MRx0518 Conference Call & Webcast Event - 23 March 2022 - NASDAQ: LBPS - 4D Pharma plc
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MRx0518 Conference Call & Webcast Event 23 March 2022 NASDAQ: LBPS AIM: DDDD
2
DISCLAIMER AND FORWARD LOOKING STATEMENTS
This document has been prepared by 4D pharma plc (together with its consolidated subsidiaries, the “Company”) for informational purposes and solely for use at a presentation concerning the Company.
This document (the "Slides") (along with any oral presentation and question and answer session) does not constitute, and should not be construed as, an admission document, listing particulars or prospectus relating to the Company and does
not constitute an offer to sell or issue securities or otherwise constitute an invitation, inducement, solicitation or recommendation to any person to purchase or subscribe for any securities of the Company, and should not be relied upon in
connection with a decision to purchase or subscribe for any such securities. The Slides do not constitute a recommendation regarding any decision to sell or purchase securities in the Company. Nothing contained herein shall form the basis
of or be relied on in connection with any contract or commitment whatsoever and, in particular, it must not be used in making any investment decision.
Some of the information contained in these Slides may be from public or third-party sources. Although reasonable care has been taken to ensure that the facts stated in this presentation are accurate and that the opinions expressed are fair
and reasonable, the contents of this presentation have not been verified by the Company or any other person. Except as required by law, no person undertakes any obligation to verify, update or keep current the information contained in these
Slides. The Slides and the accompanying verbal presentation are confidential, and the Slides are being supplied to you solely for your information and may not be reproduced, further distributed to any other person or published, in whole or in
part, for any purpose.
The distribution of this presentation in certain jurisdictions may be restricted by law, and persons into whose possession this presentation comes should inform themselves about, and observe, any such restrictions. This presentation does not
form part of any offer of securities, or constitute a solicitation of any offer to purchase or subscribe for securities or an inducement to enter into any investment activity. Recipients of this presentation are not to construe its contents, or any prior
or subsequent communications from or with the Company or its representatives as investment, legal or tax advice. In addition, this presentation does not purport to be all-inclusive or to contain all of the information that may be required to
make a full analysis of any transaction. Further, the information in this presentation is not complete and may be changed. Recipients of this presentation should each make their own independent evaluation of the information and of the
relevance and adequacy of the information in this document and should make such other investigations as they deem necessary.
This presentation may contain forward-looking statements that reflect the Company’s current views and expectations regarding future events. In particular certain statements with regard to management’s strategic vision, aims and objectives,
the conduct and results of clinical trials, the timing or likelihood of regulatory filings and approvals for of its product candidates and the anticipated launch of specified products in various markets, the Company’s ability to find partners for the
development and commercialisation of its products as well as the terms for such partnerships, anticipated levels of demand for the Company’s products (including in development), the effect of competition, anticipated efficiencies, trends in
results of operations, margins, the market and exchange rates, and estimates regarding the Company’s expenses, future revenues and future capital requirements are all forward looking in nature. Forward-looking statements involve known
and unknown risks, uncertainties and other factors that may cause the Company’s actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the
forward-looking statements.
This presentation also contains estimates, projections and other information concerning the Company’s business and the markets for the Company’s product candidates, including data regarding the estimated size of those markets, and the
incidence and prevalence of certain medical conditions. Information that is based on estimates, forecasts, projections, market research, or similar methodologies is inherently subject to uncertainties and actual events or circumstances may
differ materially from events and circumstances reflected in this information. Unless otherwise expressly stated, the Company obtained this industry, business, market and other data from reports, research surveys, clinical trials studies and
similar data prepared by market research firms and other third parties, from industry, medical and general publications, and from government data and similar sources.
Forward-looking statements represent the Company’s beliefs and assumptions only as of the date of this presentation. Although the Company believes that the expectations reflected in the forward-looking statements are reasonable, it cannot
guarantee future results, levels of activity, performance or achievements. Except as required by law, the Company assumes no obligation to publicly update any forward‐looking statements for any reason after the date of this presentation, or
to conform any of the forward-looking statements to actual results or to changes in its expectations.
This presentation has not been approved by an authorised person in accordance with Section 21 of the Financial Services and Markets Act 2000 ("FSMA") and therefore it is being delivered for information purposes within (a) the United
Kingdom only to persons (i) who have professional experience in matters relating to investments and who fall within the definition of "investment professionals" in Article 19(5) of the Financial Services and Markets Act 2000 (Financial
Promotion) Order 2005 (as amended) (the "Order") or are high net worth entities falling within Article 49(2)(a) to (d) of the Order and investment personnel of any of the foregoing (each within the meaning of the Order); and (ii) who are
"qualified investors" within the meaning of Article 2(e) of the Prospectus Regulation (Regulation (EU) 2017/1129) ("Qualified Investors", and each a "Qualified Investor"); and (iii) to whom the Presentation may otherwise lawfully be
communicated; and (b) the European Economic Area (other than the United Kingdom) (the "EEA") only to Qualified Investors (all such persons together being referred to as "Relevant Persons" and each a "Relevant Person"). By accepting
this presentation and not immediately returning it, the recipient represents and warrants that they are a Relevant Person. This presentation is not to be disclosed to any other person or used for any other purpose.
By participating in this presentation and/or accepting any copies here of you agree to be bound by the foregoing restrictions and the other terms of this disclaimer.
© 4D pharma plc
3 AGENDA
• Scott Tagawa (landscape in kidney and bladder cancer therapy)
• Introduction to MRx0518
• Design of MRx0518-I-002 study
• Part B results to date
• Petros Grivas (ICI study biomarkers)
• Biomarker data
• Next steps
© 4D pharma plc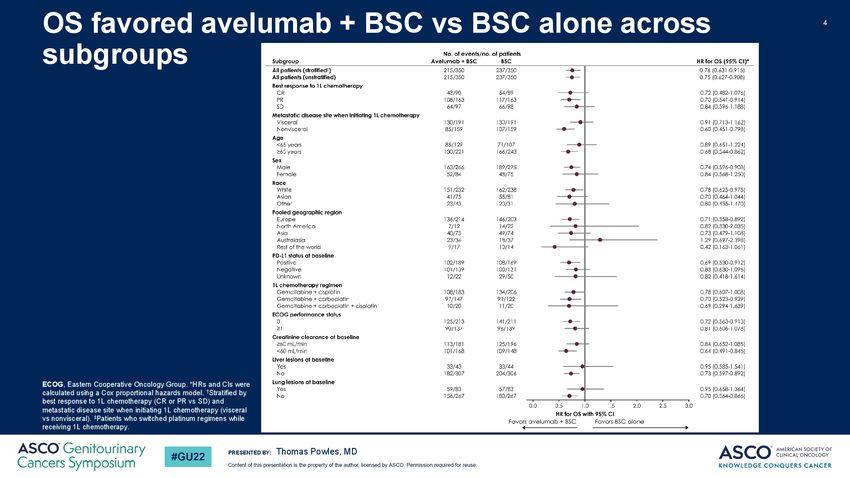
Dr. Scott Tagawa
Professor of Medicine and Urology at Weill
Cornell Medicine
Kidney and Bladder Cancer Treatment
Landscape
Renal Cell Carcinoma
Evidence / Approved Recommendations: MCC GU DMT
Pembro + Axi
Nivo + Cabo
Pembro + lenvatinib
Initial Avelumab + Axi
Nivolumab
Cabozantinib
presentation Pazopanib
High-dose IL2
Axitninb
Lenvatinib + everolimus
Cytoreductive nephrectomy
Everolimus
sorafenib
Advanced
Good Risk 2nd line
ccRCC (Gen post-
VEGF)
Localized Heavily
Renal pre-treated
Mass
Surveillance
Advanced Drugs not previously administered
chemotherapy
Nephrectomy Int/Poor Risk 2nd line
Ablation
ccRCC
Nivo/Ipi Cabozantinib
Pembro + Axi sorafenib
Nivo + Cabo everolimus
Pembro + lenvatinib temsirolimus Untreated
sunitnib
Initial Avelumab + Axi Non-clear
Cabozantinib
presentation Temsirolimus Cell RCC
Cabozantinib
Pembro
Temsirolimus
Sunitinib Standard
Alternative
@Brian_Rini “Updated table of IO doublets in mRCC after #ASCOGU22” 21Feb2022
Typical approach • IO-based combinations in 1st line setting • TKI 2nd line
RCC Unmet needs / Questions
• IO-based combinations in 1st line setting
• IO-IO vs IO-TKI?
• Which doublet is best? (is “dirtier” IO partner better?)
• What about either triplet or transition to maintenance?
• Initiate triplet therapy
• Add TKI after CTLA4/PD(L)-1 PR/SD
• can we drop TKI from PD(L)-1 after response? (maintenance IO after combo induction)
• Can we stop systemic Rx after CR or good PR?
• What about “1st-line” RX after adjuvant IO
• TKI 2nd line
• Following 1st line IO, is there utility for PD(L)-1 continuation during next
line of Rx or CTLA4 re-challenge?
• Ways to subvert resistance?
• Newer IO agents?
Urothelial Carcinoma
Evidence / Approved Recommendations: MCC GU DMT
MVAC Avelumab
Gem/Cis Avelumab
Cisplatin Pembrolizumab (if no maintenance)
fit Enfortumab vedotin (preferred)
mUC Sacituzumab govitecan
without prior PRUC Erdafitinib (if activating FGFR alteration)
systemic Rx Atezo/Nivo/Ave/Durva (if no maintenance)
Cisplatin Taxane (ram?)
unfit
Pemetrexed
Supportive care
Gem/Carbo Avelumab
Atezolizumab/Pembrolizumab
Gemcitabine
Carbo/paclitaxel
Standard
Alternative2021 Updated EAU Guidelines on Metastatic Urothelial Carcinoma
Cathomas R … Milowsky M. Eur Urol 2022 Jan; 81(1): 95-103Typical approach • Cisplatin/Carboplatin + Gemcitabine • Avelumab maintenance (or 2nd line pembrolizumab) • Enfortumab vedotin • Sacituzumab govitecan or erdafitinib
mUC Unmet needs / Questions (1)
• Cisplatin/Carboplatin + Gemcitabine
• Beat platinum-based chemo
• Beat cisplatin combo +/- maintenance
• Only carbo combo +/- maintenance
• Avelumab maintenance (or 2nd line pembrolizumab)
• Improve maintenance (add or beat)
• Improve 2nd line IO (add or beat)
• Can we stop?
• What if prior adjuvant IO?
• Enfortumab vedotin
• Biomarkers of response, mechanisms of resistance
• Combinations
• Earlier lines of therapy
• Overcome toxicity
• Additional Nectin4-targeted drugsmUC Unmet needs / Questions (2) • Sacituzumab govitecan • Biomarkers of response, mechanisms of resistance • Combinations • Earlier lines of therapy • Overcome toxicity • Additional Trop2-targeted drugs • Erdafitinib • Biomarkers of response, mechanisms of resistance • Combinations • Earlier lines of therapy • Overcome toxicity • Additional FGFR-targeted drugs
MRx0518
Combination with Keytruda® in patients
with solid tumors with acquired
resistance to ICI therapy16
MRx0518 – AN ORAL IMMUNOTHERAPY THAT STIMULATES THE ANTI-TUMOR RESPONSE
Innate immune activation via the gut Systemic immune stimulation Immune trafficking and tumor
invasion
APC
Adaptive immune activation Increased anti-tumor immune cell
MRx0518 subsets in tumor microenvironment
Enterococcus gallinarum • T cells
Gram-positive TLR9
CD8+ T • CD8+ T cells
Motile anaerobe • Natural Killer (NK) cells
Migration via lymphatic system • Cytotoxic cells
• Dendritic cells
• Macrophages
• CD8+ T / Treg ratio
Flagellin protein
Monocyte
Tumor
TLR5
Flagellin-TLR5 signalling via:
• Intestinal epithelial cells (IECs) NK
• Antigen presenting cells (APCs)
Macrophage
• Innate immune cells in lamina propria Increased circulating anti-tumor
cytokines & chemokines
Investigating potential TLR9 activation • IL-12, CXCL10
Lauté-Caly et al., Scientific Reports 2019; Pant et al., JITC 2020 (#283, #376); Lythgoe et al., JITC 2020 (#805); Parra et al., Ann Oncol 2021 (#1024P); Lythgoe et al., Ann Oncol 2021 (#543P)
© 4D pharma plc17
MRx0518: PART B - PHASE I/II COMBINATION STUDY WITH KEYTRUDA®
A phase I/II open-label, safety and preliminary efficacy study of MRx0518 in combination with pembrolizumab
in patients with advanced malignancies who have progressed on PD-1/PD-L1 inhibitors
Acquired
Resistance Part A, N = 12
Prior ICI Screening 1 capsule MRx0518 (10x1010 – 10x1011 CFU) BID
Pembrolizumab 200mg IV Q3W
Follow Up
(2 years)
Safety Review
Part B, N = up to 120
1 capsule MRx0518 (10x1010 – 10x1011 CFU) BID
Pembrolizumab 200mg IV Q3W
NCT03637803
Part B Objectives Patient population
• Safety and tolerability • Solid tumors with acquired resistance to prior
• Clinical benefit (response or stable disease ≥6 months) anti-PD-1 immune checkpoint inhibitors (ICIs)
• ≥10% pre-defined threshold for expansion • Heavily pre-treated patients, no approved
• Exploratory biomarker analyses – mechanism of action options remaining
• Signal to inform late-stage clinical strategy
© 4D Pharma plc18 PRIMARY EFFICACY ENDPOINT FOR THE RCC GROUP MET IN ADVANCE OF FULL ENROLMENT
• Recruited patients had ≥1 prior line of anti-PD-1/PD-L1 ICI therapy and experienced clinical benefit (CR, PR or SD ≥ 6m)
before losing response – developing acquired resistance
• Patients with acquired resistance to ICIs are not expected to respond to rechallenge with monotherapy ICI
Primary Efficacy Endpoint for Part B of the study (per tumor group)
• Clinical Benefit in >3 in 30 patients of a given tumor type group, defined as:
• Objective response (complete or partial), or stable disease ≥ 6 months
• Each tumor type recruited in 3 cohorts of 10 patients
• Expansion from one cohort to the next dependent on observing at least 10% clinical benefit
Primary Efficacy Endpoint met for RCC early in Part B of the study
4 of the first 16 evaluable RCC patients in Part B achieved clinical benefit
Primary efficacy endpoint met of >3 in 30 to deem the treatment worthy of further study
© 4D pharma plc19 PHASE I/II PARTS A & B, RCC BASELINE CHARACTERISTICS
• Recruited patients had ≥1 prior line of anti-PD-1/PD-L1 ICI therapy and experienced clinical benefit (CR, PR or SD ≥ 6m)
before losing response – developing acquired resistance
RCC Patient Backgrounds (Part A & Part B)
Renal cell carcinoma (N=29)
Age (years) 67 (37-82)
Male 28 (97%)
Sex
Female 1 (3%)
0 8 (29%)
ECOG
1 20 (71%)
Median prior lines of therapy (range) 3 (1-5)
ICI monotherapy 15 (52%)
ICI + ICI 8 (28%)
Prior ICI regimen
ICI + TKI 4 (14%)
ICI + experimental 10 (35%)
ICI – immune checkpoint inhibitor; TKI – tyrosine kinase inhibitor
© 4D pharma plc20 KEYTRUDA® AND MRx0518 – PART B MET PRIMARY ENDPOINT EARLY FOR RCC COHORT
• 4 of the first 16 evaluable RCC patients in Part B to date achieved clinical benefit
• Met primary endpoint: >3 of up to 30 to be recruited
2
24 total evaluable RCC
patients in Part A and B (had
scan at any timepoint post-
baseline)
Per protocol Clinical Benefit
(CR, PR, SD ≥ 6 months)
• 2 x PR
1 • 6 x SD ≥ 6 months
Disease Control Rate
(CR, PR, SD ≥ 9 weeks)
• 12 / 24 (50%)
1Patient achieved best radiographic response of -39%, but was confirmed as SD at subsequent restaging per RECIST v1.1
2Radiographic scan at week 6 indicated progression of +243% of target lesion
Arrow indicates patient remains on study treatment © 4D pharma plc21 KEYTRUDA® AND MRx0518 – PART B MET PRIMARY ENDPOINT EARLY FOR RCC COHORT
• 4 of the first 16 evaluable RCC patients in Part B to date achieved clinical benefit
• Met primary endpoint: >3 of up to 30 to be recruited
24 total evaluable RCC patients
243
in Part A and B (had scan at any
//
timepoint post-baseline)
Per protocol Clinical Benefit *
(CR, PR, SD ≥ 6 months)
• 2 x PR
• 6 x SD ≥ 6 months
# # # # 2
1
Disease Control Rate (# + * )
(CR, PR, SD ≥ 9 weeks)
• 12 / 24 (50%)
2 * Clinical Benefit
# Disease control
1 Patient achieved best radiographic response of -39%, but was confirmed as SD at subsequent restaging per RECIST v1.1
2 Patient is ongoing on study © 4D pharma plc22 RCC CASE STUDY 1
• 82 year old male, diagnosed with Stage I ccRCC in 2010
MRx0518 + pembrolizumab
• Best response to prior anti-PD-L1 ICI therapy (avelumab and axitinib) % change combined target tumour
was partial response (PR) 25 volume from baseline
• Discontinued after 88 weeks due to confirmed progressive 0
disease, continued on Axitinib monotherapy
-25
• ECOG score of 1 and Stage IV disease at enrolment in early 2020
%
-50
• Began MRx0518 and KEYTRUDA® as 3rd line of systemic treatment in
March 2020 – continues on study with 24.5 months of treatment to date -75
-100%
• Complete reduction of target lesions maintained, new lesions under -100
control with radiotherapy
Weeks on Study
• No treatment-related serious adverse events reported to date
2017 2018 2019 2020 2021 2022
AM J J A S ON D J FMAM J J A S O N D J F M A M J J A S ON D J FM A M J J A S ON D J FMAM J J A S ON D J FM
Avelumab + Axitinib PR
Axitinib + radiotherapy PR
MRx0518 +
PR
pembrolizumab
© 4D pharma plc23 RCC CASE STUDY 2
• 49 year old male, diagnosed with Stage IV mccRCC in 2017
MRx0518 + pembrolizumab
• Best response to prior anti-PD-1 ICI therapy (nivolumab and % change combined target tumour
bempegaldesleukin) was partial response 25 volume from baseline
• Discontinued after 24 weeks due to confirmed progressive disease
0
• MRx0518 and KEYTRUDA® tumor reduction below -30% but PR not
-25
confirmed on next scan
%
-50
• Had long term stable disease (SD) on study for 8.5m (36 weeks) until -39%
investigator’s decision to withdraw from study due to increase in target -75
tumors (non-PD)
-100
• No serious adverse events reported to date 0 3 6 9 12 15 18 21 24 27 30 33 36 39
Weeks on Study
2018 2019 2020 2021
F M A M J J A S O N D J F M A M J J A S O N D J F M A M J J A S O N D J F M A M
Nivolumab +
PR
bempegaldesleukin
Axitinib SD
Cabozantinib + CB839/placebo SD
Lenvatinib + everolimus Mixed
MRx0518 + pembrolizumab SD
© 4D pharma plc24 RCC CASE STUDY 3
• 58 year old male, diagnosed with Stage III mRCC in 2014 MRx0518 + pembrolizumab
% change combined target tumour
• Best response to prior anti-PD-1 ICI therapy (nivolumab + sitravatinib) volume from baseline
was partial response 50
Long-term stable
• Discontinued after 124 weeks due to confirmed progressive 25 disease >11 months
disease in September 2020 0
• ECOG score of 1 and Stage IV disease at enrolment in Dec 2020 -25
%
• Began MRx0518 and KEYTRUDA® as 4th line of systemic treatment in -50
December 2020 with no intervening regimen -75
• Patient remained on regimen for 13.1 months before disease progression -100
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57
• No serious adverse events reported to date Weeks on Study
2014 2015 2016 2017 2018 2019 2020 2021
J FMAM J J A SOND J FMAM J J A SOND J F M A M J J A SOND J F M AM J J A SOND J F M A M J J A SOND J F M A M J J A SOND J FMAM J J A SOND J FMAM J J A SOND
Autologous DC
immunotherapy + PD
Sunitinib
Axitinib PR
Sitravatinib +
PR
Nivolumab
MRx0518 +
SD
pembrolizumab
© 4D pharma plc25
BASELINE TUMOR BIOMARKER DATA SHOWS HIGHER TILs IN RESPONDERS
• Association between higher baseline densities of total T cells (CD3+) and subsets (CD8+, and Ki67+
marker of proliferation) and positive outcomes with MRx0518 + KEYTRUDA® treatment
Tumor - Total CD3+ (n/mm2) Tumor - CD3+CD8+ (n/mm2)
Tumor - CD3+Ki67+ (n/mm2)
1000 ✱ 300 0.0821 40
0.0995
800
30
CD3+CD8+ (n/mm2)
Total CD3+ (n/mm2)
CD3+Ki67+ (n/mm2)
200
600
20
400
100
10
200
0 0 0
s
s
s
s
s
s
er
er
r
r
er
r
de
de
de
nd
nd
nd
n
n
n
po
po
po
po
po
po
es
es
es
es
es
es
-R
-R
R
R
-R
R
on
on
on
N
N
N
Stroma - Total CD3+ (n/mm2) Stroma - CD3+CD8+ (n/mm2)
2500 ✱ 800
✱
2000
600
Total CD3 (n/mm )
CD3 CD8 (n/mm )
2
2
1500
400
+
+
1000
+
200
500
0 0
s
s
s
s
er
er
r
r
de
de
nd
nd
n
n
po
po
po
po
© 4D Pharma plc
es
es
es
es
-R
-R
R
R
on
on
N
N26
FLOW CYTOMETRY SHOWS GREATER T CELLS AND CD8+ T CELLS IN RESPONDERS
• In paired on-treatment samples of PBMCs for RCC patients, significant differences between responders
and non-responders, observed in the on-treatment samples at Cycle 4 Day 1 (C4D1) for total (CD3+) and
CD8+ T cells
• Trend shows a reduction in circulating Tregs at C4D1 vs baseline, particularly in responders
• Trend shows lower CTLA-4 expression in CD4+ T cells of responders vs non-responders at baseline
CD3+ CD8+ Treg CD4+ CTLA-4+
100 50 * 0.05 0.8
*
Freq. of CD45 cells
Freq. of CD45 cells
Freq. of CD45 cells
Freq. of CD45 cells
80 40 0.04
0.6
60 30 0.03
0.4
40 20 0.02
0.2
20 10 0.01
0 0 0.00 0.0
R
R
R
R
R
R
R
R
R
R
R
R
R
R
R
R
N
N
N
N
N
N
N
N
1
1
1
1
L
L
L
L
4D
4D
4D
4D
B
B
B
B
L
L
L
L
1
1
1
1
4D
4D
4D
4D
B
B
B
B
C
C
C
C
C
C
C
C
C4D1 – treatment cycle 4, Day 1; BL - baseline © 4D Pharma plc
NR – non-responder; R – responder (complete response, partial response or stable disease)27 MRx0518 + KEYTRUDA® PHASE I/II STUDY RCC RESULTS SUMMARY
Signal finding Phase I/II study has met primary endpoint for RCC group in Part B
• 4 patients to date of the first 16 evaluable RCC patients in Part B of the study achieved clinical benefit
(CR, PR, or SD > 6 months), meeting primary efficacy endpoint early ahead of total recruitment of up to
30 RCC patients
• Identified biomarkers, both in tumor and in the blood, that could potentially be used to identify patients
most likely to benefit from treatment with MRx0518 + anti-PD-1 ICI KEYTRUDA®
• Trends in changes in on-treatment biomarkers with MRx0518 + KEYTRUDA® combination, appears to
differ in responders vs. non-responders
Combined with previously reported monotherapy data* – indicative of MRx0518
being capable of decreasing tumor microenvironment immune suppression, and
ability to activate the tumor via CD8+ T cell infiltration
* SITC 2020, ESMO 2021
© 4D pharma plc28 NEXT STEPS FOR MRx0518 IN ICI-REFRACTORY SETTING
• Results enable 4D to discuss with collaborators potential pivotal study in ICI-refractory RCC
• Existing study will continue to recruit RCC patients, with potential expansion to include patients with
primary resistance – a larger refractory patient population who have no prior benefit to ICI
Of all RCC patients treated with an ICI combination first-line…
…around 50% show primary resistance …around 50% will respond
…of which >35% will develop
acquired resistance
Rini et al., NEJM 2019; 380:1116-1127; Hammers et al., ICKS 2021 (#E39); Chouieri et al., Annals of Oncology 2020; 31(8):1030-1039 © 4D pharma plc29 EMERGING IMPORTANCE OF BIOMARKERS IN THE DEVELOPMENT OF MRx0518
• Biomarkers from the combination study of
MRx0518 + KEYTRUDA® can inform future
development
• Builds on previous data from neoadjuvant
monotherapy study of MRx0518 in
treatment-naïve patients
• Can indicate patient populations that may
benefit from treatment, and additional
mechanistic information regarding settings
where MRx0518 can be effective
• Data regarding tumor, immune and genetic
signatures and biomarkers that are
associated with better outcomes in landmark
studies of ICIs in early line settings have
been established in literature
© 4D pharma plcDr. Petros Grivas
Associate Professor Clinical Research
Division at the Fred Hutchinson Cancer
Research Center
Emerging Importance of Biomarkers in ICI
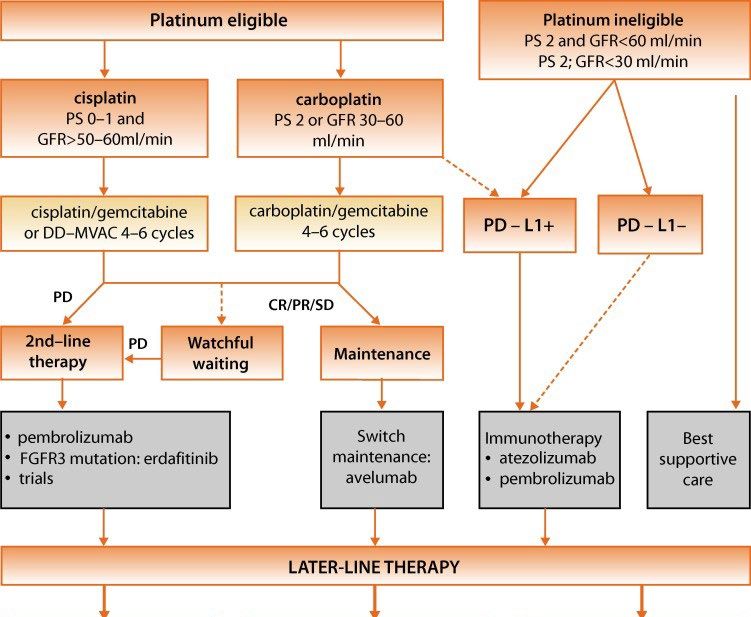
therapyAdvanced Urothelial Ca Treatment Algorithm
Disease State Setting Preferred Option Other Options
Metastatic, no prior Cisplatin-eligible Cisplatin/gemcitabine f/b avelumab aMVAC f/b avelumab maintenance
chemotherapy maintenance
Metastatic, no prior Cisplatin-ineligible Gemcitabine/Carboplatin Pembrolizumab
chemotherapy (in fit patients) f/b avelumab maintenance Atezolizumab
Single agent chemotherapy
Metastatic, prior platinum Pembrolizumab OR Avelumab
chemotherapy or relapse within Erdafitinib (tumors with FGFR2/3 activating Nivolumab
1 year of perioperative cisplatin- alteration) OR
based therapy Enfortumab vedotin (cisplatin-unfit pts)
Metastatic, prior chemotherapy Enfortumab vedotin OR Taxane (US)
& immunotherapy Sacituzumab govitecan OR Vinflunine (EU)
Erdafitinib (tumors with FGFR2/3 activating
alteration)
Clinical trials are critical throughout disease spectrum & Petros Grivas
treatment settings!ICI as 1L in Cisplatin-Ineligible Pts (phase II single arm trials)
Atezolizumab1 Pembrolizumab2
Phase Phase II (IMvigor Cohort 1) Phase II (Keynote-052)
Number of Patients 119 370
Dosing 1200mg every 3 weeks 200mg every 3 weeks
ORR 23% (9% CR) 29% (7% CR)
70% of responses ongoing at 17.2 82% of responses ongoing at ≥ 6
Duration of Response
months months
Median OS 15.9 months Not reached
Median PFS 2.7 months 2 months
Rate of Grade 3/4 Treatment-related
16% 19%
AEs
1. Balar et al. 2017 Lancet 2. Balar et al. 2017 Lancet OncologySurvival Analysis from Phase III, Open-Label Trial of
Pembrolizumab vs Chemotherapy in Advanced UC
• Longer follow-up confirms initial data
• Objective responses occurred rapidly and 100
were generally durable, with duration of
response not yet reached 80
• Safety and tolerability support pembrolizumab
Overall Survival, %
60 44.4% 36.1%
over 2nd/3rd-line chemotherapy 30.2% 20.5%
40
Events, n HR (95% CI)a Pb
20
Pembro 170 0.70
0.0004
Chemo 196 (0.57-0.86) 0
0 4 8 12 16 20 24
Months
Median (95% CI):
10.3 mo (8.0-12.3)
7.4 mo (6.1-8.1)
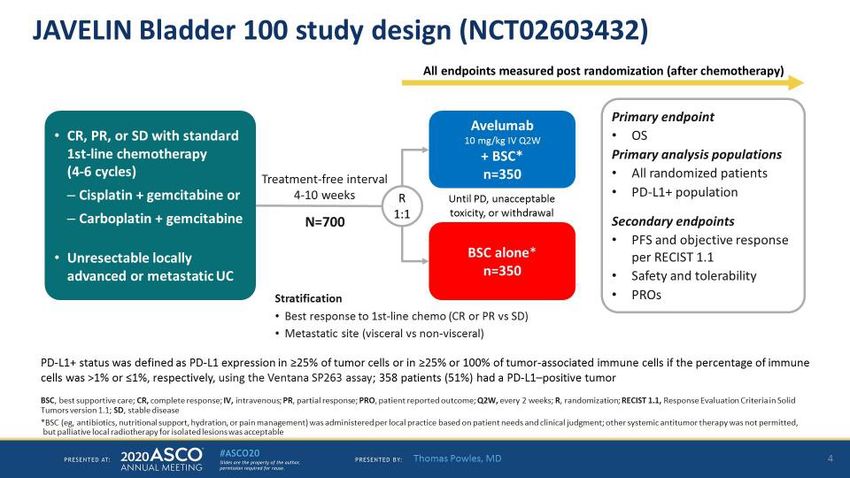
Bajorin D, et al. Presented at: ASCO Annual Meeting; 2017. Abstract 4501.JAVELIN Bladder 100 study design (NCT02603432) Presented By Thomas Powles at TBD
$Title$ Content of this presentation is the property of the author, licensed by ASCO. Permission required for reuse.
$Title$ Content of this presentation is the property of the author, licensed by ASCO. Permission required for reuse.
$Title$ Content of this presentation is the property of the author, licensed by ASCO. Permission required for reuse.
JAVELIN Bladder 100 clinical and TCGA subgroups
Abstract 4520, Powles T et al.
OS in patients with PD-L1+ tumors who PFS in patients with PD-L1+ tumors who
received 1L gemcitabine + carboplatin received 1L gemcitabine + carboplatin
1L, first line; BSC, best supportive care; HR, hazard ratio; NE, not estimable; OS, overall survival; PFS, progression-free survival.
40
Confidential. For Internal Use Only. Do Not Copy or Distribute.JAVELIN Bladder 100 clinical and TCGA subgroups
Abstract 4520, Powles T et al.
Forest plot of OS based on BICR in subgroups of interest
*HRs and CIs were calculated using a Cox proportional hazards model.
†Stratified by best response to 1L chemotherapy (complete or partial response vs stable disease) and metastatic disease site (visceral vs nonvisceral).
‡Post chemotherapy.
1L, first line; BICR, blinded independent central review; BSC, best supportive care; HR, hazard ratio; OS, overall survival; PFS, progression-free survival; TCGA, The Cancer Genome Atlas.
41
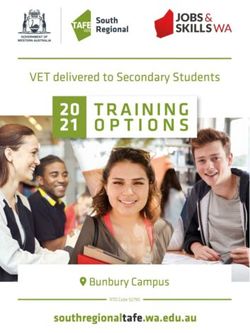
Confidential. For Internal Use Only. Do Not Copy or Distribute.OS benefit in subgroups defined by Tumor Mutation
Burden (TMB) and PD-L1 status
Neither TMB nor PD-L1 status alone fully predict OS benefit
Arm TMB HR (95% CI)
Avelumab + BSC HR (95% CI)
>Median 0.48 (0.332, 0.707)
BSC alone Subgroup Avelumab + BSC vs
BSC alone
Avelumab + BSC
100 ≤Median 0.88 (0.643, 1.197) PD-L1+ 0.56 (0.400, 0.790)
BSC alone
90
PD-L1− 0.85 (0.616, 1.181)
80 Median: 7.66 nonsynonymous SNVs/Mb
TMB-high 0.48 (0.332, 0.707)
70
60 TMB-low 0.88 (0.643, 1.197)
OS, %
50 PDL1+ TMB-high (n=190) 0.51 (0.305, 0.868)
40 PDL1+ TMB-low (n=148) 0.60 (0.382, 0.955)
30 PDL1− TMB-high (n=105) 0.44 (0.251, 0.768)
20
PDL1− TMB-low (n=140) 1.27 (0.799, 2.006)
10
0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
Months
42Impact of mutation profiles on OS benefit with avelumab
Type and location of mutations may influence utility of TMB assessment
Signatures of mutational processes
C>A C>G C>T T>A T>C T>G >Median vs ≤Median HR (95% CI)
0.2
0.48 (0.335, 0.699)
0.1 Signature 23**
0.89 (0.645, 1.226)
0.0
0.2
0.58 (0.409, 0.819)
Relative contribution
0.1 Signature 7
0.79 (0.569, 1.102)
0.0
0.2
0.66 (0.464, 0.934)
0.1 Signature 2
0.69 (0.500, 0.960)
0.0
0.2
0.98 (0.633, 1.515)
0.1 Signature 28
0.58 (0.432, 0.772)
0.0
G.C
G.C
G.C
G.C
G.C
G.C
A.C
A.C
A.C
A.C
C.G
C.G
A.C
C.G
C.G
C.G
A.C
C.G
C.C
C.C
C.C
C.C
C.C
C.C
G.G
T.G
G.G
T.G
G.G
T.G
G.G
T.G
G.G
T.G
G.G
T.G
A.G
A.G
A.G
A.G
A.G
A.G
A.T
C.T
G.T
T.T
A.T
C.T
G.T
T.T
A.T
C.T
G.T
T.T
A.T
C.T
G.T
T.T
A.T
C.T
G.T
T.T
A.T
C.T
G.T
T.T
T.C
T.C
T.C
T.C
T.C
T.C
A.A
C.A
G.A
T.A
A.A
C.A
G.A
T.A
A.A
C.A
G.A
T.A
A.A
C.A
G.A
T.A
A.A
C.A
G.A
T.A
A.A
C.A
G.A
T.A
Context DDR mutated* 0.65 (0.504, 0.847)
**Mutation signatures defined according to v2 of the Catalog of Somatic Mutations in Cancer (COSMIC), DDR wild-type* 0.89 (0.489, 1.612)
https://cancer.sanger.ac.uk/cosmic/signatures_v2.tt.
DDR, DNA damage repair. 0.0 0.5 1.0 1.5 2.0
*Classified according to DNA damage response and repair genes in pathways associated with mismatch repair, Favors avelumab + BSC Favors BSC alone
nucleotide excision repair, homologous recombination, Fanconi anemia, and checkpoint control, as reported by Teo 43
MY, et al. J Clin Oncol 2018;36:1685-1694.Tumor gene expression data can identify genes that
may be associated with OS benefit from avelumab
Immune-related genes are associated with OS benefit from avelumab
Avelumab + BSC BSC alone
6 6
GBP4
GBP1 CXCL9
LAG3
CXCL10
IFNG CD8B
TIGIT CD8A
4 FOXP3 4
-log10(nominal p‒val)
TBX21 PDCD1 NKG7
ITGAE CXCR3
CTLA4
BATF2
HLA–DMA IL2RB CXCL11 p=0.001 SNCAIP
p=0.001
GZMA LY6D CCL28
ICOS IL12RB1
CD274
2 2
0 0
0.50 0.75 1.00 1.25 1.50 0.50 0.75 1.00 1.25 1.50
HR of high vs low gene expression in the avelumab + BSC arm, HR of high vs low gene expression in the BSC arm,
adjusted for age and sex adjusted for age and sex
44
Genes of interest with pRelationship between immune cell gene expression
signatures and OS with avelumab
Multiple immune cell signatures may predict OS benefit with avelumab
Signatures with interaction term pMedian vs ≤Median
HR (95% CI)
Follicular helper T cell 0.53 (0.367, 0.757)
0.92 (0.650, 1.297)
Activated NK cell 0.53 (0.365, 0.760)
0.90 (0.641, 1.268)
T cell γδ T cell 0.52 (0.362, 0.759)
0.90 (0.642, 1.263)
0.54 (0.374, 0.774)
Resting NK cell
0.90 (0.638, 1.272)
NK cell CD4 T cell
0.55 (0.384, 0.800)
0.86 (0.614, 1.211)
0.54 (0.375, 0.785)
Regulatory T cell
Macrophage 0.88 (0.629, 1.234)
0.55 (0.379, 0.794)
CD8 T cell
0.88 (0.628, 1.230)
0.56 (0.382, 0.810)
Dendritic cell Memory activated CD4 T cell
0.84 (0.602, 1.173)
0.57 (0.400, 0.803)
Naïve B cell
0.89 (0.619, 1.269)
0.56 (0.388, 0.817)
B cell Macrophage M1 0.84 (0.603, 1.181)
0.59 (0.405, 0.846)
Activated dendritic cell 0.82 (0.581, 1.143)
0.64 (0.443, 0.921)
Plasma cell 0.78 (0.558, 1.099)
Gene signatures are from the Leukocyte gene signature 0.0 0.5 1.0 1.5 2.0
matrix (LM22), Newman et al (2015) Nature Methods, Favors avelumab + BSC Favors BSC alone
https://doi.org/10.1038/nmeth.3337 45Immune cell gene signatures suggest that cell types
expressing Fc receptors may contribute to outcomes
Different alleles with distinct IgG1 affinity
Signatures with interaction term pMedian vs ≤Median
and cellular expression
Follicular helper T cell FcγRIIA FcγRIIIA
Activated NK cell
CD CD32A CD16A
T cell γδ T cell Structure
Resting NK cell
NK cell CD4 T cell
Regulatory T cell Alleles H131 R131 V158 F158
Macrophage
CD8 T cell IgG1 affinity 5x106 3x106 2x105 1x105
Expression
Dendritic cell Memory activated CD4 T cell
NK cells - +
Naïve B cell Mono/MՓ + +
DC + -
B cell Macrophage M1 Basophil + -
Mast cell + -
Activated dendritic cell Eosinophil + -
Platelet + -
Plasma cell
0.0 0.5 1.0 1.5 2.0
Favors avelumab + BSC Favors BSC alone
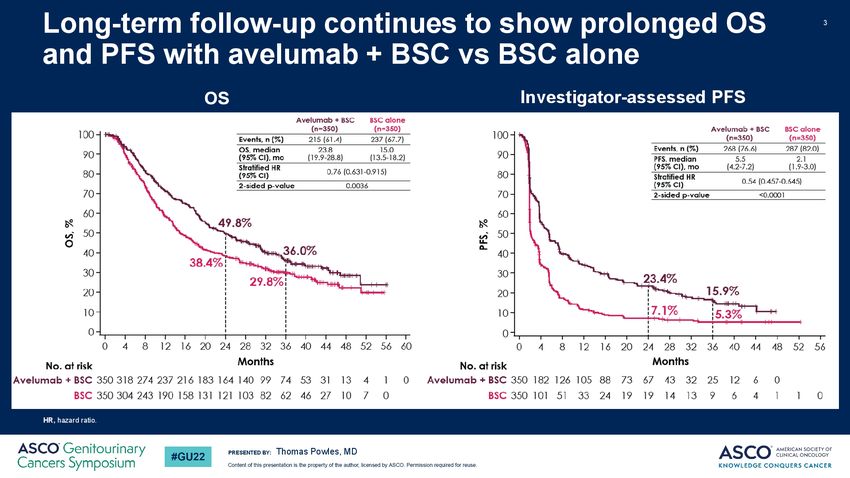
46Correlation between number of high-affinity FcγR
variants and outcomes with avelumab
May indicate contribution of FcR-mediated antitumor mechanisms
Number of loci encoding
Arm high-affinity FcγR variants HR (95% CI)
100 (FCGR2A and FCGR3A)
90
Avelumab + BSC
≥2 0.53 (0.384, 0.732)
BSC alone
80
Avelumab + BSC
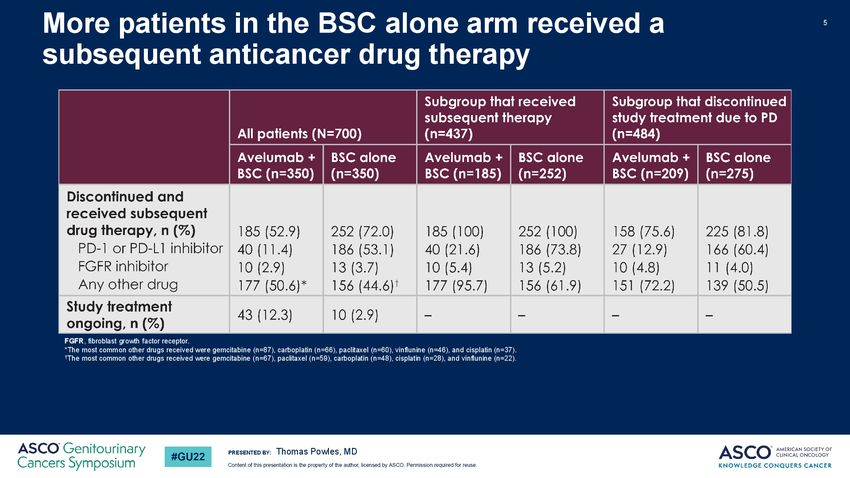
70Exploring relationships between established immune
active gene signatures and outcomes
≤Median >Median
100 100
90 90
80 80
70 70
JAVELIN-Immuno 60 60
26-gene signature tested in a trial
OS, %
50 50
of avelumab + axitinib in renal cell
carcinoma1 40 40
30 30
20
HR 0.87 (95% CI 0.618, 1.222) 20
HR 0.55 (95% CI 0.383, 0.796)
Avelumab + BSC Avelumab + BSC
10 BSC alone 10 BSC alone
0 0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
100 100
90 90
80 80
70
T cell-inflamed 60
70
60
18-gene signature defined in
OS, %
50 50
220 patients with 9 tumor
types2 40 40
30 30
20
HR 0.94 (95% CI 0.673, 1.299) HR 0.49 (95% CI 0.332, 0.719)
20
Avelumab + BSC Avelumab + BSC
10 BSC alone 10 BSC alone
0 0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
Months Months
48
1. Choueiri T.K, et al. J Clin Oncol 2019;37:(suppl; abstr 101); 2. Ayers M, et al. J Clin Invest 2017;127:2930–2940.Signaling pathways that may reduce OS benefit in
patients with elevated antitumor immunity
Possible targets of combination therapy
>Median and ≤Median
HR (95% CI)
JAVELIN-Immuno low 0.87 (0.618, 1.222)
All patients
JAVELIN-Immuno high 0.55 (0.383, 0.796)
>Median 0.59 (0.378, 0.932)
Notch
≤Median 0.42 (0.214, 0.814)
>Median 0.59 (0.384, 0.903)
Hedgehog
≤Median 0.43 (0.206, 0.904)
>Median 0.63 (0.388, 1.007)
TGFβ
≤Median 0.44 (0.240, 0.801)
>Median 0.70 (0.451, 1.079)
Angiogenesis
≤Median 0.30 (0.148, 0.628)
Pathway signatures from MSigDB Hallmark Gene Set Collection 0 0.5 1.0 1.5 2.0
Liberzon et al (2015) Cell Systems Favors avelumab + BSC Favors BSC alone
49Prevail (biomarker) study in advanced UC
Co-PIs:
Petros Grivas
Joshua Meeks
Proprietary and Confidential ©AstraZeneca 2017 • FOR INTERNAL USE ONLYImmunomodulation and TIS Proprietary and Confidential ©AstraZeneca 2017 • FOR INTERNAL USE ONLY
52
NEW BIOMARKER DATA COMPLEMENTARY TO MRx0518 MONOTHERAPY DATA
As previously reported from monotherapy data in treatment-naïve patients, MRx0518:
• increases CD8+ T cells, NK cells and antigen-presenting cells in the tumor
• increases circulating anti-tumor cytokines and chemokines (IL-12, CXCL10)
• changes expression of genes associated with key-anti tumor pathways (antigen presentation, interferon response)
• increases Tumour Inflammation Signature (TIS) – an gene expression profile associated with better ICI outcomes 1,2
All Pts Breast
(n=14) (n=7)
© 4D Pharma plc
Lythgoe et al., JITC 2020 (#805), Lythgoe et al., Ann Oncol 2021 (#543P). 1 Ayers et al., J Clin Invest 2017; 2 Damotte et al., J Transl Med 201953
CLINICAL IMMUNO-STIMULATORY ACTIVITY CONSISTENT WITH PRE-CLINICAL SIGNALS
• On study changes in biomarkers across studies to date (KEYTRUDA® combination, neoadjuvant monotherapy study,
and pre-clinical) confirms MRx0518 immuno-stimulatory activity (T cell and TIS signatures)
T cells signature TIS/approximated TIS signature
Pre-clinical samples Clinical samples Pre-clinical samples Clinical samples
5 8 8 9
8
4 6 7
T cells score
T cells score
TIS score
TIS score
7
3 6
4 6
2 5
5
2
1 4 4
8
8
e
e
rg
rg
n
n
51
51
l
l
g
g
ic
ic
Su
Su
ia
ia
x0
x0
h
h
D
D
Ve
Ve
R
R
M
M
© 4D Pharma plc54 NEXT STEPS FOR MRx0518 DEVELOPMENT
Key Takeaways
• Baseline biomarkers (including TIL infiltration, TIS) have been shown to correlate with better outcomes to ICI therapy
• The immune changes that MRx0518 induces in tumors are similar to the profiles observed in patients with better response
to ICIs in landmark studies in first-line settings
• This, paired with clinical efficacy signal observed in MRx0518 + KEYTRUDA® combination study, gives 4D pharma
confidence taking MRx0518 into earlier lines of treatment with larger patient populations
• Phase II AVENU study – combination of MRx0518 and BAVENCIO® (avelumab), first-line maintenance therapy for
urothelial carcinoma, commencing 1H 2022
• Additional potential earlier line settings in renal cell carcinoma and other tumor types
Next Steps
• Following primary endpoint being met in Part B of study in RCC group, discuss with collaborators and 4D pharma’s
Genitourinary Cancers Advisory Board options for progressing MRx0518 into a potentially pivotal study in ICI-refractory
RCC patients
• Continue to explore studies of MRx0518 in earlier line settings
© 4D pharma plc55 CONTACT US
General enquiries: info@4dpharmaplc.com
Investor Relations: ir@4dpharmaplc.com
Clinical: clinicaltrials@4dpharmaplc.com
© 4D pharma plcYou can also read