Infection Prevention Updates for Acute Care and Outpatient Settings - Nebraska ICAP
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Guidance and responses were provided based on information known on
2/9/2022 and may become out of date. Guidance is being updated rapidly, so users
should look to CDC and NE DHHS guidance for updates.
Infection Prevention Updates
for Acute Care and
Outpatient Settings
February 9, 2022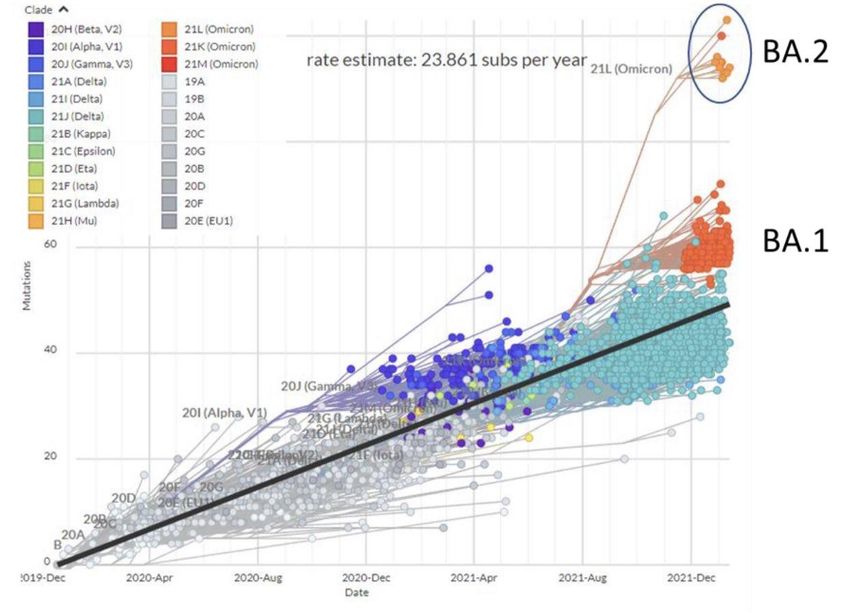
Questions and Answer Session
Presenters today are:
Gary Anthone, MD gary.anthone@nebraska.gov
Matthew Donahue, MD matthew.donahue@nebraska.gov
Ishrat Kamal-Ahmed, M.Sc., Ph.D. ishrat.kamal-ahmed@nebraska.gov
Daniel Taylor, DHHS daniel.taylor@nebraska.gov
Rebecca Martinez, BA, BSN, RN, CIC remartinez@nebraskamed.com
Daniel Brailita, MD dabrailita@unmc.edu
Panelists today are:
Richard Starlin, MD rick.starlin@unmc.edu
Josette McConville, RN, CIC jmcconville@nebraskamed.com
Kate Tyner, RN, BSN, CIC ltyner@nebraskamed.com
Jody Scebold, EdD, MSN, RN jodscebold@nebraskamed.com
Sarah Stream, MPH, CDA, FADAA sstream@nebraskamed.com
Chris Cashatt, RN, BSN, CIC ccashatt@nebraskamed.com
Moderated by Margaret Deacy mdeacy@nebraskamed.com
Please use the Q&A box in the webinar platform to type a question. Questions will be read aloud.
If your question is not answered during the webinar, please e-mail it to
nebraskaicap@nebraskamed.com or call Monday – Friday 8:00 am – 4:00 pm CST to speak with
one of our Infection Preventionists.
Slides and a recording of this presentation will be available on the Nebraska ICAP website
https://icap.nebraskamed.com/covid-19-webinars/
Learning Objectives During this series, participants should be better able to: 1. Recognize infection prevention and control issues for application of the recommendations to mitigate these issues. 2. Identify resources on infection prevention and control that will be helpful to mitigate infection prevention and control challenges. 3. Describe latest updates on COVID-19 pandemic related to infection prevention and control practices in acute and outpatient settings. Target Audience Healthcare professionals working in acute and outpatient settings. To include medical directors, nursing staff, directors of nursing, infection preventionists, quality program leaders, administrators, consultant pharmacists or other staff working in long-term care settings.

Mission and Goals To provide an educational venue that connects infection preventionists and providers from acute and outpatient facilities across Nebraska with the objective of promoting the latest research and best practices in infection prevention and control. These educational webinars are aimed to help promote and strengthen the Nebraska infection prevention and control infrastructure. The goals for this educational activity include: 1. Increase knowledge of infection control processes for acute and outpatient settings. 2. Increasing awareness of specific infection prevention and control issues that may be confronted in acute and outpatient settings. 3. Provide resources to attendees to help them with infection prevention and control efforts in their own facilities. 4. Provide resources to attendees on the most up to date COVID-19 pandemic related guidance and recommendations.

Continuing Education
1.0 Nursing Contact Hour is awarded for the LIVE viewing of this
webinar
Nebraska Medicine is approved as a provider of nursing continuing
professional development by the Midwest Multistate Division, an accredited approver by
the American Nurses Credentialing Center’s Commission on Accreditation.
In order to obtain either contact hour, you must be present for the entire live webinar
and complete the post webinar survey
No conflicts of interest were identified for any member of the planning committee,
presenters or panelists of the program content
This CE is hosted by Nebraska Medicine and UNMC along with Nebraska ICAP and
Nebraska DHHS
Continuing Education
1.0 AMA PRA Category 1 Credit™ for Physicians offered by UNMC is awarded
for the live viewing of this webinar
In support of improving patient care, University of Nebraska
Medical Center is jointly accredited by the Accreditation Council
for Continuing Medical Education (ACCME), the Accreditation
Council for Pharmacy Education (ACPE), and the American
Nurses Credentialing Center (ANCC), to provide continuing
education for the healthcare team.
The University of Nebraska Medical Center designates this live
activity for a maximum of 1 AMA PRA Category 1 Credit™.
Physicians should claim only the credit commensurate with the
extent of their participation in the activity.
Disclosure Declaration As a jointly accredited provider, the University of Nebraska Medical Center (UNMC) ensures accuracy, balance, objectivity, independence, and scientific rigor in its educational activities and is committed to protecting learners from promotion, marketing, and commercial bias. All faculty, planner and others in a position to control continuing education content participating in an accredited continuing education activity are required to disclose all financial relationships with ineligible companies. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients. The accredited provider is responsible for mitigating all relevant financial relationships in accredited continuing education. Disclosure of these commitments and/or relationships is included in these activity materials so that participants may formulate their own judgments in interpreting its content and evaluating its recommendations. This activity may include presentations in which faculty may discuss off-label and/or investigational use of pharmaceuticals or instruments not yet FDA-approved. Participants should note that the use of products outside currently FDA-approved labeling should be considered experimental and are advised to consult current prescribing information for FDA-approved indications. All materials are included with the permission of the faculty. The opinions expressed are those of the faculty and are not to be construed as those of UNMC. The accredited provider has mitigated and is disclosing identified relevant financial relationships for the following faculty, planners, and others in control of content prior to assuming their roles: FACULTY The faculty have nothing to disclose: Gary Anthone, MD Matthew Donahue, MD Ishrat Kamal-Ahmed, M.Sc., Ph.D. Daniel Brailita, MD Rebecca Martinez, BSN, BA, RN, CIC Daniel Taylor PLANNING COMMITTEE The planning committee members have nothing to disclose: Kate Tyner, RN, BSN, CIC Josette McConville, BSN, RN, CIC Margaret Deacy Jody Scebold, EdD, MSN, RN Richard Starlin, MD Sarah Stream, MPH, CDA, FADAA
Nebraska DHHS Updates
Gary Anthone, MD
Chief Medical Officer, DHHS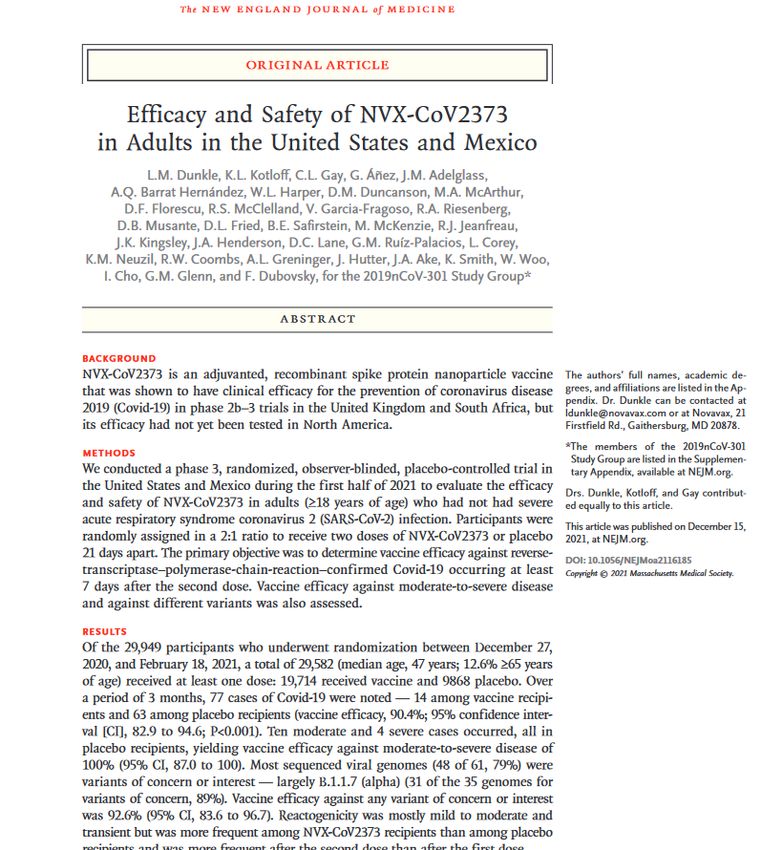
• Decrease of 112 pts (+4; +96; +37; +86; +70) • 7 Day rolling average of 16.5% (17.9; 17.5; 15.7; 13.6) • 22% of hospitalized COVID pts in ICU (20; 19; 24; 24) • 50% of COVID ICU pts on Vents (50; 57; 47; 51) • 27% of statewide ICU pts are COVID pts (29; 27; 29; 26) • Average of 66 new covid pts admitted per day (82; 88; 68; 62) • 32 Ped admits last week (31; 25; 29; 17)
Nebraska DHHS Updates
Matthew Donahue, MD
State Epidemiologist, DHHSNo additional BA.2 variants identified in NE
No BA.3 variants identified in NE
State Total
Alabama 3 Nebraska 2
Alaska 7 Nevada 3
Arizona 91 New Hampshire 7
Arkansas 1 New Jersey 6
California 96 New Mexico 1
Colorado 11 New York 26
Connecticut 8 North Carolina 15
Delaware 1 North Dakota 2
District of 1 Northern Mariana Islands 1
Columbia Ohio 18
Florida 2 Oregon 5
Georgia 2 Pennsylvania 5
Hawaii 24 Rhode Island 2
Idaho 2 Texas 21
Illinois 2 Utah 6
Indiana 17 Vermont 12
Kansas 1 Virginia 1
Louisiana 8 Washington 15
Maryland 7 Wisconsin 4
Massachusetts 64 Wyoming 1
Minnesota 7 Total 510
Mississippi 1
Missouri 1Nebraska Healthcare
Associated Infections
Program
Ishrat Kamal-Ahmed, M.Sc., Ph.D.
Healthcare Associated Infections-
Antimicrobial Resistance
EpidemiologistReport HAI/AR Event or
Organism(s) to Nebraska DHHS
https://dhhs.ne.gov/pages/Healthcare-Associated-Infections.aspx
Helping People Live Better Lives.Why use this reporting tool?
▪ Allows healthcare professionals and providers to report any healthcare-associated infections or organisms or any unusual incidence beyond
expectations with just one click of a button!
▪ Report submitted using this tool is confidential and HIPPA compliant
▪ This tool is available 24 hours a day. A report can be submitted at any time of the day or night, evenings or weekends
▪ Provides immediate notification to HAI team members when a form is completed thus eliminating phone calls/tags or emails
▪ HAI team member will contact the submitter to collect additional information and decide if further actions are warranted
▪ Ensures immediate containment while laboratory results may be pending or delayed
▪ Can be used to report suspected/confirmed HAI-related COVID-19 at acute care hospitals
Important
For those who are required to report to the state (i.e., laboratories, healthcare personnel), this tool is not a substitute for reporting mandatory
reportable disease/illness to the state.
Helping People Live Better Lives.What to report
Helping People Live Better Lives.What to report
Helping People Live Better Lives.Ishrat Kamal-Ahmed
Healthcare Associated Infections-Antimicrobial Resistance Epidemiologist
DIVISION OF PUBLIC HEALTH - EPIDEMIOLOGY & INFORMATICS UNIT
Ishrat.kamal-ahmed@Nebraska.gov
OFFICE: 402-471-7014 | CELL: 531-207-4053 | FAX: 402-471-3601
dhhs.ne.gov
@NEDH NebraskaDHHS @NEDH
HS HS
Helping People Live Better Lives.Nebraska DHHS Licensure
Daniel Taylor
DHHS Nurse Consultant / SupervisorDHHS Licensure Information New Contacts: Dan Taylor Mark Luger Phone: 402.471.2110 Email: dhhs.acutecarefacilities@nebraska.gov
Questions and Answer Session #1 Please use the QA box in the webinar platform to type a question Attendees also have the option to upvote other attendee’s questions Questions will be read aloud by the moderator A recording of the discussion will be made available on the Nebraska ICAP website Panelists: Gary Anthone, MD Matthew Donahue, MD Ishrat Kamal-Ahmed, M.Sc., Ph.D. Daniel Taylor
CDC Guidance –
2/2/22- 2/9/22 Updates
and Reminders
Rebecca Martinez, BA, BSN, RN, CIC
Infection Preventionist, NE ICAPSource Control Options Any of the below are options for source control: • N95 (NIOSH-approved N95 equivalent or higher-level respirator) • KN95 or KF94 (another country’s approved respirator like NIOSH’s N95) • Well-fitting facemask (not cloth) Reminder: • Can be worn for an entire shift if not soiled, damaged, or hard to breathe through. • When used as PPE (instead of source control) for patients in transmission-based precautions (i.e. droplet precautions for influenza); remove and discard after the patient care encounter per conventional use strategies. A new source control mask (or new PPE) should be donned. CDC - Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic Photos courtesy of Michigan.gov
Differences in Masks
Universal Respirator Use In
Some Situations
• Always follow standard precautions for all patients
• Additionally, even if the patient is not suspected to have SARS-CoV-2
infection, healthcare personnel working in counties with substantial or high
transmission should also use the below personal protective equipment (PPE):
• Eye protection for patient care encounters
• NIOSH-approved N95 respirator or higher-level respirator (i.e. PAPR) for:
• All aerosol-generating procedures (AGPs)
• Surgical procedures that might pose a higher risk of transmission if the
patient were to have SARS-CoV-2 infection such as those involving
anatomical regions where viral load might be higher (i.e. nose, throat,
oropharynx, or respiratory tract).
• Situations with additional risk factors such as poor ventilation, patients
not up to date with COVID-19 vaccinations, patients unable to use
source control, or when healthcare-associated transmission is identified.
• To simplify, facilities may consider implementing universal use of
respirators during all patient encounters or in specific units or
areas of the facility at higher risk for SARS-CoV-2 transmission.
CDC - Interim Infection Prevention and Control Recommendations for Healthcare
Personnel During the Coronavirus Disease 2019 (COVID-19) PandemicSuspected or Identified COVID-19
HAI Transmission
• Facilities should have a plan for how SARS-CoV-2 exposures in a healthcare facility
will be investigated and managed and how contact tracing will be performed.
• If healthcare-associated transmission is suspected or identified, facilities might
consider expanded testing of HCP and patients as determined by the distribution
and number of cases throughout the facility and ability to identify close contacts.
• For example, in an outpatient dialysis facility with an open treatment area,
testing should ideally include all patients and HCP.
• Depending on testing resources available or the likelihood of healthcare-
associated transmission, facilities may elect to initially expand testing only to
HCP and patients on the affected units or departments, or a particular
treatment schedule or shift, as opposed to the entire facility.
• If an expanded testing approach is taken and testing identifies additional
infections, testing should be expanded more broadly. If possible, testing
should be repeated every 3-7 days until no new cases are identified for at
least 14 days.
• Healthcare facilities responding to SARS-CoV-2 transmission within the facility
should always notify and follow the recommendations of public health authorities.
CDC - Interim Infection Prevention and Control Recommendations for Healthcare
Personnel During the Coronavirus Disease 2019 (COVID-19) PandemicCOVID FAQ Updates
How should isolation and quarantine
recommendations be applied to outpatients
and visitors in healthcare settings?
Refer to the full FAQ answer for details but key points are below:
• If infected, defer non-urgent appointments and visits until they meet criteria to
discontinue to isolation applied to patients in healthcare settings.
• If can’t be deferred, use transmission-based precautions.
• If they have had close contact and are not up to date with COVID-19 vaccinations;
• Defer non-urgent appointments and visits until they meet criteria to discontinue
to quarantine, postpone for 10 days have passed since last exposure.
• If can’t be deferred; they are to use well-fitting source control and physically
distance, HCP use full COVID-19 PPE.
• If they have had close contact and are up to date with COVID-19 vaccinations;
• Recommend deferring non-urgent appointments and visits until they meet criteria
to discontinue to quarantine, postpone for 10 days have passed since last
exposure.
• If not deferred; they are to use well-fitting source control and physically
distance. No additionally PPE for HCP.
CDC - Clinical Questions about COVID-19: Questions and AnswersIf HCP are living with someone who is diagnosed
with SARS-CoV-2 infection, should they be
excluded from work? If so, for how long?
Refer to the full FAQ answer for details but key points are below:
• HCP with exposures in the community should be managed in the same way that HCP with
exposure in a healthcare facility are managed.
• The most conservative approach is to consider the infected individual to be infectious until 10
days following their symptom onset (assuming they don’t meet criteria for longer isolation).
• HCP who are not able to avoid ongoing close contact with the infected individual while
contagious, should be managed as follows:
• If they are not up to date with all recommended COVID-19 vaccine doses, work
restriction should include the entire exposure period when their household contact is
potentially infectious (generally 10 days) and extend through the recommended
postexposure quarantine period.
• If they are up to date with all recommended COVID-19 vaccine doses, they do not require
work restriction unless they develop symptoms, test positive for SARS-CoV-2 infection,
are moderately to severely immunocompromised, or are otherwise advised to be
excluded from work by their occupational health program or public health authorities. If
these HCP continue to work, they should be tested immediately (but not earlier
than 24 hours after the initial exposure) and, if negative, again every 3 to 7 days
with the final test occurring 5 to 7 days after their last exposure.
CDC - Clinical Questions about COVID-19: Questions and AnswersCan self-tests (also known as over-the-counter or home
tests) be used when determining when healthcare
personnel (HCP) with SARS-CoV-2 infection or higher-
risk exposures may return to work?
Refer to the full FAQ answer for details but key points are below:
• Using laboratory-based or point-of-care tests are generally preferred in these
situations; these tests help ensure the test was administered correctly by a trained
provider and allow for official results to be shared with occupational health services.
• Use of self-tests might be considered in some situations; however this approach:
• May inappropriately transfer the cost of testing to HCP,
• Requires trust that HCP self-administered and interpreted the test results
correctly, and
• Requires that HCP report their own results to occupational health services.
• If self-tests are used, consideration should be given to performing a second test at
least 24 hours following an initial negative test; if negative, this increases the
confidence the HCP are not infectious. Facilities could also consider having HCP
present for a proctored test to assist with ensuring appropriate collection and
interpretation. CDC has resources to assist individuals with self-testing.
CDC - Clinical Questions about COVID-19: Questions and AnswersCOVID Testing Updates & Reminders
FDA Recall on Below Specific
COVID-19 Tests
https://www.fda.gov/medical-devices/safety-communications/stop-using-empowered-
diagnostics-covid-19-tests-fda-safety-communication?utm_source=FDAFacebookPatient Testing to End Isolation – Not
Always Required – May Be Ordered
No Retesting
No Retesting
No Retesting Required – Unless
Ordered – ID May Be Consulted
Interim Infection Prevention and Control Recommendations for Healthcare Personnel
During the Coronavirus Disease 2019 (COVID-19) Pandemic - CDCSARS-CoV-2 Disinfection Reminders
EPA - How to Use List N
Disinfectant Tips from NE ICAP
Even before the COVID-19 pandemic, it was challenging for infection preventionists (IPs) to
ensure that disinfectants for low-level disinfection (used to disinfect noncritical items that
touch intact skin) were being used according to their instructions for use (IFUs). With the
pandemic, many facilities obtained different disinfectants from their usual inventory.
As supply of disinfectants stabilizes the below are some general tips to ensure key organisms
are killed, instructions for use are known and being followed, and ease of use is a key priority.
• Institute a policy (formal or informal) that all purchasing of cleaners and disinfectants is
centralized and involves infection prevention approval.
• This can ensure only professional products are being used and that universal
disinfectants are on List N. Also ensure options are available for priority
organisms such as C. difficile and Norovirus.
• Ask your purchasing for a list of all the disinfectants purchased recently to assess what
products are within the facility.
• Categorize them by type, contact time, method, who uses, and potentially cost.
Ensure the list covers disinfection needs with a potential goal to reduce the
number of disinfectants for simplicity, increase ease of use, and avoid lengthy
contact kill times.
• Ensure that staff have competency-based training regarding disinfectant use.
• Routinely audit (monitor and document) adherence to cleaning and disinfection
procedures.Oral Antivirals
Available for
COVID-19Oral Antivirals Allocated Per
Health Department Population
• Very small amounts of oral antiviral medication are available.
• Initial supplies have been purchased by the federal government and are being
distributed to health departments proportionally based on population.
• Your local health department or district may be working with community
partners to make oral antivirals available to a limited number of pharmacies
and health systems/infusion centers.
• The below COVID-19 Public Therapeutic locator may be used to help
identify locations; however the list may change and may not be
complete or current.
• COVID-19 Public Therapeutic Locator | HealthData.gov
• Paxlovid and molnupiravir are the first oral treatments that have been approved
by the FDA for emergency use. They are indicated for early treatment (≤ 5 days
of symptom onset) of mild-to-moderate coronavirus disease (COVID-19) in
patients with positive results of direct SARS-CoV-2 viral testing, and who are at
high risk for progression to severe COVID-19, including hospitalization or
death. These oral medications are just two of the current options for early
treatment of COVID-19. Decisions on treatment will depend on patient
suitability, prioritization, and availability of each treatment.Douglas County Health Department – Oral Antiviral Communication (excerpt from 2/8/22 memo)
Vaccine Approval Updates
Daniel Brailita, MD
Assistant Professor, Division of Infectious Diseases
Associate Medical Director, Nebraska ICAPSpikevax (Moderna)- 1/31/2022- FDA approval
- 18 & Older : 2 FDA approvals
(Pfizer -Comirnaty, Moderna-Spikevax)
- 5 & Older : Pfizer is approved
2 Feb. 2022
Pfizer begins EUA process for first two
doses of its COVID-19 vaccine in children
ages 6 months to 4 years old
The FDA’s vaccine committee is
scheduled to meet on Tuesday,
February 15 to review Pfizer’s EUA
request with potential meeting of CDC
Expert Panel on February 23-24, 2022
Tue. 15 Feb.Vaccine Update- non-mRNA
Novavax – SARS-CoV-2 Recombinant Spike Protein Nanoparticle Vaccine SARS- CoV-2 rS) with Matrix-M Adjuvant
Novavax Announces Initial Omicron Cross-Reactivity Data
from COVID-19 Vaccine Booster and Adolescent Studies
Dec 22, 2021 (Company data- not CDC/FDA endorsed)
- Two-dose primary regimen of NVX-CoV2373 demonstrated cross-reactive immune responses
against Omicron (B.1.1.529) and other variants
- Third dose produced increased immune responses comparable to or exceeding levels associated
with protection in Phase 3 clinical trials
- Immune responses in adolescents were 2- to 4-fold higher than adults
- Development of Omicron-specific vaccine on track
Immune responses detail:
• Anti-spike IgG titers after Dose 3 increased 5.4-fold (prototype) to 9.3-fold (Omicron) from peak
responses seen after 2-dose primary vaccination.
– This represents a 61.1-fold (prototype) and a 73.5-fold (Omicron) increase from prior to
the Dose 3 boost.
• ACE2-inhibition titers increased 6-fold (prototype) to 19.9-fold (Omicron) compared to peak
responses following 2-dose primary series, representing a 54.4-fold (prototype), a 24.4-fold
(Delta) and a 36.3-fold (Omicron) increase from prior to the booster.
• Wild-type neutralization responses were observed after 2 doses for prototype, Delta and
Omicron. Significant increases were observed after boosting, with titers for Delta and Omicron
comparable to levels associated with protection in U.S. and Mexico and U.K. Phase 3 studies.
– After 2 doses, Omicron wild-type neutralization wasNovavax Submits Request to the U.S. FDA for Emergency Use Authorization of COVID-19 Vaccine- Jan 31, 2022 *Novavax has WHO EUL for 34 countries * Manufacturing delays and supply issues affected timeline for FDA EUA request
Questions and Answer Session #2 Please use the QA box in the webinar platform to type a question Attendees also have the option to upvote other attendee’s questions Questions will be read aloud by the moderator A recording of the discussion will be made available on the Nebraska ICAP website Panelists: Daniel Brailita, MD Richard Starlin, MD Ishrat Kamal-Ahmed, M.Sc., Ph.D. Rebecca Martinez, BA, BSN, RN, CIC Josette McConville, BSN, RN, CIC Kate Tyner, RN, BSN, CIC Sarah Stream, MPH, CDA, FADAA Jody Scebold, EdD, MSN, RN Chris Cashatt, RN, BSN, CIC
Requests?
Join us for our next webinar on February 23, 2022!
If you have suggestion(s) for future webinar
topics include them in the continuing
education (CE) survey or contact us with
your requests!
Image by rawpixel.com
Call us at 402.552.2881
Email us at nebraskaICAP@nebraskamed.com
You can also be added to our setting specific mailing lists, receive
webinar and training invites and be connected to an Infection
Preventionist that specializes in your area by filling out the contact
form at: https://nebraskamed.formstack.com/forms/icap_questionListen to New ICAP Podcasts! Twitter: @Mouthy_IP Apple Podcasts: https://podcasts.apple.com/us/podcast/the-mouthy-ip/id1573465413 Spotify: https://open.sp otify.com/show/2evXIrvZFiZFP2VZBq9cVK?si=DVhPEewJSL2xXIrDi0Y2Bg&dl_branch=1 Amazon Music: https://music.amazon.com/podcasts/2bc794ab-59af-4bbe-a8df-6a72309fa024/THE-MOUTHY-IP Podchaser: https://www.podchaser.com/podcasts/the-mouthy-ip-1955086 Twitter: @dirty_drinks Amazon Music: https://music.amazon.com/podcasts/769c29a8-1e71-46a5-9ab3-94020d7af1f7/DIRTY-DRINKS Apple Podcasts: https://podcasts.apple.com/us/podcast/dirty-drinks/id1574937193 Podchaser: https://www.podchaser.com/podcasts/dirty-drinks-1963455 Spotify: https://open.spotify.com/show/3Y8w2YVedZYnX8ZS897mU9?si=lyBNetUTTSGtlg3PmBH3Tg&dl_branch=1
ICAP Contact Info
Call 402-552-2881
Office Hours are Monday – Friday
8:00 AM - 4:00 PM Central Time
Weekends and Holidays 8:00-4:00
On-call hours are available for emergencies only
Scan the QR Code to be taken to our website
contact form. You can request a call back
from an IP, Sign up for newsletters and reminders
and request an ICAR Review for your facility.Webinar CE Process
1 Nursing Contact Hour is awarded by NE Medicine *
* Nebraska Medicine is approved as a provider of nursing continuing
professional development by the Midwest Multistate Division, an accredited
approver by the American Nurses Credentialing Center’s Commission on
Accreditation.
1 AMA PRA Category 1 CreditTM for Physicians offered by UNMC
CNE Nursing Contact Hours: AMA PRA Category 1 Credit™
➢ Completion of survey is required. Completion of survey is required.
➢ The survey must be specific to ➢ The survey must be specific to the
the individual obtaining credit. individual obtaining credit. (i.e.: 2
(i.e.: 2 people cannot be listed on people cannot be listed on the
the same survey) same survey)
➢ One certificate is issued monthly for ➢ One certificate is issued monthly for
all webinars attended all webinars attended
➢ Certificate comes directly from ICAP
via email ➢ Certificate can be downloaded from
the UNMC CCE system directly, they
➢ Certificate is mailed by/on the 15th of will email you access
the next month
➢ Survey functionality is lost on mobile ➢ Survey functionality is lost on mobile
devices devicesYou can also read

















































