REVOLUTIONARY GOVERNMENT OF ZANZIBAR - EPI/MOHSW ZANZIBAR July 2009. COMPREHENSIVE MULT YEAR PLAN - ZANZIBAR 2010
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

REVOLUTIONARY
GOVERNMENT OF ZANZIBAR.
COMPREHENSIVE MULT YEAR PLAN -
ZANZIBAR
2010 – 2014
EPI/MOHSW ZANZIBAR
July 2009.TABLE OF CONTENTS
Acronyms And Abbreviations 3
Executive Summary 4
1.0 Background 4
1.1. Introduction .........................................................................................................................................4
1.2. Location And Surface Area ............................................................................................................5
1.3 Administrative Structure ...............................................................................................................5
1.4 Climate ....................................................................................................................................................5
1.5 Population Projection 2008..........................................................................................................5
1.6 Economy.................................................................................................................................................6
1.7 Socio-Economic Status .................................................. Error! Bookmark not defined.
1.8 Health Service Delivery...................................................................................................................7
1.9 Linkage Of Epi To Moh ...................................................................................................................8
1.10 Number Of Health Facilities By Districts................................................................................8
1.11 Number Of Health Facilities Offering Immunization Services ....................................8
1.12 Users’ Fees And Immunization....................................................................................................8
2.0 Epi In The Context Of Global And National Priorities 9
2.1 Global Priorities..................................................................................................................................9
2.2 Who African Regional Strategic Plan For Epi.......................................................................9
2.3 Epi In The Context Of Global Priorities ...................................................................................9
3.1 Routine Immunization .................................................................................................................11
3.2 Cold Chain And Other Epi Logistics .......................................................................................12
3.3 Advocacy, Communication And Social Mobilization......................................................13
3.4 Capacity Building ............................................................................................................................13
3.5 Targeted Disease Initiative And Disease Surveillance..................................................14
3.5.1 Polio Eradication........................................................................................................................14
4.0 New Vaccine 20
iiACRONYMS AND ABBREVIATIONS
1. AD --------------------------- Auto –disable (syringe)
2. ADB ------------------------- African Development Bank
3. AEFI------------------------- Adverse Event Following Immunization
4. AFP-------------------------- Acute Flaccid Paralysis
5. BCG ------------------------- Bacillus Calmette Guerin
6. CMS ------------------------- Central Medical Stores
7. CFC-------------------------- Cloro –fluoro- carbon
8. DHMT ---------------------- District Health Management Team
9. DHO------------------------- District Health Officer
10. DMO ------------------------ District Medical Officer
11. DTP – HB ------------------ Diphtheria, Pertussis, Tetanus and Hepatitis B
12. DQS- ------------------------ Data quality self-audit.
13. EPI -------------------------- Expanded Programme on Immunization
14. FSP -------------------------- Financial Sustainability Plan
15. GAVI------------------------ Global Alliance for vaccines and immunizations
16. GDP------------------------- Gross Domestic Product
17. Hib---------------------------Haemophilus influenzae type b
18. HMIS------------------------ Health Management Information System.
19. LP gas ---------------------- Liquid Propane gas
20. MCH------------------------- Maternal and Child Health
21. MDVP----------------------- Multi dose Vial Policy
22. MLM------------------------ Mid Level Management
23. MNT------------------------ Maternal and Neonatal Tetanus
24. MNTE---------------------- Maternal and Neonatal Tetanus Evaluation
25. MOHSW -------------------- Ministry of Health and Social Welfare
26. NIDs ------------------------ National Immunization Days
27. NT --------------------------- Neonatal Tetanus
28. OPD ------------------------- Out Patient Department
29. OPV ------------------------- Oral Polio Vaccine
30. PIU -------------------------- Program Implementation Unit
31. PHCU ----------------------- Primary Health Care Unit
32. SIAs ------------------------- Supplemental Immunization Activities.
33. SNIDs ----------------------- Sub National Immunization Days
34. TBA----------------------- -- Traditional Birth Attendant
35. TT------------------------- -- Tetanus Toxoid
36. UNICEF--------------------- United Nations Children’s Fund
37. UNFPA-------------------- - United Nations Population Fund
38. VVM------------------------- Vaccine Vial Monitor
39. WHA ------------------------ World Health Assembly
40. WHO---------------------- World Health Organization
41. ZFDB--------------------- Zanzibar Food and Drug Board
42. ZMO---------------------- Zonal Medical officer
3EXECUTIVE SUMMARY
The immunization programme in Zanzibar has it’s the goal of reducing morbidity and
mortality due to vaccine preventable diseases. The programme broad areas of activity
include service delivery, disease surveillance and supplementary immunization activities.
The comprehensive Multi-Year Plan 2010-2014 identified several reasons for poor
immunization performance in different levels. The plan will focus on empowering and
supporting districts and utilizing the opportunity of integrated health services including
introduction of new vaccines such as Pneumococcal in 2010 and rotavirus in 2011.
Although immunization services are among the highly accepted services by the community
in Zanzibar, advocacy and social mobilization remains an essential to maintain it.
Vaccination against EPI targeted diseases is provided in government and private
Reproductive and Child Health (RCH) clinics and the coverage exceeded 80% in 80% of the
districts. The immunization program for Zanzibar aims to achieve and sustain coverage
rate of above 90% for all antigens in 80% of the districts by the end of 2014. However,
vaccine preventable diseases, particularly measles outbreaks, are major challenge for the
implementation of EPI program.
Social mobilization strategies were outlined and will be used to improve access and
utilization of immunization services in the coming five years. The program will also
strengthen its advocacy role in order to put immunization issues as an agenda for political
decision-makers and promote strengthening of routine immunization coverage at all levels.
The main issues that need to be addressed includes:-
• Increasing immunization coverage in low performing districts
• Introduction of new and under-utilized vaccines such as Pneumococcal in 2010 and
Rotavirus in 2011
• Conducting supplemental immunization activities especially for measles in 2011
and 2014.
• Strengthening integrated disease surveillance.
• MNT Validation
• Measles pre elimination
• Polio eradication and implementation of Polio importation preparedness plan.
Injection Safety will continue to be among the priority areas in 2010– 2014.
Non-Polio AFP rate in 2008 reached above 1/100,000. The 2010 – 2014 Comprehensive
Multi-Year Plan, will address more issues in integrated disease surveillance activities by
conducting training of clinicians, community sensitization and advocacy to key
stakeholders. Emphasis will be placed on those silent districts as far as AFP, Measles and
MNT reporting are concerned. Immunization infrastructures in Zanzibar are among the
areas earmarked for improvements in the coming five years. New Freezer room will be
procured and installed and cold chain replacement plan will be implemented in all vaccine
stores. This will also include the expansion of the storage capacity at Zonal vaccine store.
The Ministry of Health through EPI with the support of GAVI, WHO, UNICEF and other
partners have prepared this cMYP with full section on costing, financing and Financial
Sustainability of the programme covering the period of 2010-2014. The Multi year plan has
incorporated the activities earmarked in the previous Financial Sustainability Plan (FSP).
This includes programme costing, financing and future resource requirements activities as
well as advocacy, mobilization of resources from central and local government.
1.0 BACKGROUND
1.1. Introduction
Zanzibar is one of the political entities constituting the United Republic of Tanzania. It
consists of two large Islands, Unguja and Pemba and few sparsely populated islands such as
Tumbatu and Uzi in Unguja, Kojani, Fundo, Shamiani and Makoongwe in Pemba. Zanzibar
has considerable autonomy in her domestic affairs administered through the Revolutionary
Council and the House of Representatives. Although the Health care portfolio for Zanzibar
is not a Union Government matter, there is considerable collaboration with the mainland
on health matters. The Ministry of Health and Social Welfare remains the responsible
agency for health services in Zanzibar.
41.2. Location and surface size
Zanzibar is located in the Indian ocean, about 30km off the east coast of Africa, between
latitude 5 and 7 degrees south off the equator . Zanzibar consists of two islands , Unguja
and Pemba , and several other smaller islands some of which are uninhabited .The island
has an area of 2,654sqkm out of this, Unguja, which is the largest, has an area of 1,666
square kilometers while Pemba has an area of 988 square kilometers.
1.3 Administrative structure
Zanzibar is divided into five administrative regions, three in Unguja and two in Pemba.
Each region is subdivided into two districts, which make a total of ten districts for the
islands. The lowest government administrative structure at the community level is the
Shehia.
1.4 Climate
The climate of Zanzibar is equatorial and humid. The maximum temperatures revolve
around 30oC during the hot season lasting from December to March and minimum
temperatures are approximated at 20oC during the cool season lasting from June to
November. Zanzibar has two main rain seasons, the long rainy period (Masika) during
March to June and short rainy period (Vuli) that starts in October and ends in December.
The humidity is high ranging from 900 – 1000 mm during heavy rain season and 400 – 500
mm during short rainy period. The humidity is slightly higher in Pemba in comparison to
Unguja. Because of the two rainfall peaks, Zanzibar is usually green all the year.
1.5 Population projection 2008
The population of Zanzibar shows an increase from 640,685 in 1988 (1988 census) to
981,754 in 2002 (2002 census). The population is estimated to be 1,193,383 in 2008,
projected from 2002 National Population census. Of this population, under 1year is 47,205
and under 5year is 217,168. The details of the population are shown in Tables 1, 2 and 3
and Figure 1.
Table 1: Census Counts and Inter-censual Growth Rates by Region
Actual Population from Censuses
Inter-censual Growth Rate
(%)
Region 1967 1978 1988 2002 1978 – 1988 –2002
1988
Total 354,360 476,111 640,685 981,754 3.0 3.1
Zanziba
r
North Unguja 56,219 77,017 96,989 136,639 2.3 2.5
South Unguja 39,004 51,749 70,313 94,244 3.1 2.1
Urban West 94,894 142,041 208,571 390,074 3.8 4.5
North Pemba 71,972 106,290 137,189 185,326 2.6 2.2
South Pemba 92,271 99,014 127,623 175,471 2.6 2.3
Source: NBS, Census 2002
Table 2: District Population, Zanzibar 2008.
DISTRICT TOTAL 0 – 11 UNDER 5 UNDER 15
POPULATION MONTHS YEARS YEARS
URBAN 256,543 7,202 35,219 88,064
WEST 202,959 7,600 36,177 89,782
NORTH ‘A’ 99,186 4,277 19,253 45,457
NORTH ‘B’ 66,687 2,511 11,511 27,698
CENTRAL 71,035 2,190 10,402 27,918
SOUTH 36,776 1,055 4,883 13,273
UNGUJA TOTAL 733,186 26,138 118,449 292,192
MKOANI 116,129 5,806 25,946 59,555
5CHAKECHAKE 109,926 5,341 23,920 56,082
WETE 127,923 5,673 25,944 60,364
MICHEWENI 106,219 5,550 23,913 52,645
PEMBA TOTAL 460,196 21,806 99,158 228,646
TOTAL ZANZIBAR 1,193,383 47,205 217,168 520,838
Table 3: Projected population, Zanzibar 2010 – 2014
YEAR TOTAL 0 – 11 UNDER 5 UNDER 15
POPULATION MONTHS YEARS YEARS
2010 1,159,941 50,012 230,650 497,871
2011 1,197,005 51,321 237,471 514,219
2012 1,234,972 52,638 214,254 531,318
2013 1,403,166 53,894 251,005 616,483
2014 1,448,773 55,235 257,739 639,092
1.6 Economy
Macroeconomic policies implemented in the last five years (2003-2007) resulted into
positive growth of the economy from 5.9 percent in 2003 to 6.5 percent in 2007, which is
slightly below the target of 6.6, but 0.5 percent above the growth for the year 2006. GDP
per capita increased from TShs. 284,000 in 2003 to TShs. 518,000 in 2007 while capital
formation given up from 21 percent in 2003 to 38 percent in 2007.
The service component of GDP composition (comprising trade, hotel, restaurants,
transport and communication, among others) constitute the larger part of economic
development in Zanzibar. The sector registered remarkable growth and its contribution to
GDP, revenues, employment generation as well as attracting investment is promising. Its
share to GDP increased to 43.9 percent in 2007, exceeding 43.5 percent recorded in 2006.
The projected economic growth in Zanzibar during 2008 is 6.8 percent, but may not be
attained due to current global financial and economic crisis. However, the current global
financial and economic crisis and Zanzibar power outrage may disrupt the economic
growth in Zanzibar during 2009 and 2010.
In the fiscal year 2006/07 agricultural sector declined as a result of drought.
Investment projects registered by Zanzibar Investments Promotion Authority (ZIPA)
increased from 13 in 2003 to 65 in 2008 with a total value of US$ 1,296.8 million. The
trend of the projects registered is expected to decrease as a result of the world financial
crisis in 2009/2010. ( Zanzibar economic bulletin Vol.2 No.1 january –march,2009)
Income per capita 1990- 2005
Index 1990-1999 2000-2004 2005
GDP at market price (Tshs millions) 189,500 255,600 395,700
Population (Numbers) 725,000 966,400 1,072,000
Per capita income (Tshs) 142,000 263,800 369,000
Per capita income (USD) 157 276 327
Source: OCGS (2005) Socio-Economic Survey 1999 and 2004
6Figure 2: Map of Zanzibar
UNGUJA
PEMBA
1.7 Health Service Delivery
Zanzibar’s public health service infrastructure relies on a fairly dense network of Primary
Health Care Units (PHCU’s), that are meant to serve in principle a population of 3,000 to
5,000; they are divided into two types: PHCU-1 provide basic primary health care services,
while PHCU-2 are supposed to provide the same services, plus professional assistance with
normal deliveries, laboratory services and dental care;
The performance of the health sector in Zanzibar remains unsatisfactory even though
geographical coverage of the health facilities is considered equitably distributed to all
regions and districts, and easily accessible to 95% of the population. The access to health
services is constrained mainly by poor quality of service due to lack of equipment and
qualified staff. Furthermore, health services utilization is associated with socio-economic
conditions. Maternal and child health services in Zanzibar are provided in all health care
facilities in the country.
Traditional birth attendants (TBAs) provide a significant proportion of maternal health
services. It is estimated that there are 2000 TBAs in Zanzibar and they conduct about 40%
of all deliveries.
Almost all Primary Health Care Units (PHCU) provide integrated RCH services including
antenatal care, delivery services, prevention and management of STI and family planning
services. Over 95% of pregnant women in Zanzibar attend clinic for antenatal care, but only
about 60 percent of the them attended by trained personnel and the rest are attended by
traditional birth attendant . Immunization services are offered at all levels. In line with on
going Health Sector Reform (HSR), health services are provided at the following levels:-
Primary (Level I)
This is the lowest level of health care structure. It includes 1st and 2nd Line Primary Health
Care Units (Dispensaries) and Primary Health Care Centers (Cottage Hospitals).
Secondary (Level II)
These are the district hospitals that serve as referral points for the Primary Level health
care facilities.
Tertiary (Level III)
There is only one specialized hospital (Mnazi Mmoja Hospital) located in Unguja Island.
7This hospital provides a full range of specialized services for referred and emergency
conditions. It is also the teaching hospital in Zanzibar.
1.8 Linkage of EPI to MOH
The EPI Programme is housed within the Directorate of preventive Services in the Ministry of Health
and Social Welfare. The main task of the programme is to provide vaccination services to children and
mothers in order to prevent vaccine preventable diseases. The implementation of immunization
services in both Unguja and Pemba zones are coordinated and supervised by Health Management
Teams. Unguja has six teams while Pemba has four. The National level provides supplies, logistics and
technical assistance for the zones and districts.
1.9 Number of Health Facilities by Districts
Zanzibar has about 158 Health facilities distributed by districts as follows:-
Table 6: Health facilities offering immunization service by district, Zanzibar 2008
No. District Total No. of Offering Not offering
Health immunization immunization
facilities services services
1 Urban 18 15 3
2 West 18 15 3
3 Central 22 22 0
4 North A 13 13 0
5 North B 12 12 0
6 South 10 10 0
7 Mkoani 16 16 0
8 Chake chake 16 16 0
9 Wete 19 19 0
10 Micheweni 14 13 0
TOTAL 158 152 6
1.10 Number of Health facilities offering Immunization services and outreach per
District
Out of 158 health facilities, 152 (96%) provide immunization services. In total, there are 68
outreach sessions conducted monthly in all districts of Zanzibar. These services are
supported by either National or DHMTs. However health facilities conduct their own
outreaches according to their needs by utilizing available resources such as bicycles etc.
The minimum number of outreaches per district in a month is 3 while the maximum is 10.
About 95% of the planned outreaches were conducted in 2008 through DANIDA support.
1.11 Users’ fees and immunization
EPI services are provided free of charge to all eligible children and women of child bearing
age in both Government and private health facilities.
82.0 EPI IN THE CONTEXT OF GLOBAL AND NATIONAL PRIORITIES
2.1 Global Priorities
Expanded Programme on Immunization is considered as one of the global health priorities
as depicted in the global coverage goals. The coverage in Zanzibar has reached the global
set target of over 80% of districts to have DTP-HB3 coverage of 80% in 2008. In the coming
five years, the EPI programme is envisaged to raise the national coverage of DTP-HB3 from
86 % to 95% and above so as to meet the global set goals including WHA 1989, GAVI 2002
and UNGASS 2002. EPI contributes substantially to the achievement of the Millennium
Development Goal 4 which aims at reducing childhood mortality with a target of reducing
the under five mortality rate by two-thirds, by the year 2015.
The Global Immunization Vision and Strategies provides a strategic framework to guide all
partners in immunization, making the case for sharing linkages between immunization and
other health interventions and addressing the need to overcome system wide barriers that
go beyond immunization and affect the whole sector.
2.2 WHO African Regional Strategic Plan for EPI.
In implementing EPI activities, Ministry of Health Zanzibar is also aware and committed to
the African region strategic plan with the vision to improve the health of children through
the eradication of polio and the control of other vaccine preventable disease in the context
of health system strengthening. To attain this vision, it is expected that
At least 80% of countries attain DTP3 coverage of at least 80% in all districts.
All countries attain 100% immunization safety
All countries will have sustainable funding for EPI.
All countries attain Polio Eradication
Attainment of full regional certification.
Attain measles pre-elimination goals
Attain Neonatal tetanus elimination.
2.3 EPI in the context of Global priorities
2.3.1 National Development Plans
The government of Zanzibar is committed to ensuring that high quality and equitable
health care services are available to all Zanzibaris on a sustainable basis. In this context, the
government of Zanzibar accords special attention to the prevention, control and where
possible, the elimination of communicable diseases that are of public health importance as
well as safe motherhood and child survival.
The Zanzibar Poverty Reduction Plan (ZPRP 2002–2005) includes health related issues
aimed at improving the health of women and children. Specific activities geared towards
improving the health of women and children include strategies aimed at increasing
immunization coverage in children and women of child bearing age and creating equal
opportunities for access to basic and essential quality health care.
2.3.2 Vision 2020
The Revolutionary Government of Zanzibar has embarked on a plan of the Zanzibar
Development vision 2020 whose overall objective or goal is to eradicate absolute poverty
in the society.
The Zanzibar development vision 2020 further emphasizes that the eradication of poverty
will require, among others, sound macroeconomic managements policies aimed at creating
a stable environment for growth (including investments and trade) that will subsequently
promote sustainable livelihood through chosen productive employment and work and the
provision of basic social services including health care services. It has remained a point of
reference for subsequent development policies, strategies and programmes for Zanzibar.
2.3.3 ZSGRP (2007 – 2010).
In 2000, Zanzibar launched the Zanzibar Development Vision 2020 which gives social, political,
cultural and economic philosophy up to the year 2020. The thrust of the vision is eradication of
absolute poverty and attain sustainable development. In line with that, the first three-year Zanzibar
9Poverty Reduction Plan (ZPRP) launched in 2002 from which some significant achievements were
recorded after its implementation. However, there were also challenges highlighted by
stakeholders during the ZPRP review process which were taken as strength towards development
of this strategy; The Zanzibar Strategy for Growth and Reduction of Poverty (ZSGRP) The ZSGRP
document forms part of strategies to implement the long term development plan, the Vision 2020.
The four-year Zanzibar Strategy for Growth and Reduction of Poverty (ZSGRP) known as
Mkakati wa Kukuza Uchumi na Kupunguza Umasikini Zanzibar (MKUZA) in its Kiswahili
acronym is the second generation of national development framework to implement Vision
2020. ZSGRP is in line with Millennium Development Goals (MDGs) and other international
agreed commitments and targets. The focus is on the reduction of both, income and non-
income poverty; and ensure the attainment of sustainable growth.
The ZSGRP offers recommendations or interventions on how the stakeholders – the Government,
the Non State Actors including Development Partners, the Private Sector, Civil Society
Organizations and the Community – can engage their actions and approaches to significantly
enhance economic growth and thus poverty reduction. The ultimate objective is to achieve high
standards of social well being to the citizens.
The Zanzibar Strategy for Growth and Reduction of Poverty concentrates on strategic
interventions aimed at
i. Reducing income poverty
ii. Improving human capabilities, survival and social wellbeing
iii. Containing extreme vulnerability (including diseases)
2.3.4 MOH Priorities
Health Sector Reforms
In 2002, Zanzibar initiated a Health Sector Reform under the guidance of the Zanzibar
Health Sector Reform Strategic Plan I 2002/03 – 2006/07. The reform was seeking to
decentralise planning, prioritising and integration of services to district level. In addition, it
aims at ensuring the availability of equitable high quality health care services, which focus
on priority diseases or burden of diseases and according to an essential health care
package. The essential health care package focuses on the principles of primary health care
(PHC) approach based on the strengthening health delivery at the community level and in
Primary Health Care Units (PHCUs) and Centres (PHCCs).
A 2004 assessment of Zanzibar Health Sector Reform Strategic Plan I (ZHSRSP I) concluded
that “in general, ZHSRSP I (2002/03 –2006/07) has not been implemented as programmed
and failed to guide planning of Ministry of Health and Social Welfare (MOH&SW) and
stakeholders activities.” The current document, a more comprehensive and feasible
ZHSRSP II (2006 –2010), has been developed a year before the end of the first plan period
in order to address this concern, and to enable the sector programme to run concurrently
with the new Zanzibar Strategy for Growth and Poverty Reduction (MKUZA).
Eleven areas have been identified within the HSSP which includes:
i. Improvement of organization and management of health services
ii. Human resources development
iii. Strengthening health services delivery
iv. Health sector financing and mobilization of resources
v. Research development
vi. Health legislation
vii. Pharmaceutical, medical supplies and equipments
viii. Strengthen secondary and tertiary referral hospital
ix. Public and private Partnership in Health services delivery
x. Social services/welfare
xi. Donor coordination, advocacy and management of the reform process.
103.0 IMMUNIZATIO PROGRAMME COMPONENTS
3.1 Routine immunization
3.1.1 Immunization coverage 2004 - 2008
EPI plays a major role in contributing to the achievement of the Millennium Development
Goal 4 which aims at reducing childhood mortality with a target of reducing the under five
mortality rate by two-thirds, by the year 2015. The immunization program for Zanzibar set
a goal of achieving immunization coverage rate of 90% nationally for all antigens and over
80% in every districts by the end of 2014.
Several strategies have been outlined and will be used to improve access and utilization of
immunization services in this year. Also the programme aims at reinforcing support to all
districts in order to make sure the desired coverage is achieved and sustained.
Immunization coverage for Zanzibar 2004 – 2008
Vaccine 2004(%) 2005(%) 2006(%) 2007(%) 2008(%)
BCG 128.2 125 115 101.4% 116.3%
OPV 0 51.4 53.3 46 51.8% 57.1%
DTP Hep B3 88.8 85.7 86.0 78.4% 85.3%
Measles 89.6 93.4 88.8 87.7% 91%
OPV3 88.0 85.0 85.0 78.0% 81%
TT2+ 72.9 67 60.0 60.3% 63.6%
SOURCE: MoHSW ZANZIBAR
The plan is to maintain and sustain high immunization coverage of more than 90%. This
can be achieved by support the low performing districts ( North A and North B in Unguja
and Mkoani, Chakechake and Micheweni in Pemba ), improve data quality and eliminate
MNT in the high risk districts. The problem of high measles coverage compared to DTP-
HB3 coverage will also be addressed.
Table 1.2: Immunization Schedule in Zanzibar
Antigen Age
OPV0 At birth up to 14 days
BCG At birth or first contact
OPV1, DTP-HepB-Hib 1,PCV1 6 Weeks of age Zanzibar
OPV2, DTP-HepB- Hib2, PCV2 10 Weeks of age Zanzibar
OPV3, DTP-HepB-hib3, PCV3 14 Weeks of age Zanzibar
Measles 9 Months of age
Vitamin A – 1st dose 9 Months of age
Vitamin A – 2nd dose 15 Months of age
Vitamin A – 3rd dose 21 Months of age
TT 1 First contact
TT 2 1 Month after the 1st dose
TT 3 6 Months after the 2nd dose
TT 4 1 Year after the 3rd dose
TT 5 1 Year after the 4th dose
3.1.2 Dropout rates
Dropout rate of DTP-Hb1-DTP-Hb3 between 2004 and 2008 is within the acceptable rate
of below 10%. However, DTP-Hb1–Measles dropout rate remains questionable, since data
collected from health facilities shows the large number of children vaccinated against
Measles compared to those vaccinated with DTP-HB 1 vaccine which results in negative
drop out. This indicates the possibility of problems in the data collection at health facility
level where all immunization data are collected and sent to higher level.
Hence DQS will be among the most priority activities in the coming 5 year (2010 – 2014) so
as to verify and improve the quality of data
Table 8: Dropout rate (DTP-HB1-DTP-HB3), Zanzibar 2004-2008
11Year DTP Hb1 DTP Hb3 Dropout rate (%)
2004 38,310 37,222 3
2005 39,314 36,886 6.2
2006 39,479 38,171 3.3
2007 38,686 35,954 7.1
2008 42,594 40,246 5.5
Table 9: Drop Out Rate (DPT-HepB1-Measles) 2004-2008
Year DPT-HepB1 Measles Dropout rate (%)
2004 38,310 37,581 1.90
2005 39,314 40,237 -2.35
2006 39,479 39,441 0.10
2007 38,686 40,211 -3.94
2008 42,594 42,965 -0.87
SOURCE: MOHSW ZANZIBAR
3.2 Cold chain and other EPI logistics
There are 152 RCH clinics that offer immunization services, among them 96 (66%) RCH
clinics have refrigerators. Proportion of Health facilities with refrigerators has increased in
2007 after installation of solar Fridges in most of the small hard to reach islands..
In some areas health facilities are too closer hence it will not cost effective to put
refrigerator in each of the RCH clinic. In these areas one refrigerator serves more than one
RCH clinic, where the health facility with no refrigerator collect their vaccines from nearby
health facilities.
At health facility level, only 10% of the cold chain equipments remain non CFC free and
100% of district stores contain CFC free refrigerators. The programme has planned to
equip the remaining health facilities with CFC free equipment such as refrigerators, cold
boxes, vaccine carriers etc. Programme also intends to provide training on maintenance of
such equipments at all levels.
Three out of four districts in Pemba have started to use LP Gas Fridges as the alternative
source of energy since the electricity in Pemba is not constant and kerosene refrigerators
are not working properly. The plan is to continue using LP Gas fridges in all districts of
Pemba.
3.2.1 Vaccine Stores
3.2.1.1 Central Vaccine Store
At the moment different programmes are storing their products and supplies in the Central
Medical Stores including vaccines. Management of the Central Medical stores is greatly
incapacitated in terms of providing the required logistics support to programmes.
The central vaccine store in Zanzibar is within the Central Medical Store (CMS) in the
Ministry of Health. Operational and management of CMS is in collaboration between EPI
and Drug Management Unit (DMU).
The Central vaccine store is equipped with compression refrigerators and freezers and
walk-in cold room. The existing EPI vaccine store has small storage capacity which is
1200lts (refrigerators) and 600lts (freezers). This capacity is not adequate compared to the
increase in the population and the amount of vaccines to be stored especially the
introduction of new vaccines. Thus, there is a need to install new cold and freezer rooms
that will at least occupy a volume of 2000lts .
3.2.1.2 Zonal Vaccine Store
The introduction of Pneumococcal vaccine and Rotavirus vaccine has implication for
greater storage space. Therefore, there is a need to extend the storage services at Zonal
12levels so as to decongest the Central Medical Store and ensure required logistic support is
provided to the programmes.
The Zonal store in Pemba is equipped with compression refrigerators and freezers as well
as ice pack freezers. The programme planning to replace all non CFC free equipments in
the coming five years.
Both National and Zonal stores have generators for power back up.
3.2.1.3 District Vaccine Store
There are ten district vaccine stores that are equipped with compression refrigerators and
sibir . These Sibirs are old and non CFC Free. The replacement of CFC containing
refrigerators to CFC free refrigerators is among the activities in this plan The plan is to
equip all district stores with CFC Free equipments by the year 2014.
.
3.2.1.4 Health Facility
There are 96 health facilities with refrigerators in Zanzibar. All refrigeratotor in Unguja
zone run by electricity while more than 75% in Pemba zone run by LP gas. The remaining
25% of Pemba refrigerators are run by kerosene and unreliable electricity that
necessitates the use of kerosene. The replacement plan has been in place since year 2006
and the aim is to replace the 100% of Pemba refregirators with LP gas by 2010
The models of refrigerators available at health facility are RCW 50EK, RCW 42EG, and RCW
42EK.Sibir V110EG, Sibir V170EK, Sibir V170EG
3.3 Advocacy, Communication and Social Mobilization
One of the five components of the immunization system is advocacy and communication.
Effective communication helps to mobilize resources for the immunization programme and
encourages other sectors and organizations from various actors and the community to
participate in immunization activities. EPI will continue to maintain dialogue not only with
service providers but also with communities, including care givers, traditional healers,
politicians, religious leaders and other influential people to enhance their understanding of
the importance of immunization. Social mobilization activities in 2006- 2010 were very
limited due to scarcity of resources. Community sensitization meetings were carried out in
only villages where the outbreaks of vaccine preventable diseases occurred (i.e. Measles).
Spot announcement, TV/Radio Programmes and production of IEC materials were only
conducted during mass campaign
Advocacy for routine EPI will be conducted at National, district as well as Village (Shehia)
levels during the mass (measles) campaign and introduction of new vaccines. Furthermore
an EPI communication guideline has been developed and finalized in collaboration with
Health education unit, ZHMT, IMCI and Save the Children. Special TOT conducted for all
DHMTs to equip them with knowledge and skills in order to facilitate their work in their
respective districts. In order to strengthen communication and advocacy at all levels, the
programme will sensitize districts to incorporate advocacy and communication activities in
their district comprehensive plans.
Much emphasis also will be on social mobilization and public education at the lower levels
about immunization to ensure high community participation awareness on immunization .
Among the social mobilization activities that will be designed and implemented include the
following:
• Routine sensitization meetings with community, political and religious leaders
as well as other influential people.
• Weekly health programme in Radio and TV
• Production and distribution of IEC materials (Posters, leaflets etc).
3.4 Capacity building
3.4.1 Refresher training, MLM, Pre-service institution strengthening
Over the course of time, district and health facility staff have been exposed to different
trainings such as:- refresher training on data management, cold chain, data quality self
assessment and disease surveillance. Also DHMTs had other opportunities such as micro
planning training, social mobilization and communication training.
13Although refresher trainings are conducted, the time allocated is not adequate to cover all
the necessary aspects of EPI skills. Refresher trainings for all service providers are done
once yearly, where most of time newly employed health workers miss the opportunity of
being trained on time. Also health workers turnover causes unequal distribution of health
staff among districts leading to some districts running shortage of staff. It is the plan of EPI
programme in the coming five years to continue conducting refresher training to DHMTs
and health facilities to overcome the problem of unskilled health workers and ensure the
districts officers uses the opportunity of supervision by coaching and provide on the job
training. Human resource development and capacity building at all levels is essential.
National level capacity has improved by its five staff being trained on EPI Mid-Level
Management (MLM) course and almost all national staff has been exposed in to various
trainings such as data management and epidemiology, Data Quality Self Assessment,
retreats etc.
The responsibility of Central EPI is to coordinate local trainings at district and health
facility levels with technical assistance of partners (WHO, UNICEF, GAVI etc).
One of the challenges in training districts and service providers the limited funds provided
for training..
EPI also facilitate pre-service training on EPI subjects at the college of Health sciences on
specific programmes prepared by the college. These involves clinical officers, Health
officers, PHNB and Community Health Nurses In order to ensure sustainability and equip
the college to deliver EPI education, one tutor from the college of Health sciences has
received MLM training. There is a plan to adopt MLM modules and conduct training at the
district which will include also some tutors from Collage of health sciences in this current
strategic plan.
3.5 Targeted Disease initiative and Disease Surveillance
3.4.2. 3.5.1 Polio Eradication EPI national level capacity strengthening.
AFP Surveillance
AFP surveillance is an integral part of the Polio Eradication effort. Any case of AFP in
children younger than 15 years should be reported. Investigations should be initiated as
soon as possible, including the collection of two stool specimens, preferably within 14 days
of onset of paralysis. All Stool specimens are sent to EPI Central office Dar-es-salaam, using
the reverse cold chain.
Follow-up examinations to all cases to define residual paralysis (leftover) were done at
least 60 days after onset of paralysis. Delays in conducting 60 days follow-up made the final
classification of cases to take longer time than the time recommended. AFP surveillance
detection rate is improving (greater than 1/100,000 pop under 15 yrs) in most of the
districts.
Central and North B districts reported at least one case of AFP each in the past five years
while Chake, district has never reported any AFP case for last five years.
Availability of AFP surveillance funds and transport (vehicles and motorcycles) assisted to
stimulate the proper active case search in most of areas in Zanzibar.
3.5.1.1 Polio Certification
In the United republic of Tanzania the polio eradication activities are monitored under one
system for both Tanzania mainland and Zanzibar. These includes the formation of polio
eradication committees and polio surveillance data base.
United Republic of Tanzania was among the 8 countries who presented the polio
certification document in the African Regional Certification meeting conducted in July 2004
in Dar es Salaam, Tanzania. How ever the country was not certified as polio free. The next
presentation was in 2006 in Uganda and tTanzania document was deffered and requested
to conduct surveillance review country wide . The next presentation of the document is
planned to take place in October 2009
3.5.1.2 Laboratory Containment
The Ministries of Health (Mainland and Zanzibar) inaugurated and oriented the National
14Polio Task Force members on 10th of October 2003, marking the beginning of the
implementation of Wild Polio virus containment activities in the country. The Task Force
has identified the following activities as priority activities for Laboratory containment of
Wild Poliovirus:
Laboratory Survey to identify laboratories storing Poliovirus and potentially poliovirus
infectious materials.
National Inventory of all laboratories holding stocks of Poliovirus materials.
Storage of Poliovirus of Scientific value in secure laboratories.
Destruction of all unneeded Poliovirus and potentially Poliovirus infected materials.
The Task force has successfully managed to conduct a Laboratory survey in 60
Laboratories in the country and managed to identify the Laboratories storing Poliovirus or
potentially polio virus infectious materials. List of all Laboratories holding the stocks were
prepared. The recommendations were provided on how to work or destroy unneeded
poliovirus or infected potential infectious materials. The Laboratory containment
document formed part of the Tanzania Polio certification document presented in the ARCC
meeting.
3.5.1.3 Wild Polio virus Importation and preparedness
United Republic of Tanzania has prepared a wild poliovirus importation preparedness and
response plan. The plan identified high risk areas including bordering districts, low OPV3
coverage and districts with port of entry. Urban, West, Micheweni, North B and Mkoani
were identified. The rationale for the preparedness plan is to enable Tanzania maintains
polio free status and appropriate response towards wild polio virus importation.
3.5.1.4 Task Force Meetings (Polio committees meetings)
United Republic of Tanzania formed four committees which include: - National Polio
expert, National Certification, National wild polio virus importation and preparedness and
National Laboratories containment committees. These committees were formed by the
Ministries of Health to provide technical support for polio eradication activities.
3.5.2 Measles pre elimination activities
3.5.2.1 Supplemental Immunization Activities.
Measles mass campaign is a second strategy for measles control and also an opportunity to
reach those children who were not reached in routine immunization services.
Measles mass campaigns in Zanzibar were conducted from 1999 to 2008.
In the first two years (1999-2000), the campaign targeted children under five years of age
and covered all districts in Zanzibar. While in 2001 and 2002, the campaigns were for
children from 9 month to 15 years of age, in 2005 the measles campaign covered children
aged 9 months to 5yrs. The coverage increased from 67% in 1999 to 92% in 2002 and 84%
in 2005. The most recent measles SIAin 2008 vitamin A and mabendazole targeted the
under 10years acheved 86% nationaly
Table 10: Measles mass campaign results, Zanzibar 1999-2008
YEAR TARGET. VACCINATED. COVERAGE %.
1999 100,598 67,440 67
2000 51,250 36,977 72.2
2001 232,271 175,950 75.7
2002 204,669 189,303 92
2005 143,328 120,408 84.0%
2008 346,081 299,445 86.7%.
3.5.3 There is need to sustain the results obtained especially for the low performing
districts and the hard to reach populations. Strengthening the case search can
facilitate higher performances. Zanzibar is planning to accelerate Measles pre
elimination activities
3.5.3.1 Case based surveillance
Zanzibar started measles case based surveillance after finishing a country wide measles
campaign for under fifteen years in 2002. With this new strategy of measles control, a
15single measles suspected case is considered as an outbreak. Therefore, a blood sample for
each suspected case is collected up to a maximum of ten cases and the outbreak
investigated.
3.5.3.2 Role of Laboratory
The Virology Laboratory in Muhimbili National Hospital is responsible for testing blood
specimens of suspected measles cases from Zanzibar. Serum samples are sent to EPI
central office Dar Es salaam under reverse cold chain.
3.5.4 NNT Elimination
The goal of neonatal tetanus (NT) elimination was adopted by the WHO in 1988 and by the
World Summit for Children in 1990. In June 2000, fifty seven countries failed to meet the
target of eliminating Neonatal Tetanus. Zanzibar is one among the 57 countries that have
not yet eliminated NT. The goal of maternal and neonatal tetanus (MNT) elimination by
2005 was recently declared jointly by UNICEF, WHO, and UNFP.
3.5.4.1 High risk district activities
In 2000, maternal neonatal tetanus (MNT) elimination status review was conducted in all
10 districts of Zanzibar which found Wete and Micheweni to be MNT high risk Districts.
Following the results of the assessment three rounds of MNT campaigns were held in
Micheweni and Wete Districts in December 2001, January and July 2002. Generally, the
coverage was low, this is due to inadequate social mobilization and rumors.
The last MNT high risk assessment was conducted in 2008 in all districts using MNT
surrogate indicators. The review team found that three districts (Micheweni, Chakechake
and Mkoani) remained a high risk districts based on the NNT incidence and other low
surrogate indicators detected.. Recommendations were made to all districts in order to
achieve elimination status. The three high risk districts recommended conducting MNT
SIAs in 2008
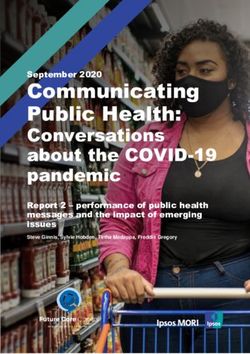
Reported Neonatal Tetanus cases and deaths from 1999 - 2007
18
16
16
14
12
10
10
8 8
CASES
8
DEATHS
6 5 5
4 3 3
2 2 2
2 1
0
0
1999 2000 2001 2002 2003 2004 2005 2006 2007
3.5.4.2 Case investigation
Neonatal tetanus case based surveillance started in 2004, which means all neonatal deaths
investigated. However, investigation of neonatal deaths is still a big challenge in many
areas of Zanzibar due to cultural and religious beliefs. Community awareness on neonatal
tetanus and strengthening of NNT surveillance through training of health workers is one of
the priority areas.
3.5.5 Hib Surveillance
A rapid assessment of the Hib disease burden was conducted in Tanzania Mainland in
2001. The findings revealed that the number of Hib disease cases ranged from 18,000 –
19,000 with deaths ranging from 3,300 – 3,500 per year using the meningitis and child
mortality based methods. Following this, MOH/EPI established Hib surveillance at
16Muhimbili National Hospital in 2001 and extended sentinel surveillance to Muheza District
Hospital in Tanga. These findings are corroborated by those of many regional studies which
suggest that Hib disease is a significant problem. In addition, the WHO Position Paper on
Hib conjugate vaccines has recommended the inclusion of conjugate Hib vaccines in all
routine infant immunization programmes in view of their demonstrated safety and
efficacy1.
3.5 Injection Safety and Adverse event following immunization
Zanzibar started practicing safe immunization injections in measles mass campaigns in
1999 using Auto-disable syringes and needles. Currently, EPI Zanzibar is using AD syringes,
needles and safety boxes in routine immunization services since 2002. EPI Zanzibar will
ensure that all immunization injections are safe to the recipient, health worker, community
and the environment by implementing the following strategies:-
Adequate supply of syringes and safe vaccines.
Surveillance and management of AEFI
Good injection practices
Proper waste management.
Communication and advocacy.
3.5.6 Injection safety and AEFI
An injection safety assessment done in 2000 shows the need for an updated assessment. It
has been observed that there is poor reporting of the AEFI, however some health facilities
have started reporting the AEFIs following sensitization and trainings. The plan is to
strengthen AEFI surveillance at health facility and district levels through on-the-job and
refresher trainings as well as supportive supervision.
3.6 National Level Program Support
At national level the proramme is led by the Programme Manager with the assistance of
other technical personnel such as:
Zonal EPI Operational Officer
EPI logistics officer
EPI Surveillance Officer
National cold chain Officer
National training Officer
National vaccine store Manager
The National EPI team mainly support the implementation of EPI national policies and
guidelines. The national team also performs monitoring and evaluation activities through
supportive supervision, compilation and analysis of monthly district reports and conducts
quarterly and annual evaluation meetings. Based on findings from several reports and for
the national team then designs a strategic guidance plan for the general implementation of
the programme. EPI Organogram attached as annex.
3.7 Monitoring and evaluation
3.7.1 Data Quality Self Assessment.
EPI Zanzibar in collaboration with EPI Tanzania mainland and partners conducted DQS
training from 16 – 24 August, 2004 for national programme officers. Field visits showed the
various weaknesses in different aspects at both districts and health facility levels. In 2006
another DQAs TOT training was conducted for the national EPI officers. The programme
plans to conduct DQS training in all DHMTS.
3.7.2 Supervision
National EPI program supervises districts on quarterly basis while districts supervise
health facilities every month. The national and district supervisors use available
supervisory checklist.
3.7.3 Immunization Coverage surveys
The last national immunization coverage survey in Zanzibar was conducted in 1993. The
EPI programme is mainly using administrative coverage data for its planning purposes. The
measles post campaign survey was conducted in 2008 but the results are not yet displayed.
17The programme is planning to conduct at least one routine coverage survey within the
planning period 2010-2014
3.7.4 Operational research.
Operations research will be used as a tool to for informing the policy and decision makers
in the country. The program will identify researchers and research assistants to conduct
identified areas/topics for research.
System will be established for assessing specific research topics to be addressed. This will
include:-
Assess the affordable and appropriate low cost incinerators for rural health facilities.
Evaluate the cost-effectiveness and impact on routine services of different
immunizations strategies, particularly in rural areas, including a comparative analysis
of fixed sites, regular outreach, and campaigns.
Asses the feasibility and cost of alternative energy source for rural refrigerators, in
order to convince partners to accept solar power and LP gases in the country
rehabilitation plan.
Studies on social mobilization and communication strategies to increase community
involvement.
3.7.5 Data Monitoring Form development/reprinting/ modification
EPI in collaboration with HMIS Zanzibar uses standard monitoring forms which include
tally sheet, health facility summary form, district summary form and national summary
forms. The other forms used by the programme are performance monitoring charts for all
levels, disease investigation forms and temperature chart monitoring forms. Health facility
is the primary source of information where all immunization data are generated. These
data are compiled monthly in a summary form. DHMTs collect monthly health facility
summary forms, compile and analyze and electronically sends to the higher level.
At the national level, the monthly district summaries are compiled and analyzed to obtain
national coverage and performance of the districts. The national level then shares these
reports with partners and other stakeholders
3.7.6 EPI Assessment
Several assessments were done in Zanzibar. Immunization service assessment was
conducted in February 2000. The assessment focused on managerial issues related to
vaccine supply, immunization services, disease surveillance, logistics, communication and
EPI financing as well as external factors such as the various sectoral reforms. The country
is due for another comprehensive immunization service assessment.
3.7.6.1 Vaccine management assessment.
The Ministry of Health and Social Welfare of Zanzibar in partnership with the WHO carried
out an EPI vaccine management assessment in Zanzibar from 2nd to 4th July 2002 and from
29 November – 12 December 2007 with a view to finding gaps and coming up with
recommendations to address the gaps. A WHO eleven criteria standard tool was used to
collect and analyze the data. All the three levels of vaccine management, the Central, the
Sub-national and the Service delivery levels were covered. One Central Vaccine Store (CVS),
five sub-national stores and eight service delivery facilities were assessed.
18A summary of the findings is indicated below:
Intermediate Service
# Criterion National
Level Level
1 Vaccine arrival process 100
2 Vaccine storage temperature 37 66 80
3 Cold store capacity 100 75 100
Building, cold chain equipment and
4 83 54 83
transport
Maintenance of cold chain equipment
5 67 76 78
and transport
6 Stock management 55 65 30
7 Effective vaccine delivery 64 55 38
Correct diluent use for freeze dried
8 0 80 48
vaccines
9 Effective VVM use 9 85 68
10 Multi-Dose Vial Policy 100 100 98
11 Vaccine wastage control 67 77 58
As depicted above, Zanzibar has a lot of work to do to improve on all indicators of vaccine
management below 80% of the standard. This is confirmed by the average score obtained
for all indicators of the standard which stand at 68%.
Stock Management Tool (SMT) was introduced at national level in the mid 2007. This tool
is not yet in use at sub-national level because the training has not been conducted. In 2008,
the programme introduced the use of SMT as well as Inventory Tool so as to better manage
the vaccines and related supplies.
The EPI programme in Zanzibar will ensure that the storage and transport of vaccines at
appropriate temperatures is vital to vaccine safety and efficacy. Attention has traditionally
focused on heat exposure of vaccines, but studies have indicated that exposure of vaccines
to freezing temperatures may be more common. Freeze-sensitive vaccines like DTP-HB can
loose their potency when exposed to freezing temperatures as a result of dissociation of the
antigen protein from the alum adjuvant. Training on how to prevent freezing during
storage and transportation will be prioritized with procurement of freeze tag indicators.
Despite the extensive operational benefits of VVMs, their use does not increase system
costs. Indeed, there is a net saving to immunization programmes when VVMs are used.
Therefore, the programme will continue to order the vaccines with VVMs and the cold
chain equipments that meet WHO specifications. The assessment was done in all vaccine-
handling levels of the country which included: Central vaccine store Zanzibar, zonal store
in Pemba, district stores and health facilities.
The overall objective of this assessment was to review vaccine management performance
(vaccine stock control, safe and effective vaccine storage and handling).
Findings showed 40% of all cold chain equipment to be CFC free, and only 48% of Health
workers had knowledge on MDVP and VVM.
194.0 NEW VACCINE
The United Republic of Tanzania is one of GAVI eligible countries for accessing GAVI
support which include ISS, HSS, Injection safety support, Civil Society Organization support,
and new and underused vaccines. Zanzibar is part of the united republic of Tanzania. The
Government of Zanzibar has committed to reduce child mortality which is clearly
articulated in the MKUZA document, MDGs, Party manifesto, HSSP II. Immunization
Programme contributes towards achieving the goals of reducing child morbidity and
mortality through vaccination. However not all available vaccines in the markets are
accessed by the children United republic of Tanzania. GAVI window of supporting poor
countries including Tanzania will facilitate further reduction of morbidity and mortality of
the children. This goal of introducing Pneumoccocal and rotavirus vaccines will accelerate
the achievement of MDG 4. To achieve these goals, the Programme has the following
planned specific objectives:-
To prepare and submit Pneumococcal and Rotavirus vaccines application to GAVI
in September 2009
To introduce Pneumococcal vaccines countrywide by the year 2010.
To introduce rotavirus vaccines countrywide by the year 2011
To conduct post introduction evaluation in 2012
To document the impact of introducing new vaccines.
Currently, the financing of the immunization programme is done by Government of
Zanzibar in collaboration with partners. The government has started the procurement of all
traditional vaccines and injection materials. The vaccine budget includes the co-financing
funds and the procurement is done through UNICEF.
Since there is MSD, which stores and distributes all vaccines, drugs, equipment and medical
supplies routinely in Mainland. The new vaccines for Zanzibar will arrive in MSD and
allocation of Zanzibar collected from MSD by EPI logistician from Zanzibar.
Prior to the introduction of the vaccines, there will be appropriate preparations to facilitate
smooth introduction and implementation of immunization services. This will include cold
chain assessment, vaccines management assessments, advocacy, training, sensitization to
the health workers and the community. However the vaccine management assessment was
conducted and results indicates that the country will be able to accommodate new vaccine. The
additional GAVI funds support for introduction of new and underused vaccines will facilitate the
activities.
20You can also read