Life is a sexually transmitted disease with an inevitably fatal outcome'
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
VOLUME 1 • NUMBER 4 • december 2009
OF PRIMARY HEALTH CARE
‘Life is a sexually Original Scientific Paper
Gender differences in general practice
utilisation
transmitted disease See page 261
Original Scientific Paper
with an inevitably Reducing gender inequality in life
expectancy
See page 270
fatal outcome’ Original Scientific Paper
Meeting the needs of men in general
See Back to Back, page 319 practice
See page 302
Original Scientific Paper
Immunisation subsidies do not cover
practice costs
See page 286
Back to Back
For and against PSA testing for
prostate cancer screening
See page 319
Ethics
Exchanging values and seeing other
world views
See page 332contents
VOLUME 1 • NUMBER 4 • December 2009
issn 1172-6164 (Print)
OF PRIMARY HEALTH CARE ISSN 1172-6156 (Online)
256 Editorials 319 Back to Back
From the Editor 319 New Zealand should introduce population screening for
256 Improving men’s health benefits us all prostate cancer using PSA testing
Felicity Goodyear-Smith Yes Robin Smart; No David Tulloch
Guest Editorial
323 Continuing Professional Development
258 Developing men’s awareness of health issues
Lannes Johnson
323 Charms & Harms: Saw palmetto
261 Original Scientific Papers Joanne Barnes
Quantitative Research 324 String of PEARLS about low back pain
261 Gender differences in general practice utilisation in 324 Cochrane Corner: NSAIDS are effective in the common cold
New Zealand for pain and sneezing but not other symptoms
Santosh Jatrana, Peter Crampton Bruce Arroll
270 Getting back the missing men of Aotearoa: declining gender 325 Pounamu: Strategies to address disparities in access to care
inequality in NZ life expectancy must be multidimensional
Peter Sandiford Peter Jansen
278 Human papillomavirus and papillomavirus vaccines:
326 Essays
knowledge, attitudes and intentions of general practitioners
and practice nurses in Christchurch
326 Who shall decide: telling the truth and avoiding the
Judith Henninger law—patient consent in the millennium
286 The cost of immunising at the general practice level Bryan Frost
Nikki Turner, Paul Rouse, Stacey Airey, Helen Petousis-Harris 328 Cardiovascular disease risk profile tools and New Zealand
297 Variation in Partnership Health general practice enrolment —the best way forward?
data related to need and hospital and national records on Pauline Boland, Helen Moriarty
ethnicity
Laurence Malcolm, Ross Barnett 332 Ethics
Qualitative Research 332 Values transparency and inter-professional communication
302 New Zealand men’s health care: are we meeting the needs of David Seedhouse
men in general practice?
Eileen McKinlay, Marjan Kljakovic, Lynn McBain 335 Letters to the Editor
311 Improving Performance 339 Book Review
311 Do invitations to attend Well Man Checks result in
increased male health screening in primary health care? 339 Healthy Bastards—Dave Baldwin
Pete Barwell Reviewer: Lannes Johnson
315 More allopurinol is needed to get gout patientsEDITORIALs
from the editor
Improving men’s health
benefits us all
T
Felicity Goodyear- his is the final issue of the first volume of and colleagues explore the possible barriers inhib-
Smith MBChB, MGP, the Journal of Primary Health Care (JPHC). iting men from using general practice.8 Sandiford
FRNZCGP, Editor Having started the journal with an empty demonstrates that the disparity in life expectancy
kete,* we now have an abundance of original New between men and women has been reducing,
Zealand research to feast on, and will soon need a and discusses how this trend may be continued.9
rua kumara† to store the remainder of this year’s Barwell describes his own practice’s initiative of
harvest. The response to the journal has been proactive invitations for well men checks.10
overwhelming and we are truly grateful to the
large number of researchers from wide-ranging The men’s health theme is continued by urolo-
disciplines who are choosing to submit their work gists Smart and Tulloch going Back to Back
to the JPHC. on prostate specific antigen (PSA) population
screening for prostate cancer.4 Charms and Harms
One of the most pleasing aspects of the journal is deals with saw palmetto, commonly employed for
the academic debate it is engendering. This is not treatment of benign prostatic hyperplasia (read to
only the Back to Back columns in each issue.1-4 find out whether the evidence supports its use).
Letters to the Editor this month continue Gilmer Baldwin’s book Healthy Bastards, an accessible
and Gorman’s discussion about the roles of nurse guide for the everyday Kiwi bloke, is reviewed
practitioners and general practitioners (GPs),3 the and a guest editorial explains why encouraging
evidence-base for acupuncture is fiercely contested, men’s awareness of, and attention to, health is-
and Hong‡ et al’s paper on prescribing of aspirin and sues is vital for our society as a whole.
statins in rest-homes5 has fuelled further discussion
on giving cardio-protective drugs to the elderly. Men’s health is by no means the only item on the
agenda for this issue. Turner and colleagues have
This issue has a men’s health focus. The health of developed a model for viewing all components of
our men contributes greatly to the health of our the cost of providing childhood immunisations.
nation. Overall men have a poorer health status They have shown that the current government
than women and use our health services less fre- subsidy does not provide adequate reimburse-
quently. They die earlier than women and more ment, with each immunisation being delivered at
of their deaths are avoidable.6 a net cost to the practice.11 A Christchurch study
looks at GP and practice nurse knowledge and
CORRESPONDENCE TO: A number of research papers address these issues. attitudes about the human papillomavirus (HPV)
Felicity Goodyear-Smith Jatrana and Crampton examine the relative under- and HPV vaccines.12 On a completely different
Associate Professor, utilisation of general practice services by men, tack, another Christchurch paper explores linking
Department of General
Practice and Primary
which cannot be accounted for by gynaecological the National Heath Index (NHI) to general prac-
Health Care, Faculty and obstetrical conditions nor women’s excess in tice and other data sources to reliably contribute
of Medical and Health visits in the child-bearing years,7 while McKinlay to a district database.13
Sciences, The University
of Auckland, PB 92019,
Auckland, New Zealand * Maori flax basket
f.goodyear-smith@ † Sweet potato storage pit
auckland.ac.nz ‡ See Errata
256 VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CAREEDITORIALs
from the editor
An improving performance paper shows another
way of using available electronic data. Clinical Errata
data from practice management systems can allow
The name of the first author of the paper Use of aspirin and statins for cardio-
benchmarking of usual care by practices, and pro-
vascular risk reduction in New Zealand: the residential care story. J Primary
vide a standard against which to measure quality
Health Care. 2009;1(3)184-189 is Jae Hong not Hoem. Corresponding author
cycle improvements. In this case, a benchmark for
Prof. Ngaire Kerse sincerely apologises for this error.
gout control was determined using the proportion
of patients with well-controlled serum uric acid
The String of PEARLS are based on the PEARLS developed by Prof. Brian
and then this was used to trial a mail and phone
McAvoy. Our apologies for not acknowledging his contribution in the
intervention to improve gout control.14
September issue.
These are just some of this issue’s offerings.
Given the depth and breadth of papers spanning 6. Johnson L, Huggard P, Goodyear-Smith F. Men’s health and
diverse aspects of primary health care which are the health of the nation. NZ Med J. 2008;121(1287):69–76.
now awaiting publication in the JPHC, readers 7. Jatrana S, Crampton P. Gender differences in general
practice utilisation in New Zealand. J Primary Health Care.
can anticipate a wide array of articles. Volume 2 2009;1(4):261–269.
therefore is unlikely to be themed; rather an 8. McKinlay E, Kljakovic M, McBain L. New Zealand men’s health
exciting assortment of contributions are in store care: are we meeting the needs of men in general practice? J
Primary Health Care. 2009;1(4):302–310.
for our 2010 readers. 9. Sandiford P. Getting back the missing men of Aotearoa:
Declining gender inequality in NZ life expectancy. J Primary
References Health Care. 2009;1(4):270–277.
10. Barwell P. Do invitations to attend well men checks result
1. Arroll B, Kerse N. Back to Back: GPs should prescribe more in increased male health screening in primary health care? J
benzodiazepines for the elderly. J Primary Health Care. Primary Health Care. 2009;1(4):311–314.
2009;1(1):57–60. 11. Turner N, Rouse P, Airey S, Petousis-Harris H. The cost of im-
2. Elley R, Toop L. A polypill is the solution to the pharmacologi- munising at the general practice level. J Primary Health Care.
cal management of cardiovascular risk. J Primary Health Care. 2009;1(4):286–296.
2009;1(3):232–236. 12. Henninger J. Knowledge, attitudes, and intentions of general
3. Gilmer M, Smith M, Gorman D. Back to Back: The nurse practi- practitioners and practice nurses in Christchurch about HPV
tioner provides a substantive opportunity for task substitution and HPV Vaccines. J Primary Health Care. 2009;1(4):278–285.
in primary care. J Primary Health Care. 2009;1(2):140–143. 13. Malcolm L, Barnett R. Variation in Partnership Health
4. Smart R, Tulloch D. Back to Back: New Zealand should general practice enrolment data related to need and hospital
introduce population screening for prostate cancer using PSA and national records on ethnicity. J Primary Health Care.
testing. J Primary Health Care. 2009;1(4):319–322. 2009;1(4):297–301.
5. Hong J, Kerse N, Scahill S, Moyes S, Chen C, Peri K, et al. Use 14. Arroll B, Bennett M, Dalbeth N, Hettiarachchi D, Cribben B,
of aspirin and statins for cardiovascular risk reduction in New Shelling G. More allopurinol is needed to get gout patients
Zealand: the residential care story. J Primary Health Care.EDITORIALs
guest editorial
Developing men’s awareness
of health issues
I
Lannes Johnson s there a need for New Zealand (NZ) to The review confirmed that health outcomes were
MBChB, FRNZCGP, develop, or encourage, men’s awareness of poorer for New Zealand men than women, in
MMedSci (Hons) health issues? Awareness by men themselves, terms of morbidity, mortality and life expectancy.
their children, their partners, or all of the above? The literature identified several factors proven
Would there be benefits in respect of health gain or suspected to cause the disparities in health
including quality of life, with a resulting reduc- outcomes between men and women. There was,
tion in secondary care health expenditure, or in however, little agreement on which of these fac-
the country’s productivity, with a consequent tors impacted most on men’s health, and how to
improvement in NZ’s gross domestic product? address these factors. The findings from the review
suggested more in-depth research was needed to
There is no dispute regarding the gender mortal- provide a foundation for effective strategies to
ity and morbidity differences between men and improve men’s health.2
women in NZ; what is uncertain is the aetiol-
ogy of the disparity and thus how to alleviate In 2006 HealthWEST Primary Health Organisa-
it. Men’s shorter lives have not been shown to tion (PHO) was commissioned by the then Min-
be due to biological differences and behavioural ister of Health (Pete Hodgson) to research men’s
differences may account for some disparities (e.g. health in NZ and investigate actions that could
accidents, suicides, cancer and deaths from cardio improve men’s health. The authors looked at the
vascular disease), but certainly in NZ we do economic ramifications of poor health in the
spend a lot more on women’s health. The role of workforce, examined men’s attitudes to health
this differential allocation of health budget has and made recommendations to the Minister:
not been fully investigated. Professor White, one
of the first chairs in men’s health in the United Health is not simply a by-product of economic
Kingdom (UK) commented: development, but is a substantial driver of economic
development as well. The health of the population
Men’s health is not a medical issue; it is societal. affects a country’s productivity, labour supply,
Therefore a much broader approach needs to be education levels, and capital formation. Healthy
taken. This leads us into research questions around people learn better, live longer—and work, earn,
men’s lifestyles and the social pressures on men and save more.3
to conduct their lives in certain ways; it makes us
look at social structures, including education, work, Limited awareness of health issues may lead to
leisure.1 poor health and one of the fundamentals for
CORRESPONDENCE TO: improving health in a population is improv-
Lannes Johnson
Clinical Director, In December 2004 the Public Health Advisory ing health literacy; the development by Janine
Harbour Health, Committee (PHAC) commissioned a literature Bycroft of Health Navigator is one tool to ad-
PO Box 9, Greenhithe review on men’s health. The review, which was dress this (http://www.healthnavigator.org.nz/).
Auckland 0756, The success of the cervical smear and breast
both comprehensive and excellent, was carried out
New Zealand
ljohnson@ by Eileen McKinlay of the Wellington School of screening campaigns relied on women’s aware-
harbourhealth.org.nz Medicine and Health Sciences, Otago University: ness of the associated health issues. There has
258 VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CAREEDITORIALs
guest editorial
been little in the way of corresponding national chair in men’s health (despite the altruistic,
awareness campaigns for men in NZ and, inter- academic and economic justification for this)
nationally, awareness efforts have been poorly and actions to improve men’s health have been
evaluated: largely left to employers who recognise the value
of good health in the workforce, a few passion-
Only a paucity of interventions have been com- ate individuals and concerned non-government
prehensively monitored and evaluated, and which organisations.
in turn have shown clear beneficial impact on
men’s health. However there is potential for men’s Men in NZ visit a GP less often than women but,
health awareness activities to catalyse interest in more importantly, they engage less in comprehen-
health and to seek advice or support. Three possible sive health checks2 and, except for cardiovascular
benefits of men’s health activities are: raised aware- disease/diabetes screening, there is limited sup-
ness of health issues, connecting men with health port for the practice team to manage this. ‘There
or other support networks, and some degree of are barriers to overcome if the practice team is
behaviour change.3 to undertake health promotions within general
practice consultations.’4
The need to promote health awareness in men
has been recognised by many national groups, It is possible that systematic population
notably the Cancer Society, the Prostate Can- screening and raising health awareness, with
Men’s shorter lives have not been shown to be due to biological
differences and behavioural differences may account for some
disparities (e.g. accidents, suicides, cancer and deaths from
cardiovascular disease), but certainly in NZ we do spend a lot
more on women’s health
cer Foundation, Aged Concern, a number of specific focus on ethnicity and socioeconomic
men’s action groups, and a (very) few District issues, may address some of the gender dispari-
Health Boards and PHOs. An excellent publica- ties and reduce health and societal costs in the
tion by rural general practitioner, Dave Baldwin community:
(Healthy Bastards) provides comprehensive men’s
health advice (and includes a chapter on women’s Men have a lower life expectancy than women,
health for male edification). There has been the and there are enormous costs associated with
occasional programme on TV and a (very) few premature death and disability that impact
press releases that relate to men’s health. There families, employers, and society as a whole. Men
is no organised ‘Men’s Health Movement’ despite play a critical role in families as fathers and
international examples and academic recogni- sons providing care and support to other family
tion of men’s health as an indexed term (MeSH members. As members of the workforce, they
or Medical Subject Headings) in MEDLINE/ are employers and employees whose health and
Pubmed in 2008. well-being greatly affect productivity and eco-
nomic well-being. Improving the health of men
However, unlike Australia, the United States through early detection of male health problems
and UK, NZ has no declared government policy and timely treatment of disease can result in
on men’s health; no national men’s awareness reduced morbidity and mortality resulting in
day, no Ministry of Men’s Affairs, no academic benefits for men, families, and society.5
VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CARE 259EDITORIALs
guest editorial
The Ministry of Health’s website, under ‘men’s have a particular perception of health which may
health’, reveals an encouraging commitment mean that they do not always recognise when to
(http://www.moh.govt.nz/menshealth): seek help and may find it difficult to engage with
the health services.6
The Ministry of Health is working on programmes
and initiatives aimed at encouraging men to be Goodyear-Smith and Birks have commented
more aware of their health and to access healthcare. on the disadvantages of a gendered approach
These include: to health and advocates a more targeted health
• providing targeted men’s health checks at policy:
convenient times and locations
• supporting workplace based men’s health New Zealand governmental agencies promote a
initiatives gendered approach to health care policy and serv-
• establishing a men’s health innovation fund ice delivery on the basis that women have special
to support community based men’s health health needs not met by the existing health
initiatives services. We argue against such an initiative on
• developing a men’s health social marketing the basis that giving priority for female services
campaign disadvantages males, who already have higher
• improving access to good quality men’s health morbidity and mortality than women. A needs
information by supporting existing websites, rather than advocacy-driven public health policy
telephone health services and a range of infor- directed at high-risk groups for specific health
mation pamphlets problems rather than specific populations may be
a more efficient, equitable and effective means of
These programmes seem to be in abeyance at the disease prevention and treatment.7
present time, although there is a small research
project looking at the ‘burden of risk’ (cardio- PHOs definitely have a role in addressing these
vascular, major cancers, self-harm, depression) difficulties, but a national policy on men’s health
in working men in Waitakere who have not could set the pace. Without political leadership
experienced a comprehensive health check in the from the Ministry of Health and possibly the
previous five years. financial sector, progress will be slow. Improving
men’s health is critical to improving productivity
Although addressing inequalities in health in NZ and thus economic recovery.
is a key focus of health strategy and policy, men’s
References
health does not specifically feature in this regard.
Rather, the focus is more on addressing inequalities 1. White AK. Men’s health in the 21st century. Int J Men’s
Health. 2006;5(1):1–17.
patterned by ethnicity and deprivation, and issues 2. McKinlay E. Men and health: a literature review. Wellington:
of men’s health within these groups appears at best Wellington School of Medicine; January 2005.
in the margins.6 3. Johnson LF FA, Stephenson P. A review of the benefits of
men’s health awareness activities and a proposal for the devel-
opment of a targeted men’s health programme. In: Healthwest
The McKinlay review highlighted many initia- PHO; 2006. p. 1–57.
tives to improve men’s health; however the issue 4. McKinlay E, Plumridge L, McBain L, McLeod D, Pullon S,
Brown S. What sort of health promotion are you talking
may be less of awareness and more of availabil- about?: A discourse analysis of the talk of general practition-
ity; in primary care many practices are not ‘man ers. Soc Sci Med. 2005;60:1099–1106.
friendly’. Hours of opening do not accommodate 5. Rich J, Ro M. A poor man’s plight: Uncovering the disparities in
men’s health. A series of Community Voices Publications. Feb
men’s difficulties in time away from work, prac- 2005, Kellogg Foundation. p 38.
tice nurses are busy with women and children, 6. Johnson L HP, Goodyear-Smith F. Men’s health and the health
and the concept, and promotion, of a comprehen- of the nation. NZ Med J. 2008;121(1287).
7. Goodyear-Smith F, Birks S. Gendered approaches to health
sive men’s health check (tailored to age) may not policy: how does this impact on men’s health? NZ Fam Phys.
be well supported in all practices. Men appear to 2003;30(1):23–29.
260 VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CAREORIGINAL SCIENTIFIC PAPERS
quantitative research
Gender differences in general
practice utilisation in New Zealand
Santosh Jatrana PhD, MPhil, MA, BA (Hons), PGD (Public Health); Peter Crampton MBChB, PhD, FAFPHM,
MRNZCGP
ABSTRACT
Introduction: This paper aims to examine gender differences in general practice utilisation in New
Zealand.
Methods: The data for this research came from 10 506 visit records gathered from 246 general practition-
ers (GPs) who took part in the National Primary Medical Care Survey (NatMedCa), a nationally representa-
tive, multistage, probability sample survey of GPs and patient visits conducted in 2001/2002. The number
of visits to a general practice in the last 12 months among those patients who visited the GP at least once
during the past 12 months was used as the outcome variable. Poisson regression was used for analysis.
Results: Women were more likely than men to visit a GP over the last 12 months (IRR=1.13; 95% CI:
1.03–1.24). We also found significant female excess in utilisation of GP services even after excluding
gynaecological and obstetric conditions and across all age groups. Asian were 39% less likely than Euro-
pean women to visit a GP (IRR=0.61; 95% CI: 0.43–0.85); a result that was not reflected in men’s utilisa-
tion of GP services. In addition, we found that women visiting GPs were 39% more likely to have reported
‘life-threatening’ problems as compared to ‘self-limiting’ problems (IRR=1.39; 95% CI: 1.00–1.94).
Conclusion: Our results do not support the body of literature that suggests that women’s excess
in service use can largely be attributed to gynaecological and obstetrical conditions or that the female
excess in visits is focussed in the childbearing years. Ethnicity and the severity of a problem contributed
significantly to explaining women’s, but not men’s, utilisation of GPs.
Keywords: Gender differences; health services utilisation; New Zealand
Introduction
While gender differences in health, assessed not important in explaining the sex difference in
in terms of mortality and morbidity, have been consultation rates.22 Still others indicate that dif-
reported in most developed countries over recent ferences are due to different experience of symp-
decades, less attention has been paid to the use toms rather than willingness to consult.14,23–27
J PRIMARY HEALTH CARE
of health care services. Research from developed Further studies suggest that males and females 2009;1(4):261–269.
countries on patterns of health service use sug- do not differ in symptom reports for specific dis-
gests that women’s rate of utilisation of almost eases where symptoms tend to be powerful and
all health services is higher than that of men.1–17 obvious.24 Some scholars found no support for the CORRESPONDENCE TO:
However, some researchers have challenged the notion that women are more likely than men to Santosh Jatrana
stereotype of women being more likely to use seek help for any particular problem.4 Research Fellow,
Department of Public
health services.18–20 For example, some scholars
Health, School of Medicine
have suggested that the largest female excess Clearly, these explanations are not mutually and Health Sciences,
in attendance is during childbearing years;21 exclusive. They do, however, serve to illustrate University of Otago,
others argue that gynaecological and obstetrical the complexity of the association between gender Wellington
PO Box 7343, Wellington,
conditions contribute significantly to the differ- and health services utilisation and warrant on-
New Zealand
ence, whereas consultation for ‘vague’ or mild going examination of the topic. The present study santosh.jatrana@
symptoms, or ‘symptoms without disease’ are examines gender differences in general practice otago.ac.nz
VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CARE 261ORIGINAL SCIENTIFIC PAPERS
quantitative research
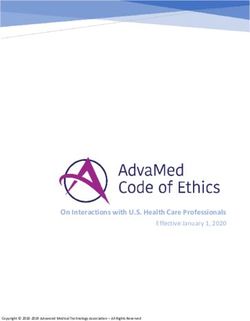
Table 1. Characteristics of patients and visits
utilisation in New Zealand (NZ) by addressing
Characteristics N Percentage
three specific questions:
Predisposing characteristics
• To what extent is there variation in general
Age group (years)
practice utilisation between men and women?
0–15 2032/10506 19.3
• To what should these differences, if there
16–24 919/0506 8.8
are indeed differences, be attributed?
25–34 1670/10506 15.9
• Are there gender differences in the de-
35–44 2593/10506 24.7
45–54 1083/10506 10.3
terminants of GP utilisation?
55–64 2064/10506 19.6
65+ 145/10506 1.4 Thus, we aim to contribute to the debate on the
Gender nature of differences in GP visits between men and
Males 4341/10430 41.6 women. Examining gender differentials in general
Females 6089/10430 58.4 practice utilisation in a NZ context is important
Missing 76 at least for two reasons. First, as suggested in a
Ethnicity of patients number of recent NZ papers, gender has received
NZ European 6794/10319 65.8 less attention in a range of areas, including re-
Maori 1730/10319 16.8 search.28–30 Research on the reduction of social in-
Pacific 721/10319 7.0 equalities in health and in access to health care has
Asian 499/10319 4.8 focussed on socioeconomic and ethnic inequalities,
Other 574/10319 5.6 and gender differentials in health service utilisa-
Missing 187 tion have received less attention in NZ. Second,
Marital status the bulk of research on gender differentials in
Married 4001/7783 51.4 health service utilisation has been carried out on
Unmarried/Never married 3782/7783 48.6 European and American data and evidence from
Missing 2723
NZ may validate existing knowledge and provide
NZDep 2001 quintile*
greater understanding of how the association
1 1575/8940 17.6
between gender and health service utilisation is
2 1552/8940 17.4
manifest across diverse social environments.
3 1628/8940 18.2
4 1791/8940 20.0
The conceptual framework of this study draws on
5 2394/8940 26.8
Missing 1566
the health behaviour model (HBM).31 The HBM
Enabling resources considers the use of health services as a function
Community Service Card (CSC)†,‡ 4992/10197 49.0 of predisposing, enabling and need factors. The
High Use Health Card (HUHC)†,‡ 519/9647 5.4 predisposing component involves characteristics
Need component–practitioner perception existing prior to the onset of disease, which reflect
Urgency of the visit a person’s propensity to contact a doctor given cer-
ASAP & today 3955/8476 46.7 tain health problems. The enabling component re-
This week 4521/8476 53.3 fers to conditions that facilitate or inhibit the use
Missing 2030 of health care facilities, such as health insurance,
Severity of the problem availability and affordability of health services,
Life-threatening 210/7893 2.7 family and work obligations. The need component
Intermediate 4153/7893 52.6 reflects the urge to seek health care because of the
Self-limiting 3530/7893 44.7 individual’s objective or subjective health.
Missing 2613
N of cases 10506 100.0 Methods
Source: National Primary Medical Care Survey, 2000
Data
* NZDep 2001 is a census-based small-area index of deprivation, where 1=the least deprived 20% of
areas, and 5=the most deprived 20% of areas.
The data for this research are based on 10 506
† The CSC and HUHC are benefit cards that entitle the user to higher levels of government payment
for consultations and prescriptions, thus reducing the amount of patient co-payment; the CSC is
visit records gathered from 246 GPs who took
means-tested and indicates low income. part in the National Primary Medical Care
‡ These variables were coded as ‘yes/no’. The ‘no’ rows are not shown. Survey (NatMedCa).32 NatMedCa, carried out
262 VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CAREORIGINAL SCIENTIFIC PAPErS
quantitative research
over 2001/2002, was a nationally representative,
multistage, probability sample of GPs and patient WHAT GAP THIS FILLS
visits. The primary purpose of the survey was to
What we already know: Previous studies have reported that women’s
collect data on the content of patient visits. For
rate of utilisation of almost all health services is higher than that of men. One
two periods, each of one week, every selected GP
of the explanations for this difference has been that gynaecological and
completed a questionnaire for a 25% systematic
obstetrical conditions contributed significantly to this difference and that the
sample of patient visits. The questionnaire was
largest female excess in attendance is during childbearing years.
adapted from the annual US National Ambulatory
Medical Care Survey (NAMCS) http://www.cdc. What this study adds: Women are more likely than men to utilise GP
gov/nchs/about/major/ahcd/ahcd1.hrm; accessed services across all age groups and even after excluding gynaecological and
25 June 2006). The overall GP response rate was obstetrical conditions. Determinants of GP consultation differed between the
71.1%, calculated as the proportion of eligible GPs sexes. Ethnicity and severity of problem contributed significantly to explain-
in the sample who completed patient visit survey ing women’s, but not men’s, utilisation of GPs.
forms for both one-week survey periods.
in New Zealand: Maori, if any of the responses
In order to obtain a nationally representative to self-identified ethnicity were Maori; Pacific, if
sample, geographic locations were sampled and any one response was Pacific but not Maori; Asian,
GPs were sampled from locations, stratified by if any one response was Asian but not Maori or
organisation type (independent; independent Pacific; and the remainder non-Maori non-Pacific
practitioner association; capitated; community- non-Asian (nMnPnA) (mostly New Zealanders
governed not-for-profit) and rural/urban (metropo- of European descent, but strictly speaking not an
lis and cities; towns and rural areas). GP and visit ethnic group). The NZDep 2001 index of socioeco-
weights were calculated to take account of differ- nomic deprivation was used as a measure of socio-
ent sampling probabilities, so that approximately economic position. It is a census-based small-area
unbiased estimates of proportions, means and index of deprivation.34 The index scale used here
measures of association could be calculated.33 is from 1 to 5, where 1 is the least deprived 20% of
areas and 5 is the most deprived 20% of areas. The
CSC (community services card) and HUHC (high
Measurement
use health card) are benefit cards that entitle the
The independent variable for this analysis is gen- user to higher levels of government payment thus
der, categorised as men and women. ‘Men’ is the reducing the amount of patient co-payment; the
reference group. The outcome variable is the self- CSC is means tested and indicates low-income.
reported number of visits to a general practice in
the last 12 months among those patients who vis-
Statistical analysis
ited a GP at least once during the past 12 months.
The utilisation of GP services was hypothesised to Since the main dependent variable—the number
depend on predisposing, enabling and need factors. of visits to the GP in the last 12 months—is a
The specific aim was to explore the extent to which count variable which can only take non-negative
observed gender differences, if there are any, are integer values, a count regression was appropri-
explained by the predictor variables (predisposing, ate.35,36 Hence, Poisson regression analyses were
enabling and need factors) considered separately used to examine the gender differences in visits
and together. Predisposing, enabling and need to a GP and also to examine the contribution of
factors selected as independent variables were predisposing and enabling factors to individuals’
respectively (a) age, ethnicity, marital status and visits to a GP. Children below age 16 years were
NZDep 2001 quintile; (b) community service card excluded from the sample for regression analyses
(CSC) status, high use health card (HUHC) status; on the assumption that up to perhaps the mid
and (c) urgency and severity of visit (Table 1). We teens, the person making the decision to visit
have used ‘prioritised’ ethnicity in this paper. the doctor is unlikely to be the patient. Usually
In the ‘prioritised’ concept, each respondent was it will be a parent, and most likely the mother.
assigned to a mutually exclusive ethnic group by In these analyses, the regression coefficient b
means of a prioritisation system commonly used is more easily interpreted as an incidence rate
VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CARE 263ORIGINAL SCIENTIFIC PAPERS
quantitative research
Ethical approval
ratio, eb, which measures the expected change in
the dependent variable as a result of a one-unit NatMedCa (National Primary Medical Care
change in the predictor variable. The incidence Survey) on which the present study is based, was
rates for the dependent variable in each of the approved by the New Zealand Ethics Committee
predictor variable categories are compared to the which reviews national and multi-regional studies.
incidence rate for the reference category. The
incidence rate for the reference category of each Results
predictor is unity. Statistical analyses were under-
Bivariate relationships between gender and GP
taken using the SUDAAN statistical package,37
utilisation are reported in Table 2, 3 and 4. There
allowing estimates to take account of clustering,
was a significant difference between men and
stratification and weights.38 Age standardisation
women in the average number of visits to the
was carried out using the direct method, with the
practice in the previous 12 months (5.4 and 6.3,
2001 census population as the standard.
respectively; p=0.00). There was also a difference
between men and women in the average number
To determine whether gender differences in the
(age standardised) of problems diagnosed (ICD-9-
utilisation of GP services could be eliminated by
CM) per visit (1.5 and 1.7 problems, respectively;
controlling for the predictor variables, both uni-
p=0.006). However, there was no significant
variate and multivariate models were fitted. The
gender difference between men and women in
statistical analysis was performed stepwise. First,
the average duration of visit (14.78 and 15.09
a univariate Poisson regression model (Model 1,
minutes, respectively). A higher proportion of
Table 5) was fitted to examine the gross effect of
male patients visited for administrative (8.33% vs
gender on GP attendance. Second, four multivari-
5.98%; p=0.01), medical (57.8% vs 53.8%; p=0.03)
ate models, based on theoretical considerations,
and surgical (44.8% vs 39.6%; p=0.01) reasons
were estimated. Models 2, 3 and 4 (Table 5)
(Table 3). Except for musculoskeletal, genitouri-
estimated the gender differences in GP attend-
nary, and rheumatologic reasons, there were no
ance after separately controlling for predisposing,
significant gender differences in the reported
enabling and need factors respectively. Finally,
diagnosis for the visits (Table 4). Men were more
Model 5 (Table 5) achieved the same objective af-
likely to visit for musculoskeletal, and rheumato-
ter controlling for predisposing, enabling and need
logic diagnosis while women were more likely to
factors simultaneously. Following Verbrugge’s
visit for genitourinary reasons.
argument (1985) that utilisation due to sex-specific
morbidities and preventive care (e.g. reproductive- Results from the univariate Poisson regression
related contacts) should be removed in analyses analysis (Model 1, Table 5) show that women
assessing the effects of gender, we excluded female were 14% more likely than men to visit a GP over
reproductive diagnoses from the total sample and a 12-month period. Controlling for predisposing
again ran regression analyses of utilisation of GP factors increased the gender difference in the use
services (results not shown). We also conducted of GP services and women were 23% more likely
separate Poisson regression models for men and to use GP services (Model 2, Table 5) than men.
women in order to examine whether the determi- Controlling for enabling (Model 3, Table 5) and
nants of utilisation of GP services were different need (Model 4, Table 5) factors brought down
according to the gender of the patient (Table 6). A gender differences in the use of GP services
variable was considered significantly associated below the unadjusted gross model (Model 1),
with GP attendance when its p-value was below or however differences still remained highly signifi-
equal to 0.05. The c2 test was used to compare male cant. For example, after controlling for enabling
and female categorical variables, with p-values and need factors, as in Model 3 and 4 respec-
computed from the Wald c2 using denominator de- tively, women were respectively 9% and 12% more
grees of freedom equal to the number of sampling likely than men to use GP services. Controlling
units minus the number of strata. For continuous simultaneously for predisposing, enabling and
variables, t-tests and associated p-values were used. need factors (Model 5), the probability of visiting
We also examined possible interactions between a GP over the last 12 months was 13% higher for
gender and predictor variables. women as compared to men.
264 VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CAREORIGINAL SCIENTIFIC PAPErS
quantitative research
The results also show that being older, being of Table 2. Gender differences in average visit duration and number of visits in previous 12
European ethnicity, holding a CSC or HUHC, months (age-standardised)
having a ‘life-threatening’ problem, urgency of Males Females P-value*
visit ‘the same day’ were all significantly related (n=3664) (n=5192)
with increased utilisation of GP services. As op- Average visit duration (minutes)
Total 14.8 15.1 0.29
posed to previous studies marital status was not a
NZDep 2001 = 1 16.2 15.5 0.29
predictor of gender differences in the utilisation NZDep 2001 = 5 13.9 14.4 0.33
of GP services in this study (Table 5); neither Average number of visits to
did it work differently for men and women practice in previous 12 months
(Table 6).39,40 We repeated all the models after Total 5.4 6.3 0.00
NZDep 2001 = 1 4.4 6.1 0.00
excluding gynaecological and obstetrical diag-
noses from the total sample. Our results did not Source: National Primary Medical Care Survey, 2000
change (results not shown). Gender still remained * NZDep2001 is a census-based small-area index of deprivation, where 1=the least deprived 20% of
areas, and 5=the most deprived 20% of areas.
an independent predictor in all the models.
In order to identify gender differences in the Table 3. Proportions of all diagnoses categorised into major groupings (age-standardised)*
determinants of utilisation of GP services, Poisson Diagnosis Male (N) Female (N) P-value
regression analyses were carried out separately for (n=3553) (n=5063)
men and women (Table 6). The results show be- Administrative† 8.3 6.0 .01
ing older and holding a CHC or HUHC were all Medical 57.8 53.8 .03
significantly related with the increased utilisation Surgical 44.8 39.6 .01
of GP services for both men and women. There was Source: National Primary Medical Care Survey, 2000
no significant difference in the utilisation of GP * Analysis limited to those visit records with disease data coded; totals sum to greater than 100%
services between those living in the most deprived because of multiple reasons for visits in some instances.
areas and the least deprived areas for both men and † Visits for documentation to be completed, and preventive care.
women. However, ethnicity and need factors had
differential effects on service use for men and wom- First, in line with the literature, gender appeared
en. While both Asian men and women have a lower to exert an important and independent effect on
number of GP visits than the number of visits by the utilisation of GP services, with women having
European men and women respectively, the results higher utilisation rates than men.3-16,39 However,
are significant only for Asian women who had 39% our results do not support the body of literature
fewer GP visits than European women. Interest- that suggests that women’s excess in service use
ingly, Maori men have more GP visits than Maori can largely be attributed to gynaecological and
women; however, the results are not statistically obstetrical conditions.22 We ran the regression
significant. The need factors also seemed to be more analyses after excluding gynaecological and
closely related with utilisation behaviour among obstetrical diagnoses, and still found an excess of
women. Women visiting the GP were 39% more female visits as compared to men. In that respect
likely to have reported ‘life-threatening’ problems we generally agree with Briscoe3 who found an
as compared to ‘self-limiting’ problems. There was excess of female consultations even after exclusion
no evidence of any interaction between gender of sex-specific consultations for pregnancy and
and any of the predictor variables that we tested for. postnatal examinations. The study does not sup-
port the view that sex-specific conditions explain
excess primary health care utilisation by women.
Discussion
This study explored the impact of gender on the Second, age, CSC and HUHC were predictors
utilisation of GP services in NZ. We also exam- of utilisation of GP services in both men and
ined systematically the extent to which predispos- women. In general, there was a positive relation-
ing, enabling and need factors might explain the ship in the use of GP services with age for both
frequently noted gender difference in use of health men and women. However, women exceeded men
services, in our case the utilisation of GP services. in visits to the GP across all age groups, thus
Many important findings emerge from this study. refuting the frequently noted reason for female
VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CARE 265ORIGINAL SCIENTIFIC PAPERS
quantitative research
Table 4. Treated prevalence (%) of major expanded diagnostic clusters (MEDCs) (age- tion behaviour in women than in men. NZ wom-
standardised)* en are more likely than men to visit a GP when a
problem is serious (Table 6). Our results diverge
Diagnosis Male Female P-value
(n=3553) (n=5063)
from those of Briscoe (1987) who found need fac-
Ear/nose/throat 17.1 15.2 .13 tors to be significantly associated with consulting
Musculoskeletal 15.4 11.8 .00 behaviour among men, but not among women,
Cardiovascular 10.9 9.5 .12 and those of Parslow et al.15 who found need
Skin 15.2 13.8 .21 factors to have a significant impact on both men’s
Psychosocial 10.1 11.9 .09 and women’s use of GP services as well as obtain-
Respiratory 9.3 8.4 .34 ing additional services. One explanation for this
Allergy 7.1 6.1 .26 divergence could be the use of different measures
General surgery 5.8 6.5 .42 of need; in Briscoe’s case, physical health status
Gastrointestinal/hepatic 7.7 6.6 .17 and the number of physical symptoms experi-
Endocrine 3.4 3.5 .89
enced over the past 12 months was used and, in
Neurologic 5.4 6.6 .15
the case of Parslow et al., self-assessed physical
Genitourinary 2.6 3.8 .05
and mental health were used. However, the di-
Eye 3.2 2.8 .41
Administrative 8.3 6.0 .01
vergence also underlines the different meaning of
Infectious 3.1 3.0 .85 health needs for men and women, suggesting that
Rheumatologic 2.5 1.2 .02 women may be more willing to admit the urgency
Reconstructive 2.6 1.6 .07 and severity of an illness and seek help. It may
Malignancies 1.8 0.9 .02 also be possible that women are more interested
Nutrition 1.0 1.6 .10 in health matters and more aware of existing and
General signs and symptoms 3.6 4.1 .38 potential health problems, and therefore more
Dental 0.7 0.5 .38 likely to obtain services from their GP, especially
Haematologic 0.6 0.9 .27 with urgent and severe illnesses. In comparison,
Renal 0.5 0.4 .57 men may be less concerned and knowledgeable
Toxic effects 0.5 0.7 .44 about their health and, consequently, less likely
Genetic 0.3 0.1 .09
to obtain health services. It is possible that NZ
Source: National Primary Medical Care Survey, 2000 men use hospital emergency services for urgent
* Analysis limited to those visit records with disease data coded. There were up to four diagnoses and life-threatening conditions or that they visit
per visit. specialists, while women use GPs. More detailed
studies are needed for a better understanding of
excess being obstetric-related.21 Holding a CSC the reasons and underlying meaning of gender
or a HUHC was also positively associated, as differences in the utilisation of health services.
expected, with high utilisation of GP services for
both men and women, as these cards entitled the
Strengths and limitations
holder to lower co-payments.
A major strength of the study is that the data de-
Our third major finding is the differential effects scribe patient visits to a nationally representative
of ethnicity and need on use of GP services for sample of GPs. However, there are several limita-
men and women. While both Asian men and tions to this study. First, bias may have been
women have a lower number of GP visits than introduced as a result of the overall GP response
European men and women respectively, the rate of 76.7%. Non-responders tended to be male
results are significant only for Asian women who and reported greater than average patient loads. If
had 39% fewer GP visits than European women. the characteristics of patient visits to the busiest
GPs differed in some systematic way, this may
Similarly, the findings from the separate regres- bias the results. The magnitude and direction of
sion analyses for men and women (Table 6) clearly such bias is unknown.
demonstrate a close relationship between consul-
tation behaviour and severity of the problem in Second, as the study is based on a cross-sectional
women but not in men, suggesting that the need survey design, directionality of any association
component was more likely to predict consulta- between predisposing, enabling and need factors
266 VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CAREORIGINAL SCIENTIFIC PAPErS
quantitative research
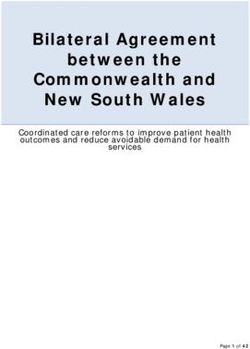
Table 5. Incidence risk ratios * (95% confidence intervals) from the Poisson regression models of the total number of GP visits
Characteristics Model 1a Model 2b Model 3b Model 4d Model 5e
Predisposing
Gender
Females 1.14 (1.06–1.23) 1.23 (1.13–1.33) 1.09 (1.01–1.18) 1.12 (1.03–1.22) 1.13 (1.03–1.24)
Males 1.00 1.00 1.00 1.00 1.00
Age group (years)
16–24 0.38 (0.33–0.45) 0.47 (0.38–0.58)
25–34 0.51 (0.43–0.61) 0.63 (0.50–0.79)
35–44 0.56 (0.48–0.66) 0.71 (0.60–0.84)
45–54 0.70 (0.57–0.87) 0.95 (0.73–1.24)
55–64 0.73 (0.64–0.83) 0.85 (0.74–0.97)
65+ 1.00 1.00
Marital status
Married 0.87 (0.79–0.96) 0.95 (0.85–1.07)
Unmarried/never married 1.00 1.00
Ethnicity of patients
Maori 1.05 (0.83–1.32) 1.05 (0.80–1.38)
Pacific 0.95 (0.77–1.18) 0.92 (0.76–1.13)
Asian 0.71 (0.54–0.94) 0.68 (0.51–0.89)
Others 0.81 (0.70–0.94) 0.76 (0.64–0.89)
NZ European 1.00 1.00
NZDep 2001 quintile
1 0.96 (0.83–1.10) 1.13 (0.98–1.29)
2 1.01 (0.87–1.17) 1.09 (0.95–1.26)
3 1.15 (0.97–1.37) 1.23 (1.02–1.48)
4 1.16 (0.99–1.37) 1.22 (1.05–1.41)
5 1.00 1.00
Enabling resources
Community Service Card (CSC)
Yes 1.49 (1.36–1.63) 1.39 (1.20–1.60)
No 1.00 1.00
High Use Health Card (HUHC)
Yes 2.64 (2.29–3.05) 2.33 (1.93–2.82)
No 1.00 1.00
Need component–practitioner perception
Urgency of the visit
ASAP 0.95 (0.72–1.25) 1.03 (0.74–1.41)
Today 1.27 (1.03–1.56) 1.34 (1.05–1.70)
This week 1.22 (1.01–1.47) 1.15 (0.93–1.43)
This month 1.00 1.00
Severity of the problem
Life-threatening 1.84 (1.25–2.70) 1.33 (1.04–1.71)
Intermediate 1.22 (1.10–1.34) 1.12 (1.00–1.26)
Self-limiting 1.00 1.00
Source: National Primary Medical Care Survey, 2000
* Incidence risk ratio measures the expected change in the dependent variable as a result of a one-unit change in the predictor variable.
a Model 1: Gross model.
b Model 2: Adjusted for age, marital status, ethnicity of patients and NZDep (predisposing characteristics).
c Model 3: Adjusted for Community Service Card (CSC) and High Use Health Card (HUHC) (enabling resources).
d Model 4: Adjusted for urgency of visit and severity of the problem (need factors).
e Model 5: Adjusted for all the predisposing, enabling, and need factors.
VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CARE 267ORIGINAL SCIENTIFIC PAPERS
quantitative research
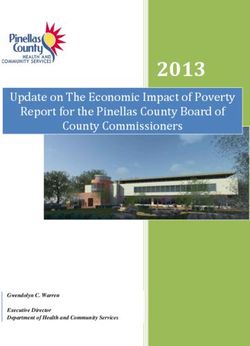
Table 6. Incidence risk ratios* (significance level) from the Poisson regression models of and use of primary health services cannot be
the total number of GP visits, separate models for men and women† inferred from our findings. We anticipate that
Characteristics Men Women future data collection through a longitudinal
Predisposing project will offer the opportunity to identify
Age group (years) causal links between health services use and vari-
16–24 0.41 (0.31–0.53) 0.50 (0.38–0.66) ous predisposing, enabling and need factors.
25–34 0.52 (0.40–0.69) 0.67 (0.52–0.88)
Third, NatMedCa was a practitioner-based, rather
35–44 0.66 (0.48–0.91) 0.73 (0.59–0.92)
than a population-based, survey. The data refer to
45–54 0.92 (0.65–1.29) 0.96 (0.68–1.38)
the actual work of GPs rather than to population
55–64 0.83 (0.68–1.01) 0.85 (0.71–1.02)
utilisation or to the needs of different popula-
65+ 1.00 1.00 tions. As a visits-based study, NatMedCa over-
Marital status represents frequent users. For this reason care
Married 0.91 (0.77–1.08) 0.95 (0.82–1.10) must be exercised when generalising results to
Unmarried/never married 1.00 1.00 the general population: the results of this study
Ethnicity of patients apply to users of primary health care services
Maori 1.39 (0.76–2.55) 0.89 (0.76–1.04) rather than to the general population.
Pacific 1.05 (0.73–1.51) 0.85 (0.69–1.06)
Asian 0.78 (0.55–1.10) 0.61 (0.43–0.85) Fourth, we did not control for the health status
Others 0.75 (0.58–0.96) 0.76 (0.62–0.94) of the patients and this may have impacted our
NZ European 1.00 1.00 results.
NZDep 2001 quintile
Fifth, although we have adjusted for many
1 1.07 (0.83–1.39) 1.15 (0.99–1.35)
confounding variables, it is possible that the dif-
2 1.21 (0.93–1.58) 1.02 (0.87–1.19)
ferences we found in the visits to the GP could
3 1.34 (0.87–2.07) 1.16 (0.99–1.36)
be the result of other factors associated with pri-
4 1.18 (0.94–1.49) 1.23 (1.02–1.48) mary care that we did not measure. For example,
5 1.00 1.00 studies have shown the effects of gender concord-
Enabling resources ance (i.e. similarity in gender of physician and
Community Service Card (CSC) patient) and ethnic concordance (i.e. similarity in
Yes 1.36 (1.11–1.67) 1.37 (1.14–1.65) ethnicity of physician and patient) on aspects of
No 1.00 1.00 health care delivery.41-46
High Use Health Card (HUHC)
Yes 2.63 (2.09–3.31) 2.22 (1.69–2.92) Conclusion
No 1.00 1.00
Need component–practitioner perception
Notwithstanding these limitations, the study
yields intriguing results. We found an inde-
Urgency of the visit
pendent and significant effect of gender on the
ASAP 1.13 (0.78–1.65) 0.98 (0.65–1.49)
utilisation of NZ GP services. This study found
Today 1.27 (0.97–1.65) 1.37 (0.99–1.90)
significant female excess in utilisation of GP
This week 1.14 (0.93–1.40) 1.16 (0.86–1.58)
services even after excluding gynaecological and
This month 1.00 1.00 obstetrical conditions and across all age groups.
Severity of the problem We also found the differential effects of ethnic-
Life-threatening 1.29 (0.88–1.90) 1.39 (1.00–1.94) ity and need (severity of a problem) on use of
Intermediate 1.14 (0.95–1.38) 1.10 (0.95–1.28) GP services for men and women. Asian women
Self-limiting 1.00 1.00 were significantly less likely to visit a GP than
Source: National Primary Medical Care Survey, 2000
European women, and women visiting GPs were
more likely to have reported ‘life-threatening’
* Incidence risk ratio measures the expected change in the dependent variable as a result of a one-
unit change in the predictor variable.
problems as compared to ‘self-limiting’ problems.
However, ethnicity and the severity of a problem
† Adjusted for all the predisposing, enabling, and need factors.
did not predict consultation behaviour in men.
268 VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CAREORIGINAL SCIENTIFIC PAPErS
quantitative research
References The differential impact of social position and social roles. Soc Sci
1. Anson O. Marital status and women’s health revisited: the Med. 1992;40:597–611.
importance of a proximate adult. J Marriage Fam. 23. Greenley MD, Clearly P. Seeking help for psychological
1989;51:185–194. problems: replication and extension. Med Care. 1987;24:1113.
2. Smith JA, Braunack-Mayer A, Wittert G. What do we know 24. Hibbard JH, Pope CR. Gender roles, illness orientation and use of
about men’s help-seeking and health service use. Med J Aust. medical services. Soc Sci Med. 1983;17:129–137.
2006;184(2):81–83. 25. Hibbard JH, Pope CR. Another look at gender differences in the
3. Briscoe ME. Why do people go to the doctor? Gender use of medical care: illness orientation and the types of morbidities
differences in the correlates of GP consultation. Soc Sci Med. for which services are used. Women Health. 1986;11:21–26.
1987;25:507–513. 26. Verbrugge LM. Gender and health: an update on hypotheses
4. Clearly PD, Mechanic D, Greenley JR. Sex differences in medical and evidence. J Health Soc Behav. 1985;26:156–182.
care utilisation: an empirical investigation. J Health Soc Behav. 27. Verbrugge LM, Ascione FJ. Exploring the iceberg. Common
1982;23:106–119. symptoms and how people deal with them. Med Care.
5. Corney RH. Sex differences in general practice attendance and 1987;25:539–569.
help seeking for minor illness. J Psychosom Res. 1990;34:525–534. 28. Callister P, Didham R. Dying differently: gendered mortality
6. Fylkesnes K, Johnsen R, Forde OH. The Tromso study: factors trends in New Zealand: IPS Working Paper 09/01. Wellington:
affecting patient initiated and provider initiated use of health Institute of Policy Studies; 2009.
care services. Sociol Health Illn. 1992;14(2):275–289. 29. Johnson L, Huggard P, Goodyear-Smith F. Men’s health and the
7. Gijsbers van Wijk CM, van Vliet KP, Kolk AM, Everaerd WT. health of the nation. N Z Med J. 2008;121(1287):69–76.
Symptom sensitivity and sex differences in physical morbidity: a 30. Neville S. Men and health. N Z Med J. 2008;121(1287):7–10.
review of health surveys in the United States and The 31. Anderson R, Newman JF. Societal and individual determinants of
Netherlands. Women Health. 1991;17:91–124. health care utilisation in the United States. Milbank Mem. Fund
8. Gijsbers van Wijk CMT, Kolk AM, van den Bosch WJ, van den Q. 1973;51:95–124.
Hoogen HJM. Male and female morbidity in general practice: 32. Raymont A, Lay-Lee R, Davies P, Scott A. Family doctors:
The nature of sex differences. Soc Sci Med. 1995;35:665–678. methodology and description of the activity of private GPs. The
9. Green CA, Pope CR. Gender, psychosocial factors and the use of National Primary Care Survey (NatMedCa), 2001/02 Report 1.
medical services: A longitudinal analysis. Soc Sci Med. Wellington: Ministry of Health. Available on the MoH website:
1999;48:1363–1372. http://www.moh.govt.nz/natmedca, 2004.
10. Kandrack MA, Grant KR, Segalml A. Gender differences in 33. Korn E, Graubard B. Epidemiologic studies utilizing surveys:
health related behaviour, some unanswered questions. Soc Sci accounting for the sampling design. Am. J. Public Health
Med. 1991;32:579–590. 1991;81:1166-1173.
11. Ladwig KH, Marten-Mittag B, Formanek B, Dammann G. Gender 34. Crampton P, Salmond C, Kirkpatrick R. A case for government
differences of symptoms reporting and medical health care ownership of primary health care services in New Zealand:
utilisation in the German population. Eur J Epidemiol. weighing the arguments. Int J Health Serv. 2004;34:709–729.
2000;16:511–518. 35. Winkelmann R, Zimmermann K. Count data models for
12. Lahelma E, Martikainen P, Rahkonen O, Silventoinen K. Gender demographic data. Math Popul Stud. 1994;4:205–221.
differences in ill health in Finland: patterns, magnitude and 36. Winkelmann R, Zimmermann K. Recent developments in count
change. Soc Sci Med. 1999;48:7–19. data modelling: theory and application. J Econ Survey 1995;9:1–24.
13. Verhaak PFM. Determinants of the help-seeking process: 37. Research Triangle Institute. SUDAAN user’s manual, release 8.0:
Goldberg and Huxley’s first level and first filter. Psychol Med. Research Triangle Park, NC, Research Triangle Institute, 2002.
1995;25:95–104. 38. Lemeshow S, Letenneur L, Dartigues J, Lafont S, Orgogozo J,
14. Williams P, Tarnopolsky A, Hand D, Shepherd M. Minor Commenges D. Illustration of analysis taking into account
psychiatric morbidity and general practice consultations: the West complex survey considerations: the association between wine
London Survey. Psychol Med. 1986; Monograph supplement 9. consumption and dementia in the PAQUID study. Am J
15. Parslow R, Jorm A, Christensen H, Jacomb P, Rodgers B. Gender Epidemiol. 1998;148:298–306.
differences in factors affecting use of health services: an analysis 39. Anson O, Paran E, Neumann L, Chernichovsky D. Gender
of a community study of middle-aged and older Australian. Soc differences in health perceptions and their predictors. Soc Sci
Sci Med. 2004;59:2121–2129. Med. 1993;36:419–427.
16. Sayer GP, Britt H. Sex differences in morbidity: case study of 40. Joung IMA, van der Meer JWB, Mackenbach JP. Marital status ACKNOWLEDGMENTS
discrimination in general practice. Soc Sci Med. 1996;42:257–264. and health care utilisation. Int J Epidemiol. 1995;24:569–575. We are grateful for the
17. Scott KM, Marwick JC, Crampton P. Utilisation of general 41. Bertakis KD, Helms LJ, Callahan EJ, Azari R, Robbins JA. The assistance, support and
practitioner services in New Zealand and its relationship with influence of gender on physician practice style. Med Care. data access provided by
income, ethnicity and government subsidy. Health Serv Manage 1995;33(4):407–416. the NatMedCa research
Res. 2003;16:45–55. 42. Frank P, Bertakis KD. Physician gender, patient gender, and group led by Prof. Peter
18. Adamson J, Ben-Shlomo Y, Chaturvedi N, Donovan J. Ethnicity, primary care. Journal of Women’s Health. 2003;12(1):73–80. Davis. The NatMedCa
socio-economic position and gender—do they affect reported 43. Greenfield S. Commentary: are we ready to act on racial survey was funded by
health-care seeking behaviour? Soc Sci Med. 2003;57:895–904. concordance? J Public Health Policy. 2003;24(3/4):324–327. the Health Research
19. Hunt K, Ford G, Harkins L, Wyke S. Are women more ready to 44. Gross R, McNeill R, Davis P, Lay-Yee R, Jatrana S, Crampton P. Council of New Zealand.
consult than men? Gender differences in family practitioner The association of gender concordance and primary care We would like to thank
consultation for common chronic conditions. J Health Serv Res physicians’ perception of their patients. Women & Health.
all those practitioners
Policy. 1999;4:96–100. 2008;48(2):123–143.
and organisations
20. Wyke S, Hunt K, Ford G. Gender differences in consulting a 45. Henderson JT, Weisman CS. Physician gender effects on
preventive screening and counselling: an analysis of male and
who provided data or
general practitioner for common symptoms of minor illness. Soc
Sci Med. 1998;46:677–689. female patients’ health care experiences. Med Care. otherwise supported
21. Waldron I. Sex differences in illness incidence, prognosis and 2001;39(12):1281–1292. the NatMedCa study.
mortality: issues and evidence. Soc Sci Med. 1983;17:1107–1123. 46. Schmittdiel J, Grumbach K, Selby JV, Quesenberry CP. Effect of
22. Gijsbers van Wijk CMT, Kolk AM, van den Bosch WJHM, van physician and patient gender concordance on patient satisfaction competing interests
den Hoogen HJM. Male and female problems in general practice: and preventive care practices. J Gen Intern Med. 2000;15:761–769. None declared.
VOLUME 1 • NUMBER 4 • DECEMBER 2009 J OURNAL OF PRIMARY HEALTH CARE 269You can also read