Improving health outcomes - A better future for New Zealanders with KiwiHealth 2017 - assets ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Improving health outcomes A better future for New Zealanders with KiwiHealth 2017 kpmg.com/nz

We passionately believe that the
flow-on effect from focusing on
helping fuel the prosperity of our
clients significantly contributes to
ensuring that our communities,
and ultimately our country and
all New Zealanders, will enjoy
a more prosperous future.
At KPMG we are all immensely proud of the contribution
we make to the future prosperity of New Zealand. This passion
and pride is manifested in the approach with which we undertake
all our work. With KPMG you can be assured of engaging with
a team of dedicated professionals who have a wide range of
specialist expertise and knowledge, specifically tailored to help
make your organisation the success you dream it to be.
This commitment reflects our passion and belief that together
New Zealand can maximise its potential, and that by helping
inspire a market full of successful enterprises, we will in turn
inspire a country of which we can be more proud.
He waka eke noa
A canoe which we are all in with no exception
HEALTH FUNDS NEW ZEALAND / SECTION NAME
Report Sponsor
KPMG was commissioned by Health Funds Association of
New Zealand (HFANZ) to develop this discussion paper
Contact the Sponsor:
Health Funds Association of New Zealand
Level 11, Resimac House, 45 Johnston Street, Wellington
Phone: 04 499 0834
Email: admin@healthfunds.org.nz
2
Contents
04 Executive Summary
08 Introduction
10 Background
12 The cost of ill health in New Zealand
18 Designing KiwiHealth
22 Who would be eligible for KiwiHealth?
24 Exploring the impacts of KiwiHealth
29 Areas for further consideration
31 Appendix 1
34 Appendix 2
IMPROVING HEALTH OUTCOMES / CONTENTS
36 Statement of Responsibility
Purpose statement
The purpose of this discussion paper is to promotes debate around how public and private health sector participants can work
together to improve access, affordability, and outcomes of healthcare in New Zealand.
This paper highlights the importance of reducing the burden of ill health and explores options with potential to benefit
individuals, the economy and society.
It is important to note that this is not intended as a policy position ready to implement.
3
Executive
Summary
Based on current spending patterns, the cost of
public healthcare will grow from 6.3% of GDP today,
to 9.7% in 2060 – an increase of 53%.
New Zealand’s health system grow from 6.3% of GDP today While the PHI market is well placed
consistently ranks well against other to 9.7% in 2060 – an increase of 53%. to play a greater role, uptake of PHI
developed countries; both in terms is at the lowest level in recent New
Although likely to result in restricted
of efficiency (cost per capita), and Zealand history. This is partly due to
access to healthcare before reaching
effectiveness (population outcomes). this level, the increasing cost of affordability, but equally reflects
healthcare would place additional New Zealanders' reluctance to spend
However, the cost of providing this
pressure on the wider government in the short term to gain the benefits
level of healthcare is increasing,
at a later date. This phenomena is
IMPROVING HEALTH OUTCOMES / EXECUTIVE SUMMARY
potentially unsustainable, and could budget, including education and
welfare. similar to the thinking behind the
result in restricted access to
introduction of KiwiSaver, which was
public healthcare. A key driver of the increasing cost
designed to address the reluctance of
pressure is the ageing population.
Both Government and industry The number of New Zealanders over New Zealanders to save for a better
participants are now actively looking the age of 65 is projected to increase retirement while they are working.
at policy options to relieve some of to 1 in 4 by the middle of this century, This paper sets out to discuss
the inherent pressures surrounding compared to just 1 in 7 in 2013. the issue of sustainability, equity,
the cost of ill health. This paper
Additionally, the productivity of the and the need to look at innovative
explores one such initiative, referred
working-age population is threatened, ways to provide and fund healthcare
to as KiwiHealth. This initiative
as non-acute illness such as chronic in the future.
encourages both employers and
employees to adopt a more proactive disease is becoming more prevalent. In discussions on healthcare, the
and preventative approach to Despite this, most working age indirect costs of ill health are often
healthcare during the employees New Zealanders rely purely on overlooked. Indirect costs are
working years. publicly provided healthcare, with society’s overall loss to illness, most
only 28% currently covered by private notably the loss of output arising
Based on current spending patterns,
health insurance (PHI). from labour force participants exiting
the cost of public healthcare will
4
5
IMPROVING HEALTH OUTCOMES / EXECUTIVE SUMMARY
the workforce or reducing their — Mandated employer What are the expected impacts
productive hours. This discussion contributions. A healthy of KiwiHealth?
becomes more relevant in the face of workforce benefits individuals
Based on current research and initial
potential increased use of restrictions as well as employers. Indicatively,
economic modelling, the expected
in the public health system. KiwiHealth has been modelled
benefits of KiwiHealth include:
on the basis that employers offer
The direct and indirect costs of ill
a subsidy to their employees — Improved access to healthcare
health are significant. The direct cost
of up to $500 per year, should for employees. Research
of public healthcare in New Zealand
the employee wish to participate. indicates that privately-funded
was approximately $15.6 billion
elective services have significantly
in 2015/16.1 Although difficult to — Minimum policy coverage for
shorter waiting times than
quantify, the Treasury estimated the major medical events. There is
services funded publicly.
indirect cost of health to be between a promising opportunity for private
Increased access to PHI would
$4.13 and $11.56 billion in 2010.2 healthcare to contribute to better
allow for increased access to
health outcomes through easier
IMPROVING HEALTH OUTCOMES / EXECUTIVE SUMMARY
elective care - potentially leading
What is KiwiHealth? and faster access to elective
to a healthier workforce.
services. This would require all
Fundamentally, KiwiHealth would
policies to cover major medical — Reduced pressure on public
be an umbrella name for certain PHI
events at a minimum; including healthcare. Economic modelling
policies from existing health insurance
specialist appointments, advanced indicates that KiwiHealth would
providers. This approach is similar to
diagnostics and elective surgery. fund approximately 50,000
that adopted for KiwiSaver.
additional elective surgical
— Utilisation of the current PHI
The key features of KiwiHealth are procedures and between 43,000
system. KiwiHealth is designed
envisaged to include: and 70,000 'other' encounters per
to utilise the current PHI system
annum by 2027 (of which some
— No Government subsidies. as far as possible, including major
would directly substitute publicly-
While the initiative relies on policy types. This would avoid
funded procedures, and some
the Government endorsing a unnecessary administrative costs,
would be additional). In addition,
mandatory employer subsidy, and means that employers already
the social impact of reducing
the fiscal impact of the scheme offering PHI to employees would
early detection and improved
should be neutral to the Crown. be able to continue their existing
management of chronic disease
coverage and schemes.
has many non-financial benefits to
families and society.
6
Expected KiwiHealth outcomes
400,000 $224
mil ion
more people covered
50,000
more elective surgeries
in potential savings
to public health per annum
per annum Improved labour
force participation
and productivity
No government
subsidy required
— Higher productivity and less Fundamentally, KiwiHealth
absenteeism and presenteeism. would be an umbrella name
With increased access to
elective care, early detection for certain PHI policies from
and intervention is more likely to existing health insurance
occur. With the right preventative providers. This approach is
treatments, this has the potential
similar to that adopted for
to reduce the burden of ill health
in future years. KiwiSaver.
Further considerations From an economic standpoint, the
The costs of KiwiHealth principally option of doing nothing and relying
relates to the insurance premiums, on publicly-funded healthcare simply
which are made up of the employer ignores an already evident trend, and
IMPROVING HEALTH OUTCOMES / EXECUTIVE SUMMARY
subsidy and the employee contribution. shifts the financial burden to future
While significant, the employer generations.
contribution is partly offset by reduced It is therefore important to highlight
absenteeism and presenteeism, these issues and set out the
increased workforce productivity, and options in order to stimulate policy
over time, wage absorption. debate in the health sector and
As with any policy initiative, there Government, whilst at the same time
are some limitations that will understanding the potential costs and
need further consideration. These benefits to New Zealanders.
include the impact on individuals
in part-time employment, those
who are self-employed, or those
performing non-market activities
such as looking after children or the
elderly. In addition, the distributional
effects of further improving access
to healthcare to those who already
have comparatively easier access, as 1
http://www.treasury.govt.nz/government/ex-
penditure/health
a means of relieving pressure on the 2
Treasury (2010), The Cost of Ill Health, New
public system, must be debated. Zealand Treasury Working Paper 10/04
7
Introduction
The New Zealand health system consistently
ranks well against other developed countries,
both in terms of efficiency (cost per capita) and
effectiveness (population outcomes). It provides
IMPROVING HEALTH OUTCOMES / INTRODUCTION
wide access to healthcare at low or no cost to
New Zealanders, with Accident Compensation
Corporation (ACC) covering accidental injury, and
private healthcare playing a complementary role
through providing access to specialist services.
8
This paper explores whether there PHI alone cannot address all the Approach
is an opportunity for PHI to play a problems that will face the public
This paper takes a high level
greater role in providing access to health system in the future. However,
approach to addressing the growing
some health services; in order to it may be effective at facilitating
demand and cost of healthcare in
improve individual health outcomes greater access to some services.
New Zealand and sets out to:
and reduce or redirect costs away
from the public health system. Objectives — Define the “problem” by
assessing the current state and
There are a number of external The key objectives of this paper
examining both direct and indirect
factors that will affect the health are to:
costs of healthcare;
system in the coming years. Like the
— Explore opportunities for PHI to
rest of the developed world, New — Outline a high level policy option
increasingly complement the public
Zealand’s population is ageing. The for consideration by Government
healthcare system and improve
first cohort of “baby boomers” retired and health sector participants; and
individual health outcomes;
IMPROVING HEALTH OUTCOMES / INTRODUCTION
in 2011 and the next 20 years will see
— Identify the key benefits and costs
a dramatic change in the distribution — Outline a policy option that could
of the proposed policy option,
of New Zealand’s population. encourage greater uptake of PHI
including distributional effects
New Zealand is also experiencing in New Zealand; and
(i.e. who benefits most vs who is
an increase in the prevalence of
— Assess the impacts of the excluded) where appropriate.
chronic disease such as obesity and
proposed policy option on
diabetes, cardiovascular disease This paper is based on domestic and
individuals, the public health
and arthritis. The combination of international research and supported
system and the economy as
demographic change and growing by econometric modeling.
a whole.
prevalence of chronic disease will
affect New Zealand in a number of
ways, including a greater demand for
healthcare services. This will place
additional pressure on the public
health system.
9
IMPROVING HEALTH OUTCOMES / BACKGROUND
10
BackgroundWhat is the problem? to make relatively small decisions
When faced with day-to-day with insignificant immediate benefits,
Like other developed countries,
financial decisions, many and so avoid underestimating the
New Zealand’s health system is
long-term value of an investment in
experiencing a number of social and individuals and New Zealand
personal health and wellbeing.
technological trends that will increase families delay expenditure As with retirement savings (where the
the future cost of healthcare services
on healthcare, including government intervened by introducing
to a point where it may become
health insurance. KiwiSaver), the government plays
unsustainable to offer universal
an important role in avoiding what
healthcare to all New Zealanders.
economists may term ‘market failure’.
Traditionally, New Zealand has relied An additional, increasingly relevant
on rationing public healthcare to problem is the way in which public The problem of Status Quo
manage demand, using techniques healthcare is provided. Publicly-
funded care tends to focus on the Long-term sustainability of the
such as:
severity of illness and those with the New Zealand health system is unlikely
— Minimum thresholds. This highest treatment need. Whilst this is to be achieved by relying on the status
involves prioritising individuals with understandable, it can often overlook quo; where public healthcare, ACC,
high needs over those with less the benefits of early diagnosis and private healthcare (funding and
severe conditions; and intervention, prevention and provision) simply co-exist.
— Managed access and capacity. disease management. There appears plenty of scope for
Restricting the range and location public agencies, ACC, and private
of services provided by the Why don’t people take more participants to work together to
publicly-funded system; such responsibility for their own identify ways to better manage
as pharmaceuticals or weight healthcare? chronic disease; deploy human and
loss surgery. Health policy and funding has physical capital more efficiently;
often struggled to tackle the wider and encourage New Zealanders
— Reliance on co-payments.
economic impact of ill health to to become engaged in their own
Basic healthcare services, such as
individuals, employers and the public healthcare. This highlights the
primary care and pharmaceuticals,
health sector; and identify ways for importance of seeking shared long-
attract co-payments, with the
aim of promoting individual individuals, families and wha-nau term solutions, as well as promoting
to become more engaged in their innovation in healthcare funding
responsibility among the adult
own health. and delivery.
population.
The public health system has a When faced with day-to-day financial
limited ability to vary co-payments decisions, many individuals and New
as a funding source without creating Zealand families delay expenditure on
serious inequities. This particularly healthcare, including health insurance.
applies to secondary and tertiary For many, this is simply a question
care or high-cost community care. of affordability; for others, it is a
By comparison, the PHI market has
IMPROVING HEALTH OUTCOMES / BACKGROUND
belief that publicly funded healthcare
created a range of policy options services are sufficient. For most, it is
which give consumers choice on the simply a decision they delay.
level of care and co-payment received.
In economic terms, this is often
Increased use of rationing tools in referred to as ‘under-investment’, or
the public health system directly ‘savings-behaviour’, and is similar
impacts on New Zealanders’ ability in nature to the problem faced by
to access healthcare and comes government policymakers when
with a significant cost to society. considering the introduction of
Any increased rationing of healthcare KiwiSaver. Similar to KiwiSaver, the
services, would widen the gap challenge is to encourage individuals
between those who can access
private healthcare out of their own
pocket – and those who can’t.
By universal healthcare, we mean that all New Zealanders have access to the full range of effective health
services they need to: be well; stay well; and get well without being exposed to financial hardship.
11The cost of il health
in New Zealand
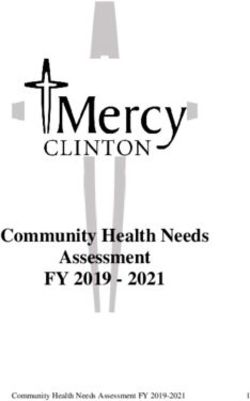
Figure 1. The Cost of ill health
DIRECT COSTS INDIRECT COSTS
Lost output as
a result of…
IMPROVING HEALTH OUTCOMES / THE COST OF ILL HEALTH IN NEW ZEALAND
Hospital
inpatient costs
…labour force …non labour force
participants… participants…
…being away …being less
…working fewer …not participating
from work productive at work
hours due to ill health
(absenteeism) (presenteeism)
Figure 1 is a reconstruction from Treasury (2010) The Cost of Ill Health, and provides an
overview of the wider cost of ill health to New Zealand.
12The cost of ill health includes both the
direct cost of healthcare, such as treatment
and rehabilitation; and the indirect costs
to society and the economy through lost
productivity and quality of life.
The direct cost of ill health — Co-payments in primary care. — A rapidly ageing population.
Co-payments for primary care, In 2013, 1 in 7 New Zealanders
The New Zealand health system
pharmaceuticals, and some ACC were over the age of 65. This is
is underpinned by three pillars: the
services are used to manage projected to increase to 1 in 4
public health system, ACC, and
demand and promote individual by the middle of this century.
private care. Chief among these
responsibility amongst the
is the public health system, which — Growth in chronic disease.
adult population.6
accounts for approximately 83% of The prevalence of certain
all health related expenditure.5 The — Income and asset testing for chronic conditions, such as
remainder is made up of PHI, out- Aged Care. All people assessed obesity related cardiovascular
of-pocket payments, and charitable for Age Related Residential Care disease and diabetes, have been
contributions. Supported by ACC and (ARRC) are income and asset increasing across the New Zealand
private care, New Zealand’s health tested; with those above the population in recent years; leading
system is relatively efficient and threshold paying for their own care to greater demand for often
delivers outcomes in line with other up to a maximum cost per week. specialist and/or expensive
IMPROVING HEALTH OUTCOMES / THE COST OF ILL HEALTH IN NEW ZEALAND
developed countries. health services.
With growing demand and
While direct costs are most expectations, it is unlikely that — The cost of new treatments
commonly seen as the cost of these policy levers will be sufficient and technology. These costs are
providing hospital care (as highlighted to manage the future demand for driven both by the increased cost
in Figure 1) they are significantly healthcare. Recent research by the of newly-developed treatments
broader than this. Direct costs also New Zealand Treasury indicates and pharmaceuticals (e.g. the
include primary care, maternity, that, were we to continue with our Keytruda cancer treatment drug),
community care, disability support, current spending pattern, the direct and greater access to care (e.g.
aged care, and some oral health. cost of public healthcare will increase bowel screening), as well as the
District Health Boards are mandated from around 6.3% of GDP today cost of technology enhancement.
to manage the demand and cost of to 9.7% in 2060.7 This equates in
— Rising expectations.
care through the introduction of: real terms to an increase of 53% in
New Zealanders have rising
direct expenditure, raising significant
— Minimum access thresholds expectations regarding the type
questions around sustainability. Key
for elective care. A points system and extent of care they receive.
drivers of this growth include:
is used to prioritise care towards
individuals with high needs, and
exclude those with conditions
less severe.
5
OECD.stats
6
Note that the ACC does not restrict access in
the same way as DHBs, but use a co-payment
system.
7
Treasury (2016), He Tirohanga Mokopuna, 2016
Statement on the long term fiscal position. Note
the projections represent ‘what if’ scenarios
based on historic spending patterns.
13The indirect cost of ill health concluded that 26.4% of Australians studies is that ill health is a primary
employed full-time suffered from barrier to workforce participation in
The cost of ill health in New Zealand
chronic disease, and 11.7% of this age group. Improved healthcare
is not limited to the direct costs
part-time employees also have a and prevention would be likely to
to the health system. Poor health
IMPROVING HEALTH OUTCOMES / THE COST OF ILL HEALTH IN NEW ZEALAND
chronic condition. Overall, 8.8% have a positive economic impact;
may mean some individuals are
reported losing productive life years reminding us that healthcare, is in fact
less productive while they are
(PLY) due to their conditions. an investment in keeping our people
at work, work fewer hours to
A further 6.4% of 45-64 year olds healthy and able to participate in the
manage their condition, or miss
were not in the workforce due to workforce and society.
work altogether. This can affect
their chronic condition9. This research
the individual’s career prospects,
highlights that a person out of the
and reduce the productivity of
labour force due to chronic disease
the employer organisation. It can
earned less than one quarter of a
also place additional costs on the
full-time employee, and less than one
employers, who have to cover the
half of a part-time employee. People This paper acknowledges the benefits of
costs of absent staff. Poor health addressing the impact of ill health using either
out of the workforce due to ill health Quality Adjusted Life Years (QALY) or Disability
may also prevent some people Adjusted Life Years (DALY), but does not
also paid 99.94% less tax compared
from participating in the workforce, explicitly model these.
to those who were employed 8
Treasury (2010) The Cost of Ill Health, New
which affects New Zealand’s Zealand Treasury Working Paper 10/04.
full-time10. Interestingly, the leading Schofield, D, et al. (2016), Economic costs
immediate and longer-term
9
chronic conditions associated with of chronic disease through lost productive
economic growth prospects. life years (PLYs) among Australians aged
premature exit from the labour force 45–64 years from 2015 to 2030: results from a
Quantifying the indirect cost is were back problems, arthritis, and microsimulation model.
10
Schofield, D et al. (2011), Economic impacts
complicated, with the Treasury mental and behavioural problems, of illness in older workers: quantifying the
estimating these costs to be as illustrated in Table 111. impact of illness on income, tax revenue and
government spending.
between $4.13 and $11.56 billion 11
Schofield, D et al. (2015), Lost productive
In these studies, the resultant loss on life years caused by chronic conditions in
in 2011.8 Australians aged 45-64 years, 2010-2030.
income, increase in welfare support, 12
Schofield D, et al. (2017), The costs of diabetes
Recent research into the economic and loss of taxation was estimated to among Australians aged 45–64 years from
be AU$20.6 billion12. The equivalent 2015 to 2030: projections of lost productive
cost of chronic disease highlights the life years (PLYs), lost personal income, lost
indirect cost of ill health. Focusing on data is not available for New Zealand; taxation revenue, extra welfare payments
and lost gross domestic product from
the 45-64 year age group, the study however the broad conclusion of these Health&WealthMOD2030.
14Table 1. Reasons people are not in the workforce (Aged 45-64) in Australia
01 Back Problems (dorsopathies)
22.16%
02 Arthritis
15.06%
03 Mental and behavioural disorders
10.14%
04 Cardiovascular disease
6.81%
54.17%
05 Depression
(excluding post natal depression)
6.81%
06 Injury/accident
5.65%
IMPROVING HEALTH OUTCOMES / THE COST OF ILL HEALTH IN NEW ZEALAND
07 Diseases of the nervous system
5.72%
08 Other diseases of the musculoskeletal
systems and connective tissue
5.36%
09 Cancer
3.62%
10 Diabetes
3.33%
15IMPROVING HEALTH OUTCOMES / THE COST OF ILL HEALTH IN NEW ZEALAND 16
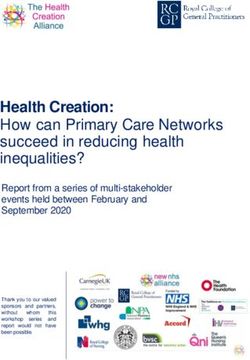
Figure 2. Average wait times for elective surgery from first GP visit13
177 76
Days public Days private
healthcare healthcare
13
TNS (2016) Assessing the demand for Elective Surgery amongst New Zealanders March 2016
Reducing the cost of ill health As illustrated in Figure 2, a recent
survey suggests that individuals
Currently, the private health sector
receiving publicly-funded surgeries
provides access to non-acute health
wait on average 101 days longer for
services. Predominantly, these
IMPROVING HEALTH OUTCOMES / THE COST OF ILL HEALTH IN NEW ZEALAND
surgery than those who have access
include specialist appointments,
to private healthcare13.
diagnostics and elective surgery.
The private sector complements the The next section explores how the
public system by providing access Government could encourage greater
to services that may be restricted by health insurance uptake without
treatment thresholds, waiting times, the use of public funds; provides a
co-payments, and capacity limits in potential high-level design of the
the public system. scheme; and outlines the benefits
and costs of greater PHI uptake.
By increasing access to elective
services, PHI can support individuals
to maximise their workplace
participation and economic
contribution and improve quality of
life. Therefore, improving access to
elective services is a channel through
which PHI can contribute to reducing
or avoiding the long-term cost of ill
health in New Zealand.
17IMPROVING HEALTH OUTCOMES / DESIGNING KIWIHEALTH 18
Designing
KiwiHealth
The primary objective of KiwiHealth is
to support working New Zealanders to
maximise labour force participation by
reducing the impacts of ill health.
What is KiwiHealth? — Mandated employer
contributions. A healthy
Like KiwiSaver, KiwiHealth would
workforce benefits individuals
be a government-endorsed, but
as well as employers. Indicatively,
employer-subsidised scheme.
a scheme has been modelled
Previous research has explored
where employers offer a subsidy
several types of interventions aimed
IMPROVING HEALTH OUTCOMES / DESIGNING KIWIHEALTH
to their employees of up to $500
at increasing the level of PHI in
per year (CPI adjusted), should the
New Zealand, and most options have
employee wish to participate.
included some form of a Government
subsidy or tax relief. However, — Minimum policy coverage:
this would not address the problem There is a promising opportunity
of fiscal sustainability. for private healthcare to
contribute to better health
The key characteristics of
outcomes through easier and
KiwiHealth are:
faster access to elective surgery.
— No Government subsidies. This would require all policies to
While the KiwiHealth policy relies cover major medical events at
on the Government endorsing a a minimum; including specialist
mandatory employer subsidy, appointments, advanced
the fiscal impact of the scheme diagnostics and elective surgery.
is neutral.
— Utilisation of the current
PHI system. Utilising the current
PHI system as far as possible
would avoid unnecessary
administrative costs.
19IMPROVING HEALTH OUTCOMES / DESIGNING KIWIHEALTH 20
Table 2: Elasticity of demand for PHI by subsidy level
10%
5.4%
20%
10.8%
50%
27%
Decrease in price Corresponding increase in demand
What is the role of Government? — To target passive decision
making. A key concept behind
Government endorsement is central
KiwiSaver and KiwiHealth is that
to the success of KiwiHealth.
individuals are more likely to join
Although not financially subsidising
and stay in a scheme if they are
the scheme, government involvement
automatically enrolled. Research
is important for the following reasons:
based on a series of decision-
— To reduce the risk of making experiments show that
under-investment. individuals disproportionately
Government plays an important remain with the status quo.16 This
role in directing proactive decision- is a key behavioural economics
making. Without government theory that was used in the
endorsement, there is a high risk development of KiwiSaver, most
there would be a low uptake for notably the auto-enrolment aspect
KiwiHealth. In economic terms, of the scheme.
the reason for this is referred to
— To mandate the incentive.
as ‘under-investment’, or ‘savings-
A further reason for government
behaviour’. These terms refer to
involvement is to mandate that
the common behavioural traits
employers offer an incentive
where individuals defer decisions
by way of subsidy, specifically
by focusing on immediate costs
targeted to PHI. The anticipated
IMPROVING HEALTH OUTCOMES / DESIGNING KIWIHEALTH
rather than future benefits.15
effect of an incentive builds on
Traditionally, government has
the relationship between the
played an important role in
price of a good or service and
identifying ways to avoid under-
the corresponding demand i.e.
investment, and should be
elasticity of demand. The exact
considered as an important feature
relationship depends on the type
of KiwiHealth.
of goods/service. Table 2 show
the relationship specific to PHI,
based on an elasticity of demand
of -0.54.14
14
NZIER (2014), Private health insurance - An
expanding role in the future of health care?
NZIER report to HFANZ.
The Treasury (2002), Treasury Report: Costs of
Subsidising Private Health Insurance.
NZIER (2001), The tax treatment of health
insurance premiums. Report to HFANZ.
15
Samuelson, W. & Zeckhauser, R. J (1988), Risk
and Uncertainty.
16
Benartzi, Shlomo; Thaler, Richard H (2007),
Heuristics and Biases in Retirement Savings
Behaviour.
21Who would be
eligible for KiwiHealth?
Fundamentally, KiwiHealth needs
to be available to all employees. It is
anticipated that pre-existing conditions
would be covered with an appropriate
stand down period.
IMPROVING HEALTH OUTCOMES / WHO WOULD BE ELIGIBLE FOR KIWIHEALTH?
This section outlines the potential acceptance of pre-existing conditions. What services would
enrolment parameters for While the actuarial implications of Kiwihealth cover?
KiwiHealth as a starting point this significant cover is out of scope
It is anticipated that an eligible
for further discussion. for this report, it is anticipated that
KiwiHealth policy would, at a
pre-existing conditions would be
minimum, cover ‘major medical’
How are people enrolled? accepted with an appropriate
events. One option is to design a
stand-down period – similar to that
Assuming Government support, there base policy based on current Major
of current PHI solutions.
are two key models for enrolment: Medical schemes, with the option to
increase the cover to match current
— automatic enrolment (opt-out) or Are there exceptions to
Comprehensive policies.
Kiwihealth?
— employee driven enrolment (opt-in).
Table 3 summarises the key public
It is potentially beneficial to allow
An opt-out scheme would most policy considerations when selecting
small business to be exempt from
effectively target passive decision the level of cover in KiwiHealth
the scheme. Granting businesses
making. A less aggressive approach, compared to a 'do nothing' scenario.
with between 1 and 5 employees
would be an opt-in scheme.
exemption would (based on 2015
data) exclude about 229,000
Would pre-existing conditions
employees.18 Consideration will
be covered?
also have to be given to part-time
Fundamentally, KiwiHealth needs to employees, temporary staff and
be available to all employees, on the contract workers. This has been
basis that all employers are mandated considered in the underlying
to subsidise the scheme. This econometric modelling.
raises an important question around 18
Ministry of Business, Innovation and Employment
(2015), Small Businesses in New Zealand
22Table 3. KiwiHealth policy options
Key benefits Policy Considerations
Major Medical Cover — Increased access to elective — Public healthcare will still need to
surgery and specialist manage the more severe cases
consultations
— Surgeries offered privately may not
— Patients spend less time waiting increase productivity
for surgery and are therefore
more productive
Comprehensive Cover — Increased access to elective — Public healthcare will still need to
surgery and specialist manage the more severe cases
consultations
— Private provision of primary care is
— Patients spend less time waiting often found to be demand-inducing
for surgery and are therefore
more productive — C omprehensive Care is less
affordable than the Major Medical
— Co-payments covered option
— Increased access to primary — Employers should only need to
care, and increased chances of subsidise base level care
early intervention
— Potentially higher impact on
productivity
Do nothing — Workforce participants are not — Waiting times increase more rapidly
treated differently to other
New Zealanders — Loss of productivity due to
absenteeism and presenteeism
— No ‘deadweight cost’ of (for cases that could otherwise
administering PHI schemes have been avoided)
— Further increased pressure on
public healthcare
IMPROVING HEALTH OUTCOMES / WHO WOULD BE ELIGIBLE FOR KIWIHEALTH?
What would happen to existing this subsidy would cover between How is KiwiHealth structured?
employer subsidised schemes? 20% and 50% of the target working
There are a number of employer-
population's average premium.
Where employers already offer subsidised health insurance schemes
existing cover, it is envisaged that The employer contribution needs to be already established in New Zealand.
these schemes would automatically significant enough to effectively drive This provides KiwiHealth with a
become approved or accredited uptake of KiwHealth while keeping the readily available administrative
KiwiHealth schemes. This would cost of labour sustainable. In effect, structure. Building on this would
avoid disruption and encourage however, the employer contribution minimise the administrative effort
employers to provide subsidies over would likely be absorbed by the required to initiate and manage
and above the minimum. employee over the long term; as many the scheme.
employers would likely, over time,
Who pays and what is the cost? include the KiwiHealth subsidy in the
total remuneration package.
In short, both employers and
employees would pay for KiwiHealth The real effect is for minimum wage
policies, with the major change being earners whose salaries would not
the obligated employer contributions. be able to absorb the contribution. A
$500 subsidy would therefore mean
In order to model KiwiHealth, it
a 1.6% salary increase for a full-time
was assumed that the employer
worker earning the minimum wage.
contribution matches the employee
contribution dollar for dollar, up to
a maximum subsidy of $500; with
the employee funding any remaining
cost. Based on current price levels,
23Exploring the
impacts of
KiwiHealth
Econometric modelling suggests that
50,000 additional elective surgeries could
be funded by PHI under KiwiHealth, at an
estimated value of $234 million.
IMPROVING HEALTH OUTCOMES / EXPLORING THE IMPACTS OF KIWIHEALTH
This section explores the benefits and The analysis is based on a number
costs of KiwiHealth on individuals, of assumptions.
the economy, and the public health
Firstly, the uptake rate is modeled
system. The policy analysis is based
based on the assumed impact of the
on domestic and international literature
employer contribution.
and econometric modeling. The policy
is designed at a high level, with the Secondly, chronic disease and other
purpose of evaluating key implications existing health problems may not be
of increasing the level of PHI in accurately reflected in the model or
New Zealand. incorporated in the assumed health of
new policy holders.
The underlying econometric model
used for this analysis is based on two Lastly, the claim to premium ratio,
key sources of data: demographic number of claims, and elective
data from Statistics NZ, and historical surgeries funded by PHI, are all
PHI industry data provided by based on historical trends. These
HFANZ. The key assumptions and assumptions may not accurately
sources of data are listed in Appendix predict the future.
1. Outputs are modeled over a 20-
year period to accommodate uptake
over time and labour force growth.
24What are the benefits For an individual accessing public For individuals, increased access
to the individual? healthcare only, this could mean to healthcare and the subsequent
an extra:19 reduced absenteeism and
The key benefit to individuals under
presenteeism could decrease:
KiwiHealth is greater access to PHI — 101 days with increased risk of
and therefore, greater access to being away from work due to the — The risk of missing out on
healthcare. Access can be assessed condition (absenteeism); and/or opportunities in the workplace;
in terms of:
— 101 days with increased risk — Financial stress and general
— Choice. Improving choice around of being less productive while anxiety linked to missing out
the type of treatment, the location at work due to the condition on work because of treatable
IMPROVING HEALTH OUTCOMES / EXPLORING THE IMPACTS OF KIWIHEALTH
for treatment, and the range of (presenteeism). conditions; and
pharmaceuticals offered.
— Higher risk of the condition — Other social impacts on family
— Thresholds. Improving access increasing in severity while waiting and community.
to healthcare for those conditions for surgery.
International research indicates a
where there is a treatment benefit,
A key driver of the cost of healthcare connection between sick leave and
but they would not currently meet
is rising expectations. Patients are a worker’s earning potential. A study
the public sector thresholds (most
increasingly well informed, and more on the casual effect of sick leave on
importantly elective surgery).
often have specific demands about subsequent employment and earnings
— Time. Reducing the time it takes the care they receive and when they found that a 1% increase in a worker’s
to access diagnostics, specialist receive it. Many countries have found sick leave reduced the worker’s
advice, and treatment (e.g. First private healthcare to be effective at earnings by 1.2% two years later21.
Specialist Assessment (FSA)). responding to patient demands for
new or more specialised services20.
The provision of elective surgery is
This means that private healthcare, to a
the most commonly cited example
larger extent, can allow consumers to
of the rationing system and resulting
tailor services to their specific needs.
waiting times for treatment. Recent
research identified a difference of
101 days between private and public
provision of elective surgery.19 Note 19
TNS (2016), op.cit.
that this excludes patients who fall *Note: this is unlikely to be the case for all condi-
below the public threshold altogether, tions that require surgery.
20
Colombo, F. and N. Tapay (2004),Private Health
and are not placed on a waiting list. Insurance in OECD Countries: The Benefits and
Costs for Individuals and Health Systems
21
Markussen, S (2011), The individual cost of sick
leave, journal of population economics
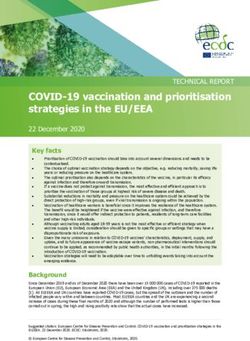
25Figure 3. Total number of (additional) claims under KiwiHealth (Scenario 1)
120,000
100,000
Number of claims
80,000
60,000
40,000
20,000
-
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
2036
Year
Other Elective surgeries
Distributional impacts Zealanders who can afford to pay for reduce or halt a conditions’ severity,
a PHI policy than those who can pay and thereby keep individuals with
The New Zealand working
for a major medical event out of their long term diseases healthier for
population – and in particular, those
own pocket. longer. This could lessen the long
in stable careers – would benefit
term burden of chronic disease.
from KiwiHealth.
Impact on the public health
While subsidised by employers, there system Impact on employers and the
is a risk that some New Zealanders, wider economy
The key benefit to the public
such as those in lower income
health system is the potential to Recent research indicates that
brackets and ‘high-risk individuals’
lighten the burden of specialist employees with subsidised health
IMPROVING HEALTH OUTCOMES / EXPLORING THE IMPACTS OF KIWIHEALTH
who are charged higher premiums,
assessments, high cost diagnostics, insurance, on average, take one less
would still not be able to afford PHI.
and elective surgeries. sick day per year23. Econometric
This risk may be partially offset as
modelling shows that this would
uptake increases, policy offerings As illustrated by Figure 3,
mean an additional 400,000 sick days
become competitive, and insurers econometric modelling suggests
saved per annum by 2027.
pool risk and ensure competitively- that about 50,000 additional elective
priced premiums. Additionally, there surgeries would be funded by PHI The same survey estimates the
is a portion of the population who under KiwiHealth in the year 2027, at median direct cost of sick leave
may not be eligible, such as people an estimated value of $234 million at (e.g. overtime payments and hire
out of the workforce, those in part the standard case weight price22. This of temporary staff) to be $131 per
time work, and the self-employed. is in addition to the current level of employee per day. As illustrated in
This is accommodated by the surgeries funded by PHI. Figure 4, the additional uptake under
uptake model, but worthy of KiwiHealth would result in more than
It is expected that surgeries funded
further consideration. $52 million in savings to employers
by PHI will fall into two categories:
per annum by 2027.
When considering the distributional those who substitute publicly-
impacts of KiwiHealth, and whether funded surgeries, and those that are
PHI is, or could be affordable, we additional (i.e. under the threshold
should not only compare PHI against for public provision). Although the
the equity within public healthcare. first category represents the direct
If an individual can realise benefits beneficial impact on the public health
from accessing the private health system, it is probable that the second
system, considerations should be category will be beneficial in the
given to the way in which as many long term by reducing the burden of 22
Based on a New Zealand Weighted Inlier Event
as possible can do so. With this in chronic disease. Pro-active access to Separation (WIESNZ16) cost weight value at
2016/17 price of $4,681.97 per WIES]
mind; there is a larger portion of New elective surgery has the potential to 23
TNS (2016), Assessing the demand for Elective
Surgery amongst New Zealanders March 2016
26Figure 4. Estimated savings from reduced direct costs of sick leave
$60m
$50m
$40m
NZ $
$30m
$20m
$10m
$00m
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
2036
Year
The direct cost of sick leave does have PHI cover. However, many
not account for productivity lost to already receive voluntary employer
absenteeism and presenteeism. With subsidies. In the long run, this
reference to Treasury’s working paper subsidy would likely be absorbed by
on the indirect cost of ill health, we the total remuneration package.
note that while quantifying this effect
In addition to reducing the economic
is challenging, there is no doubt it
cost of ill health, and improving
exists and that employers could
labour force participation, this focus
gain significant productivity from a
on prevention and early intervention
healthier workforce.
may have wider benefits to society.
IMPROVING HEALTH OUTCOMES / EXPLORING THE IMPACTS OF KIWIHEALTH
Lost productive life years (PLY) due
Recent research indicates that to chronic disease is associated with:
employees with subsidised — Lost income, and lost tax
health insurance, on average, — Increased welfare payments24
take one less sick day per
— Illness-related early retirement25
year23. Econometric modelling
shows that this would mean an In Australia this has raised calls for
“…greater investment in effective
additional 400,000 sick days preventative health interventions
saved per annum by 2027. which improve workers’ health and
work capacity.”26
What is the cost of KiwiHealth? There remains some debate whether
these benefits will amount to a net
The cost of KiwiHealth is up to
economic benefit; and whether
$500 per annum per employee,
this accrues to the employer, the
and this cost would apply to both
individual, or to the Crown. This
new and existing PHI policies.
highlights the need for New Zealand-
Employers would therefore suffer
specific research in this area.
a deadweight cost of subsidising
the approximate 1.1 million working
age New Zealanders who already
24
Schofield D, et al. BMJ Open 2017;7:e013158.
doi:10.1136/bmjopen-2016-013158
25
Schofield et al. BMC Public Health 2011, 11:418
26
Schofield, Op Cit, BMJ Open
27Figure 5. Employer/employee contributions
900m
700m
500m
NZ $
300m
100m
0
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
2036
Year
Employee Employer
Conclusion The analysis in this report shows that
even a conservative uptake of the
With a rapidly increasing cost pressure
scheme could significantly increase
in the New Zealand health system,
the number of elective services
now is the time to consider options
funded by PHI. This would in turn
around how to afford future care.
take pressure off the public health
KiwiHealth as a policy option system, decrease waiting time for
is fundamentally based on the elective care, and contribute towards
complementary relationship between keeping New Zealanders healthy
the public and private healthcare and productive.
IMPROVING HEALTH OUTCOMES / EXPLORING THE IMPACTS OF KIWIHEALTH
systems. Increasing access to
insurance means increasing access to
healthcare, which results in significant
benefits to the individual; employee
and to society; especially in the
provision of elective services and
management of chronic disease.
28Areas for further
consideration
KiwiHealth is a way of opening up a
broader discussion between public
and private healthcare industry
participants, with a common goal of
improving outcomes and creating a
more productive economy.
IMPROVING HEALTH OUTCOMES / EXPLORING THE IMPACTS OF KIWIHEALTH
There are a number of important tied to their workplace). These — Employers absorption of
areas outside the scope of this report types of schemes have a long subsidies. As with KiwiSaver, it is
that should be considered further. history in New Zealand, and are likely that PHI subsidies over time
This includes a more detailed policy considered effective in the way would be absorbed in the total
design, such as: they pool premiums across a remuneration package. There is an
workplace. They could, however, opportunity to further investigate
— Minimum policy coverage and
limit portability of policies (i.e. the impacts of this effect.
the link to New Zealanders’
an employee's opportunity to
productivity. There is an — Fringe Benefit Tax (FBT). PHI
retain PHI cover when changing
opportunity to further investigate benefits both employers and
employer). There is an opportunity
specific gaps in healthcare among employees. As with certain other
to investigate the impacts of
New Zealanders and ensure that employer-subsidised services
these schemes.
the healthcare services required to (e.g. optometry) there may be an
target these would be included in — Quantifying the cost of ill argument for exempting a portion
eligible KiwiHealth policies. health. Further quantification of of the subsidy from FBT.
the cost of ill health, and more
— Workplace Based Schemes.
specifically the costs that could
There are currently a significant
be avoided with more targeted
number of employer-provided
healthcare would be valuable.
health insurance schemes in
While this is difficult to quantify,
the market (where an employer
it would be beneficial in order
offers employees the opportunity
to assess the effects of a
to join a specific PHI scheme
potential scheme.
29IMPROVING HEALTH OUTCOMES / APPENDIX 1 30
Appendix 1
The econometric model is based on the
following key assumptions:
Table A1. The key variables used in the econometric modeling were uptake of Kiwi Saver
based on elasticity of demand, historical PHI claim rates, and demographic growth from
Statistics NZ.
Total uptake rate: Number Population Uptake of each policy:
of claims growth:
lodged:
Scenario 1 Rate based on Historical NZ Stats 70% Major Medical
elasticity of average projections: 30% Comprehensive
demand. Reaching 50th percentile
55% of the labour
force by 2027
Scenario 2 As above As above As above 50% Major Medical
50% Comprehensive
Table A2. Further data supporting the model and their sources are listed below.
Data Source
Labour force estimates (historic) NZ.Stats, data extracted on 09 Feb 2017 03:34 UTC (GMT)
IMPROVING HEALTH OUTCOMES / APPENDIX 1
Labour force projections NZ.Stats, data extracted on 16 Jan 2017 02:23 UTC (GMT)
Unemployment rates NZ.Stats, 10 year averages
Price of policies Estimates based on current Southern Cross premiums.
Claim incidence rates
Estimates based on historic HFANZ provided industry data
(and number of claims)
Premium-to-claim ratios Estimates based on histtoric HFANZ provided industry data
31Outcomes of Modelling:
Figure A1: Number of lives covered (with KiwiHealth) over time
1,600,000
Lives covered by health insurance
1,400,000
1,200,000
1,000,000
800,000
600,000
400,000
200,000
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
2036
Year
Number of lives covered
Figure A1 shows the growth in PHI uptake under KiwiHealth, which is estimated to be up to 400,000 additional
lives covered by 2028.
Figure A2: New lives covered (scenario 1)
600,000
500,000
New lives covered
400,000
300,000
IMPROVING HEALTH OUTCOMES / APPENDIX 1
200,000
100,000
-
2006
2008
2010
2012
2014
2016
2018
2020
2022
2024
2026
2028
2030
2032
2034
2036
Year
Comprehensive Major medical
Figure A2 and A3 show number of new lives covered under scenario 1 and 2.
Figures A3 and A4 summarize the expected lives covered under scenario 1 and 2
32Figure A3: New lives covered (scenario 2)
600,000
New lives covered
500,000
400,000
300,000
200,000
100,000
-
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
Year
Comprehensive Major medical
Figure A4: Premiums and claims paid
1,800
1,600
1,400
1,200
$NZD Millions
1,000
800
600
IMPROVING HEALTH OUTCOMES / APPENDIX 1
400
200
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
2036
Year
With KiwiHealth With KiwiHealth No KiwiHealth No KiwiHealth
(Premiums) (Claims) (Premiums) (Claims)
Figure A4 shows the expected premium and claim increase over time, based on historic averages. We note the value
of claims relative premiums have increased in later years and that the estimated value of claims is conservative.
33Appendix 2
Supply side considerations Recent research suggests that
PHI covers the following types of
Whether private provision of
elective surgeries :
elective surgeries will increase
the overall quality of healthcare 1. Elective surgeries that are not
in New Zealand depends on the routinely offered in the public
following two key aspects: healthcare system or offered
only in very severe cases (e.g.
— The level of public/private
varicose veins, and dental
substitution. Would privately
surgery).
funded surgeries have otherwise
been funded by the public 2. Surgeries that are offered
system? publicly, e.g. such as hip and
knee replacements and cardiac
— The elasticity of supply of
bypasses:
resources (surgeons and
healthcare professionals). a) for patients who do not meet
Would the resources used in the the public sector treatment
private system otherwise have threshold; and
been used in the public system?
b) for patients who meet the public
Furthermore, does the existence of sector thresholds but choose
ACC and PHI help attract and retain to use private health services
the supply of skilled healthcare funded by PHI.
professionals to New Zealand.
It can be argued that 2b is the only
The answer is likely to be a mix. pure public/private substitution.
In the short term, the supply of
Research does however suggest
experienced professionals in New
that PHI has, in certain health
Zealand is relatively inflexible, and
systems, ‘injected financial resources
many of them work both privately
into health systems, which has
and publicly.
contributed to the financing of
additional capacity and services’. If
IMPROVING HEALTH OUTCOMES / APPENDIX 2
there is unmet demand for elective
surgeries, and the public system is
not increasing supply to meet the
demand, investments in additional
resource need to come from
elsewhere.
34References Schofield, D et al. (2015), Lost
productive life years caused by
Benartzi, Shlomo; Thaler, Richard
chronic conditions in Australians aged
H (2007), Heuristics and Biases in
45-64 years, 2010-2030. MJA 2013
Retirement Savings Behaviour
(6) 21 September 2015
Business New Zealand and Southern
Schofield, D, et al. (2016), Economic
Cross Health, Wellness in the
costs of chronic disease through
Workplace – Survey Report 2015
lost productive life years (PLYs)
Colombo, F. and N. Tapay (2004), among Australians aged 45–64
“Private Health Insurance in OECD years from 2015 to 2030: results
Countries: The Benefits and Costs from a microsimulation model. BMJ
for Individuals and Health Systems”, Open 2016; 6:e011151. doi:10.1136/
OECD Health Working Papers, No. bmjopen-2016-011151
15, OECD Publishing, Paris
Schofield D, et al. (2017), The costs
Markussen, S. J Popul Econ (2012), of diabetes among Australians
25: 1287. doi:10.1007/s00148-011- aged 45–64 years from 2015 to
0390-8 2030: projections of lost productive
life years (PLYs), lost personal
Ministry of Health (2016)
income, lost taxation revenue,
Overview of the Health System.
extra welfare payments and lost
Available at: http://www.health.
gross domestic product from
govt.nz/new-zealand-health-system/
Health&WealthMOD2030. BMJ
overview-health-syste [Accessed 21
Open 2017;7:e013158. doi:10.1136/
February 2017]
bmjopen-2016-013158
NZIER (2001), The tax treatment of
TDB Advisory (2015),
health insurance premiums. Report
Assessing the net impacts of
to HFANZ
private health insurance.
NZIER (2014), Private health
TNS (2015), Assessing the demand
insurance – An expanding role in the
for Elective Surgery amongst New
future of health care? NZIER report
IMPROVING HEALTH OUTCOMES / APPENDIX 1
Zealanders March 2016
to HFANZ
The Treasury (2002), Treasury Report:
OECD (2017), OECD.stat Health
Costs of Subsidising Private Health
expenditure and financing [Accessed
Insurance
21 February 2017]
Treasury (2016), He Tirohanga
Samuelson, W. & Zeckhauser,
Mokopuna, 2016 Statement on the
R. J (1988), Risk and Uncertainty
long term fiscal position
Schofield, D et al. (2011), Economic
Treasury (2010), The Cost of Ill
impacts of illness in older workers:
Health, New Zealand Treasury
quantifying the impact of illness on
Working Paper 10/04
income, tax revenue and government
spending. BMC Public Health 2011,
11:418
35You can also read