Physician Health andWell-Being - CMA Guide to
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CMA Guide to
Physician Health
and Well-Being
Facts, advice
and resources
for Canadian doctorsEditor-in-chief: Dr. Michael Myers
Associate Editors: Drs. Todd Watkins and Gisele Microys
©2003 Canadian Medical Association
Published by the Canadian Medical Association
All rights reserved. No part of this book may be reproduced in any form or by any photographic, electronic,
mechanical or other means, or used in any information storage and retrieval system without the written permission
of the publisher. Contact Permissions Coordinator, CMA Publications, 1867 Alta Vista Dr., Ottawa ON
K1G 3Y6; fax 613 565-7704; permissions@cma.ca.
In the case of photocopying or other reprographic copying, contact The Canadian Copyright Licensing Agency
(Access Copyright) at 800 893-5777 (toll free) or visit www.accesscopyright.ca.
The information contained within is for reference and education only and is not intended to substitute for the advice
of a physician. The CMA assumes no responsibility for liability arising from any error in or omission from the book,
or from the use of any information contained in it.
National Library of Canada Cataloguing in Publication
CMA guide to physician health and well-being : facts, advice and
resources for Canadian doctors.
Issued also in French under title: Guide de l’AMC sur la santé et le
mieux-être des médecins.
Includes bibliographical references.
ISBN 1-894391-04-7
1. Physicians--Mental health. 2. Physicians--Health and hygiene.
3. Physicians--Health and hygiene--Canada. 4. Physicians--Mental health services--Canada.
5. Physicians--Services for--Canada. I. Canadian Medical Association.
RC451.4.P5C52 2003 610.69'52'019 C2003-900300-0
Ordering information and additional copies are available from:
Member Service Centre
Canadian Medical Association
1867 Alta Vista Dr.
Ottawa ON K1G 3Y6
Tel: 888 855-2555 or 613 731-8610 x2307
Fax: 613 236-8864
Email: cmamsc@cma.caContents Editorial: getting better at being well ..............................................................................3 Michael Myers Awareness of physician wellness issues growing ............................................................5 Gillian Wansbrough Self Being a physician can be harmful to your health...........................................................7 Barbara Sibbald Burnout — “an erosion of the soul” ...............................................................................9 Barbara Sibbald The health of women physicians...................................................................................11 Gail Beck A resident’s perspective on well-being ..........................................................................13 Laura Musselman Service Canadian physician health programs: an overview .....................................................16 Michael Kaufmann Tolerance for disruptive behaviour waning..................................................................18 Steve Wharry Back to school for health................................................................................................20 Barbara Sibbald Leadership Do you practise in an unhealthy workplace?................................................................21 Barbara Sibbald Physician health programs compulsory in US hospitals.............................................23 Barbara Sibbald When the College calls ...................................................................................................25 Pauline Anderson
The Canadian Physician Health Network Prince Edward Island — Physician Support Program........................................................................................27 Newfoundland and Labrador — Professionals’ Assistance Program...................................................................28 New Brunswick — Physician Health Program ..................................................................................................29 Nova Scotia — Professional Support Program...................................................................................................30 Quebec — Quebec Physicians Health Program.................................................................................................31 Ontario — Physician Health Program...............................................................................................................32 Manitoba — Physician at Risk Program............................................................................................................33 Saskatchewan — Physicians at Risk Committee................................................................................................34 Alberta — Physician and Family Support Program ...........................................................................................35 British Columbia — Physician Support Program of British Columbia..............................................................36
Editorial:
getting better at being well
Now is an exciting time to be involved ested and proficient at leading in our work setting,
in the field of physician health and well- our educational centres and our associations? What
being are the means — advanced degrees, continuing ed-
ucation course work, Internet offerings, workshops,
A highly successful international conference on the mentoring — we can use to stimulate and nurture
topic in Vancouver this past October, a growing others into becoming leaders? What are the rewards
body of evidence-based research, a heightened and pitfalls of these quests and the impact on our
health awareness among Canadian physicians, and self-regard, our families and our patients?
this publication are all testament to this. There is
consensus building among medical students and When I look to some of the challenges ahead, many
physicians, their loved ones, medical associations, are in the area of prevention.
provincial Colleges of Physicians and Surgeons,
Primary prevention
physician health specialists and even the general
public that there are serious problems in how we We need to continue to study and delineate risk
teach the doctors of tomorrow and how we practise factors in medical education and practice. Given the
front-line medicine. We physicians are a population changing dynamics and demands of medical prac-
at risk for illness and family breakdown. tice, do we need to change the criteria used to select
The theme of the recent conjoint Canadian medical students? How sensitive are we to the ge-
Medical Association and American Medical Associ- netic and developmental vulnerabilities of our med-
ation conference on physician health was “Steering ical school applicants, and how much do we accept
the Course: Self, Service and Leadership.” As a the elusive “woundedness” of some, in addition to
member of the planning committee for that confer- their intellectual achievements on paper and how
ence, let me explain what we intended to capture in well they perform at interview?
these overlapping concepts. Regarding our teaching methods, we must iden-
tify and deal with professors whose styles are out-
Self: How well do we take care of ourselves — dated, coercive, shaming or abusive. We continue to
physically, emotionally, spiritually? How can we im- lose gifted individuals whose life-stage commit-
prove as role models so that both our students and ments to child-bearing and child rearing conflict
our families are left a legacy of “doing it right”? with the imperative of academic productivity.
We also need sweeping reform in the culture of
Service: How can we extend our reach to colleagues medical practice. We physicians are used to hard
in distress so that we reduce suffering and isolation work and self-sacrifice in the service of our patients,
and diminish morbidity and lost productivity due to education and research. But many of us are being
illness? How do we identify those doctors living with exploited for what should be noble or admirable
life-threatening conditions, such as substance depen- qualities. The public’s expectations of its doctors are
dence and severe mood disorders, who are undiag- often unrealistic. I believe that this needs attention.
nosed, untreated, undertreated or self-treated? What
Secondary prevention
are the limits and boundaries of our intercollegial
responsibility — and how do we reach out and help, Our initiatives in educating medical students and
while simultaneously respecting each other’s rights to physicians about self-care and family-care must
autonomy, privacy and simple dignity? continue. But these will fail if we don’t make
overdue systemic changes in primary prevention.
Leadership: How can we become both more inter- Further, we must eliminate stigma. Its effects are
Facts, advice and resources for Canadian doctors 3pernicious when doctors colleagues. We need physicians who practise both
fall ill — stigma reinforces the science and art of medicine, who treat their
denial of symptoms and colleagues with respect and thoroughness and who
delays help-seeking, it dri- allow their physician-patients to be patients. This
ves self-medicating and also includes specialists in addiction medicine, psy-
noncompliance with treat- chiatrists and other mental health professionals with
ment, it augments suffer- expertise in physician health, subspecialists in mood
ing and exclusion and it disorders, rehabilitation and occupational health,
kills by self-neglect and eating disorders and forensic issues and good (and
suicide. We need to find affordable) treatment facilities.
ways of recognizing possi- We need to work closely with our Colleges of
ble illness in our trainees Physicians and Surgeons to assist and educate and
and colleagues and im- to address the perception of so many rank-and-file
prove our strategies (and physicians that their provincial College is out of
impart these to others) for touch with reality. We need to fight for more fund-
Dr. Michael Myers reaching out to them in a ing for research in many areas but especially
sensitive and helpful way. Provincial health pro- epidemiological studies on illness and treatment
grams and other resources need to be advertised nonadherence in physicians. And I hope to see im-
and “user-friendly.” And we need to listen to the provement in our relations with disability insurers
voices of doctors’ loved ones, not only to inform and what I call humanizing the medical workplace
our diagnoses and enrich our treatment plans, but for partially disabled physicians.
also to provide the support and care that they It is an honor to be invited to be editor-in-chief
might need. of this publication. I am proud to be a part of the
contingent of dedicated colleagues and CMA staff
Tertiary prevention
who work in this field and who have contributed so
If we are going to really heal and keep Canadian generously to this production.
physicians healthy and in remission, we need state-
of-the-art treatment. This means a cadre of family
physicians across this nation who are interested in Dr. Michael Myers, Clinical Professor,
and dedicated to looking after their physician Dept. of Psychiatry, University of British Columbia
4 CMA Guide to Physician Health and Well-BeingAwareness of physician wellness issues growing
Is stress over the state of our health care no specific program in the Northwest Territories;
system taking its toll on physicians? Where and the Yukon is covered by the Physician and Fam-
once drug and alcohol problems were the ily Support Program (PFSP) on contract by the
main reasons for calls to physician support pro- Alberta Medical Association.
grams, experts now say they’re seeing an increase in Most programs cater to physicians at all stages of
requests for help coping with depression and anxiety. their careers, as well as to their family members,
“We’re having a difficult time with the govern- providing support for everything from mental health
ment here,” says Dr. Paul Farnan, the newly and substance abuse problems to financial and legal
appointed clinical coordinator of the Physician problems. The new Canadian Physician Health
Support Program (PSP) of BC. “[Doctors are] trying Network (see page 27) was formed with an eye to
to ensure patients will get services while they them- coordinating and fostering the development of
selves are being bad-mouthed by the government … provincial physician health programs. “The health
it leads to a lot of stress.” In 2001, the PSP had just care doctors provide is only as good as their health,”
over 100 new cases out of about 300 calls. Farnan stresses. In 2001, 28% of calls to the BC PSP
In his inaugural speech at this year’s Canadian were psychiatric and mental health related, 23%
Medical Association (CMA) meeting in Saint John, personal, 12% behavioural (aggression, anger), 12%–
NB, CMA President Dr. Dana Hanson identified 13% addiction related and the remainder a combi-
physician health and well-being as one of his key nation. “The stigma of mental illness and addiction
priorities. “The reality of today’s practice environ- is extremely difficult for anyone to deal with in soci-
ment has brought with it an increase in stress- ety, and for physicians it’s even worse,” he says.
related illnesses,” he said. “Depression, burnout, About 85% of the calls to the Alberta Medical
family and financial crisis are all on the rise. As I Association’s PFSP are referred to an employee assis-
have travelled across Canada, I have found it deeply tance provider, according to Dr. Gisele Microys,
troubling to hear colleagues say: ‘I hate to go to clinical director of the program and chair of the
work now’ or ‘I am certain we take much better Canadian Physician Health Network. Microys says
care of our patients than anyone takes care of us.’ the program works because it takes into considera-
The goal must be to “nurture a positive and open tion the issues physicians grapple with, such as de-
attitude toward physician health and well-being… nial, delayed help seeking and confidentiality. In
We need to find the right balance between our pro- 2001, the program had 361 calls dealing with mari-
fessional and our private lives. We need to co- tal concerns (the most common), work stress,
ordinate divisional services, offer better help and get burnout, alcohol and drugs. Efforts are made to fast-
rid of the stigma that comes with asking for help.” track physicians and their family members, and
Currently, the issue is highlighted via the biennial mail-outs are done to encourage use of the service.
International Conference on Physician Health, co- Doctors’ identities are frequently wrapped up in
sponsored by the CMA and American Medical being a doctor,” says Microys, “on account of this we
Association. The larger provinces, such as Ontario tend to limit our interests and can be seen as idiot
and Alberta, also offer formal services geared toward savants of a sort,” she jokes, “There’s a need to hu-
physician health, variously supported by medical as- manize medicine, allow for balance in our lives.
sociations and other associations. Smaller provinces Some areas in need of attention ... we’re supposedly
have slightly different approaches: Nova Scotia and government employees but do not receive indexed
Newfoundland and Labrador have multiprofessional pensions. Hence many docs feel they have to work
support programs; New Brunswick has a volunteer until they drop with the “white coat” painted on and
committee; Prince Edward Island is in flux; there’s no way out.” She notes that doctors feel they have
Facts, advice and resources for Canadian doctors 5less control over the health care system and are frus- 75% of the calls have been about mental health (de-
trated with increasing bureaucracy and an inability pression, burnout, stress and anxiety). He notes a
to get the care they want quickly for their patients. lowering of the mean age of callers, from about 45
BC physician Dr. Michael Myers, known as the in 1990 to about 40 now, as well as more calls from
“doctor’s doctor” to his colleagues, cautions phy- women, general practitioners and residents.
sicians to take out insurance “today because you The good news is there is increasing recognition
never know. You may get wobbly.” Myers is past- of the importance of physician health, says
president of the Canadian Psychiatric Association Kingston, Ont., physician Dr. Raju Hajela, past-
(CPA), serves as a consultant to the BC PSP and is president of the Canadian Society of Addiction
chair of the section on physician health at the CPA. Medicine and current chair of the OMA Physician
He considers the support programs currently in Health Program Advisory Committee. “We’re start-
place to be solid, but he says more psychiatrists with ing to recognize that [as doctors] we need to look
doctor-treating expertise are needed. after ourselves. In the past, we were expected to be
Although some mental health issues physicians invincible, and there is still that expectation to pro-
grapple with have their origin in the biopsycho- duce, produce, produce — to be available to every-
social sphere, others are the result of overwork and body.”
stress, a scenario that inevitably results in strife at Hajela helps physicians vent their frustrations
home. One doctor Myers counselled sought help over a sick system, workforce issues, funding con-
because his son was addicted to heroin. Fearful of cerns and having to “operate according to evidence-
having “brilliant clinician, lousy father” carved on based decision making when the powers that be
his gravestone, he made some radical lifestyle function according to decision-based evidence mak-
changes to help improve the situation. Myers rein- ing.” He says there has been no change over the
forces that sometimes challenges can be a blessing in years in the prevalence of addiction; doctors face an
disguise and is encouraged by the fact that doctors 8%–9% risk of having a drug or alcohol-related
are seeking help at an earlier stage in life. problem in their lifetime. Marital discord is also a
In Ontario, the number of physicians seeking major problem among physicians, mainly because
help is increasing, according to Dr. Michael Kauf- doctors have a need to control and high expectations
mann, medical director of the Ontario Medical of themselves and their families, says Hajela. “The
Association (OMA) Physician Health Program, standing joke is that every physician needs a good
although this may be secondary to promotional wife, even the female physicians, to look after the
efforts in certain geographic areas. There were about home front.”
150 calls in 2001, a number that was surpassed in However, the traditional role of the doctor has
2002. The “program designed by physicians, for changed over the years, with younger doctors not
physicians” provides intervention coordination, working as many hours, more likely to look after
referral for assessment and treatment, recovery themselves and desiring a more balanced life. Al-
monitoring and advocacy. though it raises staffing issues, it is a healthy trend,
Doctors are worried by lack of resources, and “the he says. He also sees more support for doctors to
pressure on doctors’ time is seen to be adding to the come forward, both on a personal and organiza-
stress, leaving less time to look at health mainte- tional level, and a slight lessening of stigma. Hajela
nance activities,” says Kaufmann. About one-third says efforts must now focus on breaking down
of calls to the Ontario program are addiction related, silos between different specialties, improving com-
and the remainder are psychiatric. He notes that, re- munication, further decreasing stigma and boost-
cently, there has been an increase in calls about gam- ing education and resources in the area of physi-
bling. Although he sees a continuing stigma when it cian support.
comes to seeking help, he also sees a greater willing- “Healthy doctors are more productive and less likely
ness by interest groups to discuss physician health. to be disabled…It can be a win–win situation.”
Dr. André Lapierre has been director of the
Quebec Physician Support Program for 12 years. He
has also seen a steady rise in the number of calls, to Gillian Wansbrough,
about 200 annually. Since the early 1990s, about Medical writer, Toronto
6 CMA Guide to Physician Health and Well-BeingSelf
“Engrossed late and soon in professional cares … you may so lay waste that you may find,
too late, with hearts given way, that there is no place in your habit-stricken souls for those
gentler influences which make life worth living.” — Dr. William Osler, 1899
“If we don’t look after the health care of our providers, they can’t look after the health
care of [us].” — Commissioner Roy Romanow, Royal Commission on the Future of Health
Care in Canada, August, 2002
The fact that it is important for practising physicians to effectively manage the pro-
fessional and personal stressors associated with being a doctor has been emphasized
only recently. The need for physicians to maintain their own health and well-being
and thereby maximize their ability to provide quality health care to patients is now
considered extremely important. Although many sources of stress are inherent to
any demanding profession, the current medical practice environment is creating new
demands on physicians that place their health and well-being, and that of their fami-
lies, at increased risk. It has also been recognized that specific challenges face female
physicians and medical students and residents. With recognition of these problems
and challenges has come an understanding that physicians need to monitor their
own health and strive to adopt healthy lifestyles.
Being a physician can be harmful to your health
The very traits that make good physicians make bad we’re sick, these traits threaten us. We’re uncoopera-
patients, delegates attending the 2002 AMA/CMA tive patients.”
International Conference on Physician Health in Add the risk factors that go along with medical
Vancouver heard time and again. practice — sleep deprivation, excessive work and
Many physicians have compulsive personality patient demands, potential litigation, witnessing
traits, says Dr. David Dodd, director emeritus of trauma and human suffering, and job dissatisfaction
the Tennessee Physician Health Program. These — and the conclusion is clear, according to William
include a restricted ability to express warm and ten- Swiggart, a counsellor at the Vanderbilt University
der emotions; perfectionism; insistence that others Medical Center in Nashville. “Being a physician is
submit to one’s way of doing things; excessive de- harmful to your health.”
votion to work and productivity, to the exclusion Organizers of physician health and wellness pro-
of pleasure and interpersonal relationships; and in- grams must consider the reality that physicians make
decisiveness and chronic self-doubt. Dodd says lousy patients and that physicians are not health-
80% of physicians have 3 of these 5 traits; 20% maintenance oriented, says Tighe. “Our identity is as
have 4 of 5. Excessively high standards result in healers and fixers, not as preventers of symptoms.”
feelings of shame and guilt for not being good Physicians dread being patients because they feel
enough, even for being ill. helpless and vulnerable, she adds. “They do want to
“These traits keep us conscientious and are re- be taken care of, but feel guilty at accepting care and
inforced by education,” says Dr. Patti Tighe, head shame for needing it.” Accordingly, physicians tend
of the Physician Health Committee at Northwest- to be overcontrolling and noncompliant patients,
ern Memorial Hospital in Chicago. “But when and as a result, they often get poor quality, on-the-
Facts, advice and resources for Canadian doctors 7fly care from col- This is why physicians need special programs;
Today’s physician leagues. A survey of unfortunately, there has been a traditional stigma
health programs, 795 physicians (re- around seeking help. One reason may be because
sponse rate 34%) in early physician intervention programs often focused
which include early the province of Bar- on alcohol and drug abuse, and resulted in pro-
identification, celona, Spain, found bation or loss of licence. John Ulwelling of the US
intervention, that 33% had pro- Foundation for Medical Excellence cited an example
evaluation, vided abnormal care to of the enormous stigma and stress associated with
their colleagues, 39% probation: of the 40 Oregon physicians on proba-
treatment and reported that their tion in 1976–77 when there were virtually no treat-
long-term colleagues were very ment programs, 8 committed suicide and 2 others
monitoring, have difficult to care for, attempted to kill themselves. The attitude among
34% feared not acting professional medical associations was that impaired
impressive success correctly and 86% physicians should have “their licences ripped off the
rates. About 90% didn’t charge for the wall.” In short, Ulwelling said, “we had a mess.”
of all physicians consultation. Slowly, things started to change. Treatment pro-
Physicians live lon- grams opened, and physicians gained expertise in
return to practice.
ger than other profes- treating their colleagues. Today’s physician health
sionals1 — on average, programs, which include early identification, inter-
73 years compared with 70.9 years — but that vention, evaluation, treatment and long-term moni-
doesn’t mean they’re immune to illness. “The popu- toring, have impressive success rates. About 90% of
lar myth is that physicians don’t get sick and when all physicians return to practice, says Ulwelling.
they do, it’s a rare disease,” says Dr. Olaf Aasland, These programs usually meet the needs of phy-
director of the Norwegian Medical Association sicians who are physically or mentally ill, including
Research Institute. A survey of Norwegian physi- those who violate sexual boundaries, who mispre-
cians found that 80% reported being ill in the pre- scribe classified drugs, who are disruptive or who
vious year, and the most common illnesses were suffer from mood disorders (unipolar depression
influenza (36.8%) and respiratory tract problems and bipolar illness most commonly go unreported).
(24.6%). But the leading causes of illness requiring The new challenge, said Ulwelling, is to prevent
more than 2 weeks’ sick leave were burnout and problems in the first place through promotion of
depressive disorders. physician well-being. We need to reach a “larger
“It’s difficult for physicians to take the role of number of physicians who have been greatly
patient when necessary,” says Aasland, since they are discombobulated by the enormous changes in
generally reluctant to access health resources. The health care in the past 15 years.”
Spain survey also found that 49% of respondents had Physicians today are at a particularly high risk of
no family physician and only 52% had a clinical his- overwork, burnout and more serious impairment.
tory with a family physician. Of those who did seek Restructuring, financial constraints, a growing and
help, only 48% of respondents said they followed aging population and the acceleration of informa-
their FP’s instructions. Meanwhile, 82% said they tion technology all mean that “increased demands
self-prescribed and 6% had self-treated stress with are falling on the backs of [physicians] for increased
medication. Their record in preventive medicine was productivity, documentation, vigilance to prevent
also poor: 47% reported having no periodic health error and mastery of expanding areas of knowledge
test and 41.5% didn’t have up-to-date vaccines (11% and technology. The load we are carrying increas-
of physicians’ children were in the same state). ingly exceeds our carrying capacity,” says Ulwelling.
“Doctors are trained to be on one side of the
Reference
bed or desk,” said study coauthor Dr. Antoni Arte-
1. Frank E, Biola H, Burnett CA. Mortality rates and causes among
man of the Barcelona Medical Association. “They U.S. physicians. Am J Prev Med 2000;19:155-9.
refuse to act like patients … they refuse to follow
medical procedures or recommendations that they Barbara Sibbald,
don’t agree with.” Medical journalist, CMA
8 CMA Guide to Physician Health and Well-BeingBurnout — “an erosion of the soul”
Burnout caused by professional stress and and early life experiences such as conditional love,
demanding workloads may be affecting management of stress is individual.
nearly half of all physicians, a recent study “No one thing will work for everyone,” says
indicates. Boudreau. However, the strategy many physicians
“Burnout’s natural home is in the caring pro- adopt is avoidance — they leave their jobs, cut back
fession,” says Robert Boudreau, a Faculty of Man- on hours or change employment.
agement professor at the University of Lethbridge Physician burnout is characterized by emotional
and author of a 2002 study of Alberta physicians. exhaustion, cynicism, perceived clinical ineffective-
Preliminary results from the survey of 1161 phy- ness and a sense of depersonalization in relationships
sicians (response rate 17.6%) indicate that 48.6% with coworkers, patients or both. Burnout has been
are in the advanced stages of burnout as measured linked to impaired job performance, irritability and
by the Modified Maslach Burnout Inventory. By marital difficulties. It has also been associated with
comparison, 31% of Alberta nurses and 32% of US poor health — including headaches, sleep distur-
physicians (sample size of 216 physicians) are in this bances, fatigue, hypertension, anxiety, depression
advanced stage of stress. and myocardial infarction — and may contribute to
Boudreau defines burnout as a situation where alcoholism and drug addiction.2 More poignantly,
the demands at the workplace tax or exceed individ- burnout has been described as “an erosion of the
ual resources — the way of life for many physicians soul”3 that results from the dislocation between what
whose medical practices are increasingly complex people are doing and what they are expected to do.
and demanding. Nearly two-thirds of Canada’s Preventing burnout by promoting physician
physicians (64%) have a workload they consider too well-being is the impetus behind two new US ini-
heavy and more than half (58%) say their family tiatives. The Joint Commission on Accreditation of
and personal life has suffered because they chose Healthcare Organizations now calls for a “process”
medicine as a profession, according to CMA’s 2001 to address physician well-being that is separate from
Physician Resource Questionnaire.1 In addition, disciplinary processes. Another initiative comes
• 57% said patients’ expectations are unreasonably from the Accreditation Council of Graduate Med-
high, ical Education (ACGME), which is restricting the
• 29% said they are on call too often, number of hours residents can work to a maximum
• 33% said a lack of locums affects their ability to of 80 per week.
take vacations, But restricting the hours of work may actually
• 64% said it is difficult to get appropriate re- increase stress “if the expectations are the same but
sources on behalf of patients and there are fewer hours,” argues Dr. Eric Endean,
• 46% said the opportunities to change specialty chief of surgery at the University of Kentucky in
or career path are limited. Lexington. In a pilot study involving university
Despite evidence pointing to high levels of profes- teaching programs in Kentucky, Georgia and
sional stress, physicians have no advantage over the Michigan, surgical residents identified their top
general population, where less than one-quarter of stressor as ineffective use of time (average 3.56 on a
people know how to cope with stress. scale of 1 to 5); their top priorities were family
“Excess stress can lead to illness,” says Dr. Patti (27%) and career (19%). These findings, says
Tighe, head of the Physician Health Committee at Endean, are consistent with burnout. “Decreasing
Northwestern Memorial Hospital in Chicago. And work hours is not the solution. Fatigue may not be
because stress is exacerbated by genetic predisposi- the most important cause of stress.”
tion, personality traits, mood (especially depression) What is needed, he says, is education about how
Facts, advice and resources for Canadian doctors 9to cope with stress. Although Endean cites a US report burnout.4 The likelihood of burnout in-
study of 540 residents in which more than 300 creased 12%–15% for each additional 5 hours
reported high stress, he acknowledges that medical worked above 40 hours per week.
training currently offers little to help residents
cope. Accordingly, an “unhealthy response” such as References
depression, drug dependency, divorce, rage, self- 1. Martin S. Interest in alternative forms of payment on the rise:
destructive behaviour or burnout may result. Pre- CMA survey. CMAJ 2001;165:626.
2. Spickard A Jr, Gabbe SG, Christensen JF. Mid-career burnout in
liminary results from a pilot study in which resi- generalist and specialist physicians. JAMA 2002;288:1447-50.
dents take seminars on time management, stress 3. Maslach C, Leither MP. The truth about burnout. San Francisco:
management and goal setting indicate that such Josey-Bass Publishers; 1997; p. 13-5.
4. Linzer M, Konrad TR, Douglas J, McMurray JE, Pathman DE,
education is effective. Williams ES, et al. Managed care, time pressure, and physician job
Female physicians who are balancing the de- satisfaction: results from the physician worklife study. J Gen Intern
Med 2000;15:441-50.
mands of work, child care and domestic manage-
ment are also vulnerable to burnout. According to
the US Physician Worklife Study, female physicians Barbara Sibbald,
are 60% more likely than their male colleagues to Medical journalist, CMA
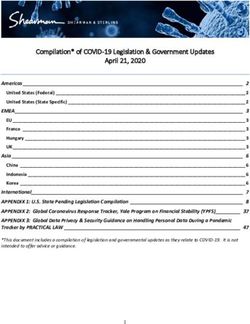
Personal strategies for preventing burnout
Influence happiness through personal values and choices
Self-awareness
Spend time with family and friends
Spend time on religious or spiritual activities
Take care of yourself (nutrition, exercise, sleep)
Adopt a healthy philosophical outlook
Find a supportive spouse or partner
Attend stress workshops, crisis counselling or coaching
Work strategies for preventing burnout
Control your environment and workload
• Shared call
• Flextime or job redesign
• Build your team
Find meaning in work and set limits
Find a mentor
Have adequate administrative support systems
Advice on preventing burnout from Dr. Anderson Spickard Jr., Vanderbilt
University Medical Center in Nashville, and Robert Boudreau, University
of Lethbridge Faculty of Management
10 CMA Guide to Physician Health and Well-BeingThe health of women physicians
As more women enter the practice of Baseline Survey,7 which drew its data from responses
medicine in Canada, there is an ever- of physicians in 2 regions of Ontario, showed that
increasing interest in how this unique female physicians were slightly more likely than
group compares with other women, women in male physicians (57% v. 41%) to have seen their
other professions and male physicians. There is also family physician within the previous year and to
a growing need to address professional and health- have engaged in exercise or a physical activity at
related issues that are unique to this group. For least once weekly (88% v. 77%).7
example, the stresses associated with balancing the
Roles as mother and spouse
responsibilities of spouse, mother and physician
may adversely affect female physicians’ mental Spouses and children are an integral part of the lives
health. It is important to monitor trends among of many female physicians, despite the stresses as-
female physicians and increase awareness of health- sociated with balancing family and career respon-
related issues so that wellness strategies and disease sibilities. According to Statistics Canada, in 1992,
prevention programs can be established for this women who were employed full time and whose
growing group of health care providers. youngest child was under the age of 6 spent an aver-
age of 5.4 hours per day on child care and domestic
What the studies reveal
work.8 The same census data indicated that women
The Women Physicians’ Health Study1-3 is a cross- in the workforce lost 6 days of paid work per year
sectional questionnaire-based survey of women due to family and personal responsibilities, whereas
physicians, aged 30 to 70 years, selected from the men lost 1 day per year. Most surveys of women in
American Medical Association’s Physician Master- medicine confirm that the division of labour is sim-
file. Women made up 19.4% of practising phy- ilar to the norms for Canada.
sicians in the United States in 1994, 24% in 2000, In her book Fruitful,9 Anne Roiphe explores the
and it is projected that, by the year 2010, women contradictions that “middle- and upper-class moth-
will comprise 29.4% of the physician workforce.4 In ers who have education and professions” live. She
2002, 29.8% of physicians in Canada were states that after 30 years of “feminist consciousness,”
women.5 By 2021, it is believed that women will we know that paid work outside of home is essential
make up approximately 43.5% of the physician for a woman’s self-esteem, income and marriage. At
workforce in Canada.6 the same time, however, most women still measure
Women in the Women Physicians’ Health Study their worth, to some extent, on their ability to care
reported healthy personal habits that exceeded for their families. Women, more than men, look to
national health-behaviour goals. 2 The fact that family for affirmation. However, it is a challenge to
health-conscious behaviours were correlated with care for vulnerable family members, raise children
self-reported prevention-related counselling and and succeed professionally within the contexts of
screening practices led the researchers to argue that the “traditional” family unit. Women who work
“if we value disease prevention, and if physicians’ outside of the home often feel that they must “pay
personal health practices are consistent predictors of for” the privilege of having both a successful career
their likelihood to be more active preventionists, we and a supportive family. Many worry that their hard
ought to try to cultivate healthy physicians.”3 work and varied commitments, which often take
Some studies indicate that female physicians them away from their families, may harm the chil-
may also be more health conscious than their male dren they innately want to protect. Roiphe de-
counterparts. Results of the 2001 OMA Physician scribes some of the conflicting emotions of a work-
Health Program’s Physician Resource Network ing mother:
Facts, advice and resources for Canadian doctors 11“I want to warn her of this and that. I try. She pays physicians — women leading women”). Other
no attention to me. I want to follow her around, re- mentorship programs, particularly on the Internet,
mind her to eat well, to sleep enough. I try. She smiles might be developed in other provinces to help
at me. I know that I should pay attention to my own women deal with some of the challenges they face.
waiting work. ... I am a mother feminist. I ask myself The Canadian Medical Association currently
if that is a contradiction…”9 p. 232 provides physician support through a joint AMA/
CMA International Physician Health Conference,
The pressures many women feel to be the “perfect and several of the provincial divisions are conduct-
mother” and the “best doctor” indicate a need to ing their own wellness initiatives as well. For a list
continue to modify our expectations. This is not to of the resources currently available to physicians in
say that male physicians do not struggle with dual Canada see page 27.
roles as well, but there are particular pressures for The importance of awareness to the prevention
many women that cannot be ignored. of health-related problems cannot be overstated.
The stigma of mental illness is felt keenly, even
Mental health of women physicians
among physicians, but we must begin among our-
An alarming study with respect to women phy- selves the difficult task of speaking about the
sicians’ mental health, conducted by North and unique stresses we face in our lives as physicians.
Ryall, reported that more than half of women phy- We must do this as we exercise, read, knit, write,
sicians may experience a psychiatric illness during reflect and laugh. We must look for time for each
their lifetime.10 Depression rates were high, and other and time for ourselves. We must continue to
suicide rates were alarmingly high. Similarly, in a practice what we preach.
systematic review of original articles of population-
References
based studies, Lindeman et al11 report the relative
1. Frank E. The Women Physicians’ Health Study: background, ob-
risk for suicide mortality in female physicians to be jectives, and methods. J Am Med Womens Assoc 1995;50(2):64-6.
2.5–5.7 and in male physicians to be 1.1–3.4, as 2. Frank E, Brogan DJ, Mokdad AH, Simoes EJ, Kahn HS, Green-
compared to the general population. These data berg RS. Health-related behaviors of women physicians vs other
women in the United States. Arch Intern Med 1998;158(4):342-8.
highlight the need to address physicians’ stress and 3. Frank E, Rothenberg R, Lewis C, Belodoff BF. Correlates of
mental health issues more effectively. physicians’ prevention-related practices. Findings from the
Women Physicians’ Health Study. Arch Fam Med 2000;9:359-67.
Ann Davidson, who recently studied the health 4. AMA Physician Masterfile. Chicago: American Medical Associa-
of women physicians in Ontario, notes that women tion; 2001.
5. CMA Masterfile. Ottawa: Canadian Medical Association; 2002.
in medicine feel “the additional stress of working 6. Newton S, Buske L. Physician resource evaluation template: a
within a vocation that has tended to uphold pro- model for estimating future supply in Canada. Ann RCPSC
1998;31(3).
fessional achievement and scientific mastery over 7. Brewster JM. Ontario Medical Association Physician Health Pro-
personal, family, and relationship needs,”12 and she gram Physician Resource Network. Baseline Survey. Toronto:
underlines the importance mentors can play as a Ontario Medical Association; 2001.
8. Statistics Canada. Household activities recent trends. General
source of support. The loneliness and isolation that Social Survey. Ottawa: Statistics Canada; 1992. Available:
many women physicians experience in the pursuit www.statcan.ca/english/freepub/92-125-GIE/html/hou.htm (ac-
cessed 17 Dec 2002).
of their careers can have a significant impact on 9. Roiphe A. Fruitful: living the contradictions: a memoir of modern
their mental health, and mentors can help them to motherhood. New York: Penguin; 1997.
10. North CS, Ryall JE. Psychiatric illness in female physicians: Are
cope. high rates of depression an occupational hazard? Postgrad Med
1997;101:239-40.
A plan for prevention 11. Lindeman S, Laara E, Hakko H, Lonnqvist J. A systematic review
on gender-specific mortality in medical doctors. Br J Psychiatry
A study similar to the US Women Physicians’ 1996:168:274-9.
Health Study might well be considered in Canada. 12. Davidson A. Examining the health of women physicians in
Ontario: a Physician Health Program perspective. Ont Med Rev
With more information about the health problems 2002;69(7):24-6. Available: www.oma.org/pcomm/OMR
faced by women in medicine, specific wellness and /jul/02maintoc.htm (accessed 27 Nov 2002).
disease prevention programs could be developed,
both locally and nationally. The Ontario Medical
Association now has an electronic mentorship pro- Dr. Gail Beck,
gram for medical women (“Physicians leading Director, Office for Women in Medicine, CMA
12 CMA Guide to Physician Health and Well-BeingA resident’s perspective on well-being
We’ve all heard the stories, the ones that trol over their lives and livelihoods during residency
begin with “back when I was a resident” training. Long work hours at the hospital coupled
or “you think you have it bad?” Inevitably, with educational commitments after hours result in
these lines are followed by descriptions of 1-in-1 call reduced personal time. This may result in poor self-
for months on end, taking call while hooked up to care, strained relationships, feelings of inadequacy
an intravenous pole or completing residency with- and other sequelae.
out ever going on vacation. With these descriptions Why are so many residents unwell? What is so
of the ‘normal’ level of commitment required to stressful about residency? Although it may seem
become a good doctor, it is easy to understand why trite to point out that residency is particularly stress-
many residents believe they have to give up all other ful, it is important to remind ourselves why this is
activities while in residency training. Many estab- the case.
lished physicians also report that although this • The supervisor–trainee relationship is fraught
intensive training may have been the cause of their with stressful points including continuous evalua-
depression, inability to relax or failed marriage, such tions and issues of intimidation and harassment.
training was in fact required to make them good • Financial burdens: It is not uncommon for resi-
doctors. dents to begin their training owing more than
If this type of training is necessary to become a $100 000.
doctor, we should ask Health Canada to place • Information explosion: knowledge is doubling
signs on the doors to medical school: “Warning: every 5 years, so what we as residents are learning
medicine can be hazardous to your health.” at the beginning of our training may no longer
Despite increasing awareness of the effects an un- be true when we complete the program.
balanced lifestyle can have, stress-related morbidity • Physician shortages: Because almost every com-
among residents and other physicians remains high. munity needs more doctors, new graduates are
Studies continue to report the complications of walking into overfilled, highly demanding, stress-
stress, such as burnout, depression and other psy- ful practices.
chiatric morbidities, at much higher levels in physi- • Patient acuity: As the practice of medicine
cians than in the general public and other profes- changes and more care is provided outside of the
sionals.1 Alarmingly, even higher rates of depression hospital, patient acuity in the hospitals where
are reported among residents.2–5 In addition, all residents train increases.
physicians, by virtue of their profession, are at a • Career choices: To get into their program of
much greater risk for suicide.6 choice, medical students are being forced to
But many physicians continue to turn a blind eye choose the right electives so they will be compet-
to the facts. Some still believe that their colleagues itive in their chosen area. However, if they realize
do not get sick — that mental illness is someone’s they have not made the right choice of specialty,
fault or a weakness of character. Their perceptions it is now harder than ever to change career paths.
keep doctors in denial of the fact that current prac- Although many trainees before us have gone
tice and training standards are not healthy. It is time through residency and survived, there is a cost asso-
to break the code of silence and admit that physi- ciated with the endurance required to make it
cians do get sick. Only then can we begin to remove through. It is time to change the system from a
the stigma and make our profession well. “survival of the fittest” philosophy to an environ-
ment that nurtures intelligent people and produces
Cause for concern: resident-specific issues
competent, well-balanced physicians. Residency
Residents may perceive that they have minimal con- should be some of the best years of your life. It
Facts, advice and resources for Canadian doctors 13should also be the idents, as they become established doctors, work to
beginning of a fulfill- maintain the healthy balance between work and
ing career — a career home life that they struggled to cultivate during
that challenges but their training.
also allows for inter-
The shift toward increased balance
ests outside of the
profession. The good news is that medical culture is slowly
Unfortunately, the beginning to change, and a strong voice in the
very design of resi- push for change is coming from new doctors.
dency programs en- With each new cohort of residents, interest in
sures that by the end finding a healthy balance between work and per-
of training a percent- sonal time increases. It is encouraging that many
age of graduates will of today’s residents believe you can be a good doc-
be stressed, burned tor and be a dedicated pianist or potter. In fact,
out, depressed or you might even be a better doctor and person
abusing substances. because of it.
In addition to the Residents have been leaders in the field of physi-
stressors associated cian health and advocates for change. Students and
with the 25- to 40- residents were the first to publish position papers
year-old demogra- on well-being and to put the issue at the forefront
Dr. Laura Musselman
phic, residents must of their organizations’ mandates. Resident associ-
contend with 2 additional sets of stressors.7 The ations have made it a priority to inform residents
first relates to the inherent characteristics, which and their families about wellness issues and have
on one hand make them excellent medical developed programs aimed at promoting balanced
school candidates, but on the other put them at lifestyles and overall physician health.
an increased risk for the sequelae of poor stress Contracts are one way of changing the current
management. These include chronic self-doubt, culture. Provincial housestaff organizations across
ability to delay gratification indefinitely and the country have successfully negotiated changes to
need for perfection and control. The second set collective agreements. Contractual provisions limit-
of stressors is systemic in nature; these training- ing maximum hours of work and workload have
related stressors can be classified into 3 main been critical in ensuring some balance in residency
categories: training. However, contracts can only provide the
Biological: Long work and study hours lead to legal framework for potential protection. It is es-
sleep deprivation, poor eating habits and a low sential that the hospitals that negotiate these con-
level of fitness. tracts mandate that the terms be enforced from the
Situational: Stressors include isolation (from fam- top down.
ily, friends and colleagues), limited time for re- The examples of healthy lifestyles that residents
laxation and entertainment, patient care issues have set are beginning to make established phy-
(e.g., inadequate support from allied health sicians reflect on their current situations. They
professionals, difficult patients, complex presen- have begun to acknowledge that how they trained
tations) and financial issues. and how they practice may not be the best. Med-
Professional: Including poor trainee–supervisor ical organizations, including the Canadian Med-
relationships, occupational hazards (e.g., blood ical Association, have recently made it a priority to
borne infections, violent patients), balancing further educate physicians about these issues and
the role of service provider, educator and to promote prevention and treatment options.8
learner (dealing with excessive work loads cou- To help residents and their families stay healthy,
pled with nonoptimal learning conditions) and many resources have been made available to resi-
career planning issues. dents through their provincial housestaff organiza-
Of course, once residents finish residency, more tions. These include, but are not limited to:
challenges await them. It is important that res- • support lines including a 24-hour helpline
14 CMA Guide to Physician Health and Well-Being• family doctor referral lists priority and begin to incorporate healthy styles of
• social events to meet other residents, decrease learning into the curriculum so that the current
isolation and increase morale among coworkers unhealthy socialization process in medicine is
• resource materials for partners and residents stopped. Residents will continue to be involved on
(books, videos, support group access) the front lines to ensure that the practice of med-
• selected expert speakers in the area of physician icine becomes a healthier endeavour, not only for
health patients, but also for physicians.
• financial planning seminars
References
• extended disability insurance coverage
1. Ramirez, AJ, Graham J, Richards MA, Cull A, Gregory WM.
Although these services are helpful, we also need Mental health of hospital consultants: the effect of stress and satis-
systemic structural and cultural changes in the faction at work. Lancet 1996;347:724-8.
practice of medicine, for both residents and estab- 2. Firth-Cozens J. Depression in doctors. In: Robertson MM,
Katona CLE, editors. Depression and physical illness. Chichester
lished physicians. Without a shift in the current (UK): John Wiley and Sons; 1997. p. 95-111.
paradigm, even the best intentions will fail. A more 3. North CS, Ryall JE. Psychiatric illness in female physicians. Are
high rates of depression an occupational hazard? Postgrad Med
appropriate structure must be developed that will 1997;101(5):233-42.
allow people to live balanced lives. Recommen- 4. Reuben DB. Depressive symptoms in medical house officers:
effects of level of training and work rotation. Arch Intern Med
dations from other organizations include: group 1985;145:286-8.
practice, job sharing, more flexible payment mech- 5. Valko RJ, Clayton PF. Depression in internship. Dis Nerv Syst
1975;36:26-9.
anisms, shared call, ‘stop-clock’ or slowed promo- 6. Lindeman S, Läärä E, Hakko H, Lonnqvist J. A systematic review
tion tracks and mentoring networks. For more on gender-specific suicide mortality in medical doctors. Br J Psy-
practical tips, see Peterkin8 and information pro- chiatry 1996;168:274-9.
7. Gautam M. Depression and anxiety. In: Goldman LS, Myers M,
vided on provincial housestaff organizations’ Web Dickstein LJ, editors. The handbook of physician health: the essential
sites (find links through www.cair.ca). guide to understanding the health care needs of physicians. Chicago:
American Medical Association; 2000.
Healthy doctors — the profession’s future 8. Hanson D. Inaugural speech. Canadian Medical Association
Annual Meeting. Saint John, NB. 2002 Aug 21.
9. Peterkin A. Staying human during residency training. Toronto:
“…some level of impairment to residents is a common University of Toronto; 1998.
and predictable sequelae to the time they spend at 10. Levey RE. Sources of stress for residents and recommendations for
programs to assist them. Acad Med 2001;76(2):142-50.
traditionally ‘catastrophic levels of stress’…”10
It is time to ensure that observations like this are Dr. Laura Musselman,
no longer valid. We must make wellness issues a General surgery resident
Facts, advice and resources for Canadian doctors 15Service
A number of effective strategies and programs exist to promote physician health
and to help physicians in need of assistance. Research is ongoing to help define the
stressors facing physicians and their families in today's environment and to identify
the most effective treatment strategies. Across Canada, assistance programs have
been established that offer a variety of preventive and treatment services to phy-
sicians and their families. These programs deal with a variety of psychological and
family issues, as well as problems related to addictions, stress and burnout.
Canadian physician health programs: an overview
In the last few decades, throughout North America, offering a range of services to doctors, trainees
the physician health initiative has been evolving. One and their families based on available community
element of that initiative has been the development resources (BC, Manitoba, Ontario, Quebec,
of physician support programs, often known by the Nova Scotia, Newfoundland and Labrador)
name Physician Health Program, amongst others. In • Professionally staffed, comprehensive program
the US, these programs began as committees made based upon an employee assistance program mod-
up of volunteer doctors who had sometimes experi- el that utilizes a professional counselling service
enced personal problems themselves, usually drug or along with other resources (Alberta and Yukon)
alcohol addiction, and who wanted to help their col- Where physician support committees still exist, such
leagues. Many of those volunteer-based committees as the Saskatchewan Physician At Risk Committee of
have grown into robust and comprehensive services the Saskatchewan Medical Association, volunteer
for doctors. The same thing is happening in Canada. members help colleagues suffering from drug, alcohol
Today, doctors call their provincial support pro- or other personal problems by reaching out to them
grams for a variety of reasons beyond drug and alco- in a personal way. They will meet with a doctor in
hol problems. These include stress and burnout, their own home or office, often sharing their own
psychological disorders, family and relationship experience and strength in a manner that only some-
problems, medico-legal problems and much more. one who has “been there” can understand.
Confidential Canadian physician support pro- The Physicians at Risk Program of the Manitoba
grams exist in every province, in some form, to serve Medical Association continues to make use of peer
the more than 1500 callers nationwide in need of volunteers and also employs a physician coordinator
help each year. These programs are similar in many on a part-time basis. One of the particular strengths
ways, and at the same time, as diverse and innovative of the Manitoba program is its support group, avail-
as the people and organizations that have created able to spouses of doctors in recovery from drug
them. Three basic models can be identified to de- and alcohol problems.
scribe Canadian programs: The Physician Support Program (PSP) of British
• Volunteer committees providing peer support Columbia is an example of a program that is jointly
(Saskatchewan, New Brunswick, PEI) funded by the regulatory body (College of Phy-
• Professionally staffed, comprehensive programs sicians and Surgeons of British Columbia) and the
16 CMA Guide to Physician Health and Well-BeingYou can also read