NEW DIABETES MEDICATIONS - BARBARA HETTINGER, MD PHD STAFF ENDOCRINOLOGIST, PORTLAND VA HEALTH CARE SYSTEM ASSISTANT PROFESSOR, OHSU ENDOCRINOLOGY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

New Diabetes Medications
Barbara Hettinger, MD PhD
Staff Endocrinologist, Portland VA Health Care System
Assistant Professor, OHSU Endocrinology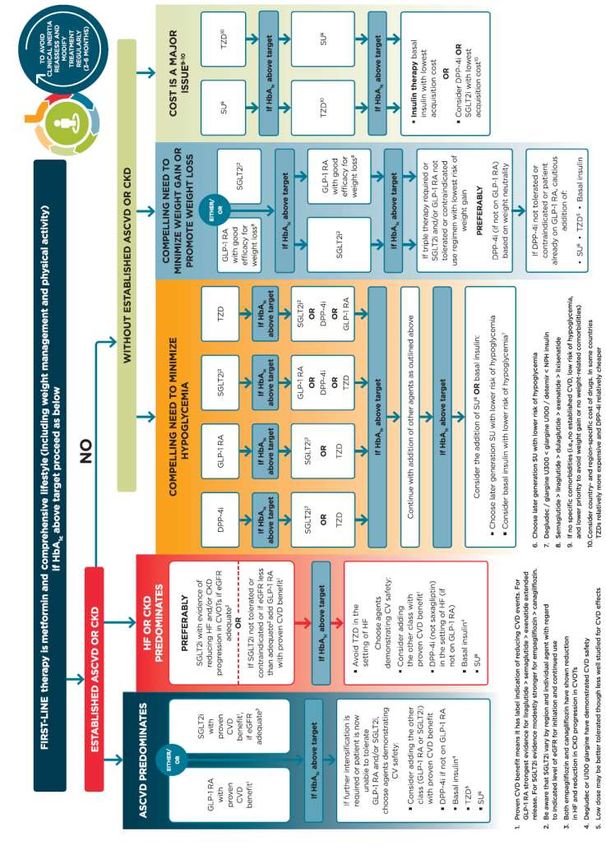
Disclosures • I have nothing to disclose.

Goals:
• Discuss patient-centered decision-making approach to choice of diabetes
management tools.
• Review ADA guidelines for medical management of type 2 diabetes with an
emphasis on the DPP-4 inhibitors, SGLT-2 inhibitors and GLP-1 agonists.
• What we will likely not have time to discuss (but I could try to answer in
the Q&A):
• It is always important to approach lifestyle changes that can be made to optimize
glycemic control and to promote microvascular/macrovascular risk reduction.
• Off label use of newer medications in type I diabetes.
• New insulin preparations
Pre-1995: Main Classes of
Glucose-Lowering Medications
α-glucosidase inhibitors DPP-4 inhibitors Biguanides
(delay digestion and (prolong GLP-1 action, stimulate (reduce hepatic
absorption of intestinal insulin secretion, suppress glucose production and intestinal SGLT-2 Inibitors
carbohydrate) glucagon release) absorption of glucose; increase (reduce plasma glucose by increased
SUs and rapid-acting
peripheral glucose uptake) urinary losses)
secretagogues
(stimulate insulin secretion)
GLP-1 analogues
(increase GLP-1 action, stimulate insulin
secretion, suppress glucagon release,
decrease appetite, delay gastric emptying) Insulin
(improves insulin secretion and TZDs
peripheral insulin sensitivity) (reduce insulin resistance
in target tissues)
Krentz AJ, Bailey CJ. Drugs 2005;65:385-411
Today: Main Classes of
Glucose-Lowering Medications
α-glucosidase inhibitors DPP-4 inhibitors Biguanides
(delay digestion and (prolong GLP-1 action, stimulate (reduce hepatic
absorption of intestinal insulin secretion, suppress glucose production and intestinal SGLT-2 Inibitors
carbohydrate) glucagon release) absorption of glucose; increase (reduce plasma glucose by increased
SUs and rapid-acting
peripheral glucose uptake) urinary losses)
secretagogues
(stimulate insulin secretion)
GLP-1 analogues
(increase GLP-1 action, stimulate insulin
secretion, suppress glucagon release,
decrease appetite, delay gastric emptying) Insulin
(improves insulin secretion and TZDs
peripheral insulin sensitivity) (reduce insulin resistance
in target tissues)
TZD = thiazolidinedione; DPP = dipeptidyl peptidase; GLP = glucagon-like peptide Krentz AJ, Bailey CJ. Drugs 2005;65:385-411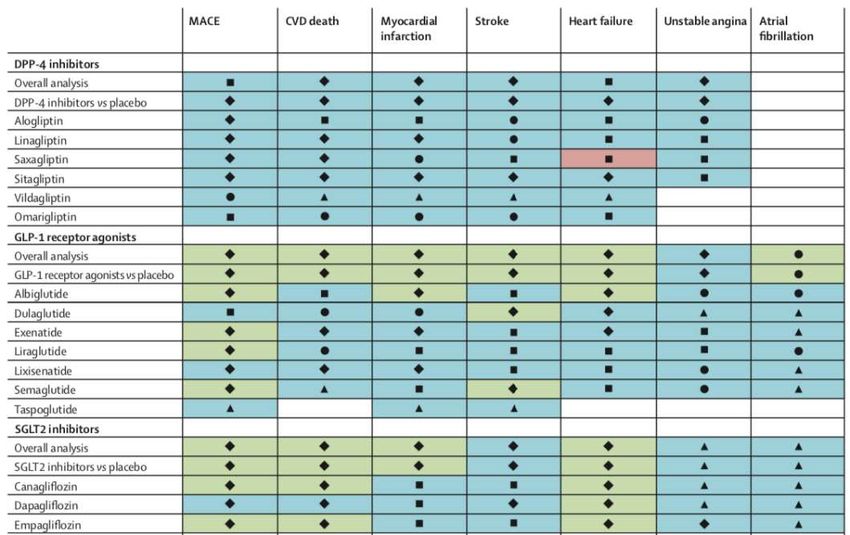
ADA Standards of Medical Care In Diabetes 2020
Case 1
• 76 yo male with type II diabetes, CAD s/p CABG 3 years prior, CKD stage II,
obesity (BMI 36) on metformin 2000 mg daily, lantus 50 units daily and
aspart 10 units tidac + somewhat arbitrary supplemental scale based on
how he feels. A1C currently 8.5% though, checking blood sugars somewhat
infrequently though on his download you note two glucose values in the
50s. He is unable to recall what preceded these low blood sugars.
• You plan a change in his regimen. Your next step would be:
a. Add acarbose 25 mg tid with meals.
b. Increase lantus to 60 units daily and discontinue metformin.
c. Introduce carbohydrate counting to the patient and ask him to use 1 unit of aspart
per 10 grams of carbohydrates.
d. Add dulaglutide 0.75 mg weekly and discontinue aspart insulin.
Case 1 – Patient Goals • Lower A1C • Reduce cardiovascular risk • Reduce complexity of medication regimen • Avoid weight gain • Minimize medication side effects • Minimize/eliminate hypoglycemia

ADA Standards of Medical Care In Diabetes 2020

Type II Diabetes: Metabolic Dysregulation • Islet cell dysfunction • Decreased relative b cell secretion of insulin • Decreased first phase of insulin release • a cell hyperfunction – increased glucagon and hepatic glucose production • Abnormal incretin secretion • Decreased GLP-1 and resistance to the action of GIP • Insulin resistance in target tissues (liver, muscle, adipose) • Glucose overproduction and underutilization • Increased fatty acid delivery to liver • Increased gluconeogenesis and hepatosteatosis
Incretin Role in Glucose Homestasis
GLP-1 Receptor Agonists • GLP-1 and GIP are secreted from L-cells in ileum/colon in response to food ingestion • Act on pancreas to stimulate glucose-dependent insulin secretion AND decrease inappropriate glucagon secretion • GLP-1 (endogenous) is degraded within minutes by DPP-4 • Gila monster saliva was noted to have a compound Exendin-4 which was resistant to breakdown by DPP-4 • GLP-1 RA are resistant to degradation by DPP-4 • Exenatide (Byetta) was the first approved GLP-1 RA in 2005.
GLP-1 RA • Short acting GLP-1 agonists – predominant effect on PPG levels • Exenatide/Byetta – 5-10 mcg twice daily • Lixisenatide/Adlyxin – 10-20 mcg once daily • Long acting GLP-1 agonists – effect on both PPG and FPG levels • Liraglutide/Victoza – 0.6-1.8 mg weekly • Exenatide XR/Bydureon – 2 mg weekly • Dulaglutide/Trulicity – 0.75-1.5 mg weekly • Semaglutide/Ozempic – 0.25-1 mg weekly • Oral GLP-1 agonist – released late 2019 • Semaglutide/ Rybelsus – 7-14 mg daily • Renal Clearance of Exenatide (and XR), Lixisenatide • Not recommended for ESRD
GLP-1 RA
GLP-1 RA Change in A1C Change in Kg GI Side Effects CV Outcomes
Exenatide -0.4 to -1.1 -0.3 to -2.8 Nausea 8-44%
AMIGO Vomiting 4-18%
Diarrhea 6-18%
Lixisenatide -0.46 to -0.99 -0.46 to -0.99 Nausea 25%
GETGOAL Vomiting 10%
Diarrhea 6-18%
Liraglutide -0.84 to -1.5 +0.3 to -3.24 Nausea 18-20% LEADER trial
LEAD Vomiting 6-9% HR 0.87 MACE
Diarrhea 10-12% HR 0.78 CV death
HR 0.78 renal
Exenatide XR -1.48 to -1.9 -2.0 to -4.0 Nausea 8.2%
DURATION Vomiting 3.4%
Diarrhea 10-12%
Dulaglutide -0.71 to -1.64 +0.2 to -3.03 Nausea 12.4-21.1% REWIND trial
AWARD Vomiting 6-12.7% HR 0.88 MACE
Diarrhea 8.9-12.6% HR 0.85 renal
Semaglutide -1.1 to -2.2 -1.4 to -6.5 Nausea 15.8-20.3% SUSTAIN-6 trial
SUSTAIN Vomiting 5-9.2% HR 0.74 MACE
Diarrhea 8.8-8.9% HR 0.64 renalGLP-1 RA Advantages Disadvantages Preserve b cell function GI side effects (N/V, diarrhea, constipation?) Target multiple pathophysiologic defects Immunogenicity risk A1C lowering Potential pancreatitis risk Body weight advantage Thyroid C-Cell tumors Low risk of hypoglycemia Most require SQ injection CV and renal benefit Different injection pen devices Once weekly administration for some Cost
Cardiovascular Benefit of GLP-1 RA
• The American Diabetes Association (ADA) and the European Association for the
Study of Diabetes (EASD) position statements on the management of type 2
diabetes (T2DM) in adults, now include additional focus on cardiovascular risk
factor management
• LEADER trial (Liraglutide)
• Marso SP et al. N Engl J Med 2016;375:311-322
• SUSTAIN-6 (Semaglutide)
• Marso SP et al. N Engl J Med 2016;375:1834-44
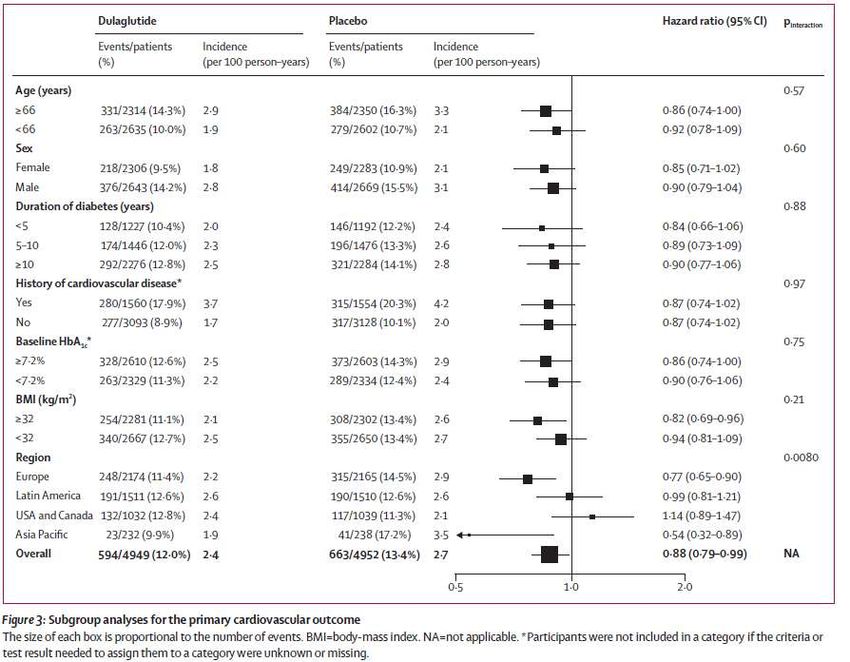
• REWIND (Dulaglutide)
• Gerstein HC et al. Lancet 2019; 394: 121–30
• Primary outcomes similar in patients with or without prior CV disease, so might be
effective for both primary and secondary prevention (longer trial follow up period)
• Reduced CV events for patients both within range and higher range A1c targetsGerstein HC et al. Lancet 2019; 394: 121–30
Endocrine SCAN-ECHO
What’s New?
N Engl J Med 2019;381:841-51.Meta analysis of 113 studies of these agents 1. Pancreatitis: 72 studies reported no events, 13 without information • GLP1 treated 60/17,623, vs 55/15,569 for comparator 2. Cholelithiasis: reported in 90 trials • GLP1 treated 141/17,232, vs 99/14,872 for comparator 3. Pancreatic Cancer: 81 trials reported no events, not available in 18 • GLP1 treated 24/14,866, vs 23/12,849 for comparator
Concerns/Limitations for GLP-1 RA
1. Pancreatitis – currently insufficient data to know if causal relationship
• Incidence of pancreatitis is low 16/14,562 among patients enrolled in trials
• In a meta-analysis of 113 trials using GLP-1 agonists, incidence of pancreatitis is not different between treatment and
comparator arms (Monami et al 2017 Diabetes Obes Metab. 19:1233-1241)
2. Pancreatic Cancer – FDA and European Medicines Agency state insufficient data to confirm
increased risk of pancreatic cancer with use of GLP-1 agonists
• Meta-analysis of cardiovascular outcomes trials found no significant difference in severe hypoglycemia, pancreatitis, pancreatic
cancer, or medullary thyroid cancer reported between GLP-1 receptor agonist treatment and placebo (Bethel et al 2017 Lancet
Diabetes Endocrinol. Dec 2017)
3. Renal Insufficiency – Exenatide should not be used in patients with creatinine clearanceSummary • Incretin based therapies provide glucose-dependent glucose lowering with low risk of hypoglycemia. • Cardiovascular benefit has been demonstrated for dulaglutide, semaglutide and liraglutide. • Weight reduction/appetite suppression is a side effect. • Cost, GI tolerance and need for injection seem to be biggest barriers to use.
Case 2 • 62 yo postmenopausal woman with type II diabetes, CAD s/p PCI. Diabetes is complicated by mild neuropathy and microalbuminuria. She has a 30 pack year history of tobacco use. Her BMI is 29, BP is 160/80. She is currently on metformin 2000 mg daily, alogliptin 25 mg daily and has a fear of injections and wishes to avoid them at all cost. A1C is 8.5%. • Your next recommendations would be: A. Tell her that insulin is the next logical step. She can get used to needles. B. Discontinue metformin, start glimepiride. C. Add empagliflozin to metformin and alogliptin. D. Adjusting her anti-hypertensives and referring her to smoking cessation.
DPP-4 Inhibition • Nutrient ingestion leads to secretion of gut derived hormones which: • Increase insulin secretion from islet b cells in a glucose dependent manner • Reduce glucagon secretion for islet a cells • Incretin effect is impaired in type II diabetes • Glucagon-like peptide-1 (GLP-1) • Glucose-dependent insulinotropic peptide (GIP)
DPP-4 Inhibitors • Sitagliptin/Januvia * (2006) • Saxagliptin/Onglyza * (2009) • Linagliptin/Tradjenta (2011) • Alogliptin/Nesina * (2013) • Dose adjustment recommended based on eGFR* for some. • Generally well tolerated, minimal GI symptoms if any. Very low risk of hypoglycemia – glucose dependent glucose lowering. • Modest A1C reduction. • EXAMINE, TECOS, SAVOR-TIMI 53 – no cardiovascular outcome benefit of DPP-4 inhibitors (alogliptin, sitagliptin, saxagliptin)
Efficacy and safety of adding the dipeptidyl peptidase‐4 inhibitor
alogliptin to metformin therapy in patients with type 2 diabetes
International Journal of Clinical Practice, Volume: 63, Issue: 1, Pages: 46-55Efficacy and safety of the dipeptidyl peptidase‐4 inhibitor alogliptin in
patients with DM2 inadequately controlled by glyburide monotherapy
Diabetes, Obesity and Metabolism, Volume: 11, Issue: 2, Pages: 167-176Alogliptin Combination therapy with Pioglitazone The Journal of Clinical Endocrinology & Metabolism, Volume 97, Issue 5, 14 March 2012, Pages 1615–1622, https://doi.org/10.1210/jc.2011-2243
NEJM 2013 369(14):1327-35 White WB, et al
NEJM 2013 369(14):1327-35 White WB, et al
GLP-1 Receptor Analogues vs DPP-4 Inhibitors
Properties/Effects DPP-4 Inhibitors GLP-1 Analogues
↑ Glucose-dependent insulin Yes Yes
secretion
↓ Glucagon secretion Yes Yes
Effect on incretins Endogenous incretins enhanced to Exogenous GLP-1:
physiological levels Possible Immune response (antibody
formation)
Effect on body weight Weight neutral, or mild loss Body weight decreased
Inhibition of gastric emptying Marginal Yes
Hypoglycemia No No
Side Effects Minimal nausea, vomiting Reported nausea, vomiting
Administration Oral Subcutaneous
Barnett A Clinical Endocrinology 2009; 70: 343–53
34Liraglutide vs Sitagliptin (GLP-1 RA vs DPP-4 inhibitor)
In this parallel-group, open-label trial, participants with T2 DM who had inadequate glycemic
control on metformin were randomly allocated to receive 26 weeks’ treatment with 1.2 mg or 1.8
mg subcutaneous liraglutide once daily, or 100 mg sitagliptin once daily.
Pratley RE et al Lancet 2010; 375: 1447–56
Liraglutide was superior to sitagliptin for reduction of HbA1c & FPG.
35Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, et al; SAVOR-TIMI 53 Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369:1317-26.
Scirica BM et al. N Engl J Med 2013;369:1317-1326 Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, et al; SAVOR-TIMI 53 Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369:1317-26.
FDA Alert Diabetes Medications Containing Saxagliptin and Alogliptin: Drug Safety Communication - Risk of Heart Failure [Posted 04/05/2016] Including: • Onglyza (saxagliptin) • Kombiglyze XR (saxagliptin and metformin extended release) • Nesina (alogliptin) http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm494252. • Kazano (alogliptin and metformin) htm?source=govdelivery&utm_medium=email&utm_source=govdelivery • Oseni (alogliptin and pioglitazone) AUDIENCE: Pharmacy, Internal Medicine, Patient, Endocrinology ISSUE: An FDA safety review has found that type 2 diabetes medicines containing saxagliptin and alogliptin may increase the risk of heart failure, particularly in patients who already have heart or kidney disease. As a result, FDA is adding new warnings to the drug labels about this safety issue. This Communication is an update to the 02/11/2014 FDA Drug Safety Communication. BACKGROUND: Saxagliptin and alogliptin are part of the class of dipeptidyl peptidase-4 (DPP-4) inhibitor drugs, which are used with diet and exercise to lower blood sugar in adults with type 2 diabetes. FDA evaluated two large clinical trials conducted in patients with heart disease. These clinical trials were also discussed at the FDA Endocrinologic and Metabolic Drugs Advisory Committee meeting in April 2015. Each trial showed that more patients who received saxagliptin- or alogliptin-containing medicines were hospitalized for heart failure compared to patients who received an inactive treatment called a placebo (see Data Summary in the FDA Drug Safety Communication for additional information). In the saxagliptin trial, 3.5% of patients who received the drug were hospitalized for heart failure versus 2.8% of patients who received a placebo. This is the same as 35 out of every 1,000 patients compared to 28 out of every 1,000 patients. Risk factors included a history of heart failure or kidney impairment. In the alogliptin trial, 3.9% of alogliptin-treated patients were hospitalized for heart failure versus 3.3% in the placebo group. This is the same as 39 out of every 1,000 patients compared to 33 out of every 1,000 patients. RECOMMENDATION: Health care professionals should consider discontinuing medications containing saxagliptin and alogliptin in patients who develop heart failure and monitor their diabetes control. If a patient’s blood sugar level is not well-controlled with their current treatment, other diabetes medicines may be required. Patients taking these medicines should contact their health care professionals right away if they develop signs and symptoms of heart failure such as: • Unusual shortness of breath during daily activities • Trouble breathing when lying down • Tiredness, weakness, or fatigue • Weight gain with swelling in the ankles, feet, legs, or stomach Patients should not stop taking their medicine without first talking to their health care professionals.
Umbrella review: 232 meta-analyses evaluating ten classes of diabetes drugs
“individual DPP-4 inhibitors were neutral for all cardiovascular outcomes except for heart failure,
which was increased by saxagliptin (relative risk [RR] 1.22; 95% CI 1.03-1.44)”
Lancet Diabetes and Endocrinology 2020; 192-205Other Cautions https://www.fda.gov/Drugs/DrugSafety/ucm343187.htm
Dipeptidyl peptidase‐4 inhibitors and pancreatitis risk:
a meta‐analysis of randomized clinical trials
Diabetes, Obesity and Metabolism
Volume 16, Issue 1, pages 48-56, 28 JUL 2013Case 2 • 62 yo postmenopausal woman with type II diabetes, CAD s/p PCI. Diabetes is complicated by mild neuropathy and microalbuminuria. She has a 30 pack year history of tobacco use. Her BMI is 29, BP is 160/80. She is currently on metformin 2000 mg daily, alogliptin 25 mg daily and has a fear of injections and wishes to avoid them at all cost. A1C is 8.5%. • Your next recommendations would be: A. Tell her that insulin is the next logical step. She can get used to needles. B. Discontinue metformin, start glimepiride. C. Add empagliflozin to metformin and alogliptin. D. Adjusting her anti-hypertensives and referring her to smoking cessation.
SGLT-2 Inhibitors
• Kidneys critical for glucose
homeostasis
• Glomerular filtration
• Reabsorption of glucose in PCT
• Urine glucose excretion
• Nondiabetic adult filters 180 grams
glucose/day and reabsorbs 99%
• SGLT2 segments 1&2 PCT kidney
• High capacity, low affinity
• SGLT1 segment 3 PCT kidney and GI
tract
• Low capacity, high affinity
• GLUT on basolateral membrane into
capillary (GLUT1 and 2)
Clinical Diabetes 2010;28(1):5-10SGLT-2 Inhibitors • SGLT-2 inhibitors prevent re-absorption of 30-50% of filtered glucose • Canagliflozin/Invokana – 100-300 mg daily • Dapagliflozin/Farxiga – 2.5-10 mg daily • Empagliflozin/Jardiance – 10-25 mg daily • Ertugliflozin/Steglatro – 5-15 mg daily • SGLT-1/2 inhibitor – Sotagliflozin – in development • Action in gut and kidney
SGLT-2 Inhibitors
Advantages Disadvantages
• A1C lowering 0.6-1.0% • Cost
• FPG lowering 19-35 mg/dL • Lower limb amputation
• Canagliflozin, ertugliflozin
• Weight loss 2-3.9 kg • Hypotension/AKI
• Minimal hypoglycemia • Ketoacidosis
• Oral formulation, daily dosing • Urogenital infections
• Positive CV outcomes • Hyperkalemia
• Canagliflozin
• Positive renal outcomes • Fracture
• Canagliflozin
• Bladder cancer
• DapagliflozinNEJM 2015;373:2117-2128.
NEJM 2017;377(7):644-657
J Am Heart Assoc. 2020;9:e014908. DOI: 10.1161/JAHA.119.014908
Arnott et al. J Am Heart Assoc. 2020;9:e014908. DOI: 10.1161/JAHA.119.014908
Umbrella review: 232 meta-analyses evaluating ten classes of diabetes drugs
Lancet Diabetes and Endocrinology 2020; 192-205Renal Outcomes of SGLT-2 Inhibition:
Meta-analysis including EMPA-REG, CANVAS, DECLARE-TIMI58
Composite of worsening of renal function, ESRD, or renal death
Meta-analysis OR 1.34 for UTIs SGLT-2 vs placebo and OR 1.42 compared to other medications.
Zelniker et al.Lancet 2019; 393:31-39.And Now The Bad News…
Arnott et al. J Am Heart Assoc. 2020;9:e014908. DOI: 10.1161/JAHA.119.014908Urogenital Infections with SGLT-2 Inhibitors • Meta-analysis: OR 1.34 for UTI SGLT-2 vs placebo • Meta-analysis: OR 3.5 for genital infections SGLT-2 vs placebo • Dapagliflozin: 2.5 mg 3.6%, 5 mg 5.7%, 10 mg 4.3%, placebo 3.7% • Empagliflozin: 10 mg 9.3%, 25 mg 7.6%, placebo 7.6% • Canagliflozin: 100 mg 5.9%, 300 mg 4.3%, placebo 4.0% • Ertugliflozin: 5 mg 4.0%, 15 mg 4.1%, placebo 3.9% • Females > Males • Typically mild and do not necessarily result in discontinuation
Lancet Diabetes and Endocrinology 2020; 8:192-205
Summary • In the past 25 years, there have been some exciting changes in pharmaceutical options for patients with diabetes. • Diabetes education regarding behavioral as well as pharmaceutical options remains an important component of diabetes care. • DPP-4 inhibitors are fairly well tolerated agents that can provide mild- moderate glycemic improvement. • GLP-1 receptor agonists and SGLT-2 inhibitors have demonstrated cardiovascular and renal benefit and have a positive weight benefit but are expensive.
You can also read

















































