Patients with Post-COVID-19 Vaccination Myocarditis Have More Favorable Strain in Cardiac Magnetic Resonance Than Those With Viral Myocarditis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Patients with Post-COVID-19 Vaccination Myocarditis Have More
Favorable Strain in Cardiac Magnetic Resonance Than Those With
Viral Myocarditis
Danish Vaiyani ( Vaiyanid@chop.edu )
Children’s Hospital of Philadelphia
Matthew D. Elias
Children’s Hospital of Philadelphia
David M Biko
Children’s Hospital of Philadelphia
Kevin K Whitehead
Children’s Hospital of Philadelphia
Matthew A Harris
Children’s Hospital of Philadelphia
Sara L Partington
Children’s Hospital of Philadelphia
Mark A Fogel
Children’s Hospital of Philadelphia
Research Article
Keywords: Myocarditis, Cardiac Magnetic Resonance, COVID-19, Pediatric, Vaccination
Posted Date: January 12th, 2023
DOI: https://doi.org/10.21203/rs.3.rs-2460008/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
Page 1/15Abstract
Introduction
There have been reports of myocarditis following vaccination against COVID-19. We sought to describe cardiac magnetic resonance
(CMR) findings among pediatric patients.
Methods and Results
Retrospective review at a large academic center of patients clinically diagnosed with post-vaccine myocarditis (PVM) undergoing CMR.
Data collected included parametric mapping, ventricular function and degree of late gadolinium enhancement (LGE). Post processing
strain analysis was performed using tissue tracking. Strain values, T1/T2 values and ventricular function were compared to age-and
gender-matched controls with viral myocarditis using a Wilcoxon Signed Rank test.
Among 12 patients with presumed PVM, 11 were male and 11 presented after the second vaccination dose, typically within 4 days. All
presented with chest pain and elevated troponin. 10 met MRI criteria for myocarditis. All had LGE typically seen in the lateral and
inferior walls; only five had prolonged T1 values. 10 met criteria for edema based on skeletal muscle to myocardium signal intensity
ratio, and only 5 had prolonged T2 mapping values. Patients with PVM had greater short-axis global circumferential and radial strain,
right ventricle function and cardiac output when compared to those with viral myocarditis.
Conclusion
Patients with PVM have greater short-axis global circumferential and radial strains compared to those with viral myocarditis. LGE was
universal in our cohort. Signal intensity ratios between skeletal muscle and myocardium may be more sensitive in identifying edema
than T2 mapping. Overall, the impact on myocardial strain by CMR is less significant in PVM compared to more classic viral
myocarditis.
Introduction
Following the Food and Drug Administration’s Emergency Use Authorization (EUA) for the Pfizer-BioNTech BNT1262b2 mRNA vaccine
in December 2020, scattered reports emerged of myocarditis temporally associated with vaccine administration. This finding was also
reported in the pediatric population after the EUA was extended to patients above age 12 in March 2021.1–14
While there are multiple studies detailing the clinical presentation and course of post-vaccine myocarditis, there is little in the way of
comparison of these findings with typical viral myocarditis. Cardiac magnetic resonance (CMR) has been used for years for the
diagnosis and management of myocarditis.15–19 However, detailed CMR data on tissue characterization and ventricular function
including strain is lacking, especially in the pediatric population. We hypothesized that vaccine myocarditis may have less effect on
ventricular function than routine viral myocarditis. The purpose of the current study was to retrospectively leverage granular CMR data
from a large volume academic institution (with consistent imaging protocols and interpretation methodologies for all patients) to
compare post-vaccine myocarditis with viral myocarditis.
Methods
This study was a retrospective chart review of patients who were clinically diagnosed with myocarditis after vaccination against
COVID-19. Inclusion criteria included age under 21 years and presenting within 30 days of a vaccination dose. Patients who presented
with an active viral infection were excluded. Each study subject was age (within 6 months) and gender-matched to a control patient
diagnosed with presumed viral myocarditis. Potential study subjects with cyanotic and/or symptomatic congenital heart disease,
cardiomyopathy, giant cell myocarditis or a plausible alternate explanation for presentation were not selected. Potential controls who
presented with fulminant myocarditis requiring extracorporeal membrane oxygenation, intubation or mechanical circulatory support
were excluded.
Cardiac magnetic resonance (CMR) for patients with suspected myocarditis include cine steady-state free precession imaging in the 4-
chamber, 2-chamber, ventricular short axis, and the left ventricular and right ventricular outflow tract views. Through-plane phase
contrast velocity mapping was performed at the aortic root and main pulmonary artery to also assess cardiac output and confirm
measurements of ventricular stroke volume. Gadobutrol was used for contrast enhanced imaging. Angiography including coronary
Page 2/15imaging was performed with inversion recovery gradient echo imaging using ECG gating with navigators for respiratory motion
adaptation. Multiparametric mapping was performed in the short axis projection in the basal, mid and apical views consisting of
Modified Look-Locker Inversion recovery sequences for T1 mapping, T2-weighted turbo-inversion recovery magnitude (TIRM)
sequences to assess signal intensity ratios of cardiac and skeletal muscle, and T2-prepared single shot steady state free precession
sequences for T2 mapping. Late gadolinium enhancement assessment was performed in the 4-chamber, long axis, and short axis
views using respiratory motion corrected magnitude and phase sensitive inversion recovery sequences.
Among 12 patients, 11 studies were performed on a 1.5 Tesla Siemens MRI system (Siemens Medical Solutions, Erlangen, Germany)
and 1 study was performed on a 3 Tesla Siemens MRI system. CMR analysis was performed using cvi42 software (Circle
Cardiovascular Imaging, Calgary, Canada). Per our center’s practice, native T1 values above 1070 ms were considered prolonged and
peak regional T2 values above 60 ms were considered abnormal for patients undergoing studies on a 1.5 Tesla scanner.20,21 Native T1
values above 1149 ms and peak regional T2 values above 62 ms were considered abnormal for studies performed at 3 Tesla.22 CMR
studies with evidence of both myocardial edema and non-ischemic myocardial injury were considered positive for myocarditis per
published guidelines.17 Strain analysis was performed with the tissue tracking technique using cines obtained in the short axis, four
chamber, two chamber and three chamber views.
Statistical analyses were performed using R version 4.0 (R Foundation, Vienna, Austria) and statistical significance was assessed at
the 0.05 level. Strain values, T1 values, extracellular volume, T2 values and ventricular function were compared to age- and gender-
matched controls with viral myocarditis using a Wilcoxon Signed Rank test. Spearman’s correlation test was used to determine
correlation between strain values, degree of late gadolinium enhancement and parametric mapping. Patient #4 was excluded from
correlation analysis between strain values and parametric mapping as their study was performed on a 3 Tesla MRI scanner. The study
protocol was approved by the institutional review board.
Results
Baseline Clinical Information
Among 12 patients with presumed post-vaccine myocarditis, 11 were male, ranging from 12 to 17 years old (median 15.5 years, IQR
13–18 years). No patients had a known history of COVID-19 infection. All patients received the BNT1262b vaccine, as the only COVID-
19 vaccine approved for this age group (Table 1) at the time of this study. 11 patients presented after their second vaccine dose, and 11
of 12 patients presented within 4 days of receiving the vaccine dose; the remaining patient presented 22 days later without any
intervening illness (median = 2.5 days, IQR 1.25–3.75 days). All patients presented with chest pain, and 7 presented with fever or
shortness of breath. Patients universally had an elevated troponin, often markedly elevated, and only three patients had mildly elevated
B-natriuretic peptide levels. Electrocardiogram (ECG) changes were present in 11 of 12 patients with the most common changes being
ST elevation in the inferolateral leads, typically corresponding to regions of late gadolinium enhancement on CMR. Echocardiograms
were performed on all patients at the time of admission. 10 patients had normal biventricular ejection. One patient (#6) had mildly
depressed left ventricular ejection that normalized two days later and one patient (#5) had mildly depressed left ventricular ejection that
was normal 7 days later. No patients had pericardial effusions or wall motion abnormalities.
Page 3/15Table 1
Study Patient Characteristics
Patient Age Gender Vaccine Vaccine Symptom Symptoms Peak Peak EKG Changes
(years) Given Dose Onset Troponin- BNP
I
1 12 M BNT1262b2 Second 3 days Chest Pain 5.87 118* T-wave inversion
(Pfizer) in inferior leads
2 16 M BNT1262b2 Second 1 day Chest Pain, 14.6 419* PR depression,
(Pfizer) Fever, Myalgias, Nonspecific T-
Malaise wave changes
3 13 M BNT1262b2 Second 1 day Chest Pain, 18.83 35 ST Elevation in
(Pfizer) Fever, Anterolateral and
Headache, Inferolateral
Nausea leads
4 17 M BNT1262b2 Second 2 days Chest Pain, 25.75 87 None
(Pfizer) Nausea
5 17 M BNT1262b2 Second 3 days Chest Pain 8.12 30.1 ST Elevation, PR
(Pfizer) Depression in
Inferolateral
Leads
6 15 M BNT1262b2 Second 1 day Chest Pain, 88.38 293.4 ST Elevation in
(Pfizer) Fever, Nausea Inferolateral
Leads
7 14 M BNT1262b2 Second 3 days Chest Pain, 1.95 < 10 Nonspecific T-
(Pfizer) Malaise, Fever, wave Changes
Nausea,
Myalgias
8 16 M BNT1262b2 Second 22 days Chest Pain 13.13 31 ST Elevation, T-
(Pfizer) wave inversion in
inferolateral
leads
9 17 F BNT1262b2 Second 2 days Chest Pain, 7.06 20.2 T wave inversion
(Pfizer) Malaise, Fever in inferior leads
10 13 M BNT1262b2 Second 2 days Chest Pain, 15.15 56.6 ST Elevation in
(Pfizer) Malaise, Fever Inferolateral
Leads, T wave
Inversions in
Inferior Leads
11 14 M BNT1262b2 First 3 days Chest Pain, 8.48 31.2 ST elevation in
(Pfizer) Malaise, Fever Inferolateral
Leads
12 16 M BNT1262b2 Second 4 days Chest Pain 22† not Sinus rhythm,
(Pfizer) drawn premature
ventricular
complex
* NT-proBNP with listed normal values < 125 pg/mL
† high sensitivity troponin level, with normal values listed as < 14 ng/mL
Troponin-I measured in ng/mL; BNP = Brain natriuretic peptide, in pg/mL
All 12 patients were admitted and were treated with supportive care consisting of nonsteroidal anti-inflammatory drugs. No patients
received corticosteroids or intravenous immunoglobulin. No patients required increased support such as inotrope infusion,
extracorporeal membrane oxygenation, or heart failure medications. All patients were discharged within 96 hours of admission.
There were 11 male and 1 female control patients, ranging from 13–17 years old (median 15.5 years, IQR 14-16.5 years). All patients
presented with chest pain while 9 of 12 had additional symptoms. (Table 2) All 12 patients were admitted and treated with supportive
care consisting of NSAIDs. 9 patients had normal ventricular function, 2 patients had mildly depressed function and 1 patient had
Page 4/15moderately depressed function. Two patients had wall motion abnormalities. 11 of 12 patients had abnormal EKGs. 7 of 12 patients
presented with ST elevation on EKG.
Table 2
Control Patient Characteristics
Patient Age Gender Symptom Symptoms Peak Peak EKG Changes
(years) Onset Troponin- BNP
I
1 13 M 2 days Chest pain, fevers, 45.96 1011.9 ST Elevation in anterolateral leads,
nausea, fatigue, nonspecific T wave changes
abdominal pain
2 16 M 1 day Chest pain, Recent 21.42 Not Nonspecific ST segment and T wave
gastrointestinal illness drawn changes
3 14 M 2 days Chest Pain 6.82 Not ST Elevation in lateral leads
drawn
4 17 M 1 day Chest pain, Nausea 12.23 93 Nonspecific T wave changes
5 17 M 1 day Chest pain, Fatigue 33.03 160.5 ST Elevation in inferior leads
*
6 15 M 2 days Fever, Dizziness, pre- 7.73 1233 Nonspecific T wave changes
syncopal symptoms
7 14 M 3 days Chest pain, Fever, 28.31 Not ST Elevation in lateral leads
Abdominal pain drawn
8 16 M 7 days Chest pain, Shortness 8.27 762.2 ST Elevation and T wave inversion in
of breath, Headache, lateral precordial leads, T wave
Fever inversion in inferior leads
9 17 F 1 day Chest pain 0.14 Not No abnormalities
drawn
10 14 M 1 day Chest pain 13.60 121.8 ST Elevation in inferior leads
11 14 M 10 days Chest pain, Headache, 23.99 36.7 Nonspecific ST changes
Nausea, Dizziness
12 16 M 2 days Chest Pain, Dizziness, 25.97 100.8 Diffuse ST segment elevation
Nausea, Headache
* NT-proBNP with listed normal values < 100 pg/mL
Troponin-I measured in ng/mL; BNP = Brain natriuretic peptide, in pg/mL
All control patients were discharged home within one week of admission. No patients received intravenous immunoglobulin or steroids,
nor did any patients require any mechanical circulatory support, endotracheal intubation or extracorporeal membrane oxygenation. All
control patients had normal ventricular function with no wall motion abnormalities at the time of follow up and none had disease that
progressed to dilated cardiomyopathy or chronic heart failure.
CMR Findings, Vaccine Myocarditis
CMR was obtained between 4 and 41 days after vaccine administration. (Table 3) Studies met criteria for myocarditis in 10 patients. All
patients had normal biventricular size and ejection fraction on CMR. Every patient met criteria for non-ischemic myocardial injury on the
basis of late gadolinium imaging (Table 4, Fig. 1–2). While the pattern of late gadolinium enhancement was heterogeneous in our
cohort, 9 of 12 patients had enhancement in the inferior or inferolateral wall at various levels (Table 4) and the remaining patients had
enhancement across the entire lateral free wall at varying short axis levels. Five patients (#4, 6, 8, 9, 11) also had a prolonged global
native T1 time; three patients had a global ECV of 30% or greater. However, six of nine patients with a global ECV less than 30% had
regional elevation of the ECV.
Page 5/15Table 3
Cardiac Magnetic Resonance Imaging Findings
Patient Vaccine Global Global Hematocrit Global Global Peak TIRM Ratio* RV LV Cardiac
to CMR Native Contrast ECV PC T2 EF EF Output
T1 Enhanced Base Mid Apex
T1
1 15 days 1010 388 ms 37% 27%§ 44% 63.0 2.5 2.0 2.1 70% 80% 4.0
ms ms
2 18 days 1016 498 ms 49% 25% 49.5% 52.5 3.3 3.6 3.0 67% 69% 4.8
ms ms
3 4 days 1062 447 ms 40% 30% 50% 63.0 2.8 2.3 2.8 66% 74% 4.9
ms ms
4† 6 days 1267 552 ms 44% 23% § 42% 47.2 1.8 4.4 4.2 56% 86% 3.7
ms ms
5 7 days 1003 415 ms 44% 22% 39% 50.4 1.3 1.6 2.1 63% 67% 4.7
ms ms
6 6 days 1201 463 ms 37% 33% 54% 66.0 2.0 2.3 2.9 58% 59% 4.1
ms ms
7 9 days 1022 491 ms 39% 28% § 46% 47.0 1.8 1.8 2.0 71% 76% 4.6
ms ms
8 26 days 1100 427 ms 43% 30% 52% 62.0 0.6 1.9 4.1 58% 61% 4.1
ms ms
9 41 days 1293 441 ms 40%‡ 28% § 45% 46.0 1.1 1.4 1.1 65% 66% 2.4
ms ms
10 4 days 1033 475 ms 41% 28% § 50% 55.0 2.0 1.8 1.7 72% 78% 5.9
ms ms
11 6 days 1089 425 ms 34% 27% 41% 61.0 1.4 1.8 2.5 70% 72% 3.8
ms ms
12 7 days 1019 448 ms 41% 28% § 47% 53.0 1.8 3.2 3.1 59% 57% 4.3
ms ms
Control N/A 1234 431 ms 31% 37% 52% 67.0 2.1 2.9 3.2 43% 44% 3.0
1 ms ms
Control N/A 1028 378 ms 34% 27% 44% 55.7 1.6 1.3 2.1 76% 61% 3.6
2 ms ms
Control N/A 1022 455 ms 40% 25% 44% N/A 2.0 2.4 1.9 68% 56% 3.5
3 ms
Control N/A 1101 412 ms 43% 32% 53% N/A 1.0 1.7 2.6 60% 63% 3.5
4 ms
Control N/A 1013 384 ms 43% 23% 43% 48.6 2.9 2.7 N/A 70% 63% 3.6
5 ms ms
Control N/A 1047 435 ms 40%‡ 25% 41% 53.5 2.0 3.0 3.0 64% 61% 3.1
6 ms ms
Control N/A 1018 438 ms 45% 26% § 48% N/A 1.6 2.2 2.4 71% 59% 3.6
7 ms
* Ratio of signal intensity on Turbo Inversion Recovery Magnitude Imaging (TIRM) between myocardium and skeletal muscle
† Study performed on a 3 Tesla MRI scanner
‡ Study done with assumed hematocrit of 40%
§ Although global ECV was within normal limits, regional ECV over 30% were noted
CMR = Cardiac Magnetic Resonance, ECV = extracellular volume, PC = partition coefficient, RV = Right Ventricle, LV = Left Ventricle,
EF = Ejection Fraction
Page 6/15Patient Vaccine Global Global Hematocrit Global Global Peak TIRM Ratio* RV LV Cardiac
to CMR Native Contrast ECV PC T2 EF EF Output
T1 Enhanced Base Mid Apex
T1
Control N/A 1173 362 ms 40% 35% 59% 74.5 3.9 4.4 4.1 53% 62% 2.7
8 ms ms
Control N/A 1009 369 ms 44% 24% 47% 52.7 2.3 2.4 2.9 66% 65% 2.6
9 ms ms
Control N/A 1032 484 ms 42% 30% 52% N/A 1.8 3.0 3.5 77% 46% 4.8
10 ms
Control N/A 1022 454 ms 38% 30% 49% 54.1 3.7 2.5 2.2 66% 57% 3.8
11 ms ms
Control N/A 1089 411 ms 40% 32% 54% 50.8 2.1 2.6 3.4 66% 47% 3.7
12 ms ms
* Ratio of signal intensity on Turbo Inversion Recovery Magnitude Imaging (TIRM) between myocardium and skeletal muscle
† Study performed on a 3 Tesla MRI scanner
‡ Study done with assumed hematocrit of 40%
§ Although global ECV was within normal limits, regional ECV over 30% were noted
CMR = Cardiac Magnetic Resonance, ECV = extracellular volume, PC = partition coefficient, RV = Right Ventricle, LV = Left Ventricle,
EF = Ejection Fraction
Table 4
Late Gadolinium Enhancement Findings
Patient Regions of Enhancement
1 Basal Inferior and Inferolateral Walls
2 Mid to Apical Lateral Wall
3 Basal, Mid and Apical Anterior, Anterolateral, Inferolateral and Inferior Walls; Mid Inferolateral Wall
4 Mid inferolateral and anterolateral walls, apical and basal anterior and lateral walls, tip of apex
5 Mid and Apical Anterolateral and inferolateral extending into the inferior wall
6 Lateral wall from base to apex, basal inferior septum
7 Basal inferior septum
8 Lateral wall of the apex extending to the mid ventricle, Apical inferior wall
9 Lateral wall at the apex
10 Basal inferior lateral wall
11 Mid lateral free wall, extending into the apical and basal lateral free wall
12 Mid to apical anterolateral free wall
Page 7/15Table 5
Cardiac Magnetic Resonance Strain Data
Study Patients Control Patients
SAX Global SAX Global LAX Global LAX Global SAX Global SAX Global LAX Global LAX Global
Circ Strain Radial Strain Long Strain Radial Strain Circ Strain Radial Strain Long Strain Radial Strain
1 -22.7 46.6 -20.8 41.4 -11.2 15.3 -13.5 21.8
2 -21.1 38 -19.3 33.1 -21.6 40.6 -22.9 51.3
3 -21.5 41.6 -20.5 36.6 -20.3 37 -17.6 32.9
4 -21.3 45 -18.6 32.9 -16.7 28 -19.9 37.3
5 -21.1 39.5 -18.4 34.4 -19.6 34.2 -19.9 35.6
6 -18.5 30.6 -15.5 24.2 -19.4 34.6 -15.3 24.3
7 -24.3 52.7 -24.4 55.1 -20.3 37.6 -18.9 34.1
8 -19.3 33.5 -15.7 25.5 -13.4 19.8 -13.5 20.6
9 -22.3 43.1 -19.4 35.4 -17.7 29.2 -17.9 30.8
10 -24.4 55.2 -21.4 41.7 -23.1 47.4 -15.8 35.8
11 -21.3 40.1 -17.3 31.5 -22.2 42.4 -20 36.2
12 -19.8 37.6 -18.9 33 -17.4 29.8 -16.9 27.4
* SAX = Short axis, LAX = Long Axis
† All strain data is expressed in percentages
Table 6
Comparison of Study Patients to Age Matched Controls
Study Patients Age Matched Controls p value
Median IQR Median IQR
LV Ejection Fraction 70.5% 63.5, 77.0 66 62.0, 70.5 0.28
RV Ejection Fraction 65.7% 58.0, 69.8 60 51.5, 62.5 0.042
Indexed Cardiac Output 4.2 3.9, 4.8 3.6 3.1, 3.7 0.024
L/min/m2
Short Axis Global Circumferential Strain -21.3% -22.5, -20.5 -19.5 -21.0, -17.1 0.006
Short Axis Global Radial Strain 40.9% 37.8, 45.8 34.4 28.6, 39.1 0.007
Long Axis Global Longitudinal Strain -19.1% -20.7, -17.9 -17.8 -19.9, -15.6 0.18
Long Axis Global Radial Strain 33.8% 32.2, 39.0 33.5 25.9, 36.0 0.18
Native T1* 1033 ms 1018, 1094 1028 1020, 1068 0.97
Contrast T1* 447 ms 426, 469 431 381, 446 0.10
ECV 28% 25.35, 30.65 30 23.25, 36.75 0.27
Peak T2 (n = 8) 54 ms 41.35, 66.65 49.5 41.75, 57.25 0.44
* Patient 4 was excluded from T1 value analysis as his study was done with a 3.0 Tesla scanner
Page 8/15Table 7
Correlation Between Strain and Parametric Mapping in Study Patients
Native Contrast Extracellular Partition Mass of Myocardium Percentage of
T1* Enhanced Volume Coefficient with Late Myocardium with Late
T1* Enhancement Enhancement
Short Axis Global r= r = -0.07 r = 0.11 r = 0.27 r = 0.33 r = 0.14
Circumferential 0.17
Strain p = 0.84 p = 0.73 p = 0.40 p = 0.30 p = 0.66
p=
0.67
Short Axis Global r= r = 0.03 r = -0.22 r = -0.34 r = -0.22 r = -0.12
-0.18
Radial Strain p = 0.94 p = 0.49 p = 0.24 p = 0.48 p = 0.72
p=
0.59
Long Axis Global r= r = -0.27 r = 0.04 r = 0.05 r = 0.45 r = 0.36
0.33
Longitudinal Strain p = 0.42 p = 0.91 p = 0.86 p = 0.14 p = 0.24
p=
0.33
Long Axis Global r= r = 0.15 r = -0.10 r = -0.16 r = -0.53 r = -0.44
-0.37
Radial Strain p = 0.67 p = 0.76 p = 0.62 p = 0.07 p = 0.15
p=
0.26
* Patient 4 was excluded from T1 value analysis as his study was done with a 3.0 Tesla scanner
Ten patients had signal intensity ratios of cardiac and skeletal muscle equal to or greater than 1.9 on T2 weighted TIRM sequences and
five patients had prolonged T2 relaxation values. (Fig. 3) Even using a cutoff of > 55 msec, this finding would not have changed. Two
patients, #9 and 10, did not meet criteria for myocardial edema for either TIRM ratio or T2 relaxation times.
One of these patients (#9) underwent her CMR 39 days after the onset of symptoms and was asymptomatic at the time of her study.
She did undergo an echocardiogram one day after symptom onset that demonstrated normal biventricular function with no wall motion
abnormalities or effusions.
One patient (#4) was incidentally diagnosed with partial anomalous pulmonary venous connection of the left upper pulmonary vein to
the innominate vein and right upper pulmonary
vein as well as right middle pulmonary vein to the right superior vena cava; his Qp:Qs was roughly 1.9:1 by CMR. Another patient (#6)
had a history of a bicuspid aortic valve; his echocardiogram and CMR demonstrated insignificant aortic insufficiency and stenosis.
CMR Findings, Viral Myocarditis: CMR was obtained within 10 days after symptoms onset in 11 of 12 patients with viral myocarditis.
One patient had CMR performed three months later that definitively met criteria for myocarditis. Eleven patients met criteria for
myocarditis; one patient was felt to be borderline positive on the basis of very minimal late gadolinium enhancement. Three patients
had mildly depressed left ventricular function, though as a whole the left ventricular function was not significantly different from the
study cohort. One patient had mildly depressed right ventricular function. Late gadolinium enhancement was universal in the control
patients. Six of 12 patients had increased global ECV; one additional patient had a normal global ECV but increased regional ECV. All
control patients met criteria for edema on the basis of signal intensity on T2 weighted TIRM sequences. Only two of eight patients who
underwent T2 mapping had prolonged T2 values. No patients had any form of congenital heart disease.
Comparison between CMR findings of vaccine and viral myocarditis: Compared to age matched controls with viral myocarditis, patients
with post-vaccine myocarditis had a higher right ventricular ejection fraction (RVEF) and cardiac index. (Table 6) They also had more
favorable short axis global circumferential and radial strain (Tables 5 and 6). There was no difference between the two cohorts in long
axis strain, T1 values and left ventricular function. Amongst patients with post-vaccine myocarditis, there was no correlation between
strain values and quantification of late gadolinium enhancement nor strain values and T1 values or extracellular volume (Tables 6 and
7).
Page 9/15Discussion
In this study comparing pediatric patients with post-vaccine myocarditis and viral myocarditis, we found that patients with post-vaccine
myocarditis have more favorable short axis global circumferential and radial strain as well an increased right ventricular ejection
fraction and cardiac index. However, there was no correlation of myocardial strain to either the burden of late gadolinium enhancement
nor extracellular volume or T1 values.
Post-vaccine myocarditis is a rare phenomenon and has been reported in vaccinations previously, including oral polio, influenza, and
smallpox vaccination.23-25 In cases not directly caused by infection of the myocardium23, the suspected pathogenesis of post-vaccine
myocarditis is “molecular mimicry” between antigens involved in producing vaccination response and those on the myocardium.24,26
CMR parametric mapping data in cases of pediatric post-COVID-19 vaccine myocarditis in the literature is limited. Shaw et al described
two pediatric patients with T1 values, T2 values, and extracellular volume ranging from 1122-1172ms (normal 950-1050ms), 56-74ms
(normal < 55ms) and 38 to 42% (normal < 28%), respectively.5 Dionne et al described 15 patients, with 4 of 15 patients showing
borderline or elevated T1 values, 1 of 15 with borderline elevated T2 values and 2 of 15 with regional hyperintensity on T2 weighted
imaging.14 Vidula et al described an 18 year old who had a T1 time and T2 time of 1089-1097ms, respectively.2 McLean et al and Park
reported hyperemia and early enhancement, respectively but without reporting T1 values.1,4 There was no comparison in any of these
studies with viral myocarditis.
All 12 patients had late gadolinium enhancement, predominantly in the lateral and inferior walls of the left ventricle. This pattern is
consistent with cases of pediatric post-COVID-19 vaccination myocarditis reported in the literature. Similar patterns have also been
found after smallpox vaccination.27 Early data suggests that this late gadolinium enhancement may improve over time,13 but long-term
CMR data and clinical outcomes are still to be determined.
We found that patients with post-vaccine myocarditis had more favorable short axis longitudinal and radial strain compared to patients
with viral myocarditis. This finding has not been previously reported in the pediatric population. Myocardial strain can be more sensitive
in identifying decreased myocardial deformation than ejection fraction as a normal global ejection fraction can mask diseased and
hypokinetic segments. Less favorable strain is associated with adverse events such as all-cause mortality, ventricular tachycardia of
longer than 30 seconds and hospitalization for heart failure in adult patients with myocarditis.28 In addition, adult patients with
fulminant myocarditis have less favorable strain than those with non-fulminant myocarditis.29 Our study cohort had normal values for
strain30 and more favorable strain for previously published strain values in children with myocarditis.31 This suggests that post-vaccine
myocarditis represents a milder variant of myocarditis.
We failed to find any correlation between parametric mapping values and the amount of discrete fibrosis with strain values. (Table 5)
This may be due to our cohort’s small sample size; a larger sample size to determine this would be needed. Previous studies in other
diseases such as tetralogy of Fallot has found a correlation between T1 mapping and left ventricular strain, however, DENSE was used
to measure myocardial deformation in that study.32
A relatively low proportion of patients both reported in the literature as well as in this case series have had elevated T2 relaxation times.
Using the myocardial to skeletal muscle signal intensity ratio may have increased sensitivity to identify patients with myocardial
edema. Alternatively, further work may be needed to identify a more appropriate cutoff for myocardial T2 values to help increase the
sensitivity of T2 mapping.
We also found that although the RVEF was normal in both cohorts, patients with post-vaccine myocarditis had a greater RVEF. Previous
studies have shown that depressed right ventricular function has been associated with adverse events.33
Despite the findings in this study, the benefits of vaccination far outweigh the risks.34 The rate of myocarditis is far higher in patients
with COVID-19 than in patients receiving the COVID-19 vaccine.35 In addition, children with COVID-19 are at risk for the subsequent
multisystem inflammatory syndrome in children (MIS-C), in which children present with severe multi-organ inflammation about 2-6
weeks after the initial infection, sometimes in shock and requiring intensive care with decreased ventricular function.36
This study was limited due to its retrospective nature and relatively small cohort as patients were enrolled from a single center.
However, these limitations allow for consistent CMR scanning techniques, sequence analysis and imaging interpretation. Each patient’s
Page 10/15diagnosis was felt to be consistent with post-vaccine myocarditis by the clinical providers, but causation cannot necessarily be proved.
Conclusion
Post-vaccine myocarditis has more favorable short axis global circumferential and radial myocardial strain than those with viral
myocarditis, lending to the notion that this illness affects ventricular function less than viral myocarditis. Typical CMR findings in our
cohort consisted of late gadolinium enhancement in the lateral and free walls of the left ventricle. Measurement of signal intensity
ratios between skeletal muscle and myocardium may be more sensitive in identifying myocardial edema compared to T2 mapping at
the current normative values used for this study. Overall, the impact on myocardial strain by CMR is less significant in post-vaccine
myocarditis compared to more classic viral myocarditis.
Declarations
Sources of Funding
This project was not funded by any internal or external funds.
Conflicts of interest/Competing interests: The authors declare that they have no conflict of interest.
Ethics approval: This retrospective chart review study involving human participants was in accordance with the ethical standards of the
institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical
standards.
Informed consent: Not obtained due to retrospective study design
Authors' contributions: All authors contributed to the study conception and design. Material preparation and data collection were
performed by Danish Vaiyani and Matthew Elias. All authors drafted, read, critically revised, and approved the final manuscript
References
1. McLean K, Johnson TJ. Myopericarditis in a previously healthy adolescent male following COVID-19 vaccination: A case report.
Acad Emerg Med 2021.
2. Vidula MK, Ambrose M, Glassberg H, et al. Myocarditis and Other Cardiovascular Complications of the mRNA-Based COVID-19
Vaccines. Cureus 2021; 13(6): e15576.
3. Dickey JB, Albert E, Badr M, et al. A Series of Patients With Myocarditis Following SARS-CoV-2 Vaccination With mRNA-1279 and
BNT162b2. JACC Cardiovasc Imaging 2021.
4. Park J, Brekke DR, Bratincsak A. Self-limited myocarditis presenting with chest pain and ST segment elevation in adolescents after
vaccination with the BNT162b2 mRNA vaccine. Cardiology in the young 2021: 1-4.
5. Shaw KE, Cavalcante JL, Han BK, Gossl M. Possible Association Between COVID-19 Vaccine and Myocarditis: Clinical and CMR
Findings. JACC Cardiovasc Imaging 2021.
6. Abu Mouch S, Roguin A, Hellou E, et al. Myocarditis following COVID-19 mRNA vaccination. Vaccine 2021; 39(29): 3790-3.
7. Marshall M, Ferguson ID, Lewis P, et al. Symptomatic Acute Myocarditis in Seven Adolescents Following Pfizer-BioNTech COVID-19
Vaccination. Pediatrics 2021.
8. Schauer J, Buddhe S, Colyer J, et al. Myopericarditis after the Pfizer mRNA COVID-19 Vaccine in Adolescents. J Pediatr 2021.
9. Watkins K, Griffin G, Septaric K, Simon EL. Myocarditis after BNT162b2 vaccination in a healthy male. Am J Emerg Med 2021.
10. Minocha PK, Better D, Singh RK, Hoque T. Recurrence of Acute Myocarditis Temporally Associated with Receipt of the mRNA
Coronavirus Disease 2019 (COVID-19) Vaccine in a Male Adolescent. J Pediatr 2021.
11. Starekova J, Bluemke DA, Bradham WS, Grist TM, Schiebler ML, Reeder SB. Myocarditis Associated with mRNA COVID-19
Vaccination. Radiology 2021: 211430.
12. Tano E, San Martin S, Girgis S, Martinez-Fernandez Y, Sanchez Vegas C. Perimyocarditis in Adolescents After Pfizer-BioNTech
COVID-19 Vaccine. J Pediatric Infect Dis Soc 2021.
13. Jain SS, Steele JM, Fonseca B, et al. COVID-19 Vaccination-Associated Myocarditis in Adolescents. Pediatrics 2021.
Page 11/1514. Dionne A, Sperotto F, Chamberlain S, et al. Association of Myocarditis With BNT162b2 Messenger RNA COVID-19 Vaccine in a Case
Series of Children. JAMA Cardiol 2021.
15. Kotanidis CP, Bazmpani MA, Haidich AB, Karvounis C, Antoniades C, Karamitsos TD. Diagnostic Accuracy of Cardiovascular
Magnetic Resonance in Acute Myocarditis: A Systematic Review and Meta-Analysis. JACC Cardiovasc Imaging 2018; 11(11): 1583-
90.
16. Friedrich MG, Sechtem U, Schulz-Menger J, et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. Journal
of the American College of Cardiology 2009; 53(17): 1475-87.
17. Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation:
Expert Recommendations. Journal of the American College of Cardiology 2018; 72(24): 3158-76.
18. Gagliardi MG, Bevilacqua M, Di Renzi P, Picardo S, Passariello R, Marcelletti C. Usefulness of magnetic resonance imaging for
diagnosis of acute myocarditis in infants and children, and comparison with endomyocardial biopsy. The American journal of
cardiology 1991; 68(10): 1089-91.
19. Heymans S, Eriksson U, Lehtonen J, Cooper LT, Jr. The Quest for New Approaches in Myocarditis and Inflammatory
Cardiomyopathy. Journal of the American College of Cardiology 2016; 68(21): 2348-64.
20. Pagano JJ, Yim D, Lam CZ, Yoo SJ, Seed M, Grosse-Wortmann L. Normative Data for Myocardial Native T1 and Extracellular
Volume Fraction in Children. Radiol Cardiothorac Imaging 2020; 2(4): e190234.
21. Alsaied T, Tseng SY, Siddiqui S, et al. Pediatric Myocardial T1 and T2 Value Associations with Age and Heart Rate at 1.5 T.
Pediatric cardiology 2021; 42(2): 269-77.
22. Roy C, Slimani A, de Meester C, et al. Age and sex corrected normal reference values of T1, T2 T2* and ECV in healthy subjects at
3T CMR. J Cardiovasc Magn Reson 2017; 19(1): 72.
23. Miller ER, Moro PL, Cano M, Shimabukuro TT. Deaths following vaccination: What does the evidence show? Vaccine 2015; 33(29):
3288-92.
24. Nagano N, Yano T, Fujita Y, et al. Hemodynamic Collapse After Influenza Vaccination: A Vaccine-Induced Fulminant Myocarditis?
Can J Cardiol 2020; 36(9): 1554 e5- e7.
25. Halsell JS, Riddle JR, Atwood JE, et al. Myopericarditis following smallpox vaccination among vaccinia-naive US military
personnel. JAMA 2003; 289(24): 3283-9.
26. Bozkurt B, Kamat I, Hotez PJ. Myocarditis with COVID-19 mRNA Vaccines. Circulation 2021.
27. Keinath K, Church T, Kurth B, Hulten E. Myocarditis secondary to smallpox vaccination. BMJ Case Rep 2018; 2018.
28. Fischer K, Obrist SJ, Erne SA, et al. Feature Tracking Myocardial Strain Incrementally Improves Prognostication in Myocarditis
Beyond Traditional CMR Imaging Features. JACC Cardiovasc Imaging 2020; 13(9): 1891-901.
29. Li H, Zhu H, Yang Z, Tang D, Huang L, Xia L. Tissue Characterization by Mapping and Strain Cardiac MRI to Evaluate Myocardial
Inflammation in Fulminant Myocarditis. J Magn Reson Imaging 2020; 52(3): 930-8.
30. Andre F, Robbers-Visser D, Helling-Bakki A, et al. Quantification of myocardial deformation in children by cardiovascular magnetic
resonance feature tracking: determination of reference values for left ventricular strain and strain rate. J Cardiovasc Magn Reson
2016; 19(1): 8.
31. Wisotzkey BL, Soriano BD, Albers EL, Ferguson M, Buddhe S. Diagnostic role of strain imaging in atypical myocarditis by
echocardiography and cardiac MRI. Pediatr Radiol 2018; 48(6): 835-42.
32. Haggerty CM, Suever JD, Pulenthiran A, et al. Association between left ventricular mechanics and diffuse myocardial fibrosis in
patients with repaired Tetralogy of Fallot: a cross-sectional study. J Cardiovasc Magn Reson 2017; 19(1): 100.
33. Mendes LA, Dec GW, Picard MH, Palacios IF, Newell J, Davidoff R. Right ventricular dysfunction: an independent predictor of
adverse outcome in patients with myocarditis. American heart journal 1994; 128(2): 301-7.
34. Writing C, Gluckman TJ, Bhave NM, et al. 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19
in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS-CoV-2 Infection, and Return to Play: A
Report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology
2022; 79(17): 1717-56.
35. Moulson N, Petek BJ, Drezner JA, et al. SARS-CoV-2 Cardiac Involvement in Young Competitive Athletes. Circulation 2021; 144(4):
256-66.
Page 12/1536. Matsubara D, Kauffman HL, Wang Y, et al. Echocardiographic Findings in Pediatric Multisystem Inflammatory Syndrome
Associated With COVID-19 in the United States. Journal of the American College of Cardiology 2020; 76(17): 1947-61.
Figures
Figure 1
Four chamber late gadolinium enhancement imaging of patient 8 demonstrating enhancement along the lateral wall of the mid left
ventricle and apex as indicated by arrows
Page 13/15Figure 2
Short axis late gadolinium enhancement imaging of patient 8 demonstrating enhancement along the inferolateral wall as indicated by
arrows
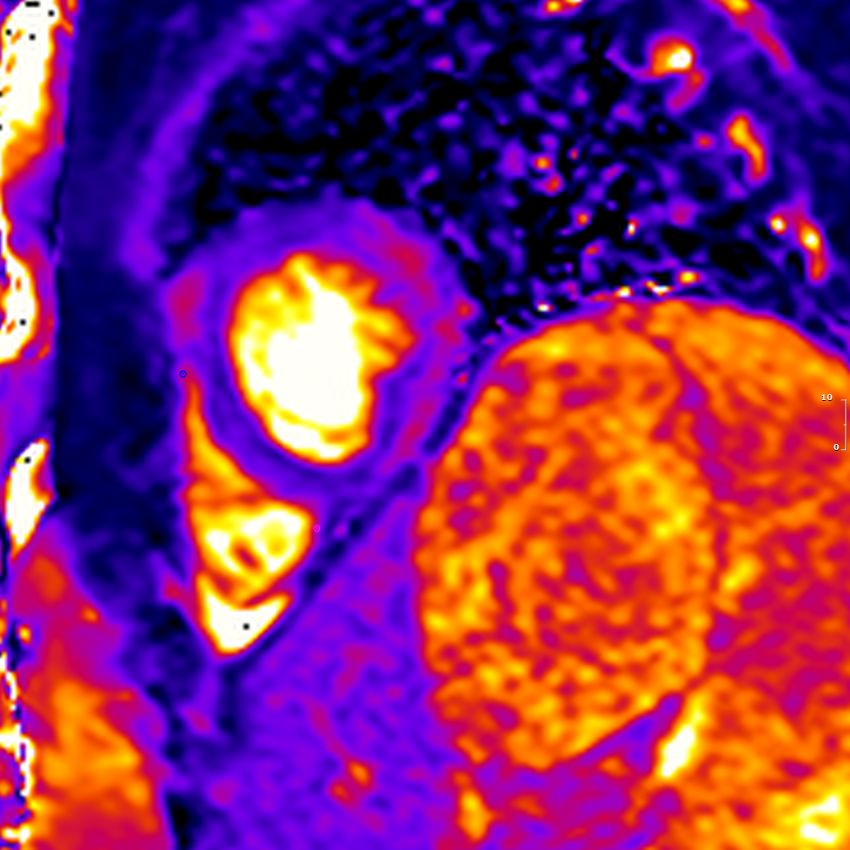
Page 14/15Figure 3
Native T2 mapping of patient 8 in the short axis projection in the apex demonstrating increased signal intensity in the lateral wall.
Page 15/15You can also read

















































