Innovation roll out Valencia's experience with public-private integrated partnerships - Institute for ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Innovation roll out Valencia’s experience with public- private integrated partnerships Healthcare public-private partnerships series, No. 3
The Global Health Group Global Health Sciences University of California, San Francisco 550 16th Street, 3rd Floor San Francisco, CA 94158 USA Website: tiny.ucsf.edu/globalhealthgroup PwC 300 Madison Avenue New York, NY 10017 USA Website: www.pwc.com/global-health PwC Mexico Mariano Escobedo 573. Col. Rincón del Bosque México, D.F. 11580 México Website: www.pwc.com/mx/sector-salud Ordering information This publication is available for electronic download from the Global Health Group and PwC websites. Recommended citation Sosa Delgado-Pastor, V., Brashers, E., Foong, S., Montagu, D., Feachem, R. (2016). Innovation roll out: Valencia’s experience with public-private integrated partnerships. Healthcare public-private partnerships series, No. 3. San Francisco: The Global Health Group, Global Health Sciences, University of California, San Francisco and PwC. Produced in the United States of America. First Edition, December 2016. This is an open-access document distributed under the terms of the Creative Commons Attribution-Noncommercial License, which permits any noncommercial use, distribution, and reproduction in any medium, provided the original authors and source are credited. Images Cover photos provided courtesy of Ribera Salud, Marina Salud, Hospital de Manises.

Table of contents Acknowledgements .......................................................................................................................... 4 List of figures and tables .................................................................................................................. 5 UCSF/PwC report series on public-private partnerships .................................................................. 6 About the report series .............................................................................................................................................. 6 About public-private partnerships ........................................................................................................................... 6 Methodology ...............................................................................................................................................................7 Audience .....................................................................................................................................................................7 Executive summary .......................................................................................................................... 8 Spain – political organization and health system design ......................................................................................... 9 The La Ribera Hospital – innovative public-private collaboration in Valencia ...................................................... 9 Innovation roll out ................................................................................................................................................... 11 Highlights of the subsequent PPIP projects ............................................................................................................ 13 Improvements in efficiency ..................................................................................................................................... 14 Strengths and opportunities .................................................................................................................................... 16 Conclusion ................................................................................................................................................................ 17 Introduction .................................................................................................................................. 18 Country profile – Spanish health & economic context ........................................................................................... 19 Spanish National Health System fundamentals ..................................................................................................... 22 Types of public-private collaboration in healthcare ............................................................................................... 24 Valencia’s PPIP model ................................................................................................................... 25 The Valencia Community ........................................................................................................................................ 25 Innovation in Valencia ............................................................................................................................................ 26 Key features of the new model ................................................................................................................................ 32 Innovation roll out – replicating the model ........................................................................................................... 48 PPIPs in Madrid ............................................................................................................................. 60 Lessons learned ............................................................................................................................. 63 Recommendations ......................................................................................................................... 67 Conclusion ..................................................................................................................................... 70 References ......................................................................................................................................71 About the authors .......................................................................................................................... 73 About the UCSF Global Health Group.................................................................................................................... 73 About PwC ............................................................................................................................................................... 73

Acknowledgements
The authors are grateful for the expertise and experience so generously shared
during the development of this report. While this report was prepared by the
UCSF Global Health Group and PwC, information and insights contained in the
report were provided by the following individuals and organizations:
• Dr. Carlos Alberto Arenas
• Dr. Alfonso Bataller Vicent
• Dr. Antonio Burgueño Carbonell
• Dr. Luis Fidel Campoy Domene
• Dr. Sergio García Vicente
• Sr. Eloy Jiménez Cantos
• Dénia Health Department
• Elche-Crevillent (Vinalopó) Health Department
• International Financial Corporation/The World Bank Group
• La Ribera Health Department
• Madrid Health Service
• Manises Health Department
• PwC Spain
• Ribera Salud
• Spanish Society for Health Directors
• Torrevieja Health Department
• Valencia Health Agency
4 Innovation roll out: Valencia’s experience with public-private integrated partnerships
List of figures and tables
Figures
Figure 1: Map of Valencia Community health departments, including the five managed as PPIPs .......................... 8
Figure 2: La Ribera PPIP design and configuration, following the 2002-03 re-tender process ............................... 10
Figure 3: Timeline of the Valencia PPIP rollout ......................................................................................................... 12
Figure 4: Comparison of health expenditures per person in PPIP vs. publicly-managed health departments ........ 15
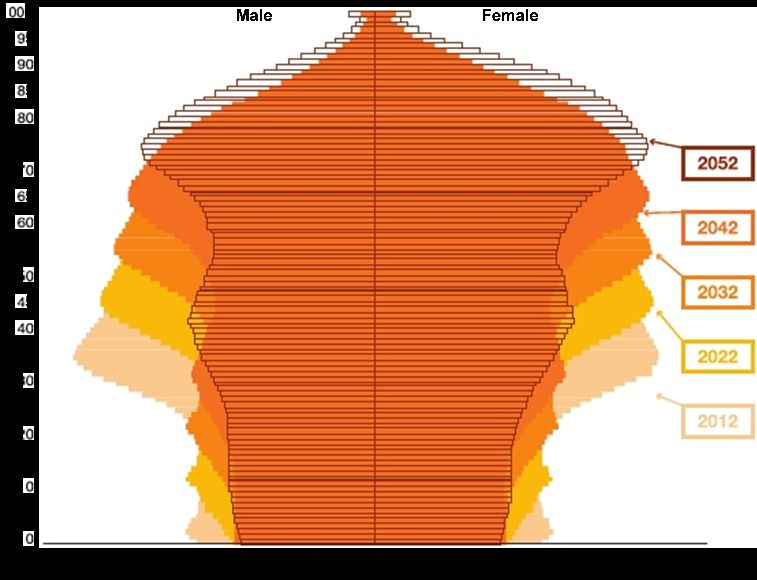
Figure 5: Demographic distribution in Spain, 2010-2050 ......................................................................................... 19
Figure 6: Changes in GDP and health spending in Spain since 2003 ........................................................................ 21
Figure 7: Organizational design of Spain’s National Health System ........................................................................ 23
Figure 8: Map of the 17 autonomous communities of Spain ..................................................................................... 25
Figure 9: (reprised): Map of Valencia Community health departments, including the five managed as PPIPs ..... 26
Figure 10: La Ribera PPIP design and configuration, 1997 vs. 2003 ........................................................................ 29
Figure 11: Collaboration mechanism within the new model ..................................................................................... 32
Figure 12: Valencia Community population and expenditure on healthcare – PPIP vs. publicly-managed
health departments ...................................................................................................................................37
Figure 13: Comparison of average per capita fees – PPIP vs. publicly-managed health departments, 2006-2011 . 38
Figure 14: La Ribera Health Department – overview of healthcare activity............................................................. 43
Figure 15: PPIP health departments – capitated payment analysis .......................................................................... 44
Figure 16: Outpatient pharmacy spending in Valencia ............................................................................................. 45
Figure 17: La Ribera Health Department human resources...................................................................................... 46
Figure 18: (reprised): Valencia PPIP model roll out.................................................................................................. 48
Figure 19: PPIP Health Department 22, Torrevieja – location, design and configuration ...................................... 49
Figure 20: PPIP Health Department 13, Dénia – location, design and configuration .............................................. 51
Figure 21: PPIP Health Department 23, L’Horta Manises – location, design and configuration ............................ 54
Figure 22: PPIP Health Department 24, Elche-Crevillent – location, design and configuration ............................ 56
Figure 23: Vinalopó Hospital – performance appraisal model ................................................................................. 58
Figure 24: Madrid PPIP model timeline ..................................................................................................................... 61
Tables
Table 1: Key features of the Valencia PPIPs ................................................................................................................ 14
Table 2: Valencia PPIP strengths and opportunities .................................................................................................. 16
Table 3: Spain summary statistics, 2015 (most recent available unless otherwise noted) ....................................... 20
Table 4: Most common forms of healthcare public-private collaboration in Spain ................................................. 24
Table 5: La Ribera Hospital and La Ribera Health Department PPIP concessions – comparison of RFP terms .... 31
Table 6: Summary of contracted risk and responsibility........................................................................................... 33
Table 7: Key players and roles under the PPIP model ............................................................................................... 35
Table 8: Committed and actual investments by PPIP health department ................................................................ 40
Table 9: Sample Valencia Community healthcare performance indicators .............................................................. 42
Table 10: Valencia Community PPIP hospital performance ..................................................................................... 42
Table 11: Snapshot of the PPIP health department roll out ...................................................................................... 48
Healthcare public-private partnerships series, No. 3 5
UCSF/PwC report series on public-private
partnerships
About the report series About public-private In the past three decades,
This report on public-private
partnerships governments from low-to high-
income countries have increasingly
integrated partnerships (PPIPs) in PPPs are a form of long-term
sought long-term partnerships with
Valencia, Spain is the third in a contract between a government and
the private sector to deliver services
series of publications on public- a private entity through which the
in sectors such as transportation,
private partnerships (PPPs) jointly government and private party
infrastructure and energy.
authored by the UCSF Global jointly invest in the provision of
Health Group and PwC. public services. PPPs are Healthcare partnerships have
distinguished from other emerged more cautiously, but have
This series aims to document and government private contracts by: rapidly expanded since the early
raise awareness of innovative PPP the long-term nature of the contract 2000s. The emerging partnerships
models in health globally, and to (typically 15+ years); the shared have tackled a range of healthcare
disseminate lessons learned to nature of the investment or asset system needs—from construction of
inform current and future contribution; and the transfer of facilities, to provision of medical
healthcare partnerships.
risk from the public to the equipment or supplies, to delivery
“Innovation roll out” explores the private sector. of healthcare services.
experience of the Valencia Under a PPP arrangement, the Most PPPs operate under a “DBOT”
Community of Spain, as it private sector takes on significant model (design, build, operate,
developed and expanded the PPIP financial, technical and operational transfer), under which the private
model to address the health needs risks and is held accountable for partner is responsible for
of its population in five health defined outcomes. PPPs provide maintaining the infrastructure
departments between 1997 and governments with alternative throughout the life of the contract.
2013. The report discusses the methods of financing, The private partner then transfers
successes and challenges infrastructure development and this responsibility back to the
encountered, and examines the service delivery. By making capital government upon expiration of the
range of innovations in patient investment more attractive to the contract. The private partner is
care, management practices, private sector, PPPs can reduce the responsible for operating the
performance management and use risk for private investment in new hospital, including services such as
of technology put in place to markets and ease barriers to entry. laundry and cafeteria. The
achieve financial efficiencies and
government retains responsibility
improved access to integrated
for the delivery of healthcare
health care for target populations.
service throughout. The most
Finally, the report explores several
common form of PPPs in health has
opportunities for both the public
been the private finance initiative
and private sectors, to optimize the
(PFI) model used to build many
success and sustainability of the
hospitals in the United Kingdom.1
model in the future.
6 Innovation roll out: Valencia’s experience with public-private integrated partnerships
Since the early 200s, an increasing Methodology Audience
number of governments have been
Study researchers conducted The primary audiences for this
exploring more ambitious models
qualitative interviews in Spain— report are the governments of low-
such as public-private integrated
mostly in the Valencia region— and middle-income countries
partnerships (PPIPs), under which
during September and October (LMICs), including policymakers in
the private partner is additionally
2013. Interviewees included: the ministries of health and finance,
responsible for delivering all
Government of Valencia (primarily who wish to consider PPPs and
clinical services at one or more
the Valencia Health Agency); key PPIPs as models for health system
health facilities, often including an
actors in the five PPIP health strengthening, as well as the wide
acute care hospital, as well as one
departments; employees from range of private sector actors who
or more primary care facilities. The
Ribera Salud; the Madrid Health seek to engage with government.
private partner designs, builds and
Agency and several insurance
operates the facilities, and delivers Lessons and findings may also be
companies involved in PPPs;
clinical care, including recruitment helpful to others studying how best
members of the Society of Spanish
and staffing of healthcare to leverage the private sector to
Health Directors; representatives of
professionals.1, 2 This model is strengthen health systems,
The World Bank Group/
commonly called the “DBOD” including donor agencies, non-
International Finance Corporation;
(design, build, operate, deliver) governmental organizations,
external advisors to the projects
model. academic institutions and private
and other key individuals with
relevant history and experience health entities.
with the Valencia PPIP projects.
The authors also reviewed grey and
peer-reviewed literature on PPPs
and PPIPs to inform the study.
Healthcare public-private partnerships series, No. 3 7
Executive summary In the late 1990s, the Valencia original project tender to address Valencia are less well known. The Community (an administrative lessons learned and adapting the authors hope that the information region) in Spain embarked on a original business model to address included in this report will provide new model for managing its evolving population, healthcare a useful reference for governments, hospitals, engaging with the private access and management needs in private actors and other policy sector to expand capacity and other facilities. makers who are considering PPPs improve quality and cost as a potential mechanism for effectiveness. Since then, the region The rich history of the La Ribera improving or expanding healthcare has continued to lead and innovate Hospital has been well documented services in their local, regional or in the public-private partnership over the last 15 years; the history of national contexts. (PPP) arena—renegotiating its the subsequent PPIP projects in Figure 1: Map of Valencia Community health departments, including the five managed as PPIPs Source: Generalitat Valenciana, Consellaria de Sanidad: Data Warehouse SIP, Sistema de Information Poblacional, November 2015: SIP Informe Mensual. http://chguv.san.gva.es/portal-de-transparencia/poblacion-atendida-e-informes-anuales, viewed on April 19, 2016 8 Innovation roll out: Valencia’s experience with public-private integrated partnerships
Spain – political of primary and specialty care for Construction of the new La Ribera
organization and health both outpatient and inpatient care— Hospital (also referred to as the
system design traditionally structured under Alzira Hospital) was tendered in
different functional divisions within 1997. A private consortium led by
Spain is a constitutional monarchy, the health department—was Adeslas and financing partner
with a hereditary monarch and a consolidated under the manager of
Ribera Salud was contracted to
parliament of two houses—the each health department.
design, finance, build, operate and
Cortes. Its 50 provinces are
maintain the hospital, and to deliver
organized administratively into 17 The La Ribera Hospital – specialized clinical care to an initial
autonomous (self-managed) innovative public-private population of 230,000 residents.4
communities and two autonomous collaboration in Valencia
cities, each with its own elected The La Ribera Hospital opened in
In 1986, following severe flooding of
authorities. Following major 1999, with an original contract term
the Jucar River that left a large
reforms in the 1980s, the Spanish of 10 years and financing based on a
portion of the local population
National Health System was per capita payment of 204 euros.
without access to healthcare, the
decentralized, with each Although a much more conservative
Valencia Community Ministry of
community’s Ministry of Health arrangement than the private
Health decided to build a new
taking on responsibility for consortium had expected, it was the
regional hospital in the city of Alzira.
healthcare delivery for its maximum that the government
Under the innovative leadership of
population. Each Ministry of Health would approve at the time.
the Health Minister and the leader
is responsible for selecting and After three years of operation, the
of Adeslas, a leading Spanish health
employing its preferred delivery parties agreed to adjust the contract
insurer, the Community embarked
model(s); the central government to address several critical
on a new vision, of opening the new
sets overarching policy and provides sustainability issues. Key design
hospital through a public-private
inter-regional coordination. changes included incorporating
partnership. This new vision went
beyond the typical model of primary care services from other
In the Valencia Community, located
engaging the private sector to simply parts of the health department into
on the east coast of Spain, health
finance and construct a new the PPIP to help manage patient
services are organized under 24
hospital, and instead contracted the demand and referrals, and making
distinct “health departments,”
private partner to also manage and improvements in infrastructure
which were established in 1982
deliver clinical services in the new management. The changes also
(see Figure 1). Each health
hospital.1,2 Today this model is often resulted in an increase in the per
department is responsible for
referred to as a public-private capita fee to better finance the
providing comprehensive healthcare
integrated partnership, or PPIP. The expanded operations, and an
services, including inpatient,
goal of this new approach was to extension of the contract period to
primary and specialty care, for up to
leverage private sector expertise in 15 years (with an option to extend
250,000 residents. The health
hospital management and systems, to 20 years).
department also provides health
promotion, disease prevention and and use carefully designed payment
The project was re-tendered in 2002
social-health support.3 In 2003, the incentives and performance
with these updates; the Adeslas-
Valencia Health Agency management clauses in the
Ribera Salud consortium was again
implemented a further reform, contract to achieve improvements awarded the contract.
known as the “one-head” model, in efficiency, quality and access
under which management to care.1
Healthcare public-private partnerships series, No. 3 9Figure 2: La Ribera PPIP design and configuration, following the 2002-03 re-tender process Source: La Ribera Department of Health. Activity Report (2012) † In 2014 Centene Corporation acquired Bancaja’s 50% share in Ribera Salud In 2015 Ribera Salud acquired Adeslas’ 51% stake in UTE-Ribera II. The new shareholders of UTE-Ribera II are Ribera Salud (96%), Dragados (2%) and Lubasa (2%). 10 Innovation roll out: Valencia’s experience with public-private integrated partnerships
Money follows the patient
The Valencia PPIP model approach is based on the principle that “money follows the patient.” The private
provider is paid an annual fee based on the size and anticipated health conditions of the population to be
served; patients are then allowed to choose where they seek medical care.
The goal of the PPIP model is to achieve the same or better healthcare for 80% of the cost. Thus, if a patient
lives in a health department that is run as a PPIP, but chooses to seek care at another public hospital or facility,
the PPIP health department must pay the government facility 100% of the cost of the patient’s treatment.
However, if a patient lives in a publicly-managed health department and seeks care at a PPIP facility, the
government reimburses the PPIP facility for the patient’s care, but only at 80% of the cost. This approach was
developed to incentivize PPIP facilities to provide high quality services to attract and retain patients.
To foster patient engagement, each of the Valencia PPIPs implemented significant community outreach
campaigns to encourage the use of PPIP hospitals, and educate patients about the services offered.
Innovation roll out stability, which allowed the further expansion of the PPIP
Valencia government to issue new management model. Frequent
Building on the initial success of
tenders with confidence, and changes in government leadership,
the La Ribera project, the Valencia
double the population covered by followed by the economic crisis in
Ministry of Health decided to
PPIP healthcare services to 18% of 2008, ultimately halted new
replicate and innovate on the
the Valencia Community.5 funding for PPIPs after 2006.6
model, to address facility and
service delivery needs in other By laying out an expansive and
health departments. longer-term vision for In the 2015 Regional Elections,
implementing PPIPs across a series Spain’s Popular Party (Partido
Between 2002 and 2006 the Popular) lost its absolute
of projects, the Ministry was able to
Ministry issued four additional majority in Valencia after 20
promote greater private sector
PPIP tenders, each geared toward a years. As this report went to
engagement and increase
particular regional challenge or print, the new regional coalition
competition for the subsequent
circumstance (see Figure 3 and government announced that it
tenders.
Table 1). Three of the tenders were will not extend the La Ribera
for new hospitals; one involved the Broader implementation of the Health Department PPIP
replacement of an aging district PPIP model also required the contract when it ends in 2018.
hospital. In each case, the 2003 La government to develop additional It remains to be seen whether
Ribera Hospital contract was management skills and capacity the government will choose to
adopted as a blueprint, with to supervise and implement bring the Health Department
adjustments made for the different the contracts. back under public management,
patient care needs of each health or whether it will pursue a new
department’s population. Despite its initial popularity, contract with Ribera Salud or
however, many public entities other private parties.
This period was marked by within Valencia did not support
widespread European economic
Healthcare public-private partnerships series, No. 3 11Figure 3: Timeline of the Valencia PPIP rollout Source: UCSF/PwC Fellowship analysis 12 Innovation roll out: Valencia’s experience with public-private integrated partnerships
Highlights of the government district hospital personnel recruitment strategy.
subsequent PPIP projects into a PPIP hospital. A New talent management
challenge in Dénia was the approaches were employed,
• Torrevieja is Valencia’s
transition of existing hospital including the sharing of staff
primary tourist destination,
staff to the new PPIP. and schedules across the
with a population that almost
Following extended three facilities.
triples during the summer. To
meet this peak demand, the negotiations, a solution was • Vinalopó. Although the
Valencia Ministry of Health agreed to allow existing staff to Elche-Crevillent Health
issued the Torrevieja Hospital retain their government status, Department already had a
tender in 2002. Although while all new staff were hired general hospital, population
initially successful, the project by the private consortium. growth demanded additional
suffered from changes to its Through close negotiations and services. The Vinalopó PPIP
covered population: in 2007, perseverance, this approach Hospital opened in 2010, a few
the Valencia government largely succeeded. The PPIP blocks from the existing public
decided that only residents of also included a significant hospital. The close proximity of
the Torrevieja Health investment in information the two facilities opened up
Department could be counted technology (IT) infrastructure care choices for patients and
toward capitated payments; and systems to help motivated healthcare
services rendered for non- coordinate care. improvements through
residents had to be reimbursed • Manises is a suburb of competition.
under the “money follows the Valencia that experienced high By the time of the Elche-
patient” model where the home population growth in the early Crevillent/Vinalopó Hospital
municipality of the visitor 2000’s, with further projections tender, private sector
would reimburse the cost of of future growth. The region’s engagement had been
services to the Torrevieja suburban population also sufficiently stimulated that the
Health Department. suffered a high rate of complex project received multiple
• Dénia. Flanked by Valencia chronic conditions and had bidders. Key features of each
and Alicante, the two largest become accustomed to seeking PPIP are listed in Table 1.
cities in the Valencia treatment at the well-known La
Community, the Dénia Health Fe Hospital 10 miles away.
Department was supported by a The Manises PPIP Hospital was
small district hospital, tendered in 2006 to address
insufficient for its growing these challenges.
population and fluctuating In addition to building a new
tourist population. Residents hospital, the scope of the
with specialized treatment Manises PPIP contract was
needs were regularly referred expanded over time, to include
to hospitals in the larger building of a second general
nearby cities. hospital, a chronic disease
To address this gap, the hospital and a hospital
Valencia Ministry of Health specialty center with 21 medical
initiated a tender in 2004 to specialties. This expansion
expand and convert the existing required an aggressive
Healthcare public-private partnerships series, No. 3 13Table 1: Key features of the Valencia PPIPs
PPIP health La Ribera Torrevieja Dénia Manises Elche-Crevillent
department (Alzira) (Vinalopó)
Private partners* Adeslas/ Asisa/ DKV/ Sanitas/ Ribera Salud/
(operating/financing) Ribera Salud Ribera Salud Ribera Salud Ribera Salud Asisa
Year tendered 1997/2002 2002 2004 2006 2006
Year opened 1999/2003 2006 2009 2009 2010
Driver Floods cutting off Summer population Need to expand the Reduce demand on Shrink specialty
populations from care influx district hospital central hospital services gap in the
southern part of the
health department
Feature/innovation First PPP to include Expansion of the Transformation of a First suburban health Leveraging economies
private management PPIP model public health department PPIP of scale
of clinical services department to a
PPIP
Committed €142M €80M €96.6M €137M €146M
investment
Population served 276,976 222,334 186,907 213,307 161,413
Hospital beds 301 269 266 354** 233
Clinical staff 1,625 1,037 911 883 925
Outpatient facilities 28 23 45 22 15
1. * In 2012, Sanitas acquired Ribera Salud’s 40% stake in the Manises Hospital. In 2015 Ribera Salud acquired Adeslas’ 51% stake in the La
Ribera UTE. In 2015 Ribera Salud acquired Asisa’s remaining 35% stake in the Torrevieja UTE. In 2015 Ribera Salud acquired Asisa’s
remaining 40% stake in the Vinalopó Salud UTE.
** The 354 beds in Manises include those of the Mislata Hospital
Improvements in focused practices, including flexible departments—for instance the
efficiency recruitment, performance Dénia Hospital coordinated with
incentives, continuous assessment the La Ribera Hospital to provide
In the years since the five PPIP
of patient experience and ‘loyalty highly specialized care services to
projects were implemented, the
strategies.’ The private partners their combined populations.
private sector partners continued to
were also able to reduce Vinalopó and Torrevieja—both
pursue mayor efficiencies. Some of
administrative costs through more managed by the same private
these were achieved through
comprehensive approaches, entity—instituted shared IT,
delivering comprehensive
including establishment of shared procurement and human resource
healthcare services as required by
service centers. systems to allow them to coordinate
National Health System reforms;
care, share staff across specialty
others were accomplished through Some of these efficiencies were units, and jointly procure medical
implementation of outcome- implemented across health supplies. All of the PPIP hospitals
14 Innovation roll out: Valencia’s experience with public-private integrated partnershipsalso continued to enhance their The Valencia Community PPIP As envisioned, the five health
patient outreach strategies and IT model is based on payment of an departments managed as PPIPs
infrastructure to better coordinate annual per-person fee linked with have achieved significant cost
primary and specialty care and give the growth of public health efficiencies compared to their
patients greater access to, and spending. To encourage efficiency, government-managed
control over, their health records. the annual per capita fee for each counterparts: as of 2011 the five
PPIP is set at 80% of the annual PPIPs were responsible for
government expenditure per person delivering care to 18% of Valencia’s
for Valencia citizens. population, yet they accounted for
only 13% of health expenditures
(see Figure 4).
Figure 4: Comparison of health expenditures per person in PPIP vs. publicly-managed health departments
Source: F.Campoy, Jornadas de Economía de la Salud, May 16, 2012
Note: Bubble size represents the percent of the total Valencia population covered by each managerial model
Healthcare public-private partnerships series, No. 3 15Strengths and Valencia Community was able to expenditures. Its experience, and
opportunities address key challenges in future opportunities, can be
healthcare delivery and bend the grouped under six major headings
In expanding its health services
rising curve of medical (see Table 2).
through the PPIP model, the
Table 2: Valencia PPIP strengths and opportunities
Strengths Opportunities
Information • Each PPIP health department has • Increase sharing of patient services data across all health
services highly reliable information systems departments to support and comply with the “money follows the
with up-to-date patient data that is patient” principle
shared as required with healthcare
providers within the department
Strategy • The PPIP model is a resource • Establish a benchmarking system to allow comparison and facilitate
efficiency-centered model rather than sharing of best practices among health departments, both publicly
a traditional budget-based model and privately run
• Response time to address health
issues is shorter due to a less
complex management structure
Government • Each PPIP has a government • Consider establishing a single government entity to supervise all
supervision Compliance Officer to ensure quality PPIPs within the Valencia Community over the lifetime of the
and affordability standards in the concessions, to increase consistency and coordination
delivery of healthcare • Increase the government’s role in planning, sharing lessons
learned, and facilitating/encouraging efficiencies such as shared
procurement
• Establish an evaluation program to continuously assess PPIP
benefits and outcomes
Operational • PPIPs have policies that allow them • Implement mechanisms to allow for planned, periodic adjustment of
flexibility to be flexible and scalable in human, per capita fees to match the changing needs of the covered
economic and material resources population
management • Ensure that the conditions of the PPIP concession are sufficiently
flexible to accommodate changes in the environment without the
need for a new contract
People and • Investments in health promotion and • Increase both government and private partner communications with
change preventive medicine have reduced potential patients around the benefits of the PPIP model in order to
healthcare costs increase trust in the benefits of this type of healthcare model
• Promotion of good health practices • Some staff do not support the PPIP model; efforts are needed to
has generated a long-term engage with them about the model and their role in achieving
engagement effect on PPIP patients successful outcomes
with their healthcare
• Human resource policies have
aligned employee incentives with the
desired outcomes of the PPIPs
Communication • The government maintained a close • Create formal communication channels to demonstrate
and sponsorship relationship with the private sector transparency and achievement of health outcomes to the public
that helps share risk and encourages
win-win situations
Source: UCSF/PwC Fellowship analysis
16 Innovation roll out: Valencia’s experience with public-private integrated partnershipsConclusion This study of the five Valencia Some members of the public health
Community PPIPs highlights four community have argued that PPIP
Since 1997, the Valencia
main factors for public-private solutions are not scalable or
Community has radically
collaboration: generally applicable to health
transformed the way in which
systems, especially in politically
public healthcare is provided. The 1. Economic stability helps to and economically unstable
PPIP model has allowed it to whet private sector appetite for countries. While these conditions
achieve a significant return on its investment and sustain major signal the need for careful
health investment for nearly 20% of government initiatives. assessment of the investment,
its population, while increasing 2. Standardized and scalable Valencia’s experience in sustaining
access to high quality medical care, business models allow greater its PPIPs through two economic
expanding and upgrading health operational and financial downturns demonstrates that PPIP
infrastructure, and encouraging benefits for the government. solutions can be viable even in
innovative practices for improving 3. A capitated funding model, uncertain environments.
healthcare management. along with the “money follows
the patient” principle, allows Although cost effectiveness
To be successful, PPIPs must be
for predictable health spending research is ongoing,6 the Valencia
designed around the unique needs
for governments, and provides PPIP model has achieved positive
of the populations to be served, as
leeway for private partners to economic results, while providing
well as the strengths and
increase system quality, high quality healthcare services. It
capabilities of the public and
efficiency and profitability. has also demonstrated how the
private sector players. This success
4. Trusted relationships between private sector can be leveraged to
can be furthered through active
public and private partners, strengthen public service delivery.
private sector involvement and
with appropriate allocation of
strong public sector leadership,
risk and reward, are critical to
coming together to work toward a
long-term project success.
clear and common set of social and
health objectives.
Healthcare public-private partnerships series, No. 3 17Introduction
The term public-private model–contracting the private financed care to almost 20% of the
partnership (PPP) is used to sector not only to build and operate Valencia Community population.
describe a form of long-term new infrastructure, but also to Overall, PPIP’s in Valencia have
contractual partnership, under deliver publicly-funded clinical succeeded in providing healthcare
which the public sector engages the health services, while maintaining services that are not only
private sector to provide one or its position as owner, controller and comparable in quality to those of
more specified public services. overseer of healthcare delivery to publicly managed services, but also
its citizenry. The approach provided more accessible, efficient and
Since the late 1900s, the Spanish the government with access to sustainable.1
health system has experimented capital in the midst of budget
with a variety of models of public- constraints and an economic This report discusses the successes
private collaboration to deliver downturn, along with an and challenges encountered by the
healthcare to its population. Several opportunity to optimize public five PPIP projects during their
regions engaged the private sector sector functions through rollout in Valencia through 2013,
to access funding and enable the incorporation of private sector and examines the range of
development of health business practices. innovations in patient care,
infrastructure through private management practices,
finance initiatives (PFIs). Others The rich history of Valencia’s first performance management and use
contracted with the private sector PPIP—the La Ribera Hospital—has of technology put in place to
to also provide non-clinical been well documented over the last achieve financial efficiencies and
services. 15 years. The purpose of this report improve access to integrated health
is to explore the Valencia care for target populations. Finally,
In 1997 the Valencia regional Community’s subsequent the report explores several
government in Spain took these experience in replicating and opportunities for both the public
partnerships to a new level, enhancing the PPIP model in Alzira and private sectors, to optimize the
becoming the first region to adopt a and four additional health success and sustainability of the
more advanced “public-private departments, eventually expanding PPIP model in the future.
integrated partnership” (PPIP) privately-delivered, publicly-
Private management of comprehensive public healthcare services
The PPIP model implemented in the Valencia Community integrates an investment in new and/or refurbished
healthcare infrastructure (hospitals and health centers) with the management of all public healthcare services
(primary and specialized) by a private partner, to improve the delivery of comprehensive public healthcare
services to a predetermined population.
Services provided through the PPIP model include:
• Primary care, including emergency care and oral and dental health services
• Curative healthcare, including specialized hospital and hospital-homecare services, diagnostic testing
(where needed), intravenous therapies and surgical procedures, as well as specialized services, including
chemotherapy, infertility treatment, invasive radiology, radiation therapy, and organ, tissue and cell
transplants
• Health promotion and protection initiatives, as well as preventive programs based on health education,
vaccination coverage and medical check-ups
• Rehabilitation support, combining a variety of existing specialties, products and supplies
• Socio-health care for disabled patients and the elderly, as well as psychiatric and mental health care
In Valencia, the PPIP model explicitly excludes the provision of medicines outside hospital facilities, and does
18not cover the cost
Innovation roll of prostheses,
out: oxygen therapy
Valencia’s experience and healthcare
with public-private transportation.
integrated partnershipsCountry profile – immigration, with immigrants indicate that the mortality rate will
Spanish health & constituting 9.6% of the total overtake the birth rate in 2018.
economic context population in 2015.8 Together with a projection of
decreasing levels of immigration,
Situated on the Iberian Peninsula, With an average age of 41.4 years, this will result in an increased old-
Spain is the third largest country in the Spanish population is aging. age dependency ratio, as shown in
Western Europe. Its territory Immigration has helped slow the Figure 5.
includes the Balearic Islands, the rate of aging in recent years;
Canary Islands and two however, current projections
autonomous cities in North Africa,
Ceuta and Melilla.
Spain is a constitutional monarchy,
with a hereditary monarch and a Figure 5: Demographic distribution in Spain, 2010-2050
parliament of two houses—the
Cortes. It is divided
administratively into 17
autonomous communities
(regions), each of which is
governed by its own directly-
elected authorities. As of 2015, the
population was estimated at 48
million, with an average growth
rate of 0.5%, or 4 million people
over the previous 10 years.7 While
the birth rate in recent years has
shown a downward trend
(estimated at 1.3 births per
woman) the mortality rate has
remained stable. Population
growth has instead been driven by
Source: National Institute for Statistics. 2013. www.ine.es
Healthcare public-private partnerships series, No. 3 19The majority (79%) of the Spanish (0.7 million).9 A characteristic represents 23.1% of GDP, while
population lives in urban areas feature of the Spanish economy is the third largest—agriculture—is of
where climate, levels of economic the predominance of the service marginal importance. Within
development and employment sector, which employs about six out industry, metallurgy, food and
opportunities are more favorable.7 of 10 economically active people transportation have shown the
As of 2014, the principal cities in and represents 74.4% of gross highest growth rates in
Spain were Madrid (3.2 million domestic product (GDP). The recent years.10
people), Barcelona (1.6 million), second largest sector—industry—
Valencia (0.8 million) and Seville
Table 3: Spain summary statistics, 2015 (most recent available unless otherwise noted)
Economy* Health Expenditures**
Gross domestic product (GDP) $1,636T USD Total expenditures on health as % of GDP 9.0% (2014)
GPD per capita $35,200 USD % Public 6.39% (2014)
Population 48.15M % Private 2.62% (2014)
Unemployment rate 22.5% % of Private expenses that are 82.38% (2014)
out-of-pocket
Population below the poverty line 21.1% (2012) Per capita expenditures on health (USD) $2,658 (2014)
Median age 42 years
Health status Health resources
Life expectancy at birth*** 83.1 (2014) Total hospitals**** 855 (2013)
Cause of death*** % Public 47% (2013)
Communicable diseases and maternal, 4.7% (2012) % Private 53% (2013)
prenatal and nutrition conditions
Injury 3.4% (2012) Hospital beds per 1,000 population* 3.1 (2011)
Non-communicable diseases 91.8% (2012) Physicians per 1,000 population* 4.94 (2013)
Sources: *CIA The World Factbook, **World Bank, ***Organization for Economic Co-Operation and Development (OECD), **** Institute for the
development and integration of health, 2015
20 Innovation roll out: Valencia’s experience with public-private integrated partnershipsEconomic context From the beginning of the aging population and the
recession, the Spanish government development of expensive
After weathering the global
instituted a number of measures to technologies; it was also a
economic recession of 1992-93,
stimulate growth and job creation consequence of greater access to
Spain stood out for its rapid growth
by encouraging transparency, more effective medicines, which
rate, its high level of capital
flexibility and competitiveness. prolonged the lives of the sick and
accumulation and its rapid job
At the same time, it promoted enhanced their quality of life. To
creation, especially in the
programs to streamline the welfare address the situation, the
construction sector, which
state, reduce costs and assure the government suggested a range of
represented between 6-11% of GDP.
sustainability of the social safety cost-containment measures,
However, after almost 15 years of
net, with a particular focus on including the closing of facilities,
better-than-average GDP growth,
austerity measures across the 17 wage cuts, price controls for
investment in the construction
autonomous communities. laboratories, co-payments for
sector led to a speculative bubble,
medicines and further public-
which burst in 2007. This slowed The health sector faced similar private collaboration to offset the
the economy and Spain officially changes, with costs growing almost lack of public resources.
entered into recession in 2008. three times as fast as GDP during
GDP shrank 3.7% in 2009 and, 2000-10. This was due in part to an
despite various fiscal and labor
reforms, a high unemployment rate
(25% in 2012) and weak consumer
spending impeded recovery.9
Nonetheless, it is expected that Figure 6: Changes in GDP and health spending in Spain since 2003
Spain will grow 2.8% in 2016 and
2.1% in 2017.11
Up until 2007, Spain boasted a
budget surplus of 1.9%, with public
debt amounting to 36.1% of GDP.
In the wake of the 2008-09
economic crisis, however, the lack
of employment and the downturn
in consumption led to a budget
deficit equivalent to 11.2% of GDP
by the beginning of 2010. A
number of austerity measures
managed to reduce this deficit by
5.7% by the end of 2014.12
Source: The World Bank, 2015. World Data Bank. http//www.worldbank.org
Healthcare public-private partnerships series, No. 3 21Spanish National Health • Inter-Regional Council— governments of the autonomous
System fundamentals responsible for coordination, communities, allowing them
cooperation, communication greater leeway in managing their
The Spanish National Health
and information sharing among resources and entrusting them with
System, considered one of the most
regional agencies and with the the organization and provision of
advanced in the world, is
Central Government. healthcare services.13 Each of the
committed to improving health
• Autonomous Communities autonomous communities has
standards and reducing social
—responsible for healthcare assigned a ministry of health,
inequality. In 1986, as mandated
planning, public health charged with regulation, healthcare
under the Spanish Constitution of
initiatives, and healthcare policy planning, and the provision
1978 to assure universal healthcare,
service management of both primary and specialized
the Spanish government
and delivery. medical services.
streamlined healthcare services,
integrating the functions of Some high-specialized services and Today, the majority of healthcare
regulation, financing and delivery a portion of pharmaceutical services is delivered free of charge
of services. provision remained under the by public providers, with a 40%
responsibility of the Central co-payment for the purchase of
The National Health System was Government through general medicine by those under 65.
consolidated under government taxation.
leadership as a coordinated group
comprised of three levels: Following a 20-year process of
decentralization and reform that
• Central Government— concluded in 2002, each of the 17
responsible for national autonomous communities assumed
coordination, policy regarding operational and financial
medicines, matters of responsibility for the health of its
international health and the population. Since then, the Central
management of healthcare Government has allocated 38% of
services in the cities of Ceuta direct and indirect taxes to the
and Melilla.
Underlying fundamentals of the Spanish National Health System
• Publically-funded system, providing universal and complimentary services (oxygen, ambulances, assisted
care, etc.)
• Well-defined rights and obligations for both users and government authorities
• Responsibility for healthcare service delivery decentralized to the 17 autonomous communities
• Provision of comprehensive healthcare with a goal of providing high-quality services
• Healthcare assessment and regulation in a common system mandated by the government
• Incorporation of structures in favor of health under the National Health System (consortia, public-private
collaboration, etc.)
22 Innovation roll out: Valencia’s experience with public-private integrated partnershipsOrganization health department is then divided The health departments serve as
further into ‘basic health zones’ the functional units of the
Within each autonomous
which serve as the gateways into healthcare system, and are
community, the healthcare system
the healthcare system. Each zone responsible for managing the basic
is subdivided into smaller health
includes a primary care team, health zones, together with a range
‘areas,’ or departments, based on
which provides services to patients of specialty centers, hospitals, and
geographic, socioeconomic, cultural
in its territory and refers those public health programs.3
and epidemiological factors—each
requiring more specialized care to
serving a population of about
specialty centers or hospitals.
200,000-250,000 residents. Each
Figure 7: Organizational design of Spain’s National Health System
Source: General Health Law 14/1986 and Law of Cohesion and Quality of the National Health System, 16/2003
Healthcare public-private partnerships series, No. 3 23Types of public-private increase access, reduce wait times, The independent authority of the
collaboration in and/or optimize the use of autonomous communities has
healthcare resources. In 2015, the Institute for enabled them to develop their own
the Development of Comprehensive organization, management and
The majority of healthcare
Healthcare (IDIS) estimated that planning policies, leading to the
infrastructure in Spain belongs to
almost 12% of the government’s emergence of 17 healthcare models
the government, including over
health budget was earmarked for in Spain. However, this diversity
90% of primary care centers and such relationships. has not led to significant
67% of hospital beds.14
differences in the level of services,
On average, 15%-20% of hospital nor in the type of treatments that
Nonetheless, the autonomous
services are delivered by the private the government is committed to
communities are allowed to sector nationally.
contract with private services based provide to the population.
on regional need, for instance to
Table 4: Most common forms of healthcare public-private collaboration in Spain
Type of collaboration Description Purpose
Administrative mutualism Mechanism to ensure healthcare coverage to • Fund and/or provide health services
public servants and judicial armed forces for government employees with
personnel. Individuals can choose whether social security
they are cared for by the public or the private
sector.
Arranged hospitals Agreements with a private provider, made by • Improve healthcare access to remote
the government through a competitive communities
process, to provide specific health services • Relieve waiting lists
and procedures in exchange for a set fee
• Provide highly-specialized and costly
services
• Provide care to specific populations
• Increase compliance with government
health-related goals
• Develop and implement specific
assistance programs
Unique concerts Private hospitals that have been strategically • Respond to a health need on a case-by-
linked to the public system to fill gaps in public case basis without increasing public debt
providers; the hospitals receive a payment for
every service they provide
Administrative concessions Partnerships between the public and private • Engage private sector to assume the
(PPPs/PPIPs) sectors to design, finance, develop, build and financial and operational risks of financing
operate infrastructure projects, and deliver infrastructure and delivering care
healthcare services, through a concession • Increase efficiency and quality through
contract performance management
Source: UCSF/PwC Fellowship analysis
24 Innovation roll out: Valencia’s experience with public-private integrated partnershipsYou can also read