Infertility in Patients With Klinefelter Syndrome: Optimal Timing for Sperm and Testicular Tissue Cryopreservation - MedReviews
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ManageMent Update
Infertility in Patients With Klinefelter
Syndrome: Optimal Timing for Sperm
and Testicular Tissue Cryopreservation
Dorota J. Hawksworth, MD, MBA,1 April A. Szafran, MD, PhD,1 Philip W. Jordan, PhD,2
Adrian S. Dobs, MD,3 Amin S. Herati, MD1
1Department of Urology, Johns Hopkins Medical Institutions, Baltimore, MD; 2Department of Biochemistry and
Molecular Biology, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD; 3Department
of Endocrinology, Johns Hopkins Medical Institutions, Baltimore, MD
Male factor infertility is a complex issue presenting many diagnostic and management
challenges. It is responsible for about 50% of all causes of infertility and thus carries
significant medical, financial, and psychological implications for the couples struggling
with conception. Klinefelter syndrome is the most common chromosomal male anomaly
associated with male infertility. This review focuses specifically on non-obstructive azo-
ospermia secondary to Klinefelter syndrome and discusses controversies surrounding
fertility management in patients with this genetic disorder.
[Rev Urol. 2018;20(2):56–62 doi: 10.3909/riu0790]
© 2018 MedReviews , LLC ®
KEY WORDS
Klinefelter syndrome • Non-obstructive azoospermia • Sperm retrieval
I
nfertility, defined as failure to conceive after 1 year level, is part of the standard evaluation of the infer-
of unprotected sexual intercourse, is estimated to tile male as it can assist in establishing an underlying
affect up to 15% of couples worldwide with a male diagnosis and can also guide medical and surgi-
factor implicated in approximately 50% of cases.1-3 cal therapy. With male infertility, FSH level values
Male infertility can manifest from numerous etiolo- inversely reflect the quality of spermatogenesis. An
gies ranging from obstruction of the vasa deferentia FSH value over 7.6 IU/mL has been shown to be a
to non-obstructive etiologies, such as genetic anom- strong predictor of spermatogenic failure, whereas
alies resulting in testicular dysfunction. a normal FSH value is predictive of normal sper-
An endocrine evaluation, consisting of a serum matogenesis. Schoor and colleagues showed that
testosterone and follicle-stimulating hormone (FSH) 91% of men with azoospermia and FSH value less
56 • Vol. 20 No. 2 • 2018 • Reviews in Urology
4170018_02_RIU0790_V2_ptg01.indd 56 9/11/18 5:15 PMInfertility in Patients With Klinefelter Syndrome
than 7.6 IU/mL had an obstructive syndrome, mixed gonadal dysgen- 49,XXXXY), or possess partial
etiology explaining their infertil- esis, autosomal translocations, and fragments of supranumery X
ity. Similarly, elevated FSH values Y-chromosome microdeletions.8 chromosomes (eg, 47,X,iXq,Y).10,12
also correlate with a lower prob- KS is the most common chromo- Whereas some mosaic patients
ability of sperm retrieval rates with somal male anomaly, the most present with less severe infertility
testicular sperm extraction (TESE) common sex chromosome disorder phenotypes and possess reduced
procedures.4,5 of infertile men, and as such, it spe- concentrations of sperm on SA
Although decreasing semen para- cifically results in NOA. (oligozoospermia), most men with
meters, such as sperm concentra- A comprehensive hormonal KS are azoospermic and for pater-
tion, and rising FSH values can be evaluation of the patients with nity reasons require assisted repro-
used as an indication of progres- NOA sub-classifies them into two ductive technologies (ART).
sive spermatogenic failure, it is not groups: those with hypogonado-
a perfect biomarker of spermato- tropic hypogonadism (HH) and Natural History of KS
genesis. Ramasamy and colleagues those with hypergonadotropic Patients may be diagnosed with KS
showed that among men with non- hypogonadism. Hypergonadotropic during different stages of their lives,
obstructive azoospermia (NOA), hypogonadism is caused by an ranging from the prenatal period
sperm retrieval rates using micro- intrinsic testicular dysfunction via amniocentesis to adulthood.
surgical testicular sperm extraction and its causes include genetic Most patients undergo chromo-
(mTESE) were higher among men defects (aneuploidy, Y-chromosome somal evaluation in their adoles-
with an FSH value of .15 IU/mL microdeletions), varicocele, expo- cence or adulthood, when delayed
than men with an FSH ,15 IU/mL.6 sure to gonadotoxins, orchitis, or incomplete puberty or infertil-
In this study, three men with FSH prior surgery/trauma, or testicular ity arise. However, an increasing
values .90 IU/mL had successful torsion.9 Of these causes, KS is the number of KS patients are detected
sperm extraction. These findings most common aneuploidy in men prenatally secondary to their par-
demonstrate the limited utility of resulting in male factor infertil- ents delaying reproduction due to
FSH and the importance of micro- ity and is characterized by a male socioeconomic factors and gender
surgical examination in men who karyotype with one or more addi- roles changes in the work force.13
are actively seeking fertility. tional X chromosomes. The disease As a consequence of increasing
In this review, we focus spe- affects 1 in 600 newborn males and maternal age, more amniocente-
cifically on non-obstructive azo- typically manifests in adolescence ses and chorionic villi biopsies are
ospermia secondary to Klinefelter or early adulthood with charac- performed thus increasing prenatal
syndrome (KS), which is character- teristic findings of hypergonado- diagnoses of KS.
ized by a high FSH level, and dis- tropic hypogonadism and primary In addition to chromosomal
cuss the optimal timing of sperm infertility.10,11 On physical exami- analysis, all men with KS should
retrieval in these patients, many nation, patients usually have nor- undergo a thorough reproductive
of whom are not actively seeking mal or tall stature, gynecomastia, workup with hormonal and SA
fertility. and small testes. Additionally, these evaluations. Levels of testosterone,
patients may have mild cognitive luteinizing hormone (LH), FSH,
impairment. Due to a wide varia- estradiol (E2), prolactin, sex hor-
Genetic Basis for Male tion in clinical presentation, many mone binding globulin (SHBG),
Infertility and Klinefelter patients may go undiagnosed. The and inhibin B should be measured.
Syndrome diagnosis, when made, depends on It has been documented that pre-
Overall, genetic and genomic a combination of history, physical pubertal males have normal lev-
abnormalities may contribute up to examination, semen analysis (SA), els of testosterone, LH and FSH,
50% of male factor infertility and and, ultimately, karyotype testing. whereas at puberty testosterone
infertile men have up to 10-fold With increasing utilization of pre- levels start to decline and FSH and
higher prevalence of chromosomal natal or other genetic testing, the LH rise. In addition to a hormonal
abnormalities when compared detection of KS is likely to increase. evaluation, at least two semen sam-
with fertile men.7 Aneuploidy is The majority of patients carry ples should be analyzed.
the most common chromosomal a 47XXY karyotype, whereas the Testicular function in KS presents
error identified in infertile men remaining 10% to 20% are mosa- a story of progressive degeneration.
and the most common of those ics (46,XY/47,XXY), have higher Ultimately, this degeneration leads
are KS, XYY syndrome, XX male grade aneuploidy (48,XXXY, to infertility as the normal testicular
Vol. 20 No. 2 • 2018 • Reviews in Urology • 57
4170018_02_RIU0790_V2_ptg01.indd 57 9/11/18 5:15 PMInfertility in Patients With Klinefelter Syndrome continued
recent investigations into the tran-
scriptome have highlighted many
candidate genes that are dysregu-
A – Aromatase HYPOTHALAMUS
ABP – Androgen Binding Protein lated in KS spermatogonial cells.
E2 – Estradiol
FSH – Follicle Stimulating Hormone
D’Aurora and colleagues analyzed
GnRH – Gonadotropin Releasing Hormone
LH – Luteinizing Hormone
the transcriptome of testicular biop-
T - Testosterone GnRH sies obtained from three men with
KS and compared them with the
PITUITARY transcriptome of three controls.12
Differential expression was observed
FSH LH in 1050 genes, with 747 genes down-
regulated and 303 up-regulated
genes. One-third of the genes up-
regulated were linked to apoptosis.
SERTOLI CELL LEYDIG CELL Gene cluster and pathway analysis
INHIBIN
A showed four possible mechanisms
T T E2
responsible for hypospermatogen-
ABP
esis in KS patients: impaired devel-
opment of spermatogonia to mature
spermatozoa, defects in the testis
architecture, pathophysiology of the
Figure 1. Representation of hypothalamus-pituitary-gonadal axis.
testis environment, and apoptosis
of the germinal and somatic cells.20
Of all the dysregulated genes, four
genes mapped to the X chromo-
architecture is replaced initially by patients occurs during puberty. some including solute carrier family
either tubular atrophy, sclerosis, or Wilkstrom and colleagues dem- 25 member 5 gene (SLC25A5) on the
maturation arrest and ultimately onstrated that prepubertal KS Par1 region, phosphoribosyl pyro-
degenerates to fibrosis and hya- patients with bilateral descended phosphate synthetase 1 (PRPS1),
linized tissue.14 Numerous stud- testes retained germ cells on biopsy, TSC22 domain family member 3
ies demonstrate already reduced though at lower levels than normal (TSC22D3), and A-kinase anchoring
numbers of germ cells in biopsies of children.18 The subjects who had protein 4 (AKAP4). Other important
47XXY fetal testes evaluated dur- undergone puberty at the time of dysregulated genes include down-
ing the prenatal period, between biopsy had no germ cells present and regulation of the cAMP responsive
18 and 22 weeks of gestation.15,16 had concomitant degeneration of element modulator (CREM) gene,
This deficit is further augmented in Sertoli cells and hyalinization of the which is an important transcrip-
non-descended testes. In the neo- seminiferous tubules.18 Therefore, tion factor for spermatogenesis,
natal period, based on lower levels activation of the hypothalamic- the HORMA domain containing
of serum testosterone during the pituitary-gonadal (HPG) axis 2 (HORMAD2) gene, which sur-
initial months of life in non-mosaic (Figure 1) and stimulation of the veils the synaptic events during
47XXY patients, Leydig cell dys- gonadal tissue appears to accelerate prophase of meiosis, and the cyclin
function is postulated to play a sig- testicular demise in puberty. This is A1 (CCNA1) gene, which is required
nificant role.17 Sertoli cells, however, thought to arise from aneuploidy- for spermatocyte passage into the
appear to be histologically intact in induced non-homologous recom- first meiotic division.21,22 Compared
both the fetal and neonatal periods bination and subsequent activation with controls, the majority of down-
in subjects with a 47XXY genotype. of apoptosis-related genes within regulated genes were those essential
These subtle changes may create a the spermatogonial cell line as for spermatogenesis, whereas apop-
platform for the later testicular fail- spermatogonia differentiate into totic genes were common among
ure that ensues in adolescence. primary spermatocytes and prog- those up-regulated.
The transition to rapid deterio- ress through meiosis.12,19 The spermatogonia of the testis
ration in production of both germ While the molecular mecha- can possess significant heterogene-
cell lines as well as in the histologi- nisms underlying spermatogenic ity, even among patients with sex
cal composition of the testes in KS failure are poorly understood, chromosome trisomy (SCT). Recent
58 • Vol. 20 No. 2 • 2018 • Reviews in Urology
4170018_02_RIU0790_V2_ptg01.indd 58 9/11/18 5:15 PMInfertility in Patients With Klinefelter Syndrome
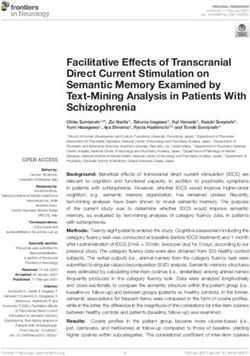
47XXY able and willing to provide an
ejaculated specimen, they may ulti-
iPSC iPSC iPSC mately avoid more invasive surgi-
cal interventions in their future.
Testicular dissection for sperm
PASSAGE 2-6
FIBROBLAST– 47XXY harvesting has well documented
negative effects and those may
result in irreversible scarring and
PGCLC PGCLC PGCLC iPSC iPSC iPSC
atrophy, potential testicular injury
DIFFERENTIATION TO
or loss, as well as further decline
46XY/46XX EPIBLAST-LIKE STATE 46XY/46XX in testicular function and resulting
decrease in testosterone levels.27
TR
ANS The need for chronic hormonal
PL
AN
T SEMINIFEROUS TUBULE therapy (HT) in these patients
further complicates their fertility
Figure 2. Trisomic chromosome loss and development of spermatozoa from euploid primordial germ cell–like potential. HT is often initiated in
cells (PGCLC) from induced pluripotent stem cells (iPSC). Methodology adapted from Hirota T et al.23
boys with KS at around 12 years of
age, especially if they exhibit evi-
data from Hirota and colleagues associated with increased rates of dence of hypergonadotropic hypo-
demonstrate a mechanism for progressive testicular germ cell gonadism. Androgen replacement
spermatogonia to escape the mas- depletion and subsequent decline in at the time of puberty supports
sive wave of apoptosis that occurs testicular function. It is also widely normal development of secondary
during puberty in KS patients accepted that small, patchy distri- sexual characteristics, body habitus,
(Figure 2).23 To demonstrate this bution of spermatogenesis exists and results in overall improvement
phenomenon, fibroblasts derived even in the adult men’s testes, as in energy levels. Furthermore, long-
from control and sex chromosome spermatozoa have been found both term HT prevents development
trisomy mice were dedifferenti- in the testicular tissue and occa- of significant medical issues, to
ated to form-induced pluripotent sionally in the ejaculate. At present, include osteoporosis, diabetes, obe-
stem cells (iPSCs). Fluorescent in thanks to the advances in testicular sity, and depression. Excess extra-
situ hybridization performed on sperm extraction (TESE) and intra- testicular androgens, however,
iPSCs derived from SCT fibroblasts cytoplasmic sperm injection (ICSI) further suppress already impaired
showed a propensity for sex chro- techniques, approximately 50% spermatogenesis in patients with
mosome loss over autosomal chro- of men with KS will have sperm KS. It has been postulated that
mosome loss, returning the iPSC detected with TESE/microTESE, sperm harvest at time of puberty,
cells to a euploid state. This concept of which a 50% pregnancy and live or prior to initiation of HT provides
of trisomic chromosome loss has birth rate can be expected.25 best chance of success.26 Although
been similarly observed in human Based on prior data indicating new approaches to medical man-
trisomic cell cultures obtained and that younger age is a major posi- agement of these patients’ hypo-
reprogrammed into iPSC from the tive predictive factor for success- gonadism allows successful sperm
fibroblasts of patients with Down ful sperm retrieval, it has been harvest, despite long-term andro-
syndrome.23,24 Hirota and col- advocated that fertility preserva- gen supplementation, sperm cryo-
leagues provide an important proof tion should be offered to prepu- preservation should be offered to
of concept for the mechanism by bertal and adolescent boys with all adolescents with KS irrespective
which KS patients may retain the KS. Because the testicular func- of their hormonal status, particu-
ability to preserve spermatogenesis tion decline begins in puberty and larly those who are either consider-
into later years of life.23 worsens in adulthood, intervention ing or receiving HT.
prior to or at the beginning of this Currently, there are no estab-
decline should yield the most suc- lished guidelines for appropriate
Pros and Cons of Early cessful sperm retrieval. Sperm has timing or and harvesting technique
Fertility Management been identified in 70% of ejaculated choices, and only sperm cryo-
It is well established that men with semen specimens in adolescents preservation is considered accepted
KS are born with spermatogonia with KS aging 12 to 20 years.26 standard of care. An important
and that the onset of puberty is Therefore, if younger patients are consideration in determining the
Vol. 20 No. 2 • 2018 • Reviews in Urology • 59
4170018_02_RIU0790_V2_ptg01.indd 59 9/11/18 5:15 PMInfertility in Patients With Klinefelter Syndrome continued
optimal timing of microTESE in chorionic villi biopsy. Alternative of micro-TESE has reduced the
KS patients is whether fresh or strategies may also become avail- amount of testicular tissue needed
cryopreserved-thawed testicular able to prevent the activation of and has minimized the damage
sperm yields different outcomes spermatogonia and their subse- to the testicular blood supply and
with in vitro fertilization (IVF) and quent apoptosis. These approaches resulted in much higher over-
ICSI. Although few studies have to fertility preservation in young all SRR. Schlegel and colleagues
compared ICSI outcomes between adolescent males are also laden with reported a significant statistical
fresh and cryopreserved-thawed significant technical challenges and difference in the overall SRR when
testicular spermatozoa from KS ethical controversy. Young patients comparing patients undergoing
patients, the available studies show may not be emotionally mature to standard TESE to those under-
comparable outcomes. In one study consider future fertility issues, may going micro-TESE (45% vs 63%)
by Friedler and colleagues, fresh not be able or willing to provide an and further demonstrated much
testicular spermatozoa resulted in ejaculated semen sample, and may higher spermatozoa yield from
improved two pronuclear fertil- be too afraid of any invasive surgi- smaller, micro-dissected samples
ization rate (66% vs 58%), embryo cal interventions. Specimen storage (64,000 vs 160,000).30 Moreover,
cleavage rate (98% vs 90%), and fees may also carry a significant sperm retrieval rates in patients
embryo implantation rate (33.3% vs long-term financial burden on both with KS have been demonstrated
21.4%) over cryopreserved-thawed the patients and their parents. At to be equivalent to those men who
testicular spermatozoa; however, this point, fertility and hormonal have NOA secondary to other
this difference was not statisti- management should be offered to reasons.31 Unfortunately, micro-
cally significant.28 These findings KS boys as early as 12 years of age. TESE requires highly specialized
are consistent with those of a 2017 With proper counseling, education microsurgical training and close
meta-analysis by Corona and col- and multidisciplinary approach to cooperation with the reproduc-
leagues, who showed no difference these patients’ complex issues, their tive endocrinologist and the ART
in pregnancy and live birth rates future reproductive and overall team. As such, patients requiring
between fresh and cryopreserved- health can be successfully managed micro-TESE are usually referred to
thawed testicular spermatozoa long term. high-volume, specialized infertility
using data extracted from 1248 centers.
KS patients from 37 studies, and Normal testosterone levels have
a 2014 meta-analysis by Ohlander Strategies to Optimize been found to be an independent
and coworkers, who observed no Sperm Retrieval Rates factor in improving SRR. Currently,
statistically significant difference Unsuccessful sperm recovery the primary goal of medical man-
between fertilization and clini- has negative impact on patients agement in men with hypergonad-
cal pregnancy rates using the two and their partners from an emo- otropic hypogonadism, in addition
types of spermatozoa in men with tional and a financial standpoint. to correcting their hypogonad-
NOA.25,29 Based on these limited Literature indicates that surgical ism, is to improve the quantity
studies, we believe that cryopre- sperm retrieval rates (SRR) in men and quality of the retrieved sperm.
served-thawed testicular sperm with KS are estimated to be approx- Antiestrogens (clomiphene citrate,
is a viable option for KS patients imately 51%, ranging from 28% to tamoxifen), aromatase inhibitors
who are not actively planning for 70% with a pregnancy and live (testolactone, anastrozole), and
conception but wish to retain their birth rate of 50%.25 Recent surgical gonadotropins (recombinant FSH
sperm for future use. advances with introduction of sur- and hCG) have been evaluated in
Other, more experimental ap- gical microscope and micro-TESE, patients with NOA and KS.
proaches, such as testicular tissue optimization of ART techniques, Non-steroidal antiestrogens block
or spermatogonial stem cell cryo- improvements in medical manage- the feedback inhibition of estro-
preservation with subsequent goal ment of hypogonadism, as well as gen on the pituitary, resulting in
of transplantation, can be offered to more proactive early approach to increased levels of LH and FSH
patients only as part of an institu- management of these patients all and subsequent rise in testoster-
tional research protocol. We antici- contribute to improved SRR and one. Clomiphene citrate has been
pate that pre-pubescent fertility ultimately fertility outcomes. used in severely oligozoospermic
management will gain in importance The use of high-power surgi- men and thus far, only one series
as more KS patients are detected cal microscope (magnification evaluated its use in NOA patients.32
prenatally via amniocentesis or of 20×-25×) and development Clomiphene citrate enabled the
60 • Vol. 20 No. 2 • 2018 • Reviews in Urology
4170018_02_RIU0790_V2_ptg01.indd 60 9/11/18 5:15 PMInfertility in Patients With Klinefelter Syndrome
detection of ejaculated sperm in severe oligozoospermia, men with References
two-thirds of men who were origi- NOA had no such benefit. The 1. Jarow J, Sigman M, Kolettis PN, et al. The optimal
evaluation of the infertile male: AUA Best Practice
nally NOA and diagnosed with experts argue, however, that use of Statement. Linthicum, MD: American Urological
either maturation arrest or hypo- non-steroidal aromatase inhibitor Association, Inc.®; 2010.
2. Templeton A, Fraser C, Thompson B. The epidemiol-
spermatogenesis on initial testicu- (anastrozole) specifically, results in ogy of infertility in Aberdeen. BMJ. 1990;301:148-152.
lar biopsy. However, it is important improved intra-testicular testoster- 3. World Health Organization. Programme of Maternal
and Child Health and Family Planning Unit. Infertil-
to emphasize that KS men often one levels that further improve SRR ity : a tabulation of available data on prevalence of
have elevated FSH values and are over a period of 3 months. primary and secondary infertility. Geneva: World
Health Organization; 1991. http://www.who.int/iris/
not candidates for clomiphene In conclusion, use of any of the handle/10665/59769.
citrate therapy. non–testosterone-based formula- 4. Schoor RA, Elhanbly S, Niederberger CS, Ross LS. The
role of testicular biopsy in the modern management of
Exogenous gonadotropins de- tions may be considered in KS men male infertility. J Urol. 2002;167:197-200.
crease the endogenous gonadotro- planning on surgical sperm extrac- 5. Bromage SJ, Falconer DA, Lieberman BA, et al. Sperm
retrieval rates in subgroups of primary azoospermic
pin levels and in turn “re-set” FSH tion. The selection of this type of males. Eur Urol. 2007; 51:534-539; discussion 539-540.
and LH receptors in the Sertoli and therapy and the decision to start it 6. Ramasamy R, Lin K, Gosden LV, et al. High serum
FSH levels in men with nonobstructive azoospermia
Leydig cells, respectively, ultimately should be made on individual basis, does not affect success of microdissection testicular
resulting in their improved func- following appropriate patient coun- 7.
sperm extraction. Fertil Steril. 2009;92:590-593.
Yatsenko AN, Yatsenko SA, Weedin JW, et al. Compre-
tion. Ramasamy and colleagues seling, especially because current hensive 5-year study of cytogenetic aberrations in 668
infertile men. J Urol. 2010;183:1636-1642.
reported improved TESE outcomes clinical evidence for this indica- 8. O’Flynn O’Brien KL, Varghese AC, Agarwal A. The
in patients with NOA and KS who tion is not well supported by large genetic causes of male factor infertility: a review. Fertil
Steril. 2010;93:1-12.
received gonadotropin therapy.6 randomized, placebo-controlled 9. Kumar R. Medical management of non-obstructive azo-
Testosterone and other andro- studies. ospermia. Clinics (Sao Paulo). 2013;68(suppl 1):75-79.
10. Foresta C, Galeazzi C, Bettella A, et al., Analysis of
gens are converted into E2 by aro- meiosis in intratesticular germ cells from subjects
matase, an enzyme present in the affected by classic Klinefelter’s syndrome. J Clin Endo-
liver, adipose tissue, and testes. Conclusions 11.
crinol Metab. 1999;84:3807-3810.
Klinefelter HF, Reifenstein EC, Albright F. Syndrome
Elevated E2 levels further suppress KS results in infertility in all characterized by gynecomastia, aspermatogen-
esis without aledyigism and increased secretion of
LH and FSH secretion from the affected men. Early fertility preser- follicle-stimulating hormone. J Clin Endocrinol Metab.
pituitary and inhibit testosterone vation, although currently not 1942;2:615-627.
12. D’Aurora M, Ferlin A, Garolla A, et al. Testis tran-
biosynthesis. Aromatase inhibitors, standard of care, is recommended, scriptome modulation in Klinefelter patients with
at doses of 1 mg anastrozole daily, as sperm retrieval rates have been hypospermatogenesis. Sci Rep. 2017;7:45729.
13. United States Census Bureau. Childlessness rises for
are designed to block the conver- higher in younger patients. women in their early 30s. https://www.census.gov
sion of androgens to E2 and thus Complex, multidisciplinary care /newsroom/blogs/random-samplings/2017/05/
childlessness_rises.html. Posted May 3, 2017. Accessed
further re-establishing a testoster- should be provided to these patients May 30, 2018.
one and E2 (T/E) balance. Although to optimize their overall health sta- 14. Aksglaede L, Link K, Giwercman A, et al. 47, XXY
Klinefelter syndrome: clinical characteristics and age-
significant improvements in sperm tus in addition to their ability to specific recommendations for medical management.
Am J Med Genet C Semin Med Genet. 2013;163C:55-63.
counts were noted in men with father children.
Main Points
• Klinefelter syndrome (KS) is the most common chromosomal disorder in men and is associated with
hypergonadotropic hypogonadism and infertility.
• Early hormonal therapy is recommended for patients with KS to assure normal puberty and prevent long-term
consequences of hypogonadism.
• Cryopreservation of ejaculated samples or testicular tissue samples should be offered to all young, post-
pubescent KS men who are starting or considering androgen replacement therapy.
• Improvements in microsurgical sperm retrieval and assisted reproductive techniques, in addition to management
of patients’ hypogonadism with non–testosterone-based formulations and interventions offered in adolescence
all contribute to significant improvements in sperm retrieval rates and provide maximum future fertility potential.
Vol. 20 No. 2 • 2018 • Reviews in Urology • 61
4170018_02_RIU0790_V2_ptg01.indd 61 9/11/18 6:48 PMInfertility in Patients With Klinefelter Syndrome continued
15. Coerdt W, Rehder H, Gausmann I, et al. Quantita- prophase via the recruitment of ATR activity. Genes 28. Friedler S, Raziel A, Strassburger D, et al. Outcome of
tive histology of human fetal testes in chromosomal Cells. 2012;17:897-912. ICSI using fresh and cryopreserved-thawed testicular
disease. Pediatr Pathol. 1985;3:245-259. 22. Liu D, Matzuk MM, Sung WK, et al. Cyclin A1 is spermatozoa in patients with non-mosaic Klinefelter’s
16. Murken JD, Stengel-Rutkowski S, Walther JU, et al. required for meiosis in the male mouse. Nat Genet. syndrome. Hum Reprod. 2001;16:2616-2620.
Letter: Klinefelter’s syndrome in a fetus. Lancet. 1998;20:377-380. 29. Ohlander S, Hotaling J, Kirshenbaum E, et al. Im-
1974;2:171. 23. Hirota, T., et al., Fertile offspring from sterile sex pact of fresh versus cryopreserved testicular sperm
17. Lahlou N, Fennoy I, Carel JC, Roger M. Inhibin B and chromosome trisomic mice. Science, 2017. 357(6354): upon intracytoplasmic sperm injection pregnancy
anti-Mullerian hormone, but not testosterone levels, p. 932-935. outcomes in men with azoospermia due to sper-
are normal in infants with nonmosaic Klinefelter syn- 24. Hirota T, Ohta H, Powell BE, et al. Altered hemato- matogenic dysfunction: a meta-analysis. Fertil Steril.
drome. J Clin Endocrinol Metab. 2004;89:1864-1868. poiesis in trisomy 21 as revealed through in vitro dif- 2014;101:344-349.
18. Wikström AM, Raivio T, Hadziselimovic F, et al. ferentiation of isogenic human pluripotent cells. Proc 30. Schlegel PN. Testicular sperm extraction: microdis-
Klinefelter syndrome in adolescence: onset of puberty Natl Acad Sci U S A. 2012; 109:17567-17572. section improves sperm yield with minimal tissue
is associated with accelerated germ cell depletion. J 25. Corona G, Pizzocaro A, Lanfranco F, et al. Sperm excision. Hum Reprod. 1999;14:131-135.
Clin Endocrinol Metab. 2004;89:2263-2270. recovery and ICSI outcomes in Klinefelter syndrome: 31. Schlegel PN. Nonobstructive azoospermia: a revolu-
19. Maiburg M, Repping S, Giltay J. The genetic origin of a systematic review and meta-analysis. Hum Reprod tionary surgical approach and results. Semin Reprod
Klinefelter syndrome and its effect on spermatogen- Update. 2017;23:265-275. Med. 2009;27:165-170.
esis. Fertil Steril. 2012;98:253-260. 26. Mehta A, Paduch DA. Klinefelter syndrome: an ar- 32. Hussein A, Ozgok Y, Ross L, Niederberger C.
20. Maranesi M, Barzanti V, Coccheri S, et al. Interac- gument for early aggressive hormonal and fertility Clomiphene administration for cases of nonobstructive
tion between vitamin B6 deficiency and low EFA management. Fertil Steril. 2012;98:274-283. azoospermia: a multicenter study. J Androl. 2005;26:
dietary intake on kidney phospholipids and PGE2 27. Ramasamy R, Yagan N, Schlegel PN. Structural and 787-791; discussion 792-793.
in the rat. Prostaglandins Leukot Essent Fatty Acids. functional changes to the testis after conventional
1993;49:531-536. versus microdissection testicular sperm extraction.
21. Kogo H, Tsutsumi M, Inagaki H, et al. HORMAD2 Urology. 2005;65:1190-1194.
is essential for synapsis surveillance during meiotic
62 • Vol. 20 No. 2 • 2018 • Reviews in Urology
4170018_02_RIU0790_V2_ptg01.indd 62 9/11/18 5:15 PMYou can also read