Rare Diseases: National Policy - Contributions for a - SPECIAL HEALTH EDITIONS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Rare Diseases: Contributions for a National Policy 1
Rare Diseases:
Contributions for a
National Policy
S ÃO PAU LO, A P R I L 2013
S P E C I A L H E A LT H E D I T I O N S
V O LU M E V
2 SUPERVISION Antônio Britto Executive President G E N E R A L C O O R D I N AT I O N Octávio Nunes Director of Communications Selma Hirai Communications Coordinator Paula Lazarini Communications Analyst Tel.: (55 11) 5180 3476 paula.lazarini@interfarma.org.br Maria José Fagundes Delgado Director Marcela Simões Access and Innovation Analyst Tel.: (55 11) 5180 3490 marcela.simoes@interfarma.org.br EDITORIAL PROJECT Nebraska Composição Gráfica EDITING Fanny Zygband – Mtb 13.464 Duplo Z Editorial IMAGES Interfarma Image Bank A B O U T I N T E R FA R M A Interfarma –The Pharmaceutical of presence in Brazil. Today, these and access, combating informality, Research Industry Association laboratories are responsible, in the as well as biotechnology and Interfarma is a non-profit industry pharmaceutical chain, for sales of 80% regulatory system. Among the group, representing national and of the leading market medications and institutional actions are interaction foreign companies and researchers also for 39% of generics, produced and closer relations with the various responsible for promoting and by companies controlled by member agents, through a frank and open encouraging the development of laboratories. dialogue, especially with health scientific and technological research Interfarma sees research and authorities, industry leaders, opinion in Brazil, focused on production of innovation as factors in economic makers and other stakeholders pharmaceutical raw materials, inputs, development and ethics as a who can assist in creating a new medications and health products. fundamental principle of its activities. healthcare scenario, with the main Founded in 1990, Interfarma currently The organization encourages debates objectives of increasing access and has 46 member companies which on topics of interest to society such as strengthening innovation in Brazil. collectively account for 1,389 years clinical research, healthcare funding
Rare Diseases: Contributions for a National Policy 3
To fight for equality whenever
differences discriminate us and
fight for differences whenever
equality mischaracterizes us
BOAVENTURA DE SOUSA CAMPOS4
Rare Diseases: Contributions for a National Policy 5 Introduction Interfarma, the Pharmaceutical Research Industry Association, presents to au- thorities, physicians, patients and other interested parties the findings of a two- -year work in defense of a National Policy for Rare Diseases in Brazil. Along with many other initiatives, together with authorities and society to con- tribute to the improvement of healthcare conditions and access, Interfarma has placed special attention on so-called rare diseases. The first step was formation of a technical group in the organization. This mea- sure was followed by the decision to seek out external consultants (IMS Health Consulting and Prospectiva) to study the size of the problem, to gather successful examples from other countries and to objectively define the peculiarities and priorities of our country. Among the many important contributions for these studies, one is fundamental: the fact that Brazil today does not have an articulated policy for rare diseases. Without this policy, good intentions are plentiful and there is a lack of planning and articulated, realistic and successful activities. What is missing is a National Policy. And in its absence, we are left with prejudices and misconceptions. From governments, the supposition is that they can examine an issue like this only from a cost perspective. And, worse, basing examination on information that does not correspond to reality. From society, there is the assumption that governments neglect these issue only due to lack of sensitivity or respect for the suffering of patients with rare diseases and their families. And from both the government and society, there exists the idea that the solution to the issue will come through the courts, which only amplifies uncertainty and insecurity. As a result of all of this, Interfarma’s defense in favor of the adoption of a Natio- nal Policy for Rare Diseases, which expresses the commitment of everyone with definitions that are sensible, clear, gradual and aligned to the duty of expanding access to treatment in a fair and sustainable manner. In addition to publishing this summary text, we will follow up this effort with a series of activities and events, including seminars and discussions with officials from the Federal Government, parliamentarians, scientists and patients. Our goals are to contribute to the debate, collaborate for policy adoption and help to expand access to treatments. We hope these goals are achieved. Happy reading! Theo van der Loo Antônio Britto President of the Board Executive President
6
Preface
Until the early 1980s, patients with rare diseases were not included on the agenda
of government authorities. Patient organizations and social movements around
the world gave not only a voice to the needs of these individuals, but also contri-
buted to consideration of rare diseases as a public health problem.
This new approach led to the creation of numerous official programs directed at
assisting these patients and the advent of economic and regulatory incentives for
the development of medications intended to treat rare diseases – orphan drugs.
To a greater or lesser extent, the treatment of rare diseases has progressed in
Brazil and abroad as a result of these measures, with medical innovations and
greater awareness among society, governments, institutions, businesses, patients
and families. But this context also raised a number of new issues regarding the
definition of rare diseases, from the cost of medications to their impact on the
healthcare system.
The main challenge, long known to public managers, is a binomial equation: ba-
lancing the need to adequately meet the demands of patients with the rising costs
in the industry due to scientific and technological advancement.
Brazil is no exception to the general rule: despite advances, the road ahead is still
long. There is no effective and safe treatment for many rare diseases and several
barriers hinder patient access to specialized treatments and drugs. There is insu-
fficient research and information about these diseases, and professionals in the
area are in need of training and education, compromising and delaying diagnosis,
with the health system itself also not offering a means of timeliness.
Within this complex scenario – a true challenge for health authorities and all
segments involved in rare diseases issues – Interfarma offers in this document a
contribution so that the topic may gain its deserving place on the national agenda,
as well as means of reflection for Executive and parliamentary officials linked to
the cause – important requirements for Brazil to advance needed care for indivi-
duals with rare diseases.
Maria José Delgado Fagundes
Director – InterfarmaRare Diseases: Contributions for a National Policy 7
or with regular medication that only helps alleviate
1. Introduction symptoms.
In Brazil, the subject is not a new one for health au-
Interest in rare diseases has increased in recent years,
alongside the recognition that they pose a public he- thorities. Although the country lacks specific policies
alth problem. The last decade has witnessed develop- for rare diseases, it has been the subject of discussions
ment of most of the official programs for rare diseases since the early 2000s – yet, it has chosen to discuss
in various parts of the world, at a time when many them from the perspective of genetic diseases. In
countries, including emerging countries, created po- 2004, the Ministry of Health created a work group in
licies specifically directed at the issue. order to systematize the proposal for a National Po-
licy for Clinical Genetics in the SUS (National Health
Although they have different definitions and appro-
aches regarding the topic, public policies developed System). The proposal was developed, but it did not
around the world have presented a range of solutions move forward.
to expand patients’ access to care. The challenge is About five years later, the National Policy for Com-
considerable, considering that 95% of rare disease tre- plete Attention for Clinical Genetics was instituted,
atments do not depend on a network of palliative care
whose results, though seen as a breakthrough, are
to guarantee or ensure the quality of patients’ lives.
considered insufficient by industry experts.
At the other end of the spectrum is a small percentage
The lack of a broad perspective that takes into account
of rare disease treatments with medical treatments
capable of interfering in progression - the so-called specificities and responds to different needs in the
orphan drugs - but the high cost of drugs has requi- rare diseases universe - those without treatment; tho-
red governments to make decisions on specific po- se that benefit from treatment of symptoms; and those
licies and procedures to ensure their continual sup- with orphan drug treatments - has been a barrier that
ply. Among one group and another, there are certain makes it difficult and sometimes even prevents pa-
forms of rare diseases that can be treated surgically tients from gaining access to appropriate assistance.
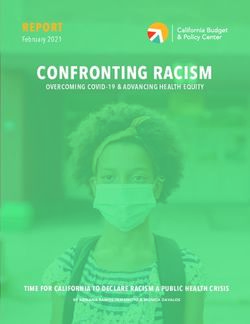
Figure 1. Most of the inclusion of rare disease programs took place in the last decade.
Regulations under
1983 1993 1996 1998 1999 2000 2002 2010 2012
development
Canada • China: rare diseases project
Regulations to China is under review by the People’s
ensure access 2 provisions Colômbia National Congress.
EUA to essential for rare “Ley 1392”
Orphan Drug medications diseases Congress of • Canada: in 2008 parliment
Act FDA the Republic approved Bill M-426 for the
development of a national
Japão approach for funding of rare
Orphan Drug Austrália União EURO México diseases medications (the proposal
Regulation Orphan Reg. 141/2000 244 BIS is awaiting approval by the
Min. Health, Drugs Gen. Congress Senate).
Labour & EMEA
Program
Welfare TGA • Chile: in September 2011 a
bill was drafted and is awaiting
approval in Congress.
Source: Dossier of rare diseases and orphan drugs: understanding the Brazilian situation in the global context (IMS - June 2012).8
illnesses are responsible for almost half of diseases in
2. Rare diseases, developing countries, investments in R & D do not
neglected diseases prioritize this area. The same criterion is used to defi-
ne the “orphan drug”. Due to a lack of a sufficient ma-
and orphan drugs rket to absorb them, there is no stimulus for research,
development and production of drugs and vaccines to
prevent or treat them.
When it comes to rare diseases, there is no unaminity
even in terms of its concept. The only commonality is
the definition that the diseases affect a small portion
of the population. In general, analyzing the various Epidemiological Profile
concepts adopted around the world, it is possible to It is estimated that there are approximately 7,000 rare
locate rare diseases with a range of maximum preva- diseases in the world. If these diseases individually
lence variable from 0.5 to 7 per 10,000 inhabitants.
reach a limited number of people, together they affect
This data, which apparently may seem irrelevant, is
a considerable proportion of the world population -
essential to define the scope and breadth of official
between 6% and 8%, or 420 million to 560 million
policies developed by each country.
people. Of this total, approximately 13 million such
Compared with other countries, Brazil lags behind: individuals are in Brazil, according to these estimates.
just as it lacks an official policy specific to rare di-
seases, it lacks an official concept to define them. In Around 80% of rare diseases have a genetic origin.
an attempt to move forward on this issue, some bills The remainder are the result of bacterial and viral
related to rare diseases and orphan drugs are cur- infections, allergies or degenerative causes. Most rare
rently under consideration in Congress. Besides es- diseases (75%) are manifested early in life and affect
tablishing guidelines for a national program for the children from 0-5 years of age. They also contribute
treatment of rare diseases under the National Health significantly to morbidity and mortality in the first 18
System (SUS), such action seeks to define rare disease years of life.
prevalence, placing it at 6.5 per 10,000 inhabitants, the
same parameters as Europe. Such disturbing indicators make it necessary to con-
sider a care policy to ensure a better future and social
The concept of rare disease is frequently confused
inclusion for these children and for their caregivers -
with neglected disease, even by health legislation in
usually family members, who abandon all activities to
some countries. At the root of this misconception
exclusively take on this role.
might be the indistinct use of the term “orphan” to
describe treatment of both rare diseases and neglected In the complex world of rare diseases, there are at
diseases. least three different situations that should be conside-
While rare diseases have this name due to its low pre- red for any healthcare policy: 95% have no treatment
valence in the population, neglected diseases refer and require specialized services for rehabilitation that
to so-called tropical diseases common in developing promote improved quality of life. Around 2% of rare
countries or regions, that typically affect low-income diseases can benefit from orphan drugs that interfere
populations. This is the case of leishmaniasis, Chagas with progression of the disease. The other 3% have al-
disease, leprosy and other endemic diseases caused by ready established treatments for other diseases, which
infectious and parasitic agents. help alleviate symptoms. In such cases, medication,
The adoption of the term “neglected” is based on lack despite being given to a patient with a rare disease, is
of incentives for research activities. Although such not considered an orphan drug.Rare Diseases: Contributions for a National Policy 9
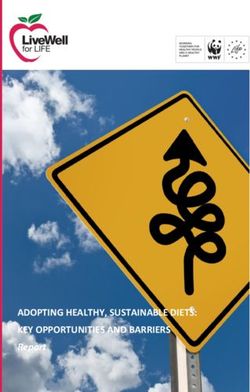
Figure 2. Less than 2% of the more than 7,000 rare
diseases are treated with orphan drugs, mainly for
3. The Scenario
oncological conditions.
in Brazil
Providing adequate care for patients with rare di-
More than 7,000 estimated rare diseases seases means formulating a policy which is able to
combine the two main facets of the issue: care and
treatment on the one hand, and the offer of orphan
drugs on the other.
Without treatment In practice, this binomial equation requires the or-
~6.600 (95%)
ganization of a network of services that merge tre-
atments and high-technology medications with low
complexity procedures and can meet the main needs
of patients: early and accurate diagnosis - one of the
major problems faced by these people. There is a lack
Treated with conventional drugs
of qualified professionals, a shortage of medical and
~250 (3.5%) scientific knowledge about these diseases, infrastruc-
Treated with orphan drugs ture for different health needs of patients, and access
~131 (1.8%)
to medications and monitoring of administered tre-
atments.
Therapeutic indications for oprhan drugs in the USA The fact that Brazil does not have an official policy
specifically for rare diseases does not mean, howe-
ver, that patients do not receive care and treatment.
They eventually secure medication, mostly through
12% the courts. And the SUS, one way or another, meets
Neurologicals
the needs of these people - but in a piecemeal fashion,
12% without planning, with great waste of public resources
Metabolics
and harm to patients.
12% Public policy for clinical protocol
Cardio and respiratory
The Ministry of Health reports that there are curren-
51% tly 26 clinical protocols related to rare diseases within
Oncologicals
the SUS - 18 developed under the aegis of the new
National Policy for Complete Attention for Clinical
13%
Immunologicals Genetics. Through these protocols – the official en-
tryway to care for rare diseases in the public system
– 45 drugs and surgical and clinical treatments were
offered, 70,000 office visits and more than 560 labo-
ratory procedures for treatment and diagnosis were
carried out, with investment of more than than R$ 4
Source: Dossier of rare diseases and orphan drugs: understanding the Brazilian situation in the
global context (IMS - June 2012).
million per year. However, although cited by the Heal-
th Ministry, some diseases such as Pompe, Homocys-10
tinuria, Fabry and all forms of Mucopo-
Figure 3. 18 diseases theoretically covered in the National Policy of
lissacaridose – have not been included in 2009 with treatment protocol granted*
any clinical protocol since the policy was
Diseases
created.
Addison’s Disease
Additionally, of the 18 most recent pro- Congenital Adrenal hyperplasia
tocols, only one - for the treatment of Congenital Hypothyroidism
Gaucher’s Disease - incorporates orphan Crohn's Disease
drugs. The others include only conventio- Cystic Fibrosis of the Pancreas
nal drugs, which lessen symptoms of di- Pulmonary Cystic Fibrosis
sease but not interfere in its progression. Gaucher's Disease
Hereditary Angioedema
Currently, almost all rare diseases registe- Hereditary ichthyosis
red with ANVISA that use orphan drugs Hypoparathyroidism
remain outside protocols, which repre- Hypopituitarism
sents a considerable barrier for accessing Myasthenia Gravis
these drugs through the SUS. According Multiple Sclerosis
to the study conducted by Interfarma, 14 Phenylketonuria
diseases are in this situation: they rely on Sickle Cell Disease
drugs approved by ANVISA and marke- Turner's Syndrome
ted in the country, but are excluded from Wilson’s desease
the government’s agenda.
The study also shows that the official * 17 protocols do not use medications that interfere in the progression of disease (orphan
policy for rare diseases itself – based on drugs), treating only symptoms.
clinical protocols for disease - helps per- Source: Dossier of rare diseases and orphan drugs: understanding the Brazilian situation in the global context (IMS -
June 2012).
petuate inadequate care in terms of diag-
Figure 4. 14 remaining diseases have a pharmacological treatment that is marketed in Brazil.
Maintained Diseases Drug marketed in Brazil (brand; active ingredient; company)
Pompe Disease Myozyme; alfalglicosidase; Genzyme
Homocystinuria Biotine: various low-cost options
Fabry’s Disease Replagal; alfagalsidase; Shire • Fabrazyme; beta-galsidase; Genzyme
Mucopolysaccharidosis I Aldurazyme; laronidase; Genzyme / BioMarin
Mucopolysaccharidosis II Elaprase; idursulfase; Shire
Mucopolysaccharidosis VI Naglazyme; galsulfase; BioMarin
Niemann-Pick Type C Zavesca; miglustate; Actelion
Pulmonary Arterial Hypertension Tracleer; bosentan; Actelion
Acute Myeloid Leukemia Evomid; idarrubicina; Evolabis • Zavedos; idarrubicina; Pfizer
Amyotrophic Lateral Sclerosis Rilutek; riluzol; Sanofi-Aventis
Gaucher’s Disease Zavesca; miglustate; Actelion • Cerezyme; imiglucerase; Genzyme • Vpriv; alfavelaglicerase; Shire
Hereditary Angioedema Firazyr; icatibant acetate; Shire
Acromegaly Somavert; pegvisomant; Pfizer
Familial Amyloid Polyneuropathy Vyndaqel; tafamidis meglumine; Pfizer
Source: Dossier of rare diseases and orphan drugs: understanding the Brazilian situation in the global context (IMS - June 2012).Rare Diseases: Contributions for a National Policy 11
nosis, infrastructure and professional training. To for the 433 lawsuits that ruled in favor of the purchase
reduce bottlenecks, it would be desirable to consider of medications for individuals with rare diseases.
rare diseases in a general context and to structure a
According to Interfarma’s study, in order to facilitate
support network capable of responding to different
patient access to orphan drugs and avoid the heavy
categories of care required by patients.
costs of lawsuits, adjusting the analysis parameters to
the particularities of rare diseases would be necessary,
replacing the criteria of cost-effectiveness for other
Incorporation of drugs vs more appropriate ones, such as clinical effectiveness.
judicialization
The supply of orphan drugs from the SUS depends
on incorporation in a clinical protocol which, in turn,
depends on an assessment of technical and economic
viability. However, the criteria employed by the go-
4. Barriers to care
vernment to assess the availability of orphan drugs in
the public system is based on cost-effectiveness and in
in Brazil
most cases this excludes patients from the possibility The lack of an official policy for rare diseases has
of obtaining this kind of treatment. transformed the lives of patients into an excruciating
obstacle course, whether in regards to care and treat-
Brazilian law establishes that medications for diseases
ment or in relation to medications, the latter subject
of low prevalence be analyzed by the same parameters
to numerous regulatory barriers that impede their en-
used for those of high prevalence for the purpose of
tries into the market and the SUS.
incorporation in the SUS. Taken into account are is-
sues such efficacy of treatment and cost impact, com-
pared with other measurements of the same nature.
Lack of access to care
If these parameters are in theory justified for plan- and treatment
ning and prioritizing public spending , in practice
they have functioned as a major obstacle to patients
with rare diseases. The low prevalence of the disease Late diagnosis
does not allow clinical trials for effectiveness of or-
phan drugs to have the same duration and number of The first major difficulty that people face is making
patients involved than those of high prevalence. people aware that they are suffering from a rare disea-
se. There are two main causes of the problem: the lack
Since it is intended for few individuals and it does of trained professionals to make the clinical diagnosis
incur cost of development diluted between large po- and the fact that the SUS does not include genetic
pulation groups, orphan drugs end up being more tests in its list of procedures needed to confirm the
expensive than conventional ones. Moreover, most of diagnosis. It is estimated that patients take an avera-
these drugs do not rely on another drug with the same ge of two to four years of seeing health services and
function which allows the realization of a comparati- professionals in various specialties until the disease is
ve analysis of cost-effectiveness, as required by law. identified.
To try to break this vicious circle that impedes access The result could not be worse for everyone. Late
to orphan drugs, many patients have resorted to the diagnosis results in disease developing rapidly and
courts, with considerable financial impact to the pu- reaching disabling and chronic stages, making the
blic. A measure of the problem lies in the fact that the treatment more of a sacrifice and less effective for
Ministry of Health disbursed, in 2011, R$ 167 million the patient. The public system, in turn, is required to12
“It is unfortunate that
some patients jump
from office to office and
take so long to receive a
PHOTO: AGÊNCIA CÂMARA
diagnosis”.
Interview with P: What is your position regarding the possible deve-
lopment of a national policy for rare diseases under
Congressman Romário the SUS?
One of the most active supporters of the Parliamentary R: I’m totally in favor. Today there exist many projects in
Front to Combat Rare Diseases (House of Representatives) the House of Representatives which present a series of
and an organizer of meetings and debates on the topic,
Government obligations to better serve people with rare
Congressman Romario advocates the need for the country
diseases. I support all those initiatives that, among other
to adopt an official program specific to these diseases.
determinations, provide medical, pharmaceutical and full
Romario says that patients are being poorly treated and rehabilitation care to patients with rare diseases.
proposes a series of initiatives to improve care and expand
P: What, in your view, are the priorities that a policy
access to orphan drugs. To facilitate this process, he highli-
of this nature should include?
ghts the need for the Government to assume responsibility
for individuals with rare diseases. R: In terms of care and treatment, early diagnosis is a pri-
mary posture that will slow, in some cases, the progress of
P: How do you evaluate the care currently given to
the diseases. But it also involves the training of professio-
patients with Rare Diseases in Brazil?
nals. It is unfortunate that some patients jump from office
R: People affected by rare diseases are poorly cared for by to office and take so long to receive a diagnosis.
the Government, even due to the complexity of the pro-
P: And in relation to the availability of orphan drugs?
blem. There are more than 8,000 types of rare diseases.
These diseases are still poorly known to science, and many R: Agility in the analysis for granting registration of medi-
without treatment. I estimate that Brazilian public health is cations should be a priority. This is a frequent complaint
crawling in terms of serving these people. of patients with rare diseases. The delay in the release of
a drug may mean the time between the life and death of
P: What is necessary fo the country to advance in this
a person.
area?
P: Today the incorporation of orphan drugs in the
R: The country should advance in genetic research, ex-
SUS is subject to many barriers. What would be ne-
pand the network of genetic counseling. According to
cessary to improve access to this type of treatment
Government’s own data, there are just 80 hospitals across
for individuals with rare diseases?
the country that offer some kind of treatment linked to
the specialty. Expanding this network would help, espe- R: The Government should subsidize research and produc-
cially for low-income people and those who live far from tion of orphan drugs. A portion of the population cannot
major centers. This portion of the population suffers the remain without help because these drugs aren’t profitable.
most and faces the greatest difficulty in obtaining an early It is very important that Brazil assumes this social respon-
diagnosis. sibility.Rare Diseases: Contributions for a National Policy 13
meet the more complex situations generated by the Direct and indirect social costs
progression of diseases - such as hospitalization and
The concentration of reference centers in South and
medication - which entail higher costs.
Southeast generates an influx of patients and caregi-
There are still a number of patients who continue vers to these regions. Given the severity of most of
orbiting in the health system without ever receiving these diseases and the fact that they occur more fre-
diagnosis, making clear the need to intensify efforts quently during childhood, require action by families
in care and assistance as in research. and loved ones, most who devote themselves exclusi-
vely to the care of patients. This is a cost that also ends
up falling on hands of the government, since family
members stop working and start relying on public
Lack of trained professionals
welfare, with virtually no prospects of resuming their
Around 80% of rare diseases have genetic origins and previous activities.
must be accompanied by medical geneticists. Cur-
rently, in Brazil there are about 200 specialized doc-
tors that are registered with the Brazilian Society of Orphan drugs
Medical Genetics - equivalent to one geneticist for
every 1.25 million Brazilians. To understand this gap,
the World Health Organization (WHO) recommends Delay in granting registration
that there be a geneticist for every 100,000 inhabi- According to Brazilian law, the sale of drugs in the do-
tants. By this criterion, Brazil has a current deficit of mestic market depends on obtaining registration with
approximately 1,800 professionals. ANVISA (National Health Surveillance Agency).
Granting such registration, in turn, is linked to the
proof of fulfillment of requirements such as product
Insufficiency and regional safety and efficacy, and this is where one of the bottle-
necks in the process is found.
concentration of reference centers.
The verification of those requirements by the regu-
In addition to a shortage of professionals, professio-
latory agency and the granting of registration, which
nals are heavily concentrated in the South and Sou-
should be carried out within a 90-day period has been
theast, where leading centers of reference in medical
delayed, on average, by two years. A considerable
genetics are located. Although linked to universities, number of registration requests for medications are
including hospitals, the centers are not formally inte- currently waiting, delaying market entry for products
grated into the SUS and financed by research funding that are important to the health of the population,
agencies or the pharmaceutical industry. including those for rare diseases.
Given the general lack of support for patients with
rare diseases, these centers end up offering informal
Public relevance
and individualized care, using part of the money that
should be allocated to research part of the resources of Brazil counts with legislation, Law no. 9.782/99, whi-
the SUS itself, which pays for some tests. ch enables ANVISA to expedite the granting of regis-
tration of medications and pharmaceutical supplies.
Yet patients who cannot access treatment centers are It also has a standard, the Resolution of the Board of
fully funded by the SUS. In general, they do not have Directors (RDC. 28/07), which provides companies
qualified professionals to conduct appropriate treat- the ability to make priority requests for products con-
ment and receive fragmented and insufficient care. sidered of public relevance. In such cases, the period14
“Although rare diseases affect the lives
of about thirteen million people, Brazil
still does not possess a positive policy
PHOTO: CONTRIBUTED PHOTO
for this specific population, nor a
organized structure for care”.
Interview with Senator People with rare diseases today face gigantic social difficul-
ties. The barriers are many times insurmountable. Prejudi-
Eduardo Suplicy ce is frequent, as well perception that these individuals are
In late 2011, Senator Eduardo Suplicy presented to the a burden rather than an integral part of society. Many end
Senate Bill no. 711, establishing the National Policy on up socially isolated, due to lack of adequate infrastructure
to meet their specific needs in schools, universities, and in
Protection of Rights of People with Rare Disease. The bill
the workplace and in leisure activities. The vast majority
is pending before the Economic Affairs Committee and of people with rare diseases do not have the conditions
awaits the opinion of the rapporteur, Senator Paulo Bauer. necessary to reach their full potential.
Suplicy also advocates creation of a National Fund for Rare
I consider change in the social culture for dealing with rare
Diseases, and about a year ago presented another bill to to
diseases to be necessary in our country. The approval of le-
make it possible gislation, as is the case of PLS 711/2011, which establishes
national guidelines for the conduct of public policies on
“I’m fully in favor of creation of a National Policy on Rare
the rights of people with rare diseases, is an important step
Diseases under the auspices of the SUS. Although rare dise- in that direction.
ases affect the lives of about thirteen million people, Brazil
I understand it would be very important to also create a
still does not possess a positive policy for this specific po-
National Fund for Rare Diseases, in order to support re-
pulation, nor a organized structure for care. Moreover, the search projects and related projects in the area of rare and
country is unaware of the magnitude of the problem and neglected diseases. I presented on May 7, 2012, Senate Bill
does not have a mapping of their specificities and needs.” no. 23 of 2012, that establishes this fund. “
of analysis and granting of registration can be shorte- Delay in setting prices
ned to 75 days.
Besides health registration, the marketing of a drug
However, since the standard does not define what rare depends on the pricing set by the CMED (Medication
diseases are, orphan drugs cannot be prioritized nor Market Regulation Chamber). This process can be
considered of public relevance. Although they are of- very slow, taking from one to two years. Some drugs
ten the only treatment option, they may take years to can take up to five years to reach the market when
reach patients, who are thus deprived of this benefit. considering the two steps together – registration andRare Diseases: Contributions for a National Policy 15
pricing. The bureaucratic obstacles, coupled with di-
fficulties in establishing prices that enable companies 5. International
to recover large investments in employee develop-
ment and production of orphan drugs eventually be- experiences
comes a disincentive for introduction of products in
The analysis of international experiences related to
the country, further damaging patient care.
rare diseases can offer important contributions to the
discussion and development of a public policy that
addresses these diseases in Brazil. While most coun-
Clinical research tries that have official programs specific to rare disea-
Clinical studies conducted to verify the safety and ses are developed, in some emerging – such as China,
efficacy of medications are an important possible me- Colombia and Chile –, there are expanding efforts to
increase patient access to treatments. The United Sta-
ans for the country to receive investments and deliver
tes, Mexico, the 27 members of the European Union,
innovative treatments to patients. However, govern-
Australia, Japan, Singapore, South Korea and Taiwan
ment bureaucracy has hampered Brazil’s participation
are examples of countries that have developed specific
in multicenter research protocols, in which research policies for rare diseases and show how this concern is
groups from different countries conduct simulta- widespread throughout the world.
neous clinical trials for a given drug.
As a backdrop to these initiatives are the recognition
While the global average for approval of clinical trials of rare diseases as a public health problem, the expan-
varies from three to four months, in Brazil it is neces- sion of public-private partnerships, the improvement
sary to wait three times as long. For this reason, the of patient recruitment for clinical trials through the
country has lost important opportunities to integrate internationalization of these studies, the strengthe-
ning of patient advocacy groups and the increase in
multicenter protocols and as a consequence, it has
industry interest in certain niche markets, including
narrowed patient access to orphan drugs as well as
rare diseases.
monitoring by a clinical body of excellence. In the
case of rare diseases, studies involving multiple coun- In general, international experience is focused on
tries and centers carry great weight, as patients are two main areas: the first refers to how some countries
recruited in different parts of the world as a result of structure differentiated services to meet the needs of
patients with rare diseases. The second relates to stra-
the disease’s low prevalence.
tegies to offer orphan drugs in national markets and
But this is not the only disincentive in the country for to incorporate them into health systems.
the sponsors of research and development of orphan
drugs. By virtue of a resolution of the National Health
Council, sponsors of clinical studies should continue Care
to provide patients the treatment being tested for the In relation to care and treatment, the countries of the
rest of their lives when there is some benefit to the European Union – which adopt a single definition for
patient, even without approval from ANVISA. Given rare diseases – are the most advanced. They base care
the low incidence of rare diseases, this is a problematic at multidisciplinary clinics and prioritize integrated
issue, since the sponsor will need to provide the drug care. France was the first country in Europe to adopt a
free of charge to almost all of its consumer market. national plan for rare diseases in 2005. The main me-
asure taken to ensure diagnosis, care and treatment
and access to orphan medications was the structuring
of reference centers, which operate within hospitals.16
In the first four years of the plan, 131 centers were Act –, followed the path of providing support and
created in the country. Italy pursued a similar path facilities for the pharmaceutical industry, in order to
with reference centers and instituted, in 2001, a na- encourage research and development of these drugs.
tional network of prevention, observation, diagnosis
Marketing exclusivity for seven years, exemption from
and treatment of rare diseases was introduced into the
existing public system, in addition to free care. The taxes, flexible criteria for approval of the drug by the
network has centers in all regions of the country and FDA (Food and Drug Administration) are some of
intends to share information between them. the incentives offered in the country, where the priva-
te system predominates. Besides being available in the
In Germany, the National League of Action for People market, most medications are covered by private he-
with Rare Diseases - under the Ministry of Health – is alth insurance and the public system. Access is rarely
discussing the implementation of the reference cen- denied, but is subject to reimbursement mechanisms
ters. The country currently has 16 research centers on and co-payment.
rare diseases.
Meanwhile, the European Union has implemented
Norway, Denmark and Sweden have adopted mul-
measures to encourage research and development of
tidisciplinary clinics for rare diseases based on the
orphan drugs common to all member countries. Ho-
concept of reference centers. The treatment optimi-
wever, the policy of access to medications is a decision
zation and cost reduction are the main drivers of the
made by each country. Some also adopt the system of
initiative.
co-payments but, unlike the U.S., the contribution of
According to a 2009 report from EURORDIS – an the patient is small.
alliance of patient organizations from 49 countries
Most countries use a cost-effectiveness assessment to
representing 544 rare diseases – the average cost per
child treated in centers corresponds to only 33% of determine the incorporation of orphan drugs into the
the cost of treatment in programs that are not integra- national health system, but with some adjustments.
ted into these institutions. Germany, for example, is more flexible in terms of the
analysis criteria. England is now studying a differen-
tiated system of evaluation.
Orphan drugs The priority of the governments of Australia and
To expedite patient access to medications, some coun- Canada is to expedite patient access to orphan dru-
tries have adopted strategies to facilitate registration gs. As a means to facilitate the registration process
– a prerequisite for marketing. Accelerated review of of these drugs, the Australian health authority, the
documentation and reduction of demands in rela- TGA, utilizes the assessment made by the American
tion to clinical studies are some of the most common FDA, adding a criterion of clinical efficacy (it does not
practices. In some cases, the designation of orphan adopt the criteria of cost-effectiveness).
drugs in other countries may be sufficient for a drug’s
In Canada, there are various mechanisms and progra-
approval. Many countries still grant incentives to ma-
ms that patients can use to obtain funding by the State
nufacturers, such as reduced rates and market exclu-
for a medication that is not on the general reimbur-
sivity in relation to competition.
sement list of the country. The government’s decision
The policy model adopted by each country in relation regarding if there will be full payment of the medica-
to orphan drugs varies according to the particularities tion or some degree of co-payment is evaluated on a
of the health system – whether it is public or private case-by-case basis. The population is making some
and who is paying for the majority of these costs. The claims for the adoption of a specific policy guaran-
United States, a pioneer with the enactment in 1983 of teeing reimbursement for orphan drugs through the
a specific policy for orphan drugs – the Orphan Drug public health system.Rare Diseases: Contributions for a National Policy 17
Figure 5. Although practices differ from country to country, some points can be used in the Brazilian case.
Items analyzed Learnings
Clinical studies are generally facilitated for orphan drugs. Some of the tools to allow this scenario
are: combination of stages (e.g., II and III), requirement of small group of patients (less than 100)
Clinical studies: requirements and and "case-by-case” analysis.
obstacles
Patient organizations (advocacy groups) play an important role in promoting drug approval in the
countries analyzed.
Requirement of efficacy profile of drugs is less demanding than that of common drugs: in some
Clinical evidence to secure approval
countries, the increased rate of survival is the main criterion considered.
Europe’s approach is less restrictive in that sense, exempting drugs from an economic analysis/
Economic evidence
budget impact in some countries.
Discount policies are not a common practice. Orphan drugs are likely to follow the same rules of
Pricing/discounts
common drugs (e.g. compulsory discounts).
Most countries reimburse/provide free orphan drugs, supported by its innovative profile and the
Reimbursement (a)
pressure of local POs.
In Europe, additional funding for highly innovative medications are granted to orphan drugs. In
some countries, a portion oftotal healthcare funding is dedicated exclusively to orphan drugs
Special financing
In the U.S., NORD offers patient assistance programs that go beyond access to medications,
especially for the uninsured (in general, low-income populations).
Fast track approval A análise de via rápida de aprovação é realizada caso a caso em alguns países da Europa
(a) the term reimbursement used throughout this document refers to the furnishment of drugs by the government.
Source:Dossier of rare diseases and orphan drugs: understanding the Brazilian situation in the global context (IMS - June 2012).
Among Latin American countries, the situation in a policy similar to the U.S., with a predominance of
Mexico, Chile and Colombia is equivalent to that of incentives for businesses.
Brazil; there is a concern about adopting specific po-
China, on the other hand, has a public health plan that
licies for patients with rare diseases, but the process is
benefits a small portion of the population and does
still ongoing.
not reach the majority of those living in rural areas.
Mexico, for example, recently passed a law that requi- Still, the country has mechanisms to ensure rapid ap-
res the government to make efforts to provide medi- proval of drugs to accelerate commercialization.
cations and foster their development. However, the From analysis of international experiences adopted
legislation does not specify how this should be done. by these countries, the combination of two equally
In Chile, a number of different bills related to rare important perspectives is evident: on the one hand,
diseases are pending. In Colombia, where the public facilitating the entry of orphan drugs in the market,
health system is not universal – unlike Brazil, Mexico and secondly, the feasibility of patient access to these
and Chile – the law guarantees full assistance to pa- drugs through the public health system and, in the
tients, but does not provide access to orphan drugs. case of diseases that have no specific treatment, offe-
ring a range of appropriate healthcare services.
In the context of the BRICS (Brazil, Russia, India and
Australia is the country that has advanced the most in
China), the closest situation to that of Brazil is Russia.
initiatives, enabling orphan drugs to reach the market
Some drugs are reimbursed by the state and the judi-
quickly and to be incorporated and available to pa-
cial process is often used to obtain others.
tients through the use of different mechanisms of eva-
In India, most of the population uses the private he- luation. It is a model that can be of great inspiration to
alth system. With a strong tradition of drug resear- Brazil, but not without considering the characteristics
ch and development, the main demand is to adopt and particularities of the SUS.18
Figure 6. The main characteristics of the public health system and access programs for orphan drugs.
Country Health System Policy for Rare Diseases – Access
USA • Dominance of the • Focus is on encouraging R&D. There is no specific policy for access to orphan drugs, which
private sector. are considered to be in the category of specialized medications.
• Access to the public • Most orphan drugs are covered by both private health insurance as well as the public
system has age and system (Medicare and Medicaid).
income restrictions. • Access ≠ "accessible" (affordable) --> just like for other specialized medications, there are
mechanisms for co-payment – which is usually high cost for specialized drugs, which can
make the drug too costly for the patient, affecting use.
• Medicare, the federal public health plan for seniors and disabled adults who qualify for the
Social Security Disability Insurance program. Children are not covered by the public plan.
• Medicaid is a state plan and it covers very low-income families. That is, much of the
population relies on private health plans, which bear most of the costs of these medications.
Australia • Universal Public System • Focus is on access to these drugs. There are no incentives for R&D.
• Includes • Fast-Track in the registry: use of information from the drug approval process by the FDA as
pharmaceutical basic document
assistance • Access to medications is done via pharmaceutical assistance programs, two of them
targeted at highly specialized medications and "life-saving medications", directed at
medications that treat diseases of low prevalence and threaten the patient's life, but were
not incorporated into the overall list of reimbursement (understanding that orphan drugs
are clinically effective, but do not fit the criteria of cost-effectiveness)
• There is an institutionalized mechanism to access drugs not yet registered in the country.
Canada • Universal Public System • Focus is on access to these drugs.
• Pharmaceutical care • There is a list of medications funded by the government.
for elderly and indigent • If the product is off the list, there are three mechanisms for access to special medications
only --> Orphan drugs are considered to be in the broader category of "special medications" or
"specialized medications"
• There is still the possibility of co-payment
• The courts do not act in this sphere.
• There is no government incentive for R&D
European • There is a unified policy of incentives for R&D and drug registration.
Union • Policies for access to orphan drugs are created individually by each country.
• European Organization for Rare Diseases.
England • Universal Public System • Access to a medication is secured via incorporation of the drug on the public system’s
• Includes reimbursement list.
pharmaceutical • The inclusion of a medication on the list depends on the favorable opinion of the National
assistance Institute for Health and Clinical Excellence (NICE), based on Health Technology Assessment
(HTA) with criteria of cost-effectiveness.
• Today, there is no specificity attributed to orphan drugs in the ATS. They are subject to the
same evaluation criteria of a medication for prevalent diseases.
• Adoption of different criteria for evaluating orphan drugs is being studied.
• NICE has already made such a proposal to be adopted by Ministry of Health.
Germany • Público Universal • The inclusion of a medication on the list depends on the favorable opinion of the G-BA,
• Assistência based on ATS criteria of cost-effectiveness.
farmacêutica para • Orphan drugs have more flexible criteria for entry on the list, no need to prove an additional
desempregados benefit over other existing therapies (do not need cost-effectiveness studies).
• If gross sales of some medication named as orphan drugs exceed 50 million euros, the
G-BA may request extra data showing additional benefit, which must be arranged within
three months, and the medication is subject to the same approval criteria as any other
medication.
• "sickness fund" can reimburse a medication that has not yet been approved.
Spain • Universal Public System • Large number of orphan drugs are on the reimbursement list.
• Includes • There may be co-payment of these drugs.
pharmaceutical • When a drug is administered in the hospital, payment comes from the Hospital budget.
assistanceRare Diseases: Contributions for a National Policy 19
Figure 6. Continue.
Country Health System Policy for Rare Diseases – Access
Italy • Universal Public System • To integrate the reimbursement list, an orphan drug passes through the same procedures
• Counts on as a common drug.
pharmaceutical • There is a fund to reimburse orphan drugs still awaiting marketing approval.
assistance • Has reference centers for rare diseases.
Mexico • Universal Public System • The Mexican legislation is a little more advanced; in the sense of establishing laws that will
make efforts to make available orphan drugs needed and try to foster their development.
• The concrete ways by which these efforts are made are not yet specified.
Chile • Universal Public System • Bills in the area that are still pending.
• Includes • There are principles in the Chilean Constitution that guarantee health care by the State.
pharmaceutical
assistance
Colombia • Mixed System • There is legislation that provides full assistance to these patients, but does not deal with
• Access to the public access to orphan drugs in particular.
system is restricted
Russia • Universal Public System • Very similar situation to Brazil: only a few medications are on the reimbursement list.
• The country also has an issue with the courts.
• Funding to purchase these drugs relies on regional health authorities (not from the federal
budget).
China • Basic public plan, • There is a mechanism for quick approval of orphan drugs.
which covers a small • There are government incentives for orphan drugs.
part of the population.
• Bill in Congress which establishes mechanisms for reimbursement of orphan drugs and for
• Greater inequality patient care network.
between rural and
urban areas
India • Universal Public System • Reimbursements offered by the public sector are very low. Much of the cost is paid by the
• Dominance of the patient, which often makes use of very expensive drugs, such as orphan drugs, not feasible.
private sector. • Does not have a policy for R&D of orphan drugs.
• The most common demands in the country are calling for an orphan drugs policy similar to
the U.S., given the potential for research and development of new medicines in the country.
Source: Proposals for a National Policy on Rare Diseases: Prospectiva Consultoria, May 201220
According to this model, each state network must
6. Proposals for a practice both Primary Care and Specialized Care. In
National Policy on the case of rare diseases, first there will be the identi-
fication and tracking of individuals and families with
Rare Diseases in problems related to congenital anomalies, genetic er-
rors of metabolism, genetically determined diseases
the SUS and rare diseases that are not genetic.
Specialized care, in turn, will cover the multidiscipli-
nary approach and other specialized procedures rela-
The analysis of the best practices adopted worldwide
ting to cases that have been referred by primary care.
shows that the formulation of an all-encompassing
This level of assistance will consist of Units of Specia-
National Policy for Rare Diseases must include three
lized Care and Rehabilitation and Reference Centers.
complementary fronts:
The existence of Reference Centers equipped with
• The first concerns the organization of assistance,
qualified professionals and specialists is fundamental
ensuring patient access to care and treatments;
to ensure the achievement of early and accurate diag-
• The second is related to the adoption of differentia- nosis and for proper monitoring and evaluation of the
ted registration mechanisms to accelerate the entry clinical progression of patients.
and sale of orphan drugs in the Brazilian market;
Because treatment with orphan drug is expensive,
• The third refers to the policy destined to facilitate these experts will also help to define eligible patients
the incorporation of orphan drugs in the SUS. to receive these drugs, according to the premises esta-
blished by clinical protocols for the diseases.
For this model to work properly, the centers must
Assistance organization: access to be present throughout the national territory and be
care and treatment linked and financed by the SUS. Furthermore, they
A major goal on this front is to provide rapid and ac- must be integrated with each other and share infor-
curate diagnosis, by trained professionals, with rapid mation, to enable the creation of a National Registry
referral of patients to health services that best meet of Rare Diseases. Since today reference centers are
the needs identified – whether it be rehabilitation, linked to genetic research groups from universities
palliative treatment or availability of orphan drugs. not affiliated with the public system, it is not possible
This assistance structure should provide further mo- to obtain official data on these diseases. Not to men-
nitoring of these individuals, with monitoring of cli- tion the difficulty patients face getting assistance in
nical progression and the effects of the medication, an integrated manner at all stages of treatment,which
and provision of incentives for training and recogni- is exacerbated by the fact that the centers and gene-
tion of medical geneticists in the SUS. ticists are concentrated in the South-Southeast (see
map below).
The path proposed to enable this type of assistance
is the constitution of a National Network for Care of
Patients with Rare Diseases, built from the linkage of
Priority for granting registration
State Networks for Patient Care with Rare Disease.
Network coordination is a model of patient care that Like some countries with specific policies for rare di-
Brazil has already adopted successfully for some dise- seases, Brazil also has rules and laws that allow the
ases. This is the case with the National Policy of Blood speeding up of the process of registration of orphan
and Blood-Related Products, which includes the tre- drugs. The possibility of applying for priority analy-
atment of hereditary coagulation disorders. sis is something that already exists through the RDCRare Diseases: Contributions for a National Policy 21
Figure 7. Location of reference centers in Brazil.
1 reference center
2 reference centers
Source: Proposals for a National Policy on Rare Diseases: Prospectiva Consultoria, May 2012
28/12, ANVISA. The norm is being revised through Incorporation of orphan drugs in
public consultation and it is an instrument that can be the SUS
adjusted to meet the specificity of these drugs and the
health needs of patients. The proposed policy outlines a specific program and
clear and differentiated criteria for the incorporation
To benefit from priority analysis in the granting of of orphan drugs in the SUS. It relies on the fact that
registration, the product needs to first receive the or- these drugs are medically necessary for the treatment
phan drug status from ANVISA. The manufacturer of certain rare diseases. The unique profile of these
may request this status for the medication directed at diseases – low prevalence, the small number of par-
treatment of diseases with a prevalence of 1 to 10,000. ticipants in clinical trials, no other drugs for compa-
This condition automatically ensures priority analysis rison of effectiveness, high cost, among other parti-
and registration concession by ANVISA within 45 cularities – prevents them from fitting the criteria of
days. Concomitantly, the price assignment is made cost-effectiveness currently employed, and, therefore,
with CMED, accelerating the availability of the drug that they be incorporated via the SUS HTA (Health
on the market. Technology Assessment).You can also read