LUNG CANCER IN LATIN AMERICA: Time to stop looking away Sponsored by: ICCP Portal
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
LUNG CANCER
IN LATIN AMERICA:
Time to stop looking away
Sponsored by:LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
CONTENTS
2 About this report
4 Executive summary
8 Chapter 1: Latin America’s lung cancer challenge
8 I. The high human cost
10 Box: What is lung cancer?
12 II. The high economic cost
17 III. A closer look at the risks: more than just tobacco
21 IV. Latin America’s future lung-cancer burden: countervailing winds
25 V. The wider context
29 Chapter 2: Assessing the policy response to lung cancer in Latin
America
29 I. Introducing The Economist Intelligence Unit’s Latin America Lung
Cancer Traffic Lights
30 Box: How to read the traffic lights
32 II. Prevention (tobacco control and non-tobacco prevention)
35 III. Access
39 IV. Early diagnosis
42 V. Treatment
44 VI. Non-curative services
46 VII. Information and advocacy
48 VIII. Data quality
50 Conclusion: Time to pay attention
51 Appendix I: Methodology of the economic model
51 1. Direct costs
57 2. Indirect costs
58 3. Interpolation of results to other Latin American countries
60 Appendix II: Methodology of the traffic-light assessment
© The Economist Intelligence Unit Limited 2018 1LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
ABOUT THIS REPORT
Lung cancer in Latin America: Time to stop looking away is an Economist Intelligence Unit report,
commissioned by Roche, which examines the burden of lung cancer in Latin America and how well
countries in the region are addressing the challenge. Its particular focus is on 12 countries in Central
and South America, chosen for various factors including size and level of economic development:
Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Ecuador, Mexico, Panama, Paraguay, Peru and
Uruguay.
This study looks in detail at the disease burden as well as the economic and social burden of lung cancer
in the region. It also introduces a major tool for stakeholders seeking to understand the policy response
to lung cancer: the Latin America Lung Cancer Traffic Lights. The traffic-light system assesses national
policy approaches, and to some extent outcomes, in Latin America. The Economist Intelligence Unit
performed a rapid literature review to identify key issues around lung cancer in Latin America. We then
held an advisory board meeting with regional experts in order to determine on which key categories,
called domains, to focus. Following the advisory board’s recommendations, we split the domains
into three Priority Traffic Lights (those without which other progress would be impossible) and five
Important Traffic Lights, which, while still crucial for successfully addressing the lung cancer challenge,
were deemed less central than the Priority Traffic Lights.
The three Priority Lights are as follows: tobacco control, access, and early diagnosis. The Important
Lights include the following five domains: treatment, non-curative services, non-tobacco prevention,
information and advocacy, and data quality. The purpose of the traffic-light system is not to rank
countries or single out countries performing less well. Rather, it will serve as the starting point for
further discussion on policy progress and gaps that will be further explored in this white paper.
Our thanks are due to the following for their time and insight (listed alphabetically):
Advisory board members
Miguel Agüero, clinical oncologist, Instituto Nacional del Cáncer, Paraguay
Oscar Arrieta, co-ordinator, lung cancer and thoracic tumours clinic, Instituto Nacional de
Cancerología, Mexico
Mauricio Burotto, oncologist (until recently), Clinica Alemana de Santiago, Chile
Eduardo Cazap, founder and first president, Latin American and Caribbean Society of Medical
Oncology
Mauricio Cuello, deputy director, Instituto Nacional del Cáncer, Uruguay
Gilberto Lopes, director of global oncology, University of Miami Miller School of Medicine
Luis Mas, executive director of medical oncology (until recently), Instituto Nacional de Enfermedades
Neoplàsicas, Peru
Patricia Mondragón, chair, Respirando con Valor, Mexico
2 © The Economist Intelligence Unit Limited 2018LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
Diego Paonessa, executive director, Liga Argentina de Lucha contra el Cáncer
Luis E Raez, medical director, Memorial Cancer Institute, Florida; visiting professor of medicine,
Cayetano Heredia University, Peru
Nilda Villacrés, executive director, National Health Council, Ecuador
Ignacio Zervino, co-ordinator of programmes, Fundación Pacientes con Cáncer de Pulmón, Argentina
Experts providing assistance with the economic model and treatment pathway
Clarissa Baldotto, director of oncology, Oncologia D’Or, Brazil
Gustavo Fernandes, president, Sociedade Brasileira de Oncologia Clinica, Brazil
Marcos Santos, health economist and bioethics professor, University of Brasília, Brazil
Stephen Stephani, clinical oncologist, Hospital do Câncer Mãe de Deus, Brazil
Other experts providing assistance
Osvaldo Aren, oncologist and executive director, Centro de Investigación Clínica Bradford Hill, Chile
Juan-Pablo Barés, president, FUNDACÁNCER, Panama
Gonzalo Vargas Chacón, co-ordinator, Consenso Nacional de Especialistas en Cáncer, Costa Rica
Ricardo Pérez Cuevas, assistant director-general for the centre for the investigation of health systems,
Instituto Nacional de Salud Pública, Mexico
Luciana Holtz, CEO, Oncoguia Institute, Brazil
Clarissa Mathias, clinical oncologist, Núcleo de Oncologia da Bahia
Milton Soria, head of the pathology unit, Instituto Nacional de Laboratorios en Salud, Bolivia
We would also like to thank the International Association for the Study of Lung Cancer for its
assistance.
The report was written by Paul Kielstra and edited by Martin Koehring of The Economist Intelligence
Unit. The development of the economic burden study was led by Christine Bishop of The Economist
Intelligence Unit Healthcare team.
September 2018
© The Economist Intelligence Unit Limited 2018 3LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
EXECUTIVE SUMMARY
Lung cancer is Latin America’s deadliest neoplasm, but frequently gets less attention than other
major cancers. Until recently, the implications were small: unless caught very early—which is difficult
given a lack of distinct symptoms at that stage—the prognosis was poor anyway. Medical advances,
though, now hold out the hope of prolonged life, or even cures, for a growing, if still small, number of
patients. It is time to look more closely at the region’s response to this disease and current strengths
and weaknesses of efforts to address it.
Doing so will require understanding the regional peculiarities of the lung-cancer burden. The drivers
of the disease differ from those in most developed countries. While tobacco smoking remains the
dominant issue, poverty—and the attendant use of indoor solid fuels for cooking and heating—appears
to play an important role in certain countries, as does the natural environment, especially sometimes
high levels of arsenic in groundwater. These differences in risk factors, in turn, affect the genetics
of lung tumours, and therefore treatment potential. The lung-cancer challenge in Latin America,
therefore, needs to be understood on its own terms.
Data deficiencies, though, inevitably impede almost any cancer-control discussion in the region.
Accordingly, for this project, The Economist Intelligence unit has conducted two substantial research
efforts: an economic model to estimate the direct and indirect costs of lung cancer in 12 countries
in the region (known as the study countries)1; and a bench-marking tool to assess, in those same
countries, the state of national lung-cancer control efforts across various domains. These, along with
insights from 23 regional experts, collectively inform this study.
Its key findings include:
Lung cancer is not a single disease, but some forms are becoming susceptible to treatment.
Lung cancer can be understood as a family of neoplasms that all strike the lung first. The main divisions
are between small-cell and non-small-cell lung cancer and, in the latter sub-group, adenocarcinoma,
squamous cell lung cancer and large-cell lung cancer. It is non-small-cell lung cancer that has seen
the biggest medical advances in recent years with inhibitors for specific genetic mutations and
immunotherapy showing great promise.
The human and economic costs are substantial. Although estimates vary, in the study countries
over 60,000 people die each year from lung cancer, which represents 12% of all neoplasm deaths there.
The estimated bill for diagnosis, treatment and palliative care (the direct costs) comes to US$823m in
2016 in Brazil. Rather than make individual calculations for other countries, for some of which the data
would not even be available, we use a process called interpolation (see Appendix I) to estimate the
total figure for the 12 study countries at US$1.35bn. Indirect costs are significant too, but substantially
lower than the direct costs, at US$286m for the entire region—a figure reduced by the large proportion
1
Argentina, Bolivia, Brazil, Chile, Colombia,
of those developing lung cancer who are past the relevant national retirement ages.
Costa Rica, Ecuador, Mexico, Panama,
Paraguay, Peru and Uruguay.
4 © The Economist Intelligence Unit Limited 2018LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
Tobacco is the dominant but far from the only risk. The link between smoking and lung cancer
is widely understood, but this knowledge can crowd out awareness of other carcinogens. The Global
Burden of Disease Study from the World Health Organisation (WHO) estimates that, in our study
countries, tobacco is responsible for 64% of lung cancer. The remaining 36%, however, on its own
would remain a major public health issue, on a par with cervical cancer in our study area. The main
non-tobacco risks in the region are indoor and outdoor air pollution, residential radon gas, and arsenic
in drinking water. The extent of these dangers is difficult to estimate because of the lack of relevant
research in much of the region.
Smoking is down, but the impact on lung cancer burden depends on the metric used. Tobacco
consumption in Latin America has seen a marked decrease in recent decades, with the WHO
estimating that Panama’s smoking prevalence fell by over half between 2000 and 2015—the biggest
drop in the world—while even the worst performer in the study, Chile, saw a decline of a fifth. This will
inevitably lead to fewer cases of lung cancer eventually, but when exactly is harder to say because of
the various lung carcinogens in the region, their typically long latency periods, and the later rise and
fall in female smoking rates compared with male ones. In most study countries, male age-standardised
lung cancer mortality rates—which factor out demographic changes—have declined to some extent
or stayed flat. In a few, such as Mexico, Colombia and Costa Rica, so have female ones. For the most
part, however, population growth and ageing mean that the crude rates of cancer for both sexes, and
case numbers, have risen or, at best, been flat. In the short term, the benefits of smoking cessation will
probably appear only slowly.
Stigma impedes various elements of lung-cancer control. As one expert told this study, “in Latin
America…the way we see lung cancer is that ‘these guys are guilty. They did it to themselves.’ There is
no compassion.” Various survey results tell the same story. As a result, lung cancer seems to be treated
as a second-class neoplasm, with surprisingly low research funding, for example, compared with its
health burden. Although high cost is also an issue, interviewees suspect that stigma may also partly
explain lower willingness to fund lung-cancer treatment than that for other cancer treatments where
resources are limited.
The Latin America Lung Cancer Traffic Lights: a national benchmarking tool. We publish here
the results of our traffic light analysis that addresses key elements of lung-cancer control in the study
countries. On our expert advisory panel’s recommendation, these fall into two groups. The first are the
Priority Lights: tobacco control; access; and diagnosis. The other five Important Lights are areas that
are also crucial: treatment; non-curative services; non-tobacco prevention; information and advocacy;
and data quality. A green light in any given area (called domains) indicates that countries are doing
well by relevant global or regional standards; amber denotes an area of concern; and red a need for
substantial attention.
The traffic lights give two overarching messages: substantial room for improvement overall
and the need to make progress beyond tobacco control and data quality. The study countries
are not doing well overall. The vast majority of lights are amber or red, with only 15% green. Experts
© The Economist Intelligence Unit Limited 2018 5LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
interviewed for this study point to the low attention given to lung cancer, and in particular a lack of
government focus as the likely explanation. In fact, efforts are concentrated almost exclusively on
tobacco control and data quality: all green lights but one appear in these two domains. Both are
necessary, but it is short-sighted to think them sufficient.
Tobacco control is a growing strength in the region, but non-tobacco lung cancer prevention
needs significant attention. Most study countries score green on tobacco control, with the rest
amber. Appropriate regulation, including on smoke-free public places, and taxation on cigarettes is
widespread. This progress has occurred mostly in the past decade and requires ongoing support in the
face of opposition from the tobacco industry. Nevertheless, these efforts appear to be bringing about
the necessarily underlying cultural change in attitudes towards smoking across the region. Prevention
related to other causes of lung cancer, however, lags far behind. In much of the region, even the levels
of radon-gas concentrations and arsenic in drinking water are uncertain, while air pollution limits
remain above WHO recommendations.
Access challenges remain a substantial barrier. Last year’s publication accompanied the release
of the Latin America Cancer Control Scorecard (LACCS), which covered the same countries discussed
here, and looked in detail at the challenges of accessing cancer diagnosis and treatment for those with
limited financial means or living away from major cities.2 These remain, with public care behind private
to a worrying extent. Worse still, public care is not always affordable. Some government programmes
that cover the high costs of other cancers do not do so for lung cancer, notably Mexico’s Seguro Popular
and Chile’s Régimen de Garantías Explícitas en Salud. Access challenges and mediation costs, both
general and specific to lung cancer, help explain why payment for lung cancer drugs is a frequent
theme in the growing patient litigation around rights to healthcare.
Diagnosis occurs too late, but screening remains controversial. Early diagnosis of lung cancer
saves lives but is difficult. In Japan, for example, 58% of patients with the disease are found at stage
III or IV. In our study countries, this figure is much worse, with most around 85% and Mexico at 99%.
Screening has helped with downstaging of other neoplasms, and a major US study indicated it could
cut lung cancer mortality by 21%. Pilot screening projects have occurred in Brazil, and one is taking
place in Mexico. Generally, however, health systems are reluctant to adopt this approach because of
cost, uncertainty over its applicability to regional populations, and lack of health-system preparedness.
Unfortunately, very few other initiatives exist to detect lung cancer earlier. Accordingly, this is one of
the areas where the study countries as a group do worst.
Treatment has some strengths, but lack of resources impedes better care. Lung-cancer
treatment varies widely by country: some, such as Uruguay and Argentina, have better provision,
even for those with limited financial means, while others, notably Paraguay and Bolivia, provide only
the very basics. Most study countries have national treatment guidelines, although it is surprising
that Chile lacks them. Putting the guidelines into practice is another matter, with health-system
2
The Economist Intelligence Unit, “Cancer
fragmentation and limited resources impeding, or reducing, the availability of multidisciplinary care.
Control, Access and Inequality in Latin
America: A tale of light and shadow”, 2017. Not surprisingly, a few leading systems are able to begin treatment as quickly as those in developed
6 © The Economist Intelligence Unit Limited 2018LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
countries, but others lag far behind, with Mexico taking on average four and a half months from
diagnosis to treatment.
Too often care stops with the end of curative interventions. The study countries are weak on care
that goes beyond curative intervention, even though, in theory, every patient could benefit. Palliative
care, broadly speaking, should have two roles with lung cancer: helping with symptom management
from the time of diagnosis, and continuing to provide such relief until death if curative care fails. In the
study countries only Argentina, Chile, Costa Rica, Panama and Uruguay have the capacity to provide
this. Meanwhile, as lung cancer transforms in some cases from a terminal to a chronic condition,
survivorship care will become a growing concern. Just Colombia and Mexico, however, have guidelines
encouraging pulmonary rehabilitation, a likely essential element of any future survivorship programme.
There are few awareness-raising efforts and patient advocacy groups. Lung-cancer awareness
is very low in the region with, for example, half of Brazilians and Argentinians unable to name a single
correct symptom. Unfortunately, most study countries are doing too little to improve knowledge.
Despite the region’s strength in tobacco control, five study countries did not conduct national anti-
smoking campaigns in 2014 or 2016 (as recorded by the Tobacco Atlas), including Chile and Bolivia,
where smoking prevalence remains high. Broader lung-cancer awareness activity, meanwhile, was rare,
with only four countries showing evidence of substantial efforts in recent years. The awareness-raising
that does occur is usually the work of patient advocacy groups, but there are few in the region.
Data quality continues to improve but lags on lung cancer. As reported in our LACCS study,
registry quality is getting better across Latin America, which helps to explain the high number of green
lights in this domain. Unfortunately, lung-cancer data quality lags that of other neoplasms, with more
than twice as many registered cases coming from death records on average. Unfortunately, mortality
data are also often weak in the region, with only five countries getting full marks. On the plus side,
in the absence of a specific lung-cancer registry, researchers are engaging in substantial data sharing
through the Latin American Consortium for the Investigation of Lung Cancer.
© The Economist Intelligence Unit Limited 2018 7LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
CHAPTER 1: LATIN AMERICA’S
LUNG CANCER CHALLENGE
I. The high human cost
Lung cancers kill more people in Latin America than any other kind. Varying estimates paint the same
picture. According to the International Agency for Research on Cancer (IARC), in 2012 (its latest data)
just above 60,000 people died from lung cancer in the countries included in this study. The WHO’s
Global Burden of Disease (GBD) figures, using a different methodology, put the 2016 figure at just
above 65,500. In both cases, this represents more than 10,000 more lives lost than the next most lethal
cancer and around 11-12% of all neoplasm deaths.3
Lung cancer’s unenviable distinction does not come from a particularly elevated incidence. In the study
countries, breast cancer (around 132,000 new cases in 2012, according to the IARC) and prostate cancer
(126,000 new cases) appear nearly twice as often as lung cancer (68,900 new cases). This is the case
despite the fact that the latter strikes both sexes, while prostate cancer affects men (the equivalent
for women strikes the Skene glands) and breast cancer primarily affects women (male breast cancer
is rare).
Medicine, however, has to date been much less successful against lung cancer. The proportion of
people who die from a disease in a given year to the number of new cases—the mortality-incidence
(M:I) ratio—is a rough measure of how health systems are coping with a disease. For lung cancer, the
M:I ratio was 87% in 2012, the third-highest after liver and pancreatic cancer.4
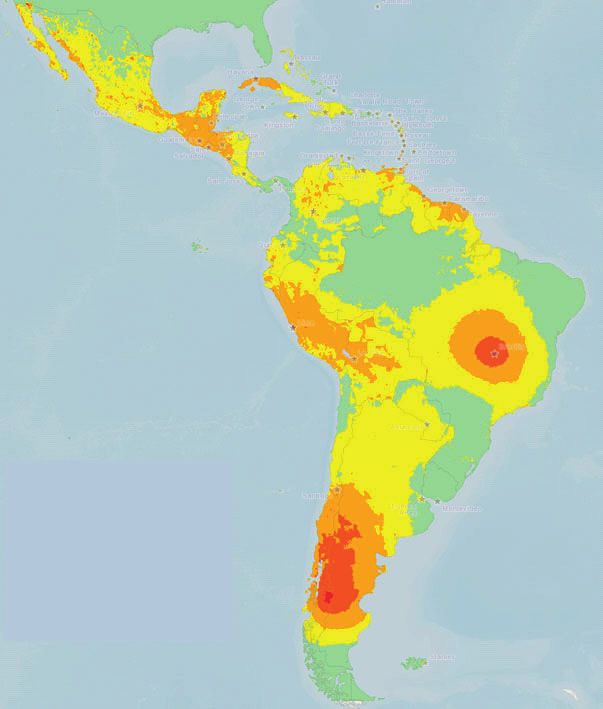
In global terms, these stark numbers are unremarkable: lung cancer is a common scourge. Latin
America’s overall incidence and mortality figures are mid-way between North America and European
highs and typically African lows (see Chart 1). Whatever challenge others face, though, even this
average burden from lung cancer poses a major public-health issue for the region.
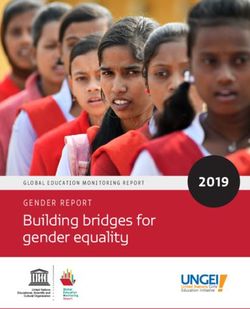
This regional overview covers marked national variation. National age-standardised rates (ASR) of
lung-cancer incidence and mortality differ substantially. For both, the burden of Uruguay, the most
affected country, is nearly six times higher than that of Bolivia, the least affected (see Table 1). More
3
Institute for Health Metrics and Evaluation constant is the disease’s ranking as a killer: for most study countries, it is among the three cancers
(IHME), GBD Results Tool. Available at: http://
causing the most deaths. The only real outliers are Costa Rica and Bolivia. As Milton Soria, head of the
ghdx.healthdata.org/gbd-results-tool & IARC
Globocan Database, Incidence/Mortality > pathology unit at Bolivia’s Instituto Nacional de Laboratorios en Salud, puts it, “here, lung cancer is not
Rates: Cancers by population. Available at: as relevant as you might think” because other forms of the disease exact a higher toll. Similar M:I ratios
http://globocan.iarc.fr/Pages/summary_table_
across the region, though, indicate that no health system is detecting or treating the disease well.
pop_sel.aspx
Dramatic medical advances could now ameliorate these bleak mortality figures. Oscar Arrieta, co-
4
IARC Globocan Database, Incidence/
ordinator of the lung cancer and thoracic tumours clinic at Mexico’s Instituto Nacional de Cancerología,
Mortality > Rates: Cancers by population.
Available at: http://globocan.iarc.fr/Pages/ reports that “the treatment pipeline has changed dramatically in the last five years”. So much so that
summary_table_pop_sel.aspx Mexico’s extensive 2013 treatment guidelines had to be revised in 2016 and are undergoing yet another
8 © The Economist Intelligence Unit Limited 2018LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
Chart 1
Lung cancer age-standardised incidence by country, 2012
Lung cancer
27.4+
15.8-27.4
8.0-15.8
2.9-8.0
Rates: Cancers by population. Available at: http://globocan.iarc.fr/
Pages/summary_table_pop_sel.aspx
© The Economist Intelligence Unit Limited 2018 9LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
reworking. Luis E Raez, medical director of the Memorial Cancer Institute in Florida and visiting
professor of medicine at Cayetano Heredia University in Peru, adds that targeted therapies and
immunotherapy have grown so much in the past five years in the US that “about 20% of lung cancer
patients can get oral therapy instead of chemotherapy”.
The results are heartening. Two studies suggest longer lives, at least for those with appropriate
biomarkers of susceptibility to given treatments. Overall, among those diagnosed at the most
advanced stage (stage IV), the potential to survive five years or more has gone from 4% a few years
ago to 16%.5 “It is still a very lethal disease,” Dr Raez warns, but for some lung-cancer patients greatly
extended lives, even cures, are now possible.
These treatments, however, come at a cost. Ricardo Pérez Cuevas is leading a team at Mexico’s Instituto
Nacional de Salud Pública that is revising earlier estimates of the cost of lung-cancer treatment made
BOX: WHAT IS LUNG CANCER?
Lung cancer is a category of diseases that have Non-small-cell lung cancer (NSCLC) is again
5
Scott Gettinger et al, “Five-Year Follow-Up
in common the body organ where they strike a category rather than a single disease and
of Nivolumab in Previously Treated Advanced
Non–Small-Cell Lung Cancer”, Journal of first. Previously, key terms for describing kinds includes almost all remaining lung cancers.
Clinical Oncology, 2018 & Jessica J Lin, “Five- of lung cancer betrayed a focus—sometimes Medicine has made far more progress here
year survival in EGFR-mutant metastatic lung
shielded by classical vocabulary—anchored than on SCLC in recent years. The main types
adenocarcinoma treated with EGFR-TKIs”,
Journal of Thoracic Oncology, 2016. around basic descriptions of what these cancers of NSCLC are:
look like or where they occur. This reflected the
l Adenocarcinoma: this is the most common
6
See, for example, Estelamari Rodriguez and limits of earlier science. The vast strides biology
NSCLC, which occurs in the lung’s mucus
Rogerio C Lilenbaum, “Small Cell Lung Cancer:
has made in recent decades, though, have
Past, Present, and Future”, Current Oncology producing glands (“adeno” from the Greek for
Reports, 2010 & Tatiana N Zamay et al, shifted consideration to how these tumours
“gland”).
“Current and Prospective Protein Biomarkers operate, thereby opening a greater, if still
of Lung Cancer”, Cancers, 2017. l Squamous cell carcinoma: the next most
limited, range of treatment options.
frequent NSCLC appears in the lung lining, the
7
American Cancer Society, “Small Cell Lung The main first division within the lung-cancer so-called squamous cells (from the Latin word
Cancer Survival Rates, by Stage”, available at
family is based on physical appearance: for “scales”).
https://www.cancer.org/cancer/small-cell-
lung-cancer/detection-diagnosis-staging/
Small-cell lung cancer (SCLC) gets its name l Large-cell carcinoma: this third major
survival-rates.html & “Non-Small Cell Lung
Cancer Survival Rates, by Stage”, available at from the size of its cells. Making anywhere NSCLC is much less prevalent than the others.
https://www.cancer.org/cancer/non-small- from around 10-25% of lung cancers, SCLC is
6
It can appear anywhere in the lung.
cell-lung-cancer/detection-diagnosis-staging/
survival-rates.html#references.
especially aggressive and difficult to treat. In
These categories are neither exclusive nor
the US, even if diagnosed at stage I, the relative
exhaustive: for example, a very small number
8
For a detailed description of the biology
five-year survival rate is only 31%; for other
of adenosquamous cancers, with the features
of the different types of lung cancer, see lung cancers, depending on sub-stage, this
William D Travis et al, “The 2015 World Health of both the first two listed, occur. These three,
figure ranges from 68% to 92%.7
Organization Classification of Lung Tumors”, though, constitute the vast majority of NSCLCs.8
Journal of Thoracic Oncology, 2015.
10 © The Economist Intelligence Unit Limited 2018LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
9
Ole Raaschou-Nielsen, “Air pollution and
Although all are called lung cancer, the division. In Latin America, the figure is 26%.13 lung cancer incidence in 17 European cohorts”,
underlying biology of these diseases has Several EGFR inhibitors exist. Lancet, 2013 & Oscar Arrieta, et al, “Clinical and
Pathological Characteristics, Outcome and
long been understood to differ. The greater
l ALK (anaplastic lymphoma kinase): Mutational Profiles Regarding Non–Small-
aggressiveness of SCLC is one clear example. Cell Lung Cancer Related to Wood-Smoke
again more common in never-smokers, an
So are non-tobacco risk factors. Air pollution Exposure”, Journal of Thoracic Oncology, 2012
ALK translocation is a rearrangement of
& How-Ran Guo et al, “Cell Type Specificity
and wood smoke, for example, are associated
an otherwise useful gene found in 4-11% of of Lung Cancer Associated with Arsenic
with high rates of adenocarcinoma, while Ingestion”, Cancer Epidemiology, Biomarkers
adenocarcinomas.14 When present, it creates
ingesting arsenic through drinking water & Prevention, 2004.
a protein that causes cell growth and spread.
increases the risk of squamous cell carcinoma.9
Several drugs target this protein too. 10
Victor Martinez et al, “Arsenic and Lung
Moreover, arsenic-induced squamous lung Cancer in Never-Smokers: Lessons from
cancers have different DNA copying patterns l KRAS (Kirsten Rat Sarcoma viral oncogene): Chile”, American Journal of Respiratory and
KRAS was one of the earliest mutations found Critical Care Medicine, 2012.
from those where smoking is the cause.10
in adenocarcinomas. It affects 25-30% of 11
Tatiana N Zamay et al, “Current and
Recent bioscience advances allow far greater such lung cancers, although in Latin America Prospective Protein Biomarkers of Lung
understanding of these biological differences, the figure appears to be 14%.15 Its biology is Cancer”, Cancers, 2017.
making our understanding of NSCLC yet more complex, interacting negatively with growth
12
Megan Baumgart and Kishan Pandya, “The
complex. factors and tumour suppressors. Despite use of biomarkers in the treatment of non-
extensive study, a therapy to inhibit KRAS’s small cell lung cancer”, Expert Review of
As with other cancers, those of the lung
Precision Medicine and Drug Development,
impact does not yet exist.16 Finding one would
produce biomarkers—strands of DNA, 2016.
be particularly useful: the mutation appears
proteins, or other molecules and attributes—
only where EGFR and ALK ones do not. Data on prevalence of mutations from:
which both indicate how they behave and
13
Megan Baumgart and Kishan Pandya, “The use
differentiate them from cancers of the l PD-1/PD-L1 (Programmed cell death 1/
of biomarkers in the treatment of non-small
same type. Currently, dozens of identified Programmed cell death ligand 1): the PD- cell lung cancer”, Expert Review of Precision
or potential biomarkers are associated with L1 protein exists in healthy cells to protect Medicine and Drug Development, 2016 &
Oscar Arrieta et al, “Updated Frequency of
different kinds of lung cancer. Not all will
11
them from autoimmunity, but cancers can EGFR and KRAS Mutations in Non Small-Cell
necessarily have clinical value, but hopes hijack them to fool immune systems into Lung Cancer in Latin America”, Journal of
Thoracic Oncology, 2015.
are high: an estimated 60% of lung-cancer not killing a tumour. This may contribute to
tumours have at least one genetic mutation anywhere from 24% to 60% of lung cancers. 14
Ibid.
that helps to initiate or drive the disease on—a Immunotherapies—which assist the immune
15
Ibid.
higher figure than for most other cancers.12 system—are showing great promise in cancers
where abnormal PD-1 activity is found.17
To date, however, a limited number of Marta Román et al, “KRAS oncogene in non-
16
small cell lung cancer: clinical perspectives
biomarkers allow targeted clinical responses. The extent and potential treatability of
on the treatment of an old target”, Molecular
These appear largely in adenocarcinomas. The EGFR- and ALK-positive tumours have made Cancer, 2018.
following mutations are particularly relevant relevant molecular testing standard practice
17
Hui Yu et al, “PD-L1 Expression in Lung
to treatment, either for their frequency or for for adenocarcinomas.18 Other biomarkers
Cancer”, Journal of Thoracic Oncology, 2016 &
their susceptibility to specific therapies: can point to specific treatment options but Xiaoling Xu et al, “The efficacy and safety of
are less common. Biomarker testing as a part anti-PD-1/PD-L1 antibodies combined with
l EGFR (epidermal growth factor receptor): chemotherapy or CTLA4 antibody as a first-
of detailed diagnosis and treatment choice
more common in never-smokers, anywhere line treatment for advanced lung cancer”,
is therefore only likely to increase as we International Journal of Cancer, 2018.
from 15% to 40% of adenocarcinomas exhibit
understand more about the range of different
a mutation that creates too much EGFR,
diseases covered by the increasingly inexact
18
William D Travis et al, “The 2015 World
a protein that encourages cell growth and Health Organization Classification of Lung
term “lung cancer”. Tumors”, Journal of Thoracic Oncology, 2015.
© The Economist Intelligence Unit Limited 2018 11LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
before targeted therapies became available. Although the study continues, the advent of these new
drugs looks to have roughly tripled the cost of treatment per patient diagnosed at stages III and IV.
II. The high economic cost
Drug prices are not the only financial issue for lung cancer. For this research programme, The Economist
Intelligence Unit modelled the economic impact of the disease in the study countries. The calculations
included direct costs (those for medical interventions, such as diagnosis, treatment and palliative care)
and indirect costs (arising out of lost productivity from work absence and early mortality).
In this analysis the region’s poor healthcare data made it necessary to use a method called
interpolation. This estimates the economic impact on countries that lack published information by
making appropriate adjustments to data from a baseline country. Appendix 1 contains further details
of the model’s methodology, data and calculations.
Our baseline country, Brazil, shares with most of Latin America a high proportion of late lung-cancer
diagnosis: in Brazil 85% are found at stages III or IV.19 Such patients not only have a worse prognosis,
they cost more to treat. The following table gives the direct costs in Brazil (per patient and total) for
lung-cancer treatment, with separate calculations for the three-quarters of the population in the
public health system and the remainder with private insurance. Spending on the latter, predictably, is
higher per head, but to such a degree that, despite the much smaller number of patients, aggregate
spending also outstrips public outlay.
Table 2: Direct lung-cancer costs in Brazil by stage, public and private
sectors, 2016 (US$)
Stage of lung cancer Patients diagnosed Cases per stage Cost per stage Total costs per stage,
per stage per patient all patients
Public sector
Stage I & II 15% 3,820 5,564 21,257,654
Stage III 39% 9,933 9,587 95,224,887
Stage IV 46% 11,716 11,417 113,751,641
Total 100% 25,469 9,825* 250,234,182
Private sector
Stage I & II 15% 1,274 7,239 9,218,352
Stage III 39% 3,311 86,132 285,178,132
Stage IV 46% 3,905 71,354 278,652,826
Total 100% 8,490 67,497* 573,049,309
Note: * denotes the weighted average (obtained by dividing total costs by total number of cases).
Source: The Economist Intelligence Unit
19
Guilherme Costa et al, “Epidemiological We next estimated direct costs in the other study countries by adjusting the Brazilian ones for relative
changes in the histological subtypes of 35,018 differences from the baseline country in: healthcare spending per person; lung-cancer prevalence; and
non-small-cell lung cancer cases in Brazil”,
the split between public and private health insurance coverage.
Lung Cancer, 2016.
12 © The Economist Intelligence Unit Limited 2018LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
These national approximations require several grains of salt. Indeed, the per-head figures in particular
say nothing specific about measured national lung-cancer treatment activities; they are simply Brazil’s
figure multiplied by a composite measure of how its health system differs on a grand scale from the
baseline country. The figures are also implicitly based on two assumptions: first, that public-health
systems in every country provide similar care levels, as do private ones, and second, that each country
devotes a similar proportion of its total health spend to cancer. As discussed later in this report, the first
is unlikely: unlike Brazil’s public health service, Sistema Único de Saúde (SUS), for example, Mexico’s
Seguro Popular does not publicly fund lung cancer care. The second assumption is also improbable,
given the different stages of study countries in the epidemiologic transition that accompanies
economic development. Bolivia, for example, would rightly focus more on acute diseases than, for
example, Uruguay would.20 Similarly, in Peru, while further than Bolivia in this transition, “policymakers
face very complicated public-health problems, such as tuberculosis as well as other communicable
diseases such as malaria or hepatitis,” explains Luis Mas, until recently executive director of medical
oncology in Peru’s Instituto Nacional de Enfermedades Neoplàsicas. Unfortunately, data to rigorously
address these issues in our model do not exist.
Table 3: Direct lung-cancer costs in the 12 study countries, 2016
Estimated direct healthcare Prevalence Estimated per patient direct
costs for lung cancer (US$) cost for lung cancer (US$)
Argentina 207,199,992 12,626 16,411
Bolivia 6,051,264 908 6,668
Brazil 823,283,491 33,958 24,244
Chile 118,494,725 3,862 30,679
Colombia 34,138,430 5,205 6,558
Costa Rica 14,238,925 409 34,832
Ecuador 15,099,247 1,104 13,678
Mexico 76,240,001 9,676 7,879
Panama 13,104,402 415 31,599
Paraguay 7,190,620 827 8,699
Peru 15,505,888 2,576 6,019
Uruguay 32,167,918 1,645 19,559
Total 1,351,654,887 73,210 18,462
Note: These national figures do not reflect actual spending data and should not be used as such. They are approximations
based on Brazil’s figures and a step in the process of estimating the regional spending total.
Source: The Economist Intelligence Unit
Our aggregate regional figure is more robust because Brazil hews closely to the average of study
countries on cancer spending and care quality. Moreover, with 46% of the lung-cancer prevalence in
the study countries, its numbers would heavily influence any overall outcome.
For 2016 direct lung-cancer healthcare costs in the study countries are an estimated US$1.35bn, or 20
The Economist Intelligence Unit, “Cancer
0.4% of healthcare outlay, with US$823m spent in Brazil, or 0.5% (based on health spending data from Control, Access and Inequality in Latin
the WHO for 2015). America”
© The Economist Intelligence Unit Limited 2018 13LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
Table 4: Indirect lung-cancer costs in the 12 study countries, 2016
Estimated indirect healthcare Prevalence Estimated per patient indirect
costs for lung cancer (US$) cost for lung cancer (US$)
Argentina 82,413,063 12,626 6,527
Bolivia 913,617 908 1,007
Brazil 116,969,038 33,958 3,444
Chile 16,961,185 3,862 4,391
Colombia 8,059,125 5,205 1,548
Costa Rica 1,791,071 409 4,381
Ecuador 3,104,970 1,104 2,813
Mexico 36,333,140 9,676 3,755
Panama 1,749,907 415 4,220
Paraguay 1,296,821 827 1,569
Peru 7,298,856 2,576 2,833
Uruguay 8,886,882 1,645 5,403
Total 285,777,674 73,210 3,904
Source: The Economist Intelligence Unit
The indirect costs include the impact of absenteeism and early mortality on economic output. Finding
these costs involved looking at, for each economy, GDP per worker per day; lung cancer’s prevalence
overall and in specific age bands; and age-specific workforce-participation rates.
This is not the whole story in Latin America. The informal economy can make up a substantial part of
economic activity. The extent of informal activity is inevitably difficult to measure, but a recent IMF
study used two techniques to estimate the size of national informal economies as a percentage of
GDP. One relied largely on incentives to be informal, including tax levels and the size of the economy
in general, while the other relied on measures of government effectiveness and the existence of
corruption. The results indicate a wide variation in our study countries, with Chile, and by one of
the measures Uruguay, doing as well as countries such as Denmark and Australia. In Bolivia, though,
informal activity accounts for wealth equivalent to around 45% of formal GDP.21
Taking the national figures (and averages for the study country where these were not available)
increases the total indirect cost of lung cancer by 26% or 29%, depending on the method used, to
US$361m or US$369m.
21
Leandro Medina and Friedrich Schneider, The resultant figures—in aggregate about a fifth of direct costs for the formal economy and a little
“Shadow Economies Around the World: What
over a quarter including the informal economy—may seem small: they constitute barely noticeable
Did We Learn Over the Last 20 Years?”, IMF
Working Paper, number WP/18/17, January fractions of total GDP in these countries. Their size reflects the interaction of biology and social policy.
2018. As discussed later in this report, lung cancer’s average age of diagnosis is typically late, at around 70
in the US.22 Retirement ages in Latin America come far earlier: as low as 60 years for men in Uruguay
22
American Cancer Society, Key Statistics for
and Paraguay, and 58 in Bolivia. Accordingly, among the newly diagnosed, retirees outnumber workers.
Lung Cancer, available at: https://www.cancer.
org /cancer/non-small-cell-lung-cancer/ Without wages to lose, the former contribute nothing to aggregate costs and diminish per-case ones
about/key-statistics.html substantially.
14 © The Economist Intelligence Unit Limited 2018LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
This is good news only to economists. To begin with, if nothing else changes, one unintended by-
product of efforts in many study countries to extend retirement ages could be a higher economic cost
for lung cancer.
More pressing at the individual level, public coverage of more than basic lung cancer care is unusual
in the region (see access section below). Accordingly, many patients must pay for treatment out of
retirement incomes and savings.
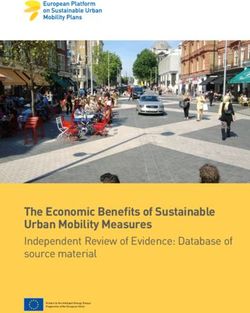
Those still in work also face huge challenges. The most common definition of middle class in Latin
America is a household income of US$10-50 per person per day in purchasing power parity (PPP)
terms,23 and therefore less, to a varying degree by country, in nominal US dollars (in which our
estimates are denominated). The accompanying graph translates the lower boundary of the middle
class into nominal US dollars and multiplies it by the average number of members per household in
each country. It also shows average lost wages per individual, by taking average lost GDP per worker
and multiplying that by the labour share of GDP in each country.
Chart 2
The middle class and the cost of productivity lost to lung cancer, 2016
(US$)
Lower average-sized middle class family income limit Lost income per worker
14,000
12,000
10,000
8,000
6,000
4,000
2,000
0
a
u
il
a
y
ia
ico
r
a
ay
le
ica
do
m
az
in
ua
r
bi
liv
i
Pe
gu
Ch
ex
nt
aR
na
om
Br
ua
g
Bo
ra
ru
ge
M
Pa
Ec
st
l
Pa
Co
U
Ar
Co
Sources: Economist Intelligence Unit calculations; University of Groningen, Penn World Tables (for labour share of GDP data);
World Bank (for PPP to US$ conversion per country).
Although relying on many assumptions, the chart’s message is clear. The average wages lost if a
household member in work were to develop lung cancer would devastate the finances of families that 23
See, for example, Renos Vakis et al, “Left
were not middle class, or at the lower-income end of that category. Even households at the upper end Behind: Chronic Poverty in Latin America and
the Caribbean”, 2015 & Luis F López-Calva
of the middle class would lose, on average in the 12 countries, 20% of annual household income in 2016.
and Eduardo Ortiz-Juarez, “A vulnerability
This, combined with direct costs of treatment in some cases, would send a large proportion of even approach to the definition of the middle class”,
middle-class patients into financial vulnerability. The Journal of Economic Inequality, 2014.
© The Economist Intelligence Unit Limited 2018 15LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
Cost context and an unknown gap
Comparing lung cancer with prostate cancer provides an interesting contrast. More than twice as many
people develop prostate cancer as lung cancer in Brazil, although 64% more die of the latter.24 A recent,
similar Economist Intelligence Unit cost analysis of prostate cancer in four Latin American countries
provides instructive comparator figures: the study found that prostate cancer cost Brazil US$1.2bn in
2015,25 thus slightly higher than lung cancer’s total costs of US$940m in 2016, which indicates that lung
cancer’s higher mortality partially counteracts prostate cancer’s much greater incidence.
The contributors to these costs differ more than their totals. Despite the much lower number of cases,
lung-cancer treatment takes up much more money than prostate cancer: about US$823m, compared
with US$620m. This is consistent with other research, including a 2016 British academic study. This
study compared the total medical costs related to cancer patients during the five years after diagnosis.
After removing underlying non-cancer healthcare outlay (derived from spending that occurred on
appropriate control groups without cancer) lung-cancer expenses were twice as high per patient as
prostate cancer ones.26
Indirect costs for prostate cancer, however, were markedly higher (US$580m to US$117m). Driving this
are: the greater absolute number of prostate cases; lower workforce participation rates of women who,
although a minority of lung-cancer cases, have no prostate gland; and lower average age of onset for
prostate cancer (by four years in the US), so that fewer who develop it will have left the workforce.27
But is this high level of direct spending for lung cancer appropriate, especially given the frequently
debated cost of many cancer treatments? Health-system resource allocation is inevitably a political
decision and any specific intervention should be cost-effective. Nevertheless, in making choices, high-
level comparisons provide a useful perspective.
In our study, the estimated direct costs for lung cancer paid by Brazil’s public health service, SUS,
is US$250m for 2016. This comes to 0.36% of government non-capital health spending (based on
24
IARC Globocan, Database, Incidence/ health spending data from the WHO for 2015). If the SUS were to spend on its three-quarters of the
Mortality > Rates: Cancers by population.
Available at: http://globocan.iarc.fr/Pages/
population at the same rate per patient as the private sector does, the equivalent figures would be
summary_table_pop_sel.aspx US$1.7bn and 2.5%.
25
The Economist Intelligence Unit, “Tackling Lung cancer’s burden depends on the measure. The disease exacted 1.2% of Brazil’s 2016 disability-
the burden of prostate cancer in Latin America: adjusted life years, a metric combining mortality and time spent living with a disease; it was also
The prospects for patient-centred care”, 2017.
responsible for 2.3% of deaths that year.28 This suggests that, while provision on the private sector’s
26
Mauro Laudicella et al, “Cost of care for scale might be inappropriate, current state spending seems markedly low given the scale of lung
cancer patients in England: evidence from cancer’s current burden in Brazil.
population-based patient-level data”, British
Journal of Cancer, 2016.
Calling spending levels further into question, our study figures may even present too generous a
picture. The process for estimating the Brazilian outlay, and therefore that for other study countries,
27
American Cancer Society, Key Statistics for
Lung Cancer. first determines treatment costs per person at specific public and private facilities, and then multiplies
the resultant numbers by national prevalence figures. This implicitly assumes that everyone who
28
IHME, GBD Results Tool.
16 © The Economist Intelligence Unit Limited 2018LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
develops lung cancer gets diagnosed and treated with the degree of aggression used in either public
or private hospitals.
This is unlikely for the region, or even Brazil. Dr Raez points out that, for those diagnosed, especially
by non-expert clinicians unaware of recent treatment advances, “cancer nihilism” all too often skews
treatment decisions. “A lot of times, general practitioners send them straight to palliative care or
hospice. They don’t think the fight is worth it.” An additional consideration, he adds, is that palliative
care is much cheaper than running a battery of genetic tests and prescribing expensive anti-cancer
treatment accordingly.
Nor does everyone with the disease even get this far. In Brazil, as in study countries overall, 20% of
lung-cancer cases come to the attention of registries only through death certificates. Poor health
service-registry communication no doubt contributes but is not the whole problem.29 For other
cancers, where the same fragmentation would also exist, only 9% of registrations depend on death
certificates.30 Gilberto Lopes, director of global oncology at the University of Miami Miller School of
Medicine, who has extensive cancer-treatment experience in Brazil, observes: “A lot of people just
don’t get diagnosed.” For these individuals, direct care costs are nil, although the indirect ones remain.
29
Economist Intelligence Unit calculations
Both missed diagnosis and undertreatment would dampen the actual spending on lung cancer in based on IARC, Cancer in Five Continents,
“Indices of data quality (Volume X): All sites
Brazil, and therefore the other countries, below the model estimates, but it is impossible to say how
except non-melanoma skin (C00-96 exc.
much. Our figures remain the most reasonable ones available if used with suitable reservation. C44)” & “Indices of data quality (Volume X):
Lung (C33-34)”.
III. A closer look at the risks: more than just tobacco 30
Ibid.
Addressing this human and economic burden of lung cancer means understanding what it is and what
drives it. Lung cancer itself is a collection of diseases rather than a monolith. Some are increasingly
31
Otis W Brawley et al, “The First Surgeon
General’s Report on Smoking and Health: The
vulnerable to new treatments, others are not (see Box: what is lung cancer?). Its risks are also 50th Anniversary”, CA: A Cancer Journal for
multifaceted. Clinicians, 2014.
32
Centers for Disease Control and Prevention,
Tobacco’s dominant, but incomplete, responsibility What Are the Risk Factors for Lung Cancer?.
For all the diversity in lung cancer, one constant is the role tobacco plays in causing it. The link with Available at: https://www.cdc.gov/cancer/
lung/basic_info/risk_factors.htm
smoking has been incontrovertible since as far back as the 1950s.31 It requires no elucidation here.
However, while the dominant cause of lung cancer in the region, it is not alone. The oft-repeated 33
Farhad Islami et al, “Global trends of lung
conventional wisdom that tobacco underlies 80% to 90% of incidence applies largely in wealthy cancer mortality and smoking prevalence”,
Translational Lung Cancer Research, 2015.
countries,32 not less developed ones.33 For lung cancer, Latin America often falls into the latter camp:
in Chile, for example, 40% of women with the disease were never-smokers. So too were, according to 34
“En Bolivia, más mujeres sufren cáncer
a recent, albeit small, study in Bolivia, 68% of those diagnosed in the past three years at the National de pulmón”, Página Siete, March 17th 2018
& “Pronóstico ytolerancia al tratamiento en
Lung Institute.34
cáncer de pulmón”, Revista Buena Salud, July
30th 2014.
Self-evidently, tobacco’s contribution to incidence varies depending on the extent of smoking and
other risks. Methodologies for weighing their relative contribution all have flaws,35 but the GBD 35
Nabil Tachfouti et al, “Mortality attributable
estimates that, on aggregate in the study countries, 64% of all lung cancers are caused by tobacco. to tobacco: review of different methods”,
Archives of Public Health, 2014.
© The Economist Intelligence Unit Limited 2018 17LU N G C A N C E R I N L AT I N A M E R I C A
TIME TO STOP LOOKING AWAY
Inevitably, the range is wide, going from just 35% in Ecuador, with its historically low smoking rates, to
82% in Uruguay, once a regional leader in tobacco consumption.36
36
Economist Intelligence Unit calculations Other key lung carcinogens
based on data from IHME, GBD Results Tool, These figures show both tobacco control’s crucial importance for addressing Latin American lung
and IARC Globocan, Database Incidence/
Mortality > Rates: Cancers by population.
cancer, but also the substantial burden arising from other causes. The GBD data are not outliers here.
Dr Lopes reports that figures available from the region indicate that at least a quarter of those with
37
Economist Intelligence Unit calculations lung cancer never smoked. Put another way, were all tobacco-attributed mortality removed, lung
based on data from IHME, GBD Results Tool.
cancer would remain the eighth deadliest form of the disease in the study countries—roughly as deadly
38
For a detailed list, see R William Field
as cancer of the cervix.37 Moreover, while the latter is declining, “we are seeing a rise in the number of
and Brian L Withers, “Occupational and lung cancers among those who have never smoked, though we don’t quite understand why”, according
Environmental Causes of Lung Cancer”, to Dr Lopes.
Clinical Chest Medicine, 2012.
The lack of information on, and awareness of, these other risks in Latin America, however, is worrying.
39
Roberto Pasetto et al, “Occupational Burden
of Asbestos-related Cancer in Argentina,
Various chemicals, through environmental or workplace contact, cause the vast majority of non-
Brazil, Colombia, and Mexico”, Annals of tobacco lung cancers.38 Most individually have limited impact: occupational exposure to asbestos, for
Global Health, 2014.
example, accounts for around 0.5% of incidence in Latin America’s four most populous countries.39
40
WHO, “WHO Handbook on Indoor Radon”, Several specific lung carcinogens are nevertheless noteworthy in the region:
2009.
Radon: globally, after tobacco, the biggest cause of lung cancer is radon-222, an odourless, colourless
41
A Ángeles and G Espinosa, “Study of
epidemiological risk of lung cancer in Mexico gas. It is a product of radioactive decay by solid radon, itself usually a result of decaying uranium. Both
due indoor radon exposure”, AIP Conference metals occur naturally worldwide. A WHO review found that radon induces 3-14% of lung cancer,
Proceedings, 2014.
depending on the country. However, while the gas increases the risk of developing lung cancer for
everyone exposed, it most often works in synergy with tobacco smoke, so that elimination of either
42
National Academy of Sciences, “Health
Effects of Exposure to Radon: BEIR VI”, 1999. would prevent a majority of radon-related lung cancer.40
43
Jan M Zielinski, “Mapping of Residential Latin America’s risk level is unclear. Presence of the gas varies as widely with geography as do its
Radon in the World”, presentation, 2014 & A precursor metals. It certainly exists at unhealthy concentrations in parts of the region. Mexican data
Canoba et al, “Indoor radon measurements
estimate that the lung-cancer effect of radon is roughly the same as in the US,41 where it contributes
in six Latin American countries”, Geofísica
Internacional, 2002. 10-14% of all lung cancers and is the main cause of 3-4%.42
44
Based on data from Nuclear Energy Agency Initial surveys over a decade ago, drawing on very limited evidence and covering only seven study
and International Atomic Energy Agency, countries, suggested that Mexico had the highest household concentrations of radon in the region.43
“Uranium 2016: Resources, Production and
Demand”. Available at: http://www.oecd-nea.
With further research, this view will probably change. Brazil, for example, possesses some of the world’s
org/ndd/pubs/2016/7301-uranium-2016.pdf & largest uranium reserves, and Peru has roughly 80% as much per km2,44 so the preconditions for radon
worldatlas, https://www.worldatlas.com/
certainly exist. A 2015 survey in Lima, where a third of Peruvians live, found that, in 88% of districts
measured, average mean concentrations exceeded WHO recommendations.45 In Brazil, although the
45
P Pereyra et al, “Concentration
Measurements of Radon 222 Indoors in Lima– national picture remains unclear, studies have found worryingly high household radon concentrations
Peru”, International Journal of Physics, 2015. in parts of Bahia, Rio Grande do Norte, Minas Gerais, São Paulo and Rio de Janeiro. An extreme case
shows the danger: Caetite, a major Brazilian uranium mining centre, has radon concentrations ten
46
“Radônio, uma ameaça”, #carta, September
21st 2015. times the WHO recommended maximum and lung cancer rates 19 times the national average.46
18 © The Economist Intelligence Unit Limited 2018You can also read