Product Catalogue 2018 - Veterinary Diagnostics - EUROIMMUN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Veterinary Diagnostics
Product Catalogue
2018
2

Table of contents
About us................................................................................................................................................4
EUROIMMUN AG............................................................................................................................6
The company.............................................................................................................................6
Global business.........................................................................................................................8
Research and development..........................................................................................................10
Scientific publications / patents...............................................................................................10
Detection methods.............................................................................................................................12
Indirect immunofluorescence......................................................................................................14
EUROIMMUN IFT: unrivalled quality and diversity..............................................................14
Microtiter ELISA............................................................................................................................16
EUROIMMUN ELISA: semi‑quantitative and precise...........................................................16
EUROIMMUN avidity ELISA: detection of acute infections.................................................18
Line blots.......................................................................................................................................20
EUROLINE: multiparameter line blots for comprehensive antibody profiles �������������������20
Veterinary diagnostics.......................................................................................................................22
Infection diagnostics.....................................................................................................................24
Anaplasma...............................................................................................................................24
Borrelia.....................................................................................................................................26 NEW
Brucella.....................................................................................................................................28
Ehrlichia....................................................................................................................................30 NEW
Leishmania...............................................................................................................................32
MERS coronavirus...................................................................................................................34
Toxoplasma..............................................................................................................................36 NEW
West Nile virus........................................................................................................................38
Tick-Borne Profile....................................................................................................................40
Health monitoring.........................................................................................................................42
Mouse monitoring...................................................................................................................42
Autoantibody diagnostics.............................................................................................................44
Autoantibodies against cell nuclei.........................................................................................44
Products for veterinary diagnostics (overview)..............................................................................46
Additional reagents and material for veterinary diagnostics........................................................52
Further parameters for veterinary diagnostics...............................................................................54 NEW
Automation.........................................................................................................................................56
Indirect immunofluorescence......................................................................................................58
MERGITE!.................................................................................................................................58
Sprinter.....................................................................................................................................60
EUROStar III Plus.....................................................................................................................62
Microtiter ELISA............................................................................................................................64
EUROIMMUN Analyzer...........................................................................................................64
EUROLabWorkstation ELISA..................................................................................................66
Immunoblots.................................................................................................................................68
EUROBlotMaster......................................................................................................................68
EUROLineScan.........................................................................................................................70
EUROBlotOne...........................................................................................................................72
Liquid handling.............................................................................................................................74
EUROLabLiquidHandler..........................................................................................................74
Laboratory management..............................................................................................................76
EUROLabOffice........................................................................................................................76
Index....................................................................................................................................................78
Visit us online at
www.vet.euroimmun.com
3
About
us
About us
4
5
About
us
EUROIMMUN AG
About
us
The company · Global business
For more information on this subject scan
the QR code or enter the Quick Link code
q109 at www.euroimmun.com
The company
EUROIMMUN is one of the leading manufacturers of medical laboratory diagnostics worldwide and stands for
innovation. Over 2500 employees in 15 countries develop, produce and sell test systems for the diagnosis of
diseases, and software and automation solutions for the performance and evaluation of these assays. Laborato‑
ries in over 150 countries use EUROIMMUN products for the diagnosis of autoimmune and infectious diseases
and allergies, and to perform genetic analyses. The company was founded 1987 from the University of Luebeck
(Schleswig-Holstein, Germany). As of December 2017, the US American company PerkinElmer, Inc. holds the
majority of the EUROIMMUN shares. PerkinElmer is an international leader in the area of medical and biotechnol‑
ogy. The enterprise has its headquarters in Waltham, Massachusetts and has 11400 employees worldwide. With
innovative detection and imaging techniques and IT systems, it provides comprehensive expertise in diagnostics,
medical research and environmental and food analytics. PerkinElmer, Inc. is a component of the S&P 500 Index.
EUROIMMUN has extensive know-how in the fields of immunology, cell biology, histology, biochemistry and
molecular biology. The company is based on state-of-the-art, partly patented production processes and micro-
analysis techniques. The great expertise in the development and production of human diagnostic products has
led to the establishment of an own business division focusing on the development of veterinary diagnostic test
systems such as IIFT, ELISA and line blots.
Great expertise and ongoing training are essential for the use and distribution of EUROIMMUN products. Every
year, the EUROIMMUN Academy receives almost 1000 customers from over 50 countries, providing train‑
ing for customers, field staff, and employees from all EUROIMMUN subsidiaries. Moreover, there are train‑
ing laboratories in several countries. The accredited Institute for Quality Assurance, an institution of the com‑
pany, organises quality assessment schemes and thus helps to maintain the high quality standard of exter‑
nal laboratories. The Institute for Experimental Immunology, another EUROIMMUN institution, is dedicated
to basic research. The institute also cooperates with universities, clinics and renowned research institutions
from all over the world. These cooperations have resulted in a large number of diploma and doctoral theses.
EUROIMMUN is ISO certified (EN ISO 9001:2008, EN ISO 13485:2012, ISO 13485/CMDCAS).
A large share of the company’s success can be attributed to the associated reference laboratory, which offers a
fast and differentiated diagnosis to the EUROIMMUN customers and clarifies several hundreds of patient samples
with difficult constellations every day.
EUROIMMUN meets its needs for qualified personnel not only through its presence at recruitment and trade fairs
and advertisements, but also through its own training program. Alongside the vocational school, the apprentices
and trainees are offered a comprehensive practical and theoretical program and intensive mentoring in the work
routine. At present, the company employs 75 trainees and more than 2500 persons worldwide. Women represent
nearly 60 % of staff and thus the majority. 1080 employees have an academic background, 175 of them hold a
doctoral degree.
6
About
us
EUROIMMUN in figures
1987 founded in Luebeck, Germany 7 offices in Germany
284 M euros of annual Group turnover in 2017 14 subsidiaries in other countries
2575 employees worldwide 412 own/in-licensed IP rights
1080 university graduates in the ranking of the most innovative
small and medium-sized enterprises
175 employees with doctoral degree 3rd
in Germany
75 apprentices (WirtschaftsWoche, April 2014)
Groß Groenau
Selmsdorf
Luebeck
Germany Dassow
Rennersdorf
Pegnitz
Bernstadt
7
EUROIMMUN AG
About
us
The company · Global business
For more information on this subject scan
the QR code or enter the Quick Link code
q111 at www.euroimmun.com
Global business
EUROIMMUN subsidiary
EUROIMMUN office
Distributor
The main country to manufacture EUROIMMUN products is Germany. From there the products – reagents, auto‑
mated analysis systems and evaluation software – are delivered to over 150 countries worldwide. Other produc‑
tion sites are Hangzhou/China and Singapore. Both subsidiaries produce EUROIMMUN products for their own
markets.
All other subsidiaries are distribution companies, which also mostly have their own laboratories for training.
8
About
us
EUROIMMUN Polska Sp. z.o.o. EUROIMMUN Medical Diagnostics EUROIMMUN US Inc.
Barbara Łobos (China) Co., Ltd. Hamid Erfanian
ul. Widna 2a Prof. Dr. Wang Jing & Li Chuan 1 Bloomfield Avenue
50-543 Wrocław Room 1908-1910, Mountain Lakes,
POLAND Building No. 1, NJ 07046
Tel: +48 71 3730808 No. 8 Beichen Dong Road, USA
Fax: +48 71 3730011 Chaoyang District, Tel: +1 8009132022
E-mail: b.lobos@euroimmun.pl 100101 Beijing, P.R.C. Fax: +1 9736561098
CHINA E-mail: info@euroimmun.us
EUROIMMUN Italia s.r.l Tel: +86 10 58045000
Dr. Fabio Valenti Fax: +86 10 58045001 EUROIMMUN Schweiz AG
Corso Stati Uniti 4 – Scala F E-mail: jing.wang@oumeng.com.cn Hansruedi Steffen
35127 Padua Hirschmattstr. 1
ITALY EUROIMMUN Med. Diagnostics 6003 Lucerne
Tel: +39 049 7800178 Canada Inc. SWITZERLAND
Fax: +39 049 7808103 Dr. Donglai Ma Tel: +41 41 3609000
E-mail: euroimmun@euroimmun.it 2566 Meadowpine Blvd. Fax: +41 41 3609020
Mississauga, ON E-mail: mail@euroimmun.ch
EUROIMMUN Diagnostics España, L5N 6P9
S.L.U. CANADA EUROIMMUN Brasil Ltda.
Pedro Cayuela Tel: +1 905 542-8828 Gustavo Janaudis
Avda. Somosierra 22, Nave 17-A Fax: +1 905 542-8988 R. José Gonçalves Galeão, 198
28703 Madrid E-mail: d.ma@euroimmun.ca São Paulo, SP
SPAIN 03227-150
Tel: +34 916591369 EUROIMMUN (South East Asia) BRAZIL
Fax: +34 916518226 Pte. Ltd. Tel: +55 11 23050170
E-mail: info@euroimmun.es Li Chuan E-mail: contato@euroimmun.com.br
No.1 Changi Business Park
EUROIMMUN Portugal, LDA Avenue 1, #01-01/05 EUROIMMUN South Africa
Manuel Sá Singapore 486058 Pty Ltd.
Rua Sacadura Cabral, 9 A/B SINGAPORE Claudia Ohst
Quinta do Borel Tel: +65 68050399 39 Clifton Crescent
2720-507 Amadora Fax: +65 65425648 Parklands, 7441 – Cape Town
PORTUGAL euroimmun@euroimmun.com.sg SOUTH AFRICA
Tel: +351 21 4996550 Tel: +27 21 5577666
Fax: +351 21 4996559 Özmen Tıbbi Laboratuar Fax: +27 21 5577666
E-mail: geral@euroimmun.pt Teşhisleri A. Ş. E-mail: c.ohst@euroimmun.co.za
EUROIMMUN TÜRKIYE
EUROIMMUN UK Ltd. Kadriye Vogt & Peter Vogt EUROIMMUN France SAS
Dr. Daniel Agustus Sultan Selim Mahallesi Claude Audiberti
Ashville House Lalegül Sokak No: 10 NEF09 A Blok Espace Villa Parc – L’Erable
131-139 The Broadway Kat: 10 Daire 108 –118 1, Avenue Marne et Gondoire
Wimbledon 34415 Kağıthane Istanbul 77600 Bussy-Saint-Martin
SW19 1QJ London TURKEY FRANCE
UNITED KINGDOM Tel: +90 212 3258504 Tel: +33 1 64616666
Tel: +44-20 85407058 Fax: +90 212 3258506 Fax: +33 1 64616220
E-mail: info@euroimmun.co.uk E-mail: p.vogt@euroimmun.com.tr E-mail: euroimmun@euroimmun.fr
9
Research and development
About
us
Scientific publications / patents
For more information on this subject scan
the QR code or enter the Quick Link code
q113 at www.euroimmun.com
Scientific publications / patents
Publications
1. Poschmann A, Seitz C, Bein G, Böcker W, Geusendam G, Stöcker 8. Müller MA, Corman VM, Jores J, Meyer B, Younan M, Liljander 14. Müller MA, Devignot S, Lattwein E, Corman VM, Maganga GD,
W. Rapid histochemical screening of monoclonal antibodies against A, Bosch BJ, Lattwein E, Hilali M, Musa BE, Bornstein, S, Drosten Gloza-Rausch F, Binger T, Vallo P, Emmerich P, Cottontail VM,
tumor associated and other antigens using the “Titerplane-tech- C. MERS coronavirus neutralizing antibodies in camels, Eastern Tschapka M, Oppong S, Drexler JF, Weber F, Leroy EM, Drosten
nique“. Immunobiol 170: 72-73 (1985). Africa, 1983-1997. Emerg Infect Dis 20(12): 2093-2095 (2014). C. Evidence for widespread infection of African bats with Crimean-
Congo hemorrhagic fever-like viruses. Sci Rep (2016) 26637.
2. Schlumberger W, Meyer W, Proost S, Dähnrich C, Müller-Kunert 9. Meyer B, Müller MA, Corman VM, Reusken CB, Ritz D, Godecke
E, Sonnenberg K, Olbrich S and Stöcker W. The New EUROBLOT GJ, Lattwein E, Kallies S, Siemens A, van Beek J, Drexler JF, Muth 15. Steinhagen K, Probst C, Radzimski C, Schmidt-Chanasit J, Emmer‑
Technology: Differentiation of Autoantibodies Against Cell Nuclei. D, Bosch BJ, Wernery U, Koopmans MP, Wernery R, Drosten C. ich P, van Esbroeck M, Schinkel J, Grobusch MP, Goorhuis A, War‑
Eur J Clin Chem Clin Biochem 33: 116 (1995). Antibodies against MERS coronavirus in dromedaries, United Arab necke JM, Lattwein E, Komorowski L, Deerberg A, Saschenbrecker
Emirates, 2003 and 2013. Emerg Infect Dis 20(4): 552-559 (2014). S, Stocker W, Schlumberger W. Serodiagnosis of Zika virus (ZIKV)
3. Stöcker W, Teegen B, Meyer W, Müller-Kunert E, Proost S, Schlum‑ infections by a novel NS1-based ELISA devoid of cross-reactivity
berger W, Sonnenberg K. Differentiated autoantibody diagnostics 10. Gutiérrez C, Tejedor-Junco MT, González M, Lattwein E, Renneker with dengue virus antibodies: a multicohort study of assay perfor-
using BIOCHIP Mosaics. In: Conrad K (Hrsg). Autoantikörper. Pabst S. Presence of antibodies but no evidence for circulation of MERS- mance, 2015 to 2016. Euro Surveill (2016)
Science Publishers 78-99 (1998). CoV in dromedaries on the Canary Islands, 2015. Euro Surveill
20(37): (2015). 16. Florey J, Viall A, Streu S, DiMuro V, Riddle A, Kirk J, Perazzotti
4. W. Meyer, T. Scheper, W. Schlumberger, W. Stöcker. Antibodies L, Affeldt K, Wagner R, Vaden S, Harris T, Allenspach K. Use of a
Against the Newly Identified Major Antigen VlsE: A milestone in 11. Müller MA, Meyer B, Corman VM, Al-Masri M, Turkestani A, Ritz D, Granulocyte Immunofluorescence Assay Designed for Humans for
the Serological Diagnosis of Lyme borreliosis. Clin Chem Lab Med Sieberg A, Aldabbagh S, Bosch B-J, Lattwein E, Alhakeem RF, Assiri Detection of Antineutrophil Cytoplasmic Antibodies in Dogs with
41(10): A90 (2003). AM, Albarrak AM, Al-Shangiti AM, Al-Tawfiq JA. Wikramaratna P, Chronic Enteropathies. J Vet Intern Med (2017) 1062-1066.
Alrabeeah AA, Drosten C, Memish ZA. Presence of Middle East
5. Voigt J, Krause C, Rohwäder E, Saschenbrecker S, Hahn M, Danck‑ respiratory syndrome coronavirus antibodies in Saudi Arabia: a 17. Frey CF, Marreros N, Renneker S, Schmidt L, Sager H, Hentrich B,
wardt M, Feirer C, Ens K, Fechner K, Barth E, Martinetz T, Stöcker W. nationwide, cross-sectional, serological study. Lancet Infect Dis Milesi S, Gottstein B. Dogs as victims of their own worms: Serodiag-
Automated indirect immunofluorescence evaluation of antinuclear 15(5): 559-564 (2015). nosis of canine alveolar echinococcosis. Parasit Vectors (2017) 422.
autoantibodies on HEp-2 cells. Clin Dev Immunol, (2012).
12. Bremer HD, Lattwein E, Renneker S, Lilliehöök I, Rönnelid J, Hans‑ 18. Munyua P, Corman VM, Bitek A, Osoro E, Meyer B, Muller MA, Lat‑
6. Aburizaiza AS, Mattes FM, Azhar EI, Hassan AM, Memish ZA, Muth son-Hamlin H. Identification of specific antinuclear antibodies in twein E, Thumbi SM, Murithi R, Widdowson MA, Drosten C, Njenga
D, Meyer B, Lattwein E, Müller MA, Drosten C. Investigation of anti- dogs using a line immunoassay and enzyme-linked immunosorbent MK. No Serologic Evidence of Middle East Respiratory Syndrome
Middle East respiratory syndrome antibodies in blood donors and assay. Vet Immunol Immunopathol.(2015) Coronavirus Infection Among Camel Farmers Exposed to Highly
slaughterhouse workers in Jeddah and Makkah, Saudi Arabia, fall Seropositive Camel Herds: A Household Linked Study, Kenya, 2013.
2012. J Infect Dis 209(2): 243–246 (2014). 13. Rasche A, Saqib M, Liljander AM, Bornstein S, Zohaib A, Ren‑ Am J Trop Med Hyg (2017) 1318-1324.
neker S, Steinhagen K, Wernery R, Younan M, Gluecks I, Hilali M,
7. Corman VM, Jores J, Meyer B, Younan M, Liljander A, Said MY, Musa BE, Jores J, Wernery U, Drexer JF, Drosten C, Corman VM. 19. Saqib M, Sieberg A, Hussain MH, Mansoor MK, Zohaib A, Latt‑
Gluecks I, Lattwein E, Bosch BJ, Drexler JF, Bornstein S, Drosten Hepatitis E virus infection in dromedaries, North and East Africa, wein E, Muller MA, Drosten C, Corman VM. Serologic Evidence
C, Müller MA. Antibodies against MERS coronavirus in dromedary United Arab Emirates, and Pakistan, 1983-2015. Emerg Infect Dis for MERS-CoV Infection in Dromedary Camels, Punjab, Pakistan,
camels, Kenya, 1992-2013. Emerg Infect Dis 20(8): 1319-1322 (2014). 22(7):1249-1252 (2016). 2012-2015. Emerg Infect Dis (2017) 550-551.
Oral presentations and scientific posters
1. Horbach E, Schaper J, Slenczka W, Gassner I, Stöcker W. Serologi- 9. Krause C, Ens K, Voigt J, Fauer H, Fechner K, Barth E, Feirer C, Koc 16. Fechner, K. Computer-aided immunofluorescence microscopy
cal diagnosis of viral infections by automatically mounted biochips. Y, Martinetz T, Stöcker W. Fully automated process for indirect (CAIFM) for ANA diagnostics. 9th International Congress on Autoim‑
Poster and presentation at the 7th International Congress of Immu‑ immunofluorescence tests (IIFT) in the diagnostics of autoimmune munity, Nice, France (2014).
nology. Abstract in the congress transcript, Berlin, Germany (1989). diseases. 11th International Workshop on Autoantibodies and Auto‑
immunity (IWAA), Shanghai, China (2011). 17. Lattwein E, Renneker S, Steinhagen K, Müller HA, Memish ZA,
2. Stöcker W. BIOCHIP Technology and TITERPLANE Technique: Ways Drosten C. Of Camels and Men – investigations using the first
to the standardisation of autoantibody diagnostics. Presentation 10. Fechner K. 1. IIFT Automation – Incubation and evaluation as a fully commercial ELISA and IFT for the detection of antibodies against
at the 30 Tagung der Arbeitsgemeinschaft Klinische Immunologie automated walk-away solution. 2. Professional ANA diagnostics – MERS coronavirus. 33. Jahrestagung des Arbeitskreises für Vet‑
der Gesellschaft für Klinische und Experimentelle Immunologie, screening by IIFT, confirmation by ELISA or immunoblot. Workshop erinärmedizinische Infektionsdiagnostik (AVID), Kloster Banz,
(“Erstes Dresdner Autoantikörper-Symposium”). Abstract in the “Multiplex-Autoantikörperdiagnostik mit BIOCHIP-Mosaiken“, IGLD- Germany (2014).
congress transcript, Dresden, Germany (1990). Symposium, Hamburg, Germany (2011).
18. Lattwein E. Investigations using the first commercial ELISA and
3. Sonnenberg K. BIOCHIP Mosaics for the serological diagnosis of 11. Schlumberger W. Innovative technologies: Designer Antigens IFT for the detection of antibodies against MERS coronavirus of
zoonotic and vector-borne viral diseases. XXXII. Türk Mikrobiyoloji and Recombinant Cell-based Immunofluorescence Assays. 7th camels and men. 5th International conference of Egyptian society of
Kongresi, Antalya, Turkey (2006). National Molecular and Diagnostic Microbiology Congress, Ankara, virology, Hurghada, Egypt (2014).
Turkey (2012).
4. Fechner K. 1. Autoimmune Diseases: Solutions for automation in 19. Stöcker W. Latest achievements towards a complete automatiza-
the detection of corresponding autoantibodies. and 2. The use of 12. Ens K, Krause C, Saschenbrecker S, Rohwäder E, Fechner K, Stöcker tion of indirect immunofluorescence. 3rd National Autoimmune
BIOCHIP Mosaics in the determination of ANA and ANCA. XIII Con‑ W, Barth E, Martinetz T, Voigt J. Automated indirect immunofluores- Diagnostics Summit, Guangzhou, China (2014).
greso Venezolano de Bioanálisis, Venezuela (2008). cence evaluation of antinuclear autoantibodies on HEp-2 cells. 20th
IFCC-EFLM European Congress of Clinical Chemistry and Laboratory 20. Renneker S. Diagnostics of tick-borne diseases at EUROIMMUN
5. Komorowski L, Janssen A, Stöcker W, Probst C. Dimerisation of Medicine and 45th Congress of the Italian Society of Clinical Bio‑ AG, Germany. Workshop on Arthropod-Borne Diseases, Leipzig,
recombinant OspC leads to an antigen with enhanced potential for chemistry and Clinical Molecular Biology (SIBioC), Milan, Italy (2013). Germany (2015).
active vaccination. 12. International Conference on Lyme Borreliosis
and other Tick-Borne Diseases, Ljubljana, Slovenia (2010). 13. Hansson-Hamlin H, Bremer H, Lilliehook I, Lattwein E, Rönnelid J. 21. Gerlach S, Hahn M, Lederer S, Lattwein E, Mielke J, Fraune J,
Antinuclear antibody specificity in dogs with immune-mediated Probst C, Gechner K, Stöcker W, Voigt J. Computer-aided immu-
6. Krause C, Ens K, Voigt J, Fauer H, Barth E, Feirer C, Koc Y, Martinetz rheumatic disease. 24th European Congress of Veterinary Internal nofluorescence microscopy of recombinant cell-based IIFT in neu-
T, Stöcker W. Fully automated process for indirect immunofluores- Medicine (ECVIM), Mainz, Germany (2014). rological diagnostics. 10th International Congress on Autoimmunity,
cence tests (IIFT) in the diagnostics of autoimmune diseases. 7. Leipzig, Germany (2016).
Jahrestagung der Deutschen Gesellschaft für Klinische Chemie und 14. Lattwein E, Lipkowski M, Rohwäder E, Fechner K. Efficient health
Laboratoriumsmedizin (DGKL), Mannheim, Germany (2010). monitoring in laboratory mice according to FELASA recomenada- 22. Renneker S. Tick-borne profile: multiplex lineblot assay for sero-
tions, by means of immunofluorescence mosaics. 33. Jahrestagung logical diagnosis of tick-borne diseases in dogs and horses and
7. Probst C, Janssen A, Meyer W, Scheper T, Schlumberger W, Stöcker des Arbeitskreises für Veterinärmedizinische Infektionsdiagnostik diagnosis of early West Nile virus infections in horses by avidity
W, Komorowski L. OspC (Δ1-18): A designer antigen with a higher (AVID), Kloster Banz, Germany (2014). determination of IgG antibodies. Workshop on Arthropod-Borne
diagnostic potential than conventional recombinant OspC. 12. Diseases, Jena, Germany (2016).
International Conference on Lyme Borreliosis and other Tick-Borne 15. Liljander A, Corman VM, Meyer B, Younan M, Said MY, Gluecks I,
Diseases, Ljubljana, Slovenia (2010). Lattwein E, Bosch BJ, Drexler JF, Bornstein S, Müller MA, Jores J, 23. Renneker S, Mackiewicz M, Lattwein E. IgG avidity as alternative
Drosten C. Presence of Middle East Respiratory Syndrome (MERS) indicator for discrimination between acute and past infections
8. Stöcker W. BIOCHIP Mosaics with designer antigen-expressing coronavirus antibodies in East African dromedary camels. Tro‑ with West Nile virus in horses and Toxoplasma gondii in cats. 18th
recombinant cells in serological diagnostics of autoimmune and pentag 2014 “Bridging the gap between increasing knowledge and International Symposium of the World Association of Veterinary
infectious diseases. Zelltechnik-Kongress, Lübeck, Germany (2011). decreasing resources“, Prague, Czech Republic (2014). Laboratory Diagnosticians, Sorrento, Italy (2017).
10About
us
Patents
1. Pfeiffer T, Wulf K, Probst C, Zerbe B, Müller-Kunert E, Stöcker W. Verfahren und Kit zum Nachweis von spezifischen Anti-
körpern mittels Immunfluoreszenz. German patent application DE 102 07 135.7 (filed 2002).
2. Meyer W, Scheper T, Stöcker W. Proprietor: EUROIMMUN Medizinische Labordiagnostika AG. Vorrichtung zur Antikörper-
diagnose mit kombinierten Membranen. German utility model DE 202 15 270.7 (filed 2003).
3. Stöcker W, Fauer H, Krause C, Barth E, Martinetz T. Verfahren zur Optimierung der automatischen Fluoreszenzmusterer-
kennung in der Immundiagnostik. German patent application DE 10 2006 027 516.0 (filed 2006) and International patent
application WO 2007/140952 (filed 2007).
4. Stöcker W, Wessel S, Morrin M, Müller M. Konstante Lichtquelle für die Fluoreszenzmikroskopie. German patent applica‑
tion DE 2006 027 518.7 (filed 2006).
5. Stöcker W, Voigt JF, Berg S, Fauer H, Roznowicz R. Network controlled method for ensuring the authenticity and quality
of visually collected diagnostic findings from indirect immunofluorescence tests. European patent application EP 1 921
552 516.0 (filed 2006) and International patent application WO 2008/058935 (filed 2007).
6. Stöcker W, Fauer H, Krause C, Barth E, Martinetz T. Method for optimizing automatic fluorescence pattern recognition in
immune diagnostics. European patent application EP 2 030 001 (filed 2007).
7. Komorowski L, Probst C, Janssen A, Stöcker W. Polypeptides and methods for the specific detection of antibodies in
patients with Borrelia infection. US patent application US 2010/0150964 (filed 2009).
8. Stöcker W, Fauer H, Krause C, Barth E, Martinetz T. Method for optimizing the automatic fluorescence pattern recognition
in immunodiagnosis. US patent application US 2010/0047811 (filed 2007).
9. Morrin M. Method and apparatus for automatic focusing of substrates in fluorescence microscopy. German patent appli‑
cation DE 10 2010 035 104.0 (filed 2010) and International patent application WO 2012/025220 (filed 2011).
10. Testkit für die Labordiagnostik. German utility model DE 20 2012 004 404 (filed 2012).
11. Stöcker W, Komorowski L, Probst C, Janssen A. Polypeptides and method for the specific detection of antibodies in pati-
ents with a Borrelia infection. US patent application US 2012 0177680 (filed 2012).
12. Stöcker W, Meyer W, Scheper T, Euken A. Test kit for laboratory diagnostics. European patent application EP 2 660 602
(filed 2013).
13. Meyer W, Scheper T, Kaffka R. Verfahren zur automatisierten Auswertung von inkubierten Blotstreifen. German patent
application DE 10 2013 008 468.7 (filed 2013) and International patient application WO 2014/173657 (filed 2014).
14. Rottmann N, Stöcker W. Transparent object holder with labelling. European patent application EP 2 896 458 (filed 2014)
and International patent application WO 2015/106774 (filed 2014).
15. Stöcker W, Wuttig D. Device and method for determining the volume of a liquid. European patent application EP 3 072 594
(filed 2015).
11Detection
methods
Detection methods
1213
Detection
methodsIndirect immunofluorescence
Detection
methods
EUROIMMUN IFT: unrivalled quality and diversity
For more information on this subject scan
the QR code or enter the Quick Link code
q115 at www.euroimmun.com
EUROIMMUN IFT:
unrivalled quality and diversity
Immunofluorescence tests from EUROIMMUN: high-tech, not old-fashioned! Numerous innovations contribute to
the standardisation and modernisation of indirect immunofluorescence:
Activation technique: Physically or chemically activated
cover glasses are coated with cultured cells or tissue sec‑ Tissue sections
tions. Frozen tissue sections are fixed to the glass surface by Antigen dots
covalent bonding. This increases the adhesion by more than
Cultured cells
100 fold, preventing detachment of the sections.
Transf.
cells
BIOCHIP Technology: Cover glasses coated with biologi‑
cal substrates are cut mechanically into millimetre-sized
fragments (BIOCHIPs). Ten or more first-class preparations
of consistent quality can be obtained per tissue section, for
cultured cell substrates even several thousands.
BIOCHIP Mosaics: When multiple BIOCHIPs coated with dif‑
ferent substrates are arranged in one reaction field, antibod‑
ies against various organs or infectious agents can be inves‑
tigated simultaneously. Comprehensive antibody profiles can
be easily established (multiplex) and the results are verified BIOCHIP Technology and Mosaics
reciprocally on different substrates.
TITERPLANE Technique: The samples or reagents are first pipetted onto the reaction fields of a reagent tray.
The slides are then placed into recesses of the reagent tray, where all BIOCHIPs come into contact with the liquids,
and the individual reactions begin simultaneously. As the fluids are confined in a closed space, there is no need
for a conventional humidity chamber.
Automation: EUROIMMUN offers a range of IFT automation options for both low and high throughput, from
sample dilution to fully automated evaluation of fluorescence images, including archiving.
14Detection
methods
Indirect immunofluorescence: one substrate (here: HEp-2 cells) – many antibodies to investigate
15Microtiter ELISA
Detection
methods
EUROIMMUN ELISA: semi-quantitative and precise · EUROIMMUN avidity ELISA: Detection of acute infections
For more information on this subject scan
the QR code or enter the Quick Link code
q116 at www.euroimmun.com
EUROIMMUN ELISA:
semi‑quantitative and precise
Optimised for fully automated processing
Simple handling:
Break-off microplate wells
Ready-to-use reagents (no mixing or diluting necessary)
Bar- and colour-coded reagents, largely exchangeable between different lots and between different parameters
Standardised incubation conditions
RF absorbent included in sample buffer (IgM tests) – no extra costs
Incubation protocols for all tests integrated in EUROIMMUN Analyzers:
no additional programming necessary
Comprehensive validation of test systems for EUROIMMUN Analyzers
in accordance with directive 98/79/EC and on the basis of EN ISO 13485:2003
Detailed validation documents available for all parameters
Years of experience in the development of ELISAs for diagnostic purposes
Over 800 parameters for human medical diagnostics
Application of this outstanding expertise to veterinary diagnostics
1617
Detection
methodsMicrotiter ELISA
Detection
methods
EUROIMMUN ELISA: semi-quantitative and precise · EUROIMMUN avidity ELISA: Detection of acute infections
For more information on this subject scan
the QR code or enter the Quick Link code
q116 at www.euroimmun.com
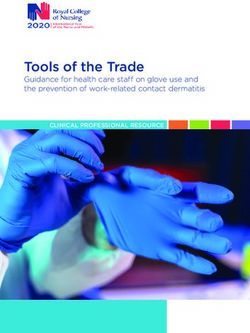
EUROIMMUN avidity ELISA:
detection of acute infections
Alternative method for the diagnosis of acute infections
The determination of the avidity of specific IgG is not affected by influencing factors of IgM analytics
No false-positive results through the influence of persisting IgM antibodies
No false-negative results through the non-production of IgM antibodies
Optimised for fully automated processing
Simple handling:
Break-off microplate wells
Ready-to-use reagents (no mixing or diluting necessary)
Bar- and colour-coded reagents, largely exchangeable between different lots and between different parameters
Standardised incubation conditions
Incubation protocols for all tests integrated in EUROIMMUN Analyzers:
no additional programming necessary
Comprehensive validation of test systems for EUROIMMUN Analyzers
in accordance with directive 98/79/EC and on the basis of EN ISO 13485:2003
Detailed validation documents available for all parameters
18Detection
methods
low-avidity IgG acute
infection
+ urea
solution binding
Maturing of the B-lymphocytes
destroyed
Increase of the avidity
antigen
high-avidity IgG past
Infection
+ urea
solution
binding
stable
antigen
19Line blots
Detection
methods
EUROLINE: line blots for comprehensive antibody profiles
For more information on this subject scan
the QR code or enter the Quick Link code
q118 at www.euroimmun.com
EUROLINE: multiparameter line blots
for comprehensive antibody profiles
Uncomplicated test performance, reliable and simple evaluation:
Quick: The total time for analysis is 115 minutes. All incubation steps are carried out at room temperature.
Automatable incubation: with EUROBlotOne or EUROBlotMaster.
Secure: The antigen lines are located at precisely defined positions. Correct performance of the individual incu‑
bation steps is indicated by staining of the control band contained on each EUROLINE test strip. The conjugates
are colour-coded. Positive and negative results can be distinguished from each other reliably and easily. The
intensity of bands correlates with the antibody titer.
Monospecific: The antigens used are purified antigens, mostly isolated by affinity chromatography, or antigen
extracts. The membrane strips do not contain superfluous proteins that may lead to unspecific positive results.
Multiparameter analysis: The use of an antigen spectrum that is specifically tailored to the diagnostic require‑
ments increases the serological detection rate.
Evaluation: The EUROLineScan program developed by EURO IMMUN allows standardised evaluation of
EUROLINE test strips, easy data management and detailed documentation of results. First, the incubated EURO‑
LINE test strips are scanned by a flatbed scanner or photographed by a camera system. EUROLineScan recog‑
nises the position of the strips, even if they have been placed inexactly, identifies the bands, and measures their
intensity. Finally, the results are saved together with the image data and a separate results sheet can be issued
for each patient. EUROLineScan can be integrated easily into EUROLabOffice or any other LIMS for optimal data
communication.
b
a
-B
-B
l
ro
A
A
C
00
b
sE
sE
bp
sp
sp
nt
9
8
8
B
p3
p5
p1
p1
Vl
Vl
Co
L-
O
O
D
Borr GE
2021
Detection
methodsdiagnostics
Veterinary
Veterinary diagnostics
2223
Veterinary
diagnosticsInfection diagnostics
diagnostics
Veterinary
Anaplasma · Borrelia · Brucella · Ehrlichia · Leishmania · MERS-CoV · Toxoplasma · WNV · Tick-Borne Profile
Anaplasma
Clinical information: Anaplasma (A.) phagocytophilum is the causative agent of anaplasmosis, a bacterial dis‑
ease which is transmitted through bites from ticks of the genus Ixodes. A. phagocytophilum is a gram-negative,
obligate intra-cellular bacterium which attacks mostly neutrophilic granulocytes, but also, in rare cases, eosino‑
philic granulocytes. Anaplasmosis occurs worldwide, its prevalence depending on the distribution area of the
transmitting vectors.
There are different names for the clinical picture of an infection with A. phagocytophilum in dogs: granulocytic
ehrlichiosis (obsolete), canine granulocytic anaplasmosis, and, simply, and most frequently used: anaplasmosis.
Clinical symptoms of canine anaplasmosis include a reduced general condition with fever, weight loss, vomiting,
dyspnoe, spleno- and hepatomegaly, lymphadenopathy, oedema of the joints, leukopenia, anaemia, haemorrha‑
gia, polyarthritis and CNS symptoms as a result of inflammation and bleeding in the meninges. In some dogs the
immune system is able to eliminate the pathogen, others show an asymptomatic or chronic course. In the chronic
form, alternating lamenesses may occur due to polyarthritis.
A. phagocytophilum infection in horses is also known under various names: granulocytic ehrlichiosis (obsolete),
equine granulocytic anaplasmosis, and in most cases also: anaplasmosis. The clinical symptoms of equine ana‑
plasmosis are a reduced general condition with fever, anorexia, lethargy, oedema of the limbs, petechia, icterus,
reluctance towards physical activity, and ataxia. Older horses show clearer symptoms than younger ones.
Diagnostics: Antibodies against A. phagocytophilum occur in the serum of infected animals after seven to
fourteen days. Different techniques are used for the serological detection of antibodies, such as ELISA or indirect
immunofluorescence test (IIFT). It needs to be taken into consideration that many dogs and horses show specific
antibodies against A. phagocytophilum but are not clinically conspicuous. For diagnosis, it is hence necessary to
investigate two blood samples at a time interval. A twofold titer increase or a seroconversion are here diagnosti‑
cally relevant. If the first blood sample tests negative, a second sample should be examined after two weeks in
cases of suspected anaplasmosis, since dogs and horses do not produce antibodies in the early phase of infection.
Borreliosis should be excluded by differential diagnosis. As of yet, no vaccines are available for dogs or horses.
24diagnostics
Veterinary
Product overview
Method Substrate Diagnostic application Order number Page
Recombinant, purified antigen
IgG ELISA; high sensitivity
ELISA from Anaplasma phagocyto‑ EI 220m-9601 GC 48/50
and specificity
philum
Product overview
Method Substrate Diagnostic application Order number Page
Recombinant, purified antigen
IgG ELISA; high sensitivity
ELISA from Anaplasma phagocyto‑ EI 220m-9601 GE 48/50
and specificity
philum
25Infection diagnostics
diagnostics
Veterinary
Anaplasma · Borrelia · Brucella · Ehrlichia · Leishmania · MERS-CoV · Toxoplasma · WNV · Tick-Borne Profile
Borrelia
Clinical information: Borrelia is the causative agent of Lyme borreliosis, a disease which is transmitted through
bites from ticks of the genus Ixodes. The gram-negative bacteria are collectively referred to as Borrelia burgdorferi
sensu lato. In this group, the genospecies Borrelia burgdorferi sensu stricto, Borrelia garinii and Borrelia afzelii
are pathogenic for dogs and horses. Whereas in the U.S. only B. burgdorferi sensu stricto is relevant, more than
80 % of Borrelia in European ticks belong to the pathogenic genospecies B. garinii or B. afzelii. Dogs and horses
have a significantly increased risk of infection because of their higher frequency of contact with ticks. Most
of the infections, however, proceed asymptomatically. Infection does not confer strong immunity. Reinfection
is therefore possible. Antibodies against B. burgdorferi can be found in the serum of specifically infected or
vaccinated animals. An infection with B. burgdorferi is associated with a variety of clinical symptoms, which
generally occur weeks or months after infection.
Primary symptoms of Lyme borreliosis in dogs include lethargy, loss of appetite and fever and are therefore
rather unspecific. The first more or less specific symptom in dogs is lameness due to myositis or arthritis, which
generally occurs in a later stage of infection. Neurological impairments and damage to the kidneys (glomerulone‑
phritis) or heart (myocarditis) are rarely described. Various vaccines are available for dogs.
Borreliosis in horses is characterised by arthritis, alternating lamenesses, algesic muscles, uveitis, encephalitis,
miscarriage, fever and lethargy. A vaccine for horses has recently been brought onto the market.
Erythema migrans, a characteristic sign of borreliosis in humans, is not relevant in either dogs or horses, since it
cannot be seen through the fur or because of dark skin.
Diagnostics: Diagnosis of canine or equine borreliosis is based on clinical symptoms, differential diagnostics
and the detection of antibodies against Borrelia antigens. Some studies recommend a two-step strategy for the
determination of Borrelia-specific antibodies. Firstly, a sensitive screening test (ELISA or IIFT) is used. Sera with
a positive or borderline screening result are investigated further using an immunoblot to differentiate between
Borrelia-specific and unspecific reactions. Since antibodies against Borrelia are first produced two to six weeks
after infection, serological tests performed in the early stage of Lyme borreliosis can be negative. A follow-up
sample taken after seven to ten days should therefore be tested in suspected cases. IgM antibodies against Bor‑
relia antigens can be found for a period of a few weeks in the early stage of infection.
26diagnostics
Veterinary
Product overview
Method Substrate Diagnostic application Order number Page
IgG ELISA; complete antigen
Antigen extract from Borrelia EI 2132-9601-2 GC 48/50
spectrum, high sensitivity
burgdorferi sensu stricto,
Borrelia afzelii and Borrelia IgM ELISA; complete
EI 2132-9601 MC
garinii antigen spectrum incl. OspC; 48/50
ELISA detection of acute infections
Recombinant and purified
IgG ELISA; highly specific
VlsE antigen (variable major
marker for early detection of EI 2132-9601-1 GC 48/50 NEW
protein-like sequence, ex‑
Borrelia infections
pressed) of Borrelia
IgG line blot with
diagnostically relevant
p18, p21, OspC (p25), OspA DN 2136-1601 GC
Borrelia antigens; 48/50
(p31), p39, p41, p100, VlsE-Bb DN 2136-3201 GC
differentiation between
Blot vaccination and infection
IgM line blot with
p18, p21, OspC (p25), p39, diagnostically relevant DN 2136-1601 MC
48/50
p41, p100 Borrelia antigens; detection DN 2136-3201 MC
of acute infections
Product overview
Method Substrate Diagnostic application Order number Page
Antigen extract from Borrelia IgG ELISA; complete
ELISA burgdorferi sensu stricto and spectrum of relevant EI 2132-9601 GE 48/51
Borrelia afzelii antigens, high sensitivity
IgG line blot with diag‑
p18, OspC (p25), OspA (p31), nostically relevant Borre‑
DN 2136-1601 GE
Blot p39, p58, p100, Lipid-Bb, VlsE- lia antigens; differentia‑ 48/50 NEW
DN 2136-3201 GE
Bb, VlsE-Ba, DbpA tion between vaccination
and infection
27Infection diagnostics
diagnostics
Veterinary
Anaplasma · Borrelia · Brucella · Ehrlichia · Leishmania · MERS-CoV · Toxoplasma · WNV · Tick-Borne Profile
Brucella
Clinical information: Brucellosis is a zoonotic disease which is caused by gram-negative bacteria from the Bru‑
cella genus. Brucella is classified as risk group III by the WHO. In camels and bovines, different Brucella species
have been identified, e.g. Brucella abortus and melitensis. Brucella can be transmitted to humans via fresh milk
or raw meat and turn into a serious health problem in the affected regions. Human brucellosis is considered as
the most widely distributed zoonosis, with 500,000 new infections per year. Transmission of the pathogen can be
oral, but also venereal, congenital or perinatal. The economic loss due to miscarriage, decreased milk production,
reduced fertility, and the transmission of the disease to other species, including humans, is significant.
Infections in non-gestating bovines usually proceed asymptomatically, whereas in pregnant bovines the following
symptoms or sequelae are observed: late abortion, retained placenta, subclinical mastitis, sterility and, in rare
cases, tendinitis and joint inflammation. Male animals experience orchitis and epididymitis.
Camels of the species Camelus bactrianus and Camelus dromedarius are often infected with Brucella, especially
if they live in direct vicinity of infected ruminants such as cattle, sheep or goats. Entry sites for Brucella are the
lungs, intestinal tract, mucous membranes and skin. Experimental infection of camels with Brucella abortus led to
mild clinical symptoms, e.g. inappetence, minimal lameness due to arthritis, and bilateral lacrimation. Orchitis and
epididymitis occurred with Brucella abortus and Brucella melitensis. Retentio secundarium, placentitis, infections
of the urogenital tract, abortion with mummification, and infertility were also observed.
Diagnostics: Reliable diagnosis can only be achieved by direct detection of Brucella in the affected tissue, e.g.
from the placenta or lymph nodes. This procedure, however, is complicated, and also constitutes a potential infec‑
tion risk for the laboratory staff. For this reason, various serological test systems for the detection of antibodies
against Brucella have been developed, including the complement fixation test (CFT) and Rose Bengal test (RBT).
But these tests are time-consuming and limited with respect to sensitivity and standardisation. The RBT can only
be used for monitoring in Brucella-free regions. The World Organisation for Animal Health OIE (“Office Interna‑
tional des Epizooties”) names various serological tests for the diagnosis of bovine antibodies against Brucella,
including the above-mentioned CFT and RBT, as well as ELISA. However, the organisation also points out that
a positive result should always be verified using a confirmatory test. ELISAs based on a large antigen spectrum
offer a high sensitivity and are therefore ideally suited for screening.
28diagnostics
Veterinary
Product overview
Method Substrate Diagnostic application Order number Page
IgG ELISA; highly sensitive
Suitable components of screening ELISA for the
ELISA EI 2189-9601 GB 48/51
Brucella, native detection of anti-Brucella
antibodies in bovines
Product overview
Method Substrate Diagnostic application Order number Page
IgG ELISA; high sensitivity;
first commercially available
Suitable components of
ELISA screening ELISA for the EI 2189-9601 GK 48/51
Brucella, native
detection of anti-Brucella
antibodies in camels
29Infection diagnostics
diagnostics
Veterinary
Anaplasma · Borrelia · Brucella · Ehrlichia · Leishmania · MERS-CoV · Toxoplasma · WNV · Tick-Borne Profile
Ehrlichia
Clinical information: Ehrlichiosis is a disease which is transmitted to animals and humans by tick bites. It was
first described in Algeria in 1935. Ehrlichiosis in dogs is mainly caused by the pathogen Ehrlichia (E.) canis, which
is transmitted by the brown dog tick (Rhipicephalus sanguineus) and may lead to canine monocytic ehrlichiosis
(CME). E. canis is a gram-negative, obligatory intracellular bacterium which mainly affects mononuclear blood
cells. CME is a worldwide distributed disease in tropical and moderate climates. The geographical occurrence of
E. canis is increasing with the proliferation of the tick vector due to the climate change.
Canine monocytic ehrlichiosis in dogs is a multisystemic disease which may manifest in acute, subclinical or
chronic forms. After an incubation period of 1 to 3 weeks an acute CME develops, which is characterised by high
fever, lethargy, weight loss, lymphadeno- and splenomegaly and haemorrhages. Damage to the eyes occurs fre‑
quently, which may even cause blindness. Inflammation or bleeding in the meninges may cause different CNS
symptoms. After 2 to 4 weeks, the subclinical phase starts. At this stage, the dogs appear generally healthy and
without any obvious symptoms, even though high titers of E. canis-specific IgG antibodies and changes in the
blood count can already be detected. Some dogs enter the chronic phase, in which the symptoms resemble those
of an acute CME, but are more pronounced.
Diagnostics: Direct detection of E. canis by staining or culture is possible, but is usually not performed since
these methods are too complicated for screening diagnostics. Detection of typical cytoplasmic morulae in the
monocytes by means of blood smears supports the diagnosis of CME. However, only a very small percentage of
the clinical cases shows characteristic morulae, which makes the search difficult and time-consuming. Culturing
of E. canis also requires much time and is therefore not suitable for routine diagnostics. PCR is regularly used
for direct detection of Ehrlichia DNA. Here, quantitative real-time PCR should be preferred over conventional PCR
due to its higher sensitivity. A decisive advantage of serological antibody detection is the possibility to determine
E. canis-specific antibodies or the titer course. The latter is recommended for assessment of therapy success.
30diagnostics
Veterinary
Product overview
Method Substrate Diagnostic application Order number Page
IgG ELISA; high specificity
Recombinant, purified
ELISA due to the use of a specific EI 220l-9601 GC 48/50 NEW
Ehrlichia canis antigen
recombinant antigen
31Infection diagnostics
diagnostics
Veterinary
Anaplasma · Borrelia · Brucella · Ehrlichia · Leishmania · MERS-CoV · Toxoplasma · WNV · Tick-Borne Profile
Leishmania
Clinical information: Leishmaniasis is a zoonotic infection that is caused by protozoa of the Leishmania genus.
Leishmania infantum, Leishmania chagasi and Leishmania donovani, which belong to the Leishmania donovani
complex, are of particular importance. These monocellular parasites are transmitted to humans or animals via
the bite of female sandflies of the genera Phlebotomus (Africa, Asia, Europe) or Lutzomyia (Central and South
America). Dogs are considered as the most important reservoir. Due to the zoonotic potential, infected dogs are
a major problem in veterinary and human medicine. It is assumed that 50 % to 80 % of dogs in endemic areas
are infected with Leishmania. However, Leishmania infection is not synonymous with canine leishmaniasis. Less
than 10 % of infected dogs show clinical symptoms. Certain dog breeds and the age of the dog are associated
with a predisposition for the development of leishmaniasis. The immune response of the dog is also crucial for
manifestation.
Leishmania infections are characterised by long incubation times, which may be months to years. The various
zymodemes of the individual Leishmania species can cause different clinical manifestations. In dogs it is often
impossible to discriminate between visceral and cutaneous leishmaniasis because the visceral form is frequently
accompanied by skin changes. The large variety of symptoms includes fever, weight loss, anorexia, various skin
changes (e.g. dermatitis, hyperkeratoses, paw pad fissures), eye problems (e.g. uveitis, keratoconjunctivitis) and
various organ problems (e.g. glomerulonephritis, hepato- and splenomegaly), diseases of the musculoskeletal
system (e.g. due to polyarthritis) and changes in laboratory results (e.g. hyperglobulinaemia, hypoalbuminaemia,
proteinuria). Clinical symptoms of canine leishmaniasis can improve or even subside with chemotherapy. How‑
ever, relapses are possible since the treatment does not allow complete elimination of the parasite. Vaccination
against Leishmania is possible.
Diagnostics: Diagnosis of Leishmania infection is generally based on serological tests (IIFT or ELISA) detecting
Leishmania-specific IgG antibodies. High antibody titers correlate with clinical leishmaniasis or indicate a possible
manifestation of canine leishmaniasis in infected asymptomatic dogs. Pathogen detection by means of PCR can
help to establish a Leishmania diagnosis, but it does not allow conclusions to be drawn with respect to a clini‑
cal manifestation. Therefore, serological detection is the method of choice for diagnosing canine leishmaniasis.
32diagnostics
Veterinary
Product overview
Method Substrate Diagnostic application Order number Page
IgG ELISA; high sensitivity
for infections with
Specific, purified antigen of Leishmania of the
ELISA the Leishmania donovani L. donovani complex; EI 2232-9601 GC 48/50
complex high specificity due to use
of Leishmania-specific
recombinant antigen
33Infection diagnostics
diagnostics
Veterinary
Anaplasma · Borrelia · Brucella · Ehrlichia · Leishmania · MERS-CoV · Toxoplasma · WNV · Tick-Borne Profile
MERS coronavirus
Clinical information: Middle East respiratory syndrome (MERS) is caused by a previously unknown coronavirus
(MERS-CoV). So far, all human MERS-CoV infections have originated in the Middle East. About 40 % of known
cases were fatal. The incubation time ranges from less than a week in the majority of cases to up to 12 days in
individual cases. Transmission between humans takes place via aerosols and smear infections. Respiratory secre‑
tions of the upper respiratory tract of infected persons play a particularly important role as they can be passed on
by sneezing, coughing, and via contaminated hands.
Camels are currently discussed as the potential source of sporadic MERS-CoV infections in humans. Antibodies
against MERS-CoV were found in camel sera that had already been collected in 1983. This leads to the assump‑
tion that the virus has been circulating in the camel population for a long time. The antibody prevalence in adult
camels in endemic areas is up to 100 %. In newborn camels, it is assumed that the virus is multiplied and shed,
as time is needed to generate neutralising antibodies. During this time the calves might be a source of infection
for humans. There is no approved vaccine available.
Diagnostics: Clinical symptoms in camels infected with MERS-CoV are
rare and generally mild. The most reliable laboratory diagnostic methods
for confirmation of suspected MERS-CoV infections in camels include the
direct detection of MERS-CoV using PCR and the detection of antibodies
against MERS-CoV using indirect immunofluorescence (IIFT), ELISA, or
neutralisation tests. Cross reactions with other coronaviruses, in particular
bovine coronaviruses, need to be taken into account in serological diag‑
nostics. These can be reduced using a specific domain of the recombinant
spike protein as the antigen in the ELISA. The IIFT based on MERS-CoV- Anti-MERS-CoV positive
infected cells as the substrate provides a highly sensitive screening test
that allows qualitative and semi-quantitative detection of antibodies against MERS-CoV. Positive results should
be confirmed with another method, ideally by means of a neutralisation test.
34You can also read