NATIONAL STRATEGIC PLAN FOR MEASLES ELIMINATION AND RUBELLA/CRS CONTROL 2015 -2020
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

1
NATIONAL STRATEGIC PLAN FOR
MEASLES ELIMINATION AND
RUBELLA/CRS CONTROL
2015 -2020
1st draft 18th June, 2014
2nd draft 24th August 20142
Contents
1. Country profile............................................................................................................................... 4
2. National Health Systems ............................................................................................................. 5
3. Epidemiology of Measles and Rubella ...................................................................................... 7
4. Support from International Collaborating partners ................................................................ 10
5. Feasibility of Measles elimination and Rubella/CRS control ............................................... 10
Operational feasibility .................................................................................................................... 10
1. Contextual ........................................................................................................................... 10
2. General health system....................................................................................................... 10
4. Research institutions ......................................................................................................... 11
6. Guiding Principles ...................................................................................................................... 12
7. Key Assumptions ........................................................................................................................ 12
Strategic Plan, Vision, Mission, Goal and Objectives ............................................................ 13
1. Vision: ......................................................................................................................................... 13
2. Mission: ...................................................................................................................................... 13
3. Goal: ............................................................................................................................................ 13
4. Outcome Objectives:............................................................................................................... 13
5. Broad key strategies and main activities: ......................................................................... 13
5.1 Achieve and maintain two doses of measles and rubella vaccination coverage
at >95%. .......................................................................................................................................... 14
5.1.1 Micro-stratification and targeted immunization intervention for low MR
vaccine coverage ..................................................................................................................... 14
5.1.2 Accelerate immunization intervention to reach out children who are not
vaccinated .................................................................................................................................. 15
5.1.3 Sustain routine high MR vaccine coverage ...................................................... 15
5.1.4 Operational research on vaccine coverage and management .................... 16
5.2 Intensify surveillance and investigation of Measles and Rubella/CRS ............. 16
5.2.1 Scale up existing MR and CRS surveillance system ............................................ 17
5.2.2 Institute active case detection, investigation and immunization response ... 17
5.2.3 Strengthen AEFI surveillance ............................................................................... 18
5.2.4 Improve data management, reporting and feedback system ....................... 18
5.2.5 Strengthen capacity to investigate outbreak and response ......................... 19
5.3 Provide quality assured laboratory diagnosis and case management ............. 19
5.3.1 Maintain accreditation of national measles and rubella laboratory ................. 193
5.3.2 Maintain institutional linkage with regional reference laboratory .................... 20
5.3.3 Strengthen local laboratory network on sample collection and shipment ..... 20
5.3.4 Ensure prompt case management ............................................................................ 21
5.3.5 Genotyping of Measles and Rubella virus............................................................... 21
5.4. Intensify advocacy and risk communication for measles elimination and
Rubella/CRS control .................................................................................................................... 22
5.4.1 Develop communication plan and intervention tools .......................................... 22
5.4.2 Engage community participation in vaccination advocacy ................................ 23
5.4.3 Sensitise and advocate local government and policy makers .......................... 24
5.4.4 Dissemination of communication materials through mass media and
appropriate information technology. .................................................................................. 24
5.5 Enhance institutional capacity and Monitoring & Evaluation .............................. 24
5.5.1 Strengthen programme capacity ............................................................................... 24
5.5.2 Strengthen vaccine inventory management ........................................................... 25
5.5.3 Strengthen regulatory system .............................................................................. 25
5.5.4 Improve cold chain management and logistic ................................................. 26
5.5.5 Strengthen M & E ..................................................................................................... 27
5.6 Strengthen governance and collaboration with international organizations to
achieve regional and global elimination targets and indicators .................................... 27
5.6.1 Garnering political support and resource mobilization ................................. 27
5.6.2 Institution of appropriate governing structure................................................. 28
5.6.3 Align and collaborate with various stakeholders and international
organization to support elimination target........................................................................ 29
Annex I: Monitoring Indicators .......................................................................................................... 29
Annex II: Estimated Costing Matrix ................................................................................................. 344 1. Country profile Bhutan is located in the eastern Himalaya with a total area of 38, 394 km2 and shares a common border with China to the north and India to the west, south and east. Administratively the country is divided into three regions, twenty "Dzongkhag" (District) and 205 Gewogs (Blocks). Gewog and Thromde (municipality area) is the lowest administrative block. The country has mainly three geographical climatic features with subtropical hot and humid conditions in the southern belt, cool temperate climate in the central and snow capped mountains with cold alpine climate in the north. Since the country is located in the heart of Himalaya, it has difficult geographical terrain which has not only developed unique socio-cultural diversities but also presents different health condition and often inaccessibility especially remote localities. The Population and Housing Census conducted in 2005 enumerated a population of 672,450 with 37,443 as floating population. The population is estimated to have grown to 720 679 in 2012 with about 70% people living in rural areas. Life expectancy has increased from 66 years in 1999 to 68 years in 2012 and the population growth rate has stabilized to around 1.3 % from 3.1% in 1994 as per 2012 National Health Survey. Bhutan is also on track to achieve most of the MDG targets by 2015 however malnutrition in children, infant mortality rate, under five mortality rate are some of the challenges to achieve the targets. Bhutan has created a series of Five Year Plans detailing its economic and development strategies since the 1960s. Bhutan has seen rapid economic and social development particularly in the last decade. The Gross Domestic Product (GDP) in 2012 was about US $ 1779.6 million. The economy is mainly based on agriculture, but also depends on forestry, tourism and hydroelectric power. The developmental activities are more significant in the western Bhutan, especially in Thimphu and Phuntsholing. This has resulted in the population movements towards these economic zones especially from the Eastern Bhutan with about 63% net in-migration to Thimphu as per the 2005 Population and Housing Census.
5
2. National Health Systems
Bhutanese people have free health care services from primary to tertiary level health
care as the right enshrined in the Constitution of the country, which states, " the
State shall provide free access to basic public health services in both modern
and traditional medicine" and “the state shall endeavour to provide security in
the event of sickness and disability or lack of adequate means of livelihood for
reasons beyond one’s control”.
The Bhutan health policy statement states that Bhutan shall continue to pursue the
comprehensive approach of Primary Health Care, provide universal access with
emphasis on disease prevention, health promotion, community participation and
intersectoral collaboration and with health services provided with integration of
modern and tradition health care systems that responds equitably, appropriately and
efficiently to the needs of all Bhutanese citizens.
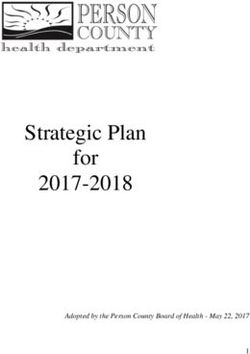
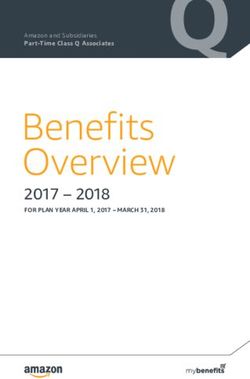
The health care is delivered through three tiered system namely; the primary,
secondary and tertiary providing preventive, promotive and curative services as
shown in figure (1) below.
Tertiary ( National and Regional
Level)
• National referral Hospital (1)
• Regionnal Referral Hospital (2)
Secondary ( District Level)
• District level Hospital (32)
• District Health Office (20)
Primary ( Block and community
level)
• Basic Health Units (192)
• Out breach clinics (550)
Figure 1: Pyramid of Health care delivery system6 To provide deliver health care services, health infrastructure are spread across the country including the remote places (figure 2). With wide coverage of health facilities across the country, most people have reasonable access to health services with only 4.6% of Bhutanese population living at a distance of more than 3 hours from the nearest health facility and 81.5 % of the population seeking help from the health professionals as the first line of treatment (National Health Survey 2012). The current health workforce working in the above heath facilities consists of 194 doctors, 736 nurses, 578 basic health unit workers, 807 technical categories and 98 traditional health workers. Figure 2: Map of Health infrastructure
7
Table 1: The main indicators as per the National Health Survey 2012
Year
Indicators
1984 1994 2000 2012
Crude rate of natural increase 2.6 3.1 2.5 1.2
Total fertility rate (Births per - 5.6 4.7 2.3
women)
Crude death rate 39.1 39.9 34.1 17.9
Infant Mortality rate/1000 live births 102.8 70.7 60.5 30.0
Under-five mortality rate 162.4 96.9 84.0 37.3
Maternal Mortality Ratio/100000 live 777 380 255 86
births
3. Epidemiology of Measles and Rubella
Measles vaccination program in Bhutan was started in 1979 along with BCG, DPT &
OPV. Measles vaccine was given as single dose at 9 months of age through routine
immunization services. During early phase of immunization programme, measles
vaccination coverage was found very low in most districts ranging from 24%- 83%.
With the implementation of EPI acceleration plan in 1988, measles vaccination
coverage increased to 89% in 1991 as per the first EPI survey report. In 2006,
Bhutan introduced rubella vaccine as combined MR vaccine.
To rapidly reduce measles morbidity and mortality, Bhutan has conducted three
nationwide measles vaccination catch up campaign using monovalent measles
vaccine in 1995 and 2001 and MR vaccine in 2006 coinciding with introduction of
rubella vaccination. Further in 2006, second dose of measles vaccine was
introduced with combined MR vaccine at 24 months. The second EPI coverage
survey conducted in 2002 reported measles vaccine increased to 92%. Since then,
the measles coverage was sustained at more than 90% which was authenticated by
EPI coverage survey conducted 2008 which reported measles rubella vaccine
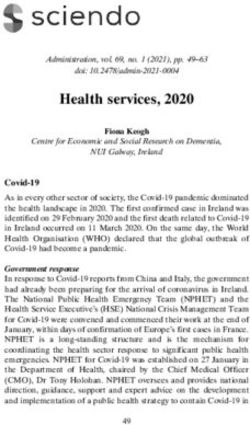
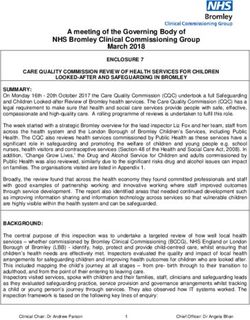
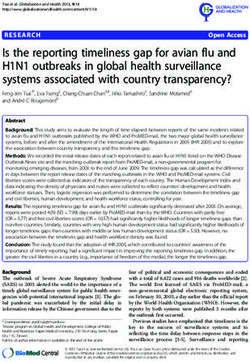
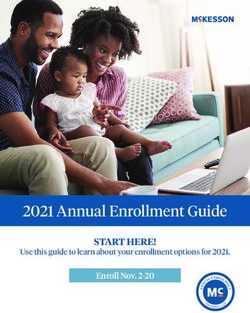
coverage at 95% (Figure 3). Further, the recent National Health Survey conducted in
2012 reported first measles rubella vaccine dose (MR1) coverage at 97%.8
120 65 70
99% 94.7%95% 95% 95% 97% 60
100 93% 90% 95%
88% 89%
Vaccien Coverage (%)
53
78% 78% 50
Number of cases
80 71% 76% 76% 85% 88%
89% 89%
40
60
30
22
40 20
20
13
20 9 10 4
6 2 10
4 3 3 9 6
0 22 7 13 0
0 0
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Year
Lab confirmed measles cases Lab confirmed rubella cases MR1 MR2
Figure 3: MR vaccine coverage and cases from 1998 - 2013
With consistent maintenance of high MR vaccine coverage, measles and rubella
cases have declined to very minimal cases. As per the WHO measles elimination
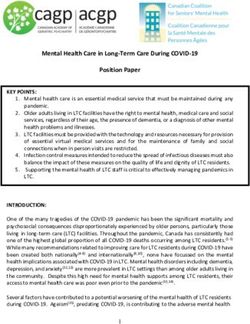
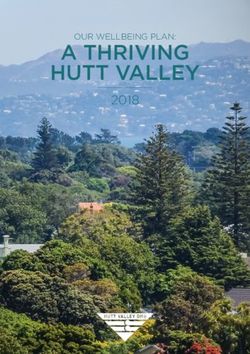
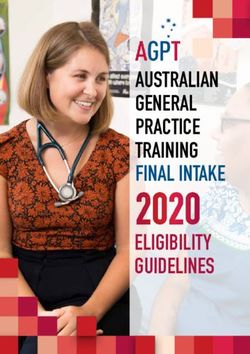
target of measles incidence {9
16
14
12
Number of cases
10
8
6
4
2
0
26yrs
Age group
2006 2007 2008 2009 2010 2011 2012 2013
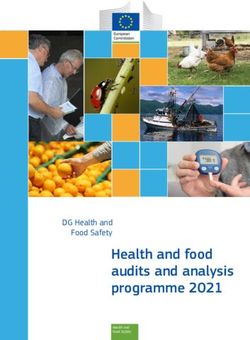
Figure 4: Age break down of measles cases from 2006-2013
Simialrly, common affected age group by rubella is among children under 5 years but
cases are prevalent among 6-10 years of age (figure 5) which is observed during
early phase of rubella vacciantion introducution and this will decline over the years.
4.5
4
3.5
Number of cases
3
2.5
2
1.5
1
0.5
0
26yrs
Age group
2006 2007 2008 2009 2010 2011 2012 2013
Figure 5: Age break down of rubella cases from 2006-2013
Bhutan has maintained measles rubella vaccine coverage more than 90% for more
than eight years and already achieved the regional target of measles morbidity and
mortality reduction in 2007. As one of the SEARO member state to adopt measles10
elimination prior to region target by 2020, Bhutan has already embarked in the pre-
elimination stage and target to eliminate measles in the country by 2016.
4. Support from International Collaborating partners
The success of VPDP was mainly due to the support from the national and
international collaborating partners. The main international collaborating partners are
WHO, UNICEF and JICA which provided both fund and technical support.
5. Feasibility of Measles elimination and Rubella/CRS control
After the introduction of immunization programme in 1979, Bhutan has come a long
way to achieve and sustain measles and rubella vaccine coverage >95% with no
measles cases reported since 2013 and no deaths since 1986. The last CRS cases
reported is in 2009 and 3 rubella lab confirmed cases reported in 2013. Furthermore,
the socio-economic status of the people has improved dramatically from one of the
poorest nation to a low middle income country along with improvements in all the
health, education and socio-economic indicators. External review of Vaccine
Preventable Disease Programme conducted by WHO in 2012 also found measles
elimination feasible in Bhutan.
Operational feasibility
1. Contextual
Political and social stability in the country - favourable
Effective government with clear geographical demarcations and division of
responsibilities - favourable
Good, collaborative relations with countries from where carriers could be
imported–favourable
2. General health system
Governance
o Politically and technically strong leadership; political stability -
favourable
o Culture of relying on evidence and reliable HIS data - favourable
Health services
o Geographically, economically and culturally accessible - favourable11
Human resources for health
o Sufficient, educated, trainable, motivated, properly remunerated, stable -
favourable
3. Vaccine Preventable Disease Programme (VPDP)
Technical and administrative capacity and leadership – favourable with
additional technical expert provided
Able to mobilize financial resources – favourable since UNICEF and JICA
is also providing fund other than WHO. Also Health Trust fund is
operational for traditional vaccine.
Enough fiscal space (can be authorized to expand budget as required) -
favourable
Excellent Laboratory service to diagnose measles and rubella or strategy for
achieving that – favourable, Infectious Diseases Serology Laboratory
under the Public health Laboratory is WHO accreditated National
Measles Laboratory.
Excellent surveillance or strategy for achieving that – favourable, needs
further improvement
Good epidemiological support – Not favourable. Need capacity building
Good management of preventive and curative services including supply chain
and human resources - favourable
Good capacity in communication and advocacy – favourable with some
improvement
Good information technology support including case mapping to stratify the
problem. - favourable, needs further improvement
4. Research institutions
a. Good research capacity for public health problems in the country -
Needs further improvement
b. Capacity for genotyping measles and rubella - Needs to be
established12
6. Guiding Principles
Achievement of Measles elimination and rubella/CRS control targets set in the
strategic plan will be guided by the following broad principles:
Forge National ownership of Measles elimination through
establishment a Measles Elimination Commission to garner political
support, resources and provide oversight and accountability
The Vaccine Preventable Disease Program, CDD, DoPH shall
coordinate the consultative planning, implementation, research,
monitoring and evaluation of Measles and rubella/CRS elimination
and control activities.
Build strong mechanisms for partnerships with line Ministries and
agencies for effective implementation of this plan.
Strengthen decentralized measles elimination and rubella/CRS
control with district health taking the onus of elimination and control
activities.
Collaborate with neighboring countries, international organizations
and agencies.
Utilize modern technology for surveillance, disease notification,
conduct research and epidemiology analysis to generate evidences
to guide measles elimination and rubella/CRS control strategies and
interventions.
7. Key Assumptions
The following key assumptions are important to achieve measles elimination and
rubella/CRS control within the time frame of this National Strategic Plan and sustain
beyond:
Continued political commitment by leadership at all levels to support
the national strategic plan and provide adequate financial and
human resources
Continued international support both in technical and financial
aspects
Further improvement in the socio-economic developments of the
people of Bhutan13
Strategic Plan, Vision, Mission, Goal and Objectives
1. Vision:
Bhutan free of indigenous Measles, Rubella and zero CRS
2. Mission:
Achieving elimination of measles and control of rubella through intensification of
immunization and surveillance system including laboratory capacity and strengthen
institutional collaboration to prevent reintroduction of measles and reduction of
rubella and CRS.
3. Goal:
To achieve zero indigenous Measles by 2016 and WHO certification by 2020, and
reduction of rubella and CRS until it is no longer public health problem.
4. Outcome Objectives:
1. To achieve measles elimination by 2016
2. To achieve and maintain two doses of measles and rubella vaccination
coverage at >95% from 2016 onwards
3. To achieve rubella/CRS control as no longer public health problem by 2016.
4. To further strengthen institutional capacity including surveillance and
laboratory to sustain measles elimination and rubella/CRS control.
To support the above objectives, the following strategies will be implemented and if
necessary will be reviewed every two years:
5. Broad key strategies and main activities:
The main strategies include achieving two doses of measles and rubella
vaccination coverage more than 95% through micro-stratification particularly MR2
and intensify surveillance and investigation of every measles, and rubella/CRS
case by use of web-based mobile networks for real time reporting. The
surveillance will be backed by quality assured laboratory and effective case
management at the health facility by the health worker. The governance
structures to provide elimination oversight will be instituted at all levels and14
monitoring, evaluation and supervision will be strengthened. Advocacy and risk
communication on measles elimination and rubella/CRS control will be
strengthened to sensitize and maximize community participation in measles
elimination and rubella/CRS control activities. Further, research capacity will be
strengthened to keep measles on the agenda beyond the elimination phase. The
specific strategies and activities for each strategy are described here below.
5.1 Achieve and maintain two doses of measles and rubella vaccination
coverage at >95%.
The studies have shown that the average sero-conversion rate with measles
vaccination at 9 months was found to be 85%. Thus, approximately 15% of
vaccinated children would remain susceptible to measles and rubella infection in
spite of receiving one dose of MR vaccine. However, sero-conversion rate improves
to >95% when the vaccine is given after one year of age, but the first dose has to be
given earlier to protect infants. Therefore, 2nd dose of MR has been recommended
at 24 months to cover those sero-conversion failure cases and achieve high
measles and rubella vaccine coverage.
In Bhutan, MR1 coverage is above 95% but MR2 coverage is still below 90%.
Therefore, to improve MR2 coverage, micro stratification and targeted immunization
will be conducted at district level.
5.1.1 Micro-stratification and targeted immunization intervention for low
MR vaccine coverage
Micro planning and stratification will be focussed in districts with low coverage of MR
vaccination such as Haa, Gasa, Tashiyangtse and Pemagatsel. Micro stratification
will be conducted for every gewog (Block) of those districts through active
engagement of the village health workers/ community leaders. This will ensure that
the unreached population is reached through targeted intervention. Mop up
campaigns will also be conducted at the gewogs level especially the unreached
population consisting of migrant population and road side workers. The adequate
vaccine and logistic supply to the Basic Health Units and outreach clinics will be
assured by district health office and programme.15
Key Activities:
1. Identification of low MR vaccine coverage areas/chiwog/gewog in district that
has coverage16
>95% nationally and 90% at the district level. In order to sustain high MR coverage,
adequate quality vaccine supply will be maintained in all health facilities. Regular Out
Reach Clinics (ORC) session will be conducted to maintain high coverage. Further,
the vaccine inventory management system will be strengthened through the
development of web based reporting at the district level to facilitate in vaccine
procurement and remobilization and cold chain inventory.
Key Activities:
• Procurement of MR vaccines and cold chain equipment
• Develop web based reporting system and training of health workers on web
based reporting
• Training of health workers on immunization techniques and cold chain
equipment preventive maintenance.
• Periodic monitoring (quarterly/Annually) and supervision from central to the
districts and district to BHUs
• Observation of Global Immunization Weeks and World Mothers Day to
sensitize the mothers on the importance of vaccination.
5.1.4 Operational research on vaccine coverage and management
In order to achieve measles elimination status by 2016, need based operational
research has to be planned and conducted to understand the local context and
generate strategic information to facilitate and promote evidence based planning and
decision making.
Key Activities:
• Conduct measles coverage survey
• Conduct study on MR immunity among general population
• Conduct study on effectiveness of Vaccine Vial Monitor (VVM)
• Conduct study on Vaccine wastage and utilization and Effective Vaccine
Management (EVM)
5.2 Intensify surveillance and investigation of Measles and Rubella/CRS
Good surveillance system with data management is critical for achieving measles
elimination and rubella.CRS control. Monitoring progress towards achieving17
elimination can only be accomplished in the presence of a surveillance system that
meets measles elimination and rubella/CRS control targets defined by WHO.
Integrated epidemiological and laboratory-based surveillance is also required to
provide the necessary sensitivity and specificity to ensure that measles and rubella
virus is detected.
5.2.1 Scale up existing MR and CRS surveillance system
The existing Measles, Rubella and CRS surveillance system is a passive
surveillance system. As a preparatory step towards measles elimination and
rubella/CRS control, the existing surveillance system will be scaled up to an active
surveillance where every measles, rubella and CRS cases will be reported
immediately and investigated within 24-48 hours. Case based surveillance has been
instituted but it is not implemented at the moment because clinicians and health care
workers are not aware and trained on it. Clinicians and health workers will also be
trained on case based surveillance and investigation. As part of active case finding,
VHW will be involved in detecting and referring fever with rashes and signs of CRS
Key Activities:
• Revise Measles and Rubella CRS surveillance guideline and develop
appropriate training modules for health workers
• Training of health workers on revised MR and CRS surveillance
guideline
• Training on basic field epidemiology on surveillance and cased
investigation.
5.2.2 Institute active case detection, investigation and immunization
response
To stop the measles and rubella transmission, the confirmed measles and rubella
cases will be followed up immediately by active contact tracing and investigation.
This is also enabling to eliminate potential source in the community and susceptible
population. All contact of the cases will be thoroughly investigated and reported.
Based on investigation findings, health workers will provide appropriate intervention18
including immunization if required. All suspected CRS case should be investigated,
managed/referred and reported.
Key Activities:
• Inclusion of contact tracing in the revised surveillance guideline
• Training of health workers on contact tracing based on revised MR and
CRS surveillance guideline
• Management and referral protocol for CRS developed and
disseminated
5.2.3 Strengthen Adverse Events Following Immunization (AEFI)
surveillance
Country has AEFI surveillance in place for routine vaccine including measles and
rubella vaccine. However, there is lack of proper reporting, documentation and data
management at the moment. Also the existing AEFI surveillance does not include
the reporting of minor AEFI’s. Therefore, existing AEFI guideline will be revised and
health workers will be trained to strengthen AEFI surveillance.
Key Activities:
• Revise AEFI surveillance guideline
• Training of health workers on revised AEFI guideline
5.2.4 Improve data management, reporting and feedback system
Measles, rubella and CRS are notifiable diseases and all notifiable diseases are
reported through web based. However, the existing case based reporting is done by
using conventional technology like faxing, telephone and email where health centers
has access to internet facility. Also, there is no software program developed to
manage data in the programme. This has been the main constraint in getting
information collected from the field for quick response and also managing reliable
data. To address this problem, VPDP in collaboration with the Public Health
Laboratory will develop web based reporting for case based investigation reporting.
At the moment, there is no feedback mechanism instituted for sharing information
collected from the field. Therefore, programme will improve data management and
institute mandatory regular feedback mechanism. This information should be shared
to relevant stakeholders (WHO and UNICEF).19
Key Activities:
• Develop web based system for reporting and data management
• Develop feedback format and mechanism
• Training of programme personnel on data analysis
• Prepare annual reports
• Printing of annual report
5.2.5 Strengthen capacity to investigate outbreak and response
The rapid response team (RRT) is instituted at district and national level for
investigation and response of any disease outbreaks. The same RRT will be used for
measles and rubella outbreak investigation and containment. The rapid response
team capacity will be built in measles and rubella outbreak investigation including
their knowledge in field epidemiology.
Key Activities:
• Develop out break preparedness and response plan
• Training of RRT on basic field epidemiology and measles and rubella
outbreak investigation and response
5.3 Provide quality assured laboratory diagnosis and case management
Laboratory plays critical role in confirming measles or rubella as clinical signs and
symptoms are generalized and difficult to diagnose clinically. Bhutan has started
measles and rubella serology in the Public Health Laboratory in 2003 and
accreditated as national measles and rubella laboratory in the country in 2008 by
WHO. As measles and rubella cases are rarely detected in the country, clinician
and health worker may lose their competency and knowledge on measles and
rubella case detection and management. Therefore, period refresher training on n
measles and rubella case detection and management will be conducted to
maintain zero mortality.
5.3.1 Maintain accreditation of national measles and rubella laboratory
Laboratory testing to confirm a clinically suspected measles and rubella is an
essential part of the surveillance system including contact tracing. Therefore,
confirmation by quality assured laboratory testing is one of the requirement for20
achieving measles elimination targets and indicators. The existing national measles
and rubella laboratory under the Public Health Laboratory is an accreditated
laboratory for measles and rubella testing and will continue to renew and maintain
accreditation status.
Key Activities:
• Participate in IEQAS programme for proficiency testing.
• Referral of 20% of samples tested to regional measles and rubella
reference laboratory for across checking.
• Invitation of WHO experts annually for onsite assessment of national
measles and rubella laboratory for renewal of accreditation status.
• Training of laboratory personnel.
5.3.2 Maintain institutional linkage with regional reference laboratory
Laboratory based surveillance and studies will be conducted to supplement
information generated through routine surveillance system. This would require
information sharing, technical support and collaboration with WHO regional
reference laboratory and also among national measles and rubella laboratory from
other members’ state in the region. There is already established regional measles
and rubella laboratory network and Bhutan will continue to participate to maintain
existing linkages and collaboration.
Key Activities:
• Supply of quality measles and rubella test kits through WHO procurement
• Supply of controls and reagents from regional reference laboratory
• Technical assistance from regional reference laboratory
• Referrals of samples to regional reference laboratory
5.3.3 Strengthen local laboratory network on sample collection and
shipment
As per the global Measles elimination strategies and indicators, country need to
achieve samples testing more than 80% from total suspected cases reported by
national accreditated measles and rubella laboratory. Also from total confirm
measles and rubella samples, more than 80% of samples need to perform
genotyping. To achieve those laboratory indicators, samples from every suspected21
case must be collected and shipped to national Measles and Rubella Laboratory.
However, problems of samples collection and shipment still exist in the districts
especially samples collection for genotyping. To overcome sample collection and
logistic problems, local laboratory network will be strengthened and laboratory
people will be trained on samples collection and shipment to the national reference
laboratory with support from VPDP.
Key Activities:
• Development of SOP for sample collection and shipment
• Training of laboratory persons on sample collection and shipment
• Established shipment mechanism from districts to national reference
laboratory
5.3.4 Ensure prompt case management
Measles and rubella cases are rapidly declining in the country and as a result there
is risk for clinicians and health workers to miss the diagnosis of measles and rubella
including case management. This may create knowledge gap in case detection and
management if there is measles and rubella outbreak. Therefore, clinicians and
health workers will be trained periodically (Annually/bi-annually) on case definition,
symptomatic management for all suspected Measles and Rubella cases, Vitamin A
supplementation, and hospitalization of all complicated cases of fever and rash. The
clinicians and health workers also will be trained on early referral and management
of all CRS cases.
Key Activities:
• Include case management in the revised surveillance guideline
• Training of clinicians and health workers on revised MR surveillance
guideline
5.3.5 Genotyping of Measles and Rubella virus
Currently, country does not have indigenous measles and rubella genotype baseline.
However, as country gears up for Measles elimination by 2016, and rubella
elimination in near future, initiating and establishing measles genotyping capacity in
the country is critical to ascertain the indigenous measles and rubella genotypes.
This genotype information will be useful to track measles imported cases and22
moreover, genotype information will be very essential to monitor the transmission
dynamic in the region. The measles and rubella genotype information will also be
used for planning appropriate interventions at the national and regional level. The
capacity for PCR and genotyping will be built in the Public Health Laboratory with
support from WHO and regional Measles and Rubella reference Laboratory.
Key Activities:
• Procurement of laboratory equipments
• Procurement of reagents and consumables
• Ex-country training of laboratory personnel in PCR and genotyping
• Institutional linkages with WHO regional Measles and rubella reference
laboratory on genotyping.
• Collaborative study with reference laboratory on Measles and Rubella
genotyping
5.4. Intensify advocacy and risk communication for measles elimination
and Rubella/CRS control
Successful measles elimination and rubella/CRS control will depend on good
advocacy and risk communication strategies to reach out policy makers, local
leaders and community on importance of measles elimination and rubella/CRS
control. Advocacy and risk communication has been successfully conducted in
past during catch up campaigns. However, over the years, advocacy and
communication has been neglected. Therefore, advocacy and risk
communication will be intensified during measles elimination stage including
rubella/CRS control.
5.4.1 Develop communication plan and intervention tools
Communication plan and other intervention tools for measles elimination and
rubella/CRS control will be developed as deemed appropriate. Information
Education and Communication materials will be developed and disseminated
through various forms of information technology to reach various section of the
population. Sensitization activities will be carried among the targeted population. M
health application will be utilized and adopted for tracking of missed out children.
Key Activities:23
• Technical support and consultative meeting for the development of the
communication plan for measles elimination and Rubella CRS control
• Development of communication materials (broadcast & print)
• Pre test of the communication action plan
• Printing of communication plan and communication materials
• Training of Health workers on implementation of communication action
plan including BCC, Risk and outbreak communication
5.4.2 Engage community participation in vaccination advocacy
Community participation is one of the key successful factors for the overall
achievement of the high immunization program. They (community health workers,
leaders and members) will act as a bridge between the health system and the
community. Ministry of Health would pursue this through active engagement of the
community leaders, community members and village health workers. This will be
implemented in close collaboration with the Village Health Workers Program and the
district health offices. Wherever necessary exposure visit and study visit will be
planned for the village health workers and other community leaders to learn the best
practices in other high coverage districts and where there is good community
participation.
Key Activities:
• Continue and enhance engagement of VHWs during the vaccination program
• Sensitize and orient the village health workers, NFE instructors and
community leaders on Routine Immunization Schedule
• Exposure visit of VHWs/community leaders to other districts with high
community participation/performance to learn and share best practices
• Training of VHWs on line listing of children eligible for immunization and
tracing dropouts
• Training of VHWs on detection/referral of fever with rash and CRS
• Training of VHWs on AEFI24
5.4.3 Sensitise and advocate local government and policy makers
Conduct sensitization workshops to the local government and policy makers to
garner their support especially in terms of resource mobilization and political will.
Key activities:
• Review meeting on MR coverage status update with the key policy makers
5.4.4 Dissemination of communication materials through mass media
and appropriate information technology.
Information Technology and other innovative means such as use of mobile
applications will be adopted wherever possible to disseminate the IEC materials to
general and targeted population.
Key Activities:
• Airing of TV/Radio spots and jingles on media
5.5 Enhance institutional capacity and Monitoring & Evaluation
Although Bhutan has reduced the reported measles cases to zero and rubella/CRS
case to very minimal level, it is important that the country has the institutions and the
technical capacity including strong M&E in place to successfully eliminate measles
and control rubella/CRS. Therefore, following enabling strategies will be adopted.
5.5.1 Strengthen programme capacity
For the success of program implementation, various management skills, like project
planning and implementing, monitoring and supervision are important. This is more
critical during the elimination and control phase, which demands the strengthening of
program capacity. To strengthen the program capacity, additional program personnel
with vaccinology and/or public health background will be recruited. The existing
program personnel and relevant officials will also be trained on vaccinology, new
vaccines introduction, surveillance, vaccine pharmacovigilance and programme
management.
Key Activities:
• Recruitment of one additional program personnel with expertise in
vaccinology/Public health25
• Train program personnel and relevant officials on vaccinology
• Training of program and relevant officials on vaccine pharmacovigilance
• Training of program and relevant officials on surveillance & AEFI
• Training of program personnel on program management
• Training on new vaccine evaluation and introduction for program and relevant
officials (can be more specific by adding no. of people at each level)
5.5.2 Strengthen vaccine inventory management
Proper vaccine inventory management system is important to reduce wastage and
enhance proper forecasting of vaccine and cold chain requirement. Vaccines are
supplied to the national program using UNICEF Procurement Services. Domestic
vaccine supply chain has four levels. National store distributes vaccines to all
regional stores. From the Regional stores, vaccines are distributed to district
hospitals and from district hospital to the BHUs. Stock registers are updated when
they get new vaccines as well as when vaccines are distributed to other health
centres. Central and Regional cold stores are using Vaccine Supply and Stock
Management (VSSM) tool for vaccine inventory management. However, capacity of
the Central and Regional EPI in-charges on the use of this electronic tool needs to
be strengthened and expanded up to the district level. Timely recording, reporting
and updating vaccine stock at all levels are weak and also needs strengthen.
Key activities:
• Develop web based vaccine inventory management system/VSSM
• Training of EPI in charges and EPI/MCH in charges on web based vaccine
inventory management system
• Training of new EPI technicians on vaccine management
5.5.3 Strengthen regulatory system
Ensure all the vaccines supplied and used in Bhutan are WHO prequalified and
registered with DRA in line with the DRA regulation and Medicine Act of Kingdom of
Bhutan, 2003. The DRA capacity on registration of new vaccines needs to be
strengthened and improve abridged registration for WHO prequalified vaccines.
Key activities:26
• Training on new vaccines registration for the DRA/Program and
relevant oficials
• Procurement of temperature monitoring devices
• Refreshers training of drug inspectors on regulatory activities for
vaccines and cold chain requirement
• Quality testing of vaccines
5.5.4 Improve cold chain management and logistic
National Cold Store has a cold room where vaccines are stored after the vaccines
arrive in the country. The vaccines are transported from the airport to the Central
Cold store and from Central Cold store to Regional cold stores by refrigerated vans.
ILR and refrigerators are also used to store the vaccines and make ice packs at
central, regional, district and BHU levels. Cold boxes are used usually during power
failure for short duration. Vaccine carriers are used to transport the vaccines to the
ORCs. Temperature monitoring devices are used to monitor the temperature of the
cold chain equipment including transportation. Trained EPI technicians are available
in the Central and Regional Cold stores to carry out maintenance and repair works of
refrigerators whenever there is breakdown of cold chain equipment. Most of the cold
chain equipment used in the country is WHO prequalified except some refrigerators.
Currently, two regional cold stores have no cold room facilities which need to be
provided. The existing refrigerated vans are old and have frequent breakdown which
hampers the transportation of vaccines to the regional stores and then to the
districts. The commercial domestic refrigerators are being used in some of the health
facilities which were objected by DRA and WHO during evaluation as the
temperature maintenance are not uniform which may lead to cold chain failure.
Therefore, these refrigerators need to be replaced by WHO prequalified refrigerators.
Key activities:
• Procurement of Walk-in cooler in two regional cold stores
• Procurement of refrigerated vans
• Procurement of WHO prequalified refrigerators
• Procurement of cold boxes and vaccine carrier
• (Try to be more specific and add Nos.)27
5.5.5 Strengthen M & E
Monitoring and supportive supervision is being done by Central Program and
districts using standard check lists on the routine immunization activities. However,
the frequency of supervisory visits is not adequate due to human resource constraint
at the central and district levels. Effective Vaccine Management Assessment needs
to be conducted every two years. Possibility of impact assessment after training
needs to be explored. The internal and external validation of measles elimination and
rubella/CRS control status needs to be conducted.
Key Activities:
• Conduct quarterly monitoring and supportive supervision from central
to districts
• Conduct quarterly monitoring and supportive supervision from districts
to BHUs
• Conduct Effective Vaccine Management Assessment
• Conduct internal validation of Measles elimination status
5.6 Strengthen governance and collaboration with international
organizations to achieve regional and global elimination targets and
indicators
Political commitment and good governance has proven to be corner stone for
success disease elimination in number of countries who have eliminated or
control public health diseases. Further, strong supports from international
agencies or donors are critical for technical and funding support.
5.6.1 Garnering political support and resource mobilization
The VPDP, DoPH under the Ministry of Health has immensely benefited from the
political will and support for the implementation of its activities. The political support
is required more than ever, as the program moves into the measles elimination and
rubella/CRS control. The international donors are phasing out their support and there
is a challenge in mobilization of adequate resources. There is need to explore the
mobilization of funding support from RGoB/BHTF or facilitate resource mobilization
for this activities. Therefore, this strategy focuses on garnering political support and
instituting governance for Measles elimination.28
Key activity:
• Sensitization of policy makers on measles elimination and rubella/CRS
control and resource mobilization and requirements
• Conduct periodic update on the status of measles elimination and
rubella/CRS control
5.6.2 Institution of appropriate governing structure
A commission needs to be constituted for oversight, policy directives and other
necessary tasks for measles elimination and rubella/CRS control. The members of
the commission will be sensitized on the importance of measles elimination and
rubella/CRS control and their roles and responsibilities. The existing NCIP will be
designated as a technical advisory committee and support measles elimination and
rubella/CRS control. Both the commission and the NCIP will hold periodic meetings
to review and to guide the program implementation towards measles elimination and
rubella/CRS control targets.
The capacity of the NCIP members will be developed on advance vaccinology,
newer vaccines, AEFI and causality assessment to enable them to carry out their
functions effectively and recommend appropriate corrective interventions.
Key Activities:
• Develop ToR for elimination commission/committee
• Formation of the Commission
• Sensitization of commission members
• Designate NCIP as technical advisory committee for measles
elimination and rubella/CRS control
• Conduct periodic commission and NCIP meetings and as and when
necessary.
• Ex country training for NCIP members on advance vaccinology, AEFI
and causality assessment.29
5.6.3 Align and collaborate with various stakeholders and international
organization to support elimination target
To successfully achieve measles elimination and rubella/CRS control, and to sustain,
there is a need to garner new partnership involving other organizations, ministries
and agencies. Their involvement will be crucial during measles elimination and
rubella/CRS control phase. Under the guidance of VPDP, MoH, the new partners
need to incorporate measles elimination and rubella/CRS control activities in their
work plans. The possible line agencies are Ministry of Education, Ministry of Home
and Cultural Affairs, DRA, NGOs and Thromdes. These stakeholders will be
sensitized on the importance of measles elimination and rubella/CRS control and the
strategic plans will be shared with them.
The commission will liaise with international development partners to align the
elimination and control activities for certification within the global perspective. The
involvement of development partners like WHO, UNICEF, GAVI, JICA and so on is
essential for further enhancing technical and financial support. The strategy and the
control plan will be shared with these partners. This document will be updated as
when new updates are available at the international level and they will advice the
government on the new elimination strategies and situation as and when emerged at
the international fora.
Key activities:
• Sensitize and share measles elimination and control strategic plan to
relevant stakeholders including international organizations for support
• Conduct coordination and consultative meeting with development
partners
• Review and adapt global and regional measles elimination and
rubella/CRS control initiatives as and when emerged at the
international fora.
Annex I: Monitoring Indicators30
Objective/Strategy Description of
Indicator
indicator
Base Target
Definition
line (%)
(2014) (2016)
1. Achieve and maintain >95% two doses of measles and rubella vaccination coverage.
1.1 Micro-stratification and Immunization
targeted immunization coverage
intervention for low MR 95
MCV1 & MCV2
vaccine coverage
coverage at the
national level
The numerator is the number of
infants who received MCV1 &
1.2 Accelerate immunization Immunization MCV2 and the denominator is the
intervention to reach out coverage surviving birth cohort multiplied by
children who are not MCV1 & MCV2
90 100
vaccinated
coverage at the
1.3 Sustain routine high MR
vaccine coverage District level
1.4 Operational research on
vaccine coverage and
management
2. Intensify surveillance and investigation of measles and Rubella/CRS
2.1 Scale up existing MR and Adequacy of
CRS surveillance system investigation
Proportion of all The numerator is the number of
suspected cases of measles or rubella
suspected measles
≥ 90 for which an adequate investigation
and rubella cases
was initiated within 48 hours of
that have had an notification and the denominator is the
adequate total number of suspected measles and
investigation initiated rubella cases, multiplied by 100
within 48 hours of
notification
2.2 Strengthen case based Timeliness of The numerator is the number of
surveillance system for measles, reporting surveillance units reporting on time and
rubella and CRS Proportion of the denominator is the total number of
100 surveillance units in the country
surveillance units
multiplied by 100 [Remember each
reporting to the
reporting unit will report 52 times a
national level on time year]
2.3 Institute active case Disease Incidence Absence of The numerator is the confirmed
detection, investigation and Annual incidence of measles number of measles or rubella cases for
immunization response confirmed measles and rubella the year and the denominator is the
indigenous population in which the cases occurred
and rubella cases
cases multiplied by 1,000,000. When
numerator is zero, the target incidence
would be zero.
2.4 Strengthen AEFI
surveillance
2.5 Improve data management,
reporting system and feedback31
2.6 Strengthen capacity to Outbreak The numerator is the number of
investigate outbreak and investigation confirmed outbreaks that meet the fully
≥ 90 investigated outbreak criteria and the
response Percentage of
denominator is the total number of
suspected measles
suspected outbreaks multiplied by 100
outbreaks fully
investigated
Percentage of The numerator is the number of
suspected outbreaks confirmed outbreaks tested for virus
≥ 90 detection and the denominator is the
tested for virus
total number of suspected outbreaks
detection
multiplied by 100
Reporting rate of The numerator is the number of non-
discarded non- measles non-rubella discarded cases
≥2 and the denominator is the total
measles non-rubella
population of the country multiplied by
cases
100,000
A national reported
discarded rate of
non-measles, non-
rubella per 100,000
population
3. Provide quality assured laboratory diagnosis and case management
3.1 Maintain accreditation of Proportion of
national measles and rubella suspected cases The numerator is the number of
laboratory with adequate suspected cases from whom adequate
≥ 90 specimens for detecting measles or
specimens for
rubella were collected and tested and
detecting acute
the denominator is the total number of
measles or rubella suspected measles or rubella cases
infection collected multiplied by 100 [Epi linked cases
and tested in a should be removed from the
proficient laboratory denominator]
3.,2 Maintain institutional linkage Timeliness of
with regional reference specimen transport The numerator is the total number of
≥ 80 specimens received in the laboratory
laboratory Proportion of
within 5 days of collection and the
specimens received
denominator is the total number of
at the laboratory
specimens received by the laboratory
within 5 days of multiplied by 100
collection
3.3 Strengthen local laboratory Timeliness of
network on sample collection reporting laboratory The numerator is the total number of
100 specimens for which laboratory results
and shipment results
were available within 4 days of
3.4 Ensure prompt case
receiving the specimen and the
management Proportion of results
denominator is the total number of
3.5 Genotyping of Measles and reported by the specimen received for testing multiplied
Rubella virus laboratory within 4 by 100
days of receiving the
specimen
4. Intensification of communication for measles elimination and Rubella/CRS control32
4.1 Develop communication plan
and intervention tools
4.2 Engage community
participation in vaccination
advocacy
4.4 Dissemination of
communication materials
through media and appropriate
information technology.
5. Enhance institutional capacity and Monitoring & Evaluation
5.1 Strengthen programme
capacity
5.2 Strengthen vaccine inventory
management
5.3 Strengthen regulatory
mechanism
5.4 Improve cold chain
management and logistic
5.5 Strengthen M & E
6. Strengthen governance and collaboration with international organizations to achieve regional
and global elimination targets
6.1 Garnering political support Sensitization of policy
and resource mobilization makers on measles
elimination and
rubella/CRS control
6.2 Institution of appropriate Develop ToR for
governing structure elimination and
control commission
Formation of the
Commission
Sensitization of
commission member
Designate NCIP as
technical advisory
committee to support
measles elimination
and rubella/CRS
control
Conduct periodic
commission and
NCIP meetings and
as and when
necessary.
Ex country training
for NCIP members on33
advance vaccinology,
AEFI and causality
assessment and
pharmacovigilance.
6.3 Align and collaborate with Sensitize and share
various stakeholders and measles elimination
international organization to and control strategic
support elimination target plan to relevant
stakeholders
Sensitize and share
measles elimination
and control strategic
plan to international
organizations for
support.
Review and adapt
global and regional
measles elimination
and rubella/CRS
control initiatives as
and when required.You can also read