LESSONS FROM EBOLA AFFECTED COMMUNITIES: Royal African Society
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

LESSONS FROM EBOLA AFFECTED COMMUNITIES: Being prepared for future health crises FEBRUARY 2016 This report is written by Polygeia and commissioned by the Africa APPG with fieldwork funding from the Royal African Society. This is not an official publication of the House of Commons or House of Lords. It has not been approved by either House or its committees. All-Party Parliamentary Groups are informal groups of Members of both Houses with a common interest in particular issues

Cover Photograph:
Restless Development ©2015
2
CONTENTS
ACKNOWLEDGEMENTS 4
FOREWORD 9
ACRONYMS AND ABBREVIATIONS 10
EXECUTIVE SUMMARY 11
INTRODUCTION 13
1 WHAT WEAKNESSES HAS THE EBOLA OUTBREAK EXPOSED? 14
1.1 The West African Ebola Outbreak 15
1.1.1 Lasting Impact on Communities 18
1.2 The Response 20
1.2.1 National Response 21
1.2.2 International Response 23
1.2.3 The UK’s Role in the Ebola Response 24
1.3 Underlying Challenges: Health Systems and Infrastructure 27
1.3.1 Health Systems in Guinea, Liberia and Sierra Leone 28
1.3.2 Rural, Peri-Urban and Urban Challenges 32
1.3.3 Legacies of War and Reconstruction 33
1.4 Summary 34
2 HOW IMPORTANT ARE COMMUNITY-LED APPROACHES TO HEALTH? 35
2.1 What is a ‘Community-Led’ Approach? 35
2.2 The Role of Communities in the Response:
Building Trust and Legitimacy 38
2.2.1 Initial Public Mobilisation Campaigns: Resistance and Fear 38
2.2.2 Community Groups: Rising to the Challenge 39
2.3 Localised Approaches: Community, Engagement and Consultation 48
2.4 Avoiding Parallel Systems: Utilising Existing Structures 51
2.5 Summary 54
3 HOW CAN THE UK AND INTERNATIONAL DONORS BEST SUPPORT
COMMUNITY-LED APPROACHES TO HEALTH SYSTEMS STRENGTHENING? 55
3.1 Putting Community at the Centre of Future Health Programmes 55
3.2 Earlier Community Consultation: Fostering Ownership 57
3.3 Recognising Communities as Experts in Themselves 58
3.4 Harnessing Local Resources: Building a Sustainable and Local
Health Workforce 60
3.5 Coordination: The Need to Strengthen Multi-Stakeholder
Partnerships 61
3.5.1 Coordinating National Stakeholders 61
3.5.2 Coordinating International Stakeholders 62
3.6 Supporting National Governments to Achieve Universal Health
Care 64
3.7 Conclusion 65
4 RECOMMENDATIONS 66
4.1 Recommendations for UK Government 66
4.2 Recommendations for UK Actors 67
REFERENCES 68
3
ACKNOWLEDGEMENTS
This report was written by Polygeia with We are especially grateful to Restless
direction and oversight from the Africa Development in Sierra Leone and Public
APPG. Health and Development Initiative (PHDI)
for their support in co-developing and
Co-editors from Polygeia: Thomas Hird & conducting the key informant interviews
Samara Linton with community leaders in their
Researchers: Maisy Grovestock, Shreya respective countries on behalf of Polygeia
Nanda, Rhys Wenlock, Waqas Haque & and the Africa APPG:-
Ben Walker.
Restless Development in Sierra Leone:
Jamie Bedson,Saiku Bah, Prince Kenneh,
George Tamba Sellu, Susan Manie, Juliana
Sama Fornah, Mohamed A Jalloh and
Alfred T M Nav
Special thanks to Lord Chidgey (Co-
Chair) for heading up the inquiry and
sessions and to Hetty Bailey the APPG
Coordinator.
Public Health and Development Initiative
(PHDI) Liberia: Dr Alaric Topka
Thank you to RAS for their support of the
Africa APPG and funding of the report and
associated field research. Special thanks
to Richard Dowden, Director at RAS and
Susana Edjang, a RAS council member for
their input and guidance. Thank you to
Gemma Haxby for proof reading.
4Parliamentarians who contributed to
report drafts or attended thematic
sessions -
• Baroness Armstrong
• Paul Burstow MP
• Lord Cameron
• Lord Chidgey
• Lord Crisp
• Lord Collins
• Mark Durkan MP
• Lord Giddens
• Baroness Hayman
• Meg Hillier MP
• Pauline Latham MP
• Lord Lea
• Jeremy Lefroy MP
• Baroness Kinnock
• Baroness Masham
• Duke of Montrose
• Lord Patel
• Lord Ribeiro
• Earl of Sandwich
• Lord Watson
5• ReBUILD, COUNTDOWN and REACHOUT
Consortium
The Africa APPG expresses their sincere • Restless Development
thanks to all those who contributed to • Save the Children
this review, without whom this report • SciDev.Net
would not have been possible.
• Professor Joanne Sharp, University of
Glasgow
Thank you to all of those that submitted
• WHO Country Office Liberia & WHO
written evidence to the inquiry-
African Programme for Onchocerciasis
• African Diaspora Healthcare Control - Oyene U.E, Prof Amazigo U.V,
Professionals for Better Health in Africa Cole I, Zoure H.G.M, Bette A.K,
initiative & Dr Titi Banjoko Dr Afework H.T & Dr Fobi G
• Amref Health Africa • World Vision International UK & Sierra
• Action Contre la Faim (ACF) Leone
• ActionAid
• Dan Cohen, Maccabee Seed Company, Thanks also to Dr Fred Martineau
Davis CA Coordinator of Ebola Response
• Doctors of the World (DotW) in Anthropology Platform and to the
partnership with Medicos del Mundo APPG on Global Health who helped
(MdM)
• Fambul Tok
• Prof Mariane Ferme, University of
California, Berkeley
• Derek Gatherer PhD CertEd, Lancaster
University
• Health Partners International
• Health Poverty Action
• Institute of Development Studies in
particular Professor Melissa Leach &
Dr Pauline Oosterhoff for their support
• International Rescue Committee
• Dr Nathaniel King, The World Bank
Group
• Dr. Jill Lewis, Living for Tomorrow
• Malaria Consortium
• Marie Stopes International
• Dr David Nabarro, UN Special Envoy on
Ebola
• Njala University, Sierra Leone in
particular Prof. Paul Richards, Roland
Suluku & Thomas Songu
• Dr Melissa Parker, Reader LSHTM & PI
of the Ebola Response Anthropology
Platform
• Pandemic and Epidemic Disease
department (PED) WHO
• Peter Penfold, CMG, OBE- former British
High Commissioner to Sierra Leone
6in circulating the Africa APPG’s call for the World Health Organisation African
evidence. region;
Thank you to those that contributed to • Dr. Adrian Thomas - Vice President of
the five thematic panels on the subject or Global Market Access & Head of Global
gave oral evidence - Public Health, Janssen Pharmaceutical
• Dr Uche Amazig - former head of the Companies of Johnson & Johnson
African Partnership for Onchoceriasis • H.E. Edward Mohamed Turay - High
Control Commissioner for Sierra Leone
• Dr Egeruan Babatunde Imoukhuede • Peter West - British High Commissioner
- Clinical Project Manager and to Sierra
Vaccinologist, The Jenner Institute
• Dr Titilola Banjoko – Royal Africa
Society
• Dr Michael Edelstein - Centre on Global
Health Security, Chatham House
• Nic Hailey, Former Director Africa at the
FCO
• Prof Catherine Hoppers - University of
South Africa
• Dr. Arif Husain - Chief Economist, World
Food Programme
• Dr. Adesina Iluyemi PhD - Executive
Board Member, NEPAD Council
• Dr. Monty Jones - Special Advisor to the
President of Sierra Leone
• Tulip Mazumdar - Global Health
Correspondent, BBC News
• Solomon Mugera - Editor, BBC Africa
• Dr David Nabarro - UN Special Envoy on
Ebola
• Baroness Northover - Former
Parliamentary Under Secretary of State
for DFID
• Dr Francis Omaswa - Executive Director
of the African Centre for Global Health
and Social Transformation and former
Director General of Health services in
Uganda;
• Dr. Robtel Neajai Pailey - Liberian
academic, activist, and author based at
SOAS, University of London
• Larissa Pelham - Emergency Food
Security & Vulnerable Livelihoods
Adviser, Oxfam
• Mr Jon Pender - Vice President,
Government Affairs, GlaxoSmithKline
• Dr. Paul Richards - Njala University,
Sierra Leone
• Dr Luis Sambo - Executive Director of
78
FOREWARD
The Ebola crisis in West Africa
demonstrated clearly how vulnerable
the region was to rampant disease.
Robust health systems, available at the
point of need, were simply not there.
There was little ability among the
populations to pay. In the circumstances
the responses from community health
workers, local health systems and the
people themselves were, in many cases,
remarkable and totally selfless.
The Republic of Guinea, Sierra Leone
and Liberia share not only common
borders, but deep cultural, language and
ethnic affinities. The borders themselves
barely exist for the local populations
that straddle them. In the mountainous
rainforest regions of the interior, there
are minimal transport networks and
non-existent utilities such as mains water,
sanitation and electricity. Communities in
remote villages are virtually inaccessible.
Congratulations are due to Polygeia in
drawing together written and verbal
evidence on the responses to the Ebola
health crisis from well over 200 sources.
Their extensive analysis of the community
engagement in the response to Ebola
alongside national, international, and
health aid agencies intervention in this
report provides important guidance for
the future.
Lord Chidgey,
Co-Chair Africa All-Party Parliamentary Group
9ACRONYMS AND ABBREVIATIONS
APPG All-Party Parliamentary Group
ACAPS Assessment Capacities Project
AFRO (World Health Organization) African Region Office
ASEOWA African Union Support to Ebola Outbreak in West Africa
AMREF African Medical and Research Foundation
AU African Union
CDC Centers for Disease Control and Prevention
CEBS Community Evidence-Based Surveillance
CHW Community Health Worker
CLEA Community-Led Ebola Action
CWC Community Watch Committee
DERC District Emergency Response Centre (Sierra Leone)
DFID Department for International Development
DHMT District Health Management Team (Sierra Leone)
EBOLA/EVD Ebola Virus Disease
ETU Ebola Treatment Unit
FGM Female Genital Mutilation
FHCI Free Healthcare Initiative
HIV/AIDS Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome
HSS Health Systems Strengthening
IDC International Development Committee
IDS Institute of Development Studies
IFRC International Federation of Red Cross
IHR International Health Recommendations
IOM Institutional Organisation for Migration
IRC International Rescue Committee
LSHTM London School of Hygiene and Tropical Medicine
MNCH Maternal Neonatal and Child Health
MOH Ministry of Health
MoHS-HED MOH Health Education Department (Sierra Leone)
MSF Médecines Sans Frontières
NGO Non-Governmental Organisation
NHS National Health Service
OECD Organisation for Economic Co-Operation and Development
PHU Public Health Unit
PPE Personal Protective Equipment
PRA Participatory Rural Appraisal
SAGE Scientific Advisory Group in Emergencies
SMAC Social Mobilisation Action Consortium
UK United Kingdom
UN United Nations
UNFP United Nations Population Fund
UNICEF United Nations Children’s Fund
UNMEER UN Mission for Ebola Emergency Response
US United States of America
USAID United States Agency for International Development
WHO World Health Organization
10EXECUTIVE SUMMARY
By January 20th 2016, an Ebola epidemic groups in the community including
in West Africa had killed 11,316 people. women, young people and community
It had begun over two years before in leaders and highlights the crucial role
Guinea and exposed under-resourced they played in creating successful
and over-burdened health systems in strategies to control Ebola. To ensure
the affected countries. The international the voices of affected communities
response was weak. However the UK were represented in the report, 23 key
played a key role by providing Sierra informants were interviewed. In Sierra
Leone with £427m worth of medical, Leone these were conducted by Restless
technical and logistical support Development, and in Liberia by Public
largely through the Department for Health & Development Initiative (PHDI).
International Development. These
funds were given to the Sierra Leone This report finds that response efforts
government, front-line NGOs and other were most effective when communities
vital actors and used to support a range demanded assistance at the local level.
of research. It therefore advocates that although
a top down approach (nationally and
At Westminster between October 2014 internationally) may always be necessary
and May 2015 the Africa All Party in a health crisis such as an Ebola
Parliamentary Group organised a series outbreak, it is only effective when the
of panel discussions on the international affected communities trust that response.
response to Ebola. Panellists who The report acknowledges that the
had worked in the Ebola-affected need to react rapidly in a health crisis
communities stressed repeatedly that makes it almost impossible to consult
the response was being hindered communities immediately. However the
by fear and a lack of trust between key lesson in ensuring preparedness for
national actors, international actors and future health crises is that health systems
affected communities. Consequently should be developed horizontally, local
the APPG, together with Polygeia, ownership should be prioritised and
launched an enquiry into attempts to investment made at community level.
engage the affected communities in Such approaches foster trust and create
the response (1). This report reviews the demand for health services. Communities
evidence submitted by key informants should be consulted about their needs
through interviews and a literature and local facilities and systems developed
review. It reflects the lessons learned to provide permanent services which
from the Ebola outbreak and explores local people trust and access and which
the importance of trust between can respond effectively during a crisis.
governments, health workers and
communities and the importance of local The chief finding of the report is that
ownership of health systems. efforts to curb the outbreak of Ebola in
West Africa were most effective when
A diverse range of actors were involved local leaders of affected communities
in the response in West Africa. They often led the demand for assistance from
had different priorities and strategies their governments and the international
and not every strategy was successful. In actors, and played an essential leadership
the early stages mistrust of and resistance role in the management of that
to responders was indicative of a lack assistance.
of community engagement. This report
analyses the engagement by different
11The chief recommendation of this report
is that the UK government and non-
governmental organisations should give
higher priority to community ownership
of health. This would strengthen local
health systems and enable them to
respond more effectively to a crisis.
The conclusions of this report will help
guide a UK response to future epidemics
and, in the long term, help reconstruct
and strengthen health systems in poor
countries.
A summary of this report and its
recommendations was included as
written evidence to the House of
Commons International Development
Committee; Ebola: Responses to a public
health emergency (2).
12INTRODUCTION
The Africa All-Party Parliamentary with community leaders in rural and
Group commissioned researchers from urban areas to gain insights into the
Polygeia, a student-run global health response of their communities in the
think tank, to explore the experiences of Ebola response.
communities affected by the 2014 - 2015
Ebola crisis in Sierra Leone, Liberia and The role of communities in the response
Guinea. The researchers also examined to a health crisis such as Ebola is complex
the role of affected communities in the and multifaceted. This report uses a
response to the outbreak and learned broad definition of community to include
lessons for community engagement any group of people who are linked by
in health crises and more broadly the social ties and common perspectives, and
implications for strengthening health engage in joint actions. Communities
systems in West Africa. vary hugely within and between these
countries so it is difficult to generalise
Chapter One explores the response and their response to the crisis. However, this
the effectiveness of national health report aims to draw out central themes
systems of countries affected by the and lessons from the Ebola outbreak,
Ebola outbreak in the context of their which could improve community
socio-political and historical factors. engagement and effectiveness in
response to a health crisis in the short
Chapter Two examines evidence of term and in the longer term contribute
community mobilisation and community- to a stronger health system.
led interventions in the Ebola crisis and
evaluates their importance.
Chapter Three focuses on how the UK
can influence, strengthen and improve
the response of communities and
national health systems to health crises.
The report includes evidence from 31
written submissions in response to a call
for evidence; the findings of 5 meetings
held by the Africa APPG to discuss the
Ebola response including the role of
the media, pharmaceutical companies
and community actors, the impacts on
economies, food security, women and
community resilience; and a review of
the literature on Ebola outbreaks. 19
parliamentarians were involved in the
process. To ensure the voices of affected
communities were represented, the
Africa APPG and Polygeia worked with
Restless Development, a youth-led
development agency, in Sierra Leone and
Public Health & Development Initiative
Liberia (PHDI) in Liberia. Researchers
conducted 23 key informant interviews
131 WHAT WEAKNESSES HAS THE
EBOLA OUTBREAK EXPOSED
The Ebola Virus Disease (Ebola) was first “Clinicians in equatorial Africa have
identified in the Democratic Republic good reasons to suspect Ebola when a
of Congo (then Zaire) and South Sudan “mysterious” disease occurs, and this
(then Sudan) in 1976 and named after favours early detection. Laboratory
the Ebola River in northern Congo. It is capacity is in place. Staff know where
believed to be zoonotic which means to send patient samples for rapid and
reliable diagnosis. Health systems are
it normally exists in animals but can
familiar with Ebola and much better
be transmitted to people. Once in the
prepared. For example, hospitals in
body, rapid viral replication affecting Kinshasa, the capital of the Democratic
immune cells and blood vessels triggers Republic of Congo, have isolation wards,
systemic inflammation and a drop in and staff are trained in procedures
blood pressure. This can lead to death for infection prevention and control.
from shock and multiple organ failure Governments know the importance of
(3). Ebola is also passed between people treating a confirmed Ebola case as a
through direct contact with the blood or national emergency.”
other bodily fluids or the secretions of an
infected person. On average, it takes 8 West African countries, having never
to 10 days for symptoms to appear and is experienced an Ebola outbreak, were
often confused with cholera and malaria, poorly prepared for this disease at
making early diagnosis difficult (4,5). every level, leading to the initial rapid
Treatment consists of intensive care, oral and undetected spread in what was to
rehydration salts and intravenous fluids. become the largest and deadliest Ebola
At present, candidate vaccines are in outbreak in history.
clinical trials with planned submission for
licensure by the end of 2017 (6).
In the 40 years since its discovery there
have been 26 Ebola outbreaks in 12
countries. The case fatality rate for each
outbreak ranges between 25% and 90%
with approximately 2361 cases and 1548
deaths prior to the 2014 - 2015 West
African Ebola outbreak (5). Countries
in equatorial Africa have experienced
the most Ebola outbreaks: seven in
the Democratic Republic of Congo
and five in Uganda. In contrast to the
recent West Africa Ebola outbreak, all
previous outbreaks were controlled in
periods ranging from three weeks to
three months. This is partly attributable
to the preparedness of health systems.
According to the World Health
Organisation (7):
141.1 THE WEST AFRICAN EBOLA OUTBREAK
In December 2013, an 18-month-old boy the UK, Spain and US were diagnosed as
in Melindou, a village in Guinea, became infected (11–13). The US-based Center
the first case in the West Africa Ebola for Disease Control warned of up to 1.4
outbreak. There is evidence that he may million cases in West Africa by January
have been infected by contact with bats 2015 (13). Local and international press
(8). Family members quickly developed began to speculate on the potential
similar symptoms, as did funeral catastrophic consequences. This spurred
attendees and several traditional healers the international response to further
and hospital staff who had treated them action, but it also created an image of
in nearby Gueckedou. Over the following Africa that created panic and fear.
three months transmission chains carried
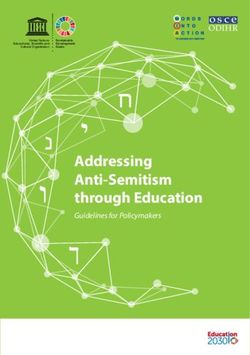
the virus cycle of exposure, cases, deaths Transmission peaked during October
and funerals to several cities, including 2014 with approximately 900 new
the capital, Conakry, and many more infections per week (see figure 1 and box
villages and rural districts (9). 1). The plateauing and eventual decline
of the incidence of the virus coincided
Initial investigations by the Meliandou with a surge in local and international
health centre, and later by staff from responses. Although direct correlation
Médecins Sans Frontières (MSF), between specific responses (medical,
suspected cholera which is endemic social or political) and the reduction in
in the region, but without conclusive cases is yet to be made.
evidence. In March 2014, a larger
investigation began which included At present – 2nd February 2016 –
the Ministry of Health, World Health The West African Ebola outbreak
Organisation (WHO), WHO Regional was declared to have ended on 14th
Office for Africa (AFRO) and Médecins January, however there has already
Sans Frontières (MSF) staff and the Ebola been re-emergence in Sierra Leone
virus was identified as the causative (14). There have been, in total, 28,638
agent. In June, MSF warned that Ebola confirmed probable and suspected cases
was “out of control” and called for the worldwide and 11,316 deaths. All but
“massive deployment of resources” as 36 cases and 15 deaths have occurred in
the disease continued to penetrate local Guinea, Liberia and Sierra Leone. The
communities in south-eastern Guinea geographical distribution of these cases is
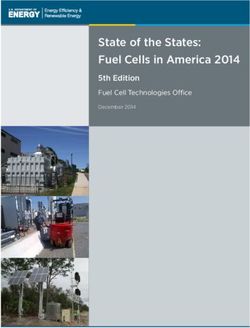
and began to spread in neighbouring shown in Figure 2 (15).
Sierra Leone and Liberia. On August 8th,
as the disease was entering its deadliest
phase, the WHO declared a Public Health
Emergency of International Concern
(PHEIC). During the following months,
Ebola intensified in both rural and urban
areas, with cases reported in Nigeria, a
country of almost 200 million people,
and Senegal.
In autumn 2014, two leading doctors,
Dr Samuel Brisbane of Liberia and Dr
Sheikh Umar Khan of Sierra-Leone,
succumbed to the disease (10), and
several healthcare workers returning to
15Figure 1 &
Box 1: Stages
of the West
African Ebola
crisis (1-4) by
the number
of confirmed
new Ebola
cases by
week.
(adapted from
presentation
by Dr Nabarro,
UN Special
Envoy for
Ebola (16)
& European
Centre for
Disease
Prevention
and Control
report (17))
Stage 1 Stage 3
• An unidentified disease spreading • Number of infections per week
through Guinea, Sierra Leone plateaus and falls
and Liberia. Lassa fever, Ebola or • Continued support from the
Cholera? international community, with the
• MSF and national governments focus moving away from care of
responded the earliest, with the infected to contact tracing
little initial buy-in from the • Community engagement is
international community instrumental in this stage
• Growing fear in communities
fuelled by misinformation and lack Stage 4
of understanding of preventative • Decrease in infections, outbreak
measures declared over in Jan 2016, but re-
emergence likely
Stage 2 • Support needs to continue to
• Most rapid increase in infections ensure that we get to zero cases
during the outbreak • Communities play key role in
• The threat of spread to Europe contact tracing and hidden cases
and North America was realised
• In September, the WHO
announced that the Ebola
outbreak was an “event of
international concern” and began
scaling up the response
• Large degrees of resistance were
displayed by the communities
16Figure 2:
Geographical
distribution
of total
confirmed
cases in
Guinea,
Liberia, and
Sierra Leone
as of 01
November
2015 (15).
Confirmed Cases
1-5
6 - 20
21 - 100
101 - 500
501 - 4000
No cases reported
171.1.1 LASTING IMPACT ON COMMUNITIES
The appalling suffering, enormous and hundreds have died from it. The
death toll and the catastrophic impact International Rescue Committee (IRC)
on affected communities cannot reports that as of January 2014, “65% of
be overstated. All the community health care worker infections occurred
leaders interviewed for this report among staff employed in non-Ebola
cited the collective trauma felt by the care facilities”. The most common cause
communities. was exposure because employees lacked
personal protective equipment (PPE) (22).
Beyond the immediate horror and loss Many people avoided health services
of life, the Ebola crisis brought the usual altogether because they feared infection
routines of daily life to a halt: restricted (15). This had adverse effects on all
population movement, interrupted major health programmes including TB,
harvests, lead to the closure of markets HIV, malaria and nutrition programmes
and restricted regional and international and routine vaccinations. The knock-
trade. Economic activity in the region on effects will be catastrophic (23). For
was reduced, reversing recent economic example, in many areas routine measles
gains in Sierra Leone, Guinea, and vaccination rates have fallen by at
Liberia. The United Nations Development least 25%. This could result in tens of
Group (UNDG) predicted a loss of GDP thousands of additional measles cases
of up to 9.6% ($315m USD) in Guinea, leading to between 500 to 4,000 deaths
8.0% ($292m USD) in Sierra Leone and (24).
18.7% ($245m USD) in Liberia (18). This
economic impact will continue to have a Ebola has disproportionately affected
considerable effect on employment and women. In the outbreak’s early stages,
household livelihoods in the region. The women were more likely to be exposed
region is predominantly rural and those to the virus than men due to their
communities which rely on subsistence care-giving role in families. This gender
farming are particularly exposed to an disparity continues in the knock-on
economic collapse (see case study below). effects of Ebola; a disproportionate
number of women in Sierra Leone,
This regional economic decline also Liberia and Guinea are employed in
caused a widespread crisis of food sectors most affected by the outbreak
security, affecting hundreds of thousands such as informal services and agriculture
of people in each country (19). In some (18,25).
areas there has been a slow economic
recovery in recent months but household Education has also been badly affected.
income remains low, food production Schools were closed in parts of Sierra
has fallen and higher food prices have Leone, Liberia, and Guinea for up to
hit already poor communities (20). The six or even eight months. Five million
World Food Programme (WFP) found children were affected (26). Loss of
that in many communities in Sierra household income may also mean more
Leone, Liberia and Guinea, transport children will drop out of school in the
issues are a key factor in reducing food longer term. Finally, some studies show
security (21). an increase in teen pregnancy and child
labour during this period (18,27).
Routine healthcare services have also
been disrupted in the region. The vast
majority of healthcare workers were
diverted to combat the Ebola outbreak
18Case Studies: The impact of the Ebola outbreak on communities
“We are hungry” on health in the district. “Clinic
Gelengasiasu Town lost eighteen attendance has been low … a lot of
people to Ebola. “The whole other people died not from Ebola, but
community was destroyed. Our houses from the fear to go to hospital when
spoiled. Human beings warm houses – they are sick. Health service delivery
with the deaths nobody was inside the has been seriously hampered, a lot of
houses” Folokula Gayn, the general gains made in healthcare have been
town chief, explains. “Our rice harvest lost as well.”
did not happen” Gayn continues. “We
are hungry; there is no way to even Interviews from Port Loko Town, Port
harvest rice”. Jackson Miller, from a Loko District, Sierra Leone
market town in neighbouring county
Gounwolaila, shares a similar story. “Children are fending for themselves”
“We have moved from town to our “Schools were closed, hospitals closed,
farms, disturbed our businesses and pregnant women were not taken
interrupted our farming. We are a care of, health practitioners were
market town”. afraid and children died of simple
ailments. Businesses were affected
Interviews from Gelengasiasu as parents were not going to work”
Town, Gbarpolu County, Liberia and Ruth Johnson from Lakpazee explains.
Kpayeakwelle, Gou Gounwolaila High School teacher, Lawrence Flomo,
County, Liberia. describes the impact on families in
Fiama community. “Records show
“A witch flight fell” over five family heads [have died
“It started with a story that a witch from Ebola]. Some children have
flight (plane) fell, so that is why been orphaned. Some children are
people were dying”. Ibrahim Fonah, fending for themselves. There are
a 32 year old from Port Loko Town, also orphans that were brought from
describes one of the many rumours other communities to Fiama”.
that spread through communities
during the early stages of the Interviews from Lakpazee and Fiama
outbreak. Dr Sesay, a medical officer Community, District 9, Liberia
shares the impact of fear and denial
191.2 THE RESPONSE
Box 2: Key Quarantine (73). However, this sometimes
tools of the • Stopping an Ebola epidemic slowed down and inhibited
Ebola response means prompt identification response workers.
and their and isolation of infected people.
challenges Ebola-infected patients must Safe burial
be quarantined to prevent it • Ebola-infected dead bodies are
spreading. extremely infectious; transmission
• Many people have highlighted through ceremonial body washing
the methods, extent and safety was common. Governments of
of some quarantine policies all three Ebola-affected countries
(189,190). The World Bank decided to provide safe burials for
highlighted the insufficient supply everyone who died. Liberia also
of food and other necessities to instituted cremation (195).
some quarantined individuals • This required huge resources
(191). In some cases, families broke (burial teams, vehicles and
quarantine in order to buy food personal protective equipment),
(192). coordination (with swab teams,
laboratories, contact tracers) and
Contact tracing planning (graves marked and
• The identification and follow-up families informed).
of persons who may have had • The deployment of burial
contact with an infected person teams and the engagement
(193). All potential contacts of communities to ensure safe
of suspected, probable and burials lead to a reduction in
confirmed Ebola cases need to unsafe burials and potential
be systematically identified and transmission.
put under observation for 21 days
(the maximum incubation period Social mobilisation and community
of the Ebola virus) (193). Efficient engagement
tracing required a list of contacts • Supporting communities to
and their location. In Sierra Leone identify and implement behaviour
only 20-30% of the contacts in the change to keep them and their
Ministry of Health’s database were communities safe was key.
usable, others were too vague for • Encourage people to come
outsiders to identify (194). forward if they were sick.
• Many people do not have Patients and families needed the
permanent addresses. There was confidence to know that they
opposition to some of the tracers would be cared for.
(194).
Expansion of treatment infrastructure
Travel restrictions • Care needed to be effective,
• Governments of the most to create high survival rates,
affected countries imposed and safe, so that Ebola was not
travel restrictions with the aim of transmitted to health workers.
preventing the spread of Ebola
201.2.1 NATIONAL RESPONSE
Guinea, Liberia and Sierra Leone had “We believe a decentralised
declared the Ebola virus disease epidemic response is going to be critical
as a national health emergency by mid- to get us to zero in the shortest
August 2014 and established National possible time.”
Task Forces. The respective National
Ebola Outbreak Response Plans were Liberia and Guinea set up similar
subsequently developed; the aims of decentralised national structures but
which were collectively agreed at the the information flows and local-level
WHO Accra Ministerial meeting in July structures varied among the countries
2014 (28): (30). An example of this decentralised
coordination can be seen in figure 3,
1. Ensure effective coordination of the which shows the social mobilisation
outbreak response activities at all pillars and sub-committees developed in
levels. Sierra Leone, Guinea and Liberia during
2. Strengthen early detection, the outbreak.
investigation, reporting, active
surveillance, and diagnostic capacity. The enormity of the required response to
3. Institute prompt and effective case Ebola meant the governments of Guinea,
management and psychosocial Liberia and Sierra Leone quickly called
support while protecting the health for an international response effort.
of health-care workers involved. Foreign Minister Samaur W. Kamara of
4. Create public awareness about Ebola, Sierra Leone in September 2014 said (31):
the risk factors for its transmission
as well as the factors that do not
“Based on the knowledge we had,
entail any risk, and its prevention and
control among the people.
based on the advice we were given
by our international partners, we
A key component of the national mobilised to meet this unfamiliar
response was to set up, with threat. But the staff, equipment,
international support, coordinating medicines and systems we had
mechanisms to contain the spread of the were inadequate and this slowed
disease. our effective response.”
In Sierra Leone, the Government created
a National Ebola Response Centre (NERC)
that, together with the United Nations
Mission for Ebola Emergency Response
(UNMEER), served as a command and
control structure for many partners in
the Ebola response. The NERC oversaw
15 District Ebola Response Centres
(DERCs) with a feedback loop between
the NERC and the DERCs. These DERCs
also coordinated with the district health
management teams for technical aspects
of the response, and were joined by
national and international partners.
According to Stephen Gaojia (29), Sierra
Leone Incident Manager for Ebola:
21Figure 3: Social Mobilisation pillars and sub-committees developed in Guinea, Liberia,
and Sierra Leone: a example of decentralised coordination in the Ebola response (30).
Liberia’s Social Mobilization Pillar
National-Level Coordination Structure for EVD Response (Current)
Chair: Health Promotion Division MOHSW
Co-Chair: UNICEF
MOH + WHO + MOH + Liberia +
MOH + CDC MOH + UNICEF
Crusaders for Peace CSOs + RBHS MOH + JHU/CCP
Media Support and Message and Materials Interpersonal
Mobilization and Research, M&E
Documentation Development Communication
Field Support Training
Sierra Leone’s Social Mobilization Pillar*
National Emergency Management System (Ebola)
Social Mobilization
Chair: MOHS HED
District SM Co-Chair: UNICEF
EOC Liaison Working Groups
Committees
Western (Urban) National Pillar Committee
(Coordination, Monitoring and Media Group
Western (Rural) Evaluation): HED, UNICEF,
Bo Sub-committee Chairs
Faith Based
Bombali
Organization Group
Bonthe
National Sub-Committees Youth and Adolescent
Kailahun
Kambia Group
Kenema C at Household-Level
Sub-Committees 1:
Koinadugu Capacity Building Group
Kono
Sub-Committees 2: Messaging IPC with Healthcare
Monyamba
and Dissemination Workers Group
Port Loko
Pujehun Special Needs Group
Sub-Committees 3: Special Needs
Tonkolili (same as subcommittee 5)
Guinea’s Social Mobilization Pillar
National
Coordination
Against Ebola
Surveillance Communications Patient Care Sanitation Research
Rumor Public Social Prevention
Management Relations Mobilization Communications
221.2.1 INTERNATIONAL RESPONSE
Figure 4: United States $ 1,955M By 14th October 2015, the international
Pledged World Bank Group $ 1,618M community (over 50 nations and many
contribution European Commission $ 955M donor organisations) had mobilised over
United Kingdom $ 687M
of funding $8.2bn USD to finance the Ebola response
African Development Bank $ 525M
to Ebola International Monetary Fund $ 394M
(32). The top five highest contributing
response Germany $ 281M donors included the US which gave $2.1bn
by donor France $ 265M USD, the UK $687m USD, the World Bank
(25 highest Japan $ 173M $1.6bn USD, the European Commission
China $ 129M
contributors) $955m USD and the African Development
Paul Allen Foundation $ 100M
(USD)(196) Canada $ 100M
Bank $525m USD (33) (see figure 4).
Netherlands $ 83M
Sweden $ 81M It is difficult to estimate how many
Norway $ 63M health workers were involved in the
Russian Federation $ 55M
response. The World Bank and the
Bill & Melinda Gates Foundation $ 54M
Belgium $ 51M
African Development Bank estimate that
Australia $ 38M more than 39,000 health workers took
Saudia Arabia $ 35M part alongside equally large numbers of
Denmark $ 32M surveillance and community mobilisation
$ 29M
Special Relief Fund
staff (34). Thousands of response workers
Mark Zuckerberg & Priscila Chan $ 25M
$ 16M
were trained, including 4,500 frontline
Islamic Development Bank
Finland $ 13M workers at the Institutional Organisation
for Migration’s (IOM) National Ebola
Training Academy in Sierra Leone. In April
Table 1: Allocation of funds (%) 2015, the World Bank estimated that
allocation more than 1300 foreign medical personnel
of disbursed Country Guinea 13%
were taking part including more than 850
funds by Sierra Leone 20% volunteers from other African countries
country, (through the African Union Support to the
Ebola-affected country
recipient (not specified)
28%
Ebola Outbreak in West Africa (ASEOWA).
category, and Approximately 1,000 WHO and nearly
Liberia 31%
purpose (36) 200 UNMEER personnel supported these
Other country 1% health workers mainly in logistic and
Unspecified 7% coordination roles.
Affected countries
Recipient 33% This was a considerable mobilisation of
(Multi-lateral)
Affected countries resources but there has been widespread
14%
(Bilateral) criticism of the time lag between the
International NGOs 12% outbreak and the response. Six months
International into the crisis, only 30 medical response
23%
Organisations teams were on the ground. Most of the
Research institutions, health workers and support teams and
31%
Regional & local NGOs
the financial and equipment/facility
Other recipients 13% investment arrived mid-way through the
Purpose Response 71% crisis (35). Table 1 shows the allocation
of funding ($6.6bn USD) from 46
Recovery 9% contributing partners between September
Research and
4% 2014 and May 2015 as reported by
Development
UNMEER, stratified by country, recipient
Other 16% type and purpose.
231.2.3 THE UK’S ROLE IN THE EBOLA RESPONSE
With its 450-year connection to Sierra Njala University and collaborations such
Leone, the UK government took the lead, as the King’s College Hospital Sierra
committing over £427m to support the Leone Partnership. Table 2 shows some
battle against Ebola. Its links included of the key projects in the UK Ebola
Sierra Leoneans working for DFID, links response.
to NGOs, an existing partnership with
1.2.3.1 MEDICAL AND TECHNICAL SUPPORT
DFID funded the construction of equip communities with the knowledge
6 treatment centres, around 200 and tools to tackle Ebola. Their review,
community care units and supported ‘Reducing Transmission of Ebola in Sierra
over 1,400 treatment and isolation beds Leone Through Changing Behaviours
- more than half the beds available for and Practices’ reports an increase in
Ebola patients in Sierra Leone (37). In community knowledge of Ebola from
addition to this, DFID focused much of 39% to 69%, reduction in stigma from
its resource allocation on improving 94% to 41% and an average of 97%
safe burials, supporting a total of 140 of burials being classified as safe and
burial teams, and expanding social dignified medical burials (38).
mobilisation efforts to educate and
Table 2:
Project Title Budget Start Date
Summary of
projects in Emergency Support to Respond to the Ebola £79.41m Jul-14
the UK Ebola Virus Disease in 2014 (Urgent Needs)
response
Sierra Leone Kerry Town Ebola Treatment Facility £89.10m Sep-14
Ebola Treatment Centres in Sierra Leone £45.90m Oct-14
Reducing Transmission of Ebola in Sierra Leone £12.55m Oct-14
Through Changing Behaviours and Practices
Ebola Care Units in Sierra Leone £43.40m Oct-14
UK Response to Ebola Crisis Through Support for £22.13m Oct-14
UNMEER and the Wider UN System
UK Support to Ebola Crisis Through Support for £33.44m Oct-14
the Joint Inter Agency Task Force (JIATF)
UK Response to Ebola Crisis Through Establishing £12.15m Nov-14
Laboratories
Ebola Central Health Care Supply Chain Platform £7.20m Nov-14
Match Funding for Ebola Response £6.20m Dec-14
Regional Preparedness £19.20m Jan-15
Transition from Ebola Response to Early Recovery £54.0m Mar-15
Ebola Vaccines Insurance £1.10m Apr-15
24These projects faced many challenges. deployed over 100 staff to run three new
One such challenge was deciding where laboratories in Sierra Leone. This reduced
to prioritise the resource allocation. the turnaround time for samples from 4-5
High risk groups included communities days to less than 24 hours (39). However,
geographically related to others with problems with backfilling in the NHS
known Ebola cases; communities with prevented more staff contributing.
attitudes and practices known to increase There were reports that more than ten
Ebola transmission risk; as well as times as many staff volunteered as were
vulnerable or marginalised groups, such able to go to Sierra Leone (39,40). Some
as women and young people (38). DFID have argued that the UK’s West African
also faces the challenge of ensuring that diaspora healthcare professionals could
the use of donor contributions and other have been utilised further, especially
forms of received capital are verified, considering their unique position to
especially as programmes draw to a close. shape culturally appropriate and socially
Nonetheless, the primary challenge DFID legitimate response programmes (41)
faces in terms of funding resources is (see box 3).
a temporal one: whether to prioritise
short-term or long-term interests. The IDC has recommended in its recent
Unpredictable spikes in the demand for report on the Ebola response that DFID
resources to tackle health emergencies, fund a formal structure to facilitate more
make it more difficult for DFID to volunteering by NHS staff (40). However,
adequately fund the more sustainable, as highlighted by Health Poverty Action,
longer term goals necessary for health sending large Western teams of health
systems strengthening (38). workers has questionable benefit
when compared to the long-term
The UK also provided human resources strengthening of local health systems
through NHS volunteers. Over 150 (42,43).
NHS Staff travelled to Sierra Leone,
with salaries covered by the NHS and
Public Health England and in addition
1.2.3.2 LOGISTICAL SUPPORT
The UK provided emergency food, for children. DFID also funded health
equipment, and logistical support promotion radio programmes in eight
to the Sierra Leonean government’s local languages, in part through working
Ebola response. It also financed Small with BBC Media Action (44).
and Medium Enterprises (SMEs), and
psychosocial and social protection
251.2.3.3 RESEARCH
The UK has also been at the forefront of response and recovery programmes.
academic research into Ebola including DFID co-funds vital research on Ebola,
epidemiological, anthropological, including clinical trials which have led to
social and economic research critical to the development of promising vaccine
understanding the underlying causes candidates (6,45).
of the Ebola outbreak and informing
Box 3: Examples of UK’s African Diaspora The wider role of the African Diaspora
The UK’s involvement in the Ebola Response: in African development:
African • Sierra Leone UK Diaspora Ebola • Remittances to Africa outweigh
diaspora in Taskforce (SLUKDET) has been Western Aid to the continent,
the Ebola involved in negotiations with accounting for an average of 5
response Public Health England, the NHS per cent of GDP and 27 per cent of
and health and DfID to recruit volunteers. exports (197,198).
systems They also delivered cultural • Members of the African diaspora
strengthening awareness training to NHS and have contributed significant
international volunteers prior to financial capital to African
their deployment (172). countries in investment capital
• SLWT have worked with local and the purchase of goods and
grassroots organisations to services from the continent (175).
provide protective raincoats to • Many professionals from
750 commercial motorbike riders, the diaspora temporarily or
as well as PPE and hand-washing permanently return to their
facilities and protective raincoats country of origin. This brain
(173). circulation and return migration
• EngAyde has provided protection strengthens knowledge
and care for Ebola children and production in African countries
psycho-social support for Ebola (177).
affected families and local health
care workers (174).
261.2.3.4 RESTRICTIONS ON TRAVEL
The UK government and 39 other nations and could consequently increase the
restricted direct flights to the region and uncontrolled migration of people from
quarantined all returning health workers. affected countries, raising the risk of
These measures have been described as international spread of Ebola”(48). Fears
disproportionate and without scientific of such an overreaction contributed to
justification and may have deterred the WHO’s decision to delay putting out
other international health workers an international alert.
(46,47). The WHO raised concerns that
they could “cause economic hardship,
1.3 UNDERLYING CHALLENGES: HEALTH
SYSTEMS AND INFRASTRUCTURE
The Ebola outbreak in West Africa reconstruction efforts. This legacy
was centered on a region with a of conflict and shortcomings in the
shared recent history of weak health reconstruction efforts are key to
systems, transnational civil war and understanding many of the weaknesses
internationally led post-conflict exposed by the outbreak.
“The health system became seriously exposed
by Ebola, because when it came it killed a lot
of health workers and community people …the
basic principles of prevention and hygiene were
lacking.”
Samuel Borbor Vandi, NGO worker
(Kailahun District, Sierra Leone)
271.3.1 HEALTH SYSTEMS IN GUINEA, LIBERIA
AND SIERRA LEONE
Some health systems in West Africa, particularly by providing services for
such as those in Nigeria and Senegal, child and maternal health and HIV/AIDS.
have the capacity to control Ebola However, crucial problems in the health
epidemics (49,50). Sierra Leone, Guinea systems of these three countries were re-
and Liberia have all made some progress exposed by the Ebola epidemic (50–53).
in strengthening their health systems,
1.3.1.1 GAPS IN HEALTH FINANCING AND GOVERNANCE
The WHO’s estimate of minimum in Guinea and Liberia between 2006
spending to provide basic lifesaving and 2012. However, spending is still
health services per person per year is well below what is needed to fund a
$44 USD (54). The governments of all functioning health system. The resulting
three Ebola-affected countries spend gap in funds for essential services is
significantly less than this, as shown manifested in out-of-pocket expenditure.
in table 3. All three countries receive Sierra Leone and Guinea have more
aid for health from donor countries than triple the WHO recommended
and agencies, however much of the proportion of spending on health by out-
funds provided are for specific disease of-pocket expenditure (55). This makes
programmes, such as HIV/AIDS, malaria it more likely that poorer people will be
and TB (55,56). Spending on health pushed further into poverty as a result of
per person per year has increased in paying for their health needs.
the region and has more than doubled
Table 3: Health
GUINEA SIERRA LEONE LIBERIA
financing
figures (57) Expenditure per person $9 $16 $20
per year spent on health
(USD)
Estimated Proportion of 66% 76% 21%
total health funding from
out-of-pocket expenditure
Amount of External $46m $93m $89m
support for health per
annum (USD)
Strong governance is needed to enable highlighted the absence of accountability
effective health systems strengthening. mechanisms and conflicting policies. The
In all three Ebola-affected countries, trickle down effects of delayed decisions
there have been attempts at health at national level are key barriers to the
systems reform, such as the notable Free development of health systems in all
Health Care Initiative in Sierra Leone. three countries (58–60).
Governance experts, however, have
281.3.1.2 CHRONIC SHORTAGE OF HEALTH WORKERS
Strong governance is needed to enable highlighted the absence of accountability
effective health systems strengthening. mechanisms and conflicting policies. The
In all three Ebola-affected countries, trickle down effects of delayed decisions
there have been attempts at health at national level are key barriers to the
systems reform, such as the notable Free development of health systems in all
Health Care Initiative in Sierra Leone. three countries (58–60).
Governance experts, however, have
Box 4: Guinea Liberia
Health • 1 health worker per 1,597 people • 1 health worker per 3,472 people
workforce • 1 public health institute with • “Emergency Human Resources
prior to limited capacity Plan” (2007) designed to rebuild
the Ebola • $25 USD health expenditure per its health workforce and double
outbreak capita (4.7% of GDP) the number of nurses but had
(64,65) limited overall success
Sierra Leone • $44 USD health expenditure per
• 1 health worker per 5,319 people capita (10% of GDP)
• 10,917 nurses and midwifes in the
country
• $96 USD health expenditure per
capita (11.8% of GDP)
Health worker absenteeism is also a than 2% in 2014. A ReBUILD research
significant problem, particularly in rural consortium attributes this to the
or remote areas and with those who introduction of the Free Health Care
work in lower-level health facilities (66). Initiative (FHCI) in April 2010 which
However, national rates of absenteeism included fee exemptions for healthcare
are quite low in Sierra Leone – at less workers (67).
291.3.1.3 RESOURCES FOR HEALTH SERVICE DELIVERY: LACK OF
SUPPLY WILL KILL DEMAND
Compounding the human resource delivery, as summarised in Box 5. The
crisis is a lack of healthcare facilities. Ebola outbreak has revealed the inability
Community mobilisation is often of many communities to mobilise
fraught with geospatial complications in resources from both national and
disconnected urban slums (68) and vast international sources, such as medical
rural areas (69) hindering the efficient equipment, trained health workers, and
distribution of goods. supplies for quarantined Ebola victims
(40,42).
Sierra Leone, Guinea and Liberia have
all made some improvements to the
delivery of services in recent years. For “[We need] training and posting
example, the Free Health Care Initiative of qualified health staff, logistics
in Sierra Leone, mentioned in the support, construction and
previous section, removed user fees from rehabilitation of health facilities
public maternal and child health services.
(PHUs), and more drugs. It has to
However, Sierra Leone still has some of
the highest rates of maternal and child
do a lot with resources.”
deaths worldwide and the health system
Dr Tom Sesay, Acting District Medical
still fails to deliver most of the WHO’s
Officer (Port Loko District, Sierra Leone).
‘building blocks’ of good health service
Box 5: • Comprehensive: A comprehensive • Person-centred: Services are
Characteristics range of health services is organised around the person, not
of good provided, appropriate to the the disease or the financing.
health service needs of the target population. • Coordinated: Across types of
delivery, • Accessible: Services are directly provider, types of care, levels
adapted from and permanently accessible of service delivery, and for
WHO building with no undue barriers of cost, both routine and emergency
blocks (70). language, culture, or geography. preparedness.
• Continuous: Service delivery across • Efficient: To achieve the core
the network of services, health elements described above with a
conditions and levels of care. minimum wastage of resources.
• High quality: Services are effective,
safe, centred on patient’s needs.
30Poor service delivery has been a services, the attempts to carry sick people
significant challenge to community for miles on stretchers and the desperate
mobilisation and community-led lack of medicinal drugs. The Ebola
efforts in the Ebola response. It is well Response Anthropology Platform (ERAP)
documented that in Sierra Leone the suggested that provision of a “solidarity
inability of health institutions to keep kit” to quarantined patients – including
up with the demand for Ebola treatment a charged phone, mobile credit, and
led to patients seeking out understaffed food – could mitigate the isolating
community health clinics not integrated consequences of quarantine (75).
into to the broader health system.
The sparse healthcare available
Lack of resources is not a purely was underscored by fragile physical
economic issue. When clinicians or infrastructure, according to evidence
technology are missing because of submitted by The Malaria Consortium
inadequate ancillary health services (76). An adequate level of general
(71,72), trust in health services is eroded. infrastructure is essential for the effective
In an extreme example, in Nimba county coordination of public health strategies.
and Bomi county, Liberia, families in For example, an outreach campaign is
some communities were boarded up unlikely to be successful when schools
in their homes without food or water are closed, households have little access
because there was no medical care or to the media, literacy levels are low and
isolation facilities (73). This fostered there are not enough clinicians to convey
fear, resentment and stigmatisation in a particular message (77,49,78,79). The
the affected communities, presenting success of community mobilisation
patients with what felt like a death efforts is crucially dependent on
sentence. Similarly, the lack of consistent adequate resourcing and the continued
food delivery to quarantined patients in development of infrastructure.
Monrovia resulted in feeling of exclusion
from their communities (74). Many of
the rural responses in our interviews
described the absence of medical
“We talked to people in quarantined homes
and counselled them, because most people in
quarantined homes are heart broken.”
Mrs Mariatu Songo Kanu,
Religious Leader (Port Loko District, Sierra Leone).
31You can also read