Psychological evaluation of patients undergoing cosmetic procedures - Practice guide
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Psychological evaluation of patients
undergoing cosmetic procedures
Practice guide
Acknowledgements We would like to acknowledge the following people who provided their expert review of the content of this practice guide: Dr Gemma Sharp MAPS Dr Ben Buchanan MAPS Dr Ryan Kaplan MAPS Australian Psychological Society. (2018). Psychological evaluation of patients undergoing cosmetic procedures. Melbourne, Vic: Author. Disclaimer and Copyright This publication was produced by The Australian Psychological Society Ltd (APS) to guide psychologists in best practice in the assessment of individuals seeking to undergo a cosmetic procedure. The information provided does not replace clinical judgment and decision-making. While every reasonable effort has been made to ensure the accuracy of the information, no guarantee can be given that the information is free from error or omission. The APS, their employees and agents shall accept no liability for any act or omission occurring from reliance on the information provided, or for the consequences of any such act or omission. The APS does not accept any liability for any injury, loss or damage incurred by use of, or reliance on, the information. Such damages include, without limitation, direct, indirect, special, incidental or consequential. Any reproduction of this material must acknowledge the APS as the source of any selected passage, extract or other information or material reproduced. For reproduction or publication beyond that permitted by the Copyright Act 1968, permission should be sought in writing. Copyright © 2018 The Australian Psychological Society Ltd
Table of Contents
Introduction ...................................................................................................................................... 4
Consultations and external review....................................................................................................... 4
Definition of cosmetic procedures as covered in this practice guide..................................... 4
Procedures not considered ‘cosmetic’ and not covered in this practice guide ................... 5
Limitations ...................................................................................................................................................... 5
Background ....................................................................................................................................... 6
Prevalence of people seeking cosmetic procedures or surgery................................................. 6
Potential adverse outcomes .................................................................................................................... 6
Patient characteristics associated with adverse outcomes ....................................................... 7
Psychosocial assessment of adults ............................................................................................... 9
Aims and outcomes of an assessment ............................................................................................... 9
Assessment step-by-step.......................................................................................................................... 9
Rating scales and assessment measures ........................................................................................ 13
Concluding the assessment ................................................................................................................. 14
Psychosocial assessment of specific populations .................................................................... 15
Assessment of transgender individuals .......................................................................................... 15
Assessment of minors............................................................................................................................. 15
Summary ........................................................................................................................................ 17
References ..................................................................................................................................... 18
psychology.org.au 3Introduction
In October 2016, the Medical Board Consultations and external review
of Australia issued the ‘Guidelines for
A draft version of this practice guide was reviewed
registered medical practitioners who by experts in the area (please see the section
perform cosmetic medical and surgical ‘Acknowledgements’ for a list of these experts).
procedures’.1 The Medical Board of Australia The writing and editorial team revised the guide in
response to reviewer suggestions.
guidelines make clear that some patients
may be unsuitable for cosmetic surgery and Reviewers were asked to review and provide feedback
on the guide, including a focus on the following four
mandate the referral of patients of concern
questions for each section:
for a psychological evaluation to establish
• Are there significant gaps (in the coverage of this
their suitability for the intended procedure. topic, the literature, other)?
• Are there errors in the content?
• Is the structure logical and easy to use?
Under the Medical Board of Australia
guidelines, a patient is considered to
require an assessment prior to undergoing Definition of cosmetic procedures
a cosmetic procedure if they are: as covered in this practice guide
• under the age of 18 and seeking a major
cosmetic procedure; or
The ‘Guidelines for registered medical
• an adult or a minor displaying indicators practitioners who perform cosmetic
of significant underlying psychological medical and surgical procedures’ provide
problems which may make them an the following definitions for cosmetic
unsuitable candidate for any cosmetic procedures and these have been adopted in
procedure. this practice guide:
Cosmetic medical and surgical procedures:
These are operations and other procedures that
This practice guide has been developed by the revise or change the appearance, colour, texture,
Australian Psychological Society (APS) to provide structure or position of normal bodily features
guidance to APS member psychologists undertaking with the dominant purpose of achieving what
assessments of individuals intending to undergo a the patient perceives to be a more desirable
cosmetic procedure, for their psychological suitability appearance or boosting the patient’s self‑esteem.
for such a procedure.
Major cosmetic medical and surgical procedures
This practice guide reviews and synthesises current (‘cosmetic surgery’): These procedures involve
evidence about best practice in the assessment of cutting beneath the skin. Examples include;
such individuals. breast augmentation, breast reduction,
rhinoplasty, surgical face lifts and liposuction.
Minor (non-surgical) cosmetic medical
procedures: These procedures do not involve
cutting beneath the skin, but may involve
piercing the skin. Examples include: non-surgical
cosmetic varicose vein treatment, laser skin
treatments, use of CO2 lasers to cut the skin,
mole removal for purposes of appearance,
laser hair removal, dermabrasion, chemical
peels, injections, microsclerotherapy and hair
replacement therapy.
4 Psychological evaluation of patients undergoing cosmetic proceduresProcedures not considered ‘cosmetic’ This practice guide applies to plastic surgery when it is
performed only for cosmetic reasons. It does not apply
and not covered in this practice guide to reconstructive surgery or surgery considered to be
The ‘Guidelines for registered medical practitioners medically justified.
who perform cosmetic medical and surgical In practice, this can be a grey area with some patients
procedures’ provide the following definitions for reporting the motivation to be functional or physical
procedures not considered cosmetic and so not whilst also desiring surgery for cosmetic reasons.2
included in this practice guide:
Regardless, determining whether a procedure is
Procedures which are medically justified: Surgery or a medically justified ultimately falls to the treating
procedure may be medically justified if it involves the medical practitioner. For the psychologist, of primary
restoration, correction or improvement in the shape concern in the evaluation is the client’s state of mind,
and appearance of body structures that are defective emotional and cognitive preparedness, and their
or damaged at birth or by injury, disease, growth or psychological fitness to undergo the procedure.
development for either functional or psychological
reasons. Surgery and procedures that have a medical
justification and which may also lead to improvement Limitations
in appearance are excluded from the definition.
While every effort has been made to provide the
Reconstructive surgery: The medical specialty of reader with current, up to date information on the
plastic surgery includes both cosmetic surgery and assessment of this client group, research is ongoing
reconstructive surgery. Reconstructive surgery differs and relevant new original studies and systematic
from cosmetic surgery as, while it incorporates reviews may be published after this practice guide has
aesthetic techniques, it restores form and function as been finalised. As such, clinicians need to continue
well as normality of appearance. to update their knowledge and skills and use their
professional judgement when evaluating clients.
Medical Board of Australia
GUIDELINES FOR REGISTERED
MEDICAL PRACTITIONERS WHO
PERFORM COSMETIC MEDICAL
AND SURGICAL PROCEDURES
1 October 2016
MBA1608 03
psychology.org.au 5Background
Prevalence of people seeking Potential adverse outcomes
cosmetic procedures or surgery Although this field of research is characterised by
Unfortunately national data is not available on methodological limitations, what is known suggests
the prevalence of cosmetic procedures or surgery that the majority of people seeking a cosmetic
use in Australia for a number of reasons. Currently, procedure are satisfied with the outcome and report
cosmetic procedures can be performed by a range of improvements in self-esteem, quality of life and
practitioners, including medical practitioners such relationships.5-7 Research also suggests however that
as plastic surgeons, GPs and dermatologists, and a minority do experience adverse psychological and
non-medical practitioners such as beauticians, and social outcomes.7
there is no single body to which such data is reported; Where there is dissatisfaction with the outcome of
secondly such procedures are elective, so are not a procedure, the patient may experience personal
covered and therefore recorded by Medicare.3 distress and adjustment problems, social isolation,
relationship strain, requests for additional and
unnecessary procedures, and anger toward the service
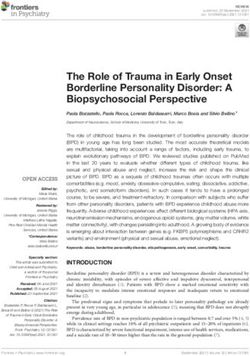
A survey conducted by the Cosmetic Physicians provider and his or her staff.7 In some individuals,
College of Australasia in 2015, estimates that pre-existing mental health concerns, particularly
Australians collectively spend more than 1 billion body dysmorphic disorder (BDD) may indeed worsen
dollars a year on minimally or non-invasive following the procedure.8
cosmetic procedures, with around one quarter Those seeking cosmetic procedures may be at higher
of the 1020 respondents reporting to have risk for self-harm and suicide than the general
had some kind of procedure performed in the population, though research is scant.9-12 While the
preceding month, double the number reported reason for this increased risk is unclear, it is speculated
in the previous year.4 There is a consensus that that unmet expectations (particularly where
the use of cosmetic surgery in Australia is on expectations are unrealistic), mental health issues, or
the rise.3 distress associated with medical complications arising
from the procedure may all contribute to negative
mood, and to the increased risk of suicide.12, 13
In Australia (2015)
Most common age
More than 35-50
$1b
spent per year on Most popular procedure
non-invasive procedures for women:
breast augmentation
90% Most popular procedure
of procedures are
performed on women for men:
liposuction
6 Psychological evaluation of patients undergoing cosmetic proceduresResearch suggests that
unrealistic goals – such as a
desire to achieve perfection
BDD in particular is associated with an increased risk rather than for more realistic,
for suicide and self-harm, with rates similar to that of
anxiety and depression and greater than that of most
specific or functional
other mental health disorders.11, 14-16 In addition to the improvements are associated
reasons for increased suicide risk above, which are all with poorer outcomes.17
relevant to understanding suicide risk in BDD, being
refused cosmetic surgery or other cosmetic procedures
is also thought to be a particular risk factor, due to the Unrealistic goals or expectations
importance people with BDD can place on cosmetic
Research suggests that unrealistic goals – such as
surgery being a solution to their distress, and the
a desire to achieve perfection rather than for more
degree of distress they experience in relation to their
realistic, specific or functional improvements are
perceived flaw.9, 11
associated with poorer outcomes.17 Unrealistic
Cosmetic professionals treating unsuitable patients expectations include those in which the hope is for
are at risk of experiencing adverse outcomes distal, exaggerated or global life improvements, such
themselves, including harassment by the patient, as obtaining a job promotion, or attracting a new
repeated demands for unnecessary procedures, romantic partner. Unrealistic expectations may also be
complaints, and legal action.7, 9 Practitioners may also reflected by vague descriptors such as a desire to be
experience threats of physical violence or in rare cases, ‘prettier’ or for a feature to be ‘nicer’.12, 18
actual harm from dissatisfied clients.9
External motivations for the procedure
External motivations such as family or partners
Potential adverse outcomes include: influencing the client to undergo the cosmetic
• dissatisfaction with the outcome of the procedure rather that the client themselves being the
procedure driver of the process, or the belief that the surgery or
procedure will improve relationships, the likelihood of
• personal distress and adjustment problems
employment, or popularity are also associated with
• social isolation poorer outcomes.7, 13
• relationship strain
• requests for additional and unnecessary Identity concerns
procedures In some cases, a certain physical characteristic
• anger toward the service provider and staff may be linked to a patient’s personal, cultural, or
familial identity. Without adequate consideration
• worsening of pre-existing mental health
of the ramifications of altering this trait, the patient
concerns (particularly body dysmorphic
may experience a loss of identity or ructions within
disorder (BDD))
relationships following the loss of a shared physical
• risk of self-harm. familial or cultural characteristic.19
Negative self-image and other psychosocial issues
Individuals seeking cosmetic procedures or surgery
Patient characteristics associated do so in response to dissatisfaction with an aspect
with adverse outcomes of their appearance, and the majority report being
satisfied with the outcome of their cosmetic procedure
Research suggests that adverse outcomes are more and with the specific change in their appearance.20
likely in patients with certain characteristics, most Many also experience broader positive outcomes post
commonly those with: cosmetic intervention, such as increased confidence
• unrealistic goals or expectations for the procedure and a more positive body image.7, 21
• external motivations for the procedure A positive global self-concept, despite dissatisfaction
• identity concerns with an aspect of one’s physical appearance, is
• negative self-image and other psychosocial issues associated with good outcomes from cosmetic
interventions.22 Satisfied patients for example often
• certain mental health concerns such as body
report feeling that their outward appearance did not
dysmorphic disorder.
match their otherwise positive internal self-concept,
psychology.org.au 7and cite wanting to align the two as motivation for
surgery.22 Therefore, apart from dissatisfaction with a
specific aspect of their appearance, those experiencing
Risk factors for
positive outcomes from their cosmetic procedure poorer outcomes
typically report being otherwise satisfied with their • unrealistic expectations for
overall body image and sense of self.23 the procedure
• external motivations or being
Conversely, pre-existing poor self-concept, low self- influenced by others to have the
esteem, negative global body image, and relationship procedure
distress are associated with poorer outcomes.7 • identity concerns
• negative self-image
Mental health concerns • relationship issues
Although the actual prevalence of mental health • certain mental health issues such
disorders in this population is poorly understood9 as body dysmorphic disorder.
a sizable minority – a proportion greater than that
found in the general population – are thought
poorer psychological outcomes, repeat cosmetic
to experience mental health issues, which
treatments, unnecessary surgical interventions, and
research suggests may increase the risk for
dissatisfaction with the procedure.13, 33, 34 Given the
patient dissatisfaction and poorer outcomes.9, 24-26
likely dissatisfaction, secondary risks include hostility
Though there is little research in this area23 the full
towards treating medical staff, increased risk for
complement of mental health disorders is likely seen
self-harm and although rare, increased risk of harm
in the cosmetic procedure-seeking population,27 with
to others such as the treating practitioner.8, 11, 34, 35
depression, anxiety, eating disorders and trauma
There is also a risk of worsening of pre-existing
history believed to be overrepresented.7, 9, 17, 25, 28
mental health concerns, body image issues or
It must be noted however that high prevalence mental BDD symptoms.25, 36, 37
health disorders should not be considered ‘absolute’
Degree of distress, reflecting substantial
contraindications for cosmetic procedures as research
preoccupation and dissatisfaction with appearance,
evidence is inconsistent regarding the benefits and
is considered an important factor in predicting poor
adverse outcomes associated with a range of mental
post-procedural outcomes in individuals with BDD
health issues.5, 9
with severity of symptoms associated with poorer
Body dysmorphic disorder (BDD) however is outcomes.38 Mild to moderate BDD symptoms
generally considered a contraindication for cosmetic may not necessarily preclude cosmetic procedures,
procedures and has received the most attention in however in such cases it is important that patient
studies characterising cosmetic procedure-seeking expectations are well-managed.39, 40
populations. BDD is estimated to affect around
1.9% of the general population29 with slightly
more females affected (2.1%) than males (1.6%).29 Within an evaluation of an individual’s suitability
Within populations seeking cosmetic surgery to undergo a cosmetic procedure, it is important
or other procedures however, the prevalence is for a psychologist to conduct a thorough
considerably higher. Among American samples, rates psychological and psychosocial evaluation,
of BDD among individuals presenting for cosmetic attending to all aspects of the client’s mental
surgery range from 7-13%.9, 29 International studies health, risk factors, and other factors relevant
using rigorous methods of evaluation estimate to understanding the client’s motivation for the
the prevalence of BDD cosmetic surgery-seeking cosmetic procedure and expectations about the
populations to be in the range of 3.2-16%. Higher psychosocial impact of the procedure.
rates of BDD have been reported in those seeking
rhinoplasty,29, 30 dermatological treatments,31 and
labiaplasty.9, 32
Unlike other mental health issues where mixed
outcomes of cosmetic procedures have been
reported, BDD is generally associated with
8 Psychological evaluation of patients undergoing cosmetic proceduresPsychosocial assessment
of adults
Aims and outcomes of an assessment
Aims of an assessment:
The primary aim of conducting a psychological • Assess the client’s psychological suitability to
assessment is to evaluate the client’s suitability to undergo the procedure
undergo a proposed cosmetic procedure, so as to • Assess and address risk
reduce the incidence of adverse outcomes and provide • Evaluate and identify any contraindications
greater opportunity for those needing psychological for the procedure
support and treatment, to access the assistance • Determine whether psychological
they require. intervention prior to the procedure may be of
The assessment therefore aims to: benefit
• Reduce the incidence of adverse psychological
• evaluate the psychological suitability of the
outcomes for the client.
candidate to undergo the intended procedure,
and assess their risk of experiencing a poor
psychological outcome
• evaluate and address any identified risk of suicide,
Assessment step-by-step
self-harm or harm to others, and determine A comprehensive psychosocial assessment generally
whether, in the client’s individual situation, involves thorough assessment and consideration of
such a risk may be a contraindication for the the client’s:
intended procedure
• psychological and social functioning
• determine whether psychological intervention
• developmental history
prior to undergoing a cosmetic procedure might
be warranted to reduce the risk of an adverse • educational history
psychological outcome • relationship history
• reduce the incidence of adverse psychological • current mental state
outcomes associated with unnecessary procedures, • mental health, including the identification and
or procedures where the prognosis is poor. evaluation of any possible mental health disorders
There are three potential outcomes of a psychosocial and associated symptoms.
assessment. The psychologist may determine that: An assessment ideally involves not only interviewing
• there are minimal or no concerns for the person’s and observing the identified patient, but obtaining
suitability to undergo the cosmetic procedure collateral information from family and significant
others.27
• there are concerns regarding the person’s current
readiness to undergo the cosmetic procedure, The next section details the key areas to evaluate
however with psychological intervention the specifically around a clients’ intended cosmetic
patient may address those issues, and following procedure.
re‑evaluation may be considered adequately
prepared and a suitable candidate for the procedure
• the person is considered a poor candidate for
the cosmetic procedure or surgery being at
significant risk of an adverse psychological
outcome, with the recommendation made that
the procedure not proceed. A recommendation
for psychological intervention might be made to
address psychological concerns identified during
the assessment.
psychology.org.au 9Assessing the degree of pre-occupation with the
When conducting an evaluation of a client perceived flaw may also be informative in determining
seeking a cosmetic procedure, assessment the client’s suitability for the intended procedure.
should also focus on evaluating the client’s: Clients who are highly pre-occupied with the perceived
flaw are more likely to have poorer psychological
• perception of the identified ‘flaw’ and degree
outcomes from cosmetic procedures.41
of pre-occupation with the ‘flaw’
• history of dissatisfaction with the perceived History of dissatisfaction with the perceived flaw
flaw and reason for seeking change now and reason for seeking change now
• motivations for seeking the cosmetic Clients may report longstanding dissatisfaction or
procedure, and their desired outcomes, goals an emerging dissatisfaction, as well as a range of
and expectations triggers that may have given rise to their desire for
• consultations with other cosmetic practitioners the cosmetic procedure. This may include a history
and previous cosmetic interventions of teasing, bullying, negative comments from a sexual
• relationships with others and their degree of partner, partner violence, or other significant life
support for the cosmetic procedure events.5, 7, 42-48
• self-concept and self-esteem in relation to the
Motivations, desired outcomes, goals, and
physical trait
expectations for the cosmetic procedure
• cultural and familial identity in relation to the
Expectations around cosmetic surgery have been
physical trait
categorised as surgical, psychological, and social.
• mental health, and the presence or absence Surgical expectations address the specific physical
of a mood, anxiety, or eating disorder, body changes expected as a result of the procedure.
dysmorphic disorder, or any other mental Psychological expectations include those which
health disorder which may significantly relate to potential improvements in psychological
impact on the client’s perception of their body functioning as a result of surgery. Social expectations
and their body image, and the severity of any address the potential social benefits.12
such disorder and its symptoms.
Better outcomes are believed to be seen in people for
whom expectations are realistic, specific, and proximal
to the procedure. Poorer outcomes are more often
Perception of the identified ‘flaw’ and degree of seen in those for whom expectations are unrealistic,
pre‑occupation with the ‘flaw’ vague and distal (for example, believing a procedure
This includes an evaluation of the accuracy of the will change one’s entire life or result in greater career
client’s perception and whether the client’s perception opportunities).
of the physical characteristic in question is realistic
and reasonable, whether the perceived difference In the assessment, include an evaluation of:
has been noted by others, and whether the degree of • whether the client’s goals for the procedure are
difference perceived by the client, or their response to realistic
this perceived difference is exaggerated or distorted in • the motivations for undergoing the procedure
any way. and what is driving the client’s desire to alter their
Poorer outcomes have been found in patients who appearance
are vague in their descriptions of what it is about • the client’s understanding and appreciation of
the specific body part they do not like, and what what the procedure involves, the limitations of
they would like changed; for example, rather than the procedure, and any associated risks of adverse
describing the length of their nose, or a bump, they outcomes.49
report just ‘not liking’ their nose, that it is just ‘not
right’ for their face, or that they just feel ‘ugly’.8, 35
Consultations with other cosmetic practitioners or
Seeking clarification from the client about the desired
experience of previous cosmetic interventions
change in appearance is therefore an important aspect Clients may have a history of seeking treatment for the
of a psychological evaluation. perceived flaw or for other perceived flaws. Consulting
multiple practitioners, having a history of undergoing
10 Psychological evaluation of patients undergoing cosmetic proceduresmultiple procedures, or having previously been refused appearance with an already positive body image and
treatment, are considered ‘red-flags’ for BDD and for self-concept.21
poorer outcomes from cosmetic interventions.33, 35
In the assessment therefore, include evaluation of
the client’s self-concept, identity and self-esteem in
Relationships and the support of others
relation to the perceived flaw.
Relationships with others can have a large influence
on the person’s desire to undergo a cosmetic Cultural, familial and personal identity
procedure. Family and friends can have a supportive
For some, particularly in regards to facial features and
influence, a coercive influence, or be significantly
cosmetic procedures to alter facial characteristics,
opposed to the procedure. The client may also believe
cultural and familial identity may be important to
that the procedure will improve their relationships
consider. Explore the perceived flaw in terms of it
with others, such as with their partner or their chance
being a potential cultural or familial trait, and whether
of attracting a partner.
this forms part of the person’s identity, even if the trait
A history of bullying or teasing from childhood or itself is seen in a negative light.
more recent negative comments from a partner
Explore a range of potential outcomes in the event the
may contribute to the client’s perceptions of
characteristic is altered – might it affect relationships
themselves.42-46 Research suggests an association
with others, with the self? Loss of identity might result
between intimate partner violence and likelihood of
where the physical characteristic in question is shared
undergoing cosmetic surgery.5, 46
amongst family members or a certain cultural group.21
Although rare, body dysmorphic disorder ‘by proxy’
Some patients may require more psychological
has also been documented, in which the focus is
adjustment to their change in appearance than
on an imagined defect or flaw in the appearance
others, which may relate to the type of procedure.
of another individual. The preoccupied individual
More extensive ‘type-change’ procedures which more
can exert considerable influence on the other and
radically alter appearance (such as rhinoplasty) may
can be a significant motivator for the procedure.50, 51
require more adjustment and may result in more
The assessment of the client should therefore screen
adverse outcomes in regards to loss of identity than
for this, particularly in cases where the presenting
‘restorative’ procedures (such as botox or facelifts).52
client is a minor and is being encouraged towards the
procedure by a parent or guardian.
Mental health
An evaluation of the client’s relationships with others A comprehensive mental health assessment, covering
therefore includes clarification of whether: the full range of potential mental health disorders
• members of the client’s social and family network should be conducted. Such an assessment includes
share a similar view of the client’s perception of the a mental state examination and symptom review,
perceived flaw covering in particular, diagnostic criteria for mood
• family or other significant people are coercing or disorders, anxiety disorders, eating disorders and body
otherwise driving the client’s motivation for the dysmorphic disorder; these being the most commonly
procedure cited mental health concerns in the cosmetic
procedure-seeking population. The main diagnostic
• the client is seeking to address relationship stress
criteria are noted below, however more complete
(such as improve a romantic relationship) or
criteria and specifiers are found in the most recent
attract a potential partner through altering their
edition of the Diagnostic and Statistical manual for
appearance.
Mental Disorders.53
Self-concept and self-esteem The client should also be asked about whether
Better outcomes are seen in clients where their symptoms they are experiencing impact on their
self-worth and self-concept are not defined by the day-to-day functioning including their capacity to
presence or absence of the perceived flaw. While self- attend to their work, activities of daily living, and
esteem might improve with a change in appearance, relationships.54
clients are more likely to experience positive
Interview questions, as in all interviews, should aim
psychological outcomes from their cosmetic procedure
to clarify the presence, absence and duration and
if what they are seeking is to align their external
frequency of symptoms, without leading the client
psychology.org.au 11to answer in a specific way.54 Observations of client Key issues to consider in the assessment of BDD:
behaviour in the context of their reported mood and 1. I s the client preoccupied with a perceived defect
experiences should also be incorporated into the or flaw in their physical appearance that is not
assessment to aid diagnosis.55, 56 observable or appears only slight to others?
2. Does the patient perform repetitive behaviours
Body dysmorphic disorder
in response to the concerns (e.g. scrutinising
Body dysmorphic disorder (BDD) is the most the feature of concern in the mirror, repeatedly
researched and most commonly cited disorder seeking reassurance, excessive grooming; skin
associated with a heightened risk for adverse picking; excessive use of makeup or other products;
outcomes in cosmetic procedure-seeking populations. camouflaging the feature with clothing, hats, or
The assessing psychologist must therefore be hairstyles)?
particularly familiar with the key criteria so as to
3. D
oes this preoccupation cause clinically significant
appropriately evaluate the client’s presenting issues,
distress or impairment in social, occupational or
behaviours and symptoms.
other important areas of functioning?
4. I s the preoccupation with appearance more
consistent with symptoms of an eating disorder
(i.e. concerns relate primarily to body fat or weight),
than with a diagnosis of BDD?53, 57
5. I s the preoccupation with appearance limited
to discomfort with primary or secondary sex
characteristics and better explained by gender
dysphoria?53
Mood disorders
In order to clarify if the client is experiencing a
current major depressive episode, the client should be
Body dysmorphic disorder DSM-5
asked about:
criteria:
• the quality, responsiveness, and pervasiveness of
• Preoccupation with appearance or flaws that their mood
are not visible or appear minor to others
• the degree of interest and pleasure in activities they
• Repetitive behaviours in response to
typically enjoy
appearance (e.g., excessive mirror checking
or/and grooming, comparing appearance to • their appetite and whether they have experienced
others) any weight gain or loss
• The preoccupation causes clinically significant • how they are sleeping, including lifestyle factors
distress and impacts on daily functioning. which may be impacting on the quality of sleep
• Preoccupation with appearance is not better • whether they are experiencing agitation or
accounted for by an eating disorder or by
conversely, a sense of ‘slowing’ of movements
body dissatisfaction associated with gender
dysphoria • their energy levels and experience of fatigue
• their sense of self-worth or worthlessness, or
excessive or inappropriate guilt
As people with BDD may wish to present in a positive • their ability to think, concentrate, or make decisions
light during evaluation, they may not report a full • their thoughts of life, death or suicide.54
range of symptoms to the assessor. Questions which
do not lead the client are important, and informal The assessor should also clarify:
observations of the client outside of the consultation, • the degree to which the client’s depressive
such as in the waiting room, may reveal behaviours symptoms are linked to their dissatisfaction about
not evident during the session.58 their physical appearance
• the pervasiveness of the client’s symptoms and
circumstances in which symptoms improve or worsen
12 Psychological evaluation of patients undergoing cosmetic procedures• whether the client ruminates about their physical Risk
appearance or experiences excessive negative Self-harm/suicide
thinking in relation to their appearance. Due to the increased risk of self-harm and suicidality
in this population, a thorough assessment of suicide
Anxiety disorders
risk must be included as part of a comprehensive
The presence of any anxiety disorder should be psychological assessment.10, 11, 15, 75
considered when conducting a mental health
assessment. Concern with appearance can translate The assessor should use a collaborative approach to
to anxiety in social situations and concern with obtain specific details about whether:
negative appraisal by others.59-62 While most research • the client has had thoughts about death, dying, or
has looked at state and trait anxiety via self-report,63 that life is not worth living
anxiety disorders of particular relevance in this • the client has made any plans for suicide
population are:64-66
• the client has access to means of self-harm/suicide
• social anxiety disorder (social phobia)
• the client has a history of attempted suicide.75-77
• generalised anxiety disorder
If there is concern for the client’s risk for suicide, a
• panic disorder collaborative, problem-solving approach should be
• agoraphobia. adopted to provide the least restrictive treatment
and risk-management response which maintains the
Again, the assessor should clarify if the person’s
client’s safety.75
concerns with their physical appearance are relevant
in understanding the aetiology of the anxiety In addition, some people with BDD may engage in, or
symptoms, such as social anxiety being a consequence consider performing self-mutilating acts in an attempt
of self-consciousness related to the person’s physical to address their perceived flaw, and as such, this risk
appearance. should also be evaluated.11
Harm to others
Eating disorders
Although rare, there is a potential risk for harm or of
Research studies report that some people seeking litigation directed to others involved in the cosmetic
cosmetic procedures, particularly body-contouring procedure such as treating staff, particularly when the
surgery may have an underlying eating disorder, with client has a pre-existing mental health or personality
the preoccupation with body weight and size thought disorder, and where the client is dissatisfied with
to influence their contemplation of cosmetic methods the outcome of a procedure or where a cosmetic
to further alter their body shape.67-70 Potential procedure is withheld due to concerns for adverse
symptoms of an eating disorder should therefore be outcomes.34, 35, 78 As such, an assessment of the
carefully screened and assessed. client’s thoughts around treating staff, their beliefs
Assessors should be familiar with the key diagnostic around the role of staff in the client’s distress, and
criteria of: thoughts or plans of aggression directed at others
• anorexia nervosa should be included in a comprehensive psychological
assessment.
• bulimia nervosa
• binge-eating disorder
• other specified feeding and eating disorders.
Rating scales and assessment
measures
Personality disorders
Client self-report and clinician-administered
Personality disorders, particularly clusters B and C
assessment measures are available which may
may be more prevalent in this population and may
assist in the evaluation of the client. While these
increase the risk for adverse outcomes of cosmetic
tools identify areas of concern in the client, these
procedures, and as such should be screened for within
scales have undergone limited validation, are not
the assessment.71-74
comprehensive enough to evaluate all aspects of a
client’s functioning, and do not provide a definitive
diagnosis or definitive evaluation of suitability to
undergo a cosmetic procedure, and should only be
used to flag further areas of assessment for the
psychology.org.au 13psychologist.79, 80 Screening tools do not take the Client feedback
place of a comprehensive but can be considered one For the client, feedback should be provided both
aspect of a broad and comprehensive psychosocial in person and in writing in the form of a detailed
evaluation.39 letter or report, to facilitate understanding of the
Tools which may be of use to the clinician include the approach taken in the assessment, and the rationale
Derriford Appearance Scale (the DAS-59 and its short for the conclusions drawn. Feedback to the client
form, the DAS-24),81 the PreFACE79, 80 and the Q-series should be provided in a collaborative, sensitive and
of patient-reported outcome measures.82-89 clear manner which takes into consideration the
client’s own vulnerabilities, mood and mental health
The Cosmetic Procedure Screening Scale (COPS),90, 91 issues.104 Having a clear, evidence-based rationale is
the Body Dysmorphic Disorder Questionnaire of particular importance when contraindications for a
(BDDQ), 92 the Dysmorphic Concern Questionnaire cosmetic procedure are identified
(DCQ),93, 94 the Body Image Disturbance Questionnaire
(BIDQ),95 the Multidimensional Body-Self Relations Where feedback is likely distressing for the client (as in
Questionnaire-Appearance Scales (MBSRQ-AS)95, 96 the case where the recommendation is to not proceed
and the Appearance Anxiety Inventory (AAI)97 are with a cosmetic procedure for someone meeting
screening tools for body image disturbance and BDD criteria for body dysmorphic disorder),105 issues of
in particular. risk should be considered and evaluated during the
feedback process with any necessary risk management
There are several clinician administered clinical plans put in place. A key risk is that a patient
interviews such as the Yale-Brown Obsessive– denied access to a procedure will immediately seek
Compulsive Scale Modified for Body Dysmorphic treatment elsewhere (“doctor shopping”).33 Clearly
Disorder (BDD-YBOCS),98, 99 the Structured Clinical communicating the rationale for the assessment
Interview for DSM-5 (SCID-5) with optional modules outcome, developing strong rapport and offering an
for the evaluation of BDD100, 101 and the Mini alternative solution for their distress (i.e. referral to
International Neuropsychiatric Interview – Plus appropriate psychological treatment) is important in
(MINI-Plus) which includes questions around BDD.102 attempts to mitigate this risk.106
These clinician administered tools may assist the
psychologist in the assessment of the patient’s Referrer feedback
symptom profile as part of a broader assessment.
For the referrer, feedback should ideally be presented
both verbally and in writing to ensure clarity regarding
Concluding the assessment the assessment outcome and to provide adequate
support for the referrer’s follow-up with the client.
Providing feedback to the client and referrer
In providing feedback to the referring practitioner,
The psychologist should provide the client and referrer the psychologist must be mindful of his or her
timely feedback on their opinion of: responsibility to protect the client’s privacy and
• the client’s readiness for the proposed cosmetic confidentiality. Feedback to the referring practitioner
procedure should be adequate to answer the referrer’s questions
• issues the client presents with that may raise their regarding the client’s fitness to undergo the proposed
risk for an adverse psychological outcome and how cosmetic procedure. Issues which arise as part of the
these issues may result in adverse psychological assessment that may help inform the psychologist of
outcomes the client’s fitness to undergo the procedure but which
• recommendations for further evaluation which may are not necessary for the referring agent to know
help clarify issues regarding client risk should not be disclosed.
• recommendations for psychotherapy which may Psychologists are advised to familiarise themselves
help address issues that increase client risk for with the APS Code of Ethics, and the APS Ethical
adverse psychological outcomes and prepare the Guidelines on Confidentiality which relate to the
client for their planned procedure sharing of information with a third party.
• whether the cosmetic procedure is contraindicated
for that client, and the rationale for that conclusion.
Psychoeducation regarding contraindications
should also be provided to the client.103
14 Psychological evaluation of patients undergoing cosmetic proceduresPsychosocial assessment
of specific populations
Assessment of transgender Issues to consider when assessing minors
individuals Capacity to consent
When working with minors, practitioners need to
Clients who identify as transgender may seek cosmetic determine if the young person is capable of providing
procedures to alter their appearance in a way that informed consent for psychological assessment and/
more closely aligns with appearance norms of the or treatment and if parental or guardian consent is
gender with which they identify.107-109 Such clients may required or would be in the best interests of the young
experience significant dysphoria about their body or person.122
other aspects of their physical appearance.110 In their
assessment of transgender clients, it is important In the case of the young person intending to undergo
that psychologists do not confuse body dysphoria a cosmetic procedure, informed consent also requires
secondary to gender dysphoria, with BDD.53, 111 that the young person understands fully the nature
of the proposed intervention, expected outcomes
It is also important to note that while body including any initial discomfort, limitations to what
dysphoria secondary to gender dysphoria is distinct can be provided, what is required of them in terms of
from BDD, BDD can affect people of all genders, self-care during recovery, and any potential adverse
including transgender individuals and individuals events or risks involved.117, 122
experiencing gender dysphoria.113 If an evaluation of
their suitability for a cosmetic procedure has been A number of APS resources are available to support
requested, as with any other patient, a comprehensive members in considering the ethical implications
mental health and risk assessment should be around gaining informed consent from minors:
conducted.114 • Ethical guidelines for working with young people
• Ethical guidelines on confidentiality.
Assessment of minors
Influence of peers and the media
As with adult evaluations, a thorough assessment While concerns with body image in young people
of minors includes an evaluation of the young is not a new phenomenon, increased exposure to
person’s desired goals, whether their expectations are idealised images of physical appearance via social
realistic, factors motivating them to seek cosmetic media, and through television programs revolving
enhancements, and their mental health,115-117 around cosmetic enhancements123 are adding to
particularly regarding symptoms of BDD which most the influences on adolescents’ satisfaction with
commonly emerge in adolescence.111, 118 their body image,124, 125 their acceptance of cosmetic
However there are additional issues to consider in interventions, and their desire to seek cosmetic
the evaluation of an adolescent’s preparedness and interventions to alter their appearance.126-129
suitability to undergo a cosmetic procedure. These Exposure to teasing and bullying may also play a
relate to their physical and emotional maturation significant role126, 130 the incidence of which appears
and changes that are likely to occur as a natural to peak during adolescence.42
course of development,115, 119 their developing sense Some argue that cosmetic procedures can indeed
of self and identity,120 and the potential for influence decrease bullying and improve social functioning in
by others.117, 121 Their capacity to provide informed young people.131 It is important however for the young
consent should therefore be carefully considered, as person to appreciate that altering one’s appearance
well as the role of parents or guardians in supporting cannot guarantee improved social connectedness.52
the decision-making process.117
Finally, undue influence of others, including family
must be considered. As mentioned, whilst exceedingly
rare, cases of body dysmorphic disorder ‘by proxy’
have been reported, where the focus is not on the self,
but on a perceived flaw or flaws in the appearance
of another individual. The preoccupied individual
can exert considerable influence on the other and
psychology.org.au 15can be a significant motivator for the procedure;50, 51 In addition, changes in weight and body shape as
a particular concern where the presenting client young people mature means that some outcomes
is a minor and is being influenced to undergo the from cosmetic procedures may also alter over time,
procedure by a parent or guardian.51 and the desired effects may be lost or distorted.
For example, young females often gain weight in
Body image and concerns for what is ‘normal’
their early 20s, and with that, dissatisfaction with
Along with a developing self-concept and concern breast-size may decrease without intervention.
for physical appearance, concern for what is ‘normal’ Some research suggests improvement in body image
may also emerge. Preliminary research suggests generally occurs in early adulthood with or without
that in some cases, education regarding normal cosmetic interventions.119
development and physical changes that are likely to
occur over the course of physical maturation can allay
fears and decrease the desire to change one’s physical
appearance through cosmetic procedures. This seems
particularly the case for adolescent labiaplasty.132
16 Psychological evaluation of patients undergoing cosmetic proceduresSummary
When assessing adults for their suitability to undergo When assessing minors, a similar processes to that
a cosmetic procedure, it is important to consider the of adults is followed, although aspects unique to the
broad range of factors which can increase the risk for developmental period, including ongoing physical
adverse psychosocial outcomes. Whilst the evidence development, the common experience of decreased
is mixed regarding the psychosocial outcomes for satisfaction with body image, the influence of peers
individuals with depression, anxiety and other high and family, the development of identity and changes in
prevalence disorders,5, 9 a substantial body of evidence self-esteem, and heightened concerns for appearance
suggests an increased risk for adverse psychosocial and what is ‘normal’ can all complicate the picture.119,
outcomes for those presenting with body dysmorphic 122, 132, 133
disorder, including post-procedural dissatisfaction,
Assessment of minors therefore includes consideration
distress, litigation, risk of self-harm, and in rare cases,
of these normative aspects of psychosocial
risk of harm to others.8, 11, 34, 35
development. The assessment of the adolescent client
A range of other factors, such as unrealistic goals or also includes establishing that the client has sufficient
expectations, external motivations for the procedure, maturity to make an informed decision, and has the
inadequate consideration of possible challenges to support of significant others such as parents.133 The
personal identity with changes in appearance, low influence of others, including the media, peers and
self-esteem beyond dissatisfaction with an aspect family is also important, to ensure that motivations
of appearance, and coercion or lack of support from for intervention are the client’s, and not externally
family or friends also increase the risk for adverse driven.119, 134
psychological outcomes and need to be considered
Clients, whether adult or adolescent, should be
when evaluating the client.7, 9, 12, 13, 17-19
evaluated on a case-by-case basis. Ensuring the client
When assessing transgender clients, it is important has support from family and significant others, specific
that psychologists do not confuse body dysphoria goals, realistic expectations regarding the procedure
secondary to gender dysphoria, with BDD.53, 111 If an including an appreciation of what the procedure
evaluation of a transgender client’s suitability for a involves, the associated risks and limitations, the
cosmetic procedure has been requested, as with any expected recovery time, and requirements for self-care
other client, a comprehensive mental health and risk to aid recovery, improves the likelihood of positive
assessment should be conducted.113 outcomes.134
psychology.org.au 17References
1. Medical Board of Australia. (2016). Guidelines for registered 14. Angelakis, I., Gooding, P. A., & Panagioti, M. (2016). Suicidality
medical practitioners who perform cosmetic medical and in body dysmorphic disorder (BDD): A systematic review
surgical procedures. Retrieved 06 March 2018, from http:// with meta-analysis. Clinical Psychology Review, 49, 55-66.
www.medicalboard.gov.au/News/2016-05-09-media- doi:10.1016/j.cpr.2016.08.002
statement.aspx
15. Krebs, G., Fernández de la Cruz, L., & Mataix-Cols, D. (2017).
2. Bramwell, R., Morland, C., & Garden, A. S. (2007). Expectations Recent advances in understanding and managing body
and experience of labial reduction: A qualitative study. BJOG, dysmorphic disorder. Evidence Based Mental Health, 20(3), 71-
114(12), 1493-1499. doi:10.1111/j.1471-0528.2007.01509.x 75. doi:10.1136/eb-2017-102702
3. Australasian Foundation for Plastic Surgery. (N.D.). Media 16. Phillips, K. A., & Menard, W. (2006). Suicidality in body
FAQs: What are the most popular cosmetic surgery procedures dysmorphic disorder: A prospective study. American
undertaken in Australia and New Zealand? Retrieved 30 Oct Journal of Psychiatry, 163(7), 1280-1282. doi:10.1176/
2017, from http://www.plasticsurgeryfoundation.org.au/ ajp.2006.163.7.1280
media/media-faqs/
17. Constantian, M. B., & Lin, C. P. (2014). Why some patients are
4. Cosmetic Physicians College of Australasia. (2016). unhappy: Part 2. Relationship of nasal shape and trauma
Increasing number of Australians considering non- history to surgical success. Plastic and Reconstructive Surgery,
surgical cosmetic treatments. Retrieved 30 October 2017, 134(4), 836-851. doi:10.1097/PRS.0000000000000552
from http://cosmeticphysicians.org.au/pdf/media%20
release/09-09-2016_One_third_of_Australians_consider_ 18. Paraskeva, N., Clarke, A., & Rumsey, N. (2014). The routine
non-surgical_cosmetic_treatments_.pdf psychological screening of cosmetic surgery patients.
Aesthetics, 1(12), 28-32
5. Brunton, G., Paraskeva, N., Caird, J., Bird, K. S., Kavanagh,
J., Kwan, I., . . . Thomas, J. (2014). Psychosocial predictors, 19. Constantian, M. B. (2012). What motivates secondary
assessment, and outcomes of cosmetic procedures: A rhinoplasty? A study of 150 consecutive patients. Plastic
systematic rapid evidence assessment. Aesthetic Plastic and Reconstructive Surgery, 130(3), 667-678. doi:10.1097/
Surgery, 38(5), 1030-1040. doi:10.1007/s00266-014-0369-4 PRS.0b013e31825dc301
6. Sarwer, D. B., Gibbons, L. M., Magee, L., Baker, J. L., Casas, L. 20. Sarwer, D. B., Wadden, T. A., & Whitaker, L. A. (2002). An
A., Glat, P. M., . . . Young, V. L. (2005). A prospective, multi-site investigation of changes in body image following cosmetic
investigation of patient satisfaction and psychosocial status surgery. Plastic and Reconstructive Surgery, 109(1), 363-369.
following cosmetic surgery. Aesthetic Surgery Journal, 25(3), doi:10.1097/00006534-200201000-00060
263-269. doi:10.1016/j.asj.2005.03.009 21. von Soest, T., Kvalem, I. L., Roald, H. E., & Skolleborg, K. C. (2009).
7. Honigman, R. J., Phillips, K. A., & Castle, D. J. (2004). A review The effects of cosmetic surgery on body image, self-esteem,
of psychosocial outcomes for patients seeking cosmetic and psychological problems. Journal of Plastic, Reconstructive
surgery. Plastic and Reconstructive Surgery, 113(4), 1229-1237. & Aesthetic Surgery, 62(10), 1238-1244. doi:10.1016/j.
doi:10.1097/01.PRS.0000110214.88868.CA bjps.2007.12.093
8. Crerand, C. E., Franklin, M. E., & Sarwer, D. B. (2008). MOC- 22. Ericksen, W. L., & Billick, S. B. (2012). Psychiatric issues in
PS(SM) CME Article: Patient safety: Body dysmorphic disorder cosmetic plastic surgery. Psychiatric Quarterly, 83(3), 343-352.
and cosmetic surgery. Plastic and Reconstructive Surgery, doi:10.1007/s11126-012-9204-8
122(Supplement), 1-15. doi:10.1097/PRS.0b013e3181888ffd 23. Crerand, C. E., Magee, L., & Sarwer, D. B. (2012). Cosmetic
9. Sarwer, D. B., & Constantian, M. B. (2018). Psychological aspects procedures. In N. Rumsey & D. Harcourt (Eds.), Oxford
of cosmetic surgical and minimally invasive treatments. In G. handbook of the psychology of appearance (pp. 330-349).
C. Gurtner & P. C. Neligan (Eds.), Plastic surgery (4th ed., Vol. 1: Oxford, UK: Oxford University Press.
Principles, pp. 24-34.e24). London, UK: Elsevier. 24. Kisely, S., Morkell, D., Allbrook, B., Briggs, P., & Jovanovic,
10. Lipworth, L., & McLaughlin, J. K. (2010). Excess suicide risk and J. (2002). Factors associated with dysmorphic concern
other external causes of death among women with cosmetic and psychiatric morbidity in plastic surgery outpatients.
breast implants: A neglected research priority. Curr Psychiatry Australian & New Zealand Journal of Psychiatry, 36(1), 121-126.
Rep, 12(3), 234-238. doi:10.1007/s11920-010-0115-9 doi:10.1046/j.1440-1614.2002.00981.x
11. Veale, D. (2000). Outcome of cosmetic surgery and ‘DIY’ surgery 25. von Soest, T., Kvalem, I. L., & Wichstrøm, L. (2011). Predictors of
in patients with body dysmorphic disorder. Psychiatric Bulletin, cosmetic surgery and its effects on psychological factors and
24(6), 218-220. doi:10.1192/pb.24.6.218 mental health: A population-based follow-up study among
Norwegian females. Psychological Medicine, 42(03), 617-626.
12. Sarwer, D. B., Brown, G. K., & Evans, D. L. (2007). doi:10.1017/s0033291711001267
Cosmetic breast augmentation and suicide. American
Journal of Psychiatry, 164(7), 1006-1013. doi:10.1176/ 26. Sarwer, D. B., Zanville, H. A., LaRossa, D., Bartlett, S. P., Chang,
ajp.2007.164.7.1006 B., Low, D. W., & Whitaker, L. A. (2004). Mental health histories
and psychiatric medication usage among persons who sought
13. Herruer, J. M., Prins, J. B., van Heerbeek, N., Verhage-Damen, cosmetic surgery. Plastic and Reconstructive Surgery, 114(7),
G. W. J. A., & Ingels, K. J. A. O. (2015). Negative predictors for 1927-1933. doi:10.1097/01.prs.0000142999.86432.1f
satisfaction in patients seeking facial cosmetic surgery: A
systematic review. Plastic and Reconstructive Surgery, 135(6), 27. Sarwer, D. B., Ritter, S., D’Almeida, T., & Weinrieb, R. (2014).
1596-1605. doi:10.1097/prs.0000000000001264 Preoperative mental health evaluations. In C. M. Hunter, C. L.
18 Psychological evaluation of patients undergoing cosmetic proceduresYou can also read