumbling E charts.
To download the app, search for “PHC Clinical In addition, HealthID also reduces your Available on the App Store for iOS devices.
Guide” in the Apple iStore or Google Play administrative burden by making it quick • EML Clinical Guide (DoH): Look up
Store. and easy to fill in chronic-illness benefit primary-care algorithms as set up by
applications, and providing you with the the DoH. The app is free on Apple iStore,
The eDL app relevant scheme formulary list. The app Google Play Store and Windows App Store.
This app is available from the Google Play can be accessed through tablet apps, the • HIV Clinical Guide (DoH): Look at HIV care
Store and updated regularly. It provides a Discovery website and certain practice- and which drugs and interventions to apply
revolutionary way to exchange electronic manager applications. in different circumstance. The app provides
discharge letters (eDL) and prevent the Discover y and the S outh Afr ican guidelines and decision support for
current problems related to the paper-based Depression and Anxiety Support Group healthcare workers treating HIV patients in
letters generated by doctors. Handwriting, (SADAG) recently launched a 24/7 mental- SA. The app is free on Apple iStore, Google
use of narratives and unstructured text, health helpline for doctors. “ We are Play Store and Windows App Store.
lack of standardisation, language barriers, proud to announce the recent launch of • Lancet Mobile: Real-time pathology
incompleteness and ambiguity are some a dedicated mental-health helpline for results on your phone or tablet. Available
of the problems addressed by the eDL app. young doctors and medical students,” from www.lancet.co.za.
It supports semantic interoperability of explains Dr Goodman. When calling • BMJ Best Practice: Fast and easy access
diagnosis and medications, raises allergy 0800 323 323, young medical professionals to the latest evidence-based information
alerts and encourages patient empowerment, now have anonymous 24/7 access to free on diagnosis and treatment for healthcare
all of which ultimately improve patient safety. psychological support services. professionals. The app highlights evidence-
based medicine and best practice. Available
Discovery Health – free apps For more information visit www.discovery.co.za. from http://bestpractice.bmj.com/best-
and helpline and free ride practice/marketing/best-practice-app.html.
Discovery Health’s Vitality Active Rewards Which apps do you use? • ICD-10 Lite: This app is for when you need
for Doctors (VARD) tailors the rewards to Dr Cobus van Niekerk kindly shared the apps an ICD-10 code on the move and you are
the needs of doctors – starting with doctors he uses regularly and finds helpful: not close to your PC to look it up. Available
currently registered for private practice. “The • HealthID (Discovery): helps with daily from https://itunes.apple.com/za/app/icd-
VARD programme is available to doctors at running of Discovery-managed patients 10-lite-2013/id435280639?mt=8.
no charge on the Discovery smartphone app (see above for more details). • DermaCompare: Used to evaluate skin
regardless of whether they have purchased • Calculate by QxMD: works out anything, lesions – benign v. malignant – and
any Discovery product. Once registered, from ideal weight to Framingham risk the risk stratification in those needing
doctors are challenged to meet personalised, score and many more. Calculate is a next- excision. Available from https://play.
weekly exercise goals based on current health generation clinical calculator and decision google.com/store/apps/details?id=com.
and activity levels,” explains Dr Goodman, support tool for iPhone, iPad, Android, emeraldmedical.dermacompareapp&hl=en.
Chief Medical Officer of Discovery Health. Windows 10 and web, freely available to
Doctors who reach their weekly goals earn the medical community. It focuses on We look forward to hearing from our readers.
6 OCTOBER 2017 SAMA INSIDER
FEATURES
ABC of fluid and electrolyte therapy
Jan Pretorius, Steve Biko Academic Hospital, University of Pretoria
F
luid therapy is drug therapy: this approach than is currently used, because Fluid therapy as
is the primar y message of this they constitute the physiological support drug therapy
communication. Choose your drug of surgical patients and of any patient
The importance of a rational concept
wisely; calculate dosages according to who is unable to ingest sufficient water
in approaching the entire perioperative
daily needs during maintenance, according and salts.
use of fluids and electrolytes cannot be
to response and sensible haemodynamic
overemphasised. The success of the concept
endpoints during shock therapy, and acc
of enhanced recovery after surgery (ERAS)
ording to measured losses when replacing The importance bears testimony to this. ERAS is a multimodal
excessive fluid losses. The use of intravenous of physiology and care pathway developed to manage and
fluids must always be approached as one
would any and all medication. This is the only pathophysiology control all treatment modalities during the
pre-, intra- and postoperative periods in
rational approach to fluid therapy today. The What happens to fluids after infusion is an
order to attenuate the stress response and
following points are important: important consideration. A large number
to promote early recovery. One of the most
• Fluid and electrolyte therapy is generally of physical and physiological principles
important issues is the judicious use of fluids
regarded as something benign, just control this: for example, capillary and
and electrolytes.
something that goes on. It is now very interstitial hydrostatic pressure, capillary and
Injudicious use of fluids and electrolytes
clear that it is a vitally important issue. interstitial oncotic pressure, inflammatory
is a good example of how things can go
• There is evidence that the type and status, the integrity of the endothelial
wrong and cause many further problems,
volume of fluid used affects outcome. Too glycocalyx, serum albumin concentration,
such as interstitial-space overload in most
little is just as harmful as too much. the amount of infused fluid and the presence
tissues and organ systems. This may affect
• Fluid therapy is the second-most-common of oedema. Many diseases can affect the
oxygen and nutrient delivery, and lead to
hospital intervention after oxygen admini patient’s volume of distribution and organ
compartment syndromes. The best-known
stration, yet the evidence regarding fluid function. The Starling equation need to be
example is abdominal hypertension, leading
and electrolyte therapy is quite limited. revised in view of new information about the
to the abdominal compartment syndrome,
• Fluids need to be given according to glycocalyx. The role of the lymphatics to clear
which affects the functioning of all other
a much more considered scientific oedema must be emphasised.
organ systems in return. It is time to concede
that fluid therapy should be precise and
Table 1. Total Fluid Management: Indications for fluid and electrolyte therapy in surgical
patients appropriate and calculated, NOT aggressive
or sparing or conservative or limited or
Total Fluid Maintenance Resuscitation Replacement
restrictive, or anything else.
Management (TFM)
It is essential to realise that there are three
1. Indication Daily requirement Hypovolaemia Abnormal or
main indications for fluid therapy (see Table 1):
continuing losses
• The need to resuscitate – to correct intra
2. Intention According to a formula “Aggressively” Collect drainage for
vascular volume deficits or acute hypo
based on body mass according to endpoints 4 hours, replace %
volaemia. The restoration of normal circulation
during next 4 hours,
is essential, to provide adequate tissue
while collecting again
perfusion, oxygenation and nutrients to
3. Infusion rate Continuously per 24 Bolus Continuously
sustain normal metabolic processes.
hours – 24 equal doses according to losses
• The need for maintenance – to specifically
4. Type of fluid Maintenance: Volume expander: According to fluid lost:
p rov i d e t h e p a t i e n t ’s d a i l y b a s a l
Maintelyte 5% Ringer’s lactate Rehydration
requirements for fluid, electrolytes and
Electrolyte No. 2 10% (modified) 5% dextrose in water
energy. This will often be extended to
sustenance 5% Plasmalyte B 0.45% NaCl
saline 0.9% NaCl parenteral or enteral nutrition.
colloids Ringer’s lactate • The need for replacement – replacement of
ongoing losses may be necessary in several
5. Monitor Serum and urine Central Serum and urine
electrolytes and osmol haemodynamics, electrolytes and osmol clinical scenarios, e.g. in the case of severe
Fluid-balance chart stroke volume burns or gastrointestinal fistulae.
variation, passive leg
raising, SvO2, lactate, It is important to understand and to rem
pH, base excess organ ember that one or all of these three fluid
functions: urine flow/ regimens may be necessary, and therefore
brain function (awake) simultaneously or in sequence. For example,
the patient admitted with a gastrointestinal
SAMA INSIDER OCTOBER 2017 7
FEATURES
fistula may need first resuscitation, followed output, or an arterial line or even an ordinary Fluid disturbances are often associated
by maintenance and nutrition as well as blood-pressure cuff. Next, lower the head and with electrolyte imbalances, as well as
replacement of ongoing losses. chest and lift the legs quickly to 45 degrees. acid-base disturbances. A typical example
Keeping an accurate daily fluid-balance This shifts about 500 mL of blood from the is found with gastric outlet obstruction
chart (intake and output) is key to successful legs and abdomen into the chest, increasing leading to dehydration (even hypovolaemic
fluid management. All fluids ingested enterally cardiac preload. An increase of more than 10% shock) and hypokalaemic, hypochloraemic
as well as administered parenterally, including in the stroke volume or an increase of more metabolic alkalosis. The serum sodium
all medications infused or dosed as boluses, than 9% in the pulse pressure or an increase of may also be low. This syndrome is typically
must be accounted for and fit into the patient’s more than 17% in the systolic blood pressure associated with a paradoxical aciduria.
calculated daily fluid allowance, to avoid fluid within 90 seconds indicate that the patient is Surviving patients pass through three
creep. Extending the fluid-balance chart to a fluid-responsive or preload-sensitive, and will phases with regard to fluid therapy
cumulative charting for the duration of the increase the cardiac output after a fluid bolus. during acute illness. The first phase is
patient’s stay often explains why a patient has Maintenance fluids constitute the physio the resuscitation period, during which
the appearance of a Michelin man. logical support of patients who cannot eat the patient is rescued by administering
Total Fluid Management (TFM) is a funda normally, are NPO (nil per mouth) post-op, fluids to restore the intravascular volume.
mental concept in fluid therapy. TFM is not do not want to eat, or who are unable to eat, In this phase fluids are therapeutic and
total fluid minimisation, as some proclaim. Too e.g. due to obstruction of the gastrointestinal essential, but should be goal-directed
few fluids are as dangerous as too many. tract. Daily maintenance must be calculated and administered early. On completion
according to the patient’s body weight. of resuscitation, maintenance therapy is
This volume should make allowance for used to re-establish stable homeostasis
How much is enough? all fluids to be infused (medications, water by optimising fluid status. Fluid strategy
From Table 1, it is clear that rules can be and electrolytes), with the exception of should now be calculated with the aim of
established for each indication for fluid resuscitation needs and replacement needs, equilibrating fluid balance. Increased fluid
therapy. Resuscitation should be conducted which have their own rules. needs may now be a biomarker of critical
considering endpoints to both trigger and Replacement of ongoing losses should illness. During the last phase, endothelial
discontinue treatment. Resuscitation should be planned in light of the patient’s total fluid integrity is restored once again and often
therefore be completed within a reasonable status. To best maintain homeostasis, fluids patients now develop a spontaneous
time frame. Triggers to initiate therapy must should be replaced as they are lost. I suggest diuresis. In this phase, one can attempt
be based on a careful history, and consider that the losses, if measurable, are collected to promote the removal of excess fluids
all the signs of intravascular volume deficit over a period of 4 hours. If the patient is using albumin infusions and small doses
and hypoperfusion. It is essential, though, passing adequate volumes of urine and has of furosemide, aiming at a negative fluid
to consider the patient’s responsiveness few other signs of fluid deficit, administer only balance. If increased capillary permeability
to fluids throughout therapy. This is not 50% of the volume collected over the next persists globally, the oedema or excess
the same as preload status. There is no 4 hours, while the fluid losses are collected fluids can be seen as toxic and part of
justification to continue fluid loading in a once again. If the patient is oliguric and thirsty, multiple-organ dysfunction.
patient who is not responsive, or in other replace 100% of the collected fluid. One can It is important to bear in mind that there
words is not able to increase stroke volume therefore vary the amount to be replaced is a time to administer fluids, a time to stop
or cardiac output. In this instance, inotropic according to the clinical situation. fluids and a time to “remove” excess fluids.
and or vasoactive medication may be needed.
Careful consideration of basic cardiac (i.e. the
Frank Starling curve) and vascular physiology Pathophysiology Conclusion
is always essential. Monitoring dynamic During stressful conditions such as trauma Fluid administration is a complex and difficult
variables (NOT static pressures such as central and sepsis, for which fluid therapy is task that is influenced by:
venous pressure) such as a passive leg raise, usually indicated and administered, the • The clinical setting
stroke volume or stroke-volume variation and pathophysiology of injury, leading to • Comorbid conditions
cardiac output is as essential as driving with increasing sympathoadrenal activation • The disease process
your lights on at night. and inflammation with endothelial acti • The use of other treatments
Performing a passive leg-raise test is safe vation, progressing to shock-induced endo • Vasoactive drugs
and simple. It is similar to a fully reversible theliopathy due to cellular and cytokine • Mechanical ventilation.
intrinsic 500 mL transfusion. It can be activation, compounds the effects of fluid
performed in ventilated and non-ventilated overload. Inflammation also cross-reacts Different strategies are needed at different
patients and it is valid in the presence of with the coagulation system, causing pro stages of acute illness, in different disease
arrthythmias. However, it is not practical found microvascular thrombosis and even states. Treatment should be individualised to
during severe hypovolaemia and abdominal thrombohaemorrhagic consumptive disorder suit a particular patient.
compartment syndrome. Sit the patient up and multiple organ dysfunction. Oedema is
45 degrees, connect the patient to a monitor therefore not something to ignore – it should References are available from the author on
that can measure stroke volume and cardiac be prevented or minimised. request.
8 OCTOBER 2017 SAMA INSIDERFEATURES
New code to change promotion of medical devices
SAMA Knowledge Management and Research Department
I
n the September edition of SAMA Insider, end, the underlying commitment from the rebates and discounts or any other pecuniary
the SAMA Communications Department industry members is that they will not offer any advantage which could be inducements to
drew members’ attention to the fact that inducement to any healthcare provider or other use, buy, administer, stock, etc., a product of a
the Department of Health has taken significant customer in order to sell, lease, recommend or company are also not allowed. Limits have been
steps towards formally regulating medical arrange for the sale or lease of their products. placed on the characteristics and monetary
devices and in-vitro diagnostics sold in SA. The code recognises that medical devices value of promotional items as well.
These regulations will impose new respon are marketed in a manner that is distinct from While the nature of devices requires that
sibilities on healthcare providers in terms of the the marketing in the pharmaceutical industry. healthcare providers have the opportunity
law, users and purchasers of medical devices The effective and safe use of medical devices to evaluate their utility and provide feedback
will in future need to be alert to the registration often requires that healthcare professionals if necessary, the code also seeks to clarify the
requirements for such devices, and adhere work closely with company representatives intent and ethical practices around provision
to requirements regarding the keeping of for the purposes of training and development. of products for the purposes of demonstration
registers for implantable devices and mandatory In addition, medical devices can be costly, or evaluation. Essentially these practices are
requirements for the reporting of any adverse representing a large investment to the acceptable only if devices for demonstration or
events associated with medical devices. healthcare-provider purchaser, and may also evaluation are provided free of charge, with no
In addition, and perhaps of more immediate require repeated use, maintenance and repairs inducements to purchase, lease, recommend
importance to medical practitioners, the SA over a long period. or prescribe, use, procure or supply the
Medical Device Industry Association (SAMED) SAMED considers that these circumstances company’s products. Delivery and return of the
launched its Medical Device Code of Ethical create strong interdependent relationships products must also be carefully managed and
Marketing and Business Practice in June 2017. between healthcare providers and the medical- documented, and the quantity and time period
SAMA was party to the launch of the code and is devices industry, which can potentially breed supplied should be suited to the conditions
in support of its principles, values and objectives the risk of manipulation, collusion and unethical necessary for healthcare professionals to
– but we recognise the potential implications incentives to purchase. familiarise themselves with the product.
for our membership and the need to raise The code seeks to facilitate ethical behaviour Infringements of the code are to be ident
awareness of the code and its requirements. across the industry, as well as making provisions ified through a complaints process, and SAMED
While the new regulations for medical devices to enforce code compliance where necessary. considers that by reporting infringements,
and in-vitro diagnostics seek to safeguard the From the point of view of healthcare prof healthcare professionals will have a substantial
quality, efficacy and safety of medical devices essionals, the code seeks to address and enforce role to play in ensuring that the code becomes
in the country, SAMED’s new code seeks to ethical business practices in: an effective instrument. Although fees apply
promote fair and ethical business practices in the • the organisation and sponsorship of events for companies to lodge complaints against
promotion and procurement of medical devices. • the use of promotional items, gifts and one another, no such fees apply to members
SA is no stranger to codes of marketing competitions of the public and healthcare providers. The
practice – the Code of Practice for the Marketing of • contracting with professionals as consultants code includes a detailed schedule of sanctions
Health Products in SA was first published in 2010, • research, royalties and registries which may be issued to companies found to be
through a collaborative effort between actors in • the placement of demonstration or evalu in breach of its provisions.
the pharmaceutical, medical-device, laboratory ation products SAMED is also pursuing alignment with other
and diagnostic and animal-health-product • the conduct of company representatives codes and regulations, including the Medicines
industries. While SAMED was originally involved • the industry utilisation of nursing professionals and Related Substances Act No. 101 of 1965,
in the drafting of this code, it has become to provide patient support. the Public Service Regulations 2016 Code of
apparent over time that the devices industry Conduct and the HPCSA policy on undesirable
requires a specific set of ethical standards to The code will apply across the board to business practices, and guidelines and ethical
apply, hence the development of the new SAMED members and their agents, third-party rules of conduct for practitioners registered
devices code as it stands today. contractors, distributors, contracted event under the Health Professions Act No. 56 of 1974.
The code is a self-regulatory mechanism, organisers and marketers. SAMA is cooperating with SAMED as
and is set to change many existing marketing The code may bring changes to the way a stakeholder to educate and assist in the
practices in the industry. Its underlying princi individual doctors and events are sponsored. dissemination and adoption of the principles
ples stem from the industry’s commitment that Direct sponsorship of healthcare professionals of the code, and the specific requirements for
SAMED members (and medical-device com to attend third-party events will no longer interactions between healthcare professionals
panies in general) have a “social responsibility be permitted from 1 January 2018. Event and the devices industry. We encourage all our
that extends beyond customers to patients and programmes will only be acceptable if they members to familiarise themselves with the
society in general” and from “SAMED’s desire to relate directly to the field of professional code, its principles and guidance.
foster co-operation and shared responsibility expertise of the healthcare professionals
with healthcare professionals for the delivery attending, and if they are held at venues that The full details of the code are available at http://
of effective and efficient healthcare”. To this are not considered tourist or leisure resorts. Gifts, www.samed.org.za/Codes-of-Practice.aspx.
SAMA INSIDER OCTOBER 2017 9Medical Practice Consulting
Inge Erasmus
0861 111 335 | werner@mpconsulting.co.za
MPC offers SAMA members FREE access to the MPC Online Medical
Education platform. SAMA members further have access to Medical
Scholarships through MPC for online CPD, CME and Short Courses as
well as the attendance of international conferences. For more
information, please visit www.mpconsulting.co.za
Mercedes-Benz South Africa (MBSA)
Refilwe Makete
012 673-6608
refilwe.makete@daimler.com
Mercedes-Benz offers SAMA members a special benefit through
their participating dealer network in South Africa. The offer includes
a minimum recommended discount of 3%. In addition SAMA
members qualify for preferential service bookings and other after
market benefits.
SAMA eMDCM | SAMA CCSA
Zandile Dube
012 481 2057 | coding@samedical.org
The first licence of the eMDCM is FREE to SAMA members
in private practice (including limited private practice). As a
SAMA member you must please log on using your
username and password to qualify for this FREE Licence.
Only the first licence is free, additional licences will be
charged.
CCSA: 50% discount of the first copy of the Complete CPT®
for South Africa book.
Tempest Car Hire
MEMBER BENEFITS
Corinne Grobler
083 463 0882 | cgrobler@tempestcarhire.co.za
SAMA members can enjoy discounted car hire rates with
Tempest Car Hire.
Tracetec
Shaun Soares
073 299 0874 | 011 793 5431 | shaun@tracetec.net
‘Simplicity is the Ultimate Sophistication!”
Tracetec in partnership with SAMA are pleased to offer
members a State of the art Wireless Recovery Solution for
their beloved assets at an exclusive membership
discounted rate.
V Professional Services
Gert Viljoen
012 348 3567 | gert@vprof.co.za
10% discount on medical practice bureau service through
V Professional Services.
Xpedient
Andre Pronk
+27 83 555 2885
Sales – 086 1973 343 | andre@xpedient.co.za
Xpedient’s goal is to enable Medical Specialists to focus on their core
competencies and allow us to assist them in making their business a
success.
As a SAMA member you qualify for a complimentary preliminary
business assessment specific to your practice to the value of R 5000 12/09/2017FEATURES
A new age of junior doctors: Unscripted
Dr Farah Jawitz, JUDASA chairperson of Western Cape branch
A
t the Junior Doctors Association of manager showed attendees the array of
SA (JUDASA)’s recent meeting, Dr rooms showcasing original equipment and
Mohammed Dalwai said: “Most junior instruments from the hospital complex. Dr
doctors enter the profession with the idea that Mohammed Dalwai and Dr Vanessa Naidoo
they need to finish medical school, internship, both later shared their experiences of joining
community service, do some medical officer the international organisation Doctors
time, become a registrar, specialise, become a Without Borders/Médecins Sans Frontières.
junior consultant, become a senior consultant, This served as a perfect backdrop against
become a professor or head of department and which to launch the reignition of the branch
then … well, eventually die.” However, it didn’t as it searches for ways to build a holistic
take much for Dr Dalwai to convince those community of junior doctors who can engage
attending the first of JUDASA Western Cape’s on challenges affecting the healthcare sector.
“Doctors Unscripted” series that a medical Having recently been instrumental in
career often presents a host of interesting and facilitating the transition from paper-based
unexpected opportunities. This was the first to online internship and community-service
of the committee’s open meetings, a chance applications, as well as the reduction of
for members, non-members and various continuous working hours for interns, it is
stakeholders to brainstorm how junior doctors with great anticipation that the branch hopes
as individuals and groups can use their careers to build on this momentum in the next few
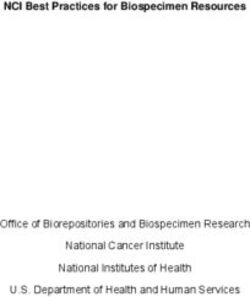
to make a difference. months to inspire a group of socially conscious Dr Mohammed Dalwai, outgoing president
of Doctors Without Borders/Médecins Sans
Juxtaposing the old with the new, the junior doctors. As Dr Naidoo reflects in her Frontières (MSF) SA, has gained vast experience
event was held at the Cape Medical Museum biography: “As doctors we have a responsibility in high-conflict zones since 2011. He has
on the original Somerset Hospital complex to be the voice of our patients and advocate worked in Pakistan, Libya, Northern Syria, Sierra
Leone, Haiti and Afghanistan. In 2012, he was
grounds, where the audience was treated for access to quality healthcare and the recognised on the Mail & Guardian list of Top
to a tour of the museum. The museum preservation of human dignity in all contexts.” 200 Young South Africans
At the Cape Medical Museum, left to right: Dr Farah Jawitz, the incoming chairperson of the Western Cape branch, who introduced the “Doctors
Unscripted” series and outlined the goals of the branch over the next few months with Zahid Badroodien, Maleeka Abrahams-Kahaar and Masudah
Paleker
SAMA INSIDER OCTOBER 2017 11FEATURES
What is the “One Health” approach?
Bernard Mutsago, SAMA health policy researcher
T
he “One Health” approach recognises and many other organisations that have stimulated by the growing antimicrobial
that the health of humans, animals and a special focus on and role in the human- resistance. The first One Health Conference
the environment is interdependent, and animal-ecosystems interface. in Africa was held on July 14 -15, 2011 in
becoming more so under the contemporary The first International One Health Con- Johannesburg. Locally and regionally, the
waves of urbanisation, globalisation, climate gress was held in February 2011 in Melbourne, One Health agenda is being peddled by
change and global biosecurity threats. One Australia, and the second in 2013 in Bangkok, a number of key scientific, educational
Health is the collaborative effort of multiple Thailand. In some parts of the world, One and professional bodies, including the
health-science professions, together with Health has gained so much currency that Southern African Centre for Infectious
their related disciplines and institutions – One Health Day was successfully launched in Disease Surveillance, the National Institute
working locally, nationally, and globally – to November 2016 as an international campaign, for Communicable Diseases (NICD), the
attain optimal health for people, domestic co-ordinated by the One Health Commission, NICD’s Centre for Emerging Zoonotic and
animals, wildlife, plants and our environment. the One Health Initiative Autonomous pro Parasitic Diseases, the University of Pretoria,
Trackable to as far back as the era of bono Team and the One Health Platform the SA Veterinary Council and the National
Hippocrates, in his treatise On Airs, Waters, Foundation. Zoological Gardens of SA. Recently, the twin
and Places, One Health is a unifying concept medical and veterinary associations in SA,
that aims to bring together human healthcare SA and the African region namely SAMA and SAVA (the SA Veterinary
practitioners, veterinarians and public- and SA is an agro-exporting nation, and is consi- Association), respectively, have become
environmental-health professionals. Over the derably dependent on livestock productivity for more interested in and visible on the One
centuries, the animal-human-environment subsistence. Zoonotics are neglected diseases Health agenda.
disease aetiology has been perpetuated in SA, despite their significant impact on the
by various physicians, epidemiologists and health of humans. Focus is disproportionately Current and emerging
veterinarians, and in the late 19th century, placed on HIV/AIDS. Zoonotic diseases are infectious diseases
German physician and pathologist Rudolf not prioritised at a political level, and there is The human-livestock-wildlife relationship
Virchow (1821 - 1902) coined the term limited capacity for surveillance. The medical sustains and spreads the zoonotic pathogens
“zoonosis”. curriculum does not adequately teach zoonotic that have caused the majority of emerging
Today the facts and terms of zoonotic diseases, resulting in doctors misdiagnosing infectious disease in the past few decades,
transmission have become clearer – albeit still zoonotics and often confusing their symptoms especially in the tropics, such as Ebola, the
poorly understood. Zoonoses, also known as with malaria symptoms. There is only one Zika virus, Middle East respiratory syndrome
zoonotic diseases, are infectious diseases that veterinary school in the country (at the (MERS), influenza H1N1 and H5N1, avian
are transmittable from living animals (wild and University of Pretoria), whose annual graduate influenza, severe acute respiratory syndrome
domestic) to humans, or vice versa in some output has recently risen from a paltry 130 to (SARS), food- and waterborne illnesses and
instances. The word zoonoses is derived from 190 per annum. Vaccination campaigns are a range of antimicrobial-resistant bacterial
Greek words zoon (animal) and nosos (disease). sometimes carried out in SA, mainly in rural diseases such as multidrug-resistant and
The World Health Organization (WHO) defines areas, for major zoonotics like rabies, but this extensively drug-resistant tuberculosis
zoonoses as “diseases and infections that are is usually in response to reports of outbreaks (MDR-TB and XDR-TB). Globally, animal-
naturally transmitted between vertebrate rather than as a routine control strategy. derived diseases are a big threat to human
animals and humans”. Interprofessional co-ordination between health. It is known that, worldwide, at least
The term One Health was introduced medical and veterinary professionals is lacking, 75% of emerging infectious diseases of
in the early 2000s as a concept that swiftly and there is a scarcity of epidemiological data. humans (including Ebola, HIV and influenza)
transformed into an approach, and is now The Animal Diseases Act No. 35 of 1984 and have an animal origin. Zoonotic diseases
regarded by some as a movement. The related regulations deal with animal diseases are caused by a range of pathogens such
approach is backed by multiple international and prescribe the necessary control schemes in as viruses, bacteria, parasites and fungi.
structures and organisations, such as the One SA. The country has experienced the ravages of In the bacteria family, for example, over
Health Commission, One Health Initiative, climate change and the associated shift in the 200 bacterial zoonoses are known. The
One Health Initiative Task Force, One Health range of some infectious-disease vectors: for most problematic zoonotics in SA are (in
Initiative Autonomous pro bono Team, the example, the geographical malaria zone is likely their order of severity): brucellosis, rabies,
European Commission, the US Department to expand to non-malaria-endemic provinces. TB and food-borne zoonotics. There is no
of State, US Department of Agriculture, US Border communities are particularly vulnerable treatment for Brucella-infected animals, so
Centers for Disease Control and Prevention, due to the easy migration or mobility of wild the “test-and-slaughter” policy is applied
the World Bank, World WHO, Food and and domestic animals, human beings, disease for the control of brucellosis, to the chagrin
Agriculture Organization of the United vectors and food products. not only of SA commercial farmers, but also
Nations, World Organisation for Animal A number of SA and other African insti- local communal farmers, for most of whom
Health, United Nations System Influenza tutions have awakened to the One Health livestock ownership is a form of wealth and
Coordination, some universities and NGOs approach. In SA, this has in part been livelihood.
12 OCTOBER 2017 SAMA INSIDERYou can also read