Prostate-specific Membrane Antigen PET: Clinical Utility in Prostate Cancer, Normal Patterns, Pearls, and Pitfalls1
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
This copy is for personal use only. To order printed copies, contact reprints@rsna.org
200
NUCLEAR MEDICINE
Prostate-specific Membrane
Antigen PET: Clinical Utility in
Prostate Cancer, Normal Patterns,
Pearls, and Pitfalls1
Michael S. Hofman, MBBS, FRACP,
FAANMS Prostate-specific membrane antigen (PSMA) is a transmembrane
Rodney J. Hicks, MD, MBBS, FRACP glycoprotein that is overexpressed in prostate cancer. Radiolabeled
Tobias Maurer, MD small molecules that bind with high affinity to its active extracel-
Matthias Eiber, MD2 lular center have emerged as a potential new diagnostic standard
of reference for prostate cancer, resulting in images with extraordi-
Abbreviations: FDG = fluorodeoxyglucose, nary tumor-to-background contrast. Currently, gallium 68 (68Ga)–
PI-RADS = Prostate Imaging Reporting and PSMA-11 (or HBED-PSMA) is the most widely used radiotracer
Data System, PSA = prostate-specific antigen,
PSMA = prostate-specific membrane antigen, for PSMA positron emission tomography (PET)/computed tomog-
SUV = standardized uptake value raphy (CT) or PSMA PET/magnetic resonance (MR) imaging.
RadioGraphics 2018; 38:200–217 Evolving evidence demonstrates superior sensitivity and specificity
https://doi.org/10.1148/rg.2018170108
of PSMA PET compared to conventional imaging, with frequent
identification of subcentimeter prostate cancer lesions. PSMA PET
Content Codes:
is effective for imaging disease in the prostate, lymph nodes, soft
1
From the Department of Molecular Imaging, tissue, and bone in a “one-stop–shop” examination. There is emerg-
Centre for Cancer Imaging, Peter MacCallum
Cancer Centre, 305 Grattan St, Melbourne, VIC ing evidence for its clinical value in staging of high-risk primary
3000, Australia (M.S.H., R.J.H.); Sir Peter Mac- prostate cancer and localization of disease in biochemical recur-
Callum Department of Oncology, University
of Melbourne, Melbourne, Australia (M.S.H.,
rence. The high sensitivity provided by PSMA PET, with frequent
R.J.H.); and Departments of Urology and Nu- identification of small-volume disease, is redefining patterns of
clear Medicine, Technical University of Munich, disease spread compared with those seen at conventional imaging.
Klinikum Rechts der Isar, Munich, Germany
(T.M., M.E.). Recipient of a Cum Laude award In metastatic castration-resistant prostate cancer, PSMA PET is
for an education exhibit at the 2016 RSNA An- frequently used for theranostic selection (eg, lutetium 177–PSMA
nual Meeting. Received April 24, 2017; revi-
sion requested June 29 and received August
radionuclide therapy), but its potential use for therapy monitoring
2; accepted August 28. For this journal-based is still under debate. However, evidence on its proper use to im-
SA-CME activity, the authors, editor, and re- prove patient-related outcomes, particularly in the setting of early
viewers have disclosed no relevant relationships.
Address correspondence to M.S.H. (e-mail: biochemical recurrence and targeted treatment of oligometastatic
michael.hofman@petermac.org). disease, is still missing. Despite the term prostate specific, PSMA
M.S.H. supported by a Movember Clinical Tri- functions as a folate hydrolase and is expressed in a range of normal
als Award from the Prostate Cancer Foundation
of Australia research program and a Clinical
tissues and in other benign and malignant processes. Knowledge of
Fellowship Award from the Peter MacCallum its physiologic distribution and other causes of uptake is essential to
Cancer Foundation. R.J.H. supported by a Na- minimize false-positive imaging findings.
tional Health and Medical Research Council
of Australia Practitioner Fellowship. M.E. sup- ©
RSNA, 2018 • radiographics.rsna.org
ported by SFB 824 (DFG Sonderforschungs-
bereich 824, Project B11) from the Deutsche
Forschungsgemeinschaft.
Current address: Department of Molecular and
2
Medical Pharmacology, David Geffen School of
Medicine, University of California Los Angeles, SA-CME LEARNING OBJECTIVES
Los Angeles, Calif.
After completing this journal-based SA-CME activity, participants will be able to:
©
RSNA, 2018 ■■Describe the characteristics and mechanism of action of the PSMA PET/CT radio-
tracer.
■■Recognize
the normal biodistribution of radiolabeled small molecules targeting
PSMA on PET images.
■■Identify potential causes of false-positive findings at PSMA PET/CT.
See www.rsna.org/education/search/RG.
RG • Volume 38 Number 1 Hofman et al 201
many published their first in-human case series
TEACHING POINTS of gallium 68 (68Ga)-PSMA-11, which dem-
■■ Physiologic high-intensity activity is seen in the lacrimal, pa- onstrated high tumor-to-background contrast
rotid, and submandibular glands.
(8–10). 68Ga-PSMA-11 is variously referred to
■■ Low PSMA uptake is also seen in the parasympathetic ganglia,
as 68Ga-PSMA-HBED-CC, 68Ga-HBED-PSMA,
most commonly the celiac and stellate ganglia, but can oc-
cur at other sites, including the presacral ganglia. Knowledge and 68Ga-DKFZ-PSMA-11 in the literature and
of the locations of ganglia together with the uptake pattern is currently the most-used agent for PSMA posi-
(linear rather than focal), intensity (low grade rather than tron emission tomography (PET).
high grade), and anatomic appearance (“adrenal gland” or 68
Ga-PSMA-11 is synthesized by labeling
comma-shaped appearance) facilitates identification of this
the precursor PSMA-11 by using the chelator
normal variant.
N,N-bis(2-hydroxybenzyl)ethylenediamine-N,N-
■■ The superior accuracy of PSMA PET over conventional imag-
ing for staging in high-risk patients may allow identification of
diacetic acid (HBED) with 68Ga. This can be per-
patients with otherwise occult distant metastatic disease and formed by using manual, semiautomated, or fully
could facilitate individualized multimodal treatment concepts, automated techniques. 68Ga is a positron emitter
especially in the setting of oligometastatic disease. with a short half-life of 68 minutes. It is eluted
■■ There is now a large volume of literature demonstrating the from a germanium 68 (68Ge)/68Ga generator, a
very high sensitivity of PSMA PET/CT in the setting of bio- small device with a shelf life of 6–12 months.
chemical recurrence, even in patients with low PSA levels 68
Ga-PSMA-11 is not currently approved
when conventional imaging has very low sensitivity.
for clinical use by the FDA, which limits its use
■■ Most of the nonprostate cancer–related uptake at PSMA PET
has low intensity or is nonfocal, in contrast to the focal and
outside of clinical trials. Regulatory rules in some
usually intense uptake in prostate cancer lesions. jurisdictions, such as parts of Europe and Austra-
lia, allow radiotracers that are compounded ex-
temporaneously on-site in hospital environments
to be used in the clinic.
Introduction Other radiotracers for PSMA PET include
Prostate-specific membrane antigen (PSMA) is 68
Ga-PSMA-I&T (11), 68Ga-THP-PSMA (12),
expressed on the cell surface in normal prostate fluorine 18 (18F)–DCFPyL (13,14), and 18F-
tissue and is overexpressed in prostate cancer by PSMA-1007 (15). These have a similar biodis-
several orders of magnitude. It is a type II trans- tribution but can differ in their binding affini-
membrane glycoprotein encoded by the folate ties and nonspecific uptake, which limits direct
hydrolase 1 (FOLH1) gene, also referred to as comparisons when assessing interval change.
the glutamate carboxypeptidase II (GCPII) gene.
PSMA expression appears to be progressively Imaging Procedure, Radiation
increased in higher-grade tumors, under andro- Dosimetry, and Biodistribution
gen deprivation, and in hormone-refractory and A weight-adjusted radiotracer dose of 1.8–2.2
metastatic disease (1–3). PSMA was recognized MBq/kg of body weight is recommended, subject
as a target in prostate cancer approximately 3 to variation that may be required owing to variable
decades ago, when the first antibodies to its in- elution during the lifetime of the 68Ge/68Ga genera-
tracellular domain were developed (4). An early tor. Imaging is performed approximately 45–75
approach was to radiolabel the antibody cap- minutes after radiotracer administration. The pa-
romab with indium 111 (111In). Although this tient should be well hydrated and should void im-
agent was approved by the U.S. Food and Drug mediately before commencement of the scan. PET
Administration (FDA), its utility was limited by images should be acquired from the pelvis toward
low uptake of the antibody and its binding to the head to minimize misregistration between the
the intracellular rather than extracellular domain CT or magnetic resonance (MR) imaging and
of PSMA, as well as the limited specificity of PET components of the study due to filling of the
single photon emission computed tomography bladder during acquisition. CT and MR imaging
(SPECT) for detection in the era before hybrid acquisition protocols vary considerably among
SPECT/computed tomography (CT) (5,6). institutions. The 68Ga-PSMA-11 is administered
In recent times, the landscape of available ra- in a microgram dose, and no pharmacologic or
diotracers for the imaging of prostate cancer has adverse effects have been reported. Joint Euro-
changed rapidly (7). Of these agents, small mol- pean Association of Nuclear Medicine (EANM)
ecules that bind to the extracellular active center and Society of Nuclear Medicine and Molecular
of PSMA appear to be the most likely to repre- Imaging (SNMMI) procedure guidelines for 68Ga-
sent a new standard of reference. Compared with PSMA-11 PET/CT have recently been published
antibodies, these have the advantages of higher (16). High reporter agreement for 68Ga-PSMA-11
binding affinity, internalization, and rapid plasma PET/CT has been demonstrated (17,18). The
clearance. In 2013, the Heidelberg group in Ger- use of 68Ga-PSMA-11 results in relatively low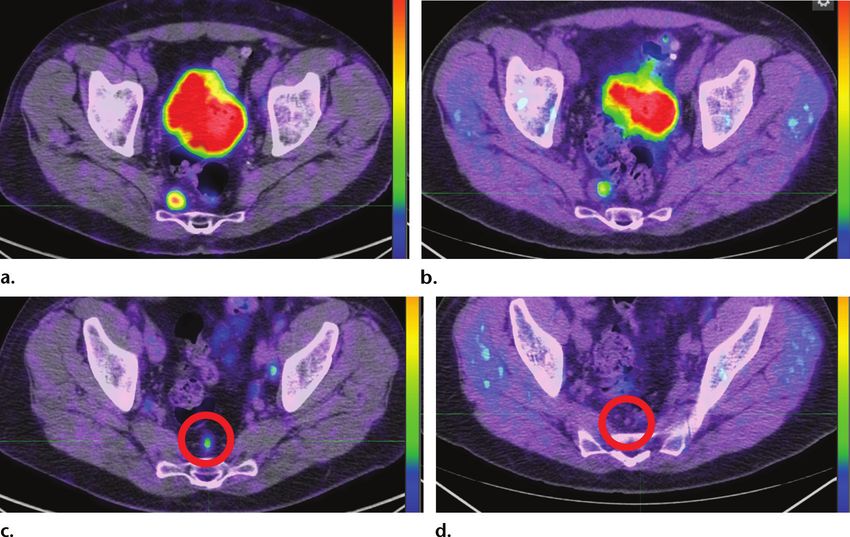
202 January-February 2018 radiographics.rsna.org
radiation exposure owing to the short half-life
of 68Ga. Injection of radiotracer producing 150
MBq results in a median effective dose of only 2.4
mSv (19). Additional radiation exposure related
to the CT scan in a hybrid PET/CT examination
depends on the protocol.
The normal physiologic biodistribution of
68
Ga-PSMA-11 at PET parallels the expression
of PSMA in normal tissues and the excretory
route of the radiotracer (20) (Fig 1). The highest-
intensity uptake is seen in the kidneys, ureters,
and bladder as the compound is renally excreted.
Very high urinary activity in the kidneys and
bladder can result in a surrounding halo artifact
on some PET/CT and PET/MR images (21),
and different reconstruction methods may need
to be applied to overcome this. Halo artifacts
as well as high activity from urinary excretion
can impede assessment of abdominal and pelvic
nodes near the ureter within or near the prostate
or prostatic bed. Several techniques, including
administration of furosemide, delay in imag-
ing, and use of intravenous contrast material in
the delayed urography phase, can be helpful in
differentiating physiologic urinary activity from
pathologic uptake.
Physiologic high-intensity activity is seen in
the lacrimal, parotid, and submandibular glands
Figure 1. Anterior maximum intensity projec-
(22). The precise mechanism of uptake remains
tion PET image shows the normal physiologic
uncertain but probably reflects a combination of distribution of 68Ga-PSMA-11. SUV = standard-
nonspecific excretion and PSMA expression in ized uptake value; +, ++, +++ = moderate-, high-,
these tissues. As with radioiodine, 68Ga-PSMA-11 and very high–intensity uptake, respectively.
is excreted in saliva, which may result in oropha-
ryngeal, laryngeal, or esophageal uptake. High-
intensity uptake may also be seen in the small lymph node involvement makes them a potential
bowel, primarily in the duodenum, where PSMA source of false-positive findings. These ganglia
expression may facilitate absorption of dietary were generally not perceivable at anatomic imag-
folates. Moderate-intensity uptake is seen in the ing before the availability of 68Ga-PSMA-11
liver and spleen. In a cohort of 106 studies, the PET, but with experience they are now readily
median SUV, in decreasing order, was 50 for kid- identifiable. The frequency of ganglia visualiza-
neys, 17 for submandibular glands, 16 for parotid tion depends on the type of PET/CT camera and
glands, 14 for duodenum, 9 for spleen, 7 for liver, reconstruction method used. The new generation
and 1.8 for blood pool. However, unlike the nar- of devices can resolve smaller lesions, especially
row range of physiologic hepatic or other organ devices with time-of-flight and point-spread func-
uptake seen at 18F-fluorodeoxyglucose (FDG) tions, which increase contrast for small struc-
PET/CT, a wide physiologic range was seen at tures. In one series, celiac ganglion uptake was
68
Ga-PSMA-11 PET in these organs (23). visualized in 60% of patients (26).
Low PSMA uptake is also seen in the para-
sympathetic ganglia, most commonly the celiac Clinical Indications in Prostate Cancer
(24) and stellate ganglia (25), but can occur The potential indications for use of 68Ga-PSMA-
at other sites, including the presacral ganglia. 11 PET/CT are summarized in the Table.
Knowledge of the locations of ganglia together
with the uptake pattern (linear rather than focal), Primary Staging of Prostate Cancer
intensity (low grade rather than high grade), Current international guidelines recommend
and anatomic appearance (“adrenal gland” or the use of CT, bone scintigraphy, or MR imag-
comma-shaped appearance) facilitates identifi- ing for high-risk patients only (28). There are
cation of this normal variant (Fig 2). The close many approaches to risk assessment. The most
proximity of these ganglia to sites of potential common D’Amico classification defines high risk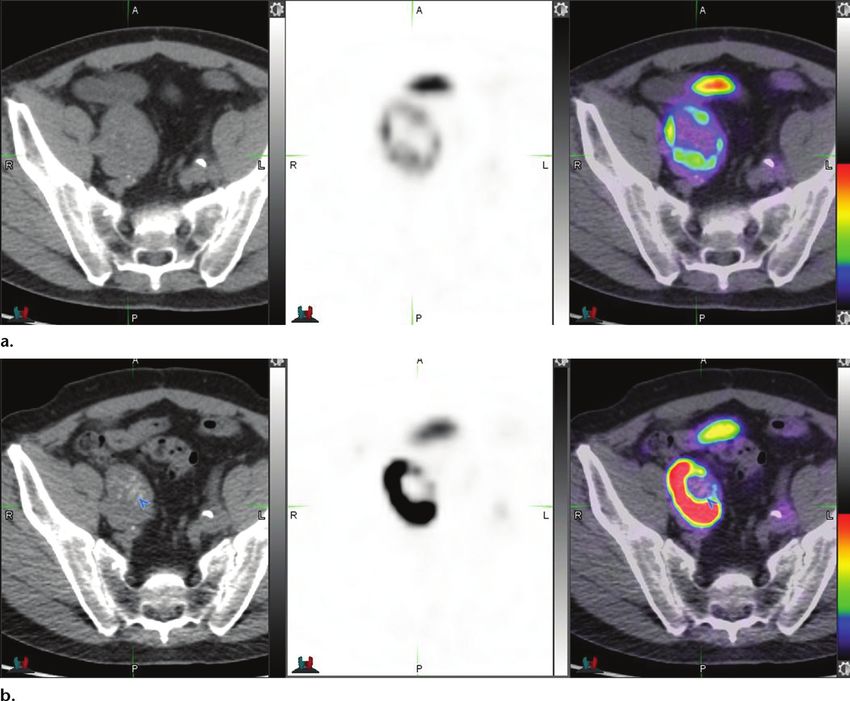
RG • Volume 38 Number 1 Hofman et al 203 Figure 2. Normal 68Ga-PSMA-11 uptake in ganglia. Axial PSMA PET images with a narrow window to increase the intensity of uptake show low uptake (arrows) in the celiac ganglia (a), presacral ganglion (c), and stellate ganglion (e). Axial CT images (b, d, f) show that the corresponding structures (arrows) are subcentimeter, with a linear comma-shaped appearance like that of an adrenal gland limb. as a PSA level greater than 20, a Gleason score 3) into two separate risk entities. Grades group 3 greater than 8, or a clinical stage of T2c or T3a. and above are considered to be high risk. The su- The Gleason score defines five histologic pat- perior accuracy of PSMA PET over conventional terns correlating with the degree of differentia- imaging for staging in high-risk patients may tion, from most (score of 1) to least (score of 5) allow identification of patients with otherwise oc- differentiated. The score assigns a primary grade cult distant metastatic disease (Fig 3) and could to the dominant pattern and a secondary grade facilitate individualized multimodal treatment to the next most frequent pattern. Recently, a concepts, especially in the setting of oligometa- new five-tier Gleason grade grouping with supe- static disease. In some cases, PSMA PET find- rior prognostic stratification has been adopted ings may be used to downstage patients who (29,30). This separates Gleason score 3+4 (grade were inaccurately classified as having metastatic group 2) and Gleason score 4+3 (grade group disease at conventional imaging (Fig 4).
204 January-February 2018 radiographics.rsna.org
Potential Indications for Use of PSMA PET/CT
Benefit Indication
High estimated benefit or diagnos- Primary staging in high-risk disease according to the D’Amico classification;
tic gain biochemical recurrence with low PSA value (0.2–10 ng/mL)
Low estimated benefit or diagnos- Primary staging in low- and intermediate-risk disease according to the
tic gain D’Amico classification
Potential application with promis- Biopsy targeting after previous negative biopsy but high suspicion for pros-
ing preliminary data tate cancer (especially in combination with multiparametric MR imaging
using PET/MR imaging)
Potential application with current Monitoring of systemic treatment in metastatic castration-resistant or meta-
lack of published data static castration-sensitive prostate cancer
Active surveillance (especially in combination with multiparametric MR
imaging using PET/MR imaging)
Treatment monitoring in patients with metastatic castration-resistant pros-
tate cancer undergoing radioligand therapy targeting PSMA (eg, 177Lu-
PSMA-ligand)
Note.—Adapted and reprinted under a CC BY 4.0 license from reference 27. 177Lu = lutetium 177, PSA =
prostate-specific antigen.
Several studies have compared 68Ga-PSMA-11 imaging as a first-line study in patients with high-
PET to conventional imaging or histopathologic risk prostate cancer before curative-intent surgery
analysis after pelvic nodal dissection. The results or radiation therapy (36).
of available retrospective studies vary owing The greater accuracy provided by 68Ga-
to different risk profiles of the studied patient PSMA-11 PET is redefining the patterns of spread
populations. The largest series to date analyzed of prostate cancer. Lymph nodes within the true
130 patients with intermediate or high-risk pros- pelvis are considered regional nodes, defined as N0
tate cancer and compared 68Ga-PSMA-11 PET or N1 according to the American Joint Committee
with cross-sectional imaging, with pelvic lymph on Cancer (AJCC) staging manual (37). Com-
node dissection results used as the standard of monly involved nodes include internal and external
reference (31). In this series, PET had superior iliac and obturator nodes. In addition, mesorectal
sensitivity (66% vs 44%) and specificity (99% (38) and presacral nodes are frequently visualized
vs 85%) compared to cross-sectional imaging. at 68Ga-PSMA-11 PET. The lateralization of nodal
The lymph nodes missed at 68Ga-PSMA-11 involvement usually parallels the dominant side of
PET were primarily less than 5 mm in size. Two prostate primary disease. Locating the subcentime-
smaller studies of 68Ga-PSMA-11 PET demon- ter nodes identified at 68Ga-PSMA-11 PET during
strated sensitivities of 33% (32) and 91% (33), lymph node dissection can be challenging for the
respectively. A small prospective study of 68Ga- surgical oncologist. Use of 111In or technetium
PSMA-11 PET demonstrated a sensitivity of 99m–radiolabeled PSMA with an intraoperative
64% and a specificity of 94% (34). False-negative gamma probe to locate lesions has shown potential
findings occurred in lymph nodes with a mean to facilitate precise surgical localization (39–41).
size of 2.7 mm. Because these studies included Nodes outside the true pelvis are classified as
patients with intermediate-risk disease, the nonregional nodes and are designated as M1a.
incidence of distant metastatic disease was low, Inferiorly, this includes inguinal nodes, and su-
which diminished the opportunity to compare periorly, this include common iliac nodes, para-
68
Ga-PSMA-11 PET with other modalities for aortic, aortocaval, and retrocrural nodes. In some
detection of distant metastatic disease. Evolv- patients, we have observed drainage to para-aortic
ing experience and literature suggest that 68Ga- nodes in the region of the left renal vein without
PSMA-11 PET has greater sensitivity and speci- pelvic nodal involvement, a drainage pathway
ficity than bone scintigraphy (35). However, in following the gonadal vessels anterior to the psoas
the absence of high-quality data, it is difficult to muscle ending in para-aortic and paracaval nodes
quantify the incremental accuracy compared with at the renal hilum (42). Above the diaphragm,
that of conventional imaging. The ProPSMA trial there is a high occurrence of supraclavicular nodal
is a multicenter randomized controlled study that involvement visualized at PSMA PET/CT. This
has commenced in Australia to establish whether can occur even in the absence of upper abdominal
PSMA PET/CT should replace conventional nodal involvement and parallels the known lym-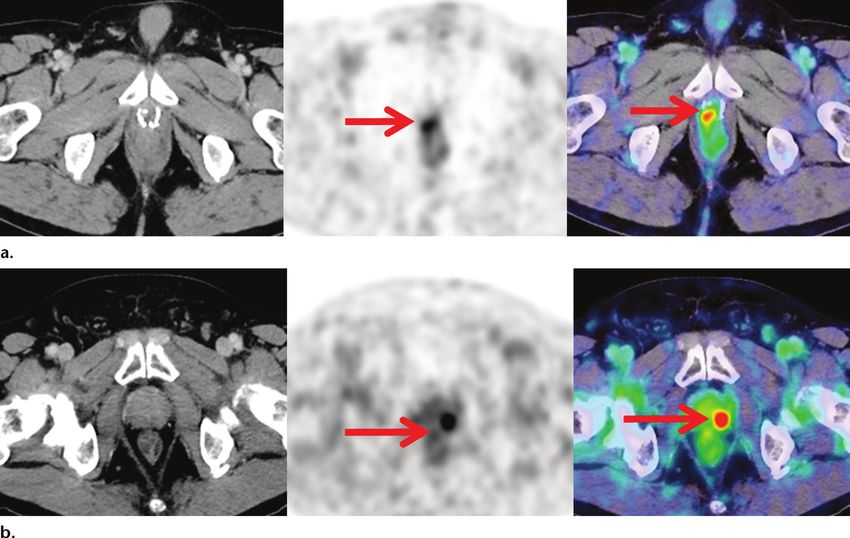
RG • Volume 38 Number 1 Hofman et al 205
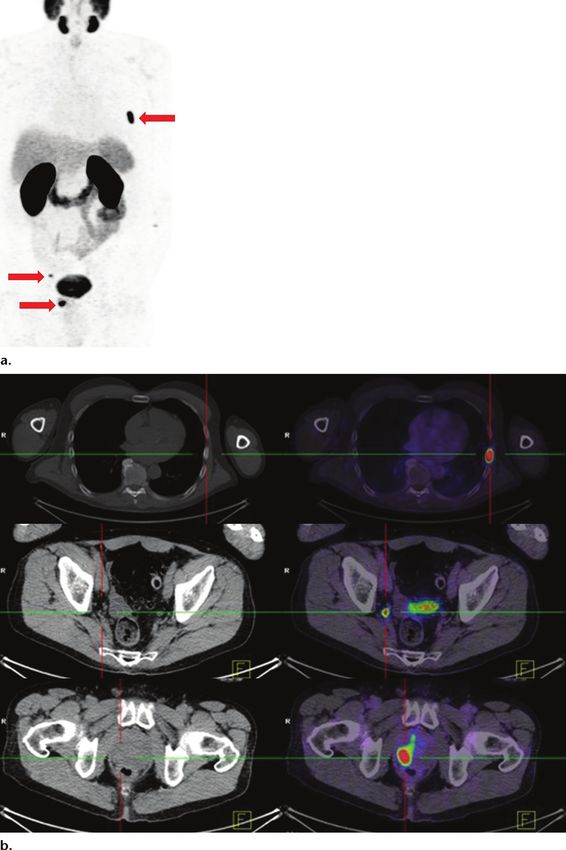
Figure 3. Newly diagnosed Gleason 4+5 prostate adenocarcinoma in
a 70-year-old man. Conventional CT and MR imaging of the pelvis and
bone scintigraphy (not shown) showed no evidence of metastatic dis-
ease. (a) Coronal maximum intensity projection 68Ga-PSMA-11 PET im-
age shows high tumor-to-background contrast (arrows) at the sites of pri-
mary disease and metastases. (b) Axial CT (left) and 68Ga-PSMA-11 PET/
CT (right) images show a metastasis to the rib (top), a subcentimeter right
obturator lymph node (middle), and primary prostate disease (bottom).
The treatment was changed from radical prostatectomy to hormonal
therapy. Follow-up 68Ga-PSMA-11 PET/CT images obtained 12 months
later (not shown) showed resolution of all findings, commensurate with
an undetectable PSA level. Although the findings at baseline bone scin-
tigraphy were negative, bone scintigraphy performed at 12 months (not
shown) showed an osteoblastic abnormality in the rib, highlighting the
limitations in differentiating a healing response from progressive disease
at bone scintigraphy.
phatic drainage pathway to the distal left thoracic but low-intensity uptake are more frequently
duct region (the Virchow node). seen. Aggressive poorly differentiated disease may
The most common type of extranodal spread even result in lytic osseous changes.
is osseous, designated as M1b. In therapy-naive 68
Ga-PSMA-11 PET is also very sensitive for
patients, 68Ga-PSMA-11 PET–positive osseous detection of visceral metastatic disease designated
lesions often show no corresponding anatomic as M1c, including metastases to the lung, liver,
abnormality at CT. In patients with more indo- pleura, adrenal gland, and brain (Fig 5). While
lent well-differentiated disease, sclerotic changes some of these organs are not commonly observed
206 January-February 2018 radiographics.rsna.org
Figure 4. Newly diagnosed
Gleason 4+5 prostate adenocarci-
noma. (a) Axial pelvic MR image
shows a focal lesion in the right
ilium. (b–d) Planar bone scan (b)
and axial SPECT/CT images (c, d)
show a corresponding sclerotic le-
sion (circle in b and c) with moder-
ate increased osteoblastic activity.
The combined MR imaging and
SPECT/CT findings were consis-
tent with metastatic disease. (e,
f) Axial 68Ga-PSMA-11 PET/CT im-
ages show intense uptake in the
prostate primary tumor (e) but no
uptake in the presumed metastatic
lesion (circle in f). On the basis of
the 68Ga-PSMA-11 PET/CT find-
ings, the patient underwent radical
prostatectomy. The postoperative
PSA level was undetectable, which
confirmed the absence of meta-
static disease.
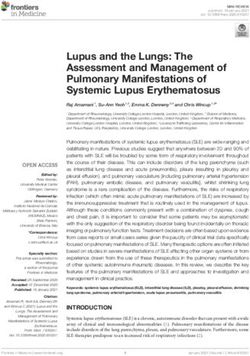
at anatomic imaging, the visualization of these combined 68Ga-PSMA-11 PET/MR imaging for
findings at PSMA PET/CT is consistent with direct comparison in 53 intermediate or high-
autopsy studies of metastatic patterns of pros- risk patients, the sensitivity of multiparametric
tate cancer (43). Notably, pulmonary metastases MR imaging when using PI-RADS criteria was
are subject to respiratory movement, which can 43%, compared with 64% for 68Ga-PSMA-11
significantly decrease the apparent intensity of PET (45). Simultaneous PET/MR imaging,
uptake, especially for small lesions. Thus, close which combined functional and multiparametric
review of the anatomic images is required. MR imaging data, further improved sensitivity
to 76%. Further research is required on how to
Localization of Intraprostatic Tumor best integrate PET and MR imaging findings for
An increasing number of studies have investi- directed biopsy or active surveillance.
gated the potential of 68Ga-PSMA-11 for intra-
prostatic tumor localization. One study showed Biochemical Recurrence
significantly higher 68Ga-PSMA-11 uptake in seg- Despite curative-intent surgery or radiation
ments with malignancy than in negative segments therapy, there is a significant risk for disease
(maximum SUV [SUVmax] of 11.8 vs 4.9) and relapse, which is usually detected by a rising PSA
suggest an SUVmax of 6.5 as an optimal discrimi- level. After radical prostatectomy, this is currently
nator, with sensitivity of 67% and specificity of defined as a PSA level of more than 0.2 ng/mL
92% for detection of tumor-involved segments that rises on at least two consecutive measures at
(44). In addition, preliminary results indicate that least 3 weeks apart. After external beam radiation
PSMA PET might be complementary to stand- therapy, a rise of 2.0 ng/mL or more above the
alone multiparametric MR imaging for intra- nadir PSA that occurs more than 6 weeks after
prostatic tumor localization (Fig 6). Exploiting therapy completion is required. However, at these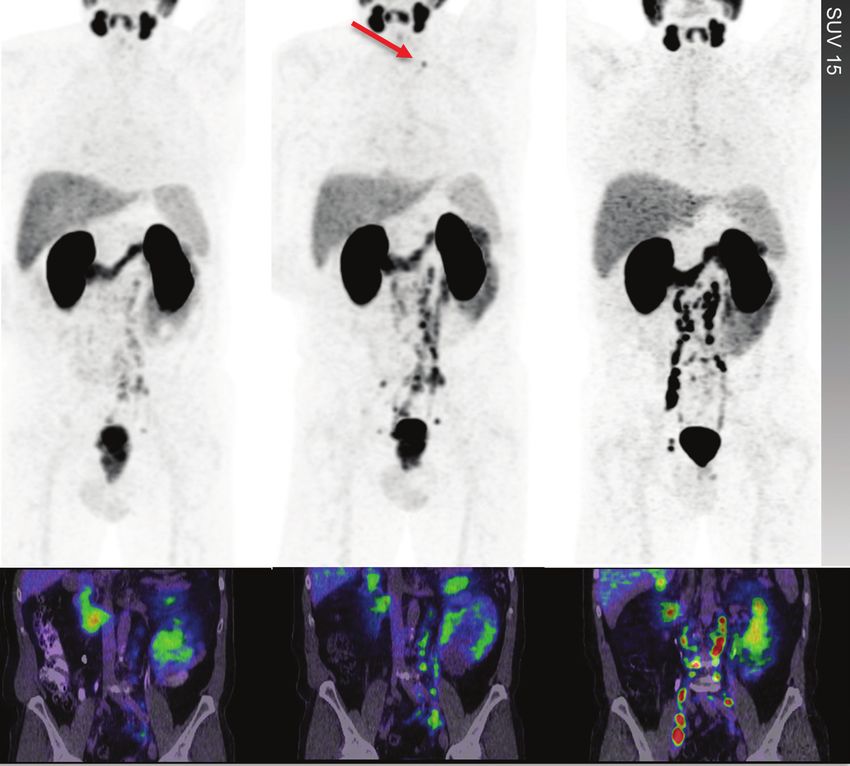
RG • Volume 38 Number 1 Hofman et al 207 Figure 5. Subcentimeter visceral metastases in four different patients seen on 68Ga-PSMA-11 PET images (first image in each row), with correlative CT and/or MR images (subsequent images in each row). Images show penile metastasis (arrows) (a), hepatic metastasis (b), pulmonary metastasis (c), and brain metastases (d). low PSA levels, conventional imaging has a limited to the prostate bed, although this treatment fails in ability to depict recurrent disease and therefore is a significant proportion of patients. not recommended (46). Following radical pros- There is now a large volume of literature tatectomy, biochemical recurrence is generally demonstrating the very high sensitivity of PSMA empirically treated with salvage radiation therapy PET/CT in the setting of biochemical recurrence,
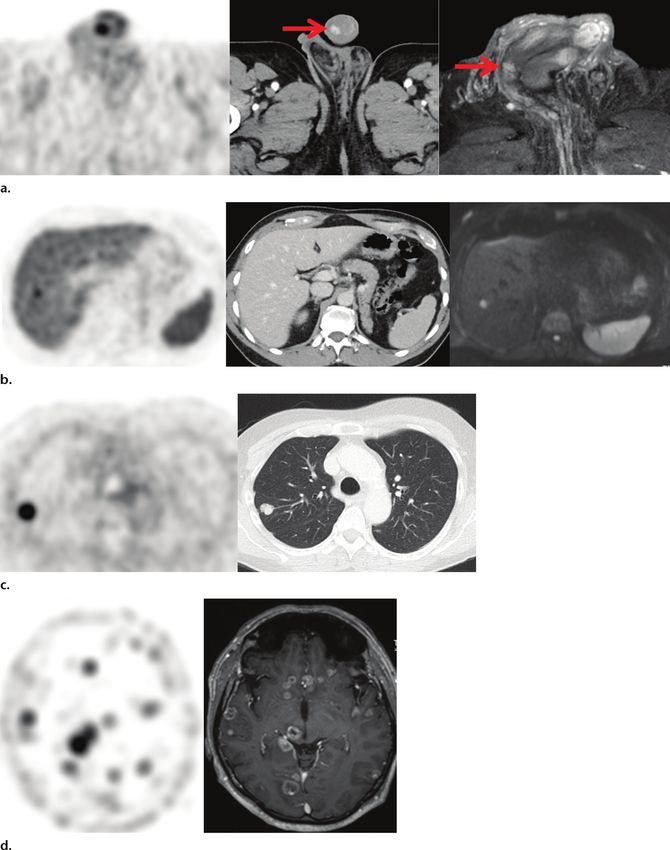
208 January-February 2018 radiographics.rsna.org Figure 6. 68Ga-PSMA-11 PET/MR imaging in a 63-year-old man with a continuously rising PSA level to 9.4 ng/mL but prior nega- tive prostate biopsies. (a–d) Multiparametric MR images indicated that the highest Prostate Imaging Reporting and Data System (PI-RADS) score was 3, attributed to a lesion in the left midgland. (e, f) 68Ga-PSMA-11 PET (e) and PET/CT (f) images show clearly increased tracer uptake in the corresponding region. A subsequent targeted biopsy revealed Gleason 4+3 prostate cancer. even in patients with low PSA levels in whom helps identifiy patients with oligometastatic conventional imaging has very low sensitivity disease, which can be potentially targeted with (10,31,47–53) (Fig 7). A meta-analysis of these stereotactic radiation therapy or salvage surgery. studies (54) has demonstrated detection rates However, there currently is a lack of high-quality of 48% at a PSA level of 0.2 ng/mL, increasing data to indicate improved patient outcomes with to 56% and 70% at levels of 0.5 and 1.0 ng/mL, use of PSMA PET in this setting (56). Of note, respectively. These rates are significantly superior the potential introduction of lead-time bias, with to those at choline PET/CT (Fig 8) or conven- the risk of early treatments causing more harm tional imaging. In an intraindividual comparison, than good, has been discussed, as the long-term 68 Ga-PSMA-11 PET/CT had a higher SUV effects on progression-free and overall survival compared with that at choline-11 or 18F-choline rates are still unclear (Fig 9) (56). PET/CT in 79% of lesions (53). In a prospective series, the detection rate with PSMA PET/CT Restaging of Metastatic Disease was 66%, versus 32% with 18F-choline PET/CT and Theranostic Selection (48). PSMA PET is capable of depicting small In patients with metastatic prostate carcinoma lymph node metastases, with one study reporting who are undergoing systemic therapy, conven- that 78% of PSMA-avid lymph nodes were less tional imaging, including bone scintigraphy, than 8 mm in size (50). CT, or MR imaging, combined with the PSA PSMA PET has been shown to have a high level and clinical presentation is currently used impact on management in patients with a PSA for response assessment. Bone scintigraphy level from 0.05 to less than 1.0 ng/mL after depicts the osteoblastic reaction to a metasta- radical prostatectomy who are candidates for sis as a surrogate marker, in contrast to PSMA salvage radiation therapy (55). Compared with PET, which depicts prostate cancer directly. blind radiation therapy to the prostate bed, 68Ga- In the restaging setting, differentiating treat- PSMA-11 PET changed the management in 29% ment response from a healing (flare) response of patients in this prospective study, as lesions can be challenging. For soft-tissue disease, CT were located in either regional lymph nodes or is generally used with the Response Evaluation bones that would not have been included in a Criteria in Solid Tumors (RECIST) for formal conventional salvage radiation therapy field. response assessment. However, subcentimeter Use of PSMA PET in the setting of biochem- target lesions that are visualized with confidence ical recurrence and a low PSA level frequently at PSMA PET/CT are not measurable at CT

RG • Volume 38 Number 1 Hofman et al 209 Figure 7. Biochemical recurrence in two patients with rising PSA levels (
210 January-February 2018 radiographics.rsna.org
Figure 9. Rising PSA level (1.0 ng/mL) in
a patient after radical prostatectomy and
salvage radiation therapy. On the basis
of findings at conventional imaging, the
management options included observa-
tion or hormonal therapy. (a, b) Axial
PSMA PET/CT (a) and coronal PSMA PET
(b) images show a single 8-mm left com-
mon iliac nodal metastasis (dashed circle
in b). Additional treatment options after
identification of oligometastatic disease at
PSMA PET included surgery or radiation therapy. The patient underwent stereotactic radiation therapy
(inset in a shows the treatment plan). (c) Coronal PSMA PET image obtained for restaging 3 months
later shows widespread nodal and osseous metastatic disease.
(Fig 10). Nevertheless, well-established criteria formation, with a high rather than low SUV that
such as the Prostate Working Group Criteria is prognostic for overall survival (60).
(PWGC) (57) for interpretation of response at PSMA PET/CT has an evolving role in
bone scintigraphy and CT exist. Whole-body PSMA-targeting treatments in advanced disease
diffusion-weighted MR imaging is sensitive for (eg, 177Lu-PSMA radioligand therapy) to evalu-
detection of osseous metastases (58), but there ate target expression and therefore potentially
is very limited evidence for its use in response predict response before treatment initiation.
assessment. High uptake at PSMA PET/CT is a prerequi-
Because PSMA PET images tumors directly, site in selecting patients who may benefit from
early experience suggests that PSMA PET may PSMA-directed radionuclide therapy. Pres-
have significant advantages over conventional ently, remarkable treatment responses have been
imaging in treatment response assessment. The observed in patients with castration-resistant
ability to evaluate local response in the prostate metastatic disease who have failed conventional
and in soft-tissue and osseous metastases in a therapies, such as docetaxel chemotherapy or
single imaging study is a significant advantage, enzalutamide/abiraterone therapy(61).
but further research is needed to define response
criteria for PSMA PET/CT. Some caution is Pitfalls
also warranted, as we have observed an increase PSMA PET/CT is a highly sensitive and spe-
in the intensity of radiotracer uptake early after cific imaging tool, but imaging specialists must
commencing hormone-deprivation therapy, be aware of a variety of physiologic and other
which may result in a “flare” phenomenon seen pathologic processes that can express PSMA
on PSMA PET images (Fig 11). This observa- and result in interpretative error. PSMA protein
tion is supported by preclinical data demonstrat- expression was discovered in prostate tissue and
ing an increase in PSMA expression following prostate cancer and is therefore termed prostate
androgen-deprivation therapy (59). PSMA PET specific. Functionally, PSMA is a folate hydrolase
may also be useful to evaluate response to taxan- that is expressed in a variety of normal tissues,
based chemotherapy. A potential limitation in tissue neovasculature, and other tumor types,
patients with advanced disease is the observation both benign and malignant. Most of the non-
of absent or low PSMA expression at sites of prostate cancer–related uptake at PSMA PET
poorly differentiated disease (eg, neuroendocrine has low intensity or is nonfocal, in contrast to
differentiated prostate cancer). In these patients, the focal and usually intense uptake in prostate
FDG PET/CT may provide complementary in- cancer lesions. Failure to recognize physiologicRG • Volume 38 Number 1 Hofman et al 211
Figure 10. Biochemically recurrent Gleason 4+5 prostate carcinoma in a patient with a PSA level of 30
ng/mL but normal findings on CT images and bone scans. Coronal PSMA PET (top row) and PSMA PET/
CT (bottom row) images were obtained. Left: Images show small-volume (subcentimeter) pelvic and
abdominal lymph node metastases. Middle: After 1 month of watch-and-wait management, the patient’s
PSA level rose to 89 ng/mL, and the images show progressive small-volume disease with a new subcen-
timeter supraclavicular node (arrow). Initiation of androgen-deprivation therapy resulted in a decline in
the PSA level to 0.5 ng/mL, followed by development of castration resistance and a rise in the PSA level
to 15 ng/mL within 2 months. Right: Repeat images show response at some sites but an overall picture of
progressive disease. Note the higher PSMA uptake in the setting of castration-resistant disease.
uptake, such as in ganglia or urinary activity as no anatomic correlate can be found. In particu-
detailed earlier, is another potential cause of lar, low-grade uptake in a single rib or in several
false-positive findings. An increasing number of contiguous ribs should be interpreted with cau-
case series and reports describe PSMA uptake tion. If there is uncertainty, ongoing monitoring
in benign processes such as osteoblastic activ- of the PSA level with follow-up PSMA PET is
ity or in benign tumors with PSMA expression, suggested as the most appropriate strategy. This is
including hemangiomas, meningiomas, and preferable to performing further imaging inves-
benign thyroid nodules. tigations, which are in many instances unlikely
to characterize equivocal PSMA PET findings
Benign Conditions with PSMA Expression with greater confidence. Moderate uptake can be
Low-to-moderate PSMA expression is observed seen in hemangiomas, including those in cutane-
in osteoblastic activity, with consequent activity ous, vertebral, and hepatic sites. Both acute and
seen in osteoarthritis, degenerative changes (Fig chronic inflammation can also be associated with
12), fibrous dysplasia (62), and fractures. After PSMA uptake. As with FDG PET, the pattern
radiation therapy to the pelvis for prostate cancer, of uptake and correlative anatomic findings are
sacral insufficiency fractures may also be visual- important in differentiation of these entities (63).
ized (Fig 13). Diffuse low-to-moderate uptake is
seen in Paget disease (Fig 12), possibly also due PSMA-negative Prostate Cancer
to osteoblastic response. Close anatomic correla- A small proportion (212 January-February 2018 radiographics.rsna.org
Figure 11. Upregulation of PSMA expression at PET after initiation of androgen-deprivation therapy in a patient 5 years after radical
prostatectomy. (a) Axial PSMA PET/CT images show moderate uptake in a 6.6 × 4.8-cm enlarged right external iliac node (SUVmax =
19). The patient’s PSA level was 0.21 ng/mL. The patient started androgen-deprivation therapy. (b) Repeat axial PSMA PET/CT im-
ages obtained 8 weeks later show a substantial reduction in the size of the node (4.8 × 3.8 cm), with progressive calcification, but
markedly increased intensity (SUVmax = 100). The fivefold increase in SUVmax despite the 60% reduction in volume highlights the
changes in PSMA expression that may be observed after androgen-deprivation therapy.
significance of PSMA-negative prostate carcinoma neovasculature rather than to PSMA expression
is currently uncertain. If the primary tumor is not in the tumor cells themselves (64). High-inten-
PSMA avid, the sensitivity for detecting nodal or sity uptake is seen in several malignant tumor
distant metastatic disease will be lower, and closer types (Fig 15), including renal cell carcinoma
attention must be given to anatomic review in this (65), salivary gland ductal carcinoma, pulmo-
setting. However, if the primary tumor is PSMA nary adenocarcinoma, glioblastoma multiforme,
avid, the metastasis will usually have a similar phe- and hepatocellular carcinoma (66). Lower-in-
notype. Therefore, in a patient with a PSMA-avid tensity uptake may be observed in a wide range
primary site, an enlarged PSMA-negative node is of tumors; experience continues to evolve, and
unlikely to represent prostate carcinoma (Fig 14). uptake has been observed in breast carcinoma
Exceptions are patients with advanced castration- (67), lymphoma, meningiomas (68), squamous
resistant metastatic disease, especially after several cell carcinoma, and well-differentiated thyroid
lines of chemotherapy have failed, where some cancer (69). Nevertheless, very-high-intensity
sites of disease have been observed to lose PSMA uptake is almost exclusively seen in prostate
expression. cancer, and the other tumor types can usually be
differentiated by different patterns of spread and
PSMA PET in Other Malignancies correlative anatomic appearances. In a review of
PSMA expression has been described in several 764 PSMA PET/CT studies in patients being
other tumor types, mainly related to the tumor evaluated for prostate cancer, identification ofRG • Volume 38 Number 1 Hofman et al 213
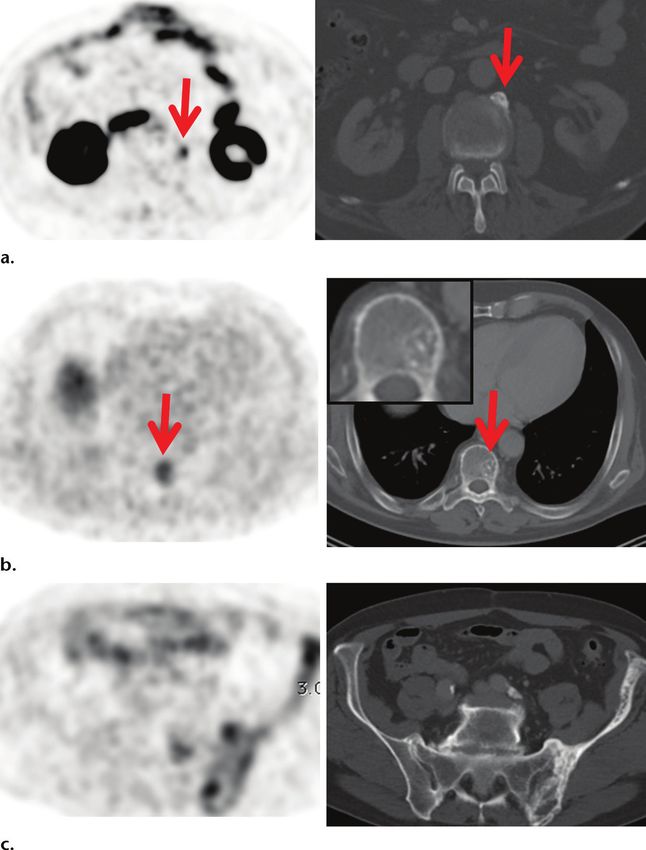
Figure 12. Radiotracer uptake at sites of osteoblastic activity, confirmed with follow-up PSA
testing and imaging, in three patients. (a) Axial PSMA PET (left) and CT (right) images show
uptake at the site of an anterior spondylophyte (arrows) at the L3–L4 level. (b) Axial PSMA
PET (left) and CT (right) images show uptake in a hemangioma (arrows), with a typical polka-
dotted appearance at CT (zoomed-in image, inset). (c) Axial PSMA PET (left) and CT (right)
images show heterogeneous increased uptake in a man with Paget disease. Comparison with
radiographs and CT and MR images obtained 5 years earlier in this patient (not shown) dem-
onstrated changes typical of Paget disease, with no interval change.
synchronous PSMA-avid malignancies were rare shop” examination. There is an emerging strong
(0.7%) (70). evidence base for staging of high-risk prostate
cancer and localization of disease in the setting
Conclusion of biochemical recurrence. However, evidence
PSMA PET/CT has rapidly emerged as a regarding proper use of PSMA PET/CT to im-
potential new reference standard for imaging prove patient-related outcomes, particularly in
of prostate cancer, with extraordinary tumor- the setting of early biochemical recurrence and
to-background contrast. Evolving evidence targeted treatment of oligometastatic disease,
demonstrates superior sensitivity and specific- is still missing. Despite the terminology prostate
ity of this method compared with conventional specific, PSMA that functions as folate hydro-
imaging, with frequent identification of sites lase is expressed in a range of normal tissues
of disease less than 10 mm in size. PSMA and in other benign and malignant processes.
PET/CT is effective for imaging disease in the Knowledge of the physiologic distribution and
prostate, soft tissue, and bone in a “one-stop– benign causes of uptake is essential to minimize214 January-February 2018 radiographics.rsna.org
Figure 13. Uptake at sites of fractures, confirmed with follow-up PSA testing and imaging. (a) Axial
PET/CT image (left) and CT image (right) in a patient with sacral pain and prior salvage radiation therapy
show symmetric low-to-moderate uptake in the sacrum. The findings were interpreted as an insufficiency
fracture. A follow-up CT image (not shown) demonstrated a fracture line with increased sclerosis and,
along with a finding of no elevation of the PSA level, helped confirm the diagnosis. (b) Axial PET/CT im-
age (left) in a patient with local recurrent disease after radiation therapy shows low-to-moderate uptake
in a rib. The findings were interpreted as a rib fracture, and a follow-up CT image (right, with magnified
view in inset) shows a clear correlate with callus formation.
Figure 14. Primary staging in a patient with a Gleason score of 4+3 and a PSA level of 20 ng/mL. Staging CT
(not shown) showed a 14-mm left common iliac node consistent with nonregional nodal metastatic disease
(M1a). (a, b) Axial PSMA PET/CT images show high uptake in the prostate primary tumor (a) but no uptake
(circle) in the suspected nodal metastasis (b). (c, d) Axial FDG PET/CT images show the opposite phenotype,
with no uptake in the prostate (c) but high uptake in the node (d). The differential phenotype suggests a second
pathologic condition. Results of nodal biopsy disclosed diffuse large B-cell lymphoma.RG • Volume 38 Number 1 Hofman et al 215
Figure 15. PSMA-avid nonprostate malignancies in three patients. (a) PSMA PET (top) and PSMA PET/CT (bot-
tom) images in a patient with prior salivary tumor excision (circle) and histologically proven androgen receptor–
positive salivary gland ductal carcinoma who subsequently presented with back pain show a thoracic vertebral
metastasis (arrow). (b) PSMA PET (top) and PSMA PET/CT (bottom) images in a patient with metastatic renal cell
carcinoma show highly PSMA-positive osseous metastatic disease. (c) PSMA PET/MR images in a patient with
recurrent glioblastoma multiforme show clear contrast enhancement and PSMA uptake in a left-sided lesion that
infiltrates the corpus callosum.
false-positive findings. PSMA PET is useful for and (111)In-capromab pendetide single photon emission
computerized tomography–computerized tomography for
imaging other PSMA-expressing tumors, with recurrent prostate carcinoma: results of a prospective clinical
the most experience currently for clear cell renal trial. J Urol 2014;191(5):1446–1453.
carcinoma. 7. Morigi JJ, Fanti S, Murphy D, Hofman MS. Rapidly chang-
ing landscape of PET/CT imaging in prostate cancer. Curr
Opin Urol 2016;26(5):493–500.
References 8. Schäfer M, Bauder-Wüst U, Leotta K, et al. A dimerized
1. Ghosh A, Heston WD. Tumor target prostate specific mem- urea-based inhibitor of the prostate-specific membrane
brane antigen (PSMA) and its regulation in prostate cancer. antigen for 68Ga-PET imaging of prostate cancer. EJNMMI
J Cell Biochem 2004;91(3):528–539. Res 2012;2(1):23.
2. Silver DA, Pellicer I, Fair WR, Heston WD, Cordon- 9. Eder M, Schäfer M, Bauder-Wüst U, et al. 68Ga-complex
Cardo C. Prostate-specific membrane antigen expression lipophilicity and the targeting property of a urea-based
in normal and malignant human tissues. Clin Cancer Res PSMA inhibitor for PET imaging. Bioconjug Chem
1997;3(1):81–85. 2012;23(4):688–697.
3. Wright GL Jr, Haley C, Beckett ML, Schellhammer PF. Expres- 10. Afshar-Oromieh A, Malcher A, Eder M, et al. PET imaging
sion of prostate-specific membrane antigen in normal, benign, with a [68Ga]gallium-labelled PSMA ligand for the diagno-
and malignant prostate tissues. Urol Oncol 1995;1(1):18–28. sis of prostate cancer: biodistribution in humans and first
4. Horoszewicz JS, Kawinski E, Murphy GP. Monoclonal evaluation of tumour lesions. Eur J Nucl Med Mol Imaging
antibodies to a new antigenic marker in epithelial prostatic 2013;40(4):486–495.
cells and serum of prostatic cancer patients. Anticancer Res 11. Weineisen M, Schottelius M, Simecek J, et al. 68Ga- and
1987;7(5B):927–935. 177
Lu-labeled PSMA I&T: optimization of a PSMA-targeted
5. Rieter WJ, Keane TE, Ahlman MA, Ellis CT, Spicer KM, theranostic concept and first proof-of-concept human studies.
Gordon LL. Diagnostic performance of In-111 capromab J Nucl Med 2015;56(8):1169–1176.
pendetide SPECT/CT in localized and metastatic prostate 12. Hofman MS, Eu P, Jackson P, et al. Cold kit PSMA PET
cancer. Clin Nucl Med 2011;36(10):872–878. imaging: phase I study of (68)Ga-THP-PSMA PET/CT
6. Schuster DM, Nieh PT, Jani AB, et al. Anti-3-[(18)F]FACBC in patients with prostate cancer. J Nucl Med doi:10.2967/
positron emission tomography–computerized tomography jnumed.117.199554. Published online October 6, 2017.216 January-February 2018 radiographics.rsna.org
13. Dietlein M, Kobe C, Kuhnert G, et al. Comparison of [(18) 33. Herlemann A, Wenter V, Kretschmer A, et al. (68)Ga-PSMA
F]DCFPyL and [ (68)Ga]Ga-PSMA-HBED-CC for PSMA- positron emission tomography/computed tomography pro-
PET imaging in patients with relapsed prostate cancer. Mol vides accurate staging of lymph node regions prior to lymph
Imaging Biol 2015;17(4):575–584. node dissection in patients with prostate cancer. Eur Urol
14. Szabo Z, Mena E, Rowe SP, et al. Initial evaluation of [(18) 2016;70(4):553–557.
F]DCFPyL for prostate-specific membrane antigen (PSMA)- 34. van Leeuwen PJ, Emmett L, Ho B, et al. Prospective
targeted PET imaging of prostate cancer. Mol Imaging Biol evaluation of 68gallium-prostate-specific membrane antigen
2015;17(4):565–574. positron emission tomography/computed tomography for
15. Giesel FL, Hadaschik B, Cardinale J, et al. F-18 labelled preoperative lymph node staging in prostate cancer. BJU Int
PSMA-1007: biodistribution, radiation dosimetry and his- 2017;119(2):209–215.
topathological validation of tumor lesions in prostate cancer 35. Pyka T, Okamoto S, Dahlbender M, et al. Comparison
patients. Eur J Nucl Med Mol Imaging 2017;44(4):678–688. of bone scintigraphy and (68)Ga-PSMA PET for skeletal
16. Fendler WP, Eiber M, Beheshti M, et al. (68)Ga-PSMA staging in prostate cancer. Eur J Nucl Med Mol Imaging
PET/CT: joint EANM and SNMMI procedure guideline 2016;43(12):2114–2121.
for prostate cancer imaging—version 1.0. Eur J Nucl Med 36. Australian and New Zealand Clinical Trials Registry [In-
Mol Imaging 2017;44(6):1014–1024. ternet]: Sydney (NSW): NHMRC Clinical Trials Centre
17. Fendler WP, Calais J, Allen-Auerbach M, et al. (68)Ga- UoSA. ACTRN12617000005358, A prospective study to
PSMA-11 PET/CT interobserver agreement for prostate assess the diagnostic accuracy and management impact of
cancer assessments: an international multicenter prospective prostate specific membrane antigen (PSMA) PET scanning
study. J Nucl Med doi: jnumed.117.190827. Published online in men with prostate cancer being considered for surgery or
April 13, 2017. radiation therapy. https://anzctr.org.au/Trial/Registration/
18. Fanti S, Minozzi S, Morigi JJ, et al. Development of stan- TrialReview.aspx?id=371669. Updated April 13, 2017.
dardized image interpretation for 68Ga-PSMA PET/CT to 37. Edge SB, Compton CC. The American Joint Committee on
detect prostate cancer recurrent lesions. Eur J Nucl Med Mol Cancer: the 7th edition of the AJCC cancer staging manual and
Imaging 2017;44(10):1622–1635. the future of TNM. Ann Surg Oncol 2010;17(6):1471–1474.
19. Pfob CH, Ziegler S, Graner FP, et al. Biodistribution and 38. Hijazi S, Meller B, Leitsmann C, et al. See the unseen: me-
radiation dosimetry of (68)Ga-PSMA HBED CC-a PSMA sorectal lymph node metastases in prostate cancer. Prostate
specific probe for PET imaging of prostate cancer. Eur J Nucl 2016;76(8):776–780.
Med Mol Imaging 2016;43(11):1962–1970. 39. Rauscher I, Düwel C, Wirtz M, et al. Value of (111)In
20. Hofman MS, Iravani A. Gallium-68 prostate-specific mem- prostate-specific membrane antigen (PSMA)–radioguided
brane antigen PET imaging. PET Clin 2017;12(2):219–234. surgery for salvage lymphadenectomy in recurrent prostate
21. Noto B, Büther F, Auf der Springe K, et al. Impact of PET cancer: correlation with histopathology and clinical follow-up.
acquisition durations on image quality and lesion detectability BJU Int 2017;120(1):40–47.
in whole-body (68)Ga-PSMA PET-MRI. EJNMMI Res 40. Maurer T, Schwamborn K, Schottelius M, et al. PSMA
2017;7(1):12. theranostics using PET and subsequent radioguided sur-
22. Kocur D, Przybyłko N, Hofman M, et al. Progressive regres- gery in recurrent prostate cancer. Clin Genitourin Cancer
sion of intracranial arteriovenous malformations after Onyx 2016;14(5):e549–e552.
embolization. Neurol Neurochir Pol 2017;51(3):270–275. 41. Robu S, Schottelius M, Eiber M, et al. Preclinical evalua-
23. Prasad V, Steffen IG, Diederichs G, Makowski MR, Wust P, tion and first patient application of 99mTc-PSMA-I&S for
Brenner W. Biodistribution of [(68)Ga]PSMA-HBED-CC SPECT imaging and radioguided surgery in prostate cancer.
in patients with prostate cancer: characterization of uptake J Nucl Med 2017;58(2):235–242.
in normal organs and tumour lesions. Mol Imaging Biol 42. Paño B, Sebastià C, Buñesch L, et al. Pathways of lymphatic
2016;18(3):428–436. spread in male urogenital pelvic malignancies. RadioGraphics
24. Krohn T, Verburg FA, Pufe T, et al. [(68)Ga]PSMA-HBED 2011;31(1):135–160.
uptake mimicking lymph node metastasis in coeliac ganglia: 43. Bubendorf L, Schöpfer A, Wagner U, et al. Metastatic pat-
an important pitfall in clinical practice. Eur J Nucl Med Mol terns of prostate cancer: an autopsy study of 1589 patients.
Imaging 2015;42(2):210–214. Hum Pathol 2000;31(5):578–583.
25. Beheshti M, Rezaee A, Langsteger W. 68Ga-PSMA-HBED 44. Fendler WP, Schmidt DF, Wenter V, et al. 68Ga-PSMA
uptake on cervicothoracic (stellate) ganglia, a common pitfall PET/CT detects the location and extent of primary prostate
on PET/CT. Clin Nucl Med 2017;42(3):195–196. cancer. J Nucl Med 2016;57(11):1720–1725.
26. Demirci E, Sahin OE, Ocak M, Akovali B, Nematyazar J, 45. Eiber M, Weirich G, Holzapfel K, et al. Simultaneous (68)
Kabasakal L. Normal distribution pattern and physiological Ga-PSMA HBED-CC PET/MRI improves the localization
variants of 68Ga-PSMA-11 PET/CT imaging. Nucl Med of primary prostate cancer. Eur Urol 2016;70(5):829–836.
Commun 2016;37(11):1169–1179. 46. Mottet N, Bellmunt J, Bolla M, et al. EAU guidelines
27. Rauscher I, Maurer T, Fendler WP, Sommer WH, Schwaiger on prostate cancer. II. Treatment of advanced, relaps-
M, Eiber M. (68)Ga-PSMA ligand PET/CT in patients with ing, and castration-resistant prostate cancer. Eur Urol
prostate cancer: how we review and report. Cancer Imaging 2011;59(4):572–583.
2016;16(1):14. 47. Afshar-Oromieh A, Avtzi E, Giesel FL, et al. The diagnostic
28. Wollin DA, Makarov DV. Guideline of guidelines: imaging value of PET/CT imaging with the (68)Ga-labelled PSMA
of localized prostate cancer. BJU Int 2015;116(4):526–530. ligand HBED-CC in the diagnosis of recurrent prostate
29. Epstein JI, Egevad L, Amin MB, et al. The 2014 International cancer. Eur J Nucl Med Mol Imaging 2015;42(2):197–209.
Society of Urological Pathology (ISUP) consensus confer- 48. Afshar-Oromieh A, Haberkorn U, Schlemmer HP, et al.
ence on Gleason grading of prostatic carcinoma: definition Comparison of PET/CT and PET/MRI hybrid systems using
of grading patterns and proposal for a new grading system. a 68Ga-labelled PSMA ligand for the diagnosis of recurrent
Am J Surg Pathol 2016;40(2):244–252. prostate cancer: initial experience. Eur J Nucl Med Mol
30. Berney DM, Beltran L, Fisher G, et al. Validation of a contem- Imaging 2014;41(5):887–897.
porary prostate cancer grading system using prostate cancer 49. Morigi JJ, Stricker PD, van Leeuwen PJ, et al. Prospective
death as outcome. Br J Cancer 2016;114(10):1078–1083. comparison of 18F-fluoromethylcholine versus 68Ga-PSMA
31. Maurer T, Gschwend JE, Rauscher I, et al. Diagnostic ef- PET/CT in prostate cancer patients who have rising PSA
ficacy of (68)gallium-PSMA positron emission tomography after curative treatment and are being considered for targeted
compared to conventional imaging for lymph node staging therapy. J Nucl Med 2015;56(8):1185–1190.
of 130 consecutive patients with intermediate to high risk 50. Giesel FL, Fiedler H, Stefanova M, et al. PSMA PET/CT
prostate cancer. J Urol 2016;195(5):1436–1443. with Glu-urea-Lys-(Ahx)-[⁶⁸Ga(HBED-CC)] versus 3D CT
32. Budäus L, Leyh-Bannurah SR, Salomon G, et al. Initial volumetric lymph node assessment in recurrent prostate can-
experience of (68)Ga-PSMA PET/CT imaging in high-risk cer. Eur J Nucl Med Mol Imaging 2015;42(12):1794–1800.
prostate cancer patients prior to radical prostatectomy. Eur 51. Ceci F, Uprimny C, Nilica B, et al. (68)Ga-PSMA PET/CT
Urol 2016;69(3):393–396. for restaging recurrent prostate cancer: which factors are as-RG • Volume 38 Number 1 Hofman et al 217
sociated with PET/CT detection rate? Eur J Nucl Med Mol in castrate-resistant metastatic prostate cancer. J Nucl Med
Imaging 2015;42(8):1284–1294. 2013;54(8):1195–1201.
52. Eiber M, Maurer T, Souvatzoglou M, et al. Evaluation of 61. Rahbar K, Ahmadzadehfar H, Kratochwil C, et al. German
hybrid ⁶⁸Ga-PSMA ligand PET/CT in 248 patients with multicenter study investigating 177Lu-PSMA-617 radioli-
biochemical recurrence after radical prostatectomy. J Nucl gand therapy in advanced prostate cancer patients. J Nucl
Med 2015;56(5):668–674. Med 2017;58(1):85–90.
53. Afshar-Oromieh A, Zechmann CM, Malcher A, et al. 62. De Coster L, Sciot R, Everaerts W, et al. Fibrous dysplasia
Comparison of PET imaging with a (68)Ga-labelled PSMA mimicking bone metastasis on (68)GA-PSMA PET/MRI.
ligand and (18)F-choline-based PET/CT for the diagnosis Eur J Nucl Med Mol Imaging 2017;44(9):1607–1608.
of recurrent prostate cancer. Eur J Nucl Med Mol Imaging 63. Hofman MS, Hicks RJ. How we read oncologic FDG PET/
2014;41(1):11–20. CT. Cancer Imaging 2016;16(1):35.
54. Perera M, Papa N, Christidis D, et al. Sensitivity, specificity, 64. Chang SS, O’Keefe DS, Bacich DJ, Reuter VE, Heston
and predictors of positive (68)Ga-prostate-specific membrane WD, Gaudin PB. Prostate-specific membrane antigen is
antigen positron emission tomography in advanced prostate produced in tumor-associated neovasculature. Clin Cancer
cancer: a systematic review and meta-analysis. Eur Urol Res 1999;5(10):2674–2681.
2016;70(6):926–937. 65. Siva S, Callahan J, Pryor D, Martin J, Lawrentschuk N,
55. van Leeuwen PJ, Stricker P, Hruby G, et al. (68) Ga-PSMA Hofman MS. Utility of (68) Ga prostate specific membrane
has a high detection rate of prostate cancer recurrence outside antigen–positron emission tomography in diagnosis and re-
the prostatic fossa in patients being considered for salvage sponse assessment of recurrent renal cell carcinoma. J Med
radiation treatment. BJU Int 2016;117(5):732–739. Imaging Radiat Oncol 2017;61(3):372–378.
56. Murphy DG, Sweeney CJ, Tombal B. “Gotta catch ‘em al,” 66. Sasikumar A, Joy A, Nanabala R, Pillai MR, Thomas B,
or do we? Pokemet approach to metastatic prostate cancer. Vikraman KR. (68)Ga-PSMA PET/CT imaging in primary
Eur Urol 2017;72(1):1–3. hepatocellular carcinoma. Eur J Nucl Med Mol Imaging
57. Scher HI, Morris MJ, Stadler WM, et al. Trial design and 2016;43(4):795–796.
objectives for castration-resistant prostate cancer: updated 67. Sathekge M, Lengana T, Modiselle M, et al. (68)Ga-PSMA-
recommendations from the Prostate Cancer Clinical Trials HBED-CC PET imaging in breast carcinoma patients. Eur
Working Group 3. J Clin Oncol 2016;34(12):1402–1418. J Nucl Med Mol Imaging 2017;44(4):689–694.
58. Lecouvet FE, El Mouedden J, Collette L, et al. Can whole- 68. Sasikumar A, Joy A, Pillai MR, et al. Diagnostic value of 68Ga
body magnetic resonance imaging with diffusion-weighted PSMA-11 PET/CT imaging of brain tumors: preliminary
imaging replace Tc 99m bone scanning and computed to- analysis. Clin Nucl Med 2017;42(1):e41–e48.
mography for single-step detection of metastases in patients 69. Lütje S, Gomez B, Cohnen J, et al. Imaging of prostate-specific
with high-risk prostate cancer? Eur Urol 2012;62(1):68–75. membrane antigen expression in metastatic differentiated
59. Afshar-Oromieh A, Malcher A, Eder M, et al. Reply to Reske thyroid cancer using 68Ga-HBED-CC-PSMA PET/CT. Clin
et al: PET imaging with a [68Ga]gallium-labelled PSMA Nucl Med 2017;42(1):20–25.
ligand for the diagnosis of prostate cancer: biodistribution 70. Osman MM, Iravani A, Hofman MS, Hicks RJ. Detection
in humans and first evaluation of tumour lesions. Eur J Nucl of synchronous primary malignancies with (68)Ga-PSMA
Med Mol Imaging 2013;40(6):971–972. PET/CT in patients with prostate cancer: frequency in 764
60. Jadvar H, Desai B, Ji L, et al. Baseline 18F-FDG PET/ patients. J Nucl Med doi: 10.2967/jnumed.117.190215.
CT parameters as imaging biomarkers of overall survival Published online June 1, 2017.
TM
This journal-based SA-CME activity has been approved for AMA PRA Category 1 Credit . See www.rsna.org/education/search/RG.You can also read