Place des thérapies néoadjuvantes dans le cancer du sein - Dr Corinne Gregoire - Chirec
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Place des thérapies
néoadjuvantes dans le cancer du
sein
Dr Corinne Gregoire
13/10/2018 1 Dr Corinne Gregoire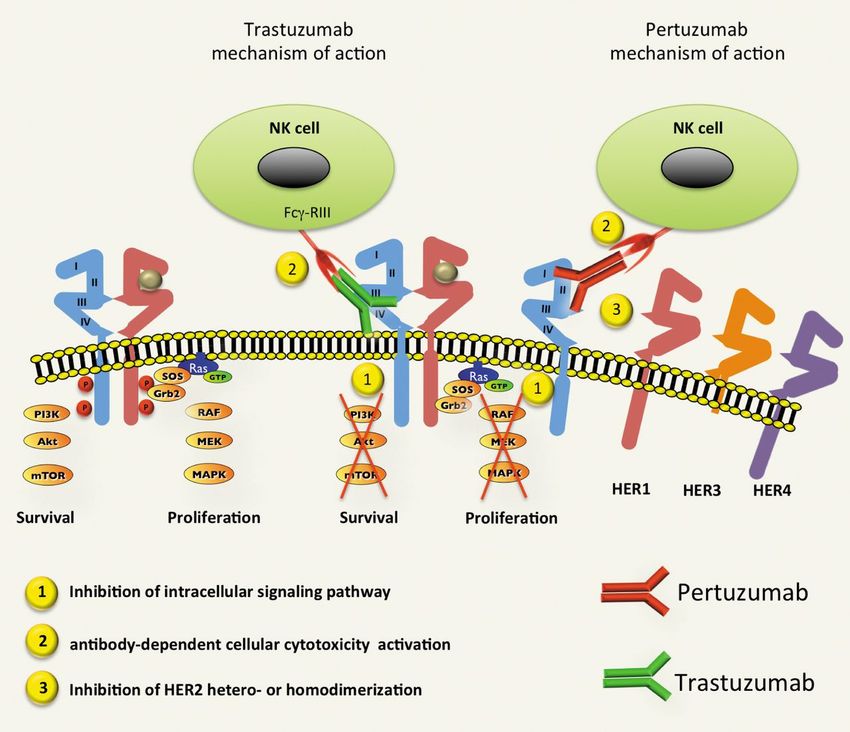
Définition: Néoadjuvant: qui précède le traitement principal.
Buts:
1.Contrôle local.
2.Augmentation du taux de chirurgie conservatrice.
3.Sensibilité individuelle au traitement.
4.Contrôle des micrométastases / résistance au traitement.
13/10/2018 2 Dr Corinne Gregoire
A Death B Disease progression
Avril/Mauriac Avril/Mauriac
Danforth
Danforth
Gazet
Makris
Makris
NSABP B18 NSABP B18
Scholl Scholl/Broet
Scholl/Broet
Semiglazov
Semiglazov
Buts:
Van der Hage
Van der Hage
ALL ALL
1.Contrôle local des tumeurs .2 .4 .6 .8 1 2
Risk ratio (95% CI) for neo-adjuvant vs. adjuvant treatment
4 .2 .4 .6 .8 1 2
Risk ratio (95% CI) for neo-adjuvant vs. adjuvant treatment
4
localement avancées. C Distant recurrence D Loco-regional recurrence
• T. inopérables Avril/Mauriac Avril/Mauriac
Danforth
Danforth
Gazet
• T. opérables Gazet
Makris
Makris
NSABP B18
NSABP B18 Scholl
Scholl/Broet
Scholl/Broet
Semiglazov
Semiglazov
Van der Hage
ALL
ALL
.2 .4 .6 .8 1 2 4 .2 .4 .6 .8 1 2 4
Risk ratio (95% CI) for neo-adjuvant vs. adjuvant treatment Risk ratio (95% CI) for neo-adjuvant vs. adjuvant treatment
Fig. 1. Meta-analysis for primary outcomes with neoadjuvant therapy compared (CI) for the risk ratio (extending lines); the summary risk ratio (ALL) and 95%
with adjuvant therapy for breast cancer. In each panel, each study [Van der Hage confidence intervals by fixed effects calculations are also shown by diamonds.
Mauri
et al. (8), Avril et al./Mauriac et al. (9,10et al,Neoadjuvant
), Semiglazov et al. (11), Schollversus
et al. (12), adjuvant systemic
For all panels, treatment
values greater inthat neoadjuvant treatment has a
than 1 indicate
Scholl et al. (13), Broet et al. (breast
14), Makriscancer:
et al. (15), NSABP B-18 (16,17), Gazet JNCI,
a meta-analysis. worse outcome
vol 97, compared
feb 2,with2005
adjuvant treatment. (A) Death. (B) Disease pro-
et al. (18), Danforth et al. (19)] is shown by the point estimate of the risk ratio gression. (C) Distant disease recurrence. (D) Loco-regional disease recurrence.
(square proportional to the weight of each study) and 95% confidence interval Arrow = 95% confidence interval extends beyond the depicted range.
13/10/2018 3 between the arms for theDroutcomes
found no difference
Corinne Gregoire
death Secondary Outcomes
(summary RR for death = 1.00, 95% CI = 0.90 to 1.12), disease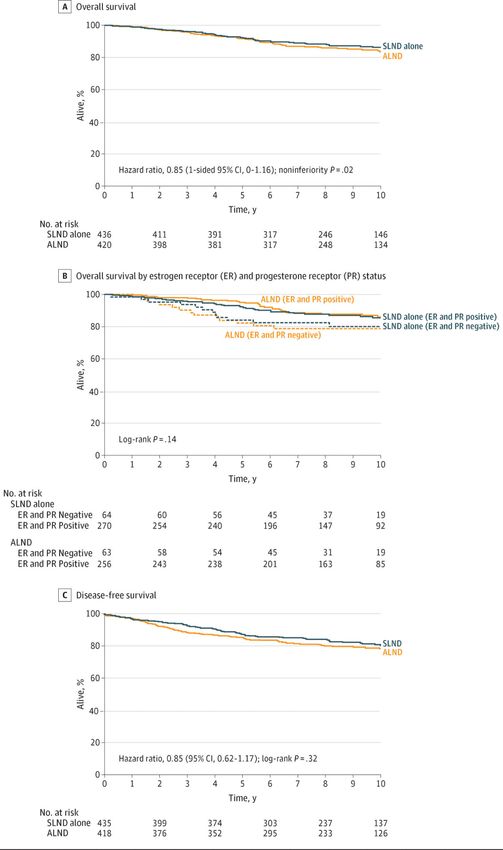
Table 2. First reported sites of treatment failure
Treatment group
Postoperative AC Preoperative AC
Type and site of failure No. % No. %
Clinically inoperable 0 0 1 0.1
Gross residual disease 11 1.5 8 1.1
IBTR only* 34 7.6 54 10.7
Buts: Other local recurrence 21 2.8 21 2.8
Regional recurrence 30 4.0 24 3.2
1.Contrôle local. Distant metastasis 155 20.6 145 19.5
(except opposite breast)
2.Augmenter le taux de chirurgie Second primary cancer 32 4.3 29 3.9
conservatrice: (except opposite breast)
Opposite breast cancer 30 4.0 25 3.4
Dead, no evidence of disease 25 3.3 16 2.2
Total first events 338 45.0 323 43.5
Alive, event free 413 55.0 419 56.5
Total No. of patients 751 100 742 100
*Percentages for ipsilateral breast tumor recurrence (IBTR) are based on the
numbers of patients who received lumpectomies.
Preoperative Chemotherapy in Patients With Operable Breast Cancer: Nine-Year Results From National
Surgical Adjuvant Breast and Bowel Project B-18, Wolmark et al, Journal of the National Cancer
Institute Table 3. Clinical
Monographs factors associated with ipsilateral breast tumor
No. 30, 2001
13/10/2018 4 Dr Corinne Gregoire
recurrence (IBTR)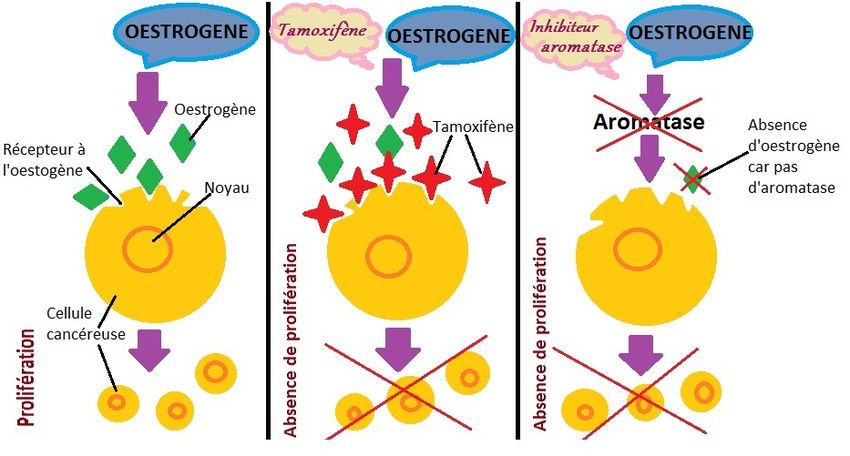
Buts:
1.Contrôle local.
2.Augmenter le taux de chirurgie
conservatrice:
Golshan et al, Impact of neoadjuvant therapy on eligibility for and frequency of breast conservation in stage II–III HER2-
positive breast cancer: surgical results of CALGB 40601 (Alliance), Breast Cancer Res Treat. 2016 November ; 160(2): 297–304.
doi:10.1007/s10549-016-4006-6.
13/10/2018 5 Dr Corinne Gregoire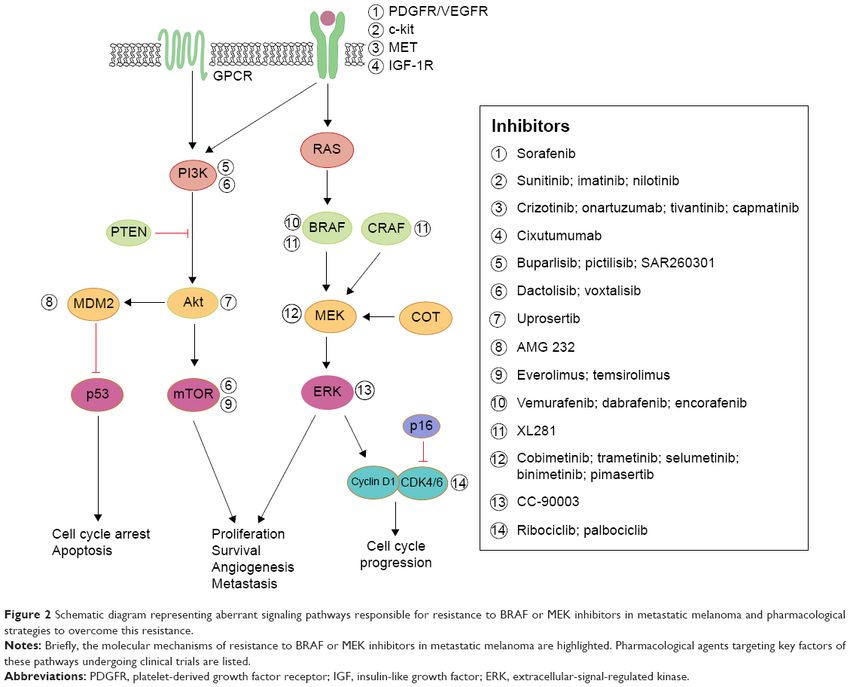
A A
Clinically node positive 100
Clinically node negative
Tumor size > 5 cm 80
Tumor size 2.1 - 5 cm
Surviving (%)
Tumor size ≤ 2 cm
60
Patients 50 + at entry
Patients < 50 at entry
40
HR = 0.32 P < .0001
OS, HR = 0.99
All eligible patients Group N Deaths
20 No pCR 599 265
pCR 86 14
0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8
Buts:
Hazard Ratio
0 2 4 6 8 10 12 14 16
Pre-OP AC Better Post-OP AC Better
Time After Random Assignment (years)
1.Contrôle local. B Clinically node positive
B
2.Augmenter le taux de chirurgie
Clinically node negative
100
Tumor size > 5 cm
conservatrice. Tumor size 2.1 - 5 cm
Tumor size ≤ 2 cm
80
Surviving (%)
3.Identifier la sensibilité individuelle
Patients 50 + at entry
Patients < 50 at entry
60
au traitement: DFS, HR = 0.93
All eligible patients 40
HR = 0.36 P < .0001
Group N Deaths
20 No pCR 1857 490
0.4 0.6 0.8 1.0 1.2 1.4 1.6 pCR 397 42
Hazard Ratio
Pre-OP AC Better Post-OP AC Better
0 2 4 6 8
C
Clinically node positive
Time After Random Assignment (years)
Preoperative Chemotherapy: Updates of National Surgical Adjuvant
Clinically node negative
Breast and Bowel Project Protocols B-18 and B-27;$, Rastogi et al, Fig 4. Survival by pathologic complete response (pCR) status in patients who
JCO, vol26 , nr5, 2008
Tumor size > 5 cm received preoperative doxorubicin and cyclophosphamide. (A) National Surgical
Adjuvant Breast and Bowel Project (NSABP) Protocol B-18: group 2 patients. (B)
Tumor size 2.1 - 5 cm
NSABP Protocol B-27: all patients. HR, hazard ratio.
Tumor size ≤ 2 cm
13/10/2018 6 Dr Corinne Gregoire
Patients 50 + at entry
post-treatment pathologic nodal status was also a strong pre-
Buts:
1.Contrôle local
2.Augmenter le taux de chirurgie conservatrice
3.Identifier la sensibilité individuelle au traitement
4.Autres intérêts:
• pCR= marqueur de substitution
• testing BRCA
• diminuer les résistances
• études
Désavantages: rechute locale???
13/10/2018 7 Dr Corinne Gregoire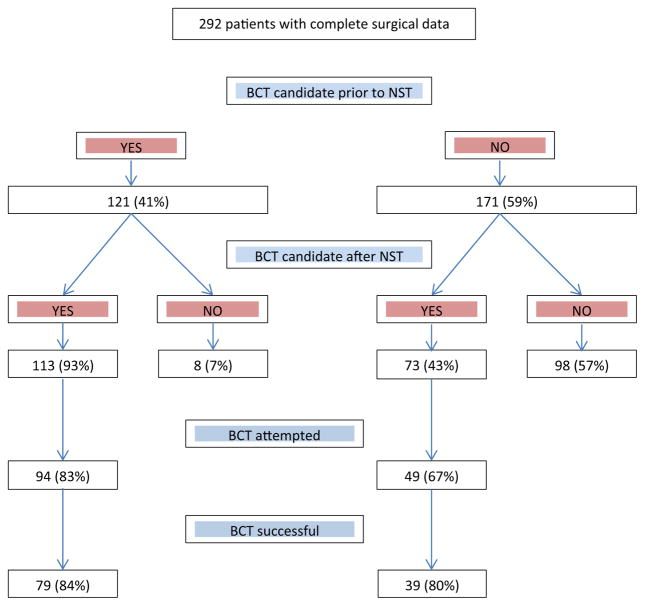
Traitement du cancer du sein
=
Traitement multimodal
13/10/2018 8 Dr Corinne Gregoire
c/article-abstract/26/suppl_5/v8/344805 by guest on 11 October 2018
Table 2. Surrogate definitions of intrinsic subtypes of breast cancer according to the 2015 St Gallen Consensus Conference [23] and also
recommended by the ESMO Clinical Practice Guidelines
Intrinsic subtype Clinicopathologic surrogate definition Notes
Luminal A ‘Luminal A-like’ *Ki-67 scores should be interpreted in the light of local laboratory values: as an
ER-positive example, if a laboratory has a median Ki-67 score in receptor-positive disease of
HER2-negative 20%, values of 30% or above could be considered clearly high; those of 10% or
Ki67 low* less clearly low,
PgR high** **Suggested cut-off value is 20%; quality assurance programmes are essential for
low-risk molecular signature (if available) laboratories reporting these results.
Luminal B ‘Luminal B-like (HER2-negative)’
ER-positive
HER2-negative
and either
Ki67 high or
PgR low
high-risk molecular signature (if
available)
‘Luminal B-like (HER2-positive)’
ER-positive
HER2-positive
any Ki67
any PgR
HER2 overexpression ‘HER2-positive (non-luminal)’
HER2-positive
ER and PgR absent
‘Basal-like’ ‘Triple-negative (ductal)’ There is ∼80% overlap between ‘triple-negative’ and intrinsic ‘basal-like’ subtype,
ER and PgR absent but ‘triple-negative’ also includes some special histological types such as (typical)
HER2-negative medullary and adenoid cystic carcinoma with low risks of distant recurrence.
13/10/2018 9 Dr Corinne Gregoire
ER, oestrogen receptor; HER2, human epidermal growth factor 2 receptor; PgR, progesterone receptor.Indications:
1.Cancer inflammatoire: indication absolue
2.Triple négatif
3.Tumeur Her2+
4.Tumeur HR+
13/10/2018 10 Dr Corinne GregoireIndications:
1.Cancer inflammatoire
2.Triple négatif: BRCA muté
3.Tumeur Her2+
4.Tumeur HR+
BRCA mutations and their influence on pathological complete response and prognosis in a clinical cohort of neoadjuvantly treated breast cancer patients. Wunderle et al, Breast
Cancer Res Treat. 2018
13/10/2018 11 Dr Corinne Gregoire1.0
98% P = .24
94%
0.9
Probability Being Alive
88%
0.8
P = .0001
0.7
Indications: 68%
0.6
1.Cancer inflammatoire pCR/non-TNBC
2.Triple négatif: 0.5
pCR/TNBC
RD/non-TNBC
3.Tumeur Her2+ RD/TNBC
0.4
4.Tumeur HR+ 1 2 3 4 5 6 7
Time After Surgery (years)
Fig 2. Overall survival as a function of response to chemotherapy (pathologic
complete response [pCR] v residual disease [RD]) and triple-negative status
(triple-negative breast cancer [TNBC] v non-TNBC).
Response to Neoadjuvant Therapy and Long-Term Survival in Patients With Triple-
Negative Breast Cancer,Liedtke et al, JCO, vol26 nr8 2008
anthracycline-based regimenDr Corinne
without a taxane) is reflected by the
13/10/2018 12 Gregoire
relatively low overall pCR rate (11% and 20% for TNBC and non-Indications:
1.Cancer
inflammatoire
2.Triple négatif
3.Tumeur Her2+
4.Tumeur HR+
13/10/2018 13 Dr Corinne Gregoire13/10/2018 14 Dr Corinne Gregoire
Indications:
1.Cancer inflammatoire
2.Triple négatif
3.Tumeur Her2+ THP: pCR 45,8%
4.Tumeur HR+
Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-
positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial, Gianni et al, Lan Onc 2012
13/10/2018 15 Dr Corinne GregoireAnnals of Oncology original a
HR-
Indications:
1.Cancer
inflammatoire
2.Triple négatif
3.Tumeur Her2+
4.Tumeur HR+
Pertuzumab plus trastuzumab in combination with standard neoadjuvant
anthracycline-containing and anthracycline-free chemotherapy regimens
in patients with HER2-positive early breast cancer: a randomized phase
II cardiac safety study (TRYPHAENA). Schneeweiss A1, Ann Inc, éà& »
Figure 2. Pathological complete response in the ITT population. pCR rates and their respective 95% CIs are shown for pCR defined as yp
ypT0, and ypT013/10/2018 16 are also presented for
ypN0. pCR rates according to ypT0/is Dr patients
Corinne Gregoire
with ER- and/or PgR-positive tumors and patients wIndications:
1.Cancer
inflammatoire
2.Triple négatif
3.Tumeur Her2+
4.Tumeur HR+
13/10/2018 17 Dr Corinne GregoireIndications:
1.Cancer
inflammatoire
2.Triple négatif
3.Tumeur Her2+
HHS Public4.Tumeur
AccessHR+
Author manuscript
JAMA Oncol. Author manuscript; available in PMC 2017 December 21.
Author Manuscript
Published in final edited form as:
JAMA Oncol. 2016 November 01; 2(11): 1477–1486. doi:10.1001/jamaoncol.2016.1897.
Neoadjuvant Endocrine Therapy for Estrogen Receptor-Positive
Breast Cancer:
A Systematic Review and Meta-analysis
Laura M. Spring, MD,
Massachusetts General Hospital Cancer Center, Harvard Medical School, Boston
Arjun Gupta, MD,
Author
Department 13/10/2018 18
of Medicine, University of Texas Southwestern Dr Corinne
Medical Center, Gregoire
DallasA B
100 100
90 90
Disease-Free Survival (%)
80 80
Overall Survival (%)
70 70
Indications: 60 60
50 50
1.Cancer 40 40
inflammatoire 30 30
2.Triple négatif 20 HR, 1.00 (95% CI, 0.78 to 1.28); P = 1.00 20 HR, 1.15 (95% CI, 0.83 to 1.59); P = .41
3.Tumeur Her2+
EC-D EC-D
10 10
DC DC
4.Tumeur HR+ 0 1 2 3 4 5 6 0 1 2 3 4 5 6
Time (years) Time (years)
No. of Patients at Risk No. of Patients at Risk
1,001 949 818 357 1,001 980 905 435
1,011 957 820 361 1,011 993 902 437
Adjuvant Cyclophosphamide and Docetaxel With or Without Epirubicin for Early TOP2A-Normal Breast Cancer: DBCG
07-READ, an Open-Label, Phase III, Randomized Trial, Ejlertsen et al, JCO vol35 • nr 23 2017
jco.org © 2017
13/10/2018 19 Dr Corinne Gregoire
Downloaded from ascopubs.org by 94.225.35.158 on October 10, 2018 from 094.225A B
Indications:
1.Cancer
inflammatoire Figure 2
2.Triple négatif (A) Overall change in Ki67 before and after treatment with neo
letrozole in combination with palbociclib. Each line represents t
3.Tumeur Her2+ for individual patient. Ki67 >15% was considered as high prolif
fraction. (B) Change in Ki67 before treatment, on day 15 and af
4.Tumeur HR+ treatment with neoadjuvant letrozole in combination with palb
Each line represents the data for individual patient. Ki67 >15%
considered as high proliferation fraction.
seven (71.4%) patients (Fig. 2B). However, only
20 (40%) patients had a Ki67 less than 2.7 at t
of surgery after treatment. Except for three patie
Figure 1
Neoadjuvant palbociclib on ER+ breast cancer (N007): clinical response and EndoPredict’s value , Chow et al, Endocrine-Related Cancer (2018) 25, 123–130 elevation after treatment, the other 17 patients sh
The volume of the cancer on three-dimensional measurement before and
significant drop in value. Eight of 17 (47.1%) patie
after treatment with neoadjuvant letrozole in combination with
13/10/2018
palbociclib. Each line represents the data for individual 20 patient. a high
Dr Corinne proliferation fraction (Ki67 >15%) before tr
GregoireEvaluation ganglionnaire prétraitement néoadjuvant.
Etude ACOSOG (2005-2017): Pas de reprise de curage en cas de GGL
Giuliano et al.
sentinel positif (≤ 2GGL+/3, T1-2, cN0 et R/ adj).
Author Manuscript
En pratique:
1.GGL clin négatif: réalisation du GS avant NACT.
2.si GS+:
• ≤2+/3, pas de reprise après NACT (sauf T », Mastec ou pas de RT)
Author Manuscript
• ≥3+: CA après NACT.
3.GGL clin positif et RC clinique après NACT: GS à discuter.
13/10/2018 21 Dr Corinne GregoireTake home message
Les traitements néoadjuvants:
• Facilitent la chirurgie conservatrice.
• Augmentent la survie sans progression.
• Participent à une médecine personnalisée.
13/10/2018 22 Dr Corinne GregoireMerci de votre attention.
13/10/2018 23 Dr Corinne GregoireYou can also read

















































