Keep it simple: peristomal skin health, quality of life and wellbeing - EXPERT OPINION CONSENSUS DOCUMENT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

EXPERT OPINION CONSENSUS DOCUMENT
Keep it simple:
peristomal skin health, quality of life and wellbeing
Supported by
This article is reprinted from the British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus Document
BJN
Lead Project Manager: Camila Fronzo
Project Manager: Angela Shaw
Medical Writer: Liam Benison
Editor: Benjamin Wakefield
Design: Carolyn Allen
Publishing Director: Andrew Iafrati
Managing Director: Anthony Kerr
Published by: MA Healthcare Ltd, St Jude’s Church, Dulwich Road, London, SE24 0PB, UK
Tel: +44 (0)20 7501 6726. Web: www.markallengroup.com
© MA Healthcare Ltd 2021
All rights reserved. No reproduction, transmission or copying of this publication is allowed without written
permission. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any
form or by any means, mechanical, electronic, photocopying, recording, or otherwise, without the prior written
permission of MA Healthcare Ltd, or in accordance with the relevant copyright legislation.
Cover image: AdobeStock/geshas
© 2021 MA Healthcare Ltd
This supplement is supported by Hollister and Dansac
Suggested citation for this document:
Burch J, Marsden J, Boyles A, Martin N,Voegeli D, McDermott B, Maltby E. Keep it simple: peristomal skin health,
quality of life and wellbeing. Best practice consensus document on skin health. Br J Nurs. 2021; 30(6, Supp 1):1–24
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus Document
BJN
Contents
Introduction5 Using products appropriately13
Convex appliances
Optimising patient care6 Colostomy irrigation
Early education and intervention Stoma care accessories
Personalised care
Therapeutic relationships Making prescribing decisions15
Personalised prescriptions
Classifying skin conditions7 Off-label prescribing
Moisture-associated skin damage Patient advocacy
Medical adhesive-related skin injury
Other dermatological conditions Keeping a record of care16
Documentation
Understanding risk factors9 Photography
Surgical factors Terminology
Comorbidities and medications
Age and demographic factors Working with evidence18
Staying up to date
Assessing peristomal skin11 Quality of evidence
Assessment tools Research participation
Asking the right questions
Holistic care Improving stoma care nursing19
Professional education
Finding the right routine12 Ongoing appraisal
Cleaning the skin Recognition of specialist roles
Forming a seal
Changing the appliance Conclusion20
Jenny Marsden, Stoma Care Nurse, York
CONSENSUS PANEL Teaching Hospital NHS Foundation Trust
Jennie Burch (chair), Head of Gastrointestinal Nuria Martin, Tissue Viability Nurse, St
Nurse Education, St Mark’s Hospital, London North Mark’s Hospital, London North West University
© 2021 MA Healthcare Ltd
West University Healthcare NHS Foundation Trust Healthcare NHS Foundation Trust
Anna Boyles, Stoma Care Nurse, King’s Benjamin McDermott, Stoma Care Nurse,
College Hospital NHS Foundation Trust Salford Royal NHS Foundation Trust
Emma Maltby, Stoma Care Nurse, Hampshire David Voegeli, Professor of Nursing,
Hospitals NHS Foundation Trust University of Winchester
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus Document
BJN
© 2021 MA Healthcare Ltd
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
Keep it simple:
peristomal skin health,
quality of life and wellbeing
A
person living with a stoma (ostomate) 2006). A large international survey of 4235 ostomates in
can face many challenges, and one of 13 countries found that 73% had reported a PSC in the
the greatest is maintaining the integrity previous 6 months (Voegeli et al, 2020). Ostomates do
and health of the skin around the stoma not always recognise PSC or seek help for skin problems
(peristomal skin). Healthy peristomal is (Herlufsen et al, 2006; Erwin-Toth et al, 2012), which
best defined as intact skin that is like the skin elsewhere suggests the possibility that the true incidence of PSCs
on the abdomen and does not cause distress or impair the may be higher than reported by some studies.
ostomate’s quality of life (Williams, 2010), and it should also PSCs typically occur as a result of a variety of
be able to support an ostomy appliance with an effective seal. interconnected factors, including chemical irritation from
However, peristomal skin is vulnerable to damage, which the leakage of stomal effluent; physical damage provoked
can present with a combination of symptoms, including by applying and removing products and accessories; allergic
discolouration, irritation, inflammation, erosion, maceration reactions; and pre-existing or emerging comorbidities.
and/or ulceration, as well as the appearance of fissures or Consequently, an ostomate’s risk of developing a PSC is
papules. Damage to skin integrity can be difficult and time- also affected by a complex variety of factors, including their
consuming to heal and can pose serious risks to an ostomate’s type of stoma, body profile and comorbidities, alongside
general wellbeing and quality of life (Boyles and Hunt, their age and other demographic factors, as well as the
2016).The presence of these peristomal skin complications nature of their stoma-forming surgery, the time since that
(PSCs) can significantly complicate the process of adaptation operation and medications they are taking.
to life with a stoma. A PSC can make it more difficult It is the role of the specialist stoma care nurse (SCN)
to learn the physical maintenance techniques of stoma to help ostomates maintain healthy peristomal skin and INTRODUCTION
care, and it can exacerbate the considerable challenges of minimise the risk of PSCs. Peristomal skin health is among
psychological adjustment to a changed body image.These the most common reasons for ostomates to consult a
issues affect all aspects of an ostomate’s life, from activities health professional and one of the most important clinical
of daily living, work and leisure, to relations with family, objectives for SCNs. Members of the consensus panel
friends and sexual partners (Ang et al, 2013;Vonk-Klaassen estimated that about two-thirds of their clinical time is
et al, 2016; Hubbard et al, 2017). devoted to addressing PSCs. SCN support involves helping
Moreover, the product prescriptions and clinical ostomates select an appropriate pouching system for their
interventions required to manage PSCs represent a individual needs; this consists of a stoma appliance (more
substantial economic burden on healthcare finances, as has often referred to by ostomates as a bag or pouch), which
been demonstrated in a number of recent studies (Taneja is worn against the skin to collect and contain the stoma’s
et al, 2017; Colwell et al, 2018; Nichols, 2018; Nichols output, sometimes supported by additional accessories.
et al, 2019; Taneja et al, 2019; Salvadalena et al, 2020). SCNs also educate ostomates on correct use of their
Ostomates themselves may also be financially burdened pouching system and regular management of the stoma
by reduced productivity or the cost of products purchased to maintain healthy peristomal skin, as well as safe and
© 2021 MA Healthcare Ltd
off prescription, although more research is required to effective self-care should a PSC occur. If a complication
confirm this (Meisner et al, 2012). does occur, the SCN will help the ostomate identify
Estimates of the incidence of PSCs vary. In a study and resolve its causes, which may include adjusting their
of 202 Danish ostomates who had a stoma for a mean pouching system and updating their self-care skills, as well
of 8 years, 45% had experienced a PSC (Herlufsen et al, as providing a treatment plan to return the skin to health.
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
SCNs also have an important role as patient advocates, including activities of daily living; their relationships
using their expertise to promote the interests of ostomates with intimates, family, and friends; and their professional,
within the wider healthcare system and ensure that they social and leisure pursuits. The needs of someone who
have access to the most effective treatments and services. works might be different from those of a retired person.
This consensus document describes the fundamentals Someone who wants to pursue an active nightlife may
of peristomal skin care and outlines best practice in the have different requirements from someone with more
prevention, assessment and management of PSCs. It draws leisurely outdoor pursuits.
on published evidence and the clinical experience of a SCNs should use this information to guide all decisions
consensus panel to demonstrate how nurses at all levels of on prevention, assessment and treatment of PSCs. This is
experience can make the best use of their knowledge and especially important in selecting the right pouching routine
skills to support ostomates to maintain healthy peristomal from the wide choice of available products. Moreover,
skin, overcome challenges and improve their quality of life. empowering ostomates to try different products, after
demonstrating how they should be used correctly, can be
OPTIMISING PATIENT CARE an important part of finding the optimal pouching routine.
Early education and intervention An experienced SCN will often be able to anticipate
Ostomates do not always recognise signs of a PSC or may be the signs of future problems and events in the ostomate’s life
slow to report them, and many are known to tolerate PSCs that increase their risk of PSCs, such as diabetes, vascular
for long periods without seeking help (Herlufsen et al, 2006; disease, immunosuppression, cancer and chemotherapy.
Erwin-Toth et al, 2012).When a PSC is left untreated, the These events require proactive prevention strategies,
skin condition is likely to worsen, become more complicated working in collaboration with other health professionals
to heal and more seriously impair quality of life. involved in the ostomate’s care.
Therefore, SCNs need to educate ostomates
about PSCs from the outset, ideally in both pre- and Therapeutic relationships
postoperative patient education, as well as give ongoing Good long-term outcomes in stoma care require that SCNs
support throughout their life with a stoma.This education develop strong therapeutic relationships with the ostomates
should involve face-to-face discussions, as well as written they care for, and relationship-building is a core skill for
information online and in printed literature. It should nurses in this specialism. These relationships are facilitated
aim to teach ostomates to recognise the signs of skin by SCNs’ rare advantage of seeing their patients over many
deterioration and remind them that regular leaks and years, and they can be built through proven pathways of care,
PSCs are not normal. Ostomates should expect to be able including annual clinical reviews.They can involve setting
to achieve a secure seal and healthy peristomal skin. This out the aims of care, treatment goals and expected outcomes,
information should include guidance on when, why and which will give ostomates an informed understanding of
how to access specialist advice and assistance in the event their situation and motivate them with something to work
a complication develops. towards (LeBlanc et al, 2019).
Should a PSC be suspected, early assessment and In such a relationship, the SCN should have an
intervention from an SCN is essential. This should be as informed and evolving knowledge of the changing needs
early as possible to achieve optimal outcomes and prevent of the particular ostomate.This means understanding what
the skin deteriorating further and causing wider problems, is most meaningful for each ostomate in achieving a good
especially as the complex and multifactorial nature of PSCs quality of life. This understanding puts SCNs in a good
means that they can be difficult to resolve once they take position to provide ongoing education and advice, as
hold (Steinhagen et al, 2017). well as achieve concordance and optimal outcomes with
prescribing and product use.
Personalised care Therapeutic relationships need to be built on trust.
The care provided by an SCN should be personalised This means holding honest conversations with ostomates
to the individual needs of each ostomate. This means that discuss the risks of products and interventions not
© 2021 MA Healthcare Ltd
getting to know their clinical history, as well as their working and the SCN’s expectations of outcomes. The
personal priorities and preferences. Ostomates will have panel’s consensus was that SCNs are gatekeepers, and trust
different goals they want or need to achieve in their lives. is needed to encourage ostomates to be independent, while
Their experience and tolerance of discomfort will vary. also providing a safety net that they feel able to call on
A stoma will affect all aspects of life in different ways, for support when needed.
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
Peter Lamb
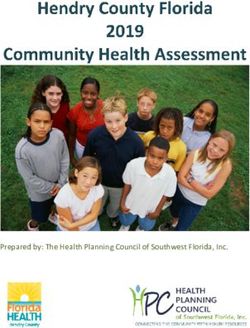
The skin comprises subcutaneous tissue, the dermis
and the epidermis. The outer layer of the epidermis
is the stratum corneum, which is constituted of
corneocytes and intercellular lipid (ceramide) layers.
The stratum corneum is coated by a film of dead skin
cells, sweat, keratin and lipids (sebum), known as the
acid mantle.
The pH of the acid mantle, normally 4–6, is one of
the most important regulators of skin function. It is
the first line of defence for the skin’s many protective
functions (Darlenski et al, 2011). The skin protects
the body against trauma, infection and excessive
fluids (Woo et al, 2017), and it is thought to have four
distinct barrier functions: microbiological, chemical,
physical and immunological (Eyerich et al, 2018).
The skin also functions to regulate the exchange
of substances between the body and the external
environment. This includes transepidermal water loss
(TEWL), the process by which moisture is evaporated
from the skin (O’Flynn, 2019). Each layer of the skin
is involved in absorbing, excreting, secreting and
thermoregulating; the corneocytes provide resistance,
while the lipid layers allow for substance exchange
(Darlenski et al, 2011).
Figure 1. Anatomy of the skin
CLASSIFYING SKIN CONDITIONS
Cheryl Thomas
PSCs can result from a wide variety of complex chemical,
physical and pathological processes. Each of these has its
own way of interacting with the anatomy of the skin
to cause breakdown in its integrity and damage to its
function (Figure 1). These aetiological factors are typically
interconnected and mutually reinforcing, and so PSCs are
usually classified according to which of these causative
factors appears to be predominant.This classification system
is imperfect, owing to the multifactorial nature of most
PSCs and variance in practice and terminology. However,
it is valuable, as highlighting the predominant cause of a
PSC will indicate the best way to treat it.
Moisture-associated skin damage
The most frequently diagnosed PSC is peristomal moisture-
associated skin damage (PMASD) (Figure 2). PMASD refers
to any PSC predominantly caused by prolonged exposure
of the skin to moisture, typically containing chemical
irritants.This moisture may comprise perspiration and/or Figure 2. Peristomal moisture-associated skin damage (PMASD)
© 2021 MA Healthcare Ltd
exudate (Voegeli, 2013), but PMASD is typically caused by
leakage of effluent (stool or urine) from the stoma onto the experienced leakage in the previous 6 months, and 91%
surrounding skin (Burch, 2014). The Ostomy Life Study were worried about it (Claessens et al, 2015).
of more than 4000 ostomates from 11 countries found PMASD typically results in maceration, irritation
that leakage was very common.Three quarters (76%) had (peristomal dermatitis) and/or breakdown of the peristomal
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
skin and erosion of the stoma’s mucocutaneous junction.
Peter Lamb
Peristomal dermatitis acquired its own code and definition
Harmful substances
unable to penetrate in the 11th revision of the International Classification of
Diseases (ICD-11) (World Health Organization, 2020),
and, for the first time, several types of MASD were classified
Stratum corneum and coded. Peristomal dermatitis (code EK02.23) is defined
(horny layer) as ‘Irritant contact dermatitis of skin surrounding stomas
or fistulas caused by prolonged or repeated contact with
Skin barrier gastrointestinal secretions, faeces, urine, pus, mucus or
(skin surface lipids) Moisture cleansing materials’. ICD-11 also classified for the first
time other forms of moisture-associated skin damage with
its own separate codes.
Normal skin barrier function Output from the small bowel contains many salts and
digestive enzymes (proteases and lipases) that thrive in an
alkaline environment, and effluent from an ileostomy has
Harmful substances a median pH of 7.2–7.4 (Fallingborg et al, 1990). This
penetrate stratum allows the effluent to disrupt the pH of the acid mantle,
corneum break down lipids and keratin and penetrate the stratum
corneum, initiating an inflammatory response and leading to
irritation (Figure 3).The process can also create an osmotic
pull, drawing more moisture, enzymes and salts into the
Reduced skin barrier skin and causing further disruption (Warner et al, 2003).
(loss of surface lipids) Moisture
PMASD is complicated by the cycle of skin damage.
Damage to peristomal skin increases the amount of
moisture on the stratum corneum, which makes it harder
to form a firm seal with the appliance. This increases the
Disrupted skin barrier function chance of leakage, which consequently exacerbates the
Figure 3. Disruption of stratum corneum and inflammatory response PSC (Woo et al, 2017).
caused by corrosive enzymes in stomal effluent
Medical adhesive-related skin injury
Cheryl Thomas
Peristomal medical-adhesive related skin injury (PMARSI)
refers to a PSC that is predominantly caused by mechanical
trauma related to use of an adhesive stoma product
(Figure 4) (Fumarola et al, 2020). A stoma appliance is
attached to the peristomal skin via an adhesive flange
(also known as a baseplate or skin barrier), and this is
sometimes secured with additional adhesive accessories.
PMARSI occurs when removal of the adhesive device
results in epidermal stripping (or skin tears), erythema,
erosion, blisters, vesicles and/or bullae (LeBlanc et al,
2019). When the outer layer of the stratum corneum is
more strongly bonded to the adhesive material than to
the layer below, removal of the adhesive will pull away
the outermost skin cells. PMARSI typically occurs when
appliance removal is traumatic, as a result of fragile skin,
© 2021 MA Healthcare Ltd
a strengthened adhesive or poor removal technique. It
is made more likely if the appliance is removed overly
frequently. PMARSI is largely avoidable with education
on good appliance removal technique, potentially assisted
Figure 4. Peristomal medical adhesive-related skin injury (PMARSI) with an adhesive remover.
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
Other dermatological conditions
Table 1. Peristomal skin complications by appearance and cause
As well as PMASD and PMARSI, peristomal skin can be
affected by a variety of dermatological conditions that are Complication Appearance Possible causes
not specific to stoma care (Table 1). For example, ostomates Moisture- Erythema, rash, Maceration from perspiration,
may develop eczema or psoriasis, which is characterised associated skin inflammation, exudate or stomal effluent
by inflammation and patches of scaly red skin. Other damage (PMASD) pruritus, papules, and/or chemical irritation from
PSCs include: plaques, scaling, enzymes in effluent
fissures
■ Pyoderma gangrenosum: Ostomates may also
experience pyoderma gangrenosum, which typically Medical adhesive Erythema, blisters, Skin stripping from traumatic
manifests as inflamed and painful ulcers with purple related skin skin tears or overly frequent appliance
injury (PMARSI) removal
edges. This relatively rare ulcerative inflammatory
skin disorder is associated with an inflammatory or Peristomal Inflammation, pain, Bacteria from surgical site,
proliferative systemic disease, such as inflammatory infection swelling, folliculitis stomal output or other source
bowel disease or cancer, and can be triggered by Allergic contact Inflammation, rash, Allergic reaction to ingredients
surgical or mechanical trauma (Lyon and Smith, dermatitis erythema, papules of skincare, hygiene or stoma
2010). Peristomal ulceration can be an outward sign products or topical medication
of a systemic condition. Granulation Lumpy lesions Infection, poor wound healing,
■ Peristomal infection: PSCs can result from (granulomas), Crohn’s disease or bowel
an infection, which may be bacterial, fungal or inflammation metaplasia
viral. It is likely to be a secondary infection of
Psoriasis Patches of Genetic disposition,
the surgical site or caused by bacteria in stomal scaly red skin, autoimmune issues, mechanical
output. These peristomal skin infections are inflammation stripping (Koebner reaction),
relatively uncommon, compared with PMASD inflammatory bowel disease
and PMARSI, and can be treated with antibiotics. Pyoderma Inflammation, Surgical or mechanical trauma
However, ostomates who present to their GP with gangrenosum extremely painful and systemic inflammatory
a PSC are sometimes incorrectly diagnosed with purple-edged ulcers disorders
an infection and prescribed antibiotics. It is only Sources: Oakley (2006); Lyon and Smith (2010); Nybaek and Jemec (2010); Blessy
when the antibiotics fail to resolve the condition et al (2019)
and the ostomate is referred to an SCN that the
diagnosis is corrected to PMASD or other stoma-
specific cause. To avoid unnecessary contributions UNDERSTANDING RISK FACTORS
to antibiotic resistance, SCNs should aim to An ostomate’s risk of developing a PSC depends on many
educate GPs on the common causes of PSCs, and factors that contribute to a more precarious peristomal
ostomates with a PSC should be encouraged to environment (Blessy et al, 2019; Salvadalena et al, 2020).
present to an SCN first where possible. If the SCN These are rarely isolated, and a PSC will typically be
does suspect a peristomal infection, this can be triggered by a combination of factors.
investigated with a swab; however, a swab is not
always possible in practice, and so diagnosis may Surgical factors
have to be made on assessment of the appearance People with an ileostomy (ileostomates) have a higher
of the skin and knowledge of the ostomate and risk of PSCs than those with a colostomy (colostomates)
their history. (Taneja et al, 2017). One study found that the incidence
■ Allergic contact dermatitis: PSCs can also result of PSC over 1 year was 57% for people with an ileostomy,
from an allergic reaction to a product. Ostomates 48% for a urostomy and 35% for a colostomy (Herlufsen
may have or go on to develop an allergy to the et al, 2006).Voegeli et al (2020) showed that people with
constituent materials of stoma appliances and an ileostomy were nearly twice as likely to develop a
© 2021 MA Healthcare Ltd
accessories, as well as those of any topical treatments PSC as those with a colostomy.This may be related to the
or other skincare, medical or hygiene products used consistency and volume of the stomal output.The output
on their skin, including soaps and washes. The more of an ileostomy is liquid or loose and high in volume, while
products an ostomate uses, the more likely they are that of a colostomy is likely to be of a formed consistency
to have a reaction. and lower in volume, and thus less prone to leakage.
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
The surgical formation of the stoma is an important PSC risk is affected by the general condition of the
factor in PSC development.A significant factor is whether ostomate’s skin. Conditions such as psoriasis, atopic
the stoma has been correctly sited by an SCN or surgeon, eczema, obesity and malnutrition, whether pre-existing
as has been highlighted by the Association of Stoma Care or developing after surgery, exacerbate vulnerability to
Nurses (ASCN) UK (2016). This requires the availability breakdown of skin integrity. Skin comorbidities, such
of an experienced SCN and is more difficult to achieve in as atopic eczema and psoriasis, are likely to present on
emergency surgery.An ostomate’s likelihood of experiencing peristomal skin because it is a site of trauma. Fissures in
a PSC if affected by the quality of the surgical construction the epidermis from xerosis, atopic eczema or other skin
of the stoma, particularly how well the stoma is spouted damage can also release excess moisture onto the skin
from the abdomen (Cottam and Richards, 2006; Koc et surface, increasing transepidermal water loss (TEWL) above
al, 2017; Steinhagen et al, 2017; Murken and Bleier, 2019). normal levels.They allow the penetration of proteases and
In addition, stomas are formed when ostomates are lying lipases from stomal effluent. Micro-organisms in the stomal
flat or tilted head down on the surgical table. Therefore, a effluent have the potential to cause infection in ostomates
stoma formed from bowel that is not under tension may who are immunocompromised as a result of diabetes,
appear to protrude sufficiently on the operating table but recent weight loss, cancer treatment, malnutrition or the
may pull inwards when the ostomate sits up. natural process of ageing (Oakley, 2006).
Although PSCs are an intermittent problem that can Many drugs can provoke dermal side effects, including
occur at any time while a person has a stoma (Meisner medicines for long-term conditions not directly related to
et al, 2012), they are particularly frequent in the period the stoma (Table 2). For example, nicorandil (Donaldson et
after stoma-forming surgery (Steinhagen et al, 2017). A al, 2009) can cause flushing and ulceration, and warfarin
retrospective cohort study by Taneja et al (2017) found that increases the risk of bleeding (Joint Formulary Committee,
one-third of ostomates had evidence of a PSC within 90 2020). Skin that is already fissured and fragile or subject to
days of surgery.Voegeli et al (2020) found that PSC risk irritation is therefore more vulnerable to further damage
was 1.5 times higher in the first 2 years compared with and breakdown in someone using these drugs. Metformin
people who had had their stoma for more than 2 years (Bouchoucha et al, 2011) commonly causes diarrhoea, as
(p=0.0002). Londono-Schimmer et al (1994) found that can warfarin (Joint Formulary Committee, 2020), and an
PSCs were more prevalent in the first 5 years following increase in loose faecal output poses a high risk of leakage
surgery than after.This is perhaps partly because these early and PSCs.Topical treatments used on the skin may cause
stages often see changes in the size of the stoma, the shape skin irritation or allergic reactions in some ostomates.
of the abdomen and the volume and consistency of the For example, topical steroids, including steroid inhalers
output, while these variables tend to stabilise over time. It prescribed off-label, risk thinning the skin. Ostomates may
may also be because it takes time for the new ostomate to
develop proficiency in self-care skills (Salvadalena, 2008).
Table 2. Dermal side effects of medications
Comorbidities and medications
Drug class Side effects
A high BMI is a risk factor for PSCs. Excessive subcutaneous
fat often results in undulating contours on the abdomen, Corticosteroids ■ Bruising
which make it more difficult to achieve an effective seal ■ Skin thinning
between the skin and appliance.Those who are overweight ■ Delayed healing
■ Fragile skin
or obese present a more difficult surgical environment
that makes it challenging to free enough bowel to make Anticoagulants (e.g. ■ Bruising
it through the adipose layer without being under tension, warfarin) ■ Prolonged bleeding
potentially resulting in a poorly spouted stoma (Cataldo et
Nicorandil ■ Ulceration
al, 2008; Beck, 2011; Salvadalena et al, 2020). More research
and guidance are required for ostomates with a high BMI. Chemotherapy ■ Rash
© 2021 MA Healthcare Ltd
Alterations in body profile, such as the development ■ Dry skin
of a parastomal hernia, can increase vulnerability to PSCs. ■ Delayed healing
■ Increased bleeding
Likewise, an ostomate may be more vulnerable to PSCs
■ Pruritus
if their stoma is flush with or recessed below, rather than
spouted from, the skin. Source: Boyles and Hunt (2016)
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
be prescribed medicines to treat skin problems, such as population, while the descendants of immigrants from the
infections, dermatitis or psoriasis. Usual care and caution Caribbean, Africa and South Asia are more susceptible to
are required to ensure that ostomates receive and use the long-term conditions (Evandrou et al, 2016). People with
right product and the right dose to treat the problem and poor English skills also experience relatively poorer health
that they understand the risk of side effects and relevant by comparison with the general population (Office for
interactions, as well as what to do if they occur. National Statistics, 2015). They find it more difficult to
Peristomal skin health can also be affected by access health services and express their care needs. Many
recreational drugs. This includes alcohol, which may also express concerns about the cultural and religious
interact with other drugs the ostomate is taking, cause appropriateness of services (Greenwood et al, 2015).Access
skin flushing and irritation and/or affect faecal and urinary to healthcare can also be impeded by discrimination on
output (Coleman, 2020). the basis of sex, sexual or gender identity and disabilities
(West et al, 2015). It can be assumed that ostomates who
Age and demographic factors face any of these health inequalities are likely to be more
Skin also changes with age (Haydont et al, 2019), suggesting vulnerable to PSCs (Cooper-Gamson, 2017; Nichols, 2018).
that the presentation of peristomal skin problems and the Therefore, SCNs should take particular care to ensure that
most suitable management will be different across the age such people receive an equal standard of care.
spectrum, from neonatal to older ostomates. Pittman et al Moreover, skin damage looks different across the
(2008) found that ostomates under 60 years experienced range of skin tones. Much of the evidence on PSC comes
more skin complications than ostomates over 80 years, from research on people with paler skin. Particular skin
but more research is needed to understand whether it pigmentations handle and respond to TEWL differently,
is changes in the skin, disease or other factors that are owing to variations in the structure and content of the skin
responsible for this observation. layers, and may respond differently to damage (Voegeli et
Best management of peristomal skin in neonates is al, 2015). In addition, observing for subtle changes in the
an under-researched area. The neonatal epidermis and skin, such as erythema, may be more difficult in people
stratum corneum are thinner and more fragile, with smaller with darker skin pigmentations. More research is needed
corneocytes in the first year of life (Blume-Peytavi et al, in this area to understand the full implications of these
2016). Clinical experience shows that the skin layers can differences for PSCs.
be easily separated by shearing forces, so adhesives must
be applied and removed with extreme caution. Moreover, ASSESSING PERISTOMAL SKIN
because newborns have a skin surface area-to-weight When an ostomate presents to an SCN, they should be
ratio about three-times greater than adults (Guzelian et assessed for the presence of a PSC. If their peristomal skin
al, 1992), infant skin will absorb more of a substance by is healthy, they can be assessed for risk factors for future
body weight than an equivalent patch of adult skin, making PSC development. If PSC symptoms are present, they
correct quantities challenging to calculate. In premature should be assessed for likely causes, which will determine
neonates with the most fragile skin, SCNs need to decide the most appropriate course of treatment.
which intervention is likely to cause the least damage: the
separation of the layers that comes from adhesive removal Assessment tools
(PMARSI) or the moisture damage from skin exposure The condition of peristomal skin and the severity of PSCs
to stomal output (PMASD). The best course will depend can be measured with some objectivity using a number
on each neonate at different points in their care (Global of tools. The Ostomy Skin Tool is a validated method to
Paediatric Stoma Nurses Advisory Board (GPSNAB), 2019). track changes in peristomal skin using standardised criteria
Data linking a variety of other demographic factors to for three domains: discolouration (D), erosion (E) and
variable health outcomes in the general population can tissue overgrowth (T) (Martins et al, 2010). Each domain
be extrapolated to ostomates (Blessy et al, 2019). Health is assigned two scores: one for the extent of skin affected,
inequalities are particularly associated with socio-economic scored 0–3, and one for severity, scored mild (0), moderate
© 2021 MA Healthcare Ltd
status, which restricts access to health services and financial (1) or severe (2). Both these scores are combined to give
resources and has a strong geographical correlation (Nazroo, the individual domains a score of 0–5, and all three domain
2003; The King’s Fund, 2020). This often overlaps with scores are combined to provide a total score of 0–15. Other
people from black and minority ethnic groups, who available tools include the Stoma Care Ostomy Research
generally have poorer general health than the rest of the Index (Williams et al, 2010) the Peristomal Lesion Scale
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
(Menin et al, 2019) and the Peristomal Skin Assessment However, these tools are subjective, and results may vary
Guide (Wound, Ostomy, and Continence Nurses Society by practitioner. Use of tools should only be supplementary to
(WOCN), 2020). a specialist’s experiential and evidence-based understanding
of the variety of complex chemical, physical and disease
factors that can precipitate PSCs. SCNs must acquire this
Box 1. Questions to determine causes of a peristomal knowledge of what to look for through a combination of
skin complication clinical experience, discussion of cases with colleagues and
Appearance reading of evidence, nurtured by habits of critical thinking
■ What is the extent and severity of discolouration? and reflective practice.
■ What is the extent and severity of erosion?
■ What is the extent and severity of tissue overgrowth? Asking the right questions
■ Are there any other distinct visual features on the skin? Example questions an SCN can ask to determine the
Potential causes likely causes of a peristomal skin complication are given
■ Has the ostomate experienced a recent leakage? in Box 1. These questions should cover patient history, as
■ What is the consistency of the stomal output? insufficient history is one of most common causes of clinical
■ Is there excessive moisture under the flange? misdiagnosis. Moreover, in the experience of the consensus
■ Is there discomfort or pain on appliance removal? panel, apparent skin signs, such as erythema or pain, may
■ Are there signs of bacterial, fungal or viral infection? prompt rapid assumptions or conclusions about the cause
■ Does the ostomate have any known allergies? of a PSC without consideration of factors that may be less
■ Has the abdomen been shaved in the past week? obvious or less well understood to the SCN. A medication
■ Does the ostomate have particularly fragile skin? review should be included, to inform the SCN of what has
Appliance leakage been previously prescribed so they can intervene to correct
■ How frequently has leakage occurred? regimens where necessary.
■ Is the abdominal area flat or contoured?
■ Is the stoma spouted or retracted, flush or prolapsed? Holistic care
■ How skilled is the ostomate at forming a seal? PSCs are often complex and multifactorial, and their causes
■ Are there visible leaks tracking along a crease in the flange? are usually not limited to the physical impact of regular
Clinical history appliance changes and management.Therefore, assessment
■ When did the skin condition occur? should be thorough and holistic, incorporating a full clinical
■ Were there any circumstances that might have triggered this? history and medication review, alongside assessment of stoma
■ What measures have already been taken to improve it? care regimen and technique, to consider the variety of factors
■ Is the stoma functioning differently to normal? that might also play a role in the ostomate’s skin condition.
■ How long has it been since the stoma-forming surgery? It is also important to consider the person’s social networks
■ What disease process or condition led to that operation? and access to support as part of an assessment (McMullen
■ What other health conditions does the ostomate have? et al, 2011). Those ostomates who have supportive friends
Product review and family, are better positioned and equipped to make
■ What stoma appliances and accessories are being used? the many transitions necessary to adapt to living with a
■ How long does the ostomate wear their appliance before changing? stoma. Health professional support also affects ostomates’
■ Is the template well-fitting? ability to become more skilled in changing appliances and
■ Is there disintegration of the flange? maintaining healthy skin, which can make the appliance
■ What is the rationale for any accessory use? less prone to leakage.
■ Have there been any recent changes in stoma care regimen?
■ Have these changes coincided with changes in skin condition?
FINDING THE RIGHT ROUTINE
Medication review Once an ostomate has undergone an assessment and been
■ What topical treatments and/or hygiene products are being used in the determined to have a PSC or risk of PSC development, they
© 2021 MA Healthcare Ltd
peristomal area? may benefit from education on good stoma care technique
■ What medications (prescribed or over the counter) are being taken?
and habits. Many problems can be prevented by appropriate
■ What recreational drugs (including alcohol) are being consumed?
cleaning of peristomal skin and correct technique in
■ Have there been any recent changes in medication?
changing the appliance, and these can be achieved through
■ Have these changes coincided with changes in skin condition?
good teaching of the ostomate by an SCN (Box 2).
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
Cleaning the skin
Box 2. How to avoid peristomal skin problems
Ideally, the skin should be cleaned with water only.
Alcohol wipes should not be used, as these risk irritation ■ Have the equipment available to formulate the template correctly
to the skin, while wet wipes should be avoided, because ■ Wash the skin with warm tap water
they contain moisturisers, such as lanolin, that prevent ■ Dry the skin gently but thoroughly
■ Formulate the template precisely to achieve a good fit
the appliance adhesive from reaching the skin layer
■ Ensure that the appliance is carefully placed and adhered around
sufficiently to ensure adherence (Mortz and Andersen,
the stoma
2008). Soap can be used to remove adhesive residue but
■ Educate the ostomate on prevention from the outset
must be carefully washed off the skin, because it contains ■ Know what risk factors to look out for
irritants that can damage the skin and trigger contact ■ Address problems as soon as they occur
dermatitis (Black, 2007; Voegeli et al, 2019; Fletcher et ■ Understand the rationale for correctly sizing the template
al, 2020; Lichterfeld-Kottner et al, 2020). After washing,
the skin must be thoroughly dried.
New ostomates should be encouraged to aim for a
Forming a seal consistent regimen of changes that are made around
A stoma appliance should be correctly fitted so that it the same time each day. Although this routine may
forms an effective seal around the stoma.This requires the occasionally be altered for special events, a consistent
template to be sized and shaped so that it sits close enough approach gives ostomates a greater sense of control over
around the stoma to avoid exposing the peristomal skin their lives. Regular appliance changes also provide more
to contact with effluent. However, the template should opportunities for the ostomates or SCN to inspect the
not be so tight that the stoma is constricted. A poorly skin and anticipate problems before they develop. As
fitting appliance increases the risk of damage to the ostomates gain experience and confidence, they will be
stoma or skin (Chandler and Lowther, 2012). This can better able to try different routines. Changing times should
be assisted with tools, such as the Fit Indicator Tool be determined to best suit their daily routines. For example,
(Hollister, 2020) or Peristomal Skin Assessment Guide an ostomate who plans to go out for the evening might
(WOCN, 2020); however, these are not validated and prefer to change before they do so, as a fresh appliance can
should only be used with caution and to supplement provide more confidence in a social setting, where access
critical clinical judgement. to bathrooms is more difficult than at home.
If an appliance leaks, it should be changed as soon as
possible. Leaks cause great distress to ostomates, as well USING PRODUCTS APPROPRIATELY
as damage to the skin. To prevent leaks and protect their peristomal skin,
ostomates need to use the right products to meet their
Changing the appliance individual needs, including the appliance that will provide
Stoma appliances need to be changed regularly, although the best fit and form the most effective seal with their
the actual and optimal frequency of changing varies skin.An appropriate appliance should avoid leaks and leave
depending on the individual’s anatomy, including type peristomal skin intact, without discomfort or distress. A
of stoma, bowel function and skin. As a broad guide number of manufacturers have recently produced stoma
and in line with Association of Stoma Care Nurses UK appliances with flanges that are infused with additives.
(ASCN) UK (2016) guidelines, the consensus panel SCNs should observe the emerging evidence on whether
recommends that: these additives have a significant positive impact on
■ Ileostomates use a drainable pouch, empty it as peristomal skin health.
necessary and change every other day (although
some change it daily) Convex appliances
■ Urostomates use a drainable appliance, typically Ostomates may find it difficult to form an effective seal
change every other day (or sometimes daily) and with a flat appliance if their stoma is situated below skin
© 2021 MA Healthcare Ltd
consider a night bag when sleeping level (retracted), at skin level (flush), excessively protruding
■ Colostomates use a closed appliance and change (prolapsed) or off-centre, or if they have an enterocutaneous
whenever their bowels function, up to a maximum fistula. When clinically necessary in order to avoid leaks
of around three changes per day, beyond which a and PSCs, a convex appliance may be indicated for these
drainable appliance should be considered. ostomates regardless of the length of time they have had
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
their stoma. An SCN should be able to anticipate those should not lead to the assumption that all accessories
who might require convexity, so this contingency can be in are optional or unnecessary. In many ostomates some
place should problems arise. However, convexity presents products, such as skin barriers, are absolutely essential
a risk of pressure damage, which may result in ulceration to maintaining a functional seal and healthy peristomal
and bruising, and therefore it should only be used under skin. However, the consensus panel agreed that accessory
the direction of an SCN (Hoeflok et al, 2017). These use can be inefficient, ineffective or liable to cause more
ostomates should be advised to be vigilant for problems and problems than it solves. Therefore, it is generally better
seek assistance from the SCN if any occur. SCNs should to keep the use of accessories simple and to a minimum,
understand the variations in appliance convexity and when, and the panel recommends that an accessory should only
for example, soft convexity might be more appropriate. be prescribed if it has been determined to be necessary
for the individual (Box 3). Moreover, ostomates must be
Colostomy irrigation taught correct and careful application of these accessories.
Some colostomates can use colostomy irrigation, which For example, if the skin has not been thoroughly dried,
involves instillation of water through the colostomy, where adhesive products can lock in moisture and make the skin
it stimulates the large bowel and causes it to empty. This more vulnerable to maceration.
provides control over bowel movements, and can achieve There are cases where stoma accessories can have a role
regular emptying of the colon, particularly if it is performed in improving the seal between appliance and skin, but they
at the same time each day.As a result, the ostomate generally should be only used when appropriate for the ostomate.
only needs to wear a small appliance, such as a cap or plug, Accessories should not be prescribed if the ostomate
and this can be worn for longer and more regular periods cannot use them because of dexterity issues. Products
between changes. Colostomy irrigation may also reduce used on the peristomal skin carry risks of disrupting the
the risk of leakage and consequent PSCs. Ostomates who pH of the acid mantle (Cressey et al, 2017), leaving a
find irrigation suitable report improvements in quality of residue that impedes the adherence of the appliance or
life (Carlsson et al, 2010; Kent et al, 2015). Ostomates may triggering an allergic reaction to the product itself, while
benefit from irrigation if they have an end colostomy, skin adhesive accessories that have to be pulled off increase the
problems and/or issues with bowel function. Irrigation risk of skin stripping and PMARSI (Grove et al, 2019;
is contraindicated in the presence of large parastomal LeBlanc et al, 2019). The more accessories are used, the
hernias or active bowel disease, such as Crohn’s disease, greater these risks become.
and consideration should be given to other health issues, ■ Fillers and seals: Fillers are pastes that can be
such as renal dysfunction (Colostomy UK, 2019).Where shaped into abdominal contours to provide a flat
appropriate, it is important that ostomates are offered surface for an appliance to adhere to, reducing
irrigation as an option, and that those who opt for to use the risk of leaks and PMASD. Meanwhile, seals
it are given good support to learn the technique. (sometimes referred to as washers, rings or discs)
are small adhesive circles that sit around the stoma,
Stoma care accessories helping form an effective seal with the appliance.
A stoma accessory is defined as any product designed to be Where possible, it is more cost-effective and time-
used in addition to a stoma appliance (NHS Supply Chain, efficient to create a seal with the optimal appliance
2018).The consensus panel emphasised that this definition alone. However, both fillers and seals can be useful
for those with especially challenging body profiles
marked by dips or creases or with a retracted or
Box 3. Less is more: questions to ask before using an accessory flush stoma. Some fillers contain alcohol, making
Before considering a range of accessories, it is necessary to ask: these inappropriate for damaged or infant skin,
■ Was the skin dried thoroughly after cleaning? although many recent products are alcohol-free
■ Has the appliance been applied correctly? (Boyles, 2010; GPSNAB, 2019).
■ Are there gaps between the appliance and the skin? ■ Adhesive removers: Adhesive remover wipes
© 2021 MA Healthcare Ltd
■ Does the patient have the dexterity to use any prescribed products? and sprays are designed to provide effective, pain-
■ Does the appliance need to be changed? If the appliance is well free adhesive removal without risking PMARSI.
adhered and there are no signs of leaks, could it be left another day and Silicone-based removers are recommended over
progress charted, to help prevent skin stripping, for example?
those with an oil or alcohol base (Boyles, 2010).
■ Would an accessory or a convex appliance work achieve a better seal?
They can be useful in certain cases and should be
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
prescribed for ostomates with evidence of PMARSI MAKING PRESCRIBING DECISIONS
or risk factors, such as fragile or damaged skin. The available selection of appliances and accessories
However, they should not be prescribed by default, is wide enough that ostomates should be able to find
as many ostomates will not need them. Adhesive something suitable for them. However, the range is so
removers do pose risks for PSCs, so the SCN wide that ostomates and GPs will typically require support
prescribing them should educate the ostomate on and advice from a specialist SCN to make an educated
correct technique (LeBlanc et al, 2019). choice on what works, what to avoid and why. Likewise,
■ Barrier films: Barrier wipes, creams and sprays the consensus panel recommends that non-specialist
create a film over the skin that acts as a barrier practitioners using stoma-related products should first
protecting it from contact with corrosive stomal discuss these with a specialist SCN.
output, thus reducing the risk of PMASD (Metcalf,
2018). This additional protective layer can increase Personalised prescriptions
appliance wear time for some ostomates, such as Prescribing decisions should be based on knowledge of
those with cystic fibrosis, whose skin is less able evidence regarding the products available and which work
to reabsorb excreted salt and can become oily better for particular skin conditions and the ostomate’s
(GPSNAB, 2019). However, the ADVOCATE trial needs. Decisions should always be informed by a
found that this protective film had the potential to comprehensive assessment undertaken by an SCN. This
impede the adhesion between the appliance and process should include a careful assessment of the dexterity
skin, particularly for ileostomates and urostomates, of the ostomate or carer who will take responsibility
and therefore updating the ostomate’s appliance for regular appliance and accessory change, because it
was usually a more effective solution in terms of is counterproductive to prescribe a product that the
cost, time and clinical outcome (Colwell et al, ostomate will not be able to use appropriately (LeBlanc
2018). Barrier films may mask an underlying PSC, et al, 2019). No product should be prescribed unless the
so, when considering a barrier, it is important to SCN knows the ostomate or carer is able to apply and
determine what is causing the complication and remove it correctly with minimal harm to the skin.
address it. Most ostomates will not require a barrier Before a product is to be prescribed, it is important
film; however they can offer valuable protection for to check the instructions for use about its risks. Nurses
those whose body profile or stoma shape makes it should resist the temptation to change approaches too
hard to form a seal that prevents stomal output from quickly. If a new product is tried, sufficient time should
reaching any part of the skin. be allowed for it to work and skin damage to heal before
■ Flange extenders: Flange extenders, including determining whether it has been effective or another
strips and tapes, are attached to the outer edge of product should be tried.
the appliance flange to extend its adhesive area and Prescribing should aim to provide the most appropriate
thus provide extra security. This can be helpful for products in the most appropriate quantity.This should be
ostomates whose body profile makes it difficult to based on careful assessment of what each individual needs
secure an appliance, such as those with a parastomal to perform their daily activities and realise their social
hernia (Black, 2016). Flange extenders can also be and professional goals. Some ostomates will require more
used to provide additional security and peace of expensive and/or a greater number of products than others.
mind on occasions where the risk of a leak is of Too many, too few or the wrong products can increase the
particular concern, such as at a swimming pool or risk of comorbidity, anxiety and/or PSCs, with associated
a party. However, in many cases, flange extenders costs for health and social care.The most clinically efficient
provide little benefit and are another thing to stoma care routine is typically the most cost-effective, as
be removed from the skin, increasing the risk of it will promote the ostomate’s health, quality of life and
PMARSI (LeBlanc et al, 2019). Flange extenders capacity to contribute to wider society.
should never be used to resolve leaks, because they
© 2021 MA Healthcare Ltd
do not treat the underlying issue and merely extend Off-label prescribing
the time the output takes to leak from the stoma Some products used to treat PSCs are used off-label,
to the edge of the adhesive area. This increases the meaning for a use that is not described in the product’s
time the effluent is in contact with the skin and thus license. Some ostomates seek out off-label products on
perpetuates the skin issue. the basis of their own research or recommendations from
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentBJN
friends or family. It is important for SCNs to initiate a stoma prescribing might be lacking in CCGs. For example,
discussion of ostomates’ use of such products to prevent in the British National Formulary, stoma care products are
them exacerbating skin damage. not given their own category and are instead listed under
A common example is Gaviscon liquid, which some wound care devices, although the Drug Tariff part 9 does
ostomates apply to the peristomal skin to soothe erythema group stoma products together. As a result, spending on
and pruritus, although there is no stronger evidence for this tissue viability items are sometimes inaccurately allocated
use other than anecdotes from SCNs and ostomates, which to stoma care.
have been shared in commercial patient literature and at Moreover, as the community prescribing spend on
conferences.Accessories with a pH-buffering technology stoma care is substantial, it is often a focus for cost-cutting.
can also be used for this purpose (Dansac, 2020).As another These cuts must be informed by an up-to-date knowledge
example of off-label prescribing, a corticosteroid inhaler of best practice. A collaborative discussion between the
is sometimes used topically to reduce a flare-up of an SCN and CCG medicines-management team can help
existing condition, such as eczema, on the peristomal ensure that the right products are available to prescribe
skin (Nicholson et al, 2014).Alternatively, a corticosteroid for ostomates and can be used cost-effectively. Savings on
lotion is applied instead of a cream or ointment for the waste can be redirected to enhancing patient pathways and
same purpose. If used correctly, corticosteroids can be very education. There is also guidance for stoma care nurses
effective at treating short-term problems, but they cannot on recommendations for product usage published by the
be used continuously, because their side effects include Patient Industry Professionals (PIPs) Forum (2014).
skin thinning, which will undermine the integrity of the
skin in the long term. KEEPING A RECORD OF CARE
Although off-label prescribing occurs for adult Documentation
ostomates, it is particularly common in neonatal and After each patient assessment, the SCN should make
paediatric ostomates.These products are often prescribed precise and detailed notes on the condition of the
by weighing up the risks and benefits. However, there peristomal skin, mentioning any evidence, protocols or
is insufficient evidence on neonatal skin’s absorption of tools used to make that assessment, with critical reflections
certain product ingredients, such as alcohol, and so some and observations from the SCN. It is also important to
SCNs may avoid using them. Summaries of product record any changes to pouching routine and product
characteristics provide little guidance. Off-label treatments use, including the precise date of and rationale for these
can be used with caution in ostomates who might benefit changes. Thorough documentation will record the
from them, but the SCN who prescribes a product off- ostomate’s progress over time.This allows the SCN to track
label is accountable and responsible for that decision. In whether the peristomal skin is healing or deteriorating,
such cases, SCNs should use their clinical judgement which can help identify possible causes of a PSC, review
and experience, as well as collaborate with medical, the efficacy of an intervention and decide whether a new
dermatology and tissue viability colleagues, where available. approach is needed.
This information can be used to develop a detailed
Patient advocacy and individualised care plan, which can be added to an
Prescribing is an area in which SCNs can exercise effective inpatient’s notes. Care plans can be shared with other health
patient advocacy. Financial pressures on health services have professionals working with the ostomate, for example,
led to cuts to and limits on prescribing budgets, which can emailed to community nurses or sent with a referral to
have serious consequences for ostomates’ quality of life and another hospital. Care plans can also be an opportunity
outcomes. Nurses can use their access to decision-makers to to educate less-experienced colleagues by explaining
advocate on behalf of ostomates’ interests.A greater patient the rationale for decisions, demonstrating good practice
voice in healthcare policy is also desirable—for example, and modelling correct techniques, such as how to size a
greater inclusion on NICE panels, patient partnerships in template around a stoma.
research and lobbying by patient groups. Documentation should be exact, thorough and updated
© 2021 MA Healthcare Ltd
Part of an SCN’s responsibility is to act in an advisory regularly. To aid communication, it is important that all
capacity at an organisational level. SCNs need to reach out terminology used is clear and consistent. Standards for
to clinical commissioning groups (CCGs) and inform the documentation are available from the Royal College
medicines-management teams about what products are of Nursing (2017) and Nursing and Midwifery
appropriate to stoma care. Knowledge of the specifics of Council (2018).
This article is reprinted from British Journal of Nursing, 2021, Vol 30, No 6, Supplement 1, Consensus DocumentYou can also read