Immune Activation, HIV Persistence, and the Cure
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
IAS–USA Topics in Antiviral Medicine
Perspective
Immune Activation, HIV Persistence, and the Cure
HIV infection is characterized by persistent immune activation, even in the body is contained in the gut. Cross-
context of suppressive antiretroviral therapy. This persistent activation, which communication occurs between mi-
appears to be fueled by microbial translocation from the gut resulting from crobes and epithelial cells or immune
HIV-related damage, is associated with deficits in immune function that in cells as part of a complex system that
turn contribute to persistent activation. The presence of latent HIV reservoirs protects what is essentially the greatest
in lymphoid tissues also provokes immune activation in the context of immune surface area of tissue in contact with
suppression, resulting in expansion of the viral reservoir and potential the outside environment. In HIV infec-
viral replication, even with suppressive antiretroviral therapy. Therapeutic tion, there is a massive loss of CD4+ T
strategies are being devised to reduce persistent immune activation and limit cells in the gut during acute infection,
the size of the HIV reservoir. This article summarizes a presentation by Daniel C. with enteropathy caused by enterocyte
Douek, MD, PhD, at the IAS–USA continuing education program held in San apoptosis and a 2- to 10-fold increased
Francisco, California, in March 2013. permeability (leakiness) of the gut. Gut
permeability allows translocation of
Keywords: HIV, immune activation, persistence, gut, microbial translocation, microbial products into the systemic
reservoir, raltegravir intensification, lymphoid tissue circulation, causing systemic immune
activation.
Viral infection is accompanied by an an altered phenotypic profile, and hy- The emerging picture of the role of
innate immune response during the perimmunoglobulinemia. microbial translocation from the gut in
acute phase of infection. For most With regard to the causes of chronic fueling persistent immune activation is
types of viral infection, immune acti- immune activation in HIV infection, it of a cyclic process in which more acti-
vation is reduced as the immune re- does not appear that HIV alone can ac- vated T cells are produced, providing
sponse acts to reduce viral load. In count for the persistence of immune ac- more target cells for HIV, and resulting
HIV infection, however, immune acti- tivation. In HIV infection, viral load is a in immune deficiency via increased
vation persists despite the initial de- poor predictor of disease progression, infection of the T cells, low thymic
cline in viral load. Persistent activation whereas measures of immune activa- output, lymphoid tissue fibrosis, and
is observed in numerous components tion, including the frequency of acti- T and B cell dysfunction (Figure 2).
of the innate immune system, includ- vated T cells, are independent predic- Increased immune deficiency results
ing cells (eg, activated phenotypes of tors of progression. Elite controllers— in persistent microbial translocation
macrophages and dendritic cells), cy- individuals who, in the absence of ther- and poor pathogen control, allowing
tokines and chemokines (tumor necro- apy, spontaneously control viral repli- other viruses (eg, cytomegalovirus)
sis factor, interleukin [IL]-1, IL-6, IL-8, cation to undetectable levels—exhibit and bacteria to replicate and further
IL-15, and IL-10), acute phase proteins high levels of activated CD38+ CD8+ priming immune activation. Ongoing
(serum amyloid A, C-reactive protein), T cells on progression.1 Further, when immune activation results in systemic
elements of the coagulation cascade viral load is suppressed with anti- inflammation, tissue damage (includ-
(D-dimers, tissue factor), elements of retroviral therapy, immune activation ing fibrosis of lymphoid tissue) in the
fibrosis (matrix metalloproteinase acti- persists and is predictive of disease heart, lungs, liver, and kidneys, and
vation, collagen deposition), and mi- progression. Potential contributors to coagulopathy, all of which are associ-
crobial sensors (lipopolysaccharide chronic immune activation include ated with non–HIV-related morbidity
binding protein, soluble CD14). In the increased antigen load, bacterial over- and mortality. By controlling HIV rep-
adaptive immune system, there is in- growth, the presence of herpes viruses, lication, antiretroviral therapy subdues
creased turnover and exhaustion of and translocation of proinflammatory some of these processes and allows
T cells, low thymic output, and estab- mediators across the gut mucosa. recovery of some T cell populations.
lishment of a viral reservoir. Similarly, However, it does not stop immune ac-
there is increased turnover of B cells, tivation, resultant inflammation, or tis-
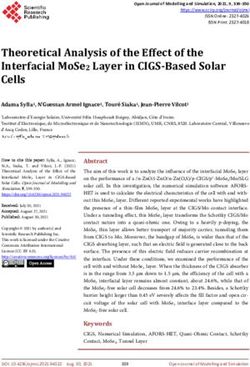
Consequences of HIV Infection
sue damage completely.
in the Gastrointestinal Tract
As shown by Hunt and colleagues,1,2
Dr Douek is Chief of the Human Immunol- A healthy gut is characterized by T cell activation does decline during
ogy Section at the National Institutes of tight epithelial junctions and a layer antiretroviral therapy but remains at
Health in Bethesda, Maryland. Dr Douek’s
of mucus (Figure 1). Antimicrobial higher than normal levels even after
presentation for the IAS–USA was per-
formed in the capacity of a private citizen peptides and large quantities of anti- many years of viral suppression. The
and does not necessarily reflect the views bodies are secreted into the lumen. higher the level of immune activa-
of the US government. The majority of CD4+ T cells in the tion (indicated by the percentage of
128Immune Activation, HIV Persistence, Cure Volume 21 Issue 4 September/October 2013
CD4+ T cell
Epithelial layer
|||
O OO
CD8+ T cell
O
O
||
|
| | | |O| | | | |O| |O| |O| | O|O
Loss of tight epithelial junctions
O| |
B cell
O
O
O O
| | | | |
Infected CD4+ T cell
O
O O O
Macrophage
| |O|O| | | | O| O
O
OOO
|O |O
O
O O
O|
O | |
|O |
O
| | | |
Dendritic cell
O O O O
Mucus layer
O
O O
| | O
Secretory immunoglobulin A
O
O
|O |
|O | |
O|
Commensal bacterium
O
O
O|
| |O
O
| |O O O
|
O
OO
Microfold cell
| |
O | |
Loss of CD4+ T cells
O
O
| | |O
O
O O Microbial translocation High endothelial venules
Enterocyte apoptosis
Defensin
Figure 1. The effects of HIV infection in the gastrointestinal tract. Adapted from Mowat,12 and Brenchley and Douek.13
activated CD38+ CD8+ T cells persist- in a substantially greater reduction in gut tissues than in peripheral blood
ing during antiretroviral therapy), the immune activation (higher percent- and reduced viral persistence (mea-
lower the recovery of CD4+ T cell lev- age of CD38+ memory CD8+ T cells) sured as HIV RNA level) in the terminal
els. Overall, these investigators have than standard antiretroviral therapy.4 ileum.8
shown that numerous markers of in- Another study showed that raltegravir
flammation and gut barrier dysfunc- intensification resulted in a substantial Ongoing HIV Replication During
tion are associated with an increased reduction in the viral reservoir of la-
Antiretroviral Therapy?
risk of mortality among HIV-infected tently infected memory CD4+ T cells
patients, independent of CD4+ cell (reduction in infectious units per mil- Although complete inhibition of viral
count and viral load (Figure 3).3 For ex- lion cells, or IUPM) and in CD8+ T cell replication is an unlikely curative strat-
ample, elevated blood levels of intesti- activation in patients with viral sup- egy for HIV infection, all functional
5 cure strategies are based on first hav-
nal fatty acid binding protein (iFABP), pression. However, yet another study
a marker of damage in the gut epithe- showed that the addition of raltegravir ing achieved complete suppression of
lial lining, are associated with an 8-fold to an antiretroviral regimen did not fur- virus. There are substantial data that
increased risk of mortality among HIV- ther reduce low-level plasma viremia indicate HIV replication is not ongoing
infected patients. and found no association between per- during suppressive antiretroviral thera-
sistence of plasma HIV RNA levels and T py, but there are also data that suggest
6
Immune Activation and HIV cell activation.
Persistence One explanation
Immune deficiency
for the seemingly
I I
I
I
In addition to the other deleterious
I
I
divergent findings
I
I
I
I
I
Gut
I
I
I I
effects noted, persistent inflamma- with raltegravir in-
I
I
I
I
I
I
I I
I I
tion appears to be associated with tensification may
I
I
I
I
I TEM Other
I
I
the persistence of HIV. Ongoing HIV be that its effects
I
I
HIV
I
and viruses
I
I I
I
replication in host reservoirs also ap- are more promi-
I
TCM (eg, CMV)
I
I
I
I
I I
I
pears to contribute to persistent in- nent in gut tissue
I
I
I
I
I
I
I
I
I
flammation. Research is under way
I
than in peripheral
I
I
Immune activation
I I
I
to determine whether novel investi- blood. A number of
I
I
I
gational approaches can reduce HIV
I
studies have shown
reservoir size, through, for example, a strong association Low thymic output Systemic inflammation
the use of antiinflammatory drugs or between cell-based Lymphoid tissue fibrosis
I
Tissue damage
I
by enhancement of HIV-specific im- T and B cell dysfunction Coagulopathy
I
measures of viral
I
I
I
munity. persistence and T
I
I
I
I I
An association between HIV per- cell activation in
sistence and persistent immune acti- gastrointestinal tis- Non–HIV-related morbidity and mortality
vation in patients with undetectable 7
sue. As shown in
plasma HIV RNA levels has been shown Figure 4, raltegra- Figure 2. The role of microbial translocation from the gut in fuel-
in studies of raltegravir intensification. vir intensification ing immune activation. CMV indicates cytomegalovirus; TCM, cen-
In one study, antiretroviral therapy reduced immune tral memory T cells; TEM, effector memory T cells. Adapted from
with raltegravir intensification resulted activation more in Klatt et al.14
129IAS–USA Topics in Antiviral Medicine
iFABP 8.3 controllers, who may ex- mucosal damage at the gut surface.
0.24
hibit immune activation These problems can result in immune
Zonulin
and disease progression, suppression, with subsequent poor
4.6
KT ratio patients in the VISCONTI control of pathogens (eg, Streptococ-
sCD14 16 study had very low levels of cus, Staphylococcus, herpes viruses),
70 T cell activation. A potential even in patients with low or undetect-
IL-6
30
implication of these findings able HIV RNA levels.
D-dimer
is that very early treatment Immune activation affects the reser-
9
TNF R1 limits the size of the latent voir of HIV, even in patients taking an-
hsCRP 11 viral reservoir, which thus tiretroviral therapy. It causes the gen-
limits the magnitude of im- eration of activated T cells, the tar-
0.01 0.1 1 10 100 1000
mune activation from the get cells for the virus. Cells that are
Probability of Mortality in 4th vs 1st Quartile
outset, potentially providing already infected with HIV will prolif-
a lower set point for ongoing erate, producing more HIV-infected
Figure 3. Markers of inflammation and gastrointes- inflammation. cells and expanding the viral reser-
tinal dysfunction that predict mortality in HIV in- voir. Viral transcription may begin,
fection. hsCRP indicates high-sensitivity C-reactive
Relationship Between and some viral replication may occur.
protein; iFABP, intestinal fatty acid binding protein;
There is increasing evidence of the
IL, interleukin; KT, kynurenine-to-tryptophan; sCD14, HIV-Specific Immunity
soluble CD14; TNF R1, tumor necrosis factor receptor 1. risk of new infection events, even in
and HIV Persistence
Adapted with permission from Hunt et al.3 patients taking fully suppressive anti-
Ongoing immune activation retroviral therapy. This increase in HIV
ongoing replication occurs and is as- adversely affects the HIV-specific T cell replication results in further immune
sociated with immune activation. In response, as well as overall CD4+ T activation and, because the patient
determining whether ongoing HIV rep- cell reconstitution. Thus, ongoing im- remains in an immune-suppressed
lication takes place, the source of the mune activation may interfere with state, poor immune control of newly
sample and the assay used to measure reconstitution of the HIV-specific T cell produced virus. Antiretroviral therapy
viral reservoir are crucial. Blood tests response. An example of the potential can profoundly reduce viral replica-
may indicate the absence of ongoing relationship between HIV-specific im- tion but does not eliminate residual
viral replication, whereas gut or other munity in the gut and viral persistence immune activation nor stop the rep-
lymphoid tissue assays that are sensi- is provided in a study by Hatano and lication of virus-containing cells or
tive enough to detect to 1 viral copy per colleagues.10 The study showed that in the expansion of the viral reservoir
million cells may demonstrate ongoing patients taking antiretroviral therapy,
replication. Lymphoid tissue is likely a stronger HIV-specific T cell response 5
the major HIV reservoir in patients on in the gut mucosa was associated with
CD38+ HLA-DR+ Level
(% of CD8+ T Cells)
0
antiretroviral therapy. The gut is actually lower levels of proviral DNA in periph-
the largest lymphoid tissue in the body, eral blood mononuclear cells (PBMCs). -5
but widespread destruction of CD4+ T
cells in the gut make the lymph nodes -10
Model for Immune Activation
or spleen the more likely primary viral
and HIV Persistence
C
um
um
n
um
-15
lo
M
reservoir during chronic infection. It is Co
en
Ile
ct
PB
Re
od
Du
in these tissues that evidence of viral If the mechanisms for the associa- Location
reservoir expansion and resultant ongo- tion between immune activation and
ing immune activation can be found. HIV persistence can be identified, it 2000
(copies/million CD4+ T cells)
Results of the recently reported may be possible to direct therapeu-
0
HIV RNA Level
VISCONTI (Viro-Immunological Sus- tic strategies at these mechanisms.
tained Control after Treatment Inter- Figure 5 shows a potential model for -2000
ruption) study9 indicate an association more fully explaining HIV pathogen-
-4000
between ongoing viral replication and esis in a way that incorporates persis-
C
um
um
on
um
M
immune activation. In this study, 14 tent immune activation and the role of
ol
en
ile
ct
PB
-6000
tc
Re
od
al
gh
in
Du
patients started taking antiretroviral the viral reservoir in fueling immune
Ri
mr
Te
therapy soon after HIV infection and activation. Persistent immune activa- Location
continued it for many years. When tion causes many problems in the im-
antiretroviral therapy was stopped, mune system, including low thymic
Figure 4. The effects of raltegravir inten-
the patients did not exhibit viral re- output, lymphoid tissue fibrosis, poor sification on immune activation (top) and
bound. Like elite controllers, these pa- immune reconstitution and renewal HIV RNA levels (bottom) in peripheral blood
tients had very low levels of cell-asso- of CD4+ T cells, and dysfunction of T mononuclear cells (PBMCs) and gut tissue
ciated HIV DNA. However, unlike elite and B cells. It also continues to cause sites. Adapted from Yukl et al.8
130Immune Activation, HIV Persistence, Cure Volume 21 Issue 4 September/October 2013
Immune suppression enhance T cell re- therapy intensification. It is also pos-
newal, antifibrotic sible that gene therapy could be used
Poor control of pathogens drugs, anti-aging to reduce the viral reservoir. It has
Translocation of microbial
products strategies, antiin- already been shown that stem-cell
flammatory agents, transplants can lead to a reduction in
Target cell generation Low thymic output and anticoagulants the size of the viral reservoir (ie, in
Infected cell proliferation Lymphoid tissue fibrosis (Table). Combination the Berlin patient11), serving as proof
Virus transcription Immune activation Poor CD4+ cell renewal
Virus production T and B cell dysfunction
approaches will like- of principle that such genetic ap-
New infection events Mucosal damage ly be necessary to proaches may be viable. Drugs with
reduce persistent biologic activity against latent virus
HIV infection
immune activation exist and are being assessed, and vac-
and counteract its cines may be developed to enhance
Effects of HIV infection effects in the body, host clearance mechanisms (ie, by
given the multifac- boosting the damaged HIV-specific
torial pathogenesis immune response). As noted, a com-
Figure 5. The central role of persistent immune activation in HIV
infection. Adapted from Klatt et al.14 of HIV infection. bination of approaches will be neces-
sary to address the many aspects of
that can result from persistent im- Conclusion: In the Context of HIV infection and persistent immune
mune activation. a Cure activation.
Although this picture of pathogen-
esis may appear daunting with regard Numerous mechanisms contribute to Presented by Dr Douek in March 2013. First
to achieving a cure for HIV infection, HIV persistence, many of which are cur- draft prepared from transcripts by Matthew
it actually suggests many points in the rently being addressed therapeutical- Stenger. Reviewed and edited by Dr Douek in
processes underlying persistent im- ly. The unifying theme in these efforts October 2013.
mune activation that can serve as ther- is to reduce the size of the HIV reser-
Financial Affiliations: Dr Douek has no rel-
apeutic targets. Among the therapeutic voir. Strategies to achieve this include
evant financial affiliations to disclose.
interventions in development are che- reducing persistent inflammation and
mokine receptor inhibitors, antiinfec- increasing immune function, potential-
tive therapies, drugs that may reduce ly including the strategies of early an- References
microbial translocation, drugs that may tiretroviral therapy and antiretroviral
1. Hunt PW, Brenchley J, Sinclair E, et al. Re-
lationship between T cell activation and
Table. Therapeutic Interventions in Development to Reduce Persistent Immune CD4+ T cell count in HIV-seropositive in-
Activation dividuals with undetectable plasma HIV
RNA levels in the absence of therapy.
Intervention Examples J Infect Dis. 2008;197:126-133.
2. Hunt PW, Martin JN, Sinclair E, et al. T
Antiinfective therapy Cytomegalovirus, Epstein-Barr virus, herpes simplex cell activation is associated with lower
virus, HCV/HBV CD4+ T cell gains in human immunode-
ficiency virus-infected patients with sus-
Antiaging Caloric restriction, sirtuin activators, vitamin D, tained viral suppression during antiretro-
omega-3 fatty acids, rapamycin, diet, exercise viral therapy. J Infect Dis. 2003;187(10):
1534-1543.
Enhance T-cell renewal Growth hormone, interleukin 7
3. Hunt P, Rodriguez B, Shive C, et al. Gut
Chemokine receptor inhibitors Maraviroc, cenicriviroc epithelial barrier dysfunction, inflamma-
Microbial translocation Sevelamer, colostrum, rifaximin tion, and coagulation predict higher mor-
tality during treated HIV/AIDS [Abstract
Antifibrotic drugs or agents Pirfenidone, angiotensin-converting enzyme inhibitors, 278]. 19th Conference on Retroviruses
angiotensin receptor blockers, keratinocyte growth and Opportunistic Infections (CROI).
factor March 5-8, 2012; Seattle, Washington.
4. Llibre JM, Buzon MJ, Massanella M, et al.
Anticoagulants Low-dose warfarin, dabigatran, aspirin, clopidogrel Treatment intensification with raltegravir
Antiinflammatory drugs Chloroquine, hydroxychloroquine in subjects with sustained HIV-1 virae-
mia suppression: a randomized 48-week
Minocycline study. Antivir Ther. 2012;17(2):355-364.
NSAIDs: COX-2i, aspirin 5. Vallejo A, Gutierrez C, Hernandez-Novoa
Statins B, et al. The effect of intensification
with raltegravir on the HIV-1 reser-
Methotrexate voir of latently infected memory CD4
Thalidomide, lenalidomide, pentoxyfyline (weak TNF T cells in suppressed patients. AIDS.
2012;26(15):1885-1894.
inhibitors) 6. Ghandi RT, Zheng L, Bosch RJ, et al. The
Biologics TNF inhibitors, interleukin 6 inhibitors, anti–alpha- effect of raltegravir intensification on
interferon antibodies, anti-PD1 antibodies low-level residual viremia in HIV-infected
patients on antiretroviral therapy: a ran-
COX-2i indicates cyclooxygenase-2 inhibitor; HCV, hepatitis C virus; NSAID, nonsteroidal domized controlled trial. PLoS Clin Trials.
antiinflammatory drug; PD1, programmed death 1; TNF, tumor necrosis factor. 2010;7(8):pii:e1000321.
131IAS–USA Topics in Antiviral Medicine
7. Sheth PM, Yi TJ, Kovacs C, et al. Mucosal HIV-infected patients with a subopti- Additional Suggested Reading
correlates of isolated HIV semen shed- mal CD4+ T cell response. J Infect Dis.
ding during effective antiretroviral thera- 2011;203(7):960-968. Armah KA, McGinnis K, Baker J, et al.
py. Mucosal Immunol. 2012;5(3):248-257. 11. Hutter G, Nowak D, Mossner M, et al. HIV status, burden of comorbid disease,
8. Yukl SA, Shergill AK, McQuaid K, et al. Ef- Long-term control of HIV by CCR5 Del- and biomarkers of inflammation, altered
fect of raltegravir-containing intensifica- ta32/Delta32 stem-cell transplantation. coagulation, and monocyte activation. Clin
tion on HIV burden and T-cell activation N Engl J Med. 2009;360(7):692-698. Infect Dis. 2012;55(1):126-136.
in multiple gut sites of HIV-positive adults 12. Mowat AM. Anatomical basis of tolerance
on suppressive antiretroviral therapy. and immunity to intestinal antigens. Nat Deeks SG, Autran B, Berkhout B, et al. To-
AIDS. 2010;24(16):2451-2460. Rev Immunol. 2003;3(4):331-341. wards an HIV cure: a global scientific strat-
egy. Nat Rev Immunol. 2012;12(8):607-614.
9. Saez-Cirion A, Bacchus C, Hocqueloux L, 13. Brenchley JM, Douek DC. HIV infec-
et al. Post-treatment HIV-1 controllers tion and the gastrointestinal immune Sandler NG, Douek DC. Microbial transloca-
with a long-term virological remission af- system. Mucosal Immunol. 2008;1(1): tion in HIV infection: causes, consequences
ter the interruption of early initiated anti- 23-30. and treatment opportunities. Nat Rev Micro-
retroviral therapy ANRS VISCONTI Study. 14. Klatt NR, Chomont N, Douek DC, Deeks biol. 2012;10(9):655-666.
PLoS Pathog. 2013;9(3):e1003211. SG. Immune activation and HIV per-
10. Hatano H, Hayes TL, Dahl V, et al. A ran- sistence: implications for curative ap-
domized, controlled trial of raltegravir proaches to HIV infection. Immunol Rev. Top Antivir Med. 2013;21(4):128-132
intensification in antiretroviral-treated, 2013;254(1):326-342. ©2013, IAS–USA
132You can also read