NEWHAM CLINICAL COMMISSIONING GROUP - Newham CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NEWHAM CLINICAL COMMISSIONING GROUP
Local Strategic Estates
Plan (interim)
December 2015
[Type the abstract of the document here. The abstract is typically a short summary of the contents
of the document. Type the abstract of the document here. The abstract is typically a short summary
of the contents of the document.]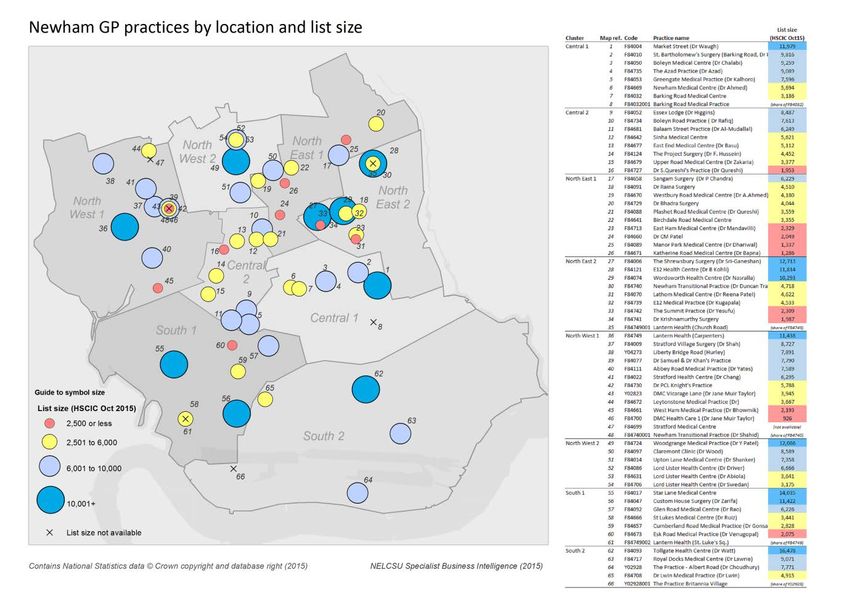
Contents
1. Executive summary ............................................................................................................................. 4
1.2 Introduction .................................................................................................................................. 5
1.3 Newham existing population and estate ...................................................................................... 6
1.4 Drivers for Change ........................................................................................................................ 6
1.5 Newham Clinical Commissioning Group’s vision for the estate ................................................... 7
1.6 Options for change........................................................................................................................ 8
1.7 Financial implications .................................................................................................................... 8
1.8 Delivering the strategy .................................................................................................................. 9
2. Scope and Methodology ................................................................................................................... 10
3. Current Position ................................................................................................................................ 12
3.1 Geography ................................................................................................................................... 12
3.2 Transport..................................................................................................................................... 13
3.3 Population background and demographics ................................................................................ 14
3.3.1 Index of multiple deprivation .............................................................................................. 14
3.4 The Current Physical Estate ........................................................................................................ 19
3.4.1 Overview .................................................................................................................................. 19
3.4.2 Current premises ..................................................................................................................... 20
3.4.2.1 Newham University Hospital- Plaistow, E13 ..................................................................... 20
3.4.2.2 East London Foundation Trust (ELFT) ............................................................................... 20
3.4.2.3 GP practices ...................................................................................................................... 22
3.4.3 Occupation, condition and utilisation .................................................................................. 23
3.4.4 Backlog maintenance ...................................................................................................... 25
3.5 Financial summary ...................................................................................................................... 26
4. Drivers for Change............................................................................................................................ 28
4.1 Introduction ................................................................................................................................ 28
4.2 Population predictions as drivers for change ............................................................................. 28
4.2.1 Distribution of Growth ......................................................................................................... 29
4.2.2 Implications of the Population Growth................................................................................ 30
4.3 Future model of care and service priorities ................................................................................ 31
4.4 Socio-economic changes impacting on services ......................................................................... 32
4.5 Highlighted service change ......................................................................................................... 33
4.5.1 Joining up primary, community and acute care services ..................................................... 33
4.5.2 Improve access to a wider range of primary care services .................................................. 33
1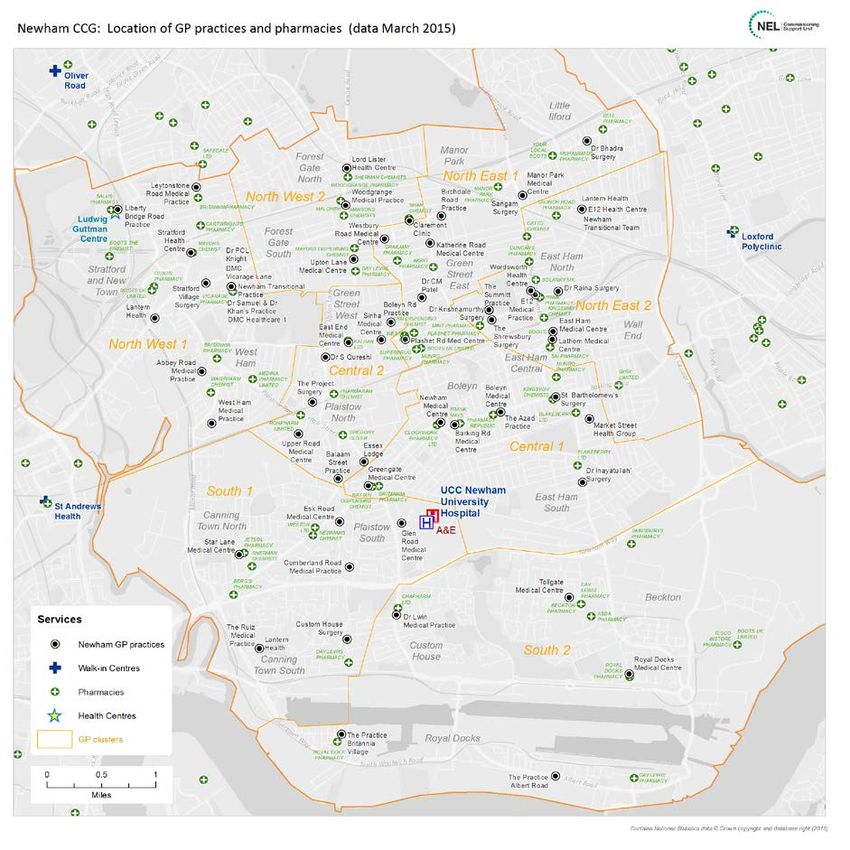
4.5.3 Provide more proactive care................................................................................................ 33
4.5.4 Improve access to specialist advice and improve the quality of referrals ........................... 34
4.5.5 Maternity and paediatric services ....................................................................................... 34
4.5.6 Out of hospital clinical services ............................................................................................ 34
4.5.7 Workforce to deliver ............................................................................................................ 34
4.6 Technology and service delivery changes ................................................................................... 35
4.7 Using estates to accommodate the changes .............................................................................. 35
4.8 Approach to commissioning for quality 2013-4 extracts ............................................................ 38
4.9 Challenges in respect of the current estate ................................................................................ 39
4.9.1 Planning and regeneration context ..................................................................................... 39
4.9.2 Community Infrastructure Levy / Section 106 (s106) .......................................................... 39
4.9.3 Other sources of capital funding.......................................................................................... 40
4.9.4 Cross boundary demand and opportunities ........................................................................ 41
4.9.5 Opportunity Areas................................................................................................................ 41
4.9.6 Housing targets .................................................................................................................... 42
4.9.7 Newham Local Plan .............................................................................................................. 43
4.9.8 Phasing of New Residential Development ........................................................................... 43
4.9.9 London Borough of Newham (LBN) Local development Plans ............................................ 43
4.9.10 Identification of sites where new health facilities may be required ................................. 44
4.9.11 Drivers Summary ................................................................................................................ 44
5. Estates Options for Change - How to get there ................................................................................ 46
5.1 Key principles and service models .............................................................................................. 46
5.2 Estates strategy assumptions and vision for primary care ......................................................... 46
5.3 Addressing the future need ........................................................................................................ 48
5.4 Opportunities and investments required. .................................................................................. 49
5.5 Summary ..................................................................................................................................... 51
6 Financial implications .................................................................................................................... 53
6.1 Background ........................................................................................................................... 53
6.2 Financial elements associated with the Strategy.................................................................. 53
6.3 Revenue Costs ....................................................................................................................... 54
6.4 Potential Financial Costs ....................................................................................................... 54
6.5 Funding the requirement ...................................................................................................... 55
7 Delivering the Strategy and Outline Implementation Plan ................................................................ 57
7.1 Priorities for years 1 -5 of the stategy (2016 -2021) ................................................................... 57
2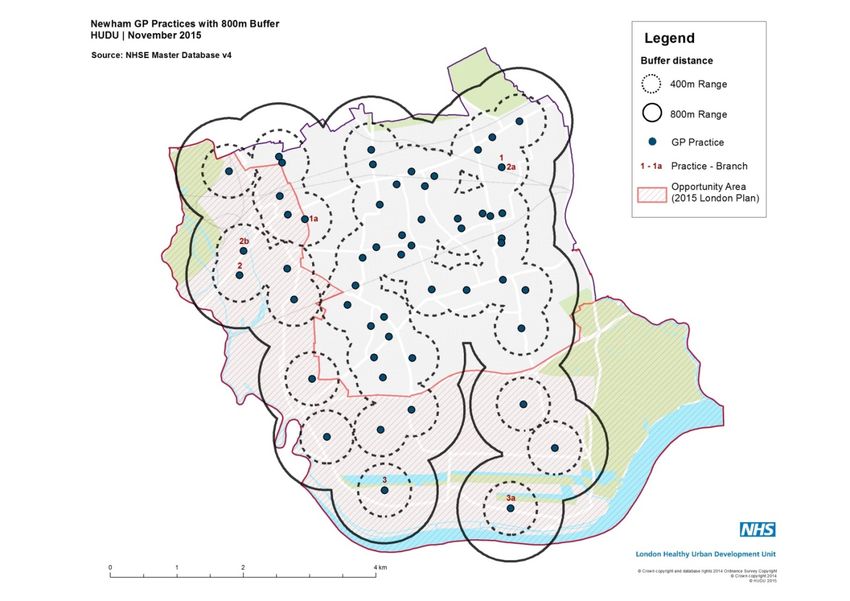
7.2 Development of the strategy ...................................................................................................... 57
7.3 Ongoing work plan and timescales ....................................................................................... 58
Planned and potential developments: ..................................................................................... 58
7.3.1 NCCG led projects – new developments.............................................................................. 58
7.3.2 Practice led NCCG supported projects ................................................................................. 58
7.4 Resources .................................................................................................................................... 59
7.4.1 Manpower ............................................................................................................................ 60
7.4.2 Enablers of change and managing constraints .................................................................... 60
7.4.3 London Borough of Newham Regeneration Plans ............................................................... 60
7.4.4 Working with the developers............................................................................................... 61
Section 3 Appendix 1 ELFT locations across Newham .......................................................................... 63
Section 3 Appendix 2 Complete list of practices................................................................................... 66
Section 3 Appendix 3 - Utilisation reviews ........................................................................................... 71
Section 3 Appendix 4 backlog maintenance ......................................................................................... 73
Section 4 Appendix 1 Outpatient transfers .......................................................................................... 75
Section 5 Appendix 1: Applications from practices for improvements, relocations and other
developments ....................................................................................................................................... 78
Section 5 Appendix 2 Transforming Services Together (TST) analysis of additional space .............. 80
Section 7 Appendix 1 DRAFT Newham Clinical Commissioning group - Strategic estates decision
framework............................................................................................................................................. 82
3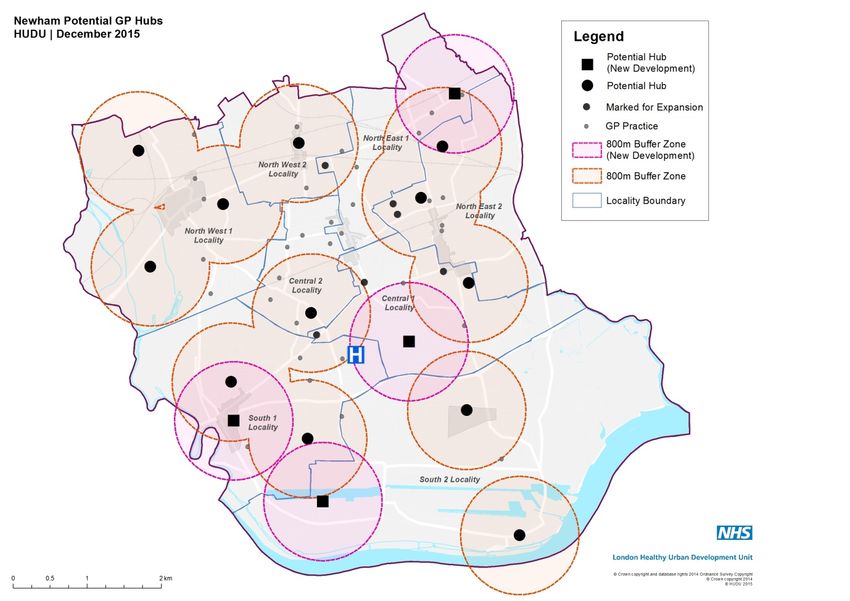
1. Executive summary
NHS England has requested all CCGs develop a local strategic estates’ plan, by 31st
December 2015. This strategy builds on national and regional guidance and more local
work to develop the case for change and strategic commissioning plans which clearly
document the scale of the challenge facing Newham health and social care services. The
strategy has an important role to play in enabling change, delivering savings, reducing
running costs and ensuring that all investment, including the Primary Care Transformation
Fund, is properly targeted.
The NHS faces funding constraints and in east London there is currently a significant
financial gap across all organisations. Whilst funding will increase due to the rising
population, this will not be enough and ways of working will need to change too. To continue
to provide safe, high quality and sustainable services in the future, Newham Clinical
Commissioning Group (NCCG) needs to work effectively and efficiently.
The key priorities of the strategy are to achieve a more efficient estate, identifying resources
to deliver new service models and ensure future investments are identified and prioritised
through the strategy. Areas where there is underutilisation or inappropriate use of valuable
estate need to be identified and brought into clinical use, where required. The estates
strategy will contribute to the delivery of Newham CCG’s primary care strategy and will
contribute as an enable to the Transforming Services Together programme as well as Better
Health for London 1 and the financial challenge faced by the NHS.
The opportunities envisaged in respect of using the existing estate more effectively include:
• reconfiguration of the estate to better meet commissioning needs
• shared property (particularly with social care and the wider public sector)
• more effective future investment and better value
• benefits for clinicians, staff and patients.
1
The Better Health for London report of the London Health Commission, published in October 2014 identified the need for significant
investment in the infrastructure of GP premises, to enable both primary care commissioners to realise their strategic plans and providers
to respond to them
The improvement grant application process launched in January 2015 as
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/184017/NHS__General_Medical_Services_-
_Premises_Costs__Directions_2013.pdf
4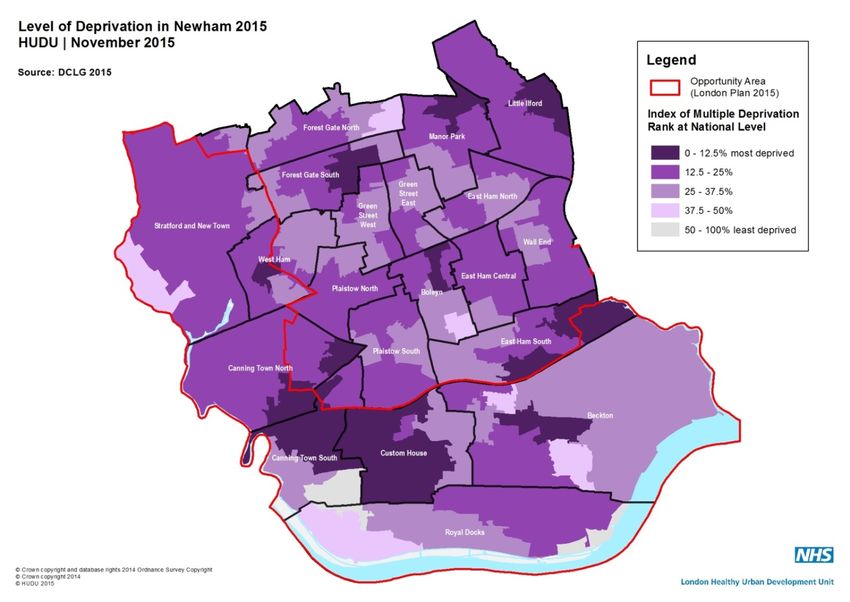
The strategy has been produced in conjunction with:
i. the Transforming Services Together (TST) workstream, which has identified the
potential changes to estates required to support delivering out of hospital services
ii. the healthy urban development unit (HUDU),
iii. London Borough of Newham (LBN) regeneration and public health teams
the latter two organisations providing information in respect of growth and population
demographics.
Three initial consultation workshops have been held during the autumn of 2015 with
i. the strategic estates working group
ii. Newham’s primary care clinicians and
iii. patient participation group leads
1.2 Introduction
Newham Clinical Commissioning Group (NCCG) has been granted full delegation for the
commissioning and performance management of primary medical services. Alongside the
transformation of services, a decisive approach needs to be taken to improve primary care
quality, by sharing the good practice high performers have developed and thus reducing
variation in outcomes for the population.
Primary care estates in Newham face a number of challenges. Significant parts of the
existing buildings and infrastructure fail to meet current and future standards and needs.
These poorer general practice facilities do not have the space to offer a wide range of
services nor support multi-disciplinary team working and this can contribute to a poor patient
experience.
However, Newham also has some excellent primary care facilities, although some of these
are not fully utilised. NHS England’s Five Year Forward View suggests primary care needs
to work at greater scale in facilities that enable teams from across health, and social care, as
well as a wider range of community services, to work together.
The London Borough of Newham (LBN) faces unprecedented demographic growth in one of
the most deprived areas of the UK, as well as epidemiological pressures due to a population
that experiences more years of life lived with poor health. The growth in population is
anticipated to be over 90k residents over the next 15 years which means the plans will need
to offer sufficient flexibility and be sustainable to meet the changes.
There is substantial financial pressure within all health economies: London alone will be
required to make a £2.4 billion saving by 2020/21, which means that finding ways to use
existing resources more effectively is urgently needed.
High level modelling suggests that in order to deliver a modern, high quality service for all,
between £310 and £810 million will need to be invested in primary and community services
in London annually. This is expected to begin with a gradual shift in total health spend of
0.40% – 1.07% each year over five years. This shift in total health spend has the potential to
deliver a significant increase in primary and community care capacity in the medium term.
Additional funding is being provided nationally in the form of:
• An increase of the primary care budget from 1.7% to 2.3%
5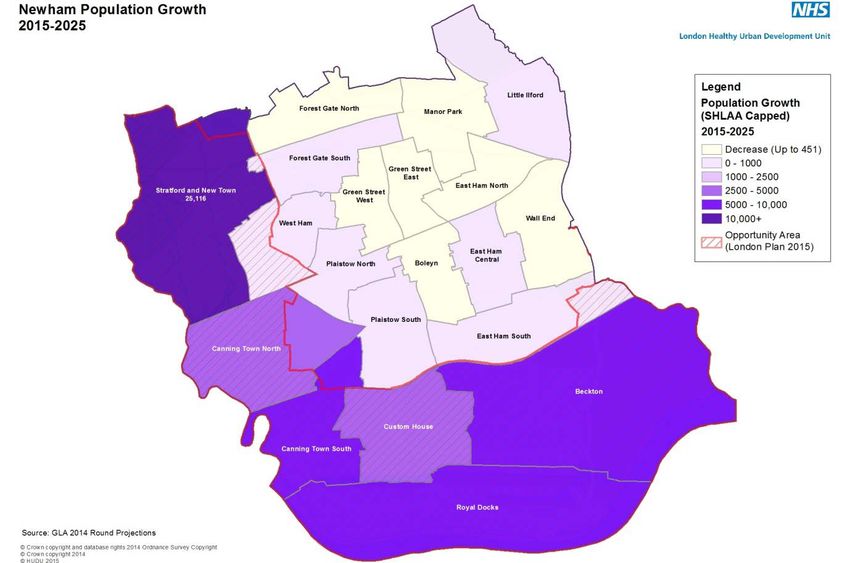
• Primary/community care infrastructure funding of £250m recurrent for four years from
2015-16
• An additional transformation budget of £200m for developing ‘vanguard’ sites
Within this context the CCG is committed to re-balancing NHS investment towards out of
hospital services and infrastructure.as set out in ourlocal commissioning intentions and in
line with the Strategic Planning Group’s five year strategic plan. The funding streams for this
programme are being identified to enable these changes.
1.3 Newham existing population and estate
Newham has a registered population of 332,582 (October 2015), the vast majority are
between 20 and 50 years, a young population, compared to the rest of the UK. Many of the
younger population are transient and do not register with general practice, favouring use of A
& E, which is a more costly intervention for the NHS.
Newham was recorded overall as the second most deprived area in England (2010).
In 2010 Newham was the second most deprived area in England, the three main factors
contribute to poor health being:
• Deprivation
• Ethnicity and language.
• Population mobility
Life expectancy in Newham has increased over the last 10 years, but despite this, the
healthy years of life remain fewer than for residents in other parts of London, putting strain
on the health and social care services required. NCCG needs to work closely with LBN to
improve the public health messages and access to appropriate services.
NCCG has over seventy buildings from which primary and community services are
delivered. The premises are owned by a large number of different organisations and
individuals, making changes more complex. Many of the GP premises are small (less than
200m2) and conversion/further development of most would not be possible or economical.
Thus the strategy sets out its vision to increase the capacity and facilities within a fewer
number of premises. This will encourage the use of shared facilities and increased
collaboration through collocation.
1.4 Drivers for Change
NCCG recognises its unique position as a borough with huge demographic change and an
increasing population predicted. This will be supported with the opportunity for regeneration
and an energy that can promote and deliver change.
The majority of the new population will live in six wards, within the area known as the
‘opportunity areas’ and additional estate and practices will be required for these residents.
Also in parallel, the existing population, many of whom have poorer life expectancy than
those in other parts of England, will be aging and are at risk of increasingly developing long
term conditions. Their needs must be considered in the development of improved facilities.
The key drivers for change in Newham are:
• Changes in population –increasing numbers and changes to demographics
• Opportunities from the regeneration programme of the borough
6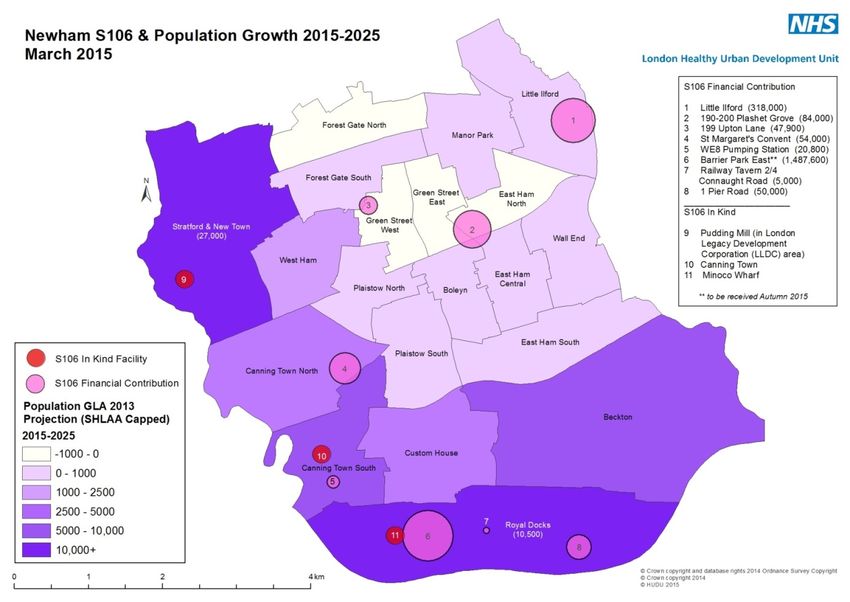
• Need to further improve the health outcomes for residents
• The need to use resources more effectively
• Primary care workforce challenges and the need to address shortages
• Benefiting from increased and improved technology
• The economic environment
• Using commissioning effectively through GP federations and out of hospital services
transfers
• Listening to the patient voice
A broader approach to the whole health economy challenges is illustrated in Fig 1 below:
Fig 1.1 Some of the challenges facing estates planning 2
1.5 Newham Clinical Commissioning Group’s vision for the estate
The overarching vision for Newham is to ensure out of hospital estate is of a high quality,
statutory compliant and in locations that support clinicians deliver the range of services to
support the health needs of their community.
i. ensure good value for money and an efficient use of resources
2
NCL SPG Workshop slides, The London Office of CCGs, 4th September 2015
7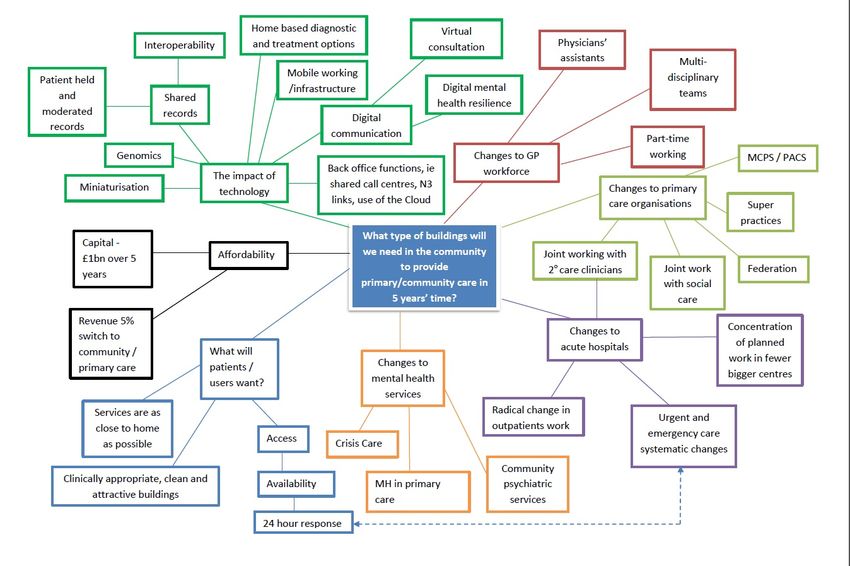
ii. maximising the use of space within existing buildings before investing in new builds’,
which will only be supported where they offer opportunities for 10-15,000 patients
which, and were possible, support the merge of smaller practices
iii. to develop a number primary care locality hubs, with the facilities to offer flexibility for
delivery of a wider range of services for a larger population, supported by GPs and
community providers working collaboratively, also wherever possible, co-locating with
wider local authority and third sector services that offer social, health and well- being
services
iv. to provide a small number of multispecialty community centres in which a wider range
of more specialist services are offered to a larger group of patients.
Developing these themes Newham will be looking to ensure those practices delivering
services from key modern facilities, for populations over 10,000 patients are invested in and
commissioned to deliver quality extended primary care services.
There will also be geographical spread of larger practices, able to offer more specialist
services to communities of over 50k residents; this will include diagnostic testing, maternity
services and long term condition clinics. At a larger scale the CCG may consider the use of
multispecialty community centres providing more specialised services for a population of
over 100k residents.
Establishing locality hubs at cluster level and multispecialty centres support patients’
preference to travel slightly further but receive a ‘one stop’ service covering all their regular
needs.
1.6 Options for change
NCCG will work on a cluster basis to determine the key premises within each locality for
investment and development, recognising the diverse ownership and interests of current
parties and its overarching need to reduce the number of properties and drive up quality.
Expansion and development of the current estate will be limited to those that fit the needs of
the area in being of sufficient size and condition to provide a valued patient experience.
The growth in population and increased health needs will mean a number of key new
opportunities will be NCCGs partnership with the London Borough of Newham and its
development partners, to secure investment in the regeneration areas or where there are
other needs are identified, to meet the patient pathways.
1.7 Financial implications
Capital investment over the period of the strategy will be available from a variety of sources,
including the CCG itself, NHS E, CIL/section 106, CHP, NHS PS or 3rd party developers.
The revenue impact on the CCG is a more significant long-term commitment required to
cover rent and rates.
This strategy will enable the forecast to be made of the required additional funding and how
this can be afforded, looking at opportunities to generate savings from mergers, utilising
space more effectively and sharing the facilities and costs with other agencies.
8
1.8 Delivering the strategy Delivering the strategy will require NCCG to share its vision and undertake further work practices and other stakeholders to secure change, ensuring full patient and public engagement at the same time. Following analysis of the premises condition and utilisation surveys the investment priorities will be reviewed and supported accordingly, assuring alignment to the geographical and demographic need of the population. The improved facilities will enable services out of hospital to be commissioned, increasing the range of diagnostic and community services to be available more locally. NCCG will need to identify resources, both financial and workforce to take forward the change agenda and secure the estate that will enable delivery of care well into the 2020’s. 9
2. Scope and Methodology
Newham Clinical Commissioning Group (NCCG) has prepared this interim estates
strategy to set out its plans and vision for the primary care estates. These will
support the clinicians to deliver the required services, in modern, fully equipped,
safe, local facilities that enable all members of the community to access their care in
a patient focussed environment.
The timing of the strategy is to:
• Meet the request from NHS England, requiring every CCG to provide a
strategy that will inform the allocation of its capital investment budget,
• Plan for the predicted significant population growth in Newham,
• Plan for the service delivery changes required to move care out of hospital,
for what is currently one of the most deprived areas of the UK and facing
epidemiological pressures due to an aging population.
• Ensure estates development are considered as part of NCCGs primary health
care strategy refresh and its strategic commissioning framework intentions
• Address the substantial financial pressure within the local health economy
and the saving requirement, which means finding ways to use existing
resources more effectively, is a priority.
Newham has set out to produce this local estates strategy in collaboration with a
wide range of local stakeholders (including the wider public estate). The formation of
a Local Strategic Estates Group (SEG) has been key to developing a robust
understanding of the available estate and aligning it to the NCCG’s commissioning
intentions to extract maximum value from NHS resources and reduce wastage.
The strategy has been challenged and endorsed by NCCGs Primary Care
Commissioning Committee.
Newham’s strategy proposes system-wide transformation and partnership working,
involving the London Borough of Newham and a range of other key organisations:
• Neighbouring CCGs - in particular Tower Hamlets, Waltham Forest (through
the Transforming Service Together programme), City and Hackney, Barking
and Dagenham, Havering and Redbridge
• Barts Health NHS Trust
• Homerton University Hospital NHS Trust
• East London NHS Foundation Trust (ELFT)
• North East London NHS Foundation Trust
• Local authorities (including public health teams) – in particular London
Borough of Newham; London Borough Tower Hamlets; London Borough of
Waltham Forest; London Borough of Redbridge
• NEL Commissioning Support Unit (CSU)
• NHS England (NHSE)
• Trust Development Authority (TDA)
• Healthy Urban Development Unit (HUDU)
• Transport for London (TfL)
Initial consultation with the community has taken place through the practice patient
group leads and wider engagement will follow the publication of the interim strategy
early in 2016.
10It is vital that service and estates planning are integrated to ensure the availability of high quality estate to deliver healthcare, driving the need for well-founded investment decisions that maximise the use of existing property, recommend where new estate should be developed to meet service needs and where, if appropriate, surplus estate can be sold. NCCG will seek to identify partners to offer the community a single point of access, developing the vision of linking health, well-being and social services together. 11
3. Current Position
3.1 Geography
The London Borough of Newham (fig 3.1) forms part of London’s East End dockland area,
situated with the river Thames as its south border, five miles east of the City of London. It
stretches 6.5miles by 6.8 miles at its widest points and covers, 22 hectares (14m2 miles
/36.2 km2). The resident population density (number of persons per hectare) is 85, which is
denser than the average for greater London (52) and England (41).
Fig 3.1 Location of the London Borough of Newham (LBN) within greater London and the UK
123.2 Transport
The borough (fig 3.2) is well served by a wide network of public transport links from
all other parts of London, Kent, East Anglia, as well as internationally through the
Eurotunnel and London City Airport. Transport includes the underground, Docklands
Light Railway, high speed rail to the south east and St Pancras, the new Crossrail
as well as a network of other over ground rail and bus transport systems.
Fig 3.2 Transport connectivity across Newham
The borough is crossed by several major road networks, the A13, A118 and A124,
which in turn link to the Blackwall tunnel and M25, and bordered to the east by the
North circular road (A 406).
Through its Local Implementation Plan, (Transport Policies and Programmes
Document) the London Borough of Newham has set out its key objectives to
achieve transport improvements- summarised in table 3.1 below.
Local Implementation Plan Objectives
Objective 1 Addressing key movement corridors, tackling congestion and improving
movement for all modes of travel
Objective 2 Connecting neighbourhoods and enabling local movement
Objective 3 Improving streetscape and environmental quality
Objective 4 Improving the condition of roads and footpaths
Objective 5 Encouraging sustainable and healthy travel behaviour
Objective 6 Tackling deprivation, improving the local economy and supporting new
development
Objective 7 Improving road safety
Objective 8 Reducing crime and fear of crime
Objective 9 Promoting the use of low emission transport including Reducing carbon
emissions from transport
Table 3.1 Key objectives to achieve transport improvements
133.3 Population background and demographics
Newham has one of the largest populations in London. In 2011, the resident population
stood at 311,912, of which 52% were male and 48% female. According to the GLA 2014
Round SHLAA Capped Population Projections, the population has continued to grow, by
circa 20,700 to some 332,582 in 2015, and is set to rise by another 55,156 persons over the
next decade.
Newham was recorded overall as the second most deprived area in England (2010). Three
particular factors contribute to poor health in Newham:
Deprivation: there are high levels of deprivation in parts of Newham. In some areas, the
levels are amongst the highest in the country.
Ethnicity and language: many people in Newham do not speak English as a first
language. This adds to the complexity of providing healthcare services. For example,
interpreters are sometimes required and consultations can take longer.
Population mobility: the East End is often the area where new immigrants move to first
and then move on, meaning the people and the ethnic mix of the population are
constantly changing. This can mean difficulties in providing continuity of care
(particularly in general practice) and health conditions remaining undiagnosed for long
periods. It is also now the area where lots of young people come and live on a temporary
basis - that causes issues for urgent care services because many young people do not
register with GP’s.
Higher level of deprivation in Newham increases demand for GP services based on
weighted average of 5.3 appointments per person/year.
3.3.1 Index of multiple deprivation
Figure 3.3 below shows how the high and low growth areas (Opportunity Area boundary)
relate to where deprivation is concentrated within the Borough (the Index of Multiple
Deprivation (IMD) is one indicator of population level need.
14Figure 3.3 Spread of Deprivation in Newham - Index of Multiple Deprivation (2015) The IMD is released by the Department for Communities and Local Governments (DCLG) and measures relative deprivation across England. The results are based on 37 different indicators across seven domains and cover Lower Super Output Areas (LSOAs). Whereas the 2010 release of the IMD ranked Newham as the 14th most deprived local authority in England, the recent 2015 release shows Newham now lying outside the top 25, suggesting significant improvements in relative deprivation. Nevertheless, Fig 3.3 shows that there are still many parts of Newham with high levels of deprivation. These include a large concentration of LSOAs within the top 12.5% of the most deprived across England within the Canning Town and Custom House wards, with scattered smaller concentrations elsewhere across the Borough. If the next band of deprivation is considered, then even larger parts of the Borough both within and outside the Opportunity Areas 3 fall within the top 25%. As the indicators cover a range of factors which directly and indirectly affect health and access to healthcare, the geographical spread of deprivation offers both challenges and opportunities for the health system. Whilst, within the Opportunity Areas, there is potentially more scope to transform the built environment and provide new facilities, elsewhere in Newham, there needs to be a different approach to generating and realising opportunities for 3 The opportunity area is identified on fig 3.3 being the wards in the south and west of the borough where regeneration and population growth is planned. 15
change and improvement including making the most of existing assets and collaboration with other health partners and stakeholders to both share and pool resources and to innovate. The age distribution across the borough (figs. 3.4, 3.5 below) shows the proportion of the population under 15 years (fig 3.4) and between 60 -74 (fig 3.5) years by ward – highlighting the different challenges across the borough. Figure 3.4 Age distribution by ward
Other
Figure 3.6 Top 10 causes of death in the male and female population of Newham 2011-13 4
The Joint Strategic Needs Assessment(JSNA) 2015 states ‘Newham has made very good
progress in improvements in life expectancy for both men and women but overall has made
poor progress in improving healthy life expectancy 5 in step with this’.
for Newham women there is a predicted 25 years of ill health before death
(6 years longer than in England). This equates to nearly one third of their
lives compared to one quarter for women on average in England.
For Newham men a predicted 19 years of ill health before death (3 years
longer than in England). This equates to one quarter of their lives
compared to one fifth for men in England.
Newham has a young population with an average age of 31 years
compared to England average age of 40 years, but Newham’s population
shows signs of early ageing leading to a higher than expected burden of
disease for health and care services
There are growing health inequalities in Newham
4
Source: ONS Public Health files, 2011-2013
5 Healthy life expectancy is a measure of the number of years that a person would expect to live in good
health based on contemporary mortality rates and self-reported good health.
17The Case for Change showed that preventing ill health; better management of conditions by
care providers before they become severe (and providing support for patients to self-care)
and treating people holistically by looking at their physical and mental health needs together
is essential to the long term future of healthcare. In Newham the top priorities for health
improvement are to tackle inactivity, obesity, high blood pressure and smoking, which
relates to improving the diseases having mot impact on ill-health, (table3.3).
Top 3 causes of ill health Men Women
Mental health illness caused 16,000 23,000
mainly from depression and
anxiety
Diabetes 11,500 10,000
Musculo-skeletal
Knee and hip arthritis 9,000 13,000
Table 3.3 Top 3 causes of ill health in the population of Newham
183.4 The Current Physical Estate
3.4.1 Overview
Newham currently delivers healthcare to its residents from Newham General
Hospital and 70 primary medical practices and community services buildings.
This section provides an overview of the current estates across Newham, based on
the NHS asset database 6, comprising all the NHS estate, acute and community trust,
individual GP practices and NHS England. Additionally, the residents are supported
by a network of pharmacies, dentists and opticians. The map (fig. 3.7 below) shows
the current distribution of health services in and around Newham.
Figure 3.7 Current distribution of health services in and around Newham
6
Source .The London NHS Asset database v5’
19The quality of the out of hospital estate in Newham is highly variable. There are a number of buildings that exemplify the specification of excellent design and facilities. However, there are a number of premises that are a real challenge to be able to improve. A poor estate potentially means poorer patient experiences, poor working conditions for clinicians and fewer opportunities to improve health and healthcare. There are currently significant gaps in the register’s formal analysis in respect of the condition and utilisation of the privately owned or third party developer leased general practice primary care estate. Work is being planned to address by early 2016. 3.4.2 Current premises 3.4.2.1 Newham University Hospital- Plaistow, E13 Newham University Hospital is part of the Barts Health NHS Trust. It offers a range of local services including a 24 hour emergency department, an urgent care centre, a modern purpose built outpatient facility and care of the elderly unit. The hospital also houses the local stroke and TIA centre. The maternity facilities opened in 2011 offer a much improved, high quality, modern and vibrant environment for mothers-to-be. The completion of the new area has also brought many services – including 24 hour maternity assessment, induction of labour and inpatient antenatal care – together into one purpose-built section of the hospital, accommodating up to 6,500 births per year. 3.4.2.2 East London Foundation Trust (ELFT) ELFT is currently commissioned to provide a wide range of community and mental health services from 18 locations across Newham, as listed in appendix Section 3 Appendix 1 ELFT locations across Newham. The provider owns 6 premises, with funding for these coming as part of the charge for services. ELFT has prepared a separate Estates Strategy 2013-18, with the key statement in respect of Newham set out in fig 3.8 below and the plans for a reduction/review of some facilities- as set out in table 3.4 below. 20
Inpatient facilities are provided through a PFI managed building and are well
maintained and generally of a good standard. The service has plans to increase
capacity by adding a number of additional bedrooms throughout its
acute wards. There are also a number of options to reconfigure the ward
space currently facilitating the Triage ward and this too will require some
capital investment.
Community services in Newham will call on a mixture of modernisation,
reconfiguration and in some cases relocation to different and fit for purpose
buildings.
Fig 3.8 ELFT overview of Newham estates
Facility Proposal Method Rationale
Take advantage of a Services expanding, insufficient space,
Francis House Disposal
break-clause in the lease dated property, not Condition B or DDA
compliant
Take advantage of a A more suitable environment required
The Hub Disposal
break-clause in the lease as soon as possible
Take advantage of a
Willow Suite Disposal Lease terminates 2014
break-clause
SW Children’s Services
Appleby Health Re-utilise The use of all CHN properties needs to
move in from Royal
Centre be reviewed with a view to improving
Docks Medical Centre
efficiency and sustainability of use for
Lord Lister Re-utilise Internal development the future
Joyce Campbell Re-utilise Internal development
West Ham Lane Redevelop Internal development
Table 3.4: ELFT Strategy extract on premises changes plans in Newham
213.4.2.3 GP practices
Newham has over 60 GP practices, caring for a total registered population of
368,021 patients (as at 1.10.2015), the list size of practices ranging from 926 to
16,478 patients. The fig 3.9 below shows the geographical distribution of the
practices and with a representative of list size by circle size and colour.
Fig 3.9 Practice distribution across Newham by location and size of practice list
The full list of practices and their ownership is set out in appendix 7 Section 3 Appendix
2 Complete list of practices. Table 3.5 below gives a summary of the ownership and
partnership arrangements.
Owner/leaseholder Number of properties Number of practices Number of which are
single handed
NHS PS 12 15 4
CHP 3 8 0
(1 branch)
3rd party 18 18 5
developer/private (2 branch)
GP owned 24 24 11
Table 3.5 Summary of the ownership and partnership arrangements.
7
As taken from London Asset register v 5 October 2015- note this changes as GPs retire/merge
22NCCG has committed through its Approach to Quality Commissioning strategy to
support GPs to deliver a quality framework of services promoting improved
outcomes. Whilst there is minimal evidence to connect the quality of the estate to
successful outcomes, it has been demonstrated that patients are more likely to
attend healthcare services where these are local and familiar, thus delivering a wider
range of primary care services from larger premises will support this aim.
The fig 3.10 shows the current GP estate and a 400m and 800m zone around. This
indicates that the vast majority of the population are well within the NHS E travel
distance from a surgery (1.3 km).
Fig 3.10 400m and 800m distance zones from practices
3.4.3 Occupation, condition and utilisation 8
3.4.3.1 Occupation and ownership
Barts Health own Newham General Hospital – further work needs to be undertaken
through TST to agree opportunities for full utilisation.
8
Source of information -The London Asset base v5 identifies
23Across Newham there are four LIFT 9 premises, operated by Community Health
Partnerships (CHP) 10 which offer accommodation to GP practices, ELFT and Barts
health. These are:
• Boleyn Medical Centre
• Centre Manor Park
• East Ham Care Centre
• Vicarage Lane
There are 16 properties for which NHS Property services holds the lease, 18
premises privately rented or rented through third party developers and c20 premises
owned by individual GPs Section 3 Appendix 2 Complete list of practices
3.4.3.2 Utilisation
The chart below illustrates the net internal areas of the five largest non-acute sites in
Newham, used by a range of providers, including GP practices.
Shrewsbury Road Vicarage Lane Health
East Ham Care Centre
Health Centre Centre
LIFT
NHSPS LeaseholdLIFT LIFT
6,083m2
3,060m2 3,289m2
Sir Ludwig Guttmann
Centre Manor Park
Health Centre
LIFT
NHSPS Leasehold
2,280m2
5,211 m2
Detailed utilisation studies have been carried out by CHP on the three LIFT
properties, shown in Section 3 Appendix 3 - Utilisation reviews Occupancy utilisation is
based on 21 sessions being available over a 7 day period- thus the expectation on
Monday – Friday opening alone is 71%. NCCG is undertaking further work to
establish the utilisation of all premises, in order to inform where developments are
required, linked to service need.
The accommodation’s gross internal area (GIA), as used by GP practices (where the
information is available is set out in table 3.6 below).
9
LIFT is Local Improvement Finance Trust
10
Community Health Partnerships is a Department of Health owned company in the United Kingdom. Its role is to
set up public-private partnerships to invest in new healthcare facilities in England via the NHS Local Improvement
Finance Trust programme.
24Available space Number of practices
750m2 4
Unconfirmed 5
Table 3.6 Accommodation gross internal area (GIA)
Reviewing areas of under-utilisation within the existing estate will enable NCCG to maximise
the existing estates ahead of developing new facilities. Two key opportunities are:
• to convert under-utilised or administration space into new clinical areas
• to ensure that paper records are digitised to minimise on-site storage requirements
3.4.3.3 Asset condition
NCCG has not undertaken a full asset condition survey of GP premises (a 6 Facet survey)
since 2005, but is working with the London-wide LMC to rectify this situation early in 2016. A
6 Facet survey will review the primary care estate and assess the physical condition,
functional suitability, space utilisation, quality audit, statutory compliance, environmental
management, disabled access, reception privacy and public transport accessibility. In turn
this will facilitate the appropriate approval of practices requesting improvement grants and
primary care transformation funding.
From soft intelligence it is known that a number of premises require urgent work to rectify
maintenance issues or require critical investment to improve patient care. Investment will be
prioritised by NCCG, as part of this strategy.
3.4.4 Backlog maintenance
Backlog maintenance is the investment required by the landlord of the property or the head
lease tenant (eg NHS PS) to bring these premises up to condition B standard.
A risk-based methodology for establishing and managing backlog, provides trusts with
guidance on how to review the estate and indicate immediate and future investment
requirements. The breaking down of backlog costs together with a risk-adjusted backlog
figure is a compulsory requirement of the Estates Return Information Collection (ERIC) data
set for all trusts, including NHS foundation trusts.
Taking into account the different levels of risk to patients, visitors and staff arising from
deficiencies in statutory safety and physical condition of the built environment provides a
representation of the investment priorities and is a methodology supported by the secretary
25of state, Monitor and the CQC. This relates to the concept of risk adjusted backlog
maintenance, which focuses on where investment needs to be undertaken, based on risk.
NCCG is not responsible for this cost directly as it should be covered within the rental
agreements with GP practices 11 or within the cost for delivered services. All contractors must
comply with the NHS – GMS Premises directions 2013, schedule 1, Minimum Standards for
Practice Premises, Statutory and contractual standards12 (or the equivalent clause within
their PMS contracts). Those paid notional rents are required to bear the ‘costs of internal
repairs and decoration maintain’
However, it is a cost to the system and providers. There has been a history of under-
investment in the fabric of the buildings hence there is a high accumulated backlog cost.
TST have provided some estimates eg Barts Health has £144m in backlog cost further
details in, Section 3 Appendix 4 backlog maintenance
3.5 Financial summary
The NHS Five Year Forward View (FYFV) released in October 2014 outlines the following
three challenges facing the NHS:
1. The health and wellbeing gap: if the nation fails to get serious about prevention
then recent progress in healthy life expectancies will stall, health inequalities will
widen, and our ability to fund beneficial new treatments will be crowded-out by the
need to spend billions of pounds on wholly avoidable illness.
2. The care and quality gap: unless we reshape care delivery, harness technology,
and drive down variations in quality and safety of care, then patients’ changing needs
will go unmet, people will be harmed who should have been cured, and unacceptable
variations in outcomes will persist.
3. The funding and efficiency gap: if we fail to match reasonable funding levels with
wide-ranging and sometimes controversial system efficiencies, the result will be
some combination of worse services, fewer staff, deficits, and restrictions on new
treatments.
All planning for the future will be underpinned by these three foundations and all future
investment will have to prove that these meet these core principles.
Even with an £8bn national funding increase, the NHS in London faces a £4.76bn
affordability gap between forecast funding levels and rise in demand for healthcare by
2020/21, see Figure 3.11.
11
12
http://www.pcc-cic.org.uk/sites/default/files/articles/attachments/5196903.pdf
26Fig 3.11: NHS London funding gap There are several other areas which will contribute to the financial shortfall, these include the need to renegotiate Private Finance Initiative (PFI) contracts; the reconfiguration of estates to maximise utilisation; and making efficiencies in order to have the capacity to treat patients currently diverted to the private sector. There is also a need for provider organisations to make general efficiencies as required by Monitor (of at least 3.5%). 27
4. Drivers for Change
4.1 Introduction
Newham faces unprecedented population growth in one of the most deprived areas of the
UK, as well as epidemiological pressures due to an anticipated high birth rate and an aging
population, with poor health expectations. There is substantial financial pressure within the
local health economy, which means that finding ways to use existing resources more
effectively is urgently needed.
There are significant opportunities to invest not just in new and re-configured health
infrastructure, but to pilot new models of care and ways of working, and to harness the wider
opportunities to create healthier places and people.
The major drivers for change are the need to support:
• A significantly increasing population
• An aging and deprived population
• Progressing the out of hospital care programme
• Addressing the current use of estate and support reconfiguration of general practice
4.2 Population predictions as drivers for change
Newham’s population is growing and changing and the local NHS and its workforce need to
respond accordingly. The Greater London Authority predicts that in the next 20 years:
• The population of Newham will grow by over 100,000 residents
• Growth will occur in all age bands, but the greatest increases will be among
people of working age
• Over 65s will increase by 37,000 (60%) and form 9% of the population. There will
also be 15,000 extra children. As children and the over 65s are heavy users of
health services, this shift will significantly raise demand for health services.
There is a predicted 16.6% increase in population up to 2025 which means Newham has the
fourth highest increase across London over the period, (as set out in table 4.1 below).
Borough Population 2015-2025 2015-2035
%
2011 2015 2025 2035 Increase Increase Increase % Increase
Newham 311,912 332,582 387,738 417,415 55,156 16.6% 84,833 25.5%
Table 4.1 10 and 20 Year Population Growth (GLA 2014 round SHLAA Capped Borough Projection)
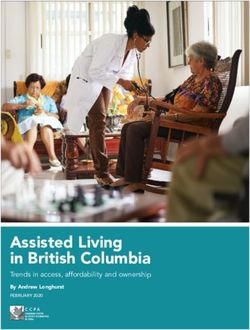
284.2.1 Distribution of Growth
Figure 4.1 shows how this growth is distributed by ward across Newham. Growth is
concentrated in the 6 wards which border the western and southern boundaries of the
borough which are within the boundaries of the London Plan Opportunity Areas (red
boundary and cross hatching) -the area is often referred to as Newham’s ‘arc of opportunity’.
Figure 4.1 Population growth 2015-2025 by ward (GLA 2014 round SHLAA Capped Projection)
Table 4.2 sets out the actual population change figures which underpin the map.
29Ward 2015 2015-2025 2015-2020 2020-2025 2015-2035
Population Change Change Change Change
(10 Years) (5 Years) (5 Years) (20 Years)
Stratford and New
Town 28,066 25,116 10,810 14,306 37,214
Royal Docks 13,311 9,998 4,599 5,399 15,638
Canning Town South 17,717 5,767 3,923 1,844 6,433
Beckton 15,589 5,074 3,611 1,463 10,581
Custom House 14,081 3,610 610 3,000 5,071
Canning Town North 16,592 2,990 1,611 1,379 4,647
Forest Gate South 18,011 945 362 583 1,168
Little Ilford 17,397 925 382 543 1,411
West Ham 16,030 712 433 279 701
East Ham Central 16,440 584 352 232 1,111
East Ham South 16,087 356 229 127 824
Plaistow South 16,760 296 392 -96 485
Plaistow North 16,077 38 187 -149 -138
Green Street East 16,651 -21 188 -209 -13
Green Street West 15,745 -54 75 -129 -138
Boleyn 16,547 -66 -118 52 -198
Wall End 15,451 -128 101 -229 -219
Manor Park 15,591 -177 23 -200 66
East Ham North 14,037 -371 -208 -163 622
Forest Gate North 16,420 -451 -130 -321 -472
Total 332,600 55,143 27,432 27,711 84,794
Table 4.2 Population Growth by Ward (GLA 2014 round SHLAA Capped Projection) 13
4.2.2 Implications of the Population Growth
This geographical pattern of growth has significant implications for the NCCG estates
strategy as the scale of growth in the arc of opportunity/growth wards is likely to require
investment in additional capacity.
Table 4.2 above shows the predicted changes for all wards and table 4.3 (below)
summarises this for the opportunity area wards:-
• Stratford and New Town is the highest growth ward by a significant margin, with growth
of over 25,000 people projected over the 10 years 2015-25 (45.5% of the total).
• Royal Docks, Canning Town South and Beckton wards are the next highest with
projected ten year growth of 9,998, 5,767 and 5,074 respectively.
• A further 2 wards (Custom House and Canning Town North) have growth of 3,610 and
2,990 respectively; with growth in Canning Town South and Beckton projected to be
significantly higher over the first the 5 years of the period 2015-25 than the second half.
13
The GLA produce different population projections variants, but recommend the use of housing-linked
projections incorporating data from the 2013 Strategic Housing Land Availability Assessment (SHLAA), short
term (five year) migration trends and using a Capped Household Size projection model (April 2015). Projections
are available at a borough and ward level. *Note discrepancies in totals may occur due to rounding
30• Growth in the Boroughs remaining 14 central and north eastern wards ranges from 945
to a decrease of 451 over 10 years. Net growth across the entire area covered by the
wards amounts to 2,588 people – ie less in total than projected growth in the 6th highest
growth ward of Canning Town North.
• The twenty year projections show a broadly similar ranking, with Stratford and New Town
remaining the highest growth ward over the second decade.
There are over 20,000 new units being built but the borough is unable to predict who
might move into these housing developments. There are houses designated for
social housing but other units will form part of the open market. Thus, it is also
difficult to make assumptions based on the size/type of dwelling, four/five bedroom
houses may not end up being occupied by families instead it may be a group of
young sharers, especially as some of the new dwellings are expensive in
comparison to other parts of Newham and some may also end up being bought by
corporations and empty for large periods at a time.
Population Estimated % Estimated %
2015 growth increase growth increase
2021 2026
Royal docks 13292 4599 34.6 9982 75.1
Stratford New
Town 28078 10810 38.5 25130 89.5
Canning Town
South 17751 3923 22.1 5787 32.6
Beckton 15565 3611 23.2 5059 32.5
Custom House 14186 610 4.3 3632 25.6
Table 4.3 Summary of the population changes in the 5 key wards – opportunity areas
Each of these has a different local planning and development context which affects the
nature of the opportunity for change.
The TST programme work described below in section 4.7 has modelled predicted increased
activity levels across a range of primary care and out of hospital services and highlighted the
relative strength of population growth as a key driver of change in Newham. Other drivers
such as shifts in outpatient activity away from hospitals are less dominant, but nevertheless
need to be considered in terms of potential estate impacts.
4.3 Future model of care and service priorities
NCCGs challenge is to commission high quality services meet the needs of its local
population and reduce health inequalities, whilst managing demand and improving
the efficiency and effectiveness of the local health system. It shares this role as local
NHS commissioner for shaping local health and public services with the LBN.
The ‘Case for Change’ showed there are significant opportunities to make patients’
experience of care safer and quicker across the health and social care system,
though for example, better access to tests and outpatients. It identifies that demand
for services will increase during the coming years with a growing population and
increasing health needs. Some services need to be provided more sustainably,
closer to home, meaning there will continue to be a shift of care away from
31You can also read