AMR in Liver Transplantation: Note on DSA - Presence of DSA associated with increased risk of
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

AMR in Liver Transplantation:
Note on DSA
• Presence of DSA associated with increased risk of
• Chronic rejection
• Acute rejection with ductopenia
• Unexplained graft fibrosis
• Unexplained biliary complications
• De-novo AIH (non-HLA DSA)
www.cancer.gov
AMR in Liver Transplantation:
Note on DSA
• Differences in class I vs class II DSA
• Liver allograft in simultaneous liver-kidney transplant was thought to
provide protection from DSA and decrease risk of kidney AMR, but high
MFI HLA Class II DSA still at risk
• Likely higher MFI cut-off values than in other SOT
• DSA IgG subclass may be important
• IgG3 strongly associated with graft loss
• DSA found in control patients with no other signs, symptoms,
or risk factors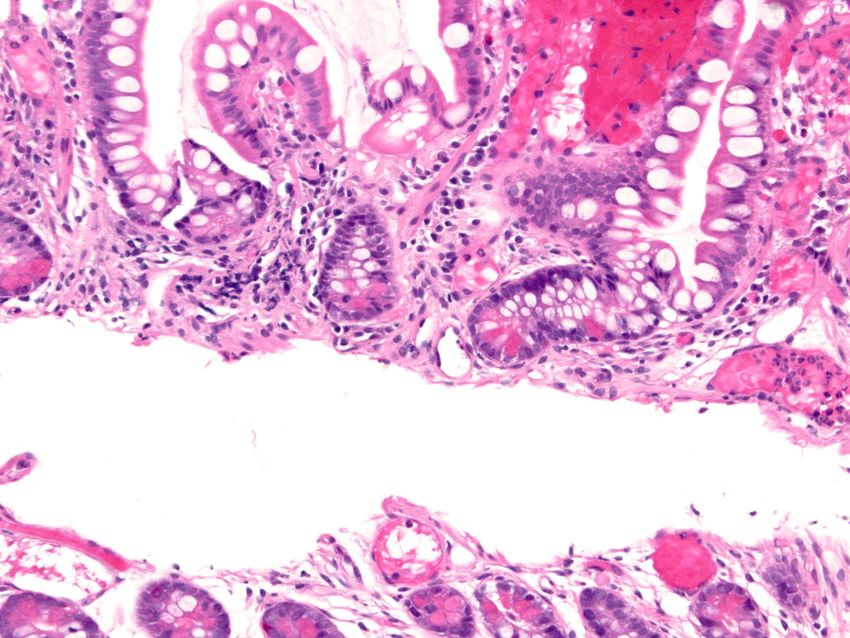
AMR in Liver Transplantation: Role of C4d
In studies that do include the full
clinicopathologic correlation and clear
diagnostic terms:
• Diffuse clearly positive C4d staining in >50% of
portal tracts (IHC) or sinusoids (IF)
• Correlates with presence of DSA
• Correlates with histologic features of AMR
• Prevalence of reported cases of liver AMR meeting
criteria of other solid-organ systems: 0.6-3.7%
AMR in Liver Transplantation: Role of C4d • Take Home Message • Utility of looking for C4d not clearly established • No consensus diagnosis of AMR which includes C4d • IHC: small portal vessel staining is most specific • IF: sinusoidal staining is most specific • C4d staining may be seen in other conditions • Banff 2011 liver group goal for 2013: • Better understanding of spectrum of AMR and consensus guidelines for C4d interpretation

AMR in Liver Transplantation: Differential
Diagnosis
• Hyperacute rejection
• Since not often biopsied, histologic features are
derived from failed explanted allografts and are
not specific
• Severe preservation-reperfusion injury
• Graft ischemia
• Idiopathic massive hemorrhagic graft necrosis
AMR in Liver Transplantation: Differential
Diagnosis
• Acute antibody mediated rejection
– Biliary obstruction/technical biliary complications
• Histologic features overlap:
– Bile ductular reaction
– Portal tract neutrophils
– Cholestasis
– Preservation-reperfusion injury
– Acute cellular rejection
– Infection/Sepsis
– Cholestasis
– Acute ascending cholangitis
– Ischemic injury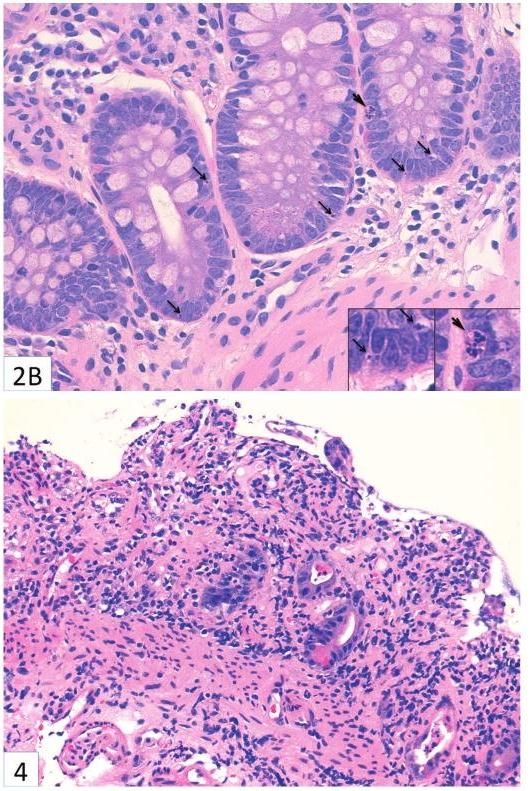
Take Home Message: AMR dx • Due nonspecificity of histologic findings, AMR should only be suggested as an etiology of the findings • Definitive diagnosis requires supportive clinical/serologic features and exclusion of the histologic mimics

AMR in Liver Transplantation: Pitfalls • The four major diagnostic criteria for AMR dx in renal and cardiac allografts have not been adopted for liver – Clinical graft dysfunction – Compatible histologic features – Deposition of C4d – Serologic evidence of DSA • No routine testing for DSA in liver recipients • C4d immunostaining is less established/less reliable

AMR in Liver Transplantation: Clinical
Aspects
• Prophylaxis
• For ABO-incompatible grafts (living donor)
• B-cell directed immunosuppression
• Rituximab, IVIg, Plasma exchange, Splenectomy
• Treatment
• B-cell directed immunosuppression
• Bortezomib: proteasome inhibitor, depletes
plasma cells→ decreased Ab production
AMR in Intestinal
Transplantation: Background
Townsend: Sabiston Textbook of Surgery, 18th ed.
Copyright © 2007 Saunders, An Imprint of ElsevierAMR in Intestinal Transplantation: Clinical
Aspects
• Extremely limited literature
• More common in patients undergoing retransplantation
after failed graft/chronic rejection
• DSA alone associated with worse outcome
• DSA with histologic ACR – consider concurrent AMR
• High PRA is a risk factor for rejection
• DSA can persist asymptomatically after hyperacute
rejection resolvesAMR in Intestinal Transplantation: Clinical
Aspects
• Presentation
• First 2 weeks post-transplant
• Increased stoma output
• ACR poorly responsive to standard therapy
• Persistent mucosal
ischemia/congestion/hemorrhage
• Peri- and post-operative syndromeAMR in Intestinal Transplantation: Clinical
Aspects
Peri- and post-operative syndrome
• Patients with strong crossmatch (T-cell cytotoxicity test) and
high PRA
• Segmental graft spasm, cyanosis, petechial hemorrhage
at reperfusion, lasting 45m
• Blood-tinged ostomy content within a few hours
• Ileostomy mucosal congestion for 1-2weeks
• Endoscopically, graft mucosa dusky with congestion,
hemorrhagic
Wu et al. Human Pathology, 2004 Nov;35(11):1332-9.Wu et al. Human Pathology, 2004 Nov;35(11):1332-9.
AMR in Intestinal Transplantation:
Background
• Hyperacute rejection (hours)
• Disseminated thrombosis
• Total ischemic necrosis
• Associated with presensitization
• high PRA, DSA
• Prophylaxis – desensitization
• IVIg to reduce PRA
• Protocols not standardizedAMR in Intestinal Transplantation: Histologic Features • Capillary endothelial cell enlargement • Fibrin thrombi • Vascular congestion • Hemorrhage • Neutrophil margination • Ulceration • Crypt apoptosis +/-
AMR in Intestinal Transplantation:
Histologic Features
• Features of ACR may be present
• Crypt apoptosis
• Crypt epithelial injury
• Lamina propria mononuclear inflammatory
infiltrate
• Ulceration +/-
• Architectural distortion +/-
• Severe ACR with arteritisCrypt apoptosis
Crypt injury & dropout
Denudation
Remotti et al. Arch Pathol Lab Med, 2012 Jul;136AMR in Intestinal Transplantation: Role of
C4d
• Nonspecific:
• C4d + in 36% of intestinal allografts with rejection
• And in 27% without rejection
• May be positive in small arterioles of normal intestine
Troxell et al. Arch Pathol Lab Med, 2006 130:1489-96.AMR in Intestinal Transplantation: Role of C4d • Take Home message • C4d deposition is nonspecific and may be present independent of rejection or absent during hyperacute rejection
AMR in Intestinal Transplantation:
Differential Diagnosis
• Vascular insufficiency/thrombosis
• Ischemic change
• Preservation/Reperfusion injury
• First few days post-op, resolves within 1 week
• Ischemic change, regenerative epithelium, villous
blunting, minimal inflammation
• Prior biopsy siteAMR in Intestinal Transplantation:
Differential Diagnosis
• Chronic rejection
• Arteriopathy: Mesenteric, serosal, and submucosal
vessels
• Luminal narrowing associated with intimal and medial
hyperplasia
• Associated mucosal changes
• Mucin loss, submucosal fibrosis
• Also paneth cell loss, neural hyperplasia
• Nonspecific changes: crypt apoptosis and dropout, villous
blunting, lamina propria fibrosisAMR in Intestinal Transplantation: Chronic
rejection
Does AMR have a role in chronic rejection?
• Intestinal allograft explants
• Contracted mesentery with fibrosis and chronic
arteriopathy
• Sampling mesenteric vessels for AMR before
this stage is technically not feasibleAMR in Intestinal Transplantation: Diagnosis Take Home message • Suspect AMR with DSA, histologic evidence of vascular alteration, and early/severe/resistant clinical signs of rejection • Treating a suspicion since no way to confirm AMR dx
AMR in Intestinal Transplantation: Clinical Aspects • Treatment • OKT3 • Steroids • Prostaglandin E • Prognosis • May not be associated with chronic rejection • Does not contribute to overall mortality or graft loss
AMR in Pancreas Transplantation
• Pancreas allograft infrequently biopsied due to perceived
risk
• AMR does occur in pancreas allograft
• Diagnosis requires 3 components (Banff 2011):
• Histology
3/3 = acute AMR
• C4d IHC 2/3 = consistent with acute AMR
1/3 = clinical exclusion of AMR required
• DSA
• (Clinical graft dysfunction not required)Acute AMR in Pancreas Transplantation
• Histology: evidence of tissue injury
• Inflammation of interacinar capillaries (capillaritis)
• Acinar cell damage (swelling, necrosis, apoptosis,
dropout)
• Vasculitis
• Thrombosis
• C4d positive:
• Diffuse C4d staining of interacinar capillaries (≥ 5% of
acinar lobule surfaceChronic Active AMR in Pancreas
Transplantation
Diagnosis requires:
• Combined features of AMR and chronic allograft
rejection/graft fibrosis
• Fibrotic expansion of fibrous septae; exocrine atrophy
• Exclusion of features of acute T-cell-mediated
rejection
• Acinar inflammation→damage; also inflammation of
septae, ducts, venulesSummary
• Liver
• AMR can be suggested as dx, as histologic features
overlap with other dx
• C4d utility not clearly established
• No consensus diagnostic criteria
• Small bowel
• Histologic features and clinical syndrome described
• C4d nonspecific
• Pancreas
• Consensus dx criteria including histology, C4d IHC, and
DSA
• Infrequently biopsiedSummary
• Kidney
• AMR very significant, acute and chronic forms, C4d done routinely
(IF preferred)
• Heart
• About 15% of patients, markedly increased risk of chronic rejection
and death, C4d very helpful, IHC or IF
• Lung
• Rare, diagnosis based on clinical graft dysfunction, circulating
antibodies, absence of cellular rejection, non-specific C4d staining
common, however strong endothelial staining reportedReferences
• Hübscher SG. Antibody-mediated rejection in the liver allograft. Curr Opin Organ Transplant. 2012
Jun;17(3):280-6.
• Fayek SA. The value of C4d deposit in post liver transplant liver biopsies. Transpl Immunol. 2012
Dec;27(4):166-70.
• Ratner LE, Phelan D, Brunt EM, Mohanakumar T, Hanto DW. Probable antibody-mediated failure of two
sequential ABO-compatible hepatic allografts in a single recipient. Transplantation. 1993 Apr;55(4):814-9.
• Musat AI, Agni RM, Wai PY, Pirsch JD, Lorentzen DF, Powell A, Leverson GE, Bellingham JM, Fernandez
LA, Foley DP, Mezrich JD, D'Alessandro AM, Lucey MR. The significance of donor-specific HLA antibodies
in rejection and ductopenia development in ABO compatible liver transplantation. Am J Transplant. 2011
Mar;11(3):500-10.
• Mengel M, Sis B, Haas M, Colvin RB, Halloran PF, Racusen LC, Solez K, Cendales L, Demetris AJ,
Drachenberg CB, Farver CF, Rodriguez ER, Wallace WD, Glotz D; Banff meeting report writing committee.
Banff 2011 Meeting report: new concepts in antibody-mediated rejection. Am J Transplant. 2012
Mar;12(3):563-70.
• Dick AA, Horslen S. Antibody-mediated rejection after intestinal transplantation. Curr Opin Organ
Transplant. 2012 Jun;17(3):250-7.
• de Kort H, Roufosse C, Bajema IM, Drachenberg CB. Pancreas transplantation, antibodies and rejection:
where do we stand? Curr Opin Organ Transplant. 2013 Jun;18(3):337-44.
• Wu T, Abu-Elmagd K, Bond G, Demetris AJ. A clinicopathologic study of isolated intestinal allografts with
preformed IgG lymphocytotoxic antibodies. Hum Pathol. 2004 Nov;35(11):1332-9.
• Swanson BJ, Talmon GA, Wisecarver JW, Grant WJ, Radio SJ. Histologic analysis of chronic rejection in
small bowel transplantation: mucosal and vascular alterations. Transplantation. 2013 Jan 27;95(2):378-82.You can also read

















































